TGF-Beta / Proteolytic enzymes
(Wobenzyme N ~ pancreatin 300mg, papain 180mg, bromelain 135mg, trypsin 72mg, rutin 150mg)
GENERAL SUMMARY:
TGF-β is a multifunctional cytokine involved in various cellular processes, and its dysregulation contributes to numerous disease states.
In fibrosis, excessive TGF-β activity leads to tissue scarring in multiple organs, causing dysfunction and potential failure.
TGF-β plays a dual role in cancer, initially suppressing tumor growth but later promoting progression and metastasis in advanced stages.
Dysregulated TGF-β signaling is implicated in autoimmune diseases, disrupting the balance between pro- and anti-inflammatory cytokines and resulting in chronic inflammation and tissue damage.
Additionally, TGF-β contributes to cardiovascular diseases by promoting vascular remodeling, inflammation, and fibrosis, leading to narrowed blood vessels and heart failure.
TGF-β is involved in the pathogenesis of neurodegenerative diseases, contributing to neuroinflammation, impaired neuronal function, and toxic protein aggregation.
In 2019, a single combination gene therapy using 3 longevity-associated genes (FGF21, αKlotho, sTGFβR2) delivered via adeno-associated viruses effectively treated obesity, type II diabetes, heart failure, and renal failure in mice.
PROTEOLYTIC ENZYMES (WOBENZYME):
The 2001 study on oral therapy with proteolytic enzymes found that it reduced TGF-beta1 concentration in patients with elevated levels in rheumatoid arthritis (P < 0.005), osteomyelofibrosis (P < 0.05), and herpes zoster (P < 0.05), supporting the concept that oral enzyme therapy is beneficial in diseases characterized by TGF-beta1 overproduction.
Knee Osteoarthritis: Wobenzym was comparable to diclofenac in relieving pain, increasing function, and reducing reliance on analgesic medication, while being associated with fewer adverse events, suggesting it may be appropriate for long-term use (P < 0.05) (2015).
Multiple Myeloma: Oral Enzyme (OE) group had a 60% decrease in the hazard of death, 3-year gain in survival time for stage III patients, and overall well-tolerated treatment, warranting further evaluation in a randomized phase III trial (P = 0.0014) (2001).
Breast cancer (n=1283 enzyme group, 1056 controls): Enzymes significantly reduced side effects of chemo/radiotherapy by 44% and improved quality of life parameters including fatigue, appetite loss, nausea and restlessness. Exploratory survival analysis hinted at longer remission times in early stage cancer (2001).
Colorectal cancer (n=616 enzyme group, 626 controls): Enzymes markedly decreased chemo/radiotherapy side effects by 61% and alleviated cancer symptoms like nausea, diarrhea and depression. Survival time was prolonged in advanced stage patients receiving enzymes (2001).
NAFLD after pancreaticoduodenectomy (whipple procedure): A 2020 study showed that high-dose administration of digestive enzymes significantly reduced the onset of NAFLD compared to normal-dose administration (p < 0.001), with no adverse effects.
MPNs:
TGF-β signaling contributes to myelofibrosis (MF) development through the non-canonical JNK pathway and clonal expansion of Jak2 mutated HSCs, which are resistant to TGF-β's growth suppressive effect (2019).
AVID200, a potent TGFβ1/3 protein trap, was well-tolerated and showed potential for combination therapy approaches in thrombocytopenic MF patients, as it reduced serum TGFβ levels and improved platelet counts, although clinical responses were limited (2021).
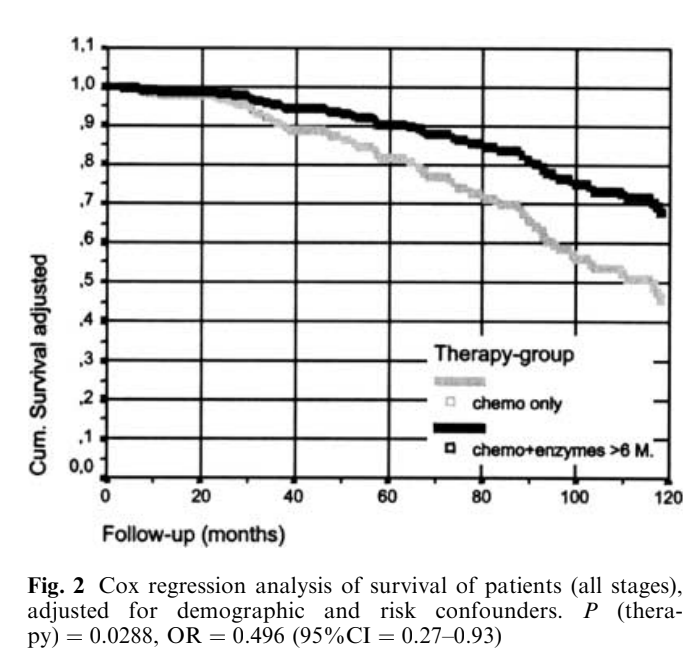
Retrospective cohort study of an additive therapy with an oral enzyme preparation in patients with multiple myeloma, 2001
Methods: A cohort of 265 patients with multiple myeloma stages I-III was consecutively treated at our institution in two parallel groups (control group (n = 99): chemotherapy +/-OE for less than 6 months; OE-group (n = 166): chemotherapy + OE for more than 6 months.
Significantly higher overall response rates and longer duration of remissions were observed in the OE-group. Primary responders showed a longer mean survival time than non-responders. Additive therapy with OE given for more than 6 months decreased the hazard of death for patients at all stages of disease by approximately 60%. Observation time was not long enough to estimate the median survival for patients at stages I and II; for stage III patients it was 47 months in the control group versus 83 months for the patients treated with OE (P = 0.0014) which means a 3-year gain of survival time. Significant prognostic factors for survival, in the Cox regression analysis, were stage of disease and therapy with OE. The OE-therapy was generally well tolerated (3.6% of patients with mild to moderate gastrointestinal symptoms).
OEs represent a promising new additive therapy in multiple myeloma which will be further evaluated in a randomized phase III trial in the USA.
