Vitamin K2
CANCER:
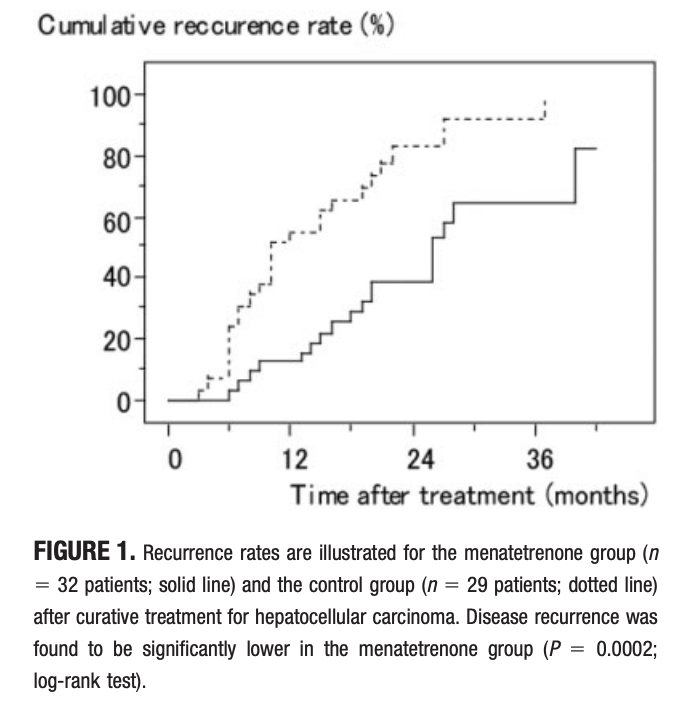
A 2006 pilot study found that menatetrenone, a vitamin K2 analog, significantly reduced recurrence rates of hepatocellular carcinoma (HCC) at 12, 24, and 36 months and suggested potential benefits on survival, compared to a control group (P = 0.0002).
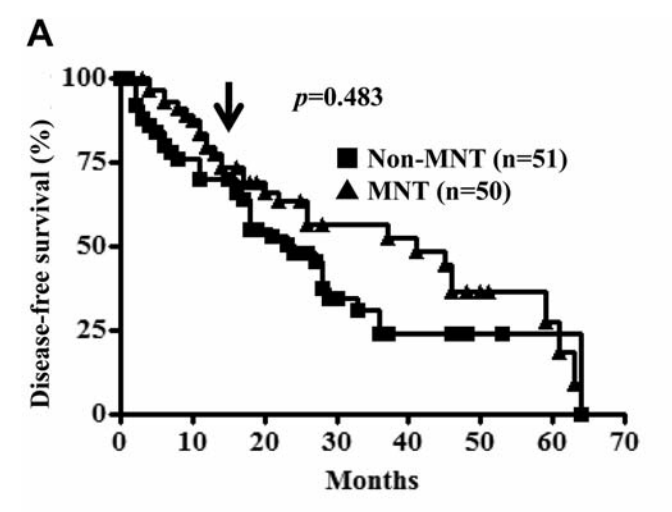
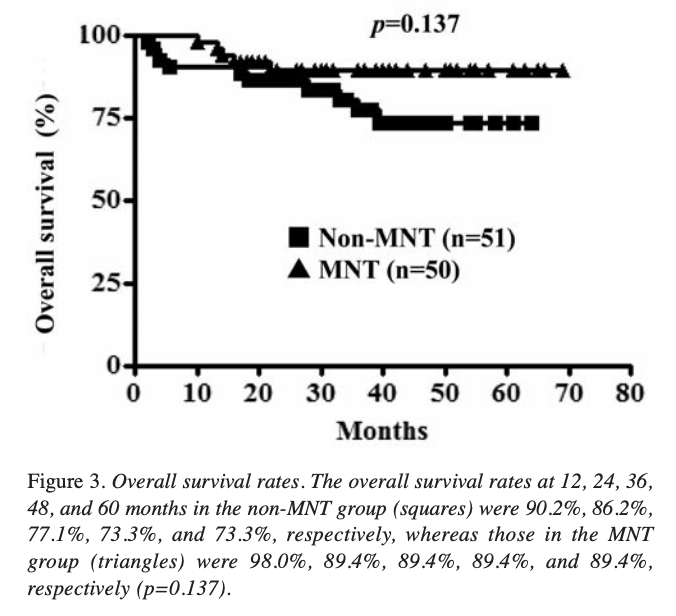
A 2012 prospective randomized controlled trial showed that menatetrenone moderately suppressed HCC recurrence after hepatectomy, particularly in patients with normal preoperative Des-γ-carboxy-prothrombin levels (p=0.060).
Vitamin K2 (3-10 μM) treatment in vitro induced apoptosis in leukemic blast cells from 15 MDS patients, with a more significant effect on blastic cells than mature myeloid cells or CD3-positive lymphoid cells, suggesting potential for MDS treatment in blastic transformation (1998)
Administration of menatetrenone (45 mg daily) improved pancytopenia and transfusion-dependence in an 80-year-old MDS patient, suggesting potential for restoring hematopoiesis in MDS patients by inducing differentiation (1999).
Vitamin K2 treatment effectively induced apoptosis in leukemic cells and promoted differentiation of healthy white blood cells in myelodysplastic syndrome (MDS) patients, showing potential as a therapy for MDS and leukemia (2012).
