Ezetimibe
Ezetimibe is a medication that helps lower levels of cholesterol in the body. Its mechanism of action is different from other cholesterol-lowering drugs like statins, which work primarily in the liver.
Ezetimibe works in the digestive tract, where it blocks the absorption of cholesterol. Specifically, it targets the Niemann-Pick C1-Like 1 (NPC1L1) protein in the brush border of the small intestine. NPC1L1 is critical for the uptake of dietary and biliary cholesterol from the intestine.
By blocking the NPC1L1 protein, ezetimibe prevents cholesterol from being absorbed into the body, and as a result, less cholesterol ends up in the bloodstream. This helps to reduce the overall levels of LDL ("bad") cholesterol and can reduce the risk of developing atherosclerotic plaques, which are associated with heart disease.
It should be noted that ezetimibe doesn't inhibit the absorption of triglycerides, fat-soluble vitamins, or other important nutrients. It is also often used in combination with statins, as the two drugs have complementary mechanisms and can achieve a greater reduction in cholesterol levels than either drug alone.
Ezetimibe for the treatment of non-alcoholic fatty liver disease: A meta-analysis, 2017
Aim: Several studies on the efficacy of ezetimibe, a potent inhibitor of cholesterol absorption, in treating non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) have been published; however, the results are inconsistent. We undertook a meta-analysis to evaluate the efficacy of ezetimibe in treating NAFLD and NASH.
Methods: PubMed, Medline, and Cochrane Library Full Text Database were searched until June 2016. The main inclusion criteria included original studies investigating the use of ezetimibe for the treatment of NAFLD and NASH. Identification of published work and data extraction were carried out by two reviewers based on the inclusion and exclusion criteria. All analyses were carried out using Comprehensive Meta-Analysis version 3 software.
Results: An initial search identified 103 peer-reviewed articles and abstracts. Six studies (two randomized controlled and four single-arm trials) involving 273 participants with NAFLD and NASH were identified. Ezetimibe significantly reduced serum aspartate aminotransferase, alanine aminotransferase, and γ-glutamyl transpeptidase levels, and hepatic steatosis and hepatocyte ballooning. However, hepatic inflammation and fibrosis did not improve by ezetimibe treatment in patients with NAFLD and NASH. In randomized controlled trials, only hepatocyte ballooning improved with ezetimibe treatment.
