Vitamin E
In human RCTs, doses equal to or lower than 200 IU daily are associated with slightly reduced all cause mortality, Higher doses are associated with neutral or slightly increased all cause mortality.
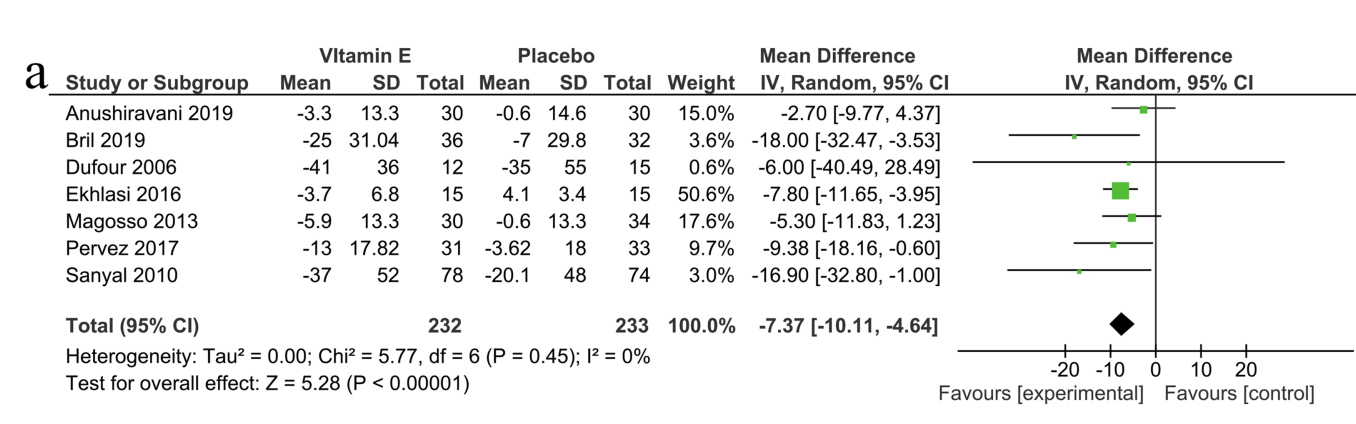
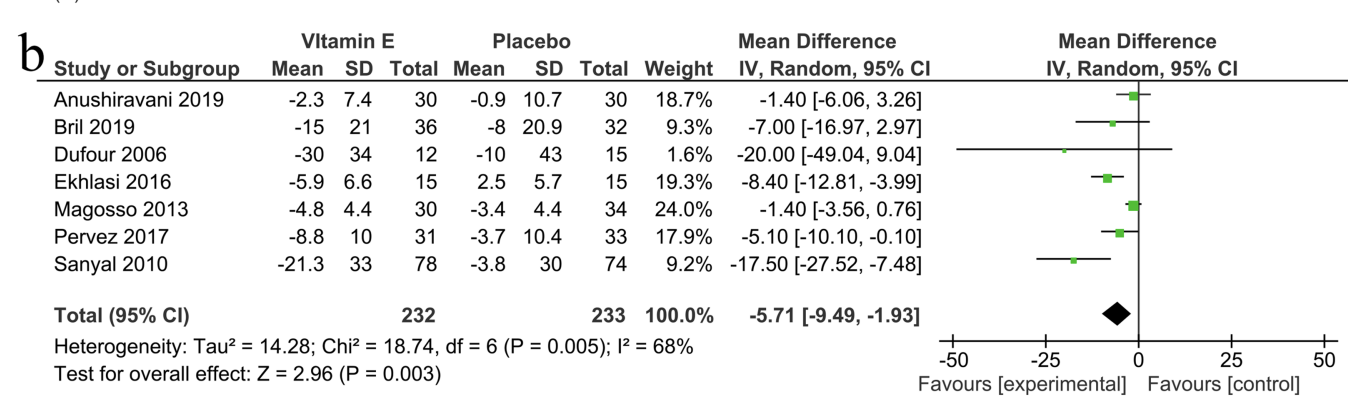
In NAFLD/NASH patients, vit E supplementation reduced the values of liver enzymes compared to placebo ALT (−7.37 IU/L, 95% CI: −10.11 to −4.64), and AST (−5.71 IU/L, 95% CI: −9.49 to −1.); significantly improved liver function and histology.
Supplementation lowered HS-CRP significantly -0.62 mg/l (95% confidence interval=−0.92, −0.31; P<0.001). Lowered IL-6 in individuals with insulin resistance.
One mice study reported +15% increased lifespan, another reported neutral.
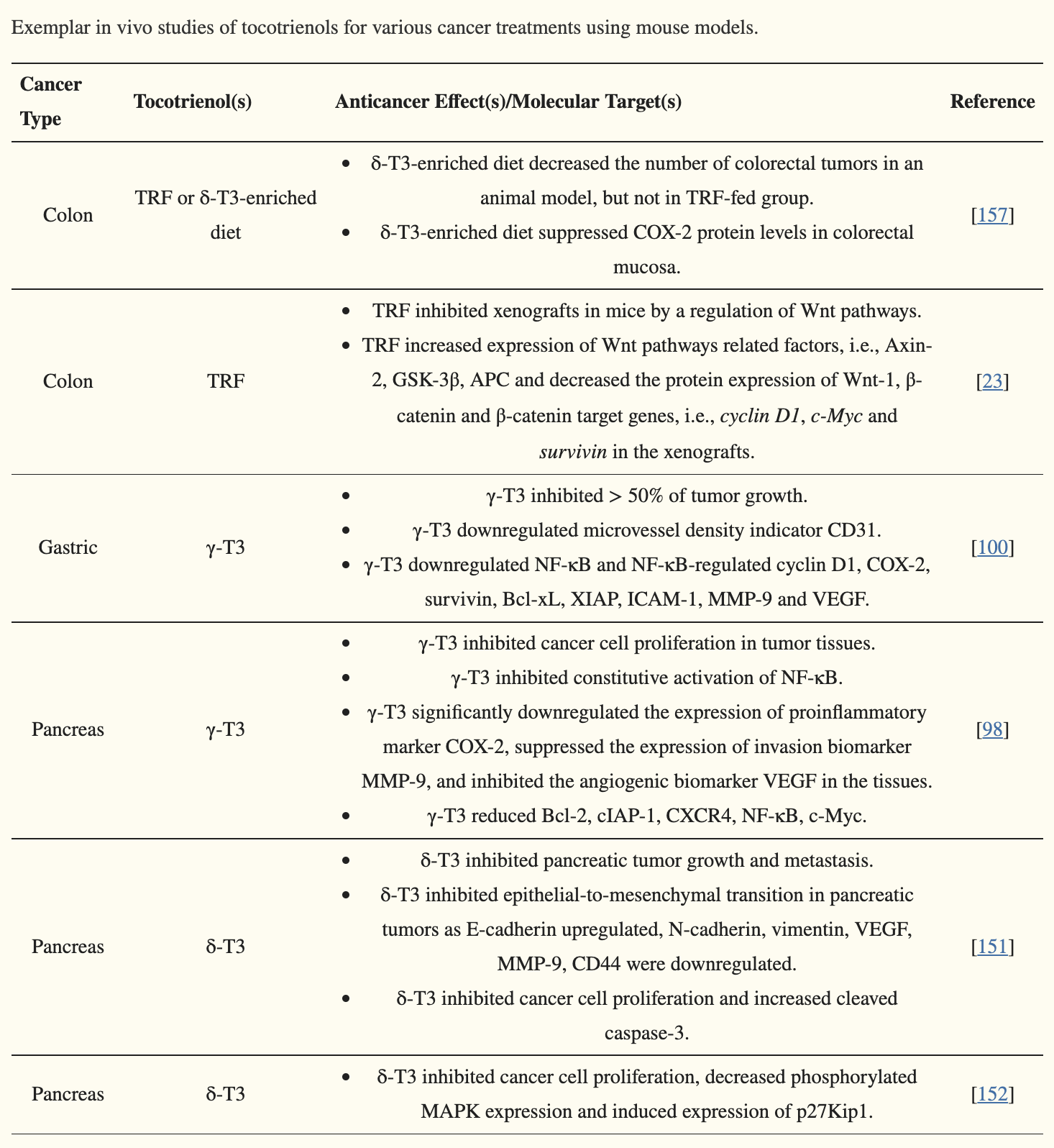
Delta-tocotrienol: Have promising anti-cancer evidence from cell and mice studies.
Alpha-tocopherol: Evidence on cancer is mixed, close to neutral. Most and largest studies show no effect. There’s one large study which found detrimental effects on prostate cancer. One study with head-and-neck cancer found increased risk of recurrence and secondary cancers with 400IU/day.