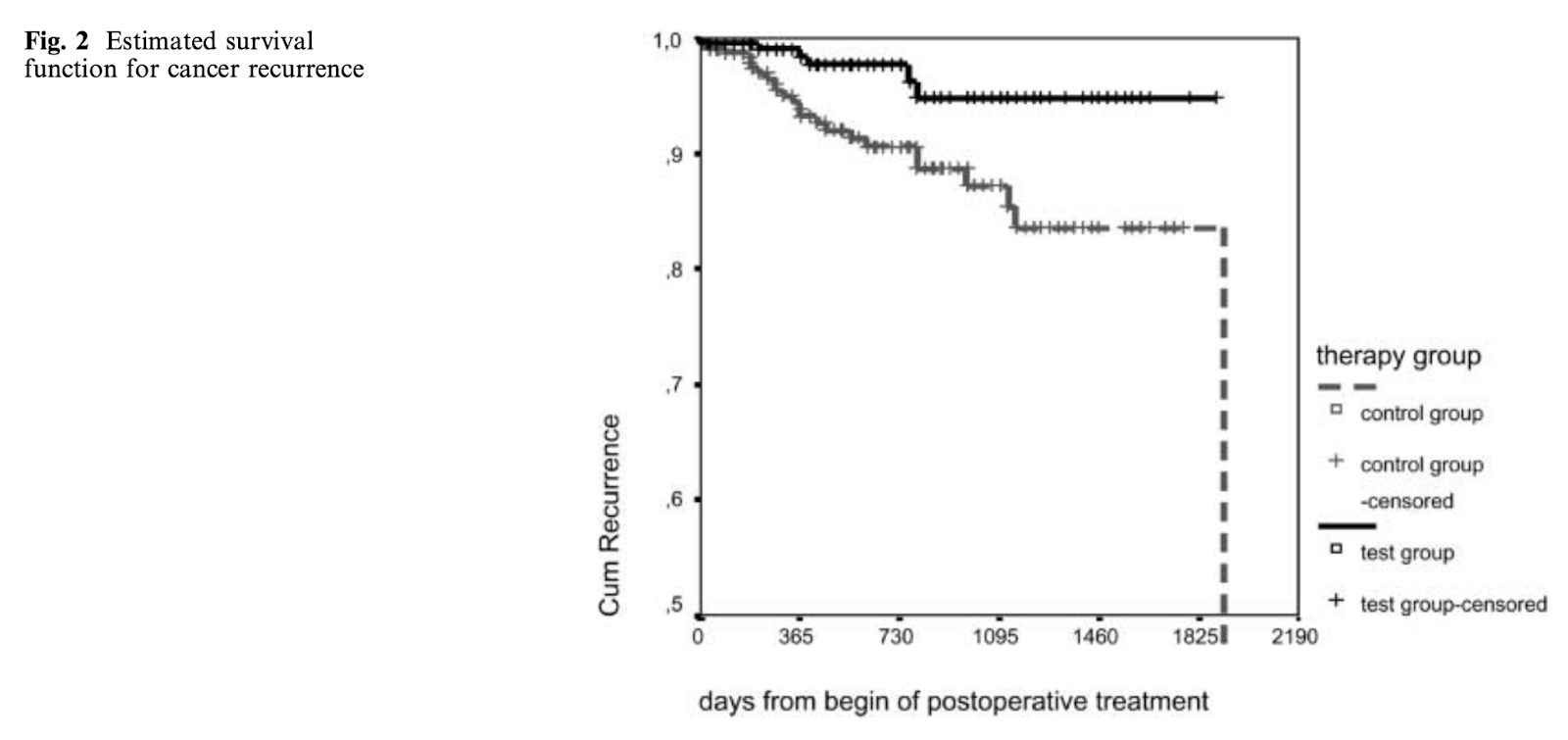
Impact of complementary oral enzyme application on the postoperative treatment results of breast cancer patients--results of an epidemiological multicentre retrolective cohort study (2001)
Breast cancer (n=1283 enzyme group, 1056 controls): Enzymes significantly reduced side effects of chemo/radiotherapy by 44% and improved quality of life parameters including fatigue, appetite loss, nausea and restlessness. Exploratory survival analysis hinted at longer remission times in early stage cancer (2001)
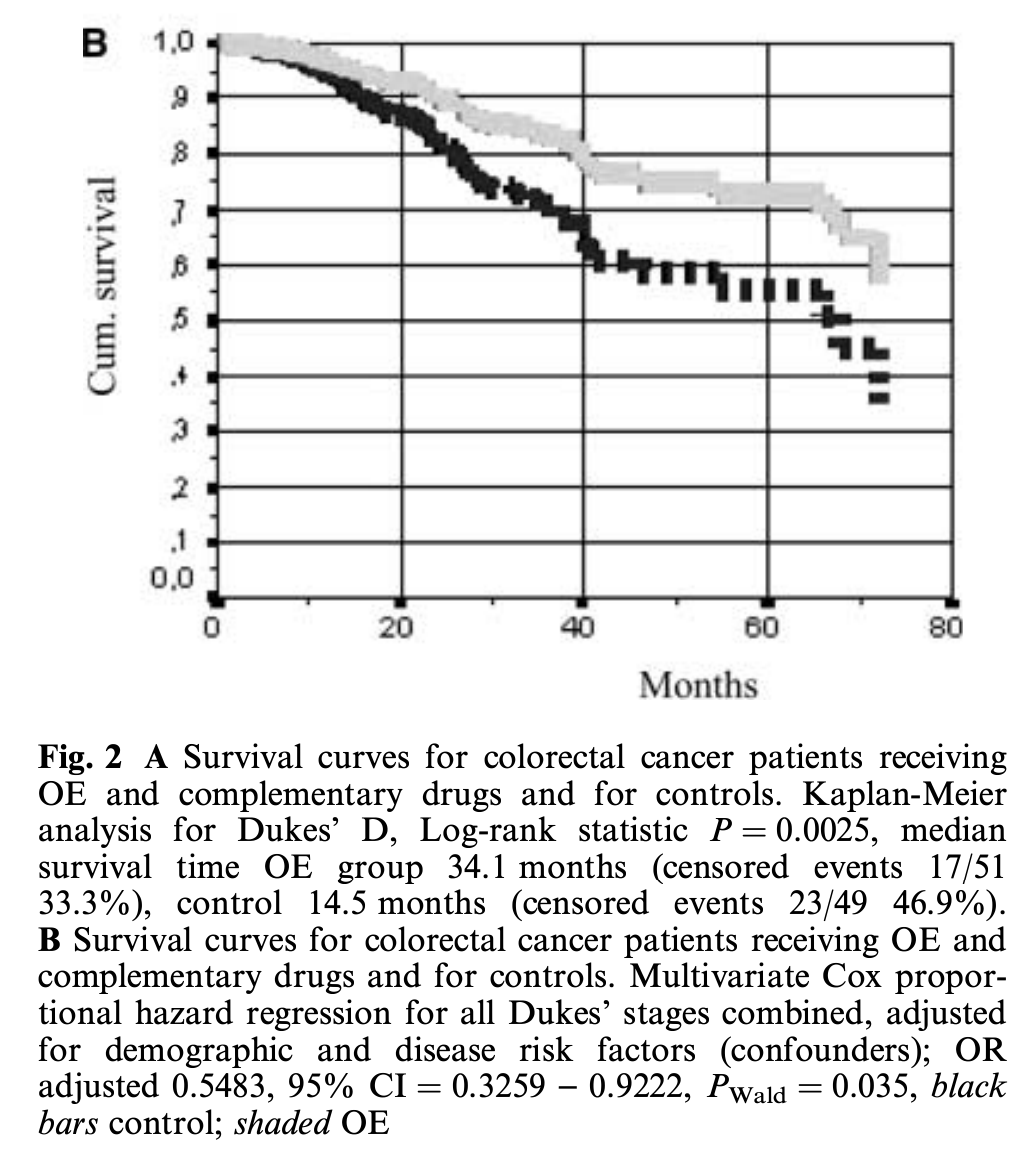
Influence of a complementary treatment with oral enzymes on patients with colorectal cancers--an epidemiological retrolective cohort study (2001)
Colorectal cancer (n=616 enzyme group, 626 controls): Enzymes markedly decreased chemo/radiotherapy side effects by 61% and alleviated cancer symptoms like nausea, diarrhea and depression. Survival time was prolonged in advanced stage patients receiving enzymes (2001).