Conclusions: Although ezetimibe attenuated serum liver enzymes and hepatic steatosis and ballooning in six studies, it improved only hepatocyte ballooning in randomized controlled trials. Larger studies and more randomized placebo-controlled trials are necessary to determine the effects of ezetimibe on NAFLD and NASH.
Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: an open-label randomized controlled trial (ESSENTIAL study), 2022
Background
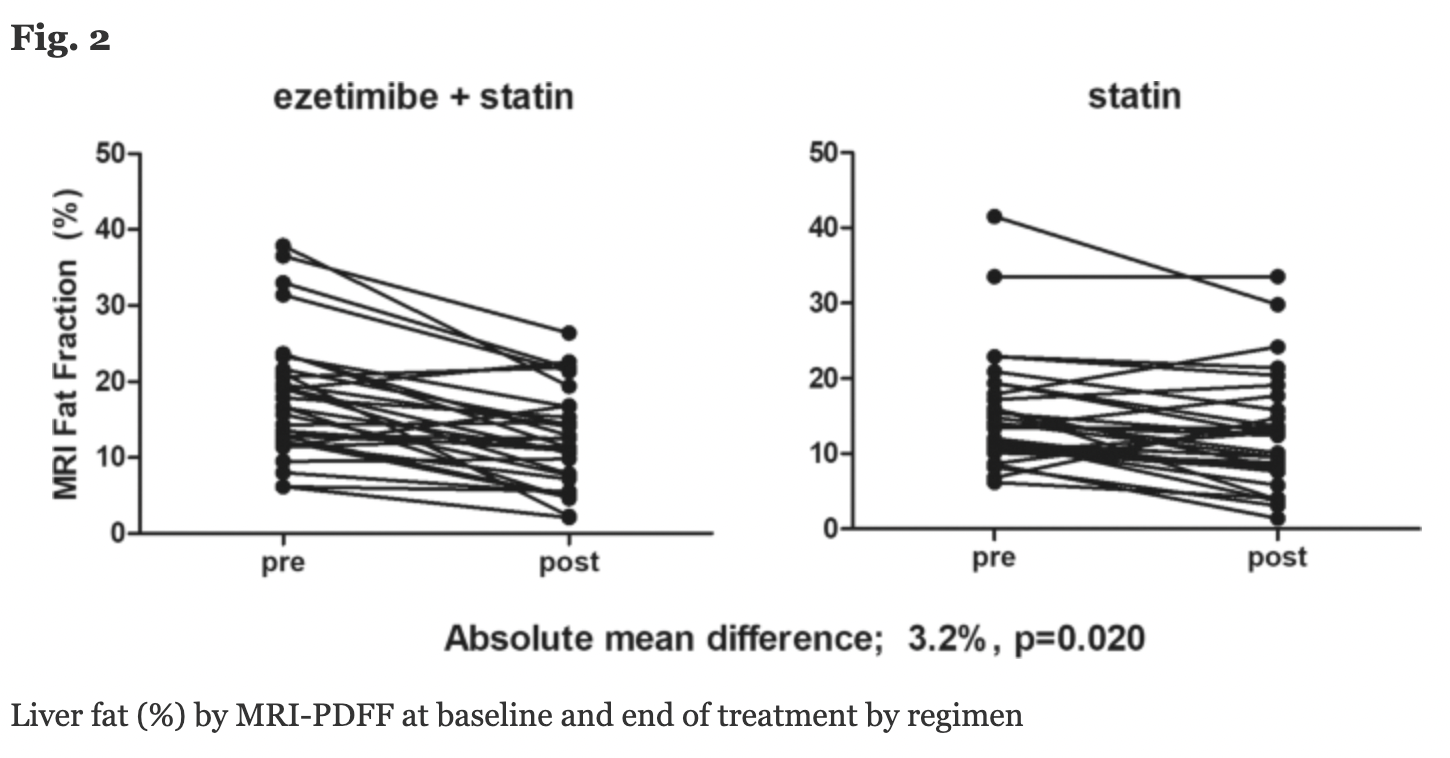
The effect of ezetimibe, Niemann-Pick C1-like 1 inhibitor, on liver fat is not clearly elucidated. Our primary objective was to evaluate the efficacy of ezetimibe plus rosuvastatin versus rosuvastatin monotherapy to reduce liver fat using magnetic resonance imaging-derived proton density fat fraction (MRI-PDFF) in patients with non-alcoholic fatty liver disease (NAFLD).
Methods
A randomized controlled, open-label trial of 70 participants with NAFLD confirmed by ultrasound who were assigned to receive either ezetimibe 10 mg plus rosuvastatin 5 mg daily or rosuvastatin 5 mg for up to 24 weeks. The liver fat change was measured as average values in each of nine liver segments by MRI-PDFF. Magnetic resonance elastography (MRE) was used to measure liver fibrosis change.
Results
Combination therapy significantly reduced liver fat compared with monotherapy by MRI-PDFF (mean difference: 3.2%; p = 0.020). There were significant reductions from baseline to study completion by MRI-PDFF for both the combination and monotherapy groups, respectively (18.1 to 12.3%; p < 0.001 and 15.0 to 12.4%; p = 0.003). Individuals with higher body mass index, type 2 diabetes, insulin resistance, and severe liver fibrosis were likely to be good responders to treatment with ezetimibe. MRE-derived change in liver fibrosis was not significantly different (both groups, p > 0.05). Controlled attenuation parameter (CAP) by transient elastography was significantly reduced in the combination group (321 to 287 dB/m; p = 0.018), but not in the monotherapy group (323 to 311 dB/m; p = 0.104).
Conclusions
Ezetimibe and rosuvastatin were found to be safe to treat participants with NAFLD. Furthermore, ezetimibe combined with rosuvastatin significantly reduced liver fat in this population.