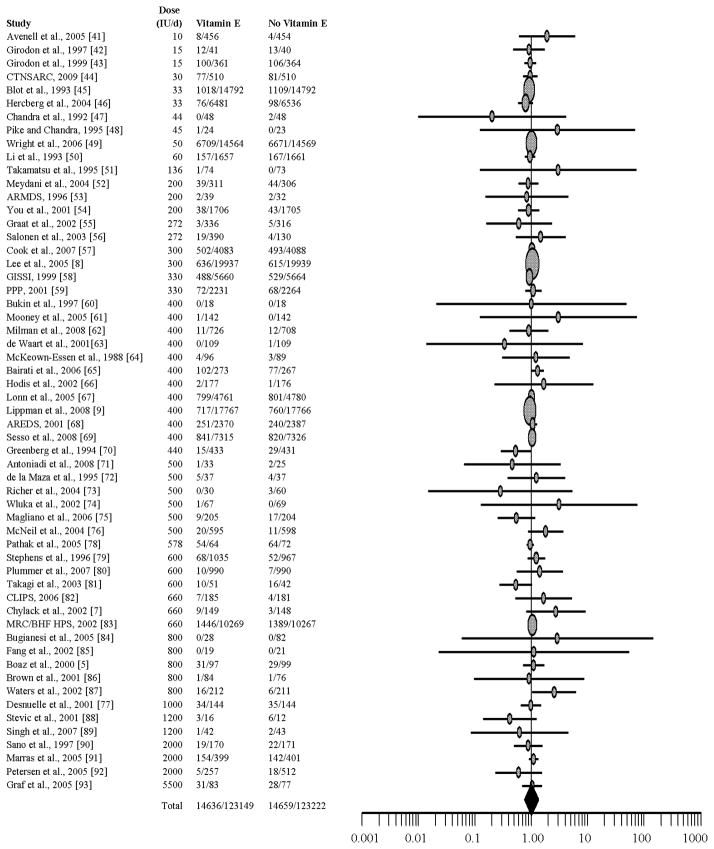
Vitamin E and all-cause mortality: A meta-analysis, 2011
The current analysis reexamines the relationship between supplemental vitamin E and all-cause mortality. All randomized, controlled trials testing the treatment effect of vitamin E supplementation in adults for at least one year were sought. MEDLINE, the Cochrane Library, and Biological Abstracts databases were searched using the terms “vitamin E,” “alpha-tocopherol,” “antioxidants,” “clinical trial,” and “controlled trial” for studies published through April 2010; results were limited to English, German, or Spanish language articles. Studies were also obtained through reference mining. All randomized controlled trials using vitamin E, with a supplementation period of at least one year, to prevent or treat disease in adults were identified and abstracted independently by two raters. Mortality data from trials with a supplementation period of at least one year were pooled. The selected trials (n = 57) were published between 1988 and 2009. Sample sizes ranged from 28 to 39,876 (median = 423), yielding 246,371 subjects and 29,295 all-cause deaths. Duration of supplementation for the 57 trials ranged from one to 10.1 years (median = 2.6 years). A random effects meta-analysis produced an overall risk ratio of 1.00 (95% confidence interval: 0.98, 1.02); additional analyses suggest no relationship between dose and risk of mortality. Based on the present meta-analysis, supplementation with vitamin E appears to have no effect on all-cause mortality at doses up to 5,500 IU/d.
Studies ranked from low dose to high dose:
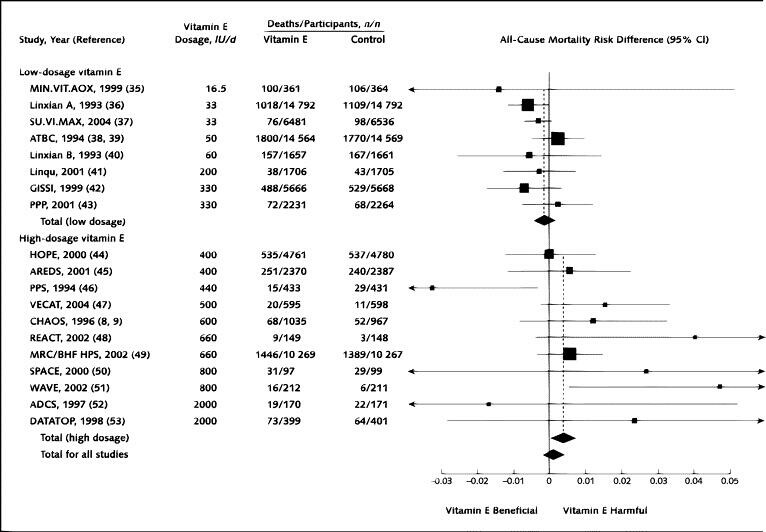
Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality, 2005
Abstract
Background: Experimental models and observational studies suggest that vitamin E supplementation may prevent cardiovascular disease and cancer. However, several trials of high-dosage vitamin E supplementation showed non-statistically significant increases in total mortality.
Purpose: To perform a meta-analysis of the dose-response relationship between vitamin E supplementation and total mortality by using data from randomized, controlled trials.
Patients: 135,967 participants in 19 clinical trials. Of these trials, 9 tested vitamin E alone and 10 tested vitamin E combined with other vitamins or minerals. The dosages of vitamin E ranged from 16.5 to 2000 IU/d (median, 400 IU/d).
Data sources: PubMed search from 1966 through August 2004, complemented by a search of the Cochrane Clinical Trials Database and review of citations of published reviews and meta-analyses. No language restrictions were applied.
Data extraction: 3 investigators independently abstracted study reports. The investigators of the original publications were contacted if required information was not available.
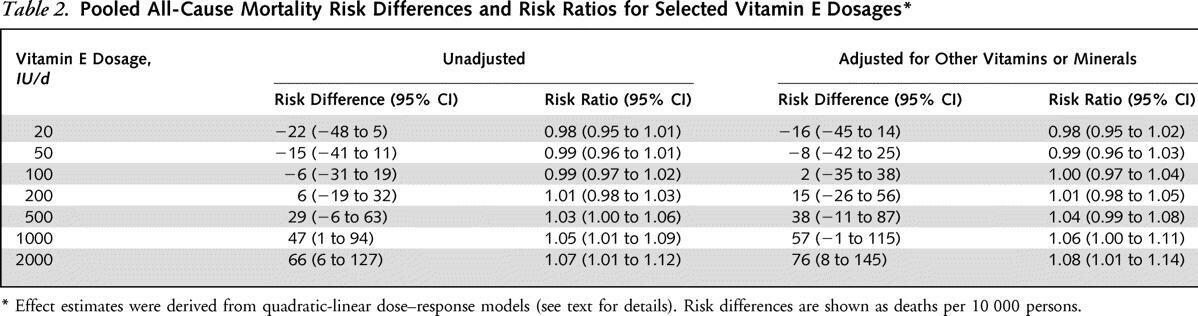
Data synthesis: 9 of 11 trials testing high-dosage vitamin E (> or =400 IU/d) showed increased risk (risk difference > 0) for all-cause mortality in comparisons of vitamin E versus control. The pooled all-cause mortality risk difference in high-dosage vitamin E trials was 39 per 10,000 persons (95% CI, 3 to 74 per 10,000 persons; P = 0.035). For low-dosage vitamin E trials, the risk difference was -16 per 10,000 persons (CI, -41 to 10 per 10,000 persons; P > 0.2). A dose-response analysis showed a statistically significant relationship between vitamin E dosage and all-cause mortality, with increased risk of dosages greater than 150 IU/d.
Limitations: High-dosage (> or =400 IU/d) trials were often small and were performed in patients with chronic diseases. The generalizability of the findings to healthy adults is uncertain. Precise estimation of the threshold at which risk increases is difficult.
Conclusion: High-dosage (> or =400 IU/d) vitamin E supplements may increase all-cause mortality and should be avoided.