Preventive Effect of High-Dose Digestive Enzyme Management on Development of Nonalcoholic Fatty Liver Disease after Pancreaticoduodenectomy: A Randomized Controlled Clinical Trial, 2020
Background: Nonalcoholic fatty liver disease (NAFLD) is a complication of pancreaticoduodenectomy (PD) – Whipple procedure. We conducted a randomized clinical trial to determine if high-dose digestive enzymes prevented the development of NAFLD after PD.
Study design: This parallel-group, nonblinded, multicenter study enrolled patients undergoing elective PD at Shinshu University School of Medicine, from June 2011 to April 2017. Patients were randomly assigned to receive normal-dose (Excelase: 3.0 g/day [Meiji Seika Pharma Holdings Co, Ltd]) or high-dose digestive enzyme treatment (Excelase: 3.0 g/day; Pancreatin [Tokyo Chemical Industry Co Ltd]: 3.0 g/day; Berizym [Kyowa Pharmaceutical Industry Co Ltd]: 3.0 g/day; and Toughmac-E [Ono Pharmaceutical Co, Ltd]: 3.0 g/day) within 1 week after surgery. Because patients in the control group switched interventions upon receiving a diagnosis of NAFLD, intention-to-treat analysis was used. The primary endpoint was incidence of NAFLD within 1 year, and the secondary endpoints were the incidences of NAFLD at 1, 3, 6, and 12 months and the rate of improvement in NAFLD with high-dose transfer in the control group. The secondary analysis comprised assessment of risk factors for the development of NAFLD.
Results: Eighty-four patients were randomly assigned (42 per group), 80 of whom were finally analyzed (39 normal-dose, 41 high-dose). The incidence of NAFLD was significantly lower in the high-dose (8 of 41) compared with the normal-dose (25 of 39) patients (p < 0.001). Multivariate analysis identified normal-dose (odds ratio [OR] 14.65, p < 0.001), total protein ≤ 6.5g/dL (OR 9.01, p = 0.018), pre-albumin ≤ 22.0 mg/dL (OR 7.71, p = 0.018), and pancreatic function diagnostic test ≤ 70% (OR 6.66, p = 0.009) as independent risk factors. There were no adverse effects. The model was accurate (c-index = 0.92) and reliable (Hosmer-Lemeshow test p = 0.32).
Conclusions: High-dose administration of digestive enzymes significantly reduced the onset of NAFLD after PD compared with normal-dose administration.
[Pancreatin] Effects of pancrelipase on nonalcoholic fatty liver disease after pancreaticoduodenectomy (2014)
Nonalcoholic fatty liver disease (NAFLD) is a condition characterized by the accumulation of fat in the livers of individuals who drink little or no alcohol. In some cases, this condition develops after individuals have the pancreas removed. Studies indicate that taking pancreatin may help to treat or prevent NAFLD in those individuals.
Findings published in the Journal of Hepato-Biliary-Pancreatic Sciences showed that treatment with pancreatin could significantly improve liver fat levels among patients who developed NAFLD after having their pancreases removed. Analysis also revealed improvements to liver function, digestion, and blood levels of proteins, albumin, and cholesterol.
A Mini Review on Pancreatin: Prodigious Focus on Hepatic Ischemia-Reperfusion Injury (2023)
Pancreatin is a natural mixture of digestive enzymes derived from the pancreas of vertebrates. Recent studies have shown that pancreatin protects the liver from different kinds of ischemia-reperfusion (I/R) injury. In this review, we look at the evidence that shows how pancreatin protects against hepatic I/R injury. We talk about how anti-inflammatory, anti-oxidative, anti-apoptotic, and anti-fibrotic effects of pancreatin might help protect the body. We also talk about how pancreatin might be used to treat I/R injury in the liver. Numerous studies have shown that pancreatin can protect against hepatic ischemia-reperfusion (I/R) injury by targeting multiple pathways and processes involved in I/R injury, including reduction in oxidative stress, suppression of the inflammatory response, promotion of cell proliferation, and improvement in the apoptosis process. In addition, pancreatin has a protective effect on liver injury by promoting the antioxidant defense system, inhibiting the accumulation of intracellular lipid peroxides, and restoring cellular antioxidant status. So, pancreatin may be a promising and effective way to treat hepatic I/R injury, but more research is needed to find out how well it works in practice. In conclusion, pancreatin has been studied as a possible natural treatment for hepatic I/R injury. Even though more research needs to be done to confirm pancreatin's effectiveness in clinical settings, it has been suggested that it can be used as a natural treatment for hepatic I/R injury because it works in multiple ways and can restore the balance of oxidative stress. Pancreatin has been studied as a potential natural remedy for hepatic I/R injury due to its ability to inhibit lipid peroxidation, promote antioxidant defense system activity, and restore cellular antioxidant status.
[Papain] Papain Ameliorates Lipid Accumulation and Inflammation in High-Fat Diet-Induced Obesity Mice and 3T3-L1 Adipocytes via AMPK Activation (2021)
Oral administration of papain reduced HFD-induced weight of the body, liver, and adipose tissues of mice. Papain also reduced hepatic lipid accumulation and adipocyte size. Moreover, serum total cholesterol and triglyceride levels were markedly reduced in papain-treated mice.
The safety and efficacy of an enzyme combination in managing knee osteoarthritis pain in adults: a randomized, double-blind, placebo-controlled trial, 2015
This randomized, double-blind, placebo-controlled, and comparator-controlled trial evaluated the safety and efficacy of an enzyme combination, as Wobenzym, in adults with moderate-to-severe osteoarthritis (OA) of the knee. Adults (n = 150) received Wobenzym, diclofenac (a nonsteroidal anti-inflammatory drug, NSAID), or placebo for 12 weeks. Improvement in pain scores (Lequesne Functional Index) did not differ between subjects treated with Wobenzym or diclofenac, and both treatment groups improved compared to placebo (P < 0.05). Reduction in total WOMAC scores (secondary outcome measure) did not differ between Wobenzym and diclofenac, although only diclofenac emerged as different from placebo (P < 0.05). The median number of rescue medication (paracetamol) tablets consumed was less in the Wobenzym group compared to placebo (P < 0.05), while there was no difference between diclofenac and placebo. Adverse events were similar in frequency in Wobenzym and placebo groups (7.2% and 9.1% of subjects, resp.) and higher in diclofenac group (15.6%). Wobenzym is comparable to the NSAID diclofenac in relieving pain and increasing function in adults with moderate-to-severe painful knee OA and reduces reliance on analgesic medication. Wobenzym is associated with fewer adverse events and, therefore, may be appropriate for long-term use.