A Comparison of Ezetimibe and Acarbose in Decreasing Liver Transaminase in Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial, 2013
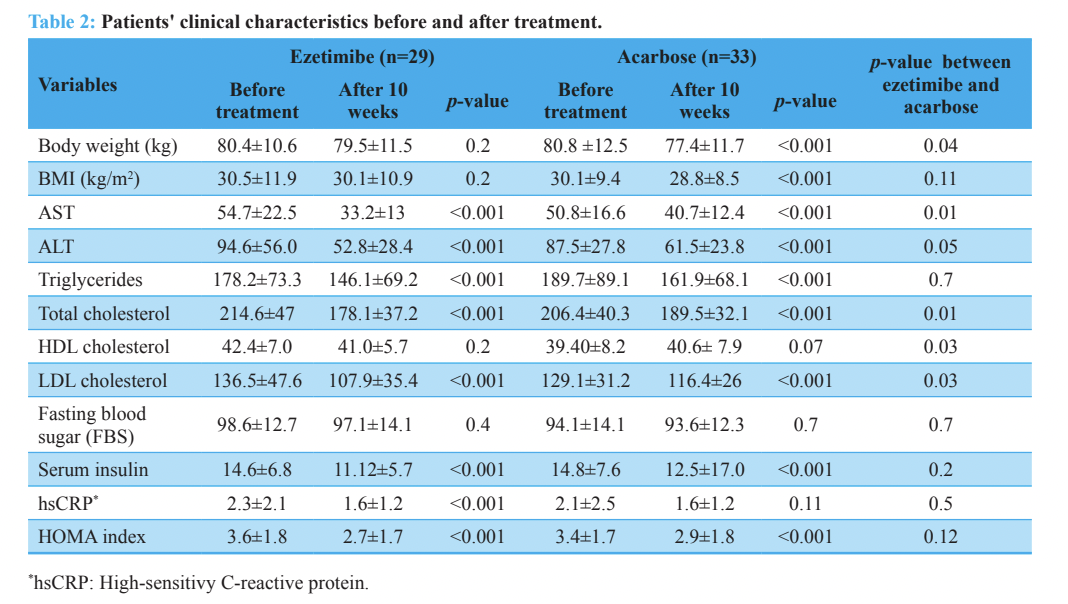
This was a single center, double-blind, parallel-group study conducted at Bu-Ali Sina Hospital, Qazvin, Iran. In this trial, we enrolled, by simple randomization, a total of 62 patients diagnosed with NASH. There were 29 patients treated with ezetimibe and 33 who were treated with acarbose over a ten-week period.
Results
Ezetimibe treatment significantly reduced ALT, AST, triglycerides, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-sensitivity C-reactive protein (hsCRP), and serum insulin levels and the insulin resistance homeostasis model assessment (HOMA-IR) index compared to patients treated with acarbose (p<0.001). Ezetimibe treatment decreased ALT (p=0.05), AST (p=0.01), total cholesterol (p=0.01), HDL cholesterol (p=0.03) and LDL cholesterol (p=0.03) levels to a significantly higher extent.
Conclusion
Both ezetimibe and acarbose improved metabolic and biochemical abnormalities in patients with NASH, however these effects were more prominent with ezetimibe.
Novel Role of NPC1L1 in the Regulation of Hepatic Metabolism: Potential Contribution of Ezetimibe in NAFLD/NASH Treatment
Abstract
Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in Western countries and also in other parts of the world. NAFLD encompasses a histological spectrum ranging from simple steatosis to steatohepatitis, advanced fibrosis and inflammatory changes. It frequently occurs with features of the metabolic syndrome including obesity, type 2 diabetes mellitus, dyslipidemia and hypertension. In fact, the metabolic syndrome is a strong predictor of NAFLD. Recently, Niemann-Pick C1-like 1 (NPC1L1) has been shown to play a pivotal role in cholesterol absorption. Unlike mouse NPC1L1 protein, predominantly expressed in the intestines, human and rat NPC1L1 is also abundantly expressed in the liver. Though the exact functions of hepatic NPC1L1 remain unknown, NPC1L1 may facilitate the hepatic accumulation of cholesterol. This raises a potential possibility that ezetimibe may improve fatty liver formation. In this review, potential role of lipid metabolism in NAFLD and its possible modulation through NPC1L1 blockade is discussed.