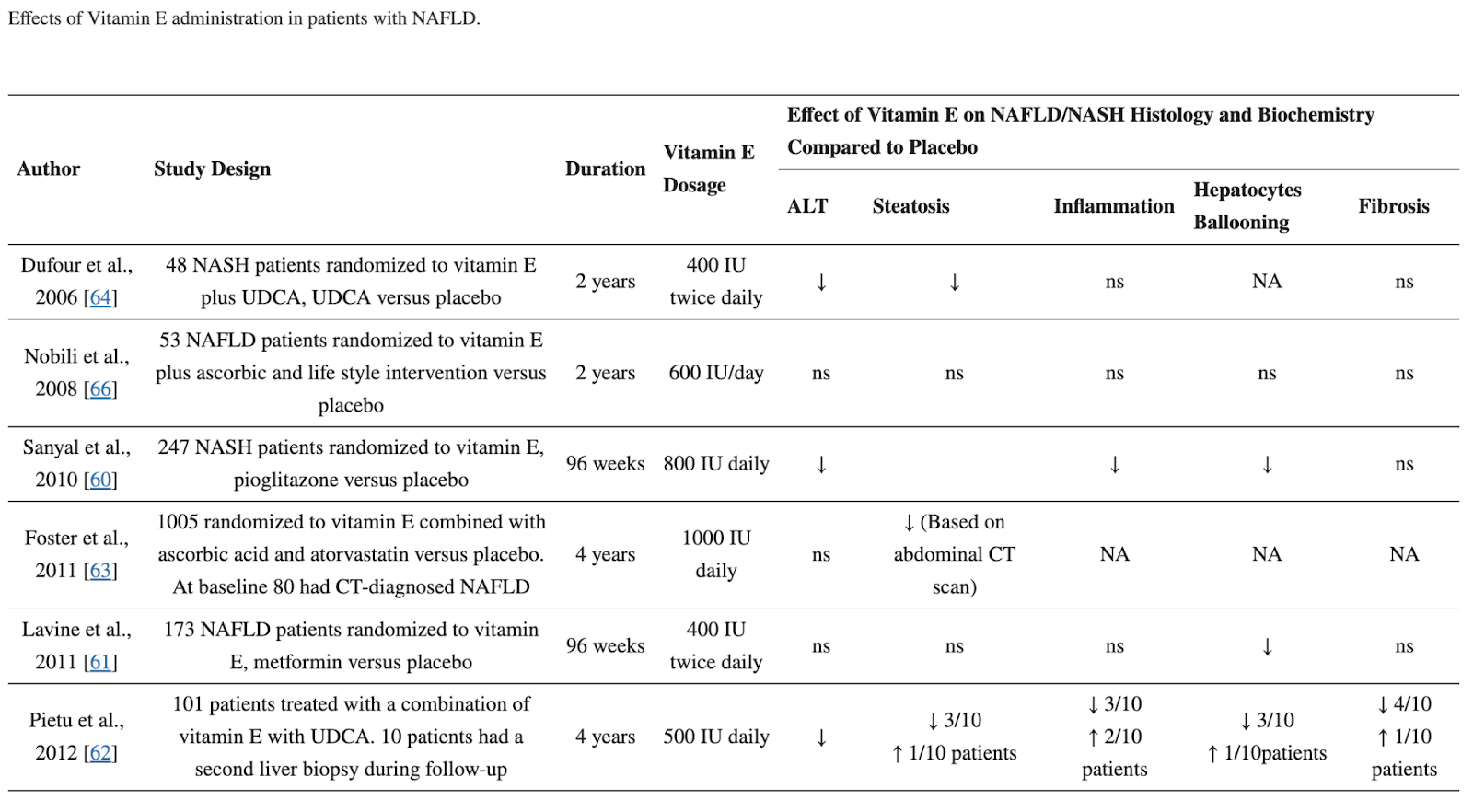
Vitamin E as a Treatment for Nonalcoholic Fatty Liver Disease: Reality or Myth? 2018
Vitamin E is a potent antioxidant that has been shown to reduce oxidative stress in NAFLD.
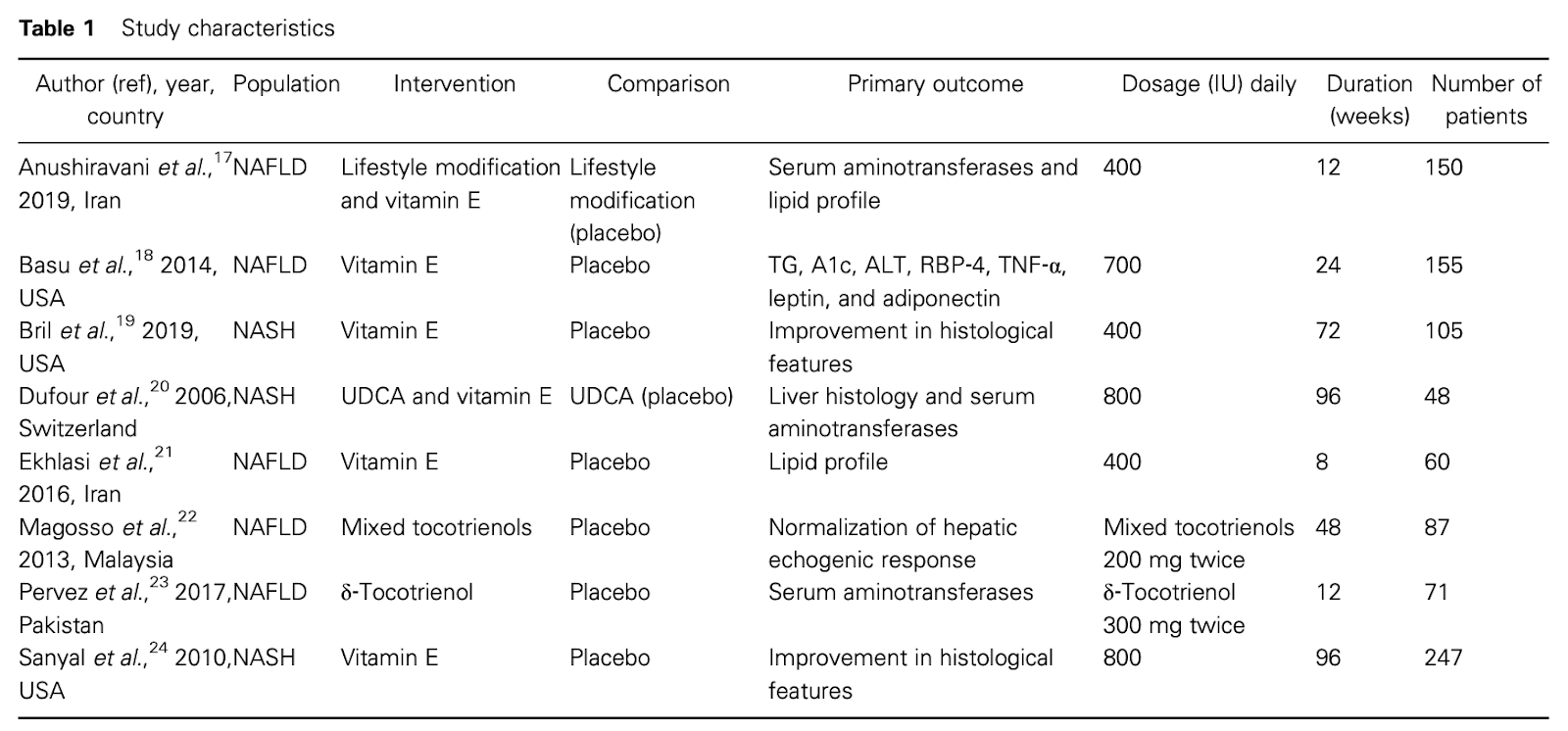
Systematic review with meta-analysis: The effect of vitamin E supplementation in adult patients with non-alcoholic fatty liver disease, 2021
Νon-alcoholic fatty liver disease (NAFLD) is estimated to be the most common cause of end-stage liver disease in the next years. Vitamin E has shown beneficial effects as a possible “scavenger” of oxidative stress products, which play a major role in pathogenesis of the disease. The purpose of the present meta-analysis is to investigate the effects of vitamin E supplementation in biochemical and histological parameters in adult patients with NAFLD.
Methods
Literature search was performed in major electronic databases (MEDLINE, CENTRAL, and Embase) up to June 2020 for randomized clinical trials, which examined vitamin E versus placebo treatment in adults with NAFLD. Changes in liver enzymes were considered as primary outcomes while changes in histological, biochemical, and metabolic parameters as secondary. Quality of evidence was assessed through risk of bias according to the Cochrane risk of bias tool.
Results
Eight studies were included in qualitative analysis and seven in quantitative analysis. Vitamin E reduced the values of liver enzymes compared with placebo (−7.37 IU/L, 95% confidence interval: −10.11 to −4.64 for alanine aminotransferase, and −5.71 IU/L, 95% confidence interval: −9.49 to −1.93 for aspartate aminotransferase). Additionally, vitamin E improved statistically significantly liver pathology in every individual histological parameter as well as low-density lipoprotein cholesterol, fasting blood glucose, and serum leptin values.
