Colchicine
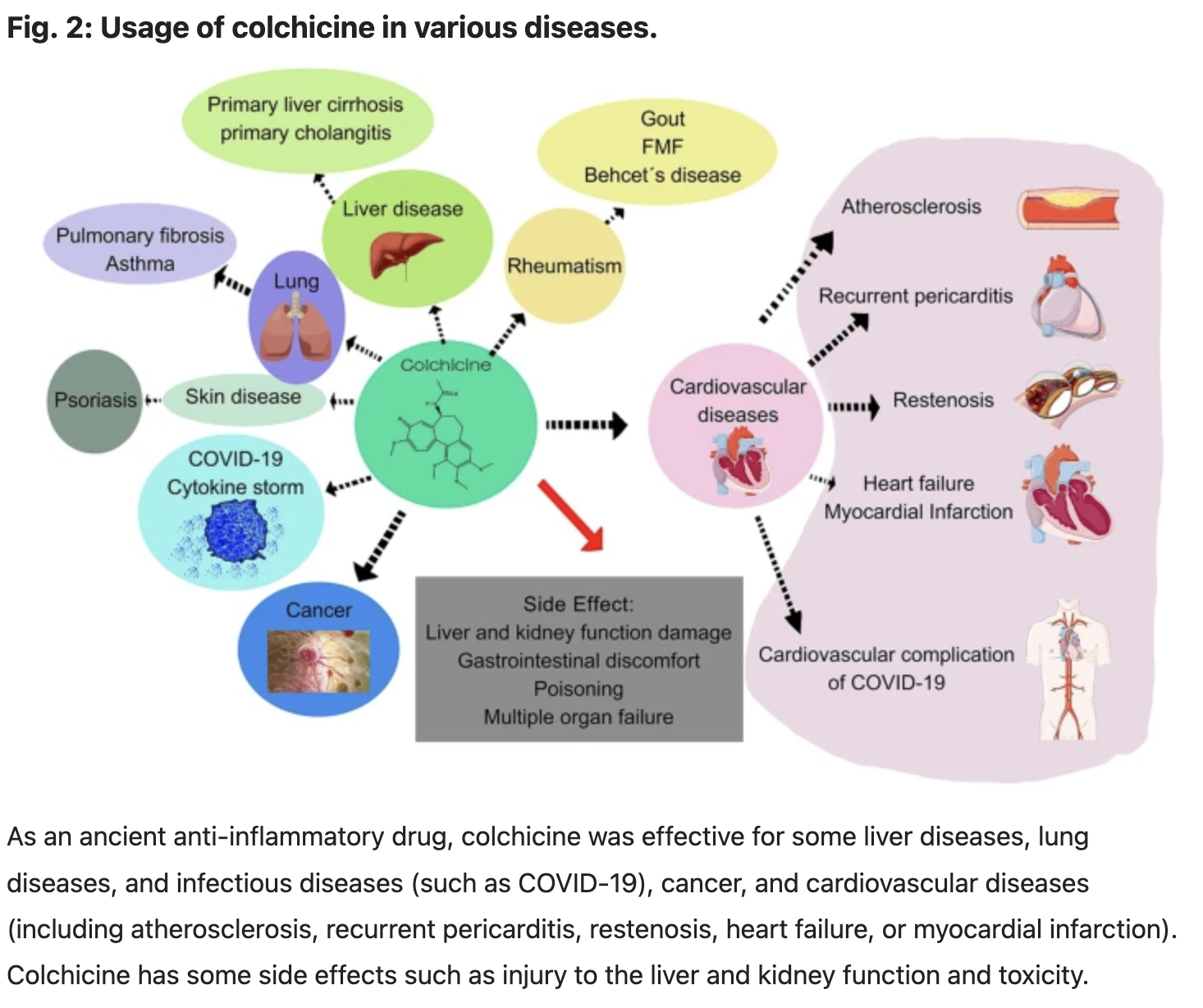
Colchicine is a medication primarily used to treat and prevent gout flares and familial Mediterranean fever. It reduces inflammation through several key molecular pathways and mechanisms:
Microtubule Disruption:
Colchicine binds to tubulin, a protein that forms microtubules, and prevents its polymerization into microtubules. This disrupts the cytoskeleton of cells, affecting their ability to move and function properly. In inflammatory cells, particularly neutrophils, this disruption inhibits their ability to migrate to sites of inflammation.