Combination Therapy of Ezetimibe and Rosuvastatin for Dyslipidemia: Current Insights, 2022
Rosuvastatin is one of the most potent HMG-CoA reductase inhibitors available and can lower LDL-C up to 55%.5 Additional beneficial impacts on the cholesterol panel include an increase in HDL-C by approximately 6% and lowering of triglycerides (TG) by 15% or greater as well as a decrease in the cholesterol content in atherosclerotic plaques.6 Rosuvastatin also exerts pleiotropic effects including anti-inflammatory effects, endothelial protection, and antioxidant effects.7,8 Benefits of rosuvastatin over other statins include its hydrophilicity which is associated with very low rates of myopathy and rhabdomyolysis as well as its long duration of action allowing it to be taken at any time of day.9 Additionally, only approximately 10% of the drug is transformed by the Cytochrome P450 enzymes and the other 90% is excreted via biliary means leading to very few drug–drug interactions.
Ezetimibe is the only drug in its class and works by inhibiting NPC1L1 leading to a decrease in absorption of cholesterol by up to 67% resulting in a lowering of LDL-C by about 15–20%.10 The impact on HDL-C is an increase of about 3% with no impact on TG. In addition to its anti-inflammatory effects, the combination of ezetimibe and statin lower high sensitivity CRP approximately 10% more than statin monotherapy.11 Ezetimibe is metabolized via glucuronidation and thus has minimal drug interactions, like rosuvastatin.12
Ezetimibe is a cost-effective choice for improving LDL-C reduction in patients at risk for cardiovascular disease or those who are statin intolerant, being preferable to PCSK9-inhibitors due to its oral administration, lower cost, and comparable benefits.
The EXPLORER trial compared rosuvastatin combination therapy with ezetimibe (40/10 mg) to rosuvastatin monotherapy (40 mg) in high-risk cardiovascular patients with hypercholesterolemia. Patient’s mean LDL-C levels significantly decreased in the combination group at 69.8% (mean 189 to 57 mg/dl) compared to 57.1% (mean 191 to 82 mg/dl) in the monotherapy group (p < 0.001). Most patients on combination therapy were able to achieve their LDL-C goal of less than 100 mg/dL in comparison to patients on monotherapy (94.0% vs 79.1%, p < 0.001). Moreover, combination therapy showed superior decreases in non-HDL-C, total cholesterol, and triglycerides, and had a greater effect on reducing inflammation, measured by high-sensitivity C-reactive protein. Both treatments were similarly tolerated, affirming rosuvastatin/ezetimibe as a more efficacious yet similarly safe option for achieving LDL-C targets in high-risk ASCVD or CAD patients.
Studies Assessing Atherosclerotic Plaque Burden
Additional benefits of LDL reduction therapy include a prevention of ASCVD events which are often mediated via reduction of atherosclerotic plaque volume. Masuda et al conducted a prospective, open-label, randomized, single-center study examining the effect of 6 months of rosuvastatin 5 mg and ezetimibe 10mg to rosuvastatin 5 mg alone on coronary plaque regression.22 Patients were eligible if they had stable angina and were to receive an elective percutaneous coronary intervention (PCI) with at least one obstructive lesion and an LDL-C greater than 100 mg/dL. A total of 51 patients were randomized, and while reductions in plaque volume were seen in the combination arm as measured by intravascular ultrasound (IVUS), statistical significance was not seen (−13.2% vs −3.1%; p = 0.05) which may be due to the small number of patients studied. Despite not reaching statistical significance in the primary measure, secondary measures of correlation between percent change in plaque volume and LDL (r = 0.384, p = 0.015) and non-HDL (r = 0.334, p = 0.035) both reached statistical significance.
A prospective, single center, randomized study in China compared patients with borderline or severe atherosclerosis receiving either rosuvastatin/ezetimibe 10/10 mg or rosuvastatin 10 mg.23 A total of 106 patients were randomized and atherosclerotic plaque measurement was completed via IVUS 12 months post treatment with combination versus monotherapy as a secondary outcome. This assessment determined a statistically significant reduction in percent plaque burden (62.1%±7.2 vs 68.2%±8.3) in those receiving combination rosuvastatin/ezetimibe (p < 0.05), suggesting that the combination may impact coronary plaque burden in patients with coronary artery disease.