Conclusions
Vitamin E can improve biochemical and histological characteristics of NAFLD patients, especially of non-alcoholic steatohepatitis patients. The results indicate that vitamin E could be a promising choice and be considered as a treatment option in patients with NAFLD.
Forest plots of the effect of vitamin E in (a) alanine aminotransferase and (b) aspartate aminotransferase.
Effects of Delta-tocotrienol Supplementation on Liver Enzymes, Inflammation, Oxidative stress and Hepatic Steatosis in Patients with Nonalcoholic Fatty Liver Disease, 2018
Background/aims: Non-alcoholic fatty liver disease (NAFLD) is a growing public health problem worldwide and is associated with increased morbidity and mortality. Currently, there is no definitive treatment for this disease. δ-Tocotrienol has potent anti-inflammatory and antioxidant properties and may reduce liver injury in NAFLD. The present study aims to evaluate the efficacy and safety of δ-tocotrienol in the treatment of NAFLD.
Materials and methods: The present study was a randomized, double-blind, placebo-controlled pilot study conducted in patients aged > 20 years, belonging to both sexes, having ultrasound-proven fatty liver disease, having a fatty liver index (FLI) of ≥ 60, and persistent elevation of alanine transaminase. A total of 71 patients were assigned to receive either oral δ-tocotrienol (n=35, 300 mg twice daily) or placebo (n=36) for 12 weeks. At the baseline and at the end of the study, clinical and biochemical parameters, including lipid profile, liver function tests, high-sensitivity C-reactive protein (hs-CRP), and malondialdehyde (MDA) were measured. Body mass index and FLI were calculated, and ultrasound grading of hepatic steatosis was performed.
Results: Out of 71 enrolled patients, 64 patients, 31 in the δ-tocotrienol group and 33 in the placebo group, completed the study. After 12 weeks of supplementation, δ-tocotrienol showed greater efficacy than placebo by decreasing serum aminotransferases, hs-CRP, MDA, and FLI score (p<0.001). However, it did not improve hepatic steatosis on ultrasound examination. No adverse effects were reported.
Conclusion: δ-Tocotrienol was safe, and it effectively improved aminotransferase levels and inflammatory and oxidative stress markers in patients with NAFLD. Large-scale randomized clinical trials are warranted to further support these findings.
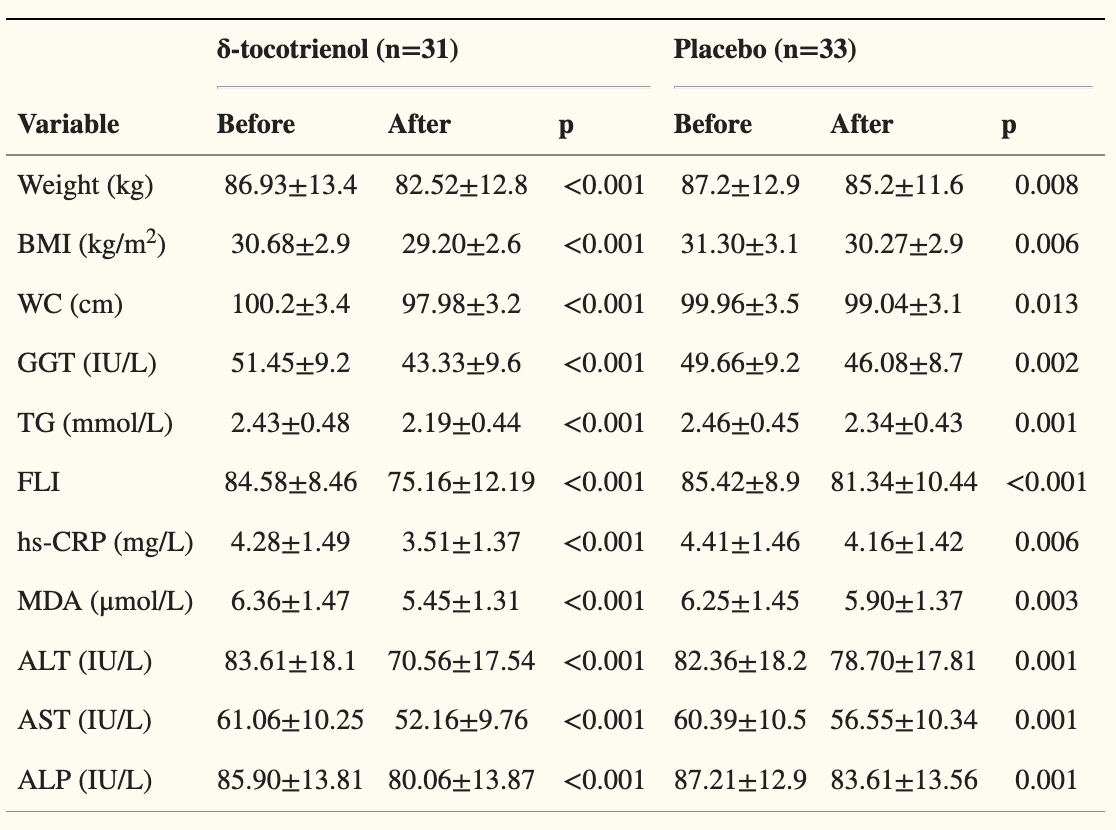
(FLI = Fatty liver index)
Tocotrienols for normalisation of hepatic echogenic response in nonalcoholic fatty liver: a randomised placebo-controlled clinical trial, 2013
Eighty-seven untreated hypercholesterolaemic adults with ultrasound-proven NAFLD were enrolled and randomised into control group (n = 44) and tocotrienols group (n = 43). The treatment, either mixed tocotrienols 200 mg twice daily or placebo, had a 1-year duration.
Normalisation of hepatic echogenic response, being the trial primary aim, was used in sample size calculations. The data were assessed according to intention to treat principle as primary outcome. Per protocol analysis was also carried out as secondary outcome measurement.
Results
Thirty and 34 participants concluded the study in the tocotrienols and placebo group respectively. Alpha-tocopherol levels were within the normal range for all subjects. As primary outcome, the normalisation of hepatic echogenic response was significantly higher for the tocotrienols treated group compared to the placebo group in the intention to treat analysis (P = 0.039; 95% CI = 0.896-6.488). As secondary objective, the per protocol assessment also showed significant rate of remission (P = 0.014; 95% CI = 1.117-9.456). Worsening of NAFLD grade was recorded in two patients in the placebo group, but none in the group treated with tocotrienols. No adverse events were reported for both groups.
Conclusion
This is the first clinical trial that showed the hepatoprotective effects of mixed palm tocotrienols in hypercholesterolemic adults with NAFLD.
