Pioglitazone
Pioglitazone (Thiazolidinediones / TZDs / PPARγ activators)
GENERAL EFFECTS:
Pioglitazone, and Thiazolidinediones (TZD) in general, is a unique class of glucose-lowering drugs that function as PPAR-gamma activators, improving insulin sensitivity and target many features of aging and T2D (2021).
Across studies in diabetics and non-diabetics, Pioglitazone
Helps lower fasting insulin levels and insulin resistance significantly.
Reduces the levels of chronic inflammation significantly with effects additive to a Statin (2010).
Reduces visceral fat (2005), specifically in the liver, helping resolve conditions like NASH (2010, 2018).
Boosts adiponectin production.
On the negative side, Pioglitazone
Increases subcutaneous fat and fluid retention by redistributing fat from visceral to subcutaneous areas (2005).
Increases body weight but this side effect can be managed by keeping the dose low (e.g. 7.5mg daily) (2006, 2018, 2022).
Is associated with increased rates of heart failure (RR 1.32; CI 1.14 to 1.54), bone fracture (RR 1.52, 95% CI 1.17 to 1.99), oedema (RR, 1.63; CI 1.52 to 1.75) (2017).
Due to its negative side-effects, Pioglitazone is usually considered a fourth line of therapy in T2D after metformin, GLP1-RA and SGLT2 (2021). However, its insulin sensitizing and visceral fat reducing effects are among the very best.
AGING OUTCOMES:
33% reduction in the risk of all-cause mortality when exposed to Pioglitazone in a European study of 56,337 T2D patients (2017, 2018).
53% reduction in the risk of all-cause mortality in a 13-year retrospective cohort study from Taiwan in patients with T2DM receiving insulin (2020).
Meta-analysis of RCTs comparing Pioglitazone with either placebo or active comparators didn’t find a statistically-significant effect on MACE (MH–OR: 0.90, 95% CI 0.78–1.03) or all-cause mortality (0.91, 95% CI 0.77, 1.09). Pioglitazone statistically significantly reduced MACE in patients with prior cardiovascular events (MH–OR 0.84, 95% CI 0.72–0.99) (2022).
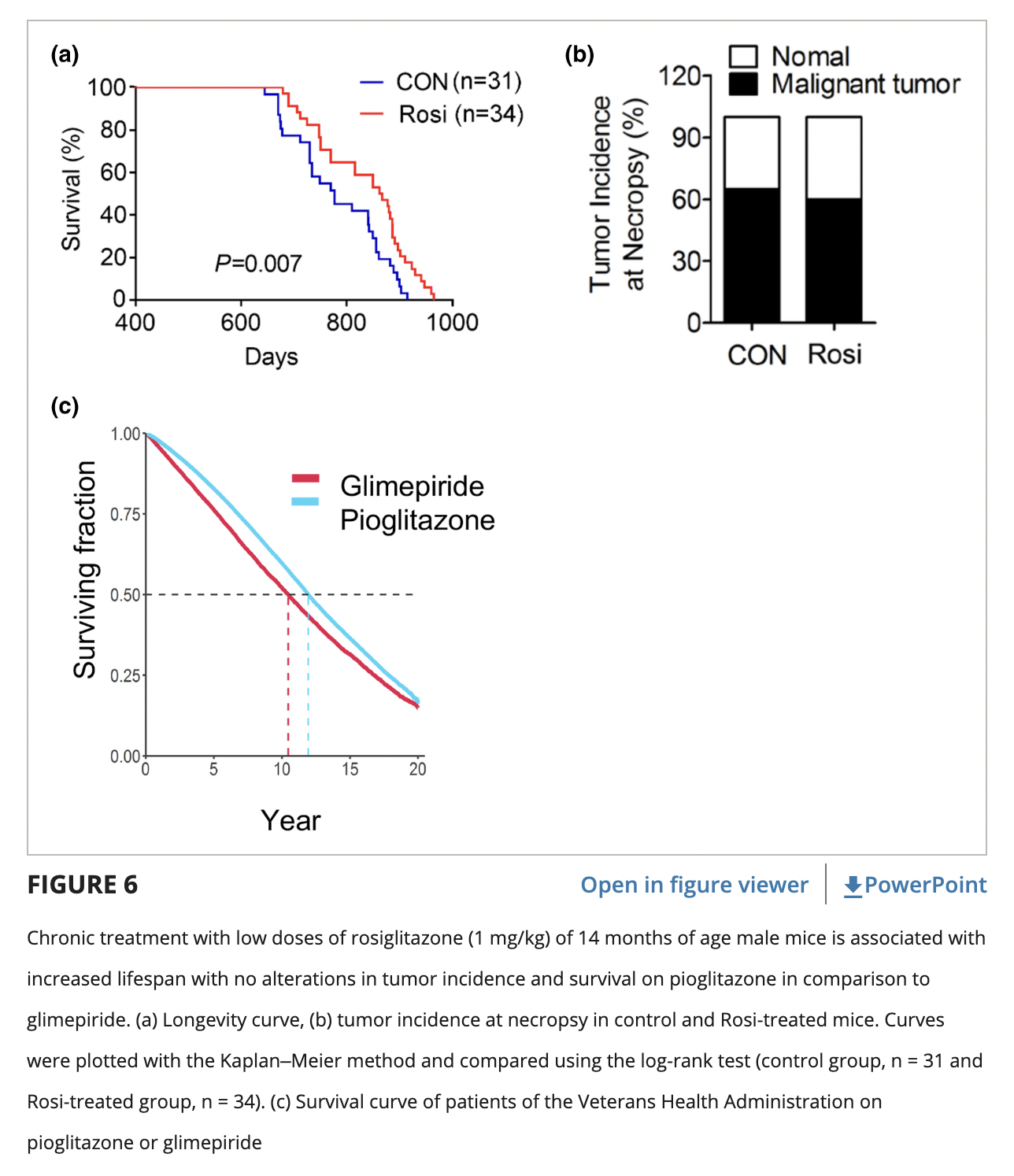
Rosiglitazone, another PPAR-gamma agonist, extended mice lifespan when started at 14 months of age. It improved glucose metabolism and mitochondrial functionality, reduced inflammation and tissue atrophy, improved cognitive function, and diminished anxiety- and depression-like behaviors (2020).
Pioglitazone significantly extended C. Elegans lifespan and healthspan through the inhibition of insulin/insulin-like signaling (IIS) and reproductive signaling pathways, activation of dietary restriction-related pathways, and its antioxidative activity (2022).
NASH:
A 2010 study compared compared Pioglitazone against placebo:
Serum ALT (-40 U/L), AST (-20 U/L) and GGT (-21 U/L) levels were significantly reduced with Pioglitazone as compared with placebo (P<0.001).
The difference in the rate of improvement in NASH with Pioglitazone vs placebo was relatively minor (34% vs. 19%, P=0.04).
Pioglitazone was associated with reductions in hepatic steatosis and lobular inflammation but not with an improvement in fibrosis score.
A 2018 study compared Pioglitazone against placebo in patients with and without T2D:
The primary outcome of a reduction in NALFD score of 2 points or more was met by 48% of patients with type 2 diabetes and by 46% without diabetes.
Pioglitazone led to NASH resolution in 44% of patients with type 2 diabetes vs. 26% without diabetes. Only patients with type 2 diabetes observed a significant reduction in liver fibrosis (P = .035).
Pioglitazone reduced intrahepatic triglyceride content by 11% ± 2% in patients with diabetes vs. a reduction of 9% ± 2% in patients without diabetes (P = .62); it also reduced the plasma level of alanine aminotransferase by 50 ± 10 U/L in patients with diabetes vs. a reduction of 36 ± 5 U/L in patients without diabetes.
ANTI-CANCER:
In Myeloproliferative Neoplasms (MPNs), Pioglitazone was found to promote the resolution of myelofibrosis by reducing myeloproliferation, modulating inflammation, and protecting the bone marrow stroma in three separate mouse models 2021.
In Chronic Myeloid Leukemia (CML), Pioglitazone combined with imatinib demonstrated an enhanced therapeutic response by 12 months compared to imatinib alone in a human trial 2017.
In Acute Myeloid Leukemia (AML), the complete remission rate was 20% higher in the pioglitazone group compared to the control group (P = .202) 2019. The mean serum ALT in the fourth treatment week was significantly more in pioglitazone group compared to the control group (65.5 vs. 33.6 mg/dL, P = .039). The mean serum creatinine in all treatment phases was significantly higher in the pioglitazone group compared to the control group (P < .05).