In 2002 Vitamin K2 analog menatetrenone treatment led to a short average response time of 3 months, with no adverse effects, and improvement in anemia in 6 of 13 RA (refractory anemia) patients, suggesting potential for MDS treatment.
In 2002 Menatetrenone ameliorated cytopenia in 5 of 9 MDS-RA patients (56%) with refractory anemia of myelodysplastic syndrome vs 11% of controls.
In 2005, vitamin K2 with vitamin D3 achieved combined effectiveness against leukemia cells, suggesting that it might be effective therapy for both MDS and leukemia.
In 2010, the addition of vitamin D3 to vitamin K2 more than doubled the response rate of MDS patients with refractory anemia and low white blood counts, from 13% to 30%.
HEART DISEASE:
Vitamin K does not consistently prevent progression of calcification, atherosclerosis or arterial stiffness. There may be some benefit in people with calcification at study entry. (2020)
In 2015, a three year double-blind randomized clinical trial showed that supplementation of Menaquinone-7 (vitamin K2) improved arterial stiffness in healthy postmenopausal women, particularly those with high baseline arterial stiffness.
BONE LOSS (ref):
A meta-analysis of 4 studies found vitamin K supplementation reduced the odds of vertebral fractures compared to control (OR 0.42, 95% CI 0.27-0.66).
A meta-analysis of 4 studies found vitamin K supplementation reduced the odds of clinical fractures compared to control (OR 0.44, 95% CI 0.23-0.88).
A meta-analysis of 5 studies found no significant effect of vitamin K on femoral neck BMD compared to control (mean difference -0.03, 95% CI -0.03 to 0.20).
One study gave 45 mg/day vitamin K2 for 24 months to rheumatoid arthritis patients and found no difference in BMD compared to control.
One study gave 500 μg/day vitamin K1 for 3 years to older adults and found no significant difference in BMD compared to control.
One study gave 360 μg/day vitamin K2 (MK-7) for 1 year to postmenopausal women and found no significant difference in BMD compared to placebo.
The effect of menatetrenone, a vitamin K2 analog, on disease recurrence and survival in patients with hepatocellular carcinoma after curative treatment: a pilot study, 2006
Abstract
Background: The high recurrence rate of hepatocellular carcinoma (HCC) determines the long-term prognosis for patients with HCC. In the current study, the authors tested the effects of menatetrenone, a vitamin K2 analog, on recurrent HCC and survival after curative treatment.
Methods: Sixty-one patients who were diagnosed as free of HCC after surgical resection or percutaneous local ablation were assigned randomly assigned to either a menatetrenone group (n = 32 patients) or a control group (n = 29 patients). Patients in the menatetrenone group received a daily oral dose of 45 mg of menatetrenone. Disease recurrence and survival rates were analyzed in patients with HCC.
Results: The cumulative recurrence rates in the menatetrenone group were 12.5% at 12 months, 39.0% at 24 months, and 64.3% at 36 months; and the corresponding recurrence rates in the control group were 55.2%, 83.2%, and 91.6%, respectively (P = 0.0002). Similar results were obtained even for patients who had low baseline levels of serum des-gamma-carboxy-prothrombin. Univariate and multivariate Cox proportional hazard analyses showed that the administration of menatetrenone was the only factor related to the recurrence rate of HCC. The cumulative survival rates for the patients who received menatetrenone were 100% at 12 months, 96.6% at 24 months, and 87.0% at 36 months; and the corresponding survival rates for patients in the control group were 96.4%, 80.9%, and 64.0%, respectively (P = 0.051).
Conclusions: The current study findings suggested that menatetrenone may have a suppressive effect on recurrence of HCC and a beneficial effect on survival, although a larger, placebo-controlled trial will be required to prove these effects.
Effect of menatetrenone, a vitamin k2 analog, on recurrence of hepatocellular carcinoma after surgical resection: a prospective randomized controlled trial, 2012
The aim of this study was to investigate whether menatetrenone (MNT) suppresses hepatocellular carcinoma (HCC) recurrence in patients undergoing hepatectomy. Between January 2005 and September 2009, 101 patients who underwent curative hepatectomy for primary HCC were enrolled in the study. Patients were divided into two groups: a non-MNT group (n=51), and an MNT group (n=50) that was administered 45 mg of MNT daily. During the observation period, recurrence was observed in 33 patients in the non-MNT group and in 28 patients of the MNT group (p=0.545). In patients with a preoperative Des-γ-carboxy-prothrombin (DCP) level lower than 40 AU/l (n=38), the cumulative disease-free survival rates at 12, 36, and 60 months in the non-MNT group, were 81.3%, 0.0%, and 0.0%, respectively, while those in the MNT group were 78.3%, 58.1%, and 31.0%, respectively (p=0.060). MNT has a moderately suppressive effect on HCC recurrence after hepatectomy, especially in patients with a normal preoperative DCP level.
Vitamin K2 in Action: The Case of Myelodysplastic Syndrome (link)
"Myelodysplastic syndrome" (MDS) is a disorder related to leukemia; in fact it was formerly known as "pre-leukemia."38,39 In patients with MDS, the bone marrow begins churning out increasingly young white blood cells of various kinds. In most cases it goes on to full-blown leukemia, with all of the disastrous consequences of that disease. But unlike leukemia, MDS cells, at least early on, can be induced to develop into mature normal blood cells.39,40 And that's where vitamin K comes in.