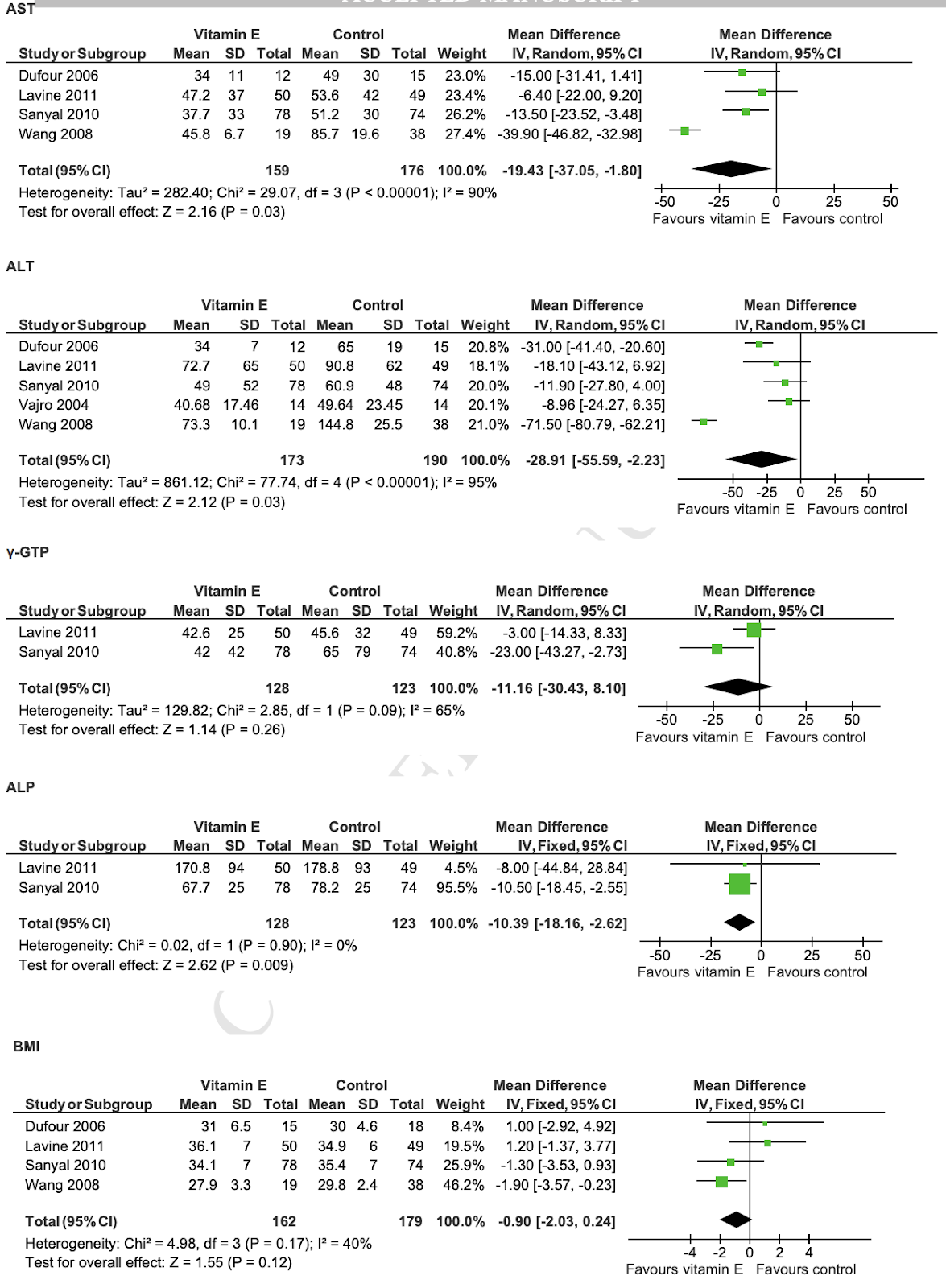
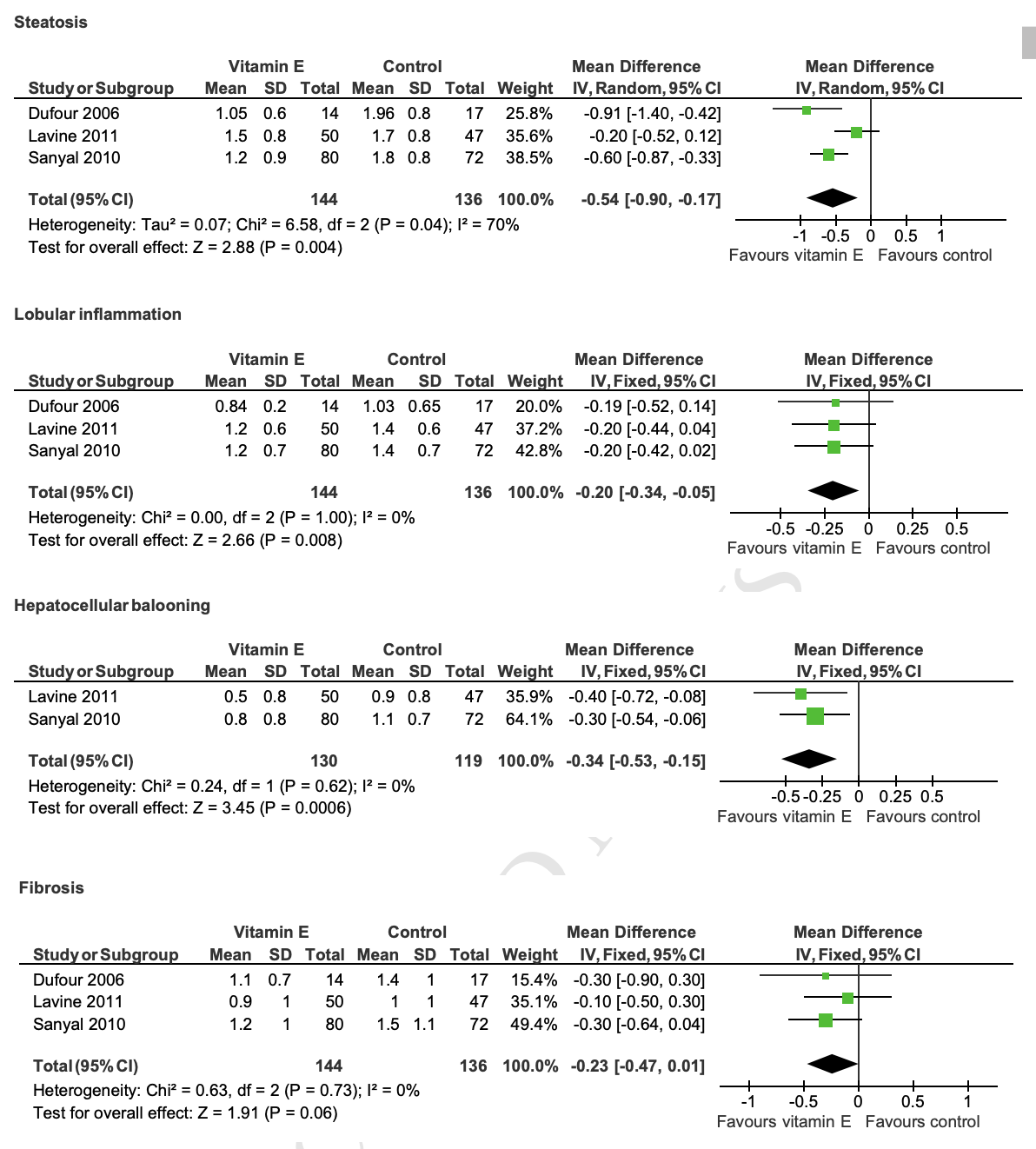
Vitamin E has a beneficial effect on nonalcoholic fatty liver disease: A meta-analysis of randomized controlled trials, 2015
Abstract
Objectives
Vitamin E is often used in the treatment of nonalcoholic fatty liver disease (NAFLD), including nonalcoholic steatohepatitis (NASH); however, the magnitude of treatment response associated with vitamin E in improving liver function and histology in NAFLD/NASH has not, to our knowledge, been quantified systematically. Thus, we conducted a meta-analysis of randomized controlled trials (RCTs) using vitamin E in the treatment of NAFLD/NASH.
Methods
PubMed, Medline, and Cochrane Library Full Text Database, and Japan Medical-Literature Database (Igaku Chuo Zasshi) were searched until March 2014, and five RCTs were identified for meta-analysis.
Results
According to a random effect model analysis of the five studies, vitamin E significantly reduced aspartate transaminase (AST) by −19.43 U/L, alanine aminotransferase (ALT) by −28.91 U/L, alkaline phosphatase (ALP) by −10.39 U/L, steatosis by −0.54 U/L, inflammation by −0.20 U/L, and hepatocellular ballooning by −0.34 U/L compared with the control group. Vitamin E treatment with NASH adult patients showed obvious reductions in not only AST of −13.91 U/L, ALT by −22.44 U/L, steatosis of −0.67 U/L, inflammation of −0.20 U/L, but also fibrosis of −0.30 U/L compared to the control treatment.
Conclusions
Vitamin E significantly improved liver function and histologic changes in patients with NAFLD/NASH.
Effect of vitamin E supplementation on serum C-reactive protein level: a meta-analysis of randomized controlled trials (2015)
C-reactive protein (CRP), a marker of chronic inflammation, has a major role in the etiology of chronic disease. Vitamin E may have anti-inflammatory effects. However, there is no consensus on the effects of vitamin E supplementation on CRP levels in clinical trials. The aim of this study was to systematically review randomized controlled trials (RCTs) that report on the effects of vitamin E supplementation (α- and γ-tocopherols) on CRP levels. A systematic search of RCTs was conducted on Medline and EMBASE through PubMed, Scopus, Ovid and Science Direct, and completed by a manual review of the literature up to May 2014. Pooled effects were estimated by using random-effects models and heterogeneity was assessed by Cochran’s Q and I2 tests. Subgroup analyses and meta-regression analyses were also performed according to intervention duration, dose of supplementation and baseline level of CRP. Of 4734 potentially relevant studies, only 12 trials met the inclusion criteria with 246 participants in the intervention arms and 249 participants in control arms. Pooled analysis showed a significant reduction in CRP levels of 0.62 mg/l (95% confidence interval=−0.92, −0.31; P<0.001) in vitamin E-treated individuals, with the evidence of heterogeneity across studies. This significant effect was maintained in all subgroups, although the univariate meta-regression analysis showed that the vitamin E supplementation dose, baseline level of CRP and duration of intervention were not the sources of the observed heterogeneity. The results of this meta-analysis suggest that supplementation with vitamin E in the form of either α-tocopherol or γ-tocopherol would reduce serum CRP levels.