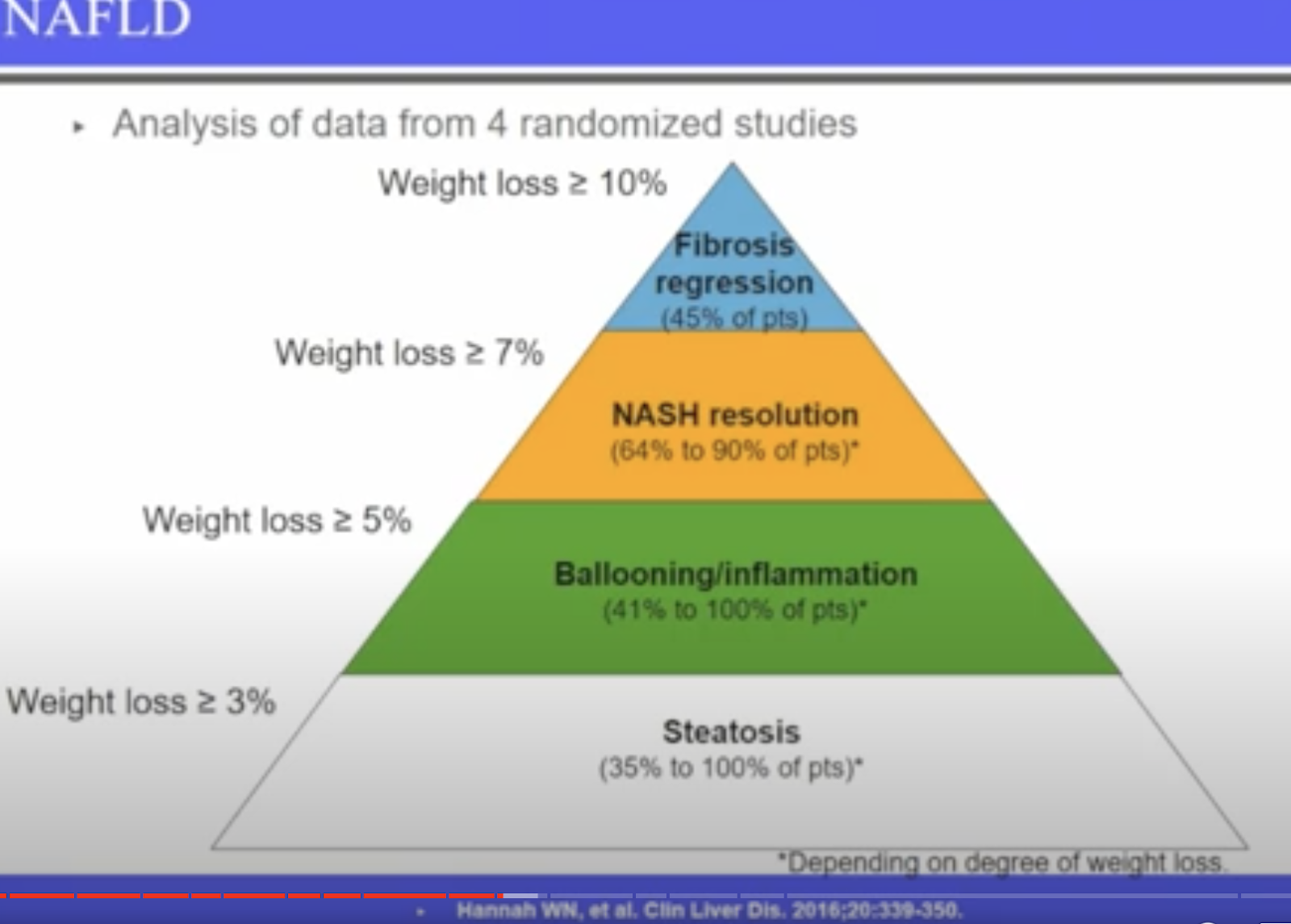
NAFLD/NASH Present & Future Management Options (video)

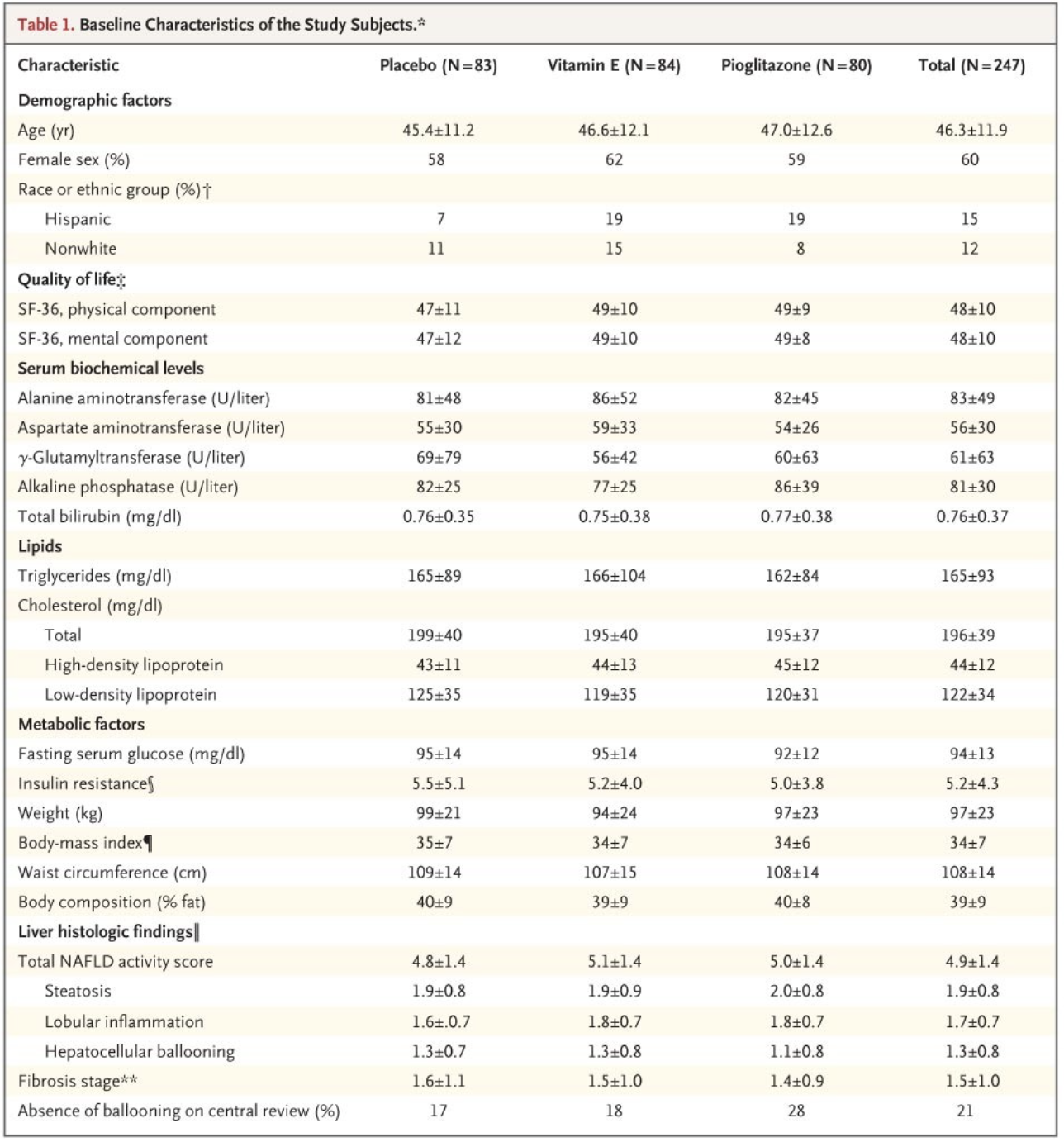
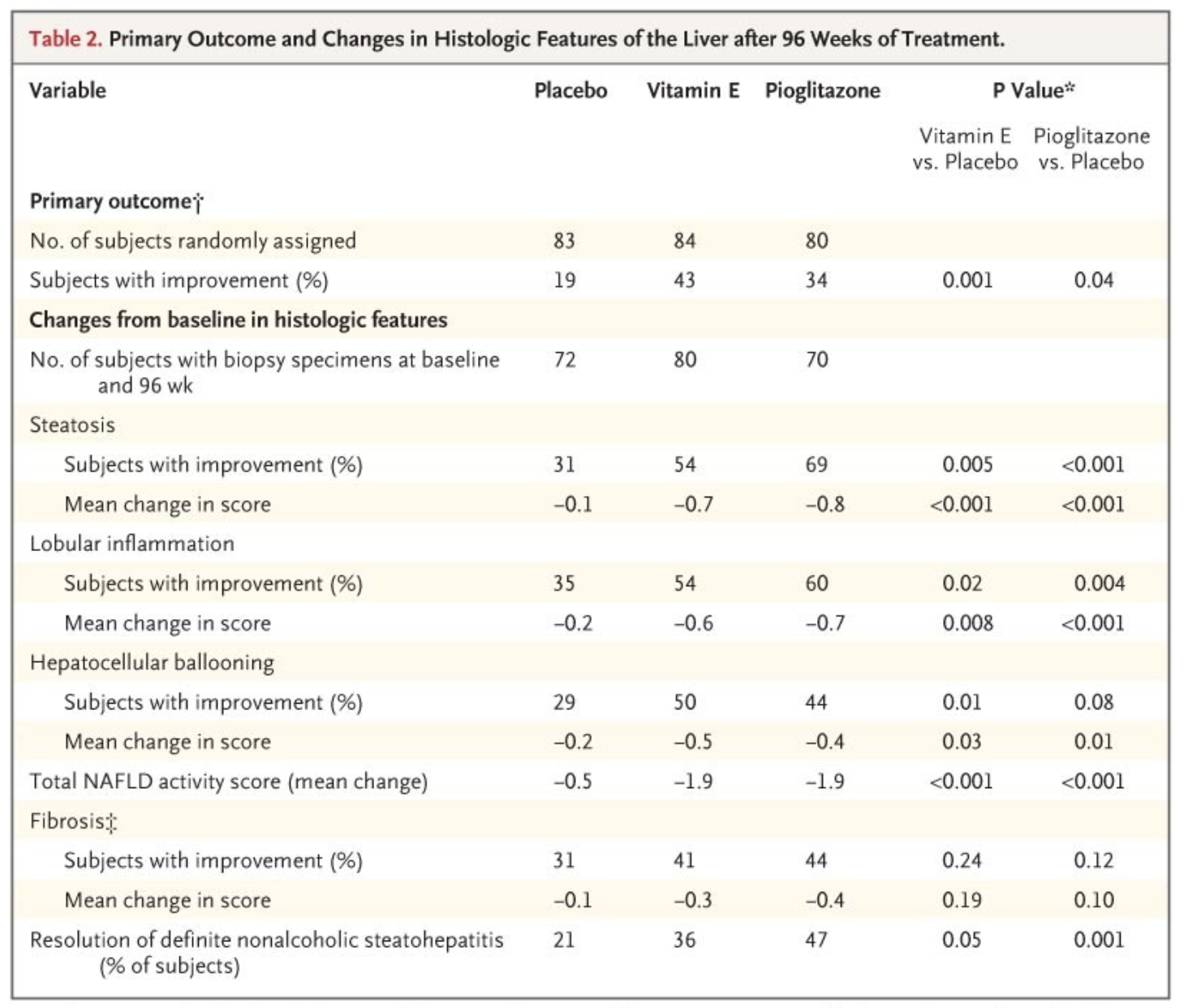
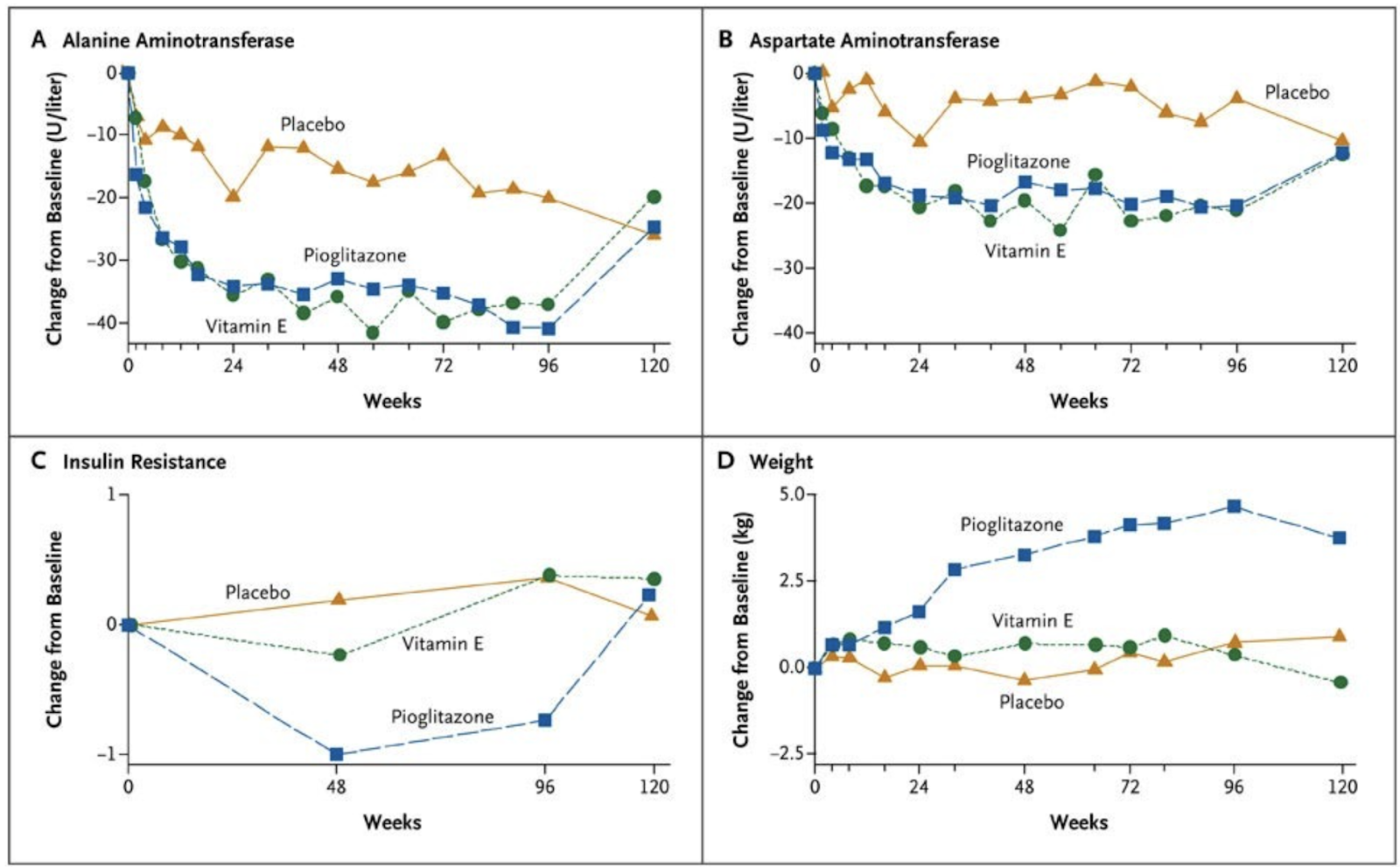
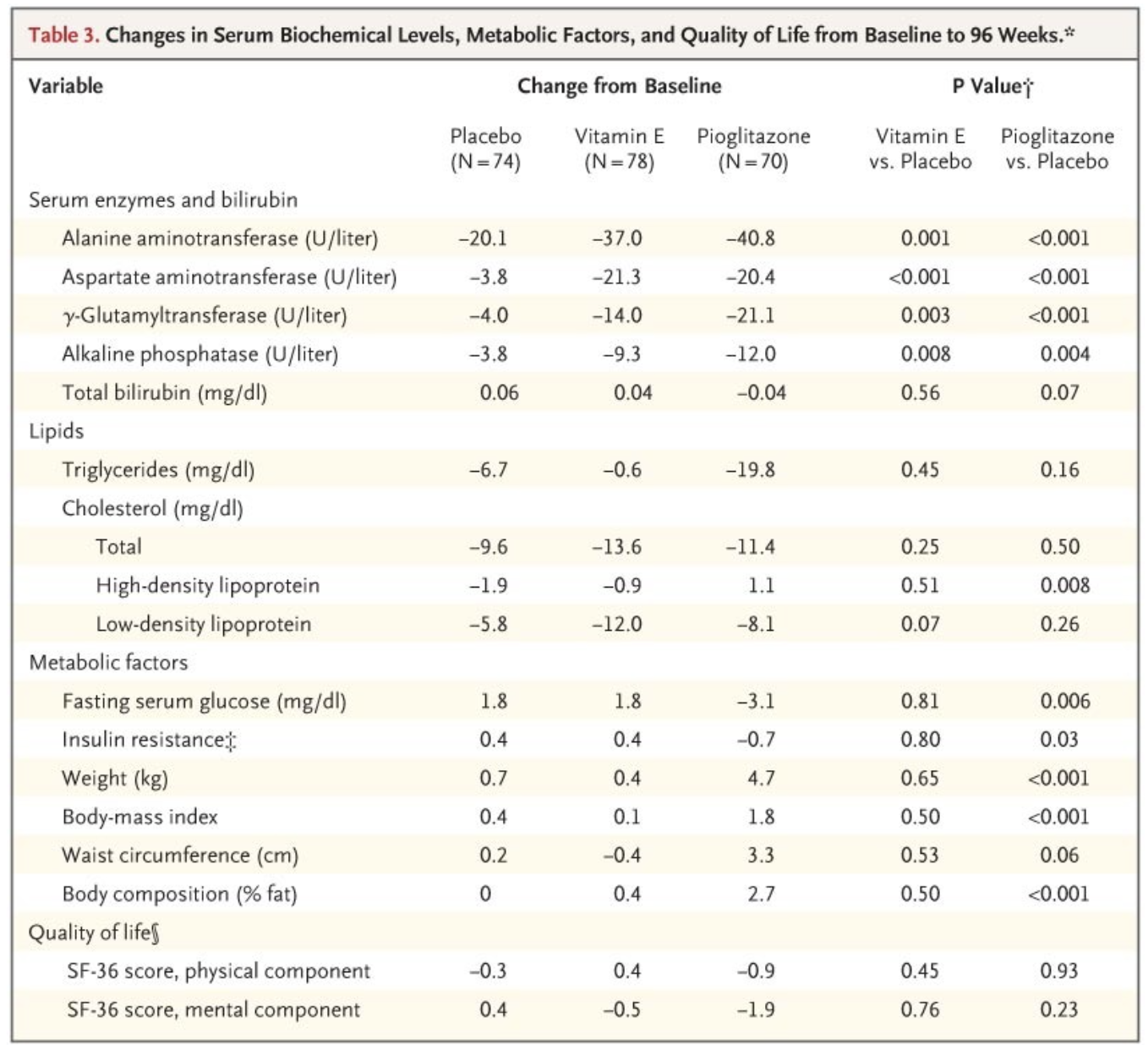
Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis, 2010
247 adults with nonalcoholic steatohepatitis and without diabetes to receive pioglitazone at a dose of 30 mg daily (80 subjects), vitamin E at a dose of 800 IU daily (84 subjects), or placebo (83 subjects), for 96 weeks. The primary outcome was an improvement in histologic features of nonalcoholic steatohepatitis, as assessed with the use of a composite of standardized scores for steatosis, lobular inflammation, hepatocellular ballooning, and fibrosis.
Vitamin E therapy, as compared with placebo, was associated with a significantly higher rate of improvement in nonalcoholic steatohepatitis (43% vs. 19%, P=0.001), but the difference in the rate of improvement with pioglitazone as compared with placebo was not significant (34% and 19%, respectively; P=0.04). Serum alanine and aspartate aminotransferase levels were reduced with vitamin E and with pioglitazone, as compared with placebo (P<0.001 for both comparisons), and both agents were associated with reductions in hepatic steatosis (P=0.005 for vitamin E and P<0.001 for pioglitazone) and lobular inflammation (P=0.02 for vitamin E and P=0.004 for pioglitazone) but not with improvement in fibrosis scores (P=0.24 for vitamin E and P=0.12 for pioglitazone). Subjects who received pioglitazone gained more weight than did those who received vitamin E or placebo; the rates of other side effects were similar among the three groups.

Response to Pioglitazone in Patients With Nonalcoholic Steatohepatitis With vs Without Type 2 Diabetes, 2018
Background & aims: Pioglitazone is effective for long-term treatment of patients with nonalcoholic steatohepatitis (NASH) with prediabetes or type 2 diabetes. However, it is not clear how the presence of type 2 diabetes affects the drug's efficacy. We compared metabolic and histologic responses to pioglitazone in patients with NASH and prediabetes vs type 2 diabetes.