Vitamin K treatment of bone marrow cells from MDS patients potently induces apoptosis (programmed cell death) of the leukemic cells, with the effect much more prominent on blast cells than on mature white cells.41,42 Vitamin K2 also induces MDS cells to differentiate into healthy white blood cells, even when full-blown leukemia has developed.43
Successful therapy of MDS with vitamin K2 was first reported in 1999, in an 80-year-old woman with persistent anemia from the disease. Prior to treatment she had required regular blood transfusions; 14 months later she was independent of them.44 Similar benefits were found in a small group of MDS patients with refractory anemia in 2002.45 And some improvements were also found in MDS patients with low white blood counts compared with those receiving no treatment.46
Vitamin K2 selectively induces apoptosis of blastic cells in myelodysplastic syndrome: flow cytometric detection of apoptotic cells using APO2.7 monoclonal antibody, 1998
We have previously reported that vitamin K2 (VK2) but not VK1 has a potent apoptosis-inducing effect on freshly isolated leukemia cells from patients with various types of leukemia. By multi-color flow cytometric analysis using monoclonal antibody (mAb), APO2.7, which detects mitochondrial 7A6 antigen specifically expressed by cells undergoing apoptosis, we further investigated the apoptosis-inducing effect of VK2 on minor populations of leukemic blast cells in bone marrow from patients with myelodysplastic syndrome (MDS) and overt myeloid leukemia (post-MDS AML). Limiting dilution of CD95 (anti-Fas) mAb-treated apoptotic Jurkat cells with nonapoptotic CTB-1 cells revealed that APO2.7-positive Jurkat cells were consistently detectable by flow cytometry when present at levels of at least 5% in the CTB-1 suspension. In patient samples the gating area for leukemic clone was determined using cell surface antigen-specific mAbs conjugated with either fluorescein isothionate (FITC) or phycoerythrin (PE) and subsequently the cells stained with phycoerythrin cyanine (PE-Cy5)-conjugated APO2.7 mAb were assessed within the gating area of the leukemic clone for monitoring apoptosis. Treatment of the bone marrow mononuclear cells with 3-10 microM of VK2 (menaquinone-3, -4 and -5) in vitro potently induced apoptosis of the leukemic blast cells as compared with the untreated control cells in all 15 MDS patients tested. This effect was more prominent on blastic cells than that on mature myeloid cells such as CD34-/CD33+ gated cells. In addition, VK2 performed much less effectively on CD3-positive lymphoid cells. In contrast to VK2, VK1 did not show apoptosis-inducing activity. These data suggest that VK2 may be used for treatment of patients with MDS in blastic transformation.
Vitamin K2 induces apoptosis of a novel cell line established from a patient with myelodysplastic syndrome in blastic transformation, 1999
We have previously reported that vitamin K2 (VK2) has a potent apoptosis inducing activity toward various types of primary cultured leukemia cells including acute myelogenous leukemia arising from myelodysplastic syndromes (MDS). We established a novel cell line, designated MDS-KZ, from a patient with MDS in blastic transformation, and further investigated the effects of VK2 using this novel cell line. MDS-KZ shows complex chromosomal anomaly including −4, 5q−, −7, 13q+, 20q−, consistent with that seen in the original patient. Culture of MDS-KZ cells in RPMI1640 medium containing 10% FBS lead to steady but very slow proliferation with a doubling time of 14 days. However, the cellular growth rate was significantly accelerated in the presence of various growth factors such as granulocyte colony-stimulating factor, stem cell factor, granulocyte–macrophage colony-stimulating factor, interleukin-3, and thrombopoietin. Most of the cultured cells show the morphological features of myeloblasts. They are positive for CD7, CD33, CD34, CD45, CD117, and HLA-DR. However, about 10% of the cells are more mature metamyelocytes and neutrophils with various dysplastic characteristics such as pseudo-Pelger nuclear anomaly and hypersegmentation, suggesting a potential for differentiation in this cell line. As previously reported for cultured primary leukemia cells, exposure to VK2, but not to VK1, resulted in induction of apoptosis of MDS-KZ cells in a dose-dependent manner (IC50: 5 μM). In addition, VK2 treatment induced down-regulation of BCL-2 and up-regulation of BAX protein expression with concomitant activation of caspase-3 (CPP32). A tetrapeptide functioning as antagonist of caspase-3, Ac-DEVD-H, suppressed the VK2-induced inhibition of cell growth, suggesting that caspase-3 is, at least in part, involved in VK2-induced apoptosis. These observations suggest that the MDS-KZ cell line can serve as a model for the study of the molecular mechanisms of VK2-induced apoptosis.