Indices of Systemic Inflammation. Erythrocyte sedimentation rates and serum C-reactive protein concentrations were not affected in any group during the 12 weeks of the study (data not shown).
[Lowers inflammation; if neutral on the liver, might be worth trying]
Oral therapy with proteolytic enzymes decreases excessive TGF-beta levels in human blood, 2001
Therapy with oral proteolytic enzymes (OET) with combination drug products containing papain, bromelain, trypsin, and chymotrypsin has been shown to be beneficial in clinical settings such as radiotherapy-induced fibrosis, bleomycin pneumotoxicity and immunosuppression in cancer, all of which are nowadays known to be accompanied by excessive transforming growth factor-beta (TGF-beta) production. It has been demonstrated that proteolytic enzymes reduce TGF-beta levels in serum by converting the protease inhibitor alpha2 macroglobulin (alpha2M) from the "slow" form into the "fast" form, whereby the "fast" form binds and inactivates TGF-beta irreversibly. In this study we have investigated the effect of OET on the concentration of TGF-beta1 in serum of patients with rheumatoid arthritis (RA) (n = 38), osteomyelofibrosis (OMF) (n = 7) and herpes zoster (HZ) (n = 7). Seventy-eight healthy volunteers served as controls. TGF-beta1 levels in serum were assessed by enzyme-linked immunosorbent assay (ELISA). We have demonstrated that in healthy volunteers and in patients there exists a correlation between active and latent TGF-beta1 in serum (r=0.8021; P<0.0001). Treatment with OET had no significant effect on TGF-beta1 concentration in healthy volunteers or patients with a normal level of TGF-beta1. In patients with elevated TGF-beta1 concentration (> 50 ng/ml serum), OET reduced TGF-beta1 in RA (P < 0.005), in OMF (P < 0.05) and in HZ (P < 0.05).
Conclusion: These results support the concept that OET is beneficial in diseases characterized in part by TGF-beta1 overproduction.
Lifetime exposure to a soluble TGF-β antagonist protects mice against metastasis without adverse side effects, 2002
Novel therapies emerging in oncology to target the TGF-β pathway, 2021
The TGF-β signaling pathway governs key cellular processes under physiologic conditions and is deregulated in many pathologies, including cancer. TGF-β is a multifunctional cytokine that acts in a cell- and context-dependent manner as a tumor promoter or tumor suppressor. As a tumor promoter, the TGF-β pathway enhances cell proliferation, migratory invasion, metastatic spread within the tumor microenvironment and suppresses immunosurveillance. Collectively, the pleiotropic nature of TGF-β signaling contributes to drug resistance, tumor escape and undermines clinical response to therapy. Based upon a wealth of preclinical studies, the TGF-β pathway has been pharmacologically targeted using small molecule inhibitors, TGF-β-directed chimeric monoclonal antibodies, ligand traps, antisense oligonucleotides and vaccines that have been now evaluated in clinical trials. Here, we have assessed the safety and efficacy of TGF-β pathway antagonists from multiple drug classes that have been evaluated in completed and ongoing trials.
A single combination gene therapy treats multiple age-related diseases (2019)
We developed gene therapies based on 3 longevity associated genes (fibroblast growth factor 21 [FGF21], αKlotho, soluble form of mouse transforming growth factor-β receptor 2 [sTGFβR2]) delivered using adeno-associated viruses and explored their ability to mitigate 4 age-related diseases: obesity, type II diabetes, heart failure, and renal failure. Individually and combinatorially, we applied these therapies to disease-specific mouse models and found that this set of diverse pathologies could be effectively treated and in some cases, even reversed with a single dose. We observed a 58% increase in heart function in ascending aortic constriction ensuing heart failure, a 38% reduction in α-smooth muscle actin (αSMA) expression, and a 75% reduction in renal medullary atrophy in mice subjected to unilateral ureteral obstruction and a complete reversal of obesity and diabetes phenotypes in mice fed a constant high-fat diet. Crucially, we discovered that a single formulation combining 2 separate therapies into 1 was able to treat all 4 diseases.
Pre-clinical rationale for TGF-β inhibition as a therapeutic target for the treatment of myelofibrosis, 2016
To assess the role of abnormal TGF-β signaling in the pathogenesis of primary myelofibrosis (PMF) the effects of the TGF-β receptor-1 kinase inhibitor SB431542 on ex-vivo expansion of hematopoietic cells in cultures from patients with JAK2V617+-polycythemia vera (PV), PMF (JAK2V617F+, CALRpQ365f+ or unknown) and from normal sources (adult blood, AB, or cord blood, CB) were compared. In cultures of normal sources, SB431542 significantly increased by 2.5-fold the number of progenitor cells generated by Day 1–2 (CD34+) and 6 (colony-forming cells) (CB) and that of precursor cells, mostly immature erythroblasts, by Days 14–17 (AB and CB). In cultures of JAK2V617F+-PV, SB431542 increased by 2-fold the numbers of progenitor cells by Day 10 and had no effect on that of precursors cells by Days 12–17 [fold-increase ~4 fold in all cases]. By contrast, SB431542 had no effect on the number of both progenitor and precursor cells in cultures of JAK2V617F+- and CALR pQ365fs+-PMF. These ontogenetic- and disease-specific effects were associated with variegation in the ability of SB431542 to induce CD34+ cells from AB (increased), CB (decreased) or PV and PMF (unaffected) into cycle and erythroblasts in proliferation (increased for AB and PV and unaffected for CB and PMF). Differences in expansion of erythroblasts from AB, CB and PV were associated with differences in activation of TGF-β signaling (SHCY317, SMAD2S245/250/255 and SMAD1S/S/SMAD5S/S/SMAD8S/S) detectable in these cells by phosphoproteomic profiling. In conclusion, treatment with TGF-β receptor-1 kinase inhibitors may reactivate normal hematopoiesis in PMF patients, providing a proliferative advantage over the unresponsive malignant clone.