Methods: We performed a prospective study of adults with biopsy-proven NASH (52 with type 2 diabetes and 49 with prediabetes), enrolled from the general population of San Antonio, Texas, from 2008 through 2014. After a run-in period of approximately 4 weeks, when all baseline measurements were made (liver magnetic resonance proton spectroscopy, euglycemic insulin clamp with glucose turnover measurements, dual-energy absorptiometry, and liver biopsy), subjects were randomly assigned to groups given pioglitazone or placebo (45 mg/d) for 18 months; all procedures performed at baseline were then repeated. The primary outcome was a reduction in nonalcoholic fatty liver disease activity score of 2 points or more (for at least 2 components) without worsening of fibrosis (and expressed as difference vs placebo). Secondary outcomes included NASH resolution, individual histologic components, intrahepatic triglyceride content (measured by 1H magnetic resonance spectroscopy), and insulin sensitivity (measured by euglycemic insulin clamp).
Results: The primary outcome was met by 48% of patients with type 2 diabetes vs 46% without diabetes. Resolution of NASH was achieved in 44% of patients with type 2 diabetes vs 26% without diabetes. A significant reduction in fibrosis, from baseline, was observed only in patients with type 2 diabetes (P = .035). Intrahepatic triglyceride content was reduced by 11% ± 2% in patients with diabetes vs a reduction of 9% ± 2% in patients without diabetes (P = .62); the plasma level of alanine aminotransferase was reduced by 50 ± 10 U/L in patients with diabetes vs a reduction of 36 ± 5 U/L in patients without diabetes (P = .22). Pioglitazone was associated with a significantly greater insulin sensitivity in adipose tissue of patients with diabetes vs without diabetes (P < .001), but nonsignificant differences in responses in hepatic (P = .49) and skeletal muscle (P = .32) insulin sensitivity.