Inhibition of Neutrophil Activation:
By impairing microtubule formation, colchicine reduces the activation, mobility, and degranulation of neutrophils. Neutrophils are key players in the inflammatory response, and their reduced activity diminishes the release of pro-inflammatory substances like lysosomal enzymes and reactive oxygen species.
Reduction of Cytokine Production:
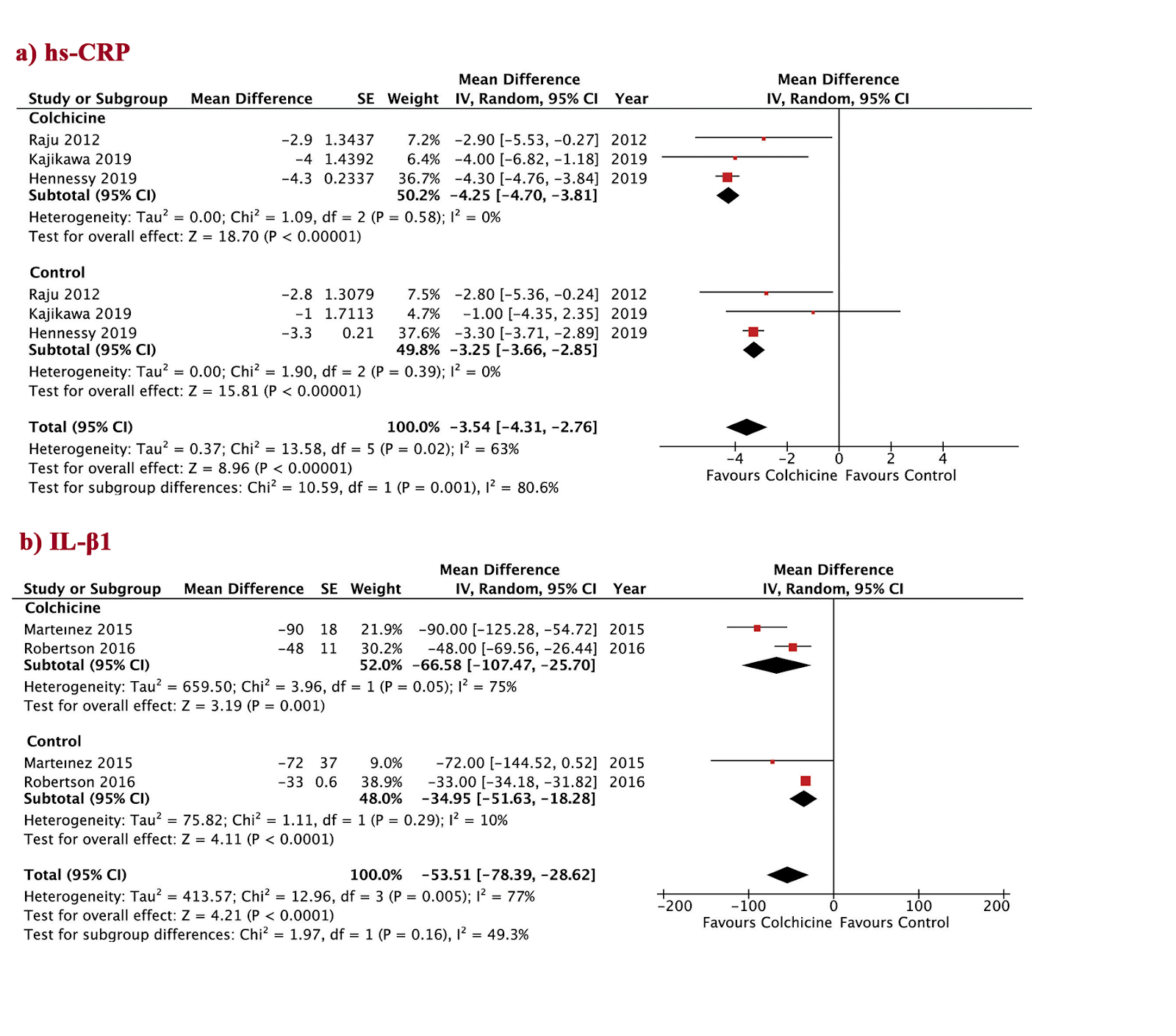
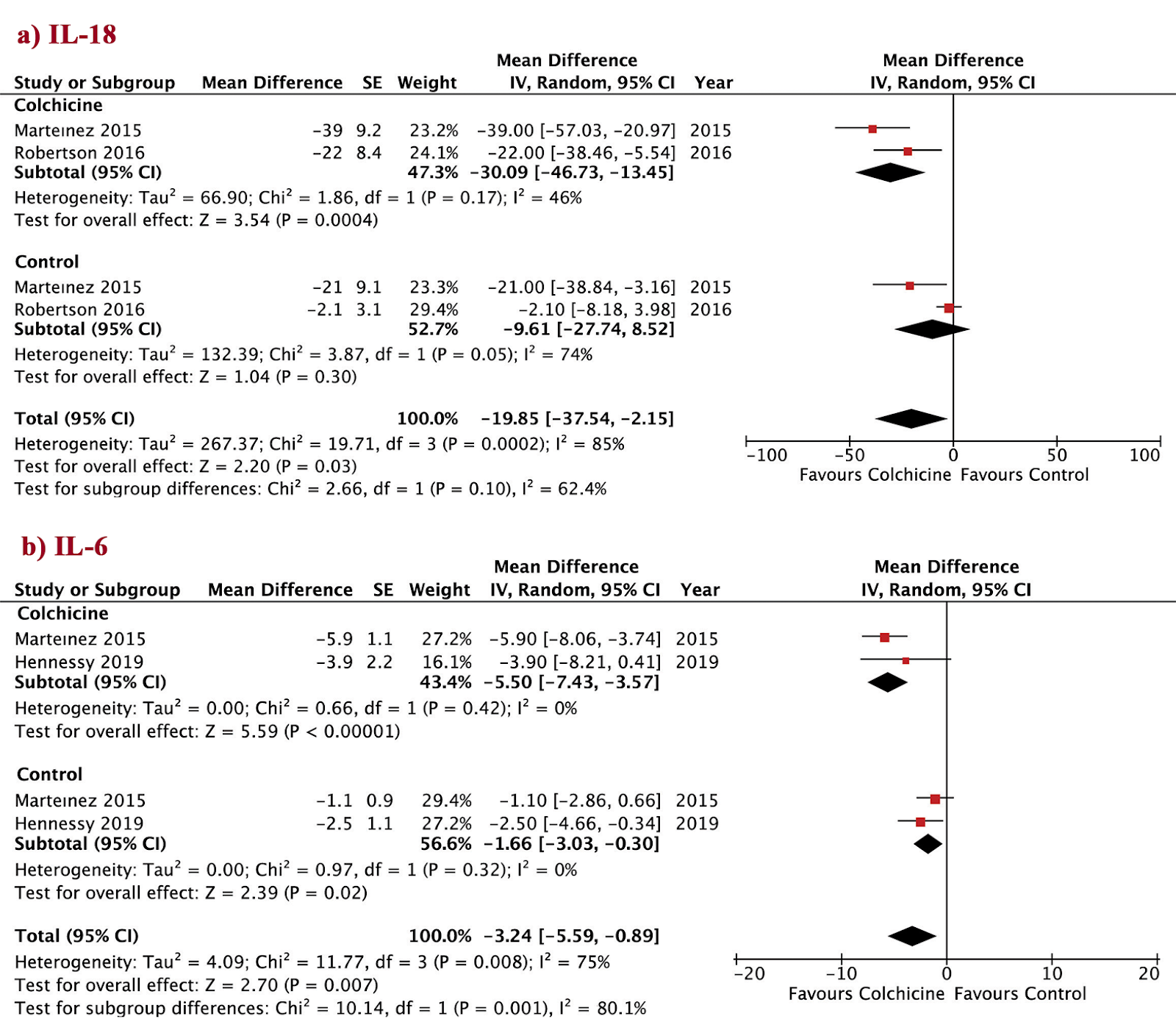
Colchicine interferes with the production of pro-inflammatory cytokines such as interleukin-1 beta (IL-1β) and tumor necrosis factor-alpha (TNF-α). This reduces the overall inflammatory response, as these cytokines are critical in promoting inflammation.