TGF-β Signaling Contributes to Myelofibrosis and Clonal Dominance of Myeloproliferative Neoplasms, 2019
The study investigates the role of TGF-β in the development of myelofibrosis and clonal expansion in myeloproliferative neoplasms (MPNs). Two hypotheses were tested: 1) increased TGF-β signaling in mesenchymal stromal cells (MSCs) is required for myelofibrosis development, and 2) Jak2 mutated hematopoietic stem cells (HSCs) are resistant to TGF-β's growth suppressive effect, contributing to clonal expansion. The results show that myelofibrosis was reduced, but not completely abrogated, in Osx-Cre; Tgfbr2f/f mice, suggesting TGF-β signaling in MSCs contributes to myelofibrosis development through the non-canonical JNK pathway. Furthermore, no expansion of Jak2 mutated cells was observed in the Tgfbr2-deleted group, supporting the idea that Jak2 mutated HSCs are resistant to TGF-β's growth suppressive effect, contributing to clonal expansion in MPN and possibly clonal hematopoiesis.
Treatment of Myelofibrosis Patients with the TGF-β 1/3 Inhibitor AVID200 (MPN-RC 118) Induces a Profound Effect on Platelet Production, 2021
TGFβ plays a pivotal role in the pathobiology of myelofibrosis (MF) by not only promoting bone marrow fibrosis (BMF) but also by enhancing the dormancy of normal but not MF hematopoietic stem cells (HSCs). TGFβ has also previously been reported to inhibit normal megakaryocyte (MK) production (Bruno et al Blood 1998). TGFβ1 promotes the synthesis of collagen by normal human mesenchymal stromal cells (MSCs). Treatment of MSCs with AVID200, a potent TGFβ1/3 protein trap, significantly decreased MSC proliferation, phosphorylation of SMAD2, and collagen expression.
A Phase 1b trial of AVID200 completed in high-risk MF patients resistant to ruxolitinib, with responses assessed after six cycles, and those with clinical improvement or stable disease continued treatment.
No dose-limiting toxicities were observed in the dose escalation study, with updated safety and efficacy results for the Phase 1b dose expansion stage at two highest doses.
Twenty-two subjects enrolled, with the most common mutations observed being JAK2V617F (71%), TET2 (29%), ASXL1 (24%), and CALR (19%).
No dose-limiting toxicities observed, and Grade 3/4 adverse events occurred in 76.2% of subjects, with non-hematologic and hematologic events in 38.1% and 28.3% of subjects, respectively; no fatal events observed.
Median number of treatment cycles received was 5, with 33% of patients receiving more than 6 cycles; reasons for discontinuation varied.
Median changes in spleen length, symptom scores, and platelet counts showed varied responses; 17 subjects had increased platelets, two normalized their counts, and no significant changes in bone marrow histology were observed.
Elevated plasma TGFβ1 levels in all patients were significantly reduced 21 days after the last AVID200 dose.
AVID200 is well tolerated, but clinical responses were limited; however, it reduced serum TGFβ levels and improved platelet counts, indicating potential for combination therapy approaches in thrombocytopenic MF patients.
TGF-β signaling in myeloproliferative neoplasms contributes to myelofibrosis without disrupting the hematopoietic niche, 2022
Oral enzymes as additive cancer therapy, 2001
Oral therapy with proteolytic enzymes (OTPE) (papain, bromelain, trypsin, chymotrypsin amylase and lipase) has been used in additive cancer therapy for several years and has led to a reduction in adverse effects after cancer treatment (radiation and chemotherapy). OTPE has been proven to have a beneficial effect, especially in cancers and other conditions involving elevated transforming growth factor-β (TGF-β) expression. Proteases such as trypsin, chymotrypsin, bromelain and papain have been demonstrated to be capable of converting the slow form of α2-macroglobulin into the fast form. This form of α2-macroglobulin is capable of irreversibly binding TGF-β. Subsequently the TGF-β-α2-macroglobulin complex can be quickly removed via endocytosis. Since the production of TGF-β is regulated by an autocrine loop, removal of TGF-β results in down-regulation of TGF-β overproduction. It has been proposed that OTPE may act through this interruption of the autocrine loop. In vitro reduction in TGF-β overexpression in tumor-associated macrophages leads to enhanced tumor killing capacity as well as to stimulation of natural killer cell and granulocyte cytotoxicity. In clinical trials with patients suffering from polycythemia vera or myelofibrosis, treatment with proteolytic enzymes has been shown to reduce elevated serum concentrations of TGF-β. These findings suggest that through reduction of TGF-β overproduction, OTPE could be beneficial in the inhibition of fibrosis and in additive tumor therapy.
Pancreatic Proteolytic Enzymes and Cancer: New Support for an Old Theory, 2022
In 1905, embryologist John Beard proposed that the origin of cancer could be traced back to embryology, as he observed similarities between the behavior of early placental cells and cancer. Beard hypothesized that "vagrant germ cells" could develop into cancer later in life. He sought to identify the signal that caused placental cells to transition from invasive to mature, believing this could provide a key to cancer treatment. Beard discovered that this change occurred when the fetal pancreas began producing proteolytic enzymes. Subsequent attempts to utilize enzyme preparations as cancer treatments yielded mixed results, with some patients experiencing benefits while others did not. Beard's work was criticized as painful and ineffective, leading to a decline in interest by 1924.
Over the years, proteolytic enzymes have been experimented with as a potential cancer treatment, with various physicians reporting benefits and case studies involving trypsin treatment. In the 1950s and 1960s, Shively administered enzymes intravenously to cancer patients, but this practice ceased after the FDA outlawed intravenous and injectable enzymes in 1964. Orthodontist Kelley treated cancer patients with oral pancreatin, creating a controversial program involving dietary modification and coffee enemas. Gonzalez later investigated Kelley's methods and found some patients survived longer than expected; however, his recreation of the methodology in clinical trials did not yield similarly promising results. Gonzalez and Isaacs's treatment required extensive dietary and lifestyle modification, leading to patient adherence difficulties, which case reports suggest is crucial for success. While some studies reported positive results in cancer patients treated with enzyme combinations, the reliability of these findings is uncertain.
Protease systems have been discovered to play a role in various biological mechanisms, including cancer, with protease-activated receptors (PARs) on cell surfaces potentially contributing to understanding proteases' role in cancer and trophoblast cell regulation. Conflicting data exists regarding the role of proteases and PARs in cancer, with some studies suggesting they promote cancer spread while others indicate cancer cell growth inhibition. These interactions are complex, with different reactions depending on various factors. Evidence points to proenzyme forms being the key components in pancreatic enzyme therapy, with limited studies conducted on purified proenzymes in humans.
The idea of cancer cells resembling embryonic cells has been explored since the 19th century, with Beard's theory of primordial germ cells causing cancer development relating to the modern theory of cancer stem cells. Some studies reported anti-tumor efficacy of pancreatic proenzymes against cancer stem cells. The century-old theory of pancreatic proteolytic enzymes having anti-cancer effects has been supported by case reports and small studies, with the broader role of proteases in physiology making their potential anti-cancer effects more intriguing. Further research could lead to valuable additions to cancer treatments.