The effect of vitamin E supplementation on selected inflammatory biomarkers in adults: a systematic review and meta-analysis of randomized clinical trials, 2020
The previous meta-analysis of clinical trials revealed a beneficial effect of vitamin E supplementation on serum C-reactive protein (CRP) concentrations; however, it is unknown whether this vitamin has the same influence on other inflammatory biomarkers. Also, several clinical trials have been published since the release of earlier meta-analysis. Therefore, we aimed to conduct a comprehensive meta-analysis to summarize current evidence on the effects of vitamin E supplementation on inflammatory biomarkers in adults. We searched the online databases using relevant keywords up to November 2019. Randomized clinical trials (RCTs) investigating the effect of vitamin E, compared with the placebo, on serum concentrations of inflammatory cytokines were included. Overall, we included 33 trials with a total sample size of 2102 individuals, aged from 20 to 70 years. Based on 36 effect sizes from 26 RCTs on serum concentrations of CRP, we found a significant reduction following supplementation with vitamin E (− 0.52, 95% CI − 0.80, − 0.23 mg/L, P < 0.001). Although the overall effect of vitamin E supplementation on serum concentrations of interleukin-6 (IL-6) was not significant, a significant reduction in this cytokine was seen in studies that used α-tocopherol and those trials that included patients with disorders related to insulin resistance. Moreover, we found a significant reducing effect of vitamin E supplementation on tumor necrosis factor-α (TNF-α) concentrations at high dosages of vitamin E; such that based on dose–response analysis, serum TNF-α concentrations were reduced significantly at the dosages of ≥ 700 mg/day vitamin E (Pnon-linearity = 0.001). Considering different chemical forms of vitamin E, α-tocopherol, unlike other forms, had a reducing effect on serum levels of CRP and IL-6. In conclusion, our findings revealed a beneficial effect of vitamin E supplementation, particularly in the form of α-tocopherol, on subclinical inflammation in adults. Future high-quality RCTs should be conducted to translate this anti-inflammatory effect of vitamin E to the clinical setting.
Vitamin E supplementation and mammalian lifespan, 2010
Vitamin E refers to a family of several compounds that possess a similar chemical structure comprising a chromanol ring with a 16-carbon side chain. The degree of saturation of the side chain, and positions and nature of methyl groups designate the compounds as tocopherols or tocotrienols. Vitamin E compounds have antioxidant properties due to a hydroxyl group on the chromanol ring. Recently, it has been suggested that vitamin E may also regulate signal transduction and gene expression. We previously reported that lifelong dietary vitamin E (alpha-tocopherol) supplementation significantly increased median lifespan in C57BL/6 mice by 15%. This lifespan extension appeared to be independent of any antioxidant effect. Employing a transcriptional approach, we suggest that this increase in lifespan may reflect an anti-cancer effect via induction of the P21 signalling pathway, since cancer is the major cause of death in small rodents. We suggest that the role of this pathway in life span extension following supplementation of vitamin E now requires further investigation.
Lack of an effect of vitamin E on lifespan of mice, 2001
It has been speculated that ageing results from accumulation of damage to macromolecules, particularly DNA, owing to the action of oxidising free radicals. This possibility would predict that administration of anti-oxidants might prolong lifespan, but previous data on this prediction are conflicting. Three groups of mice were exposed throughout life, from the time of conception until death, to 20, 40 and 400 mg/kg of vitamin E in the diet. No effect on lifespan was observed and the median lifespans in the three groups were 804, 830 and 801 days, respectively. The design of the study also enabled an effect of parental age on lifespan of female progeny to be sought, but no effect was detected.
Tocotrienols Modulate a Life or Death Decision in Cancers, 2019
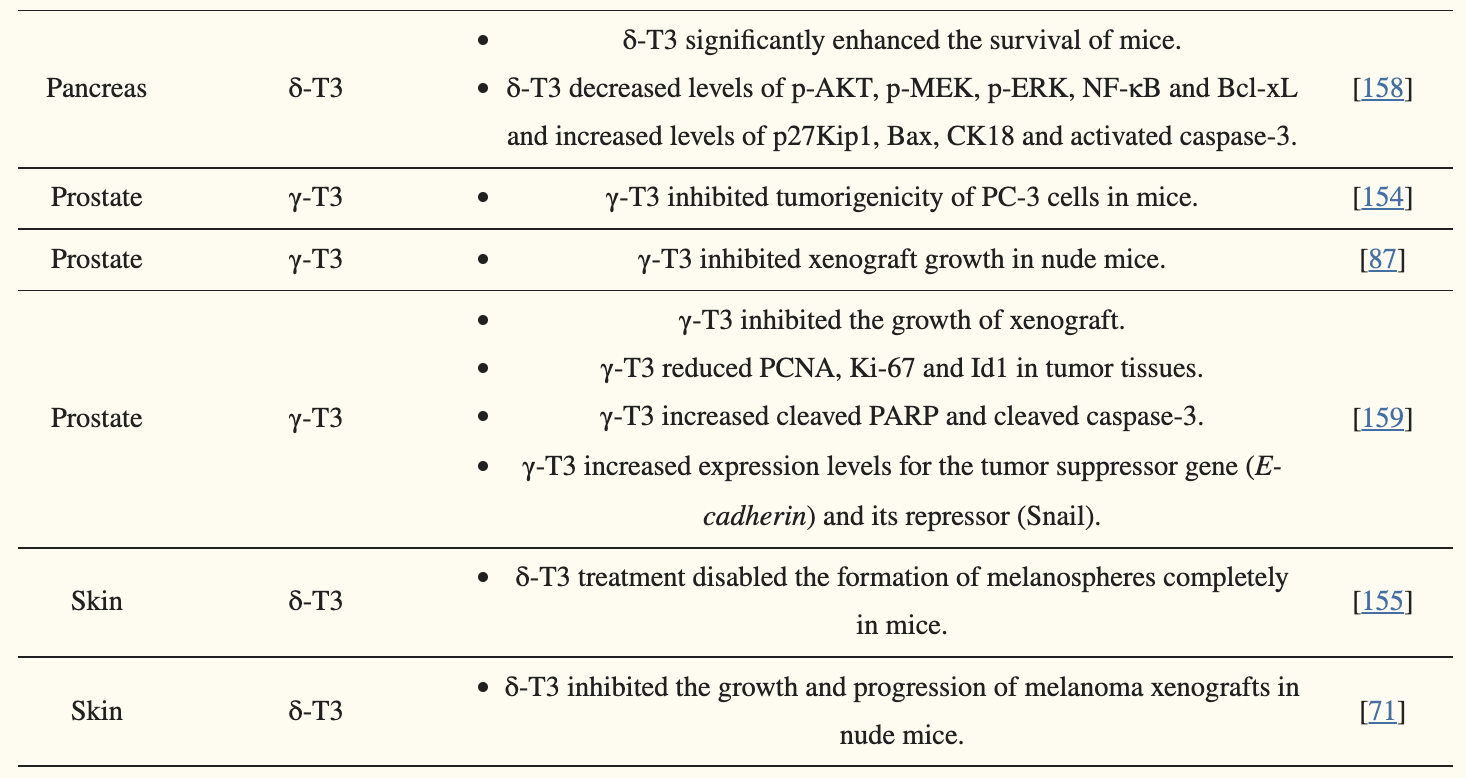
The Vitamin E Derivative Gamma Tocotrienol Promotes Anti-Tumor Effects in Acute Myeloid Leukemia Cell Lines, 2019
Acute myeloid leukemia (AML) is a blood cancer characterized by the formation of faulty defective myelogenous cells with morphological heterogeneity and cytogenic aberrations leading to a loss of their function. In an attempt to find an effective and safe AML treatment, vitamin E derivatives, including tocopherols were considered as potential anti-tumor compounds. Recently, other isoforms of vitamin E, namely tocotrienols have been proposed as potential potent anti-cancerous agents, displaying promising therapeutic effects in different cancer types. In this study we evaluated the anti-cancerous effects of γ-tocotrienol, on AML cell lines in vitro. For this purpose, AML cell lines incubated with γ-tocotrienol were examined for their viability, cell cycle status, apoptotic cell death, DNA fragmentation, production of reactive oxygen species and expression of proapoptotic proteins. Our results showed that γ-tocotrienol exhibits time and dose-dependent anti-proliferative, pro-apoptotic and antioxidant effects on U937 and KG-1 cell lines, through the upregulation of proteins involved in the intrinsic apoptotic pathway.