Apoptosis/differentiation-inducing effects of vitamin K2 on HL-60 cells: dichotomous nature of vitamin K2 in leukemia cells, 2001
We originally reported that vitamin K2 (VK2) analogs, including menaquinone 4 (MK4) but not vitamin K1, effectively induce apoptosis in various types of primary cultured leukemia cells and leukemia cell lines in vitro. It has also been reported by others that VK2 showed the differentiation-inducing activity in leukemia cell lines. To investigate the discrepancy between apoptosis- and differentiation-inductions of leukemia cells by VK2 treatment, we used bcl-2 gene transfected HL-60 cells (HL-60-bcl-2) which resulted in five-fold over-expression of BCL-2 protein, and then compared the effects of MK4 to the control HL-60-neo cells. Seventy-two hours of exposure to various concentrations of MK4 resulted in growth inhibition of these cells in a dose-dependent manner (0.1-50 microM), however, HL-60-bcl-2 was less sensitive against MK4. MK4 potently induced apoptosis of HL-60-neo cells along with the depolarization of mitochondrial membrane potential and caspase-3 activation. Notably, HL-60-bcl-2 was almost completely resistant to apoptosis induction in response to MK4, although cell growth inhibition was still observed. In spite of the abrogation of apoptosis induction, about 90% of HL-60-bcl-2 cells were arrested in the G0/G1 phase within 48 h of exposure to 10 microM of MK4 accompanied by up-modulation of p27KIP1 expression. Concomitantly, HL-60-bcl-2 cells underwent monocytic differentiation. These data suggest that VK2 also shows the differentiation inducing effects on leukemia cells which are resistant against VK2-inducing apoptosis. The dichotomous nature of VK2 against leukemia cells appears to have clinical benefits for the treatment of patients with leukemias and myelodysplastic syndromes.
Successful therapy of myelodysplastic syndrome with menatetrenone, a vitamin K2 analog, 1999
Although vitamin K2 is an inducer of the in vitro differentiation of myeloid leukemic cell lines, its clinical efficacy in the treatment of myelodysplastic syndrome (MDS) is unclear. We administered a vitamin K2 analog, menatetrenone, at 45 mg daily to an 80-year-old woman with MDS (refractory anemia) heavily dependent on red-cell transfusions. The patient's pancytopenia gradually improved, and she became transfusion-independent after 14 months. Pancytopenia recurred when menatetrenone was discontinued but recovered again with readministration. Administration of menatetrenone at a dose effective in improving osteoporosis may also be useful in restoring hematopoiesis in MDS patients, possibly by way of inducing differentiation.
Vitamin K2 therapy for myelodysplastic syndrome, 2002
Vitamin K2 is reported to induce apoptosis or differentiation of leukemic cell lines in vitro. We administered a vitamin K2 analog, menatetrenone, at 45 mg daily to 23 patients with myelodysplastic syndrome (MDS): 13 patients with RA, 2 with RARS, 6 with RAEB and 2 with RAEB-T. Good response (GR) and partial response (PR) were defined as an increase of hemoglobin concentration exceeding 2 g/dl and 1-2 g/dl without transfusion, respectively. Six of the RA patients showed improvement of anemia (GR, 3 patients; PR, 3 patients). RA patients who did not have a hypocellular bone marrow and were transfusion-independent tended to be responsive to vitamin K2 therapy in combination with vitamin D3 or anabolic steroids. No adverse effect of vitamin K2 was observed, and the time required to obtain the hematological response was short, being 3 months on average. We believe that vitamin K2 therapy has potential as a treatment for patients with MDS.
Menatetrenone, a vitamin K2 analog, ameliorates cytopenia in patients with refractory anemia of myelodysplastic syndrome, 2002
Vitamin K2 induces differentiation of leukemic cell lines and apoptosis of immature blasts in myelodysplastic syndrome (MDS). We recently reported a case of MDS-refractory anemia (MDS-RA) with trilineage hematologic response to oral administration of menatetrenone, a vitamin K2 analog. To determine a possible role of this agent in treatment of MDS-RA, we conducted a prospective randomized trial assessing the safety and efficacy of menatetrenone. A total of 18 consecutive patients newly diagnosed with MDS-RA were randomized to receive either 45 mg of oral menatetrenone (group 1) or no menatetrenone (group 2). Administration of menatetrenone was well tolerated. Of the nine patients in group 1 (56%), five improved with menatetrenone treatment while only one (11%) of the group 2 patients improved. Three patients (33%) showed a major response in absolute neutrophil count (ANC), two (22%) showed a major response in hemoglobin concentration, and two of the nine (22%) showed a major response in platelet count. The ANC of group 1 patients rose after treatment, while that of group 2 patients decreased slightly at follow-up after 16 weeks ( p=0.03). Significant improvement was also seen in final platelet count ( p=0.01), but not in hemoglobin concentration. Given the absence of toxicity, menatetrenone can be recommended for all patients with MDS-RA.
Combined treatment of leukemia cells with vitamin K2 and 1alpha,25-dihydroxy vitamin D3 enhances monocytic differentiation along with becoming resistant to apoptosis by induction of cytoplasmic p21CIP1, 2005
Vitamin K2 (VK2) effectively induces apoptosis in leukemia cell lines, including HL-60 and U937. However, combined treatment of cells with VK2 plus 1alpha,25-dihydroxy vitamin D3 (VD3) resulted in suppression of VK2-inducing apoptosis and pronounced induction of monocytic differentiation as compared with that by VD3 alone. After achieving monocytic differentiation by pre-exposure to VK2 and VD3, the cells became resistant to various apoptotic stimuli including VK2- and H2O2-treatment and serum deprivation. Accumulation of cytoplasm p21CIP1 along with disappearance of nuclear p21CIP1 was detected in cells in response to 96-h treatment with VK2 plus VD3. A stable transfectant, U937-deltaNLS-p21CIP1, which lacked the nuclear localization signal of p21CIP1 and showed overexpression of cytoplasm p21CIP1 without monocytic differentiation, was resistant to apoptosis. These data suggest that a change of intracellular distribution of p21CIP1 from nucleus to cytoplasm along with differentiation appears to be anti-apoptotic. Clinical benefits of using VK2 for treatment of patients with leukemia and myelodysplastic syndrome (MDS) have been reported. Our data suggest that VK2 plus VD3 may be an effective combination for differentiation-based therapy for leukemia and also MDS whose cytopenias are mediated though apoptosis.