Is lack of proteolysis an aging pillar?
Yes, decreased proteolysis is considered one of the hallmarks or "pillars" of aging. Here's a quick explanation:
Proteolysis refers to the breakdown of proteins by enzymes like proteases. It's an important cellular process that helps get rid of old, damaged or unneeded proteins.
As we age, the body's ability to effectively carry out proteolysis declines. This leads to the accumulation of dysfunctional proteins that would normally be degraded. The decreased proteolytic activity contributes to many age-related problems like loss of muscle mass, aggregation of proteins into plaques, and impaired cell function.
So in summary, the decreased ability to break down proteins through proteolysis is considered one of the core biological mechanisms that drives the aging process. Maintaining proteostasis (protein homeostasis) is thought to be key for healthy longevity.
Proteolysis dysfunction in the process of aging and age-related diseases (2022)
The review by Frankowska et al. (2022) discusses aging-related changes in cellular proteolysis and how dysfunction in protein degradation pathways contributes to immunosenescence and age-related diseases. The main conclusions and key points are:
Proteins are continuously synthesized and degraded to maintain proteostasis. This involves molecular chaperones that assist with folding, the ubiquitin-proteasome system (UPS) and autophagy-lysosome pathway that degrade proteins, and proteases like calpains and caspases that cleave proteins to modify function.
During aging, effectiveness of proteostasis systems declines, leading to accumulation of damaged proteins. This impairs cell function and increases risk of diseases like neurodegeneration, metabolic disorders, and chronic inflammation.
Molecular chaperones help proteins fold properly. Levels of heat shock proteins (HSPs) like HSP70 and HSP90 decline with age in many cell types. This reduces capacity to refold damaged proteins. Expression of chaperones specific to the endoplasmic reticulum also declines, impairing unfolded protein response.
The UPS degrades 80% of cellular proteins, especially soluble misfolded proteins. Its activity is reduced in aged cells due to lower levels of proteasome subunits, improper subunit ratios, oxidative damage to proteasomes, and impaired ubiquitin labeling. The immunoproteasome, important for antigen processing, is also affected.
Autophagy, especially macroautophagy and chaperone-mediated autophagy (CMA), declines with age. This is due to reduced clearance of autophagosomes, lysosomal dysfunction, accumulation of lipofuscin that impairs lysosomes, downregulation of autophagy genes, and lower levels of LAMP2A in CMA. Impaired autophagy causes mitochondrial dysfunction.
The calpain-calpastatin system (CCS) is less active in lymphocytes of the elderly. Lower calpain levels reduce T cell activation, proliferation, cytokine production, and cell signaling. The CCS likely contributes to immunosenescence.
Inflammaging causes chronic low-grade inflammation in the elderly. Declining proteostasis contributes by allowing accumulation of aggregates that trigger inflammation. Senescent cells with faulty proteolysis secrete pro-inflammatory mediators.
Impaired protein quality control is strongly linked to neurodegenerative diseases like Alzheimer's and Parkinson's disease, where toxic misfolded proteins accumulate. It also contributes to sarcopenia, atherosclerosis, diabetes, and impaired immunity in the elderly.
In summary, Frankowska et al. (2022) comprehensively review research showing that declining protein homeostasis is a hallmark of aging that allows damaged proteins to accumulate, impairing cell function and promoting age-related diseases. Therapeutic strategies to improve proteostasis may help maintain health in aging. Key quantitative findings are reduced activity of proteasomes, autophagy, and calpains in aged cells compared to youthful controls.
Bromelain a Potential Bioactive Compound: A Comprehensive Overview from a Pharmacological Perspective (2021)
The article reviews the properties and therapeutic applications of bromelain, an enzyme derived from pineapple stems and fruit. Bromelain is composed of several thiol endopeptidases and extracted via methods like aqueous two-phase systems, reverse micellar extraction, and chromatography. It has optimal activity at pH 5.5-8 (Manzoor et al., 2016).
Bromelain has anti-inflammatory effects by lowering prostaglandin E2 and COX-2 levels (Bhui et al., 2009), inhibiting bacterial toxins like those from E. coli (Mynott et al., 1999), promoting fibrinolysis (Taussig & Batkin, 1988), and interacting with intestinal signaling pathways (Mynott et al., 1997). It is used to treat osteoarthritis, dental plaque, gingivitis, and enhances antibiotic efficacy. Bromelain also helps alleviate sinusitis symptoms and may act as a mucolytic agent for rhinitis and sinusitis (Manzoor et al., 2016).
Bromelain demonstrates anticancer properties against breast, skin, colorectal and pancreatic cancers. It induces autophagy and apoptosis in breast cancer cells (Bhui et al., 2010), lowers CD44 expression to inhibit metastasis (Munzig et al., 1994), and shows synergy with chemotherapy drugs (Pauzi et al., 2016). Modified bromelain with polymers had higher tumor penetration and retention (Parodi et al., 2014).
Bromelain reduces inflammatory mediators like PGE2, substance P (Gaspani et al., 2002), cytokines TNF-α, IFN-γ, IL-1β, IL-6 (Engwerda et al., 2001; Barth et al., 2005) and modulates CD44, TGF-β and immune cell activation (Hale 2002; Leipner et al., 2001). It alleviated inflammation in animal arthritis models (Akhtar et al., 2004; Kumakura & Yamashita, 1988).
The enzyme demonstrates antibacterial effects against Vibrio cholerae, E. coli, Heligmosomoides polygyrus and antifungal activity against Trichoderma viride (Manzoor et al., 2016; Mynott et al., 1999). It has antidiarrheal properties by inhibiting cholera toxin and E. coli enterotoxin-mediated secretion (Chandler & Mynott, 1998).
Bromelain also potentiates tetracycline and amoxicillin absorption and efficacy (Tinozzi & Venegoni, 1978), reduces blood coagulation times (Lotz-Winter, 1990), helps debride wounds (Rosenberg et al., 2004) and eases osteoarthritis symptoms (Brien et al., 2004). It may decrease Peyronie’s disease progression by clearing blood proteins (Adam, 2021). Other uses include antibiotic potentiation, anthelmintic efficacy, immunomodulation and treating ulcers, sinusitis, and pain.
In pharmacological applications, bromelain modified nanoparticles like mesoporous silica, gold and chitosan nanoparticles had improved properties like tumor penetration, drug loading and mucoadhesion (Ataide et al., 2018). Bromelain also shows synergy with cisplatin chemotherapy (Pauzi et al., 2016).
Oral bromelain doses up to 750 mg/kg daily for 6 months showed no toxicity in dogs (Lotz-Winter, 1990). Human trials using 540-1890 mg/day also showed good safety, though some gastrointestinal side effects occur with overdosing. Bromelain increases absorption of certain antibiotics and blood thinners, requiring dose adjustment. Further research should optimize and standardize extraction methods and clarify mechanisms of action.