The role of vitamin E in the prevention of cancer: a meta-analysis of randomized controlled trials, 2007
BACKGROUND
There are conflicting results on published randomized controlled trials (RCTs) on the role of vitamin E in the prevention of cancer. We conducted a meta-analysis of RCTs to evaluate the role of vitamin E in the prevention of cancer in adults.
METHODS
We included RCTs in which the outcomes of the intake of vitamin E supplement alone or with other supplements were compared to a control group. The primary outcomes were total mortality, cancer mortality, total incidence of cancer, and incidence of lung, stomach, esophageal, pancreatic, prostate, breast and thyroid cancers. All identified trials were reviewed independently by the two reviewers to determine whether trials should be included or excluded. The quality of all included studies was scored independently by the two reviewers.
RESULTS
Twelve studies, which included 167 025 participants, met the inclusion criteria. There were no statistically significant differences in total mortality (relative risk, 0.99; 95% CI 0.96–1.03), cancer incidence (odds ratio, 0.96; 95% CI 0.92–1.01), and cancer mortality (odds ratio, 1.00; 95% CI, 0.96–1.03) among the different groups of patients included in this meta-analysis. Vitamin E was associated with a significant reduction in the incidence of prostate cancer (relative risk, 0.85; 95% CI, 0.73–0.96, number needed to treat=500), but it did not reduce the incidence of any other types of cancer.
CONCLUSIONS
Vitamin E supplementation was not associated with a reduction in total mortality, cancer incidence, or cancer mortality, but it was associated with a statistically significant reduction in the incidence of prostate cancer. Vitamin E can be used in the prevention of prostate cancer in men who are at high risk of prostate cancer.
Vitamin E in the primary prevention of cardiovascular disease and cancer: the Women's Health Study: a randomized controlled trial, 2005
Abstract
Context: Basic research provides plausible mechanisms and observational studies suggest that apparently healthy persons, who self-select for high intakes of vitamin E through diet or supplements, have decreased risks of cardiovascular disease and cancer. Randomized trials do not generally support benefits of vitamin E, but there are few trials of long duration among initially healthy persons.
Objective: To test whether vitamin E supplementation decreases risks of cardiovascular disease and cancer among healthy women.
Design, setting, and participants: In the Women's Health Study conducted between 1992 and 2004, 39 876 apparently healthy US women aged at least 45 years were randomly assigned to receive vitamin E or placebo and aspirin or placebo, using a 2 x 2 factorial design, and were followed up for an average of 10.1 years.
Intervention: Administration of 600 IU of natural-source vitamin E on alternate days.
Main outcome measures: Primary outcomes were a composite end point of first major cardiovascular event (nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death) and total invasive cancer.
Results: During follow-up, there were 482 major cardiovascular events in the vitamin E group and 517 in the placebo group, a nonsignificant 7% risk reduction (relative risk [RR], 0.93; 95% confidence interval [CI], 0.82-1.05; P = .26). There were no significant effects on the incidences of myocardial infarction (RR, 1.01; 95% CI, 0.82-1.23; P = .96) or stroke (RR, 0.98; 95% CI, 0.82-1.17; P = .82), as well as ischemic or hemorrhagic stroke. For cardiovascular death, there was a significant 24% reduction (RR, 0.76; 95% CI, 0.59-0.98; P = .03). There was no significant effect on the incidences of total cancer (1437 cases in the vitamin E group and 1428 in the placebo group; RR, 1.01; 95% CI, 0.94-1.08; P = .87) or breast (RR, 1.00; 95% CI, 0.90-1.12; P = .95), lung (RR, 1.09; 95% CI, 0.83-1.44; P = .52), or colon cancers (RR, 1.00; 95% CI, 0.77-1.31; P = .99). Cancer deaths also did not differ significantly between groups. There was no significant effect of vitamin E on total mortality (636 in the vitamin E group and 615 in the placebo group; RR, 1.04; 95% CI, 0.93-1.16; P = .53).
Conclusions: The data from this large trial indicated that 600 IU of natural-source vitamin E taken every other day provided no overall benefit for major cardiovascular events or cancer, did not affect total mortality, and decreased cardiovascular mortality in healthy women. These data do not support recommending vitamin E supplementation for cardiovascular disease or cancer prevention among healthy women.
Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial, 2005
Design, setting, and patients: A randomized, double-blind, placebo-controlled international trial (the initial Heart Outcomes Prevention Evaluation [HOPE] trial conducted between December 21, 1993, and April 15, 1999) of patients at least 55 years old with vascular disease or diabetes mellitus was extended (HOPE-The Ongoing Outcomes [HOPE-TOO]) between April 16, 1999, and May 26, 2003. Of the initial 267 HOPE centers that had enrolled 9541 patients, 174 centers participated in the HOPE-TOO trial. Of 7030 patients enrolled at these centers, 916 were deceased at the beginning of the extension, 1382 refused participation, 3994 continued to take the study intervention, and 738 agreed to passive follow-up. Median duration of follow-up was 7.0 years.
Intervention: Daily dose of natural source vitamin E (400 IU) or matching placebo.
Main outcome measures: Primary outcomes included cancer incidence, cancer deaths, and major cardiovascular events (myocardial infarction, stroke, and cardiovascular death). Secondary outcomes included heart failure, unstable angina, and revascularizations.
Results: Among all HOPE patients, there were no significant differences in the primary analysis: for cancer incidence, there were 552 patients (11.6%) in the vitamin E group vs 586 (12.3%) in the placebo group (relative risk [RR], 0.94; 95% confidence interval [CI], 0.84-1.06; P = .30); for cancer deaths, 156 (3.3%) vs 178 (3.7%), respectively (RR, 0.88; 95% CI, 0.71-1.09; P = .24); and for major cardiovascular events, 1022 (21.5%) vs 985 (20.6%), respectively (RR, 1.04; 95% CI, 0.96-1.14; P = .34). Patients in the vitamin E group had a higher risk of heart failure (RR, 1.13; 95% CI, 1.01-1.26; P = .03) and hospitalization for heart failure (RR, 1.21; 95% CI, 1.00-1.47; P = .045). Similarly, among patients enrolled at the centers participating in the HOPE-TOO trial, there were no differences in cancer incidence, cancer deaths, and major cardiovascular events, but higher rates of heart failure and hospitalizations for heart failure.
Conclusion: In patients with vascular disease or diabetes mellitus, long-term vitamin E supplementation does not prevent cancer or major cardiovascular events and may increase the risk for heart failure.
Prostate cancer and supplementation with alpha-tocopherol and beta-carotene: incidence and mortality in a controlled trial, 1998
Abstract
Background: Epidemiologic studies have suggested that vitamin E and beta-carotene may each influence the development of prostate cancer. In the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study, a controlled trial, we studied the effect of alpha-tocopherol (a form of vitamin E) and beta-carotene supplementation, separately or together, on prostate cancer in male smokers.
Methods: A total of 29133 male smokers aged 50-69 years from southwestern Finland were randomly assigned to receive alpha-tocopherol (50 mg), beta-carotene (20 mg), both agents, or placebo daily for 5-8 years (median, 6.1 years). The supplementation effects were estimated by a proportional hazards model, and two-sided P values were calculated.
Results: We found 246 new cases of and 62 deaths from prostate cancer during the follow-up period. A 32% decrease (95% confidence interval [CI] = -47% to -12%) in the incidence of prostate cancer was observed among the subjects receiving alpha-tocopherol (n = 14564) compared with those not receiving it (n = 14569). The reduction was evident in clinical prostate cancer but not in latent cancer. Mortality from prostate cancer was 41% lower (95% CI = -65% to -1%) among men receiving alpha-tocopherol. Among subjects receiving beta-carotene (n = 14560), prostate cancer incidence was 23% higher (95% CI = -4%-59%) and mortality was 15% higher (95% CI = -30%-89%) compared with those not receiving it (n = 14573). Neither agent had any effect on the time interval between diagnosis and death.
Conclusions: Long-term supplementation with alpha-tocopherol substantially reduced prostate cancer incidence and mortality in male smokers. Other controlled trials are required to confirm the findings.
