CoQ10
Coenzyme Q10 and Degenerative Disorders Affecting Longevity: An Overview (2019)
Declining CoQ10 Levels with Age: The body's natural production of CoQ10 diminishes as we age, potentially leading to a higher risk of developing degenerative diseases (Kalén et al., 1989).
Cardiovascular Disease:
Two randomized controlled trials, Q-SYMBIO and KiSEL-10, found CoQ10 supplementation significantly reduced mortality in heart failure patients and elderly subjects, respectively.
In Q-SYMBIO, 3 x 100 mg/day CoQ10 for 2 years reduced the risk of major adverse cardiovascular events (MACE) by 42% and all-cause mortality by ~40% compared to placebo in chronic heart failure patients (Mortensen et al, 2014).
In KiSEL-10, a 5-year intervention of 200 mg/day CoQ10 + 200 mcg/day selenium reduced cardiovascular mortality by 53% and showed sustained protective effects for several years after ending supplementation in elderly subjects (Alehagen et al, 2013).
CoQ10 levels decline with age. CoQ10 and selenium may benefit heart health via roles in energy production, as antioxidants, and by preventing deficiency in the elderly.
Diabetes:
Diabetes patients often have low CoQ10 levels. Several randomized controlled trials have reported 100-200 mg/day CoQ10 for 3-6 months improves glycemic control, insulin sensitivity and vascular function in type 2 diabetes (e.g. Hodgson et al, 2002; Koladouz-Mohammadi et al, 2013; Zahedi et al, 2014; Zhang et al, 2018).
A meta-analysis found CoQ10 improves fasting glucose, HbA1c, and blood lipid profiles in type 2 diabetes (Zhang et al, 2018, 2022).
CoQ10 may benefit diabetes through roles in cellular energy, as an antioxidant, anti-inflammatory, and via gene expression (Amin et al, 2014; Heidari et al, 2018).
Statins increase diabetes risk, possibly by depleting CoQ10. Supplemental CoQ10 may help prevent statin-induced diabetes.
Chronic Kidney Disease (CKD):
CKD patients, especially those on hemodialysis, have low CoQ10 levels.
In a randomized trial, 3 x 100 mg/day CoQ10 for 3 months improved renal function and reduced the need for dialysis in end-stage CKD patients (Singh et al, 2000).
100 mg/day CoQ10 for 3 months reduced inflammation in CKD patients on hemodialysis (Zahed et al, 2016). High-dose CoQ10 (1800 mg/day) safely reduced oxidative stress in a dose-escalation study (Yeung et al, 2015).
A meta-analysis confirmed CoQ10 supplementation improves renal function, reduces inflammation and oxidative stress in CKD (Bakhshayeshkaram et al, 2018).
CoQ10 may reduce mortality in CKD by lowering risk of cardiovascular disease, a major cause of death in CKD patients.
Liver Disease:
The liver is the main site of CoQ10 synthesis. Liver disease may impair CoQ10 production.
Non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease increase risks of cardiovascular disorders. CoQ10 supplementation could help reduce these risks.
Animal studies show CoQ10 has anti-inflammatory, antioxidant and anti-fibrotic effects that may slow progression of liver disease (e.g. Tarry-Adkins et al, 2016; Fouad & Jresat 2012).
Two randomized controlled trials found 100 mg/day CoQ10 for 4-12 weeks improved markers of inflammation and liver damage in NAFLD patients (Farhangi et al, 2014; Farsi et al, 2016, 2023).
Oral CoQ10 supplementation, possibly combined with selenium, shows promising results in reducing mortality risk from various degenerative disorders. This is primarily attributed to CoQ10's critical role in cellular energy production, antioxidant capabilities, and anti-inflammatory effects. The efficacy of CoQ10 supplementation is significantly influenced by the quality and bioavailability of the product used. When appropriately formulated and administered, CoQ10 could be a valuable addition to the treatment plans for patients with cardiovascular disease, diabetes, kidney disease, and liver disease, thereby positively impacting longevity.
Coenzyme Q10 and cardiovascular disease: an overview (2015)
Based on the review article "Coenzyme Q10 and cardiovascular disease: an overview" by David Mantle published in the British Journal of Cardiology in October 2015, the following are the key points, conclusions and numerical results regarding coenzyme Q10 (CoQ10) and its role in cardiovascular disease:
Functions and importance of CoQ10 (Mantle, 2015):
CoQ10 has three key functions relevant to cardiovascular health: 1) It plays a vital role in cellular energy production, particularly in tissues with high energy requirements like the heart. 2) It acts as an important fat-soluble antioxidant. 3) It can directly regulate expression of genes involved in inflammation and fat metabolism.
CoQ10 levels decrease with age, with optimal production around age 25 and then declining thereafter. Levels can also be depleted by exercise, illness, and some medications. This provides a rationale for CoQ10 supplementation.
Congestive heart failure (CHF) (Mantle, 2015):
Early studies in the 1970s by Langsjoen, Folkers and Littarru found CHF patients had CoQ10 deficiencies that correlated with severity of CHF. The first clinical trial showed long-term efficacy and safety of CoQ10 in over 100 CHF patients over 6 years (Langsjoen et al, 1990).
24 out of 28 randomized controlled trials (RCTs) over a 40-year period up to 2010 reported positive outcomes of CoQ10 supplementation in CHF.