Eliminating atherosclerotic cardiovascular disease residual risk, 2023
Many facts suggest that a desirable, physiologic level of LDL cholesterol is far lower than previously assumed:
Serum LDL-C in utero and in newborns averages 20–40 mg/dL (0.52–1.03 mmol/L). During gestation and after birth, humans are forming new cells at prodigious rates yet require little contribution of cholesterol from LDL.
All cells of the body make their own cholesterol (plus a small portion derived from HDL-C).
Those born with complete absence of proprotein convertase subtilisin kexin type 9 (PSCK9; loss of function mutation) suffer no ill consequences from lifelong near zero circulating LDL-C and have no atherosclerosis.
Brown and Goldstein showed that fibroblast receptors for LDL are maximized at a concentration of 25 mg/dL (0.67 mmol/L) due to feedback control. Excess cholesterol beyond that is taken up either by hepatocytes or scavenger receptors on intimal macrophages that have no feedback control and thus accumulate much larger amounts of cholesterol.
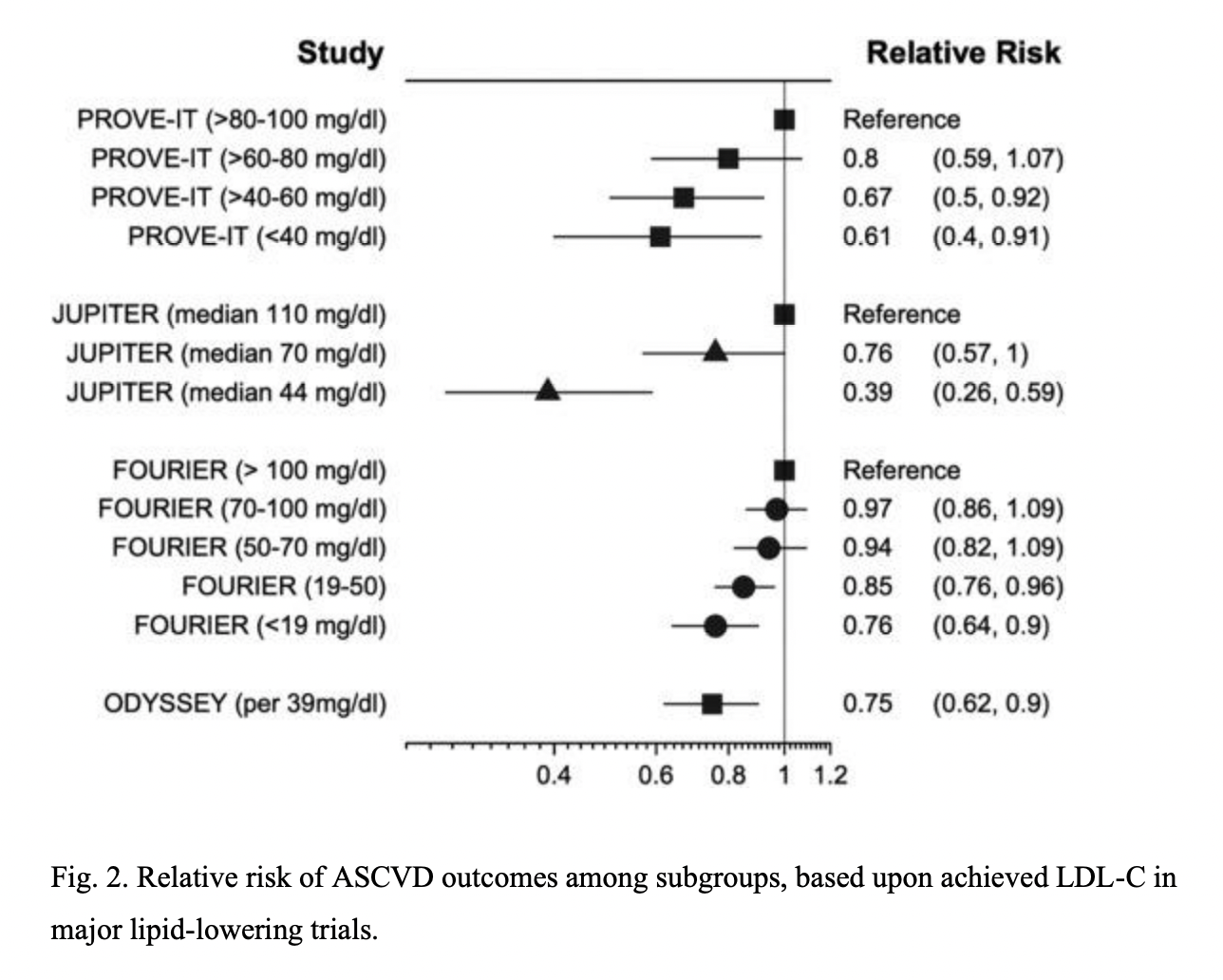
Randomized controlled trials (RCTs) and Mendelian randomization analyses demonstrate that there is log-linear relationship between atherosclerotic cardiovascular disease (ASCVD) and LDL-C at the highest levels down to near zero. The hazard ratio of 1.0 (meaning no excess risk) is achieved at an LDL-C of approximately 38 mg/dL (0.98 mmol/L).