Multicenter phase II trial of vitamin K(2) monotherapy and vitamin K(2) plus 1alpha-hydroxyvitamin D(3) combination therapy for low-risk myelodysplastic syndromes, 2010
We performed an open-labeled single-arm prospective phase II clinical trial of vitamin K(2) (menatetrenone: VK2) monotherapy and VK2 plus 1alpha-hydroxyvitamin D(3) (alfacalcidol: VD3) combination therapy for myelodysplastic syndromes (MDS) with refractory anemia and refractory cytopenia with multilineage dysplasia, having either low or intermediate-1 risks of the IPSS. The overall response rate to VK2 monotherapy (45mg/day) after 16 weeks was 13% (5/38) including 4 cases with improvement of both anemia and thrombocytopenia and 1 case with thrombocytopenia. We then enrolled and evaluated 20 out of 33 VK2-monotherapy non-responders for VK2 plus VD3 (0.75microg/day) combination therapy. The overall response rate at 16 weeks after initiation of VK2 plus VD3 was 30% (6/20). HI for hemoglobin (Hb) was observed in 6 out of 11 patients (55%) and for thrombocytopenia in 3 out of 11 patients (27%), respectively. No HI was observed for neutropenia in VK2 monotherapy and VK2 plus VD3 combination therapy. It was suggested that IPSS scores and absolute neutrophil counts positively correlated, and Hb levels inversely correlated with the response to VK2 plus VD3 combination therapy. Our study demonstrated that VK2 plus VD3 combination therapy appears to be promising for improvement of anemia and thrombocytopenia with low/intermediate-1 MDS.
In 2010, Vitamin K2 plus vitamin D3 combination therapy showed a 30% overall response rate, with a positive correlation between IPSS scores, absolute neutrophil counts, and response to treatment, indicating promise for improving anemia and thrombocytopenia in low/intermediate-1 MDS patients.
Vitamin K2 and its derivatives induce apoptosis in leukemia cells and enhance the effect of all-trans retinoic acid
Geranylgeraniol, a polyprenylalcohol composing the side chain of vitamin K2 (VK2), was previously reported to be a potent inducer of apoptosis in tumor cell lines (Ohzumi H et al, J Biochem 1995; 117: 11-13). We examined the apoptosis-inducing ability of VK2 (menaquinone 3 (MK3), MK4 and MK5) and its derivatives such as phytonadione (VK1), as well as polyprenylalcohols with side chains of various lengths including farnesol (C15-OH; FO), geranylgeraniol (C20-OH; GGO), and geranylfarnesol (C25-OH; GFO) toward leukemia cells in vitro. MK3, MK4, MK5 and GFO (at 10 microM) showed a potent apoptosis-inducing activity for all freshly isolated leukemia cells tested and for leukemia cell lines such as NB4, an acute promyelocytic leukemia (APL)-derived cell line and MDS92, a cell line derived from a patient with myelodysplastic syndrome, although there were some differences depending on the cells tested. In contrast, VK1 showed no effect on any of the leukemia cells. The combination of MK5 plus all-trans retinoic acid (ATRA) resulted in enhanced induction of apoptosis in both freshly isolated APL cells and NB4 cells as compared to each reagent alone. These data suggest the possibility of using VK2 and its derivatives for the treatment of myelogenous leukemias, including APL.
The Remarkable Anticancer Properties of Vitamin K, 2010
Additional positive findings came in the form of two case reports, also from Japan. In the first, a 72 year-old woman with leukemia who had failed standard therapy experienced complete remission after vitamin K2 was added to her therapeutic regimen.29 In the second, an 85 year-old man with hepatocellular carcinoma after hepatitis C infection chose to take vitamin K but no chemotherapy.30 His tumor markedly regressed by CT scan, and his tumor markers in blood all normalized.