The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers, 1994 (SELECT Study)
Methods: We performed a randomized, double-blind, placebo-controlled primary-prevention trial to determine whether daily supplementation with alpha-tocopherol, beta carotene, or both would reduce the incidence of lung cancer and other cancers. A total of 29,133 male smokers 50 to 69 years of age from southwestern Finland were randomly assigned to one of four regimens: alpha-tocopherol (50 mg per day) alone, beta carotene (20 mg per day) alone, both alpha-tocopherol and beta carotene, or placebo. Follow-up continued for five to eight years.
Results: Among the 876 new cases of lung cancer diagnosed during the trial, no reduction in incidence was observed among the men who received alpha-tocopherol (change in incidence as compared with those who did not, -2 percent; 95 percent confidence interval, -14 to 12 percent). Unexpectedly, we observed a higher incidence of lung cancer among the men who received beta carotene than among those who did not (change in incidence, 18 percent; 95 percent confidence interval, 3 to 36 percent). We found no evidence of an interaction between alpha-tocopherol and beta carotene with respect to the incidence of lung cancer. Fewer cases of prostate cancer were diagnosed among those who received alpha-tocopherol than among those who did not. Beta carotene had little or no effect on the incidence of cancer other than lung cancer. Alpha-tocopherol had no apparent effect on total mortality, although more deaths from hemorrhagic stroke were observed among the men who received this supplement than among those who did not. Total mortality was 8 percent higher (95 percent confidence interval, 1 to 16 percent) among the participants who received beta carotene than among those who did not, primarily because there were more deaths from lung cancer and ischemic heart disease.
Conclusions: We found no reduction in the incidence of lung cancer among male smokers after five to eight years of dietary supplementation with alpha-tocopherol or beta carotene. In fact, this trial raises the possibility that these supplements may actually have harmful as well as beneficial effects.
Vitamin E and Cancer, 2017
Alpha-Tocopherol, beta-Carotene (ATBC) Cancer Prevention Study
The ATBC study randomly assigned 29,133 male smokers aged 50 to 69 living in Finland to receive beta-Carotene (20 mg daily), alpha-tocopherol (50 mg daily), beta-Carotene (20 mg daily) plus alpha-tocopherol (50 mg daily), or placebo for a median follow-up of 6.1 years.2 Compliance was excellent, with a median 99% of capsules taken across intervention groups.
The incidence of lung, colorectal, liver, urinary tract, and aerodigestive tract cancers were similar among subjects who received alpha-tocopherol compared with placebo.2-6
Physicians’ Health Study II
The double-blind Physician’s Health Study II randomly assigned 14,641 men aged at least 50 to receive alpha-tocopherol (400 IU), vitamin C (500 mg), a multivitamin with or without beta-carotene, or placebo for a mean follow-up of 8 years.7 The incidence of lung, prostate, colorectal, or other cancers was similar among the vitamin E and placebo groups, which was further confirmed by a long-term follow-up.8
Selenium and Vitamin E Cancer Prevention Trial (SELECT)
SELECT randomly assigned 35,533 men aged 50 or older to receive selenium, alpha-tocopherol (400 IU daily), the combination, or placebo.9 The initial analysis found a nonsignificant increased risk of prostate cancer with vitamin E supplementation compared with placebo (relative risk [RR], 1.13; 99% CI, 0.95-1.35; P = .06).
During long-term follow-up, the researchers found an increased risk of prostate cancer with vitamin E supplementation compared with placebo (hazard ratio [HR], 1.17; 99% CI, 1.004-1.36; P = .008), with an absolute increased risk of 1.6 per 1000 person-years.10 The combination of selenium and vitamin E did not increase prostate cancer risk.
Another analysis found similar incidences of bladder cancer in the vitamin E and placebo groups.11
Women’s Health Study
The Women’s Health Study randomly assigned 39,876 female health professionals aged 45 or older living in the United States to receive beta-Carotene (50 mg every 2 days) with or without aspirin (100 mg every 2 days) and/or vitamin E (600 IU every 2 days), or placebo.12 The trial lasted for 12 years, though the beta-Carotene component ended after a median treatment duration of 2.1 years. Current smokers comprised 13% of the cohort at baseline. Vitamin E supplementation did not lower the risk of total cancer or cancers of the breast, lung, or colon.
Other Studies
Other studies also recorded no change in overall cancer incidence or death, or incidence of lung, oral and pharyngeal, colorectal, breast, melanoma, prostate, or liver cancers with vitamin E supplementation, even among high-risk patients.13-15
Outcomes After Anticancer Treatment
A multicenter, double-blind trial randomly assigned 540 patients with stage I or II head and neck cancer to receive alpha-tocopherol (400 IU per day) and beta-Carotene (30 mg/day) or placebo on their first day of radiation and continued for 3 years.17 beta-Carotene was discontinued, however, because of ethical concerns.
Vitamin E supplementation increased the risk of second primary cancers (HR, 2.88; 95% CI, 1.56-5.31) and recurrence/second primary cancer (HR, 1.86, 95% CI, 1.27-2.72) compared with placebo during the intervention period, but trended toward a decreased risk after supplementation was discontinued (HR, 0.41; 95% CI, 0.16-1.03 and HR, 0.71; 95% CI, 0.33-1.53, respectively).
An analysis of the ATBC trial, however, found improved survival among patients with prostate cancer who had high serum levels of alpha-tocopherol at baseline (HR, 0.67; 95% CI, 0.45-1.00) and who received alpha-tocopherol supplementation and also had high baseline (HR, 0.51; 95% CI, 0.20-0.90) or 3-year (HR, 0.26; 95% CI, 0.09-0.71) serum levels.18
Antioxidants speed cancer in mice (link)
Bergö and his colleague, Per Lindahl, also a molecular biologist at the University of Gothenburg, stumbled into the antioxidant debate accidentally. The team was conducting unrelated experiments in mice that were genetically engineered to develop lung cancer, and decided to dose the mice with NAC as a control. If anything, they thought that NAC might slow the tumours slightly, says Lindahl. Instead, the control tumours grew three times faster than expected. “The real experiment turned out to be a disappointment,” he says. “But the control was quite interesting.”
The team decided to dig deeper, and expanded its study to include another common antioxidant, vitamin E. The researchers fed either NAC or vitamin E to the mice, using doses of 5 or 50 times higher than the daily recommended amount for mice. Human dietary supplements often have 4 to 20 times the recommended daily intake of vitamin E for humans, says Lindahl. The results for the two antioxidants were similar: tumours grew about three times faster than those in animals that did not receive the treatment. Treated mice also died from their cancers about twice as quickly as untreated mice.
Treatment with NAC or vitamin E also spurred the growth of human lung-cancer cells grown in culture. In both mouse models and human cells, the antioxidants seemed to protect cancer cells by reducing the amount of DNA damage. That, in turn, reduced expression of a protein called p53. Known as the ‘guardian of the genome’, p53 is a protein that normally suppresses tumour growth and is activated by damaged DNA.
Vitamin E supplementation and cardiovascular events in high-risk patients, 2000
Methods: We enrolled a total of 2545 women and 6996 men 55 years of age or older who were at high risk for cardiovascular events because they had cardiovascular disease or diabetes in addition to one other risk factor. These patients were randomly assigned according to a two-by-two factorial design to receive either 400 IU of vitamin E daily from natural sources or matching placebo and either an angiotensin-converting-enzyme inhibitor (ramipril) or matching placebo for a mean of 4.5 years (the results of the comparison of ramipril and placebo are reported in a companion article). The primary outcome was a composite of myocardial infarction, stroke, and death from cardiovascular causes. The secondary outcomes included unstable angina, congestive heart failure, revascularization or amputation, death from any cause, complications of diabetes, and cancer.
Results: A total of 772 of the 4761 patients assigned to vitamin E (16.2 percent) and 739 of the 4780 assigned to placebo (15.5 percent) had a primary outcome event (relative risk, 1.05; 95 percent confidence interval, 0.95 to 1.16; P=0.33). There were no significant differences in the numbers of deaths from cardiovascular causes (342 of those assigned to vitamin E vs. 328 of those assigned to placebo; relative risk, 1.05; 95 percent confidence interval, 0.90 to 1.22), myocardial infarction (532 vs. 524; relative risk, 1.02; 95 percent confidence interval, 0.90 to 1.15), or stroke (209 vs. 180; relative risk, 1.17; 95 percent confidence interval, 0.95 to 1.42). There were also no significant differences in the incidence of secondary cardiovascular outcomes or in death from any cause. There were no significant adverse effects of vitamin E.
Conclusions: In patients at high risk for cardiovascular events, treatment with vitamin E for a mean of 4.5 years had no apparent effect on cardiovascular outcomes.
Multivitamins contain relatively small amount of Vit E (33 IU)


Comments