Many RCTs show that lowering LDL-C at any stage is beneficial, but doing so as early as possible is far better.
Elevations in mid-life LDL-C also correlate with increased risk for neurologic disease, especially vascular and Alzheimer’s dementia, as well as Parkinson’s disease.

How much should LDL cholesterol be lowered in secondary prevention? Clinical efficacy and safety in the era of PCSK9 inhibitors, 2022
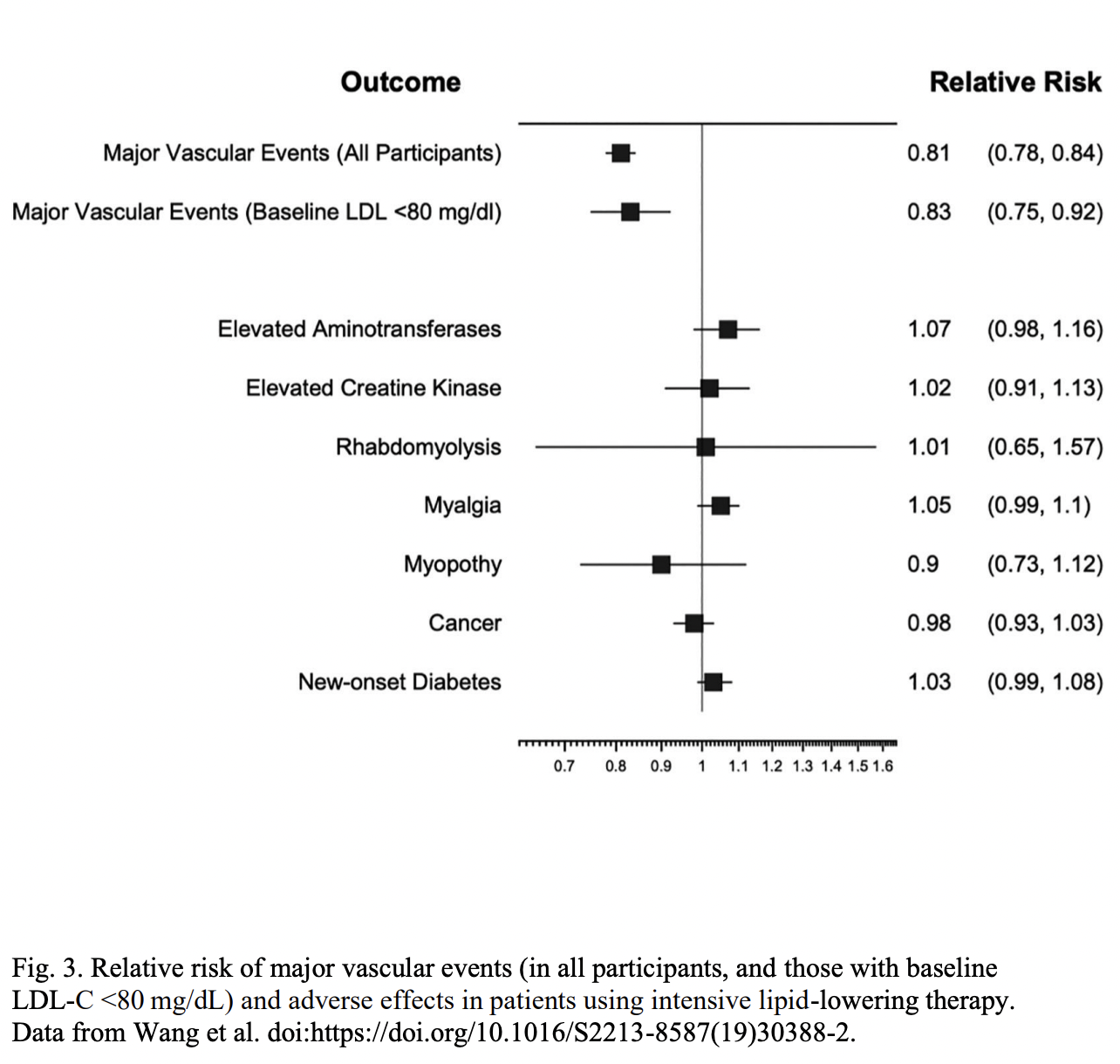
There is a strong evidence that more marked lowering of low-density lipoprotein cholesterol (LDL-C) leads to progressively lower risk of cardiovascular disease (CVD) events. The evidence on validity of this hypothesis comes from epidemiological, genetic and clinical studies. The hypothesis "the lower the better" has been recently strongly supported by the results of secondary prevention trials with PCSK9 inhibitors. The combination of PCSK9 inhibitors and statins has resulted in achieving extremely low LDL-C levels with additional reduction of CVD events in secondary prevention. However, despite large clinical benefits, the safety of aggressive LDL-C lowering should be always taken into consideration, and there is still an ongoing discussion on whether very low LDL-C might result in some non-CVD adverse events. However, based on the available knowledge, so far the serious adverse events associated with achieving of very low LDL-C levels or intensive drug therapy have not been noted. These positive clinical effects were reflected in current ESC/EAS Guidelines (2019) for dyslipidaemia management. The experts strongly recommended the LDL-C lowering to levels that have been achieved in trials of PCSK9 inhibitors. In this state of the art review, we aimed to finally justify the critical need for LDL-C reduction to very low levels in secondary prevention patients in order to be as low as possible, as early as possible, and preferably lifelong.
LDL-C targets in patients with acute coronary syndromes (ACS) have been incrementally reduced in response to the results of randomized clinical trials (RCTs).