A study from Uruguay demonstrated that serum markers in a group of prostate cancer patients indicated tumor cell destruction following supplementation with vitamins C and K.31
Menaquinone-7(Vit K2) supplementation improves arterial stiffness in healthy postmenopausal women. A double-blind randomised clinical trial, 2015
Observational data suggest a link between menaquinone (MK, vitamin K2) intake and cardiovascular (CV) health. However, MK intervention trials with vascular endpoints are lacking. We investigated long-term effects of MK-7 (180 µg MenaQ7/day) supplementation on arterial stiffness in a double-blind, placebo-controlled trial. Healthy postmenopausal women (n=244) received either placebo (n=124) or MK-7 (n=120) for three years. Indices of local carotid stiffness (intima-media thickness IMT, Diameter end-diastole and Distension) were measured by echotracking. Regional aortic stiffness (carotid-femoral and carotid-radial Pulse Wave Velocity, cfPWV and crPWV, respectively) was measured using mechanotransducers. Circulating desphospho-uncarboxylated matrix Gla-protein (dp-ucMGP) as well as acute phase markers Interleukin-6 (IL-6), high-sensitive C-reactive protein (hsCRP), tumour necrosis factor-α (TNF-α) and markers for endothelial dysfunction Vascular Cell Adhesion Molecule (VCAM), E-selectin, and Advanced Glycation Endproducts (AGEs) were measured. At baseline dp-ucMGP was associated with IMT, Diameter, cfPWV and with the mean z-scores of acute phase markers (APMscore) and of markers for endothelial dysfunction (EDFscore). After three year MK-7 supplementation cfPWV and the Stiffness Index βsignificantly decreased in the total group, whereas distension, compliance, distensibility, Young's Modulus, and the local carotid PWV (cPWV) improved in women having a baseline Stiffness Index β above the median of 10.8. MK-7 decreased dp-ucMGP by 50 % compared to placebo, but did not influence the markers for acute phase and endothelial dysfunction. In conclusion, long-term use of MK-7 supplements improves arterial stiffness in healthy postmenopausal women, especially in women having a high arterial stiffness.
Vitamin K2 supplementation and arterial stiffness among renal transplant recipients-a single-arm, single-center clinical trial, 2017
Subclinical vitamin K deficiency is prevalent among renal transplant recipients and is associated with an increased risk of cardiovascular disease. However, the association between vitamin K supplementation and improvement of arterial stiffness has not been explored in the renal transplant population. The KING trial (vitamin K2 In reNal Graft) is a single-arm study that evaluated the association between the change in vitamin K status and indices of arterial stiffness following 8 weeks of menaquinone-7 (vitamin K2) supplementation (360 μg once daily) among renal transplant recipients (n = 60). Arterial stiffness was measured using carotid-femoral pulse wave velocity (cfPWV). Subclinical vitamin K deficiency was defined as plasma concentration of dephosphorylated-uncarboxylated matrix Gla protein (dp-ucMGP) >500 pmol/L.At baseline, 53.3% of the study subjects had subclinical vitamin K deficiency. Supplementation was associated with a 14.2% reduction in mean cfPWV at 8 weeks (cfPWV pre-vitamin K2 = 9.8 ± 2.2 m/s vs. cfPWV post-vitamin K2 = 8.4 ± 1.5 m/s; P < .001). Mean dp-ucMGP concentrations were also significantly reduced by 55.1% following menaquinone-7 supplementation with a reduction in the prevalence of subclinical deficiency by 40% (P = .001). When controlled for age, durations of hemodialysis and transplantation, and the change in 24-hour mean arterial pressure, the improvement in arterial stiffness was independently associated with the reduction in dp-ucMGP concentration (P = .014).Among renal transplant recipients with stable graft function, vitamin K2 supplementation was associated with improvement in subclinical vitamin K deficiency and arterial stiffness.
Effect of vitamin K supplementation on serum calcification propensity and arterial stiffness in vitamin K-deficient kidney transplant recipients: A double-blind, randomized, placebo-controlled clinical trial, 2023
Vitamin K deficiency is common among kidney transplant recipients (KTRs) and likely contributes to progressive vascular calcification and stiffness. In this single-center, randomized, double-blind, placebo-controlled trial, we aimed to investigate the effects of vitamin K supplementation on the primary end point, serum calcification propensity (calciprotein particle maturation time, T50), and secondary end points arterial stiffness (pulse wave velocity [PWV]) and vitamin K status in 40 vitamin K-deficient KTRs (plasma dephosphorylated uncarboxylated matrix Gla protein [dp-ucMGP] ≥500 pmol/L). Participants (35% female; age, 57 ± 13 years) were randomized 1:1 to vitamin K2 (menaquinone-7, 360 μg/day) or placebo for 12 weeks. Vitamin K supplementation had no effect on calcification propensity (change in T50 vs baseline +2.3 ± 27.4 minutes) compared with placebo (+0.8 ± 34.4 minutes; Pbetween group = .88) but prevented progression of PWV (change vs baseline -0.06 ± 0.26 m/s) compared with placebo (+0.27 ± 0.43 m/s; Pbetween group = .010). Vitamin K supplementation strongly improved vitamin K status (change in dp-ucMGP vs baseline -385 [-631 to -269] pmol/L) compared with placebo (+39 [-188 to +183] pmol/L; Pbetween group < .001), although most patients remained vitamin K-deficient. In conclusion, vitamin K supplementation did not alter serum calcification propensity but prevented progression of arterial stiffness, suggesting that vitamin K has vascular effects independent of calciprotein particles. These results set the stage for longer-term intervention studies with vitamin K supplementation in KTRs.
The effect of menaquinone-7 supplementation on dp-ucMGP, PIVKAII, inflammatory markers, and body composition in type 2 diabetes patients: a randomized clinical trial, 2022
Background: Type 2 diabetes mellitus (T2DM) is a common disorder that is characterized by chronic hyperglycemia and chronic inflammation, which also have a reinforcing effect on each other. The present research studied the effects of menaquinone (MK-7) supplementation on serum dp-ucMGP (dephospho uncarboxylated Matrix Gla Protein), PIVKAII (Prothrombin Induced by Vitamin K Absence), inflammatory markers and body composition indices in type 2 diabetes mellitus (T2DM) patients.