Inhibition of Inflammasome Activation:
Colchicine inhibits the assembly of the NLRP3 inflammasome, a multi-protein complex that plays a crucial role in the activation of IL-1β. By preventing inflammasome activation, colchicine reduces the maturation and secretion of IL-1β, thus attenuating inflammation.
Leukocyte Infiltration:
By preventing the release of chemotactic factors and inhibiting the adhesion of leukocytes to endothelial cells, colchicine reduces the infiltration of inflammatory cells into tissues.
These mechanisms collectively contribute to colchicine's anti-inflammatory effects, making it effective in treating conditions characterized by excessive inflammation.
Therapeutic potential of colchicine in cardiovascular medicine: a pharmacological review (2022)
Side effects and pharmacokinetic properties of colchicine
Colchicine has had limited clinical use because of its toxicity. The toxicity of colchicine is thought as the result of its overaction. Colchicine binds tubulin and destroys the microtubular network [157], which decreases endocytosis and exocytosis, damages organelle localization and protein assembly, alters cell shape, inhibits cell migration and division. Most cells of the body will be affected by colchicine, actively dividing cells in particular[158].
The pharmacokinetic properties of colchicine are now well described. Colchicine is absorbed by gastrointestinal tract and distributes rapidly around the body. The bioavailability of colchicine is 44% after oral ingestion and uptake in jejunum and ileum [159]. Higher concentrations of colchicine are observed in erythrocytes and leukocytes rather than plasma and its retention is up to 7 days [160], which indicated that the circulating concentrations of colchicine are maintained for a few days after a single oral dose. Many patients experience gastrointestinal discomfort after 24 h of medication, and common side effects are vomiting, diarrhea, and abdominal cramps [161] (side effects were shown in Fig. 2). Colchicine is metabolized by the liver and eliminated by the kidney. It will aggravate liver and kidney burden in patients with liver damage and renal failure or dysfunction [162], which will lead to the side effects even when given in low-dose. Cytochrome CYP3A4 [163] and P-glycoprotein [164] are two important elements in colchicine metabolism. CYP3A4, an isoform of cytochrome P450, is associated with demethylation and deacetylation of colchicine in liver [165]. P-glycoprotein, an integral membrane ATPase-dependent efflux pump is a colchicine transporter to expel colchicine out of the cell [166]. Specific inhibitory drugs of P-glycoprotein and CYP3A4, such as clarithromycin [167] will increase blood drug concentration and metabolic burden and even cause acute colchicine toxicity.
Short-term effect of low-dose colchicine on inflammatory biomarkers, lipids, blood count and renal function in chronic coronary artery disease and elevated high-sensitivity C-reactive protein (2020)
In 138 consecutive patients with chronic coronary artery disease and a high sensitivity C-reactive Protein (hs-CRP) ≥ 2 mg/L, inflammatory markers, lipids, haematologic parameters and renal function were measured at baseline and after 30 days exposure to colchicine 0.5mg once daily. Hs-CRP decreased from baseline 4.40 mg/L (interquartile range [IQR] 2.83–6.99 mg/L) to 2.33 mg/L (IQR 1.41–4.17, median of the differences -1.66 mg/L, 95% confidence interval [CI] -2.17 – -1.22 mg/L, p-value <0.01), corresponding to a median change from baseline of -40%. Interleukin-6 decreased from 2.51 ng/L (IQR 1.59–4.32 ng/L) to 2.22 ng/L (median of the differences -0.36 ng/L, 95%CI -0.70 – -0.01 ng/L, p-value 0.04), corresponding to a median change from baseline of -16%. No clinically relevant changes in lipid fractions were observed. Both leukocyte and thrombocyte count decreased (median change from baseline -7% and -4% respectively). Estimated glomerular filtration rate decreased with a mean change from baseline of -2%.
Effect of colchicine on inflammatory markers in patients with coronary artery disease: A meta-analysis of clinical trials (2022)
Efficacy and safety of colchicine in patients with coronary artery disease: A systematic review and meta-analysis of randomized controlled trials (2021)
Low-Dose Colchicine for Secondary Prevention of CAD: Key Points (2023)


Comments