Initially, the target LDL-C level for secondary prevention was <100 mg/dL. This was based on the results of the Cholesterol and Recurrent Events (CARE) study, which showed that pravastatin 40 mg/d reduced LDL-C level by 32% and the risk of coronary death and myocardial infarction by 24% in patients after myocardial infarction (MI).
The target LDL-C level for post-ACS patients was then reduced to <70 mg/dL based on the results of the Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis In Myocardial Infarction 22 (PROVE IT TIMI 22) study. This study showed that intensive statin therapy (atorvastatin 80 mg/d) reduced LDL-C level by 32% and the combined endpoint of death, myocardial infarction, unstable angina requiring hospitalization, coronary revascularization, and stroke by 16% compared to moderate-intensity statin therapy (pravastatin 40 mg/d).
The current target LDL-C level of <55 mg/dL for the highest risk patients, including those with ACS and/or CVD, was decided based on the results of the IMPROVE-IT, FOURIER, and ODYSSEY OUTCOMES studies.
The IMPROVE-IT study showed that simvastatin 40 mg/d + ezetimibe 10 mg/d reduced LDL-C level by 32% and the rate of CV events by 6.4% compared to simvastatin 40 mg/d alone in patients with ACS and LDL-C level 50-100 mg/dL.
The FOURIER study showed that evolocumab 140 mg every two weeks or 420 mg every four weeks subcutaneously reduced LDL-C level by 59% and the risk of cardiovascular events by 15% in patients with atherosclerotic CVD and baseline LDL-C level ≥70 mg/dL.
The ODYSSEY OUTCOMES study showed that alirocumab 75 mg every two weeks subcutaneously reduced LDL-C level by 40% and the rate of cardiovascular events by 15% in patients with a history of ACS and LDL-C ≥70 mg/dL, non-HDL-C ≥100 mg/dL, or apo B level ≥80 mg/dL.
These trials demonstrated that a progressive reduction of atherosclerotic cardiovascular events could be achieved by reducing LDL-C levels using intensive combined lipid-lowering therapy.


Comments