Methods: This 12-week double-blind placebo-controlled randomized clinical trial allocated 60 T2DM patients equally into a MK-7 (200 mcg/day) group or a placebo group. All patients also received dietary advice at the beginning of study and their dietary intakes were checked using a 3-day food record. The body composition of each patient was also measured and their vitamin K status was assessed using the ELISA method to measure serum dp-ucMGP and PIVKAII. In addition, inflammatory status indices were also measured, including hsCRP (high-sensitivity C-reactive protein), IL-6 (interleukin-6) and TNF-α (tumor necrosis factor alpha). All measurements were made both before and after the intervention period.
Results: In total 45 patients completed the trial (MK-7 group = 23 and placebo group = 22). The calorie and macronutrient intake of the two groups were similar pre and post intervention. There were statistically significant increases in dietary vitamin K intake for both groups over the course of the study (p < 0.05), but the intergroup differences were not significant. The body composition indices (i.e., body fat percentage, fat mass, fat free mass, muscle mass, bone mass and total body water) were not significantly different between groups or across the trial. The serum levels of the vitamin K markers, PIVKAII and dp-ucMGP, decreased significantly in the MK-7 group over the course of the study (p < 0.05), but there was no decrease in the placebo group. However, after adjusting for the baseline levels and changes in vitamin K intake, the between group differences were only significant for PIVKAII (p < 0.05). Following the intervention, the serum levels of the inflammatory markers (hsCRP, IL-6, and TNF-α) were significantly lower in the MK-7 group (p < 0.05), but not in the placebo group. However, the between group differences in the inflammatory markers were not statistically significant.
Conclusions: Although further studies are needed, it appears that MK-7 supplementation can be effective in improving PIVKAII levels, but not for improving dp-ucMGP, inflammatory status or the body composition indices of T2DM patients.
Six months vitamin K treatment does not affect systemic arterial calcification or bone mineral density in diabetes mellitus 2, 2020
Purpose
Vitamin K-dependent proteins are involved in (patho)physiological calcification of the vasculature and the bones. Type 2 diabetes mellitus (DM2) is associated with increased arterial calcification and increased fractures. This study investigates the effect of 6 months vitamin K2 supplementation on systemic arterial calcification and bone mineral density (BMD) in DM2 patients with a history of cardiovascular disease (CVD).
Methods
In this pre-specified, post hoc analysis of a double-blind, randomized, controlled clinical trial, patients with DM2 and CVD were randomized to a daily, oral dose of 360 µg vitamin K2 or placebo for 6 months. CT scans were made at baseline and follow-up. Arterial calcification mass was quantified in several large arterial beds and a total arterial calcification mass score was calculated. BMD was assessed in all non-fractured thoracic and lumbar vertebrae.
Results
68 participants were randomized, 35 to vitamin K2 (33 completed follow-up) and 33 to placebo (27 completed follow-up). The vitamin K group had higher arterial calcification mass at baseline [median (IQR): 1694 (812–3584) vs 1182 (235–2445)] for the total arterial calcification mass). Six months vitamin K supplementation did not reduce arterial calcification progression (β [95% CI]: − 0.02 [− 0.10; 0.06] for the total arterial calcification mass) or slow BMD decline (β [95% CI]: − 2.06 [− 11.26; 7.30] Hounsfield units for all vertebrae) when compared to placebo.
Conclusion
Six months vitamin K supplementation did not halt progression of arterial calcification or decline of BMD in patients with DM2 and CVD. Future clinical trials may want to pre-select patients with very low vitamin K status and longer follow-up time might be warranted.
Vitamin K2 and D in Patients With Aortic Valve Calcification: A Randomized Double-Blinded Clinical Trial, 2022
Background:
Menaquinone-7 (MK-7), also known as vitamin K2, is a cofactor for the carboxylation of proteins involved in the inhibition of arterial calcification and has been suggested to reduce the progression rate of aortic valve calcification (AVC) in patients with aortic stenosis.
Methods:
In a randomized, double-blind, multicenter trial, men from the community with an AVC score >300 arbitrary units (AU) on cardiac noncontrast computer tomography were randomized to daily treatment with tablet 720 µg MK-7 plus 25 µg vitamin D or matching placebo for 24 months. The primary outcome was the change in AVC score. Selected secondary outcomes included change in aortic valve area and peak aortic jet velocity on echocardiography, heart valve surgery, change in aortic and coronary artery calcification, and change in dp-ucMGP (dephosphorylated-undercarboxylated matrix Gla-protein). Safety outcomes included all-cause death and cardiovascular events.
Results:
From February 1, 2018, to March 21, 2019, 365 men were randomized. Mean age was 71.0 (±4.4) years. The mean (95% CI) increase in AVC score was 275 AU (95% CI, 225–326 AU) and 292 AU (95% CI, 246–338 AU) in the intervention and placebo groups, respectively. The mean difference on AVC progression was 17 AU (95% CI, –86 to 53 AU; P=0.64). The mean change in aortic valve area was 0.02 cm2 (95% CI, –0.09 to 0.12 cm2; P=0.78) and in peak aortic jet velocity was 0.04 m/s (95% CI, –0.11 to 0.02 m/s; P=0.21). The progression in aortic and coronary artery calcification score was not significantly different between patients treated with MK-7 plus vitamin D and patients receiving placebo. There was no difference in the rate of heart valve surgery (1 versus 2 patients; P=0.99), all-cause death (1 versus 4 patients; P=0.37), or cardiovascular events (10 versus 10 patients; P=0.99). Compared with patients in the placebo arm, a significant reduction in dp-ucMGP was observed with MK-7 plus vitamin D (–212 pmol/L versus 45 pmol/L; P<0.001).