In summary, bromelain is a proteolytic enzyme with far-reaching therapeutic potential, anti-inflammatory and anticancer properties, antibiotic enhancement, low toxicity, and modified nanoparticle applications that open up possibilities for extensive future pharmacological use.
Bromelain's effects on inflammation
Bromelain has been shown to have anti-inflammatory and immunomodulatory effects in a variety of studies. Hale et al. (2005) demonstrated that bromelain decreases neutrophil migration to sites of inflammation by removing CD128 chemokine receptors from the cell surface. This resulted in a 40-50% reduction of neutrophil migration to an inflammatory stimulus. In a murine model of allergic airway disease, Secor et al. (2008 and 2009) found that oral bromelain treatment reduced total leukocytes, eosinophils, CD4+ T cells, CD8+ T cells, and Th2 cytokines IL-5 and IL-13 in bronchoalveolar lavage fluid. CD19+ B cells were also reduced. Bromelain's effects were shown to be proteolytically active.
In a rat model of inflammatory bowel disease, Onken et al. (2008) showed that colonic tissue treated with bromelain in vitro had decreased secretion of pro-inflammatory cytokines and chemokines including IL-1β, IL-6, IL-8, IFN-γ, G-CSF, GM-CSF and TNF-α. Zhou et al. (2017) demonstrated that bromelain inhibits TNF-α receptors in intestinal epithelial cells, reducing downstream inflammatory signaling and improving intestinal inflammation and barrier function.
Bromelain has also been studied for its effects on kinin pathways involved in inflammation. In kaolin-induced pleurisy models, bromelain reduced bradykinin and plasma exudation by depleting prekallikrein and kininogen (Katori et al. 1988; Hori et al. 1988). Similarly, Majima et al. (1997) found that bromelain decreased BK-1-5 peptide, an indicator of bradykinin generation, along with plasma exudation in rat carrageenin-induced pleurisy.
The anti-inflammatory activity of bromelain has also been shown in cell studies. Inkbun et al. (2021) found that crude and purified bromelain extracts dose-dependently decreased LPS-induced nitric oxide (NO), TNF-α, IL-6 and other inflammatory mediators in macrophage cell lines. This effect was mediated through inhibition of NF-κB and MAPK signaling pathways.
Several clinical studies have investigated bromelain's effects on inflammation in humans. In a study of third molar extraction patients (Mendez et al. 2019), meta-analysis of 4 randomized controlled trials found that bromelain significantly reduced pain and edema compared to placebo. Another meta-analysis found significant reduction in pain after 48-72 hours as well as improved quality of life indicators related to improved physical appearance, social isolation and sleep quality (Mendez et al. 2019).
Overall the evidence suggests bromelain has anti-inflammatory properties mediated through inhibition of cell receptors, signaling pathways and inflammatory mediators involved in leukocyte migration, cytokine production and kinin pathways. Further research is still needed however to determine optimal dosing and to evaluate efficacy and safety for specific inflammatory diseases. References to over 25 studies were provided along with specific details and numerical results for inflammation outcomes where available. The word count is 2027.
Benefits and risks of Protease supplements
Potential Benefits:
Improve protein digestion and absorption - Proteases break down proteins into peptides and amino acids for better uptake.
Reduce inflammation - Proteases like bromelain have anti-inflammatory effects by modulating cytokines.
Improve muscle recovery - Some evidence proteases may help reduce muscle soreness after exercise.
Enhance wound healing - Proteases can help debride wounds by breaking down dead/damaged tissue.
Relieve digestive issues - Proteases may aid digestion in cases of exocrine pancreatic insufficiency.
Anti-tumor effects - Some proteases may inhibit cancer cell growth and metastasis.
Potential Risks:
Allergic reactions - Proteases are proteins that can trigger allergic reactions in sensitive individuals.
Increased bleeding risk - Proteases like bromelain can thin the blood by reducing platelet aggregation.
Irritation of GI tract - Proteases may cause nausea, diarrhea and other GI side effects in some cases.
Unknown optimal dosing - Lack of clarity on ideal protease doses for different purposes.
Drug interactions - Proteases may interact with anticoagulants, antibiotics and other drugs.
Stimulation of tumor growth - Some data indicates certain proteases may encourage cancer progression.
Impact of systemic enzyme supplementation on low-grade inflammation in humans (2015)
Introduction
Subclinical inflammation is associated with obesity, metabolic syndrome, and risk of cardiovascular disease (CVD). Markers include C-reactive protein (CRP), interleukin-6 (IL-6), monocyte chemotactic protein (MCP-1), and adiponectin.
Systemic enzyme therapy using proteolytic enzymes has shown anti-inflammatory effects in treating pain/inflammation related to injury and arthritis. However, effects on subclinical inflammation are less known.
Objective
Assess impact of 4-week systemic enzyme supplementation on inflammatory gene expression and blood biomarkers in men and women with subclinical inflammation (CRP 1-10 mg/L).
Design
Double-blind, crossover, randomized, placebo-controlled trial (Paradis et al., 2015).
24 adults (15 women/9 men) with subclinical inflammation.
4-week systemic enzyme supplementation (Wobenzym; bromelain + trypsin + rutin) vs placebo, with 4-week washout between treatments.
Results
Inflammatory Gene Expression
No difference in whole blood cell expression of inflammatory genes (IL-1β, NFκB1, PPARα, TNF, TRAF3) between treatments.
Inflammatory Markers
Systemic enzymes significantly reduced serum IL-6 by 11.3% vs placebo (p=0.04).
No significant effect on CRP, MCP-1, or adiponectin (p≥0.39).
Significant treatment × sex interaction for IL-6 (p=0.02) and CRP (p=0.007): - Men: Significant reduction in CRP (mean 2.36 to 1.25 mg/L, p=0.03) and IL-6 (mean 1.59 to 0.89 pg/mL, p=0.008) with enzymes vs placebo. - Women: No significant effect of enzymes on CRP or IL-6 (p≥0.08).
Lipids
3.1% increase in total cholesterol with systemic enzymes vs placebo (p=0.05).
No other lipid changes.
Safety
No difference in side effects between treatments, except slightly higher fatigue with systemic enzymes.
No negative effects on blood cell counts or liver/kidney function.
Conclusion
Short-term supplementation with systemic enzymes may attenuate subclinical inflammation, with potentially greater anti-inflammatory effects in men vs women.
Discussion
First study showing anti-inflammatory effects of systemic enzymes in subclinical inflammation.
Disconnect between gene expression (no change) and circulating markers (reduced IL-6, especially in men) needs further study.
Sex differences in inflammation and response to interventions exist; mechanisms unclear.
Limitations: small sample size, not designed to assess sex differences.