Conclusions: In a prospective study, we found pioglitazone to be effective in patients with and without type 2 diabetes. However, pioglitazone reduced liver fibrosis and increased adipose tissue insulin sensitivity at significantly greater levels in patients with type 2 diabetes than in patients with prediabetes.
The Effect of Pioglitazone and Metformin on Liver Function Tests, Insulin Resistance, and Liver Fat Content in Nonalcoholic Fatty Liver Disease: A Randomized Double Blinded Clinical Trial, 2013
The aim of study was to compare the effects of two different insulin sensitizers, pioglitazone, and metformin, on liver function tests (LFT), lipid profile, homeostasis model assessment-IR (HOMA-IR) index, and liver fat content (LFC) in NAFLD patients.
Materials and Methods
This double blind clinical trial was performed on patients who were referred to a gastroenterology clinic with evidence of fatty liver in ultrasonography. After excluding other causes, participants with persistent elevated alanine aminotransferase (ALT) levels and “NAFLD liver fat score” greater than -0.64 were presumed to have NAFLD and were enrolled. They were randomly assigned to take metformin (1 g/day) or pioglitazone (30 mg/day) for four months. Fasting serum glucose (FSG), ALT, aspartate aminotransferase (AST), alkaline phosphatase (ALP), triglyceride, cholesterol (CHOL), high and low density lipoprotein (HDL, LDL), HOMA-IR, and LFC were checked at the baseline, two and four months post-treatment. LFC was measured by a validated formula.
Results
Eighty patients (68 males) with mean age of 35.27 (± 7.98) were included. After 2 months, LFT was improved significantly in the pioglitazone group and did not change in the metformin group. After four months, both medications significantly decreased serum levels of LFT, FSG, CHOL, LDL, HOMA-IR, and LFC, and increased serum level of HDL. No statistically significant differences were seen between the two treatment groups with regard to the changes of laboratory parameters and LFC from baseline to four months post-treatment.
Conclusions
During the four months, the use of metformin (1 g/day) and pioglitazone (30 mg/day) were safe and might have equally affected LFT, HOMA-IR, lipid profile, and LFC in NAFLD patients.
Pioglitazone for NAFLD Patients With Prediabetes or Type 2 Diabetes Mellitus: A Meta-Analysis, 2021
Objective
To systematically evaluate the effects of pioglitazone in the treatment of patients with prediabetes or T2DM combined with NAFLD.
Results
A total of 4 studies were included. Compared with placebo, pioglitazone significantly improved steatosis grade, inflammation grade and ballooning grade, while in the fibrosis stage, there was no significant improvement in pioglitazone compared with placebo. In addition, pioglitazone can also improve blood glucose and liver function.
Conclusion
Pioglitazone can significantly improve the histological performance of the liver and insulin sensitivity. Additionally, it can significantly reduce fasting blood glucose, glycosylated hemoglobin, plasma AST, ALT and other liver biological indicators. Due to the lack of relevant randomized controlled trials and short intervention times, long-term studies are still needed to verify its efficacy and safety.
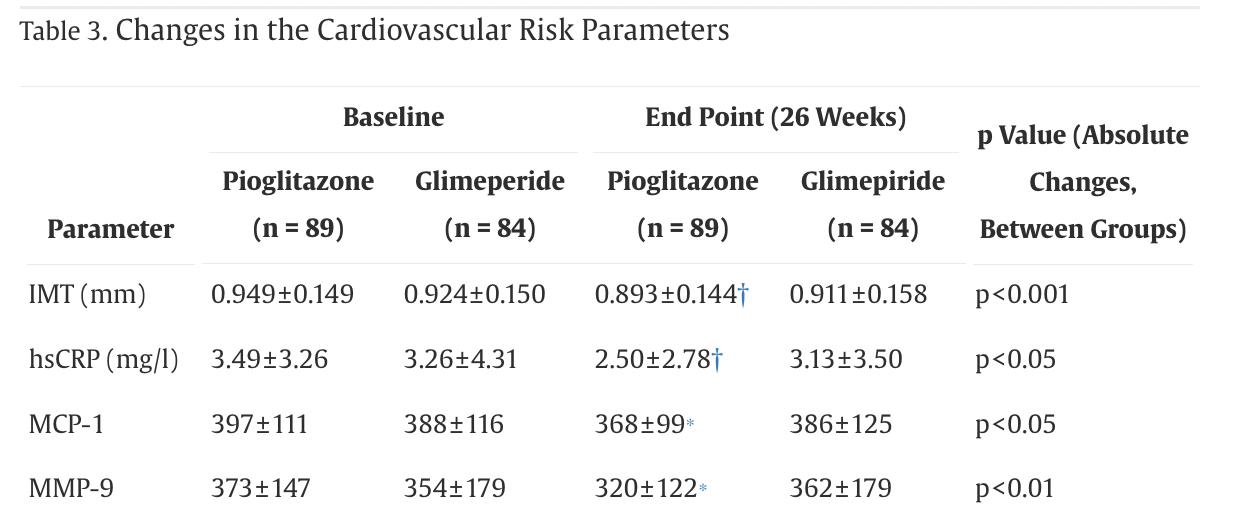
Improvement of Cardiovascular Risk Markers by Pioglitazone Is Independent From Glycemic Control: Results From the Pioneer Study, 2005

High-Sensitivity C-Reactive Protein Predicts Cardiovascular Risk in Diabetic and Nondiabetic Patients: Effects of Insulin-Sensitizing Treatment with Pioglitazone, 2010

Pioglitazone and risk of mortality in patients with type 2 diabetes: results from a European multidatabase cohort study, 2017
56 337 patients with type 2 diabetes mellitus first prescribed pioglitazone between 2000 and 2011, and 56 337 patients never prescribed pioglitazone matched by treatment stage, history of diabetes, diabetes complications and cardiovascular disease, and year of cohort entry using exact and propensity score matching. Patients were followed-up for a mean of 2.90 (SD 2.21) and 2.83 (SD 2.37) years in the pioglitazone-exposed and non-pioglitazone-exposed groups, respectively.
The crude overall mortality rate per 10 000 patient years was 206 (95% CI 199 to 213) in the pioglitazone-exposed group and 448 (95% CI 438 to 458) in the non-pioglitazone-exposed group. The crude HR comparing pioglitazone to alternative antidiabetic exposure was 0.46 (95% CI 0.45 to 0.48). This reduced in magnitude to 0.67 (95% CI 0.64 to 0.70) following further adjustment for matching variables, propensity scores, age, gender and time-dependent variables representing use of alternative antidiabetic drugs.
In this large observational cohort study of patients with type 2 diabetes, pioglitazone exposure was associated with a statistically significant decrease in the risk of all-cause mortality across four European countries. Results should be interpreted with caution due to the potential for residual confounding.
Pioglitazone and cause-specific risk of mortality in patients with type 2 diabetes: extended analysis from a European multidatabase cohort study, 2018
Abstract
Objectives Describe and compare the risk of cardiovascular and non-cardiovascular mortality in patients whose antidiabetic therapy is modified to include pioglitazone compared with an alternative antidiabetic medication at the same stage of disease progression.
Research design and methods This exploratory linked database cohort analysis used pooled health and mortality data from three European countries: Finland, Sweden and the UK. Propensity score together with exact matching was used to match 31 133 patients with type 2 diabetes first prescribed pioglitazone from 2000 to 2011, to 31 133 patients never prescribed pioglitazone. Exact matching variables were treatment stage, history of diabetes, diabetes complications and cardiovascular disease, and year of cohort entry. Mean follow-up time was 2.60 (SD 2.00) and 2.69 (SD 2.31) years in the pioglitazone and non-pioglitazone-exposed groups, respectively. Crude cause-specific mortality rates were ascertained. Association with pioglitazone use was estimated using Cox proportional hazards models adjusted a priori for country, age, sex, the propensity score quintile and time-dependent variables representing use of antidiabetic drugs. Stepwise testing identified no additional confounders to include in adjusted models.
Results The crude mortality rate was lower in the pioglitazone-exposed group than the non-exposed group for both cardiovascular and non-cardiovascular mortality. Adjusted HRs comparing pioglitazone to alternative antidiabetic exposure were 0.58 (95% CI 0.52 to 0.63) and 0.63 (95% CI 0.58 to 0.68) for cardiovascular and non-cardiovascular mortality, respectively. A protective effect associated with pioglitazone was also found for all specific cardiovascular causes.
Conclusions This analysis suggests that pioglitazone is associated with a decrease in both cardiovascular and non-cardiovascular mortality. Results should be interpreted with caution due to the potential for residual confounding in this exploratory analysis. Further studies, specifically designed to test the association between pioglitazone use and patient-focused outcomes, are suggested.
Pioglitazone Exposure Reduced the Risk of All-Cause Mortality in Insulin-Treated Patients with Type 2 Diabetes Mellitus, 2020
Design, setting and patients: We conducted a 13-year retrospective cohort study by using data from the population-based National Health Insurance Research Database in Taiwan. A total of 20 376 patients with type 2 diabetes mellitus (T2DM) receiving insulin therapy were enrolled during 2000 to 2012. Overall, the incidence rates of all-cause mortality and CV events were compared between 2579 pioglitazone users and 2579 matched nonusers.
Results: After adjustment for age, sex, comorbidities, Diabetes Complications Severity Index scores, and drugs used, mortality rates were 30.26 and 15.02 per 1000 person-years for pioglitazone nonusers and users, respectively. The adjusted hazard ratio (aHR) of mortality was 0.47 (95% confidence interval [CI]: 0.38-0.58, P < 0.001) for pioglitazone users compared with nonusers. The aHRs of CV and non-CV deaths were 0.78 (95% CI: 0.51-1.19) and 0.50 (95% CI: 0.38-0.66), respectively. The aHRs of hospitalized coronary artery disease, hospitalized stroke, and incident heart failure were not significantly different between pioglitazone users and nonusers.
Conclusions: This nationwide cohort study demonstrated that pioglitazone use reduced the risks of all-cause mortality and non-CV death for patients with T2DM undergoing insulin therapy.
Effects of pioglitazone on cardiovascular events and all-cause mortality in patients with type 2 diabetes: A meta-analysis of randomized controlled trials, 2022
A MEDLINE database search was performed to identify RCTs, up to June 1st, 2021, with duration≥52 weeks, in which pioglitazone was compared with either placebo or active comparators. The principal endpoints were MACE and HHF (restricted for RCT reporting MACEs within their outcomes), all-cause mortality (irrespective of the inclusion of MACEs among the pre-specified outcomes). Mantel-Haenszel odds ratio (MH–OR) with 95% Confidence Interval (95% CI) was calculated for all the endpoints considered.