Conclusions:
In elderly men with an AVC score >300 AU, 2 years MK-7 plus vitamin D supplementation did not influence AVC progression.
Vitamin K2 (Menaquinone-7) supplementation does not affect vitamin K-dependent coagulation factors activity in healthy individuals, 2021
Background:
Vitamin K has long been regarded as a procoagulant drug by physicians, and concerns have been raised with regard to its effects on hemostasis. Although many studies have shown that vitamin K supplementation is safe for thrombotic events, the effect of vitamin K supplementation on the activities of vitamin K dependent procoagulation factors in healthy individuals is not available.
Objectives:
This study aimed to investigate whether vitamin K2 supplementation at recommended doses affects the activity of vitamin K dependent procoagulation factors in healthy individuals without any anticoagulation treatment.
Design:
Forty healthy volunteers between 25 and 40 years of age were recruited. Menaquinone-7 (MK-7) was administrated at 90 μg for 30 days. Prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), and blood coagulation factors II, VII, IX, and X activities and Protein induced by vitamin K absence or antagonist-II (PIVKA-II) were measured on days 0 and 30 after MK-7 administration.
Results:
PT, APTT, and TT showed no significant differences on day 30 when compared with baseline. The activities of coagulation factors II, VII, IX, and X on day 30 showed no significant differences with those at baseline. PIVKA-II levels were unchanged after 30 days of MK-7 supplementation.
Conclusions:
MK-7 supplementation at recommended dosage does not affect vitamin K-dependent coagulation factors’ coagulation activity, and does not enhance the carboxylation of prothrombin in healthy individuals. This indicated that MK-7 administration does not alter hemostatic balance in healthy populations without anticoagulation treatment.
Vitamin K2 & Dental Calculus: How to Reverse Heart Disease, link
Cancer – German researchers studied more than 24,000 participants for 10 to 14 years. They found that those with the highest intake of Vitamin K-2 had a 62% reduction in the risk of lung cancer and a 35% reduction in the risk of prostate cancer. They also found that those with the highest intake of Vitamin K-2 who did get cancer experienced a 28% lower risk of dying from it.(9)
In another recent study conducted by the Mayo Clinic, researchers reported that the risk of developing Non-Hodgkin lymphoma was approximately 45% lower for participants whose vitamin K intakes were in the top 25% of the group.(10)
Other “blood thinning” medications such as aspirin, anti-platelet aggregators (e.g. Plavix), non-warfarin-type blood thinners (e.g. Pradax), cardiac or other medication do not interact with vitamin K2.
Recently published studies have revealed vitamin K's power to reduce recurrence of liver cancer—extending and even saving lives. The first reported on 61 patients documented to be free of their cancers following surgical treatment. Thirty-two were assigned to receive a vitamin K2 analogue called menatetrenone, while 29 received placebo.32 The supplemented group had recurrence of tumors of 12.5% at 12 months, 39.0% at 24 months, and 64.3% at 36 months. In the control group the recurrence rates were significantly higher: 55.2%, 83.2%, and 91.6%, respectively. And 100% of the supplemented group survived a full year, with 87% still alive at 36 months; among controls those numbers were 96.4% and a dismal 64%, respectively.
In a smaller study with 45 patients,33 rates of recurrence were only 33.3% in patients treated with vitamin K compared with 50% in controls. And survival rates tended to be modestly higher in treated patients.
How much Vit K2 in 100g Natto?
Natto contains 500 mcg Vit K per 50 grams. About 90% of Natto’s K2 is in MK-7 form (link).
Vit K Antagonists
Warfarin is a blood-thinning drug that functions by inhibiting vitamin K–dependent clotting factors. Warfarin is prescribed for people with various heart conditions such as atrial fibrillation, artificial heart valves, clotting disorders (hypercoagulability), or placement of indwelling catheters/ports.
Usually, blood tests must be done regularly to evaluate the extent of blood thinning, using a test for prothrombin time (PT) or international normalized ratio (INR). Vitamin K can decrease the blood-thinning effects of warfarin and will therefore lower the PT or INR value. This may increase the risk of clotting.
People taking warfarin are usually warned to avoid foods with high vitamin K1 content (such as green leafy vegetables) and to avoid vitamin K1 supplements. Conversely, vitamin K1 is used to treat overdoses or excess anticoagulant effects of warfarin and to reverse the effects of warfarin prior to surgery or other procedures.
Because the effects of warfarin on anticoagulation are usually delayed by several days, the PT/INR may not increase immediately at the time of overdose. If a patient’s blood becomes too thin, the person should be placed under strict medical supervision and may use oral or injected vitamin K1 to help reverse the effects of warfarin.
The anticoagulation reversal dose is one dose of 2.5 mg of vitamin K1 followed by immediate reevaluation ”, The Emerging Role of Vitamin K2 .
Comments