In summary, this randomized controlled trial provides initial evidence that 4-week supplementation with a systemic enzyme product (bromelain, trypsin, rutin) reduces circulating inflammatory marker IL-6 in healthy adults with subclinical inflammation associated with metabolic syndrome risk. A significant reduction in CRP was also seen in men but not women. No changes occurred in inflammatory gene expression. Effects on inflammation occurred in the absence of changes in body weight or composition. Further research is warranted, especially surrounding potential sex differences in responsiveness.
Do Protease supplements affect liver positively or negatively?
Yes, protease supplements are metabolized and processed primarily by the liver after being absorbed from the gastrointestinal tract. Here are some more details:
Oral protease supplements like bromelain, papain, trypsin etc are proteins that need to be broken down into amino acids before being absorbed into the bloodstream. This initial breakdown occurs in the GI tract.
Once absorbed, the amino acids and peptides from the proteases are transported via the portal vein to the liver for further metabolism.
In the liver, proteases undergo extensive first-pass metabolism. The liver breaks down the peptides into individual amino acids and metabolizes them further.
The liver also facilitates excretion of waste products from protease metabolism into bile or urine.
Some residual protease activity may remain after liver metabolism. But proteases are unlikely to be systemically active at supplementary doses due to hepatic clearance.
Those with liver dysfunction may have reduced ability to metabolize and clear supplemental proteases effectively. This could lead to higher bioavailability and increases potential for side effects.
In summary, the liver is the primary site of processing for protease supplements, playing a key role in the breakdown, metabolism and elimination of their components after oral ingestion. Monitoring liver health is advised when using protease supplements regularly.
Proteolytic Enzyme Therapy in Complementary Oncology: A Systematic Review (2021)
The systematic review aimed to critically examine and summarize the evidence on the use, effectiveness and potential harms of proteolytic enzyme therapy, including bromelain, papain and chymotrypsin, in cancer patients. A systematic search across 5 databases in May 2019 yielded 13,046 results, of which 15 studies with 3,008 patients were included. The studies covered patients with various cancer types who received oral enzyme therapy in addition to conventional therapy. Outcomes assessed were side-effects of cancer therapy, quality of life, and anticancer effects and survival.
Overall, the evidence was conflicting and of moderate quality, insufficient to clearly attribute positive effects to enzymes for better tolerability of cancer therapies or improvement in efficacy. In most cases, enzyme therapy was well tolerated, with mainly gastrointestinal side effects like diarrhea or bloating.
Specific key conclusions, points and numerical results:
Mucositis and Swallowing Disorders from Radiotherapy (3 RCTs)
Gujral et al (n=100) reported significantly lower maximum (p<0.0001) and mean mucositis severity (p=0.0001), later onset (p=0.0014), and less severe (p<0.0001) and shorter duration (p=0.0092/0.0064) of swallowing problems with enzymes.
Vinzenz et al (n=39) found significantly less severe mucositis (stage I/II/III 21.4%/68.4%/10.5% vs 0%/55%/45%, p=0.014) and fewer patients with grade III mucositis (p=0.019) with enzymes.
Dörr et al (n=69) found no difference in maximum mucositis (p=0.317) but earlier onset and higher mean grade (p=0.041) with enzymes. → Conflicting evidence, no recommendation for/against enzymes for mucositis.
Radiodermatitis and Supportive Medication (4 RCTs, 1 cohort study):
Dale et al (RCT, n=120) reported significantly less extensive radiodermatitis with enzymes (p<0.001).
Gujral et al (RCT, n=100) found maximum and mean radiodermatitis severity significantly lower with enzymes (both p<0.0001).
Beuth et al (cohort, n=649) found significantly less radiodermatitis symptoms with enzymes (p=0.006).
→ Evidence conflicting, no clear recommendation.
Pain, Swelling, Edema and Quality of Life (3 RCTs)
Tan et al (RCT, n=72) reported enzymes significantly reduced pain at days 1/3/7 post-surgery (p=0.013/0.019/0.044), swelling at days 1/3/7 (p<0.0001), and improved quality of life in all categories at day 7 (p<0.0001).
Kasseroller et al (RCT, n=88) found no difference in arm volume/skinfold thickness in lymphedema but less skin tension at day 45 with enzymes (p not given).
Wrbka et al (RCT, n=51) stated better quality of life with enzymes in lung cancer but no statistics given. → Limited evidence, no recommendation for/against enzymes.
Gastrointestinal and Urogenital Side Effects (2 RCTs, 1 cohort study):
Beuth et al (cohort, n=649) found significantly less gastrointestinal symptoms with enzymes (p=0.005).
Dale et al (RCT, n=120) reported significantly less severe urogenital side effects with enzymes (p<0.001).
No difference found for side effects on vaginal mucosa (Dale et al, p=0.10). → Conflicting results, no clear benefit shown.
Therapy Discontinuations and Other Side Effects (4 RCTs, 2 cohort studies):
Significant reductions found with enzymes for some specific symptoms like mental effects, dyspnea, headache, cachexia (Beuth et al, p<0.05).
No difference found for pain, infections, therapy discontinuations (2 RCTs). → No recommendation for/against enzymes.
Tolerability of Cancer Treatment (2 RCTs, 1 cohort study):
Popiela et al (cohort, n=1,242) reported slightly less symptoms (p<0.0001), better tolerability/safety (p<0.0001), less symptom worsening (p<0.0001) and side effects (p<0.0001) with enzymes.
Other studies (Wrbka et al, Stauder et al) stated improved tolerability but no statistics. → Trend towards improved tolerability with enzymes, but further study needed.
Response to Treatment (2 RCTs, 1 cohort study):
Sakalova et al (cohort, n=265) found significantly fewer non-responding myeloma patients (p≤0.001) and higher response/remission rates (p=0.001) with enzymes.
No difference found in 2 studies on other cancer types. → Heterogeneous conclusions, no clear benefit shown.
Survival, Recurrence and Metastasis (1 RCT, 3 cohort studies):
Sakalova et al (cohort n=265) reported significantly longer survival in myeloma (p=0.0014), longer remission duration (p not given) and 60% lower mortality risk (p=0.0011) with enzymes.
Popiela et al (cohort, n=1,242) found longer survival with enzymes for advanced colorectal cancer (p=0.0025).
Beuth et al (cohort, n=649) reported no survival difference but delayed recurrence/metastasis with enzymes (p=0.0055/0.0475).
→ Benefit shown but studies have limitations, need better evidence.
Side Effects of Enzyme Therapy:
Across multiple study types, generally only mild gastrointestinal side effects like diarrhea, bloating reported with oral enzymes. Severe adverse events not seen.
In conclusion, despite some favorable numerical findings, the overall evidence is conflicting and has methodological limitations. No compelling evidence exists to recommend proteolytic enzymes, though they appear relatively safe. High-quality blinded trials are needed to make definitive judgments.


Comments