Eight RCTs were included in the analysis for MACEs and HF (5048 and 5117 patients in the pioglitazone and control group, respectively), and 24 in that for all-cause mortality (10,682 and 9674 patients). Pioglitazone neither significantly increased nor reduced the risk of MACE, all-cause mortality, and HHF in comparison with placebo/active comparators (MH–OR: 0.90, 95% CI 0.78–1.03, 0.91, 95% CI 0.77, 1.09, and 1.16, 95% CI 0.73, 1.83, respectively). Pioglitazone was associated with a significant reduction of MACE in patients with prior cardiovascular events (MH–OR 0.84, 95% CI 0.72–0.99).
Conclusions
This meta-analysis showed no significant effects of pioglitazone on incident MACE, all-cause mortality, and HHF.
Pioglitazone is an oral anti-hyperglycemic drug in the thiazolidinedione class that improves insulin sensitivity and may lower HbA1c by 1%.
PPARγ agonists delay age‐associated metabolic disease and extend longevity, 2020
Aging leads to a number of disorders caused by cellular senescence, tissue damage, and organ dysfunction. It has been reported that anti-inflammatory and insulin-sensitizing compounds delay, or reverse, the aging process and prevent metabolic disorders, neurodegenerative disease, and muscle atrophy, improving healthspan and extending lifespan. Here we investigated the effects of PPARγ agonists in preventing aging and increasing longevity, given their known properties in lowering inflammation and decreasing glycemia. Our molecular and physiological studies show that long-term treatment of mice at 14 months of age with low doses of the PPARγ ligand rosiglitazone (Rosi) improved glucose metabolism and mitochondrial functionality. These effects were associated with decreased inflammation and reduced tissue atrophy, improved cognitive function, and diminished anxiety- and depression-like conditions, without any adverse effects on cardiac and skeletal functionality. Furthermore, Rosi treatment of mice started when they were 14 months old was associated with lifespan extension. A retrospective analysis of the effects of the PPARγ agonist pioglitazone (Pio) on longevity showed decreased mortality in patients receiving Pio compared to those receiving a PPARγ-independent insulin secretagogue glimepiride. Taken together, these data suggest the possibility of using PPARγ agonists to promote healthy aging and extend lifespan.
Pioglitazone Hydrochloride Extends the Lifespan of Caenorhabditis elegans by Activating DAF-16/FOXO- and SKN-1/NRF2-Related Signaling Pathways (2022)
Pioglitazone hydrochloride (PGZ), a nuclear receptor peroxisome proliferator-activated receptor gamma (PPAR-γ) agonist, is a universally adopted oral agent for the treatment of type 2 diabetes (T2D). Previous studies reported that PGZ could ameliorate the symptoms of aging-related diseases and Alzheimer’s disease. However, whether PGZ participates in aging regulation and the underlying mechanism remain undetermined. Here, we found that PGZ significantly prolonged the lifespan and healthspan of Caenorhabditis elegans (C. elegans). We found that a variety of age-related pathways and age-related genes are required for PGZ-induced lifespan extension. The transcription factors DAF-16/FOXO, HSF-1, and SKN-1/NRF2, as well as the nuclear receptors DAF-12 and NHR-49, all functioned in the survival advantage conferred by PGZ. Moreover, our results demonstrated that PGZ induced lifespan extension through the inhibition of insulin/insulin-like signaling (IIS) and reproductive signaling pathways, as well as the activation of dietary restriction- (DR-) related pathways. Additionally, our results also indicated that beneficial longevity mediated by PGZ is linked to its antioxidative activity. Our research may provide a basis for further research on PGZ, as an anti-T2D drug, to interfere with aging and reduce the incidence of age-related diseases in diabetic patients.
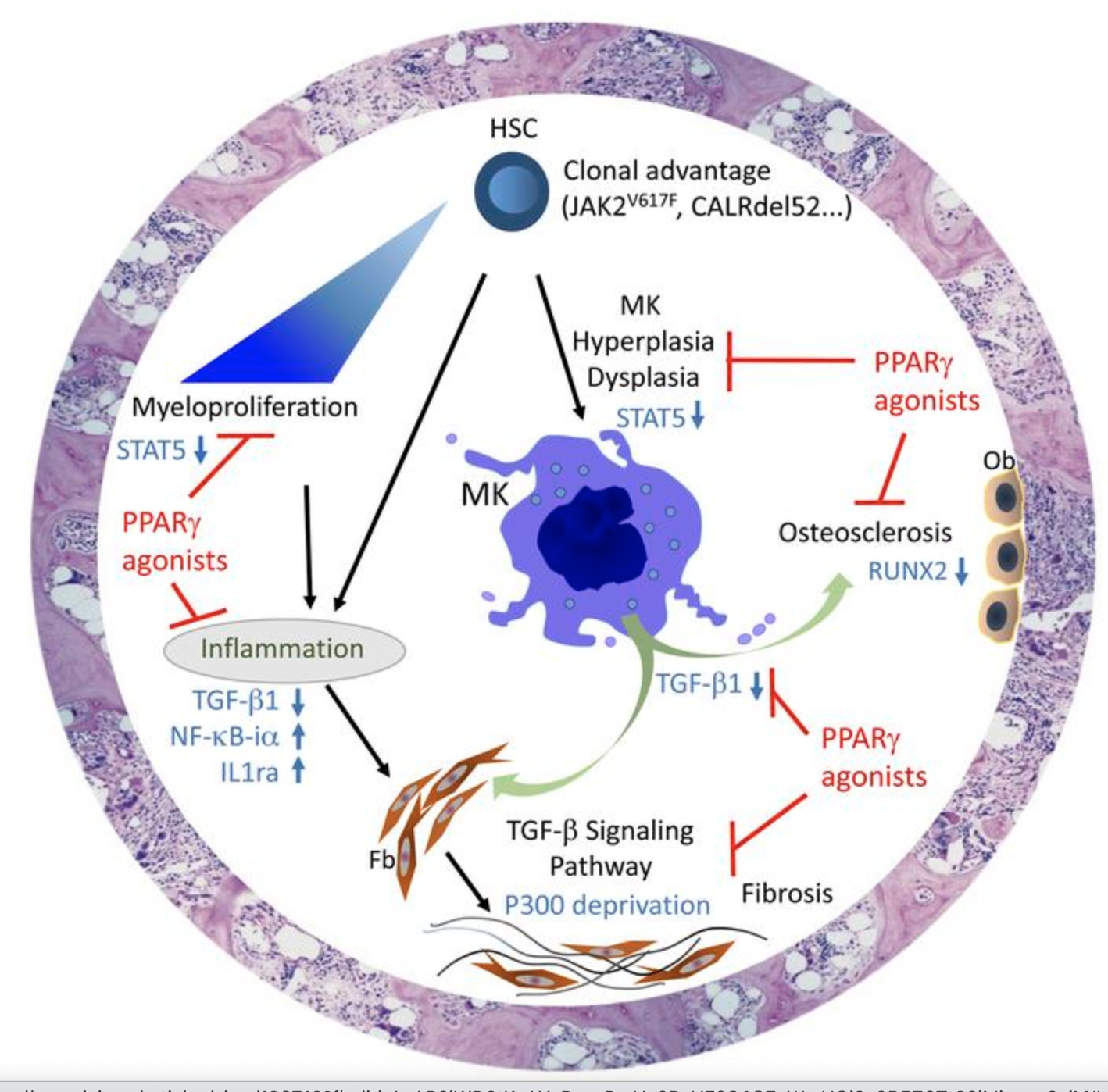
PPARγ agonists promote the resolution of myelofibrosis in preclinical models, 2021
Myelofibrosis (MF) is a non–BCR-ABL myeloproliferative neoplasm associated with poor outcomes. Current treatment has little effect on the natural history of the disease. MF results from complex interactions between (a) the malignant clone, (b) an inflammatory context, and (c) remodeling of the bone marrow (BM) microenvironment. Each of these points is a potential target of PPARγ activation. Here, we demonstrated the therapeutic potential of PPARγ agonists in resolving MF in 3 mouse models. We showed that PPARγ agonists reduce myeloproliferation, modulate inflammation, and protect the BM stroma in vitro and ex vivo. Activation of PPARγ constitutes a relevant therapeutic target in MF, and our data support the possibility of using PPARγ agonists in clinical practice.
Pioglitazone together with imatinib in chronic myeloid leukemia (CML): A proof of concept study, 2017
We recently reported that peroxisome proliferator‐activated receptor γ agonists target chronic myeloid leukemia (CML) quiescent stem cells in vitro by decreasing transcription of STAT5. Here in the ACTIM phase 2 clinical trial, we asked whether pioglitazone add‐on therapy to imatinib would impact CML residual disease, as assessed by BCR‐ABL1 transcript quantification.
CML patients were eligible if treated with imatinib for at least 2 years at a stable daily dose, having yielded major molecular response (MMR) but not having achieved molecular response 4.5 (MR4.5) defined by BCR‐ABL1/ABL1 IS RNA levels ≤ 0.0032%. After inclusion, patients started pioglitazone at a dosage of 30 to 45 mg/day in addition to imatinib. The primary objective was to evaluate the cumulative incidence of patients having progressed from MMR to MR4.5 over 12 months.
RESULTS
Twenty‐four patients were included (age range, 24‐79 years). No pharmacological interaction was observed between the drugs. The main adverse events were weight gain in 12 patients and a mean decrease of 0.4 g/dL in hemoglobin concentration. The cumulative incidence of MR4.5 was 56% (95% confidence interval, 37%‐76%) by 12 months, despite a wide range of therapy duration (1.9‐15.5 months), and 88% of 17 evaluable patients who were still on imatinib reached MR4.5 by 48 months. The cumulative incidence of MMR to MR4.5 spontaneous conversions over 12 months was estimated to be 23% with imatinib alone in a parallel cohort of patients.
CONCLUSION
Pioglitazone in combination with imatinib was well tolerated and yielded a favorable 56% rate (vs 23% in baseline). These results provide a proof of concept needing confirmation within a randomized clinical trial
Adding Oral Pioglitazone to Standard Induction Chemotherapy of Acute Myeloid Leukemia: A Randomized Clinical Trial, 2019
The hypothesis of an effect by thiazolidinedione on leukemia cells was proposed 2 decades ago, but there is little clinical evidence regarding its efficacy. We evaluated the safety and efficacy of adding pioglitazone to standard induction chemotherapy in patients with acute myeloid leukemia (AML).
In this randomized clinical trial, newly diagnosed AML patients were randomized to 1 of 2 groups. Patients in both groups received cytarabine (100 mg/m2 per day for 7 days) and daunorubicin (60 mg/m2 per day for 3 days). Patients in the pioglitazone group additionally received oral pioglitazone (45 mg per day). The 2 groups were compared according to remission rate, laboratory findings, and adverse events during treatment.
Forty patients were evaluated, 20 patients in each group. The complete remission rate was 20% more in the pioglitazone group compared to the control group (P = .202). Complications due to pioglitazone discontinuation were observed in 2 cases. The mean serum alanine aminotransferase in the fourth treatment week was significantly more in pioglitazone group compared to the control group (65.5 vs. 33.6 mg/dL, P = .039). The mean serum creatinine in all treatment phases was significantly higher in the pioglitazone group compared to the control group (P < .05). There were no significant differences between the 2 groups regarding other laboratory findings (P > .05).
Adding pioglitazone to cytarabine and daunorubicin increased the remission rate in AML patients compared to control subjects. Although this difference in remission rate between the 2 groups was not statistically significant, it could be important in the clinical setting. Pioglitazone may provide benefits as an adjuvant therapy for AML patients without causing serious adverse events.
Low dose Pioglitazone 7.5mg tested below with favorable results:
(Less weight gain, same efficacy)
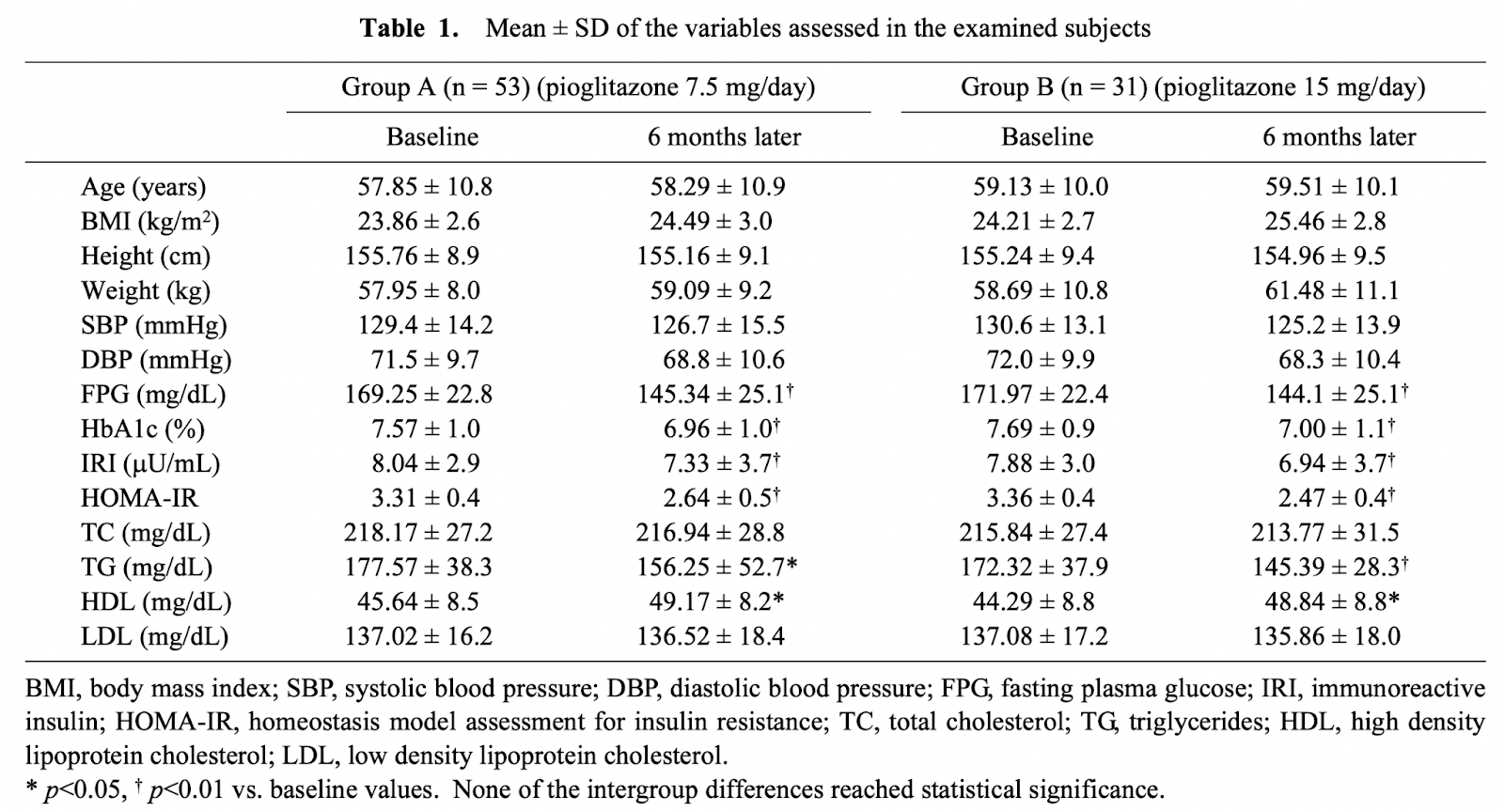
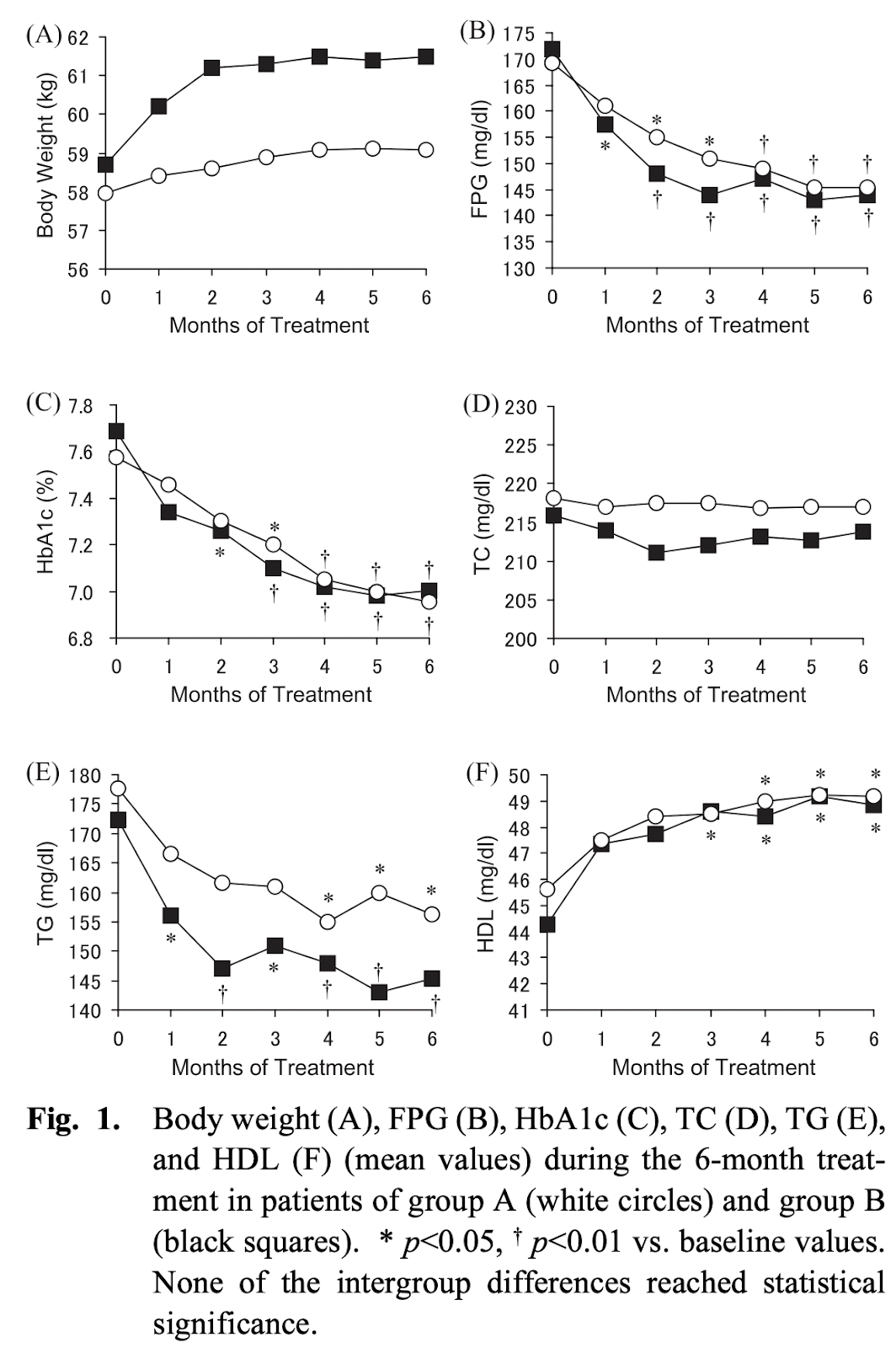
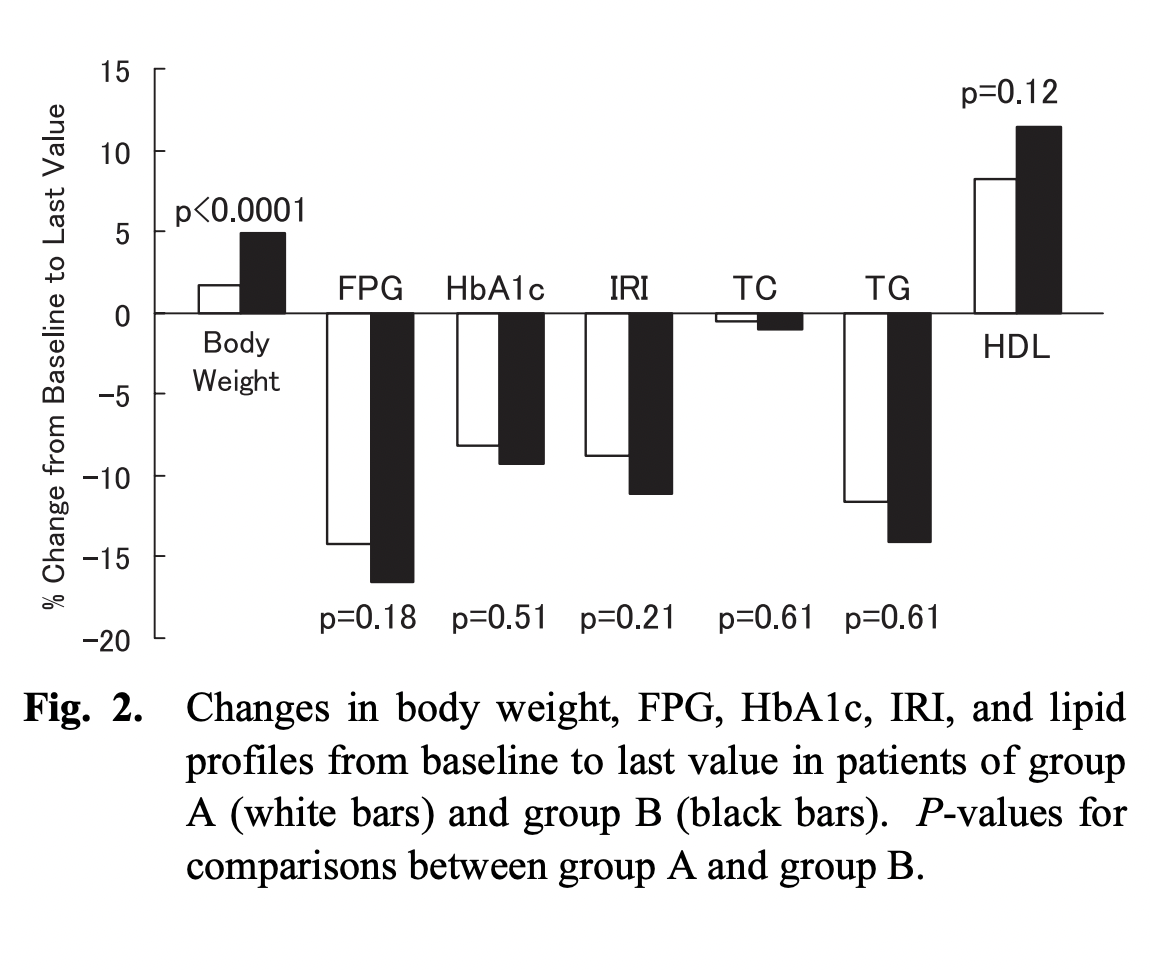
Safety and Efficacy of Low-dose Pioglitazone (7.5 mg/day) vs. Standard-dose Pioglitazone (15 mg/day) in Japanese Women with Type 2 Diabetes Mellitus, 2006
It is well known that pioglitazone, a potent thiazolidinedione, improves metabolic control. However, weight gain or peripheral edema may be of major clinical concern when using this agent. The purpose of our study was to prospectively evaluate the effects of low-dose pioglitazone (7.5 mg/day) on metabolic control, weight gain and the incidence of edema compared with a standard dose of pioglitazone (15.0 mg/day) in patients with type 2 diabetes mellitus (T2DM). Ninety-five Japanese female patients (mean age 58.4 ± 10.4 years) with newly diagnosed T2DM were selected for this study. They were randomly divided into the following 2 groups according to therapy regimens, and examined every month for 6 months after diagnosis. Group A consisted of 54 patients treated with low-dose pioglitazone orally; Group B, the control-group, consisted of 41 patients treated with standard-dose pioglitazone orally. The incidence of peripheral edema was significantly much lower in group A (2/54) than in group B (11/41) (p = 0.0014). In addition, % change of body weight during the 6-month treatment in group A was significantly less than that in group B (p<0.0001). On the other hand, the % change of biochemical parameters including HbA1c did not differ significantly between group A and group B, although glucose and lipid control significantly improved from baseline in both groups. Our results demonstrate the safety and efficacy of low-dose pioglitazone, suggesting that it could be another good choice of treatment for Japanese women with T2DM.
Safety and efficacy of low dose pioglitazone compared with standard dose pioglitazone in type 2 diabetes with chronic kidney disease: A randomized controlled trial, 2018
Methods
A total of 75 patients with type 2 diabetes and CKD and inadequate glycemic control receiving any pharmacological antidiabetic treatment were randomly assigned to 2 groups. One group consisted of 37 patients treated with standard dose pioglitazone (15 mg/day) and another group consisted of 38 patients treated with low dose pioglitazone (7.5 mg/day). Glycosylated hemoglobinA1c (HbA1c) and metabolic profiles were monitored every 8 weeks for 24 weeks. Body composition was assessed using bio-electrical impedance analysis (BIA).
Results
After 6 months of therapy, HbA1c levels decreased in both standard and low dose pioglitazone groups. The mean changes in HbA1c for standard and low dose pioglitazone were 1.1±1.6 and -1.4±1.5 (P = 0.543), respectively. Compared with low dose pioglitazone, standard dose pioglitazone treatment led to a greater increase in body weight, fat mass, total body water and extracellular water composition. No major adverse effects including hypoglycemia, congestive heart failure and abnormal liver function were identified.
Conclusion
Pioglitazone 7.5 mg once daily treatments presented similar glycemic control to standard dose pioglitazone and exhibited beneficial effects on weight gain and fluid retention among patients with type 2 diabetes and CKD.
Efficacy of lower doses of pioglitazone after stroke or transient ischaemic attack in patients with insulin resistance, 2022
Materials and methods: Efficacy [myocardial infarction (MI) or recurrent stroke] new-onset diabetes) and adverse outcomes (oedema, weight gain, heart failure and bone fracture) were examined for subjects assigned to pioglitazone or placebo within strata defined by mode dose of study drug taken (i.e. the dose taken on most days in the study).
Results: Among the 1938 patients randomized to pioglitazone, the mode dose was <15 mg/day in 546 participants, 15 mg/day in 128, 30 mg/day in 89, and 45 mg/day in 1175. There was no significant effect on stroke/MI or new-onset diabetes with <15 mg/day. For 15 mg/30 mg/day pooled, the adjusted hazard ratios (95% CI) for stroke/MI were 0.48 (0.30, 0.76; p = .002) and 0.74 (0.69, 0.94) for 45 mg/day. For new-onset diabetes, the adjusted hazard ratios were 0.34 (0.15, 0.81; p = .001) and 0.31 (0.59, 0.94; p = .001) respectively. For oedema, weight gain and heart failure, the risk estimates for pioglitazone were lower for subjects taking <45 mg daily. For fractures, the increased risk with pioglitazone was similar across all dose strata.
Conclusions: Lower doses of pioglitazone appear to confer much of the benefit with less adverse effects than the full dose. Further study is needed to confirm these findings so that clinicians may optimize dosing of this secondary prevention strategy in patients with stroke.
Pioglitazone after Ischemic Stroke or Transient Ischemic Attack, 2016
METHODS
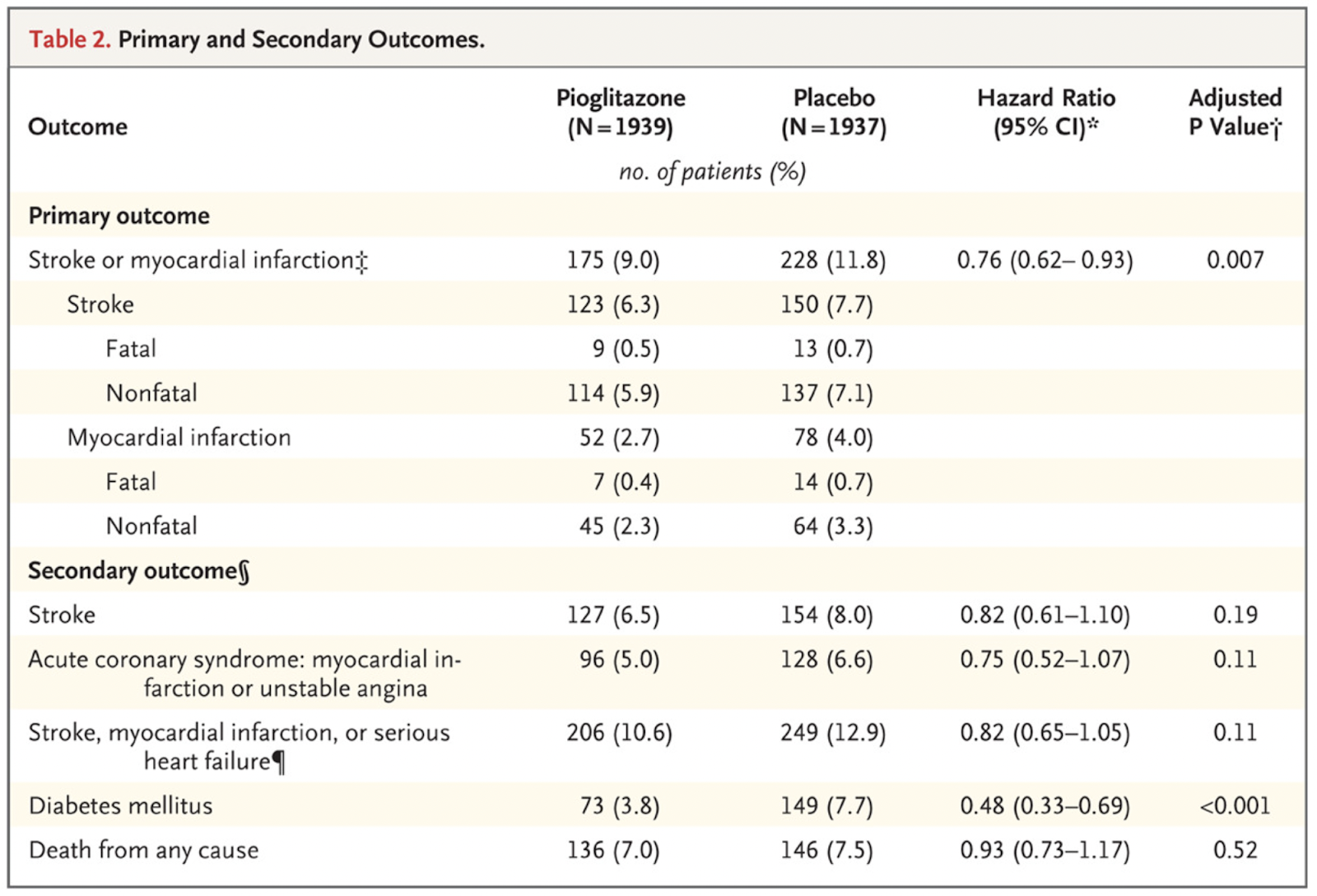
In this multicenter, double-blind trial, we randomly assigned 3876 patients who had had a recent ischemic stroke or TIA to receive either pioglitazone (target dose, 45 mg daily) or placebo. Eligible patients did not have diabetes but were found to have insulin resistance on the basis of a score of more than 3.0 on the homeostasis model assessment of insulin resistance (HOMA-IR) index. The primary outcome was fatal or nonfatal stroke or myocardial infarction.
RESULTS
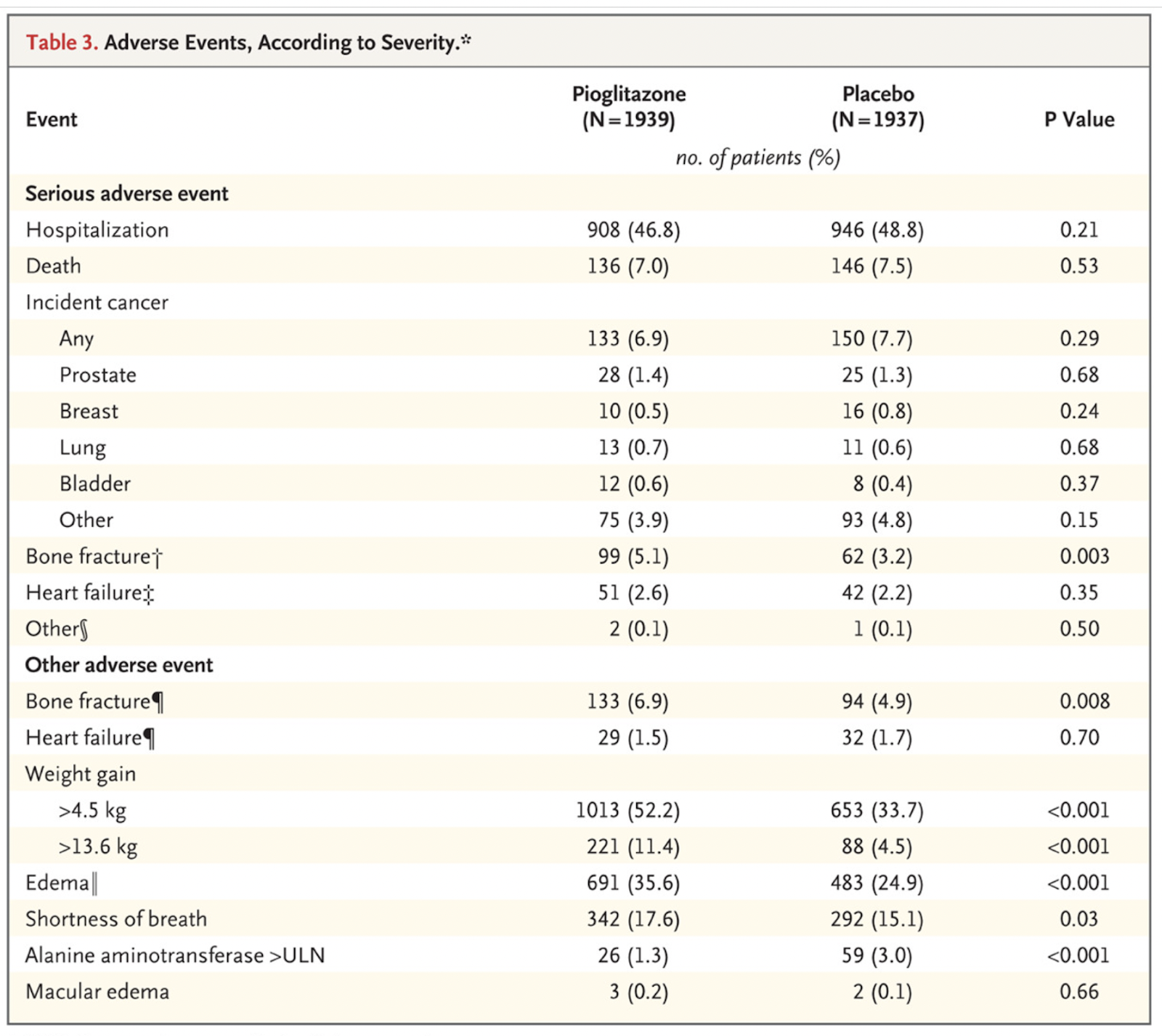
By 4.8 years, a primary outcome had occurred in 175 of 1939 patients (9.0%) in the pioglitazone group and in 228 of 1937 (11.8%) in the placebo group (hazard ratio in the pioglitazone group, 0.76; 95% confidence interval [CI], 0.62 to 0.93; P=0.007). Diabetes developed in 73 patients (3.8%) and 149 patients (7.7%), respectively (hazard ratio, 0.48; 95% CI, 0.33 to 0.69; P<0.001). There was no significant between-group difference in all-cause mortality (hazard ratio, 0.93; 95% CI, 0.73 to 1.17; P=0.52). Pioglitazone was associated with a greater frequency of weight gain exceeding 4.5 kg than was placebo (52.2% vs. 33.7%, P<0.001), edema (35.6% vs. 24.9%, P<0.001), and bone fracture requiring surgery or hospitalization (5.1% vs. 3.2%, P=0.003).
CONCLUSIONS
In this trial involving patients without diabetes who had insulin resistance along with a recent history of ischemic stroke or TIA, the risk of stroke or myocardial infarction was lower among patients who received pioglitazone than among those who received placebo. Pioglitazone was also associated with a lower risk of diabetes but with higher risks of weight gain, edema, and fracture.
Pioglitazone - Wikipedia
Pioglitazone inhibits platelet function and potentiates the effects of aspirin: a prospective observation study, 2012
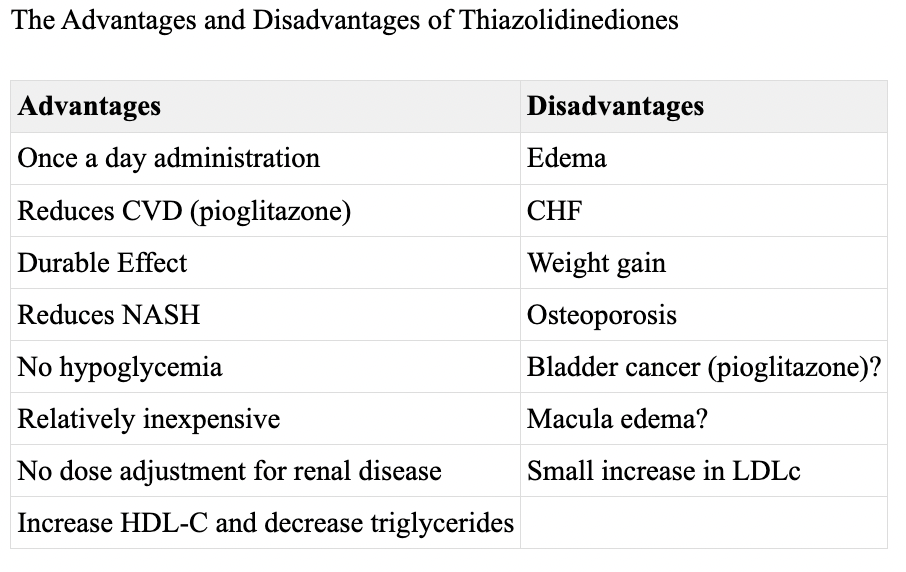
Excellent summary article: Are thiazolidinediones a preferred drug treatment for type 2 diabetes? 2021
Table 12. [The Advantages and Disadvantages of Thiazolidinediones]. - Endotext - NCBI Bookshelf
Pioglitazone and cardiovascular outcomes in patients with insulin resistance, pre-diabetes and type 2 diabetes: a systematic review and meta-analysis, 2017
Pioglitazone Improves Insulin Sensitivity Among Nondiabetic Patients With a Recent Transient Ischemic Attack or Ischemic Stroke, 2003
Effect of Pioglitazone on Abdominal Fat Distribution and Insulin Sensitivity in Type 2 Diabetic Patients, 2002
Pioglitazone increases circulating adiponectin levels and subsequently reduces TNF-alpha levels in Type 2 diabetic patients: a randomized study, 2006
The hsCRP Lowering Effect of Pioglitazone Correlates with the Baseline hsCRP Level and the Changes in Abdominal Adiposity, 2009
Anti-inflammatory effects of pioglitazone and/or simvastatin in high cardiovascular risk patients with elevated high sensitivity C-reactive protein: the PIOSTAT Study, 2007
Effect of pioglitazone therapy on high sensitive C-reactive protein and lipid profile in diabetic patients with renal transplantation; a randomize clinical trial, 2015
Effects of pioglitazone on erectile dysfunction in sildenafil poor-responders: a randomized, controlled study, 2008
Effect of pioglitazone on testosterone in eugonadal men with type 2 diabetes mellitus: a randomized double-blind placebo-controlled study, 2013
Objectives: Pioglitazone is an insulin sensitizer used for the management of type 2 diabetes mellitus (T2DM). It has been shown to reduce testosterone level in patients with polycystic ovarian syndrome. However, its effect on testosterone in men has not been studied.
Research design and methods: A randomized, double-blind, placebo-controlled trial with 6 months follow-up. Fifty (25 in each group) eugonadal men (well virilized and total testosterone ≥ 12 nm) with T2DM, aged 30-55 year and HbA1c of ≤ 7.5% were randomly assigned to receive pioglitazone 30 mg per day or placebo along with existing glimepiride and metformin therapy.
Results: As compared to placebo, 6 months of pioglitazone therapy in patients with T2DM resulted in significant reduction in mean total testosterone level (16.1 to 14.9 vs 17.1 to 17.0 nm; P = 0.031), calculated free testosterone (P = 0.001) and bioavailable testosterone (P = 0.000) despite significant increase in sex hormone-binding globulin (P = 0.000). Plasma androstenedione (∆(4) ) level increased (1.5 to 1.9 vs 1.7 to 1.7 ng/ml; P = 0.051) following pioglitazone therapy. The decrease in testosterone was independent of change in body weight, body fat and HbA1c.
Conclusion: Pioglitazone therapy significantly decreases total, free and bioavailable testosterone in eugonadal men with T2DM. The effects of these alterations need to be determined by further long-term studies.


Comments