A study by Morisco et al (1993) in about 600 NYHA class III-IV patients found CoQ10 significantly reduced hospitalizations and serious complications.
3 meta-analyses have reported CoQ10 supplementation significantly improves parameters like ejection fraction in CHF (Soja & Mortensen, 1997; Sander et al, 2006; Fotino et al, 2013).
The Q-SYMBIO study, a 2-year RCT in 420 CHF patients, found 3x100mg/day CoQ10 in addition to standard therapy reduced risk of major adverse cardiovascular events (MACE) by 42%, cardiac death by 44% and all-cause mortality by 42% vs placebo (Mortensen et al, 2014). This is a greater reduction than the 18% decrease in MACE reported with the drug LCZ696 vs enalapril in the PARADIGM study.
Atherosclerosis (Mantle, 2015):
CoQ10, though in lower concentrations than vitamin E, is the first line of defense against LDL oxidation, a key step in atherosclerosis (Stocker et al, 1991). The CoQ10:LDL ratio may be more important than the HDL:LDL ratio (Tomasetti et al, 1999).
CoQ10 supplementation (150 mg/day for 2 weeks) reduced LDL levels by about 13% in healthy men (Schmelzer et al, 2011).
Singh et al (2003) found 120 mg/day CoQ10 for 1 year reduced atherosclerosis risk after MI in addition to statin therapy.
Lee et al (2013) reported 300 mg/day CoQ10 for 3 months increased antioxidant enzymes and reduced inflammation in atherosclerosis patients on statins.
A meta-analysis found CoQ10 supplementation significantly improved endothelial function (Gao et al, 2012).
Hypertension (Mantle, 2015):
CoQ10 acts as a vasodilator. Its antioxidant effects increase nitric oxide availability in blood vessels, promoting vasodilation.
Several RCTs have reported CoQ10 can significantly lower blood pressure, alone or with antihypertensive drugs, without adverse effects:
Singh et al (1999): 120 mg/day CoQ10 for 8 weeks lowered systolic BP by 16 mmHg and diastolic by 9 mmHg.
Burke et al (2001): 120 mg/day CoQ10 for 12 weeks reduced systolic BP by about 18 mmHg in isolated systolic hypertension.
A meta-analysis concluded CoQ10 can lower systolic BP by up to 17 mmHg and diastolic by 10 mmHg (Rosenfeldt et al, 2007).
Cardiovascular disease prevention (Mantle, 2015):
The KiSel-10 study, a 5-year RCT in 440 elderly Swedes given 200 ug selenium + 200 mg CoQ10 daily, found a >50% reduction in cardiovascular mortality (5.9% vs 12.6%) and improved cardiac function vs placebo (Alehagen et al, 2013).
Statins and CoQ10 (Mantle, 2015):
Statins inhibit HMG-CoA reductase, the rate-limiting enzyme for both cholesterol and CoQ10 synthesis. Statins can deplete CoQ10 levels, which may account for some of their adverse effects.
Several RCTs in approx. 50-60 patients have reported CoQ10 supplementation (100-300 mg/day for 1-4 months) significantly reduced statin-related muscle symptoms (Caso et al, 2007; Fedacko et al, 2013; Skarlovnik et al, 2014).
Safety of CoQ10 (Mantle, 2015):
Extensive safety data show CoQ10 is well-tolerated with no serious adverse effects, even at high doses. It cannot be overdosed. Some studies used up to 1200 mg/day.
Over 200 RCTs in various disorders have confirmed its safety (Hidaka et al, 2008). Post-marketing surveillance data also support its safety.
In conclusion, this comprehensive review by Mantle (2015) presents extensive evidence from laboratory research, clinical trials and meta-analyses supporting the efficacy and safety of CoQ10 supplementation in congestive heart failure, atherosclerosis, hypertension, and statin-related muscle symptoms. The well-established mechanisms of action of CoQ10 provide a sound scientific rationale for its use in cardiovascular disorders. However, Mantle emphasizes that the dose and bioavailability of the CoQ10 supplement is important to achieve therapeutic blood levels and effects. Overall, this review makes a strong case for the benefits of CoQ10 supplementation in cardiovascular disease prevention and treatment.
Reduced Cardiovascular Mortality 10 Years after Supplementation with Selenium and Coenzyme Q10 for Four Years: Follow-Up Results of a Prospective Randomized Double-Blind Placebo-Controlled Trial in Elderly Citizens (2015)
Reduction in blood viscosity by treatment with coenzyme Q10 in patients with ischemic heart disease (1990)
The effects of coenzyme Q10 (CoQ10) on blood viscosity were studied in twelve patients (mean age 49 +/- 16 years) with ischemic heart disease. Twenty mg of CoQ10 was orally administered three times daily for two months (total dose 60 mg per day). Blood viscosity was measured with a cone-plate type viscometer at the shear rates of 37.5, 75, 150, and 375 s-1. Yield shear stress was calculated from Casson's plot. Blood viscosity decreased at each shear rate after the administration of CoQ10. Yield shear stress decreased significantly by the treatment with CoQ10. Hematocrit and fibrinogen were also measured, but showed no significant change. These results suggest that CoQ10 decreases the blood viscosity, i.e., improves the rheological properties of blood in ischemic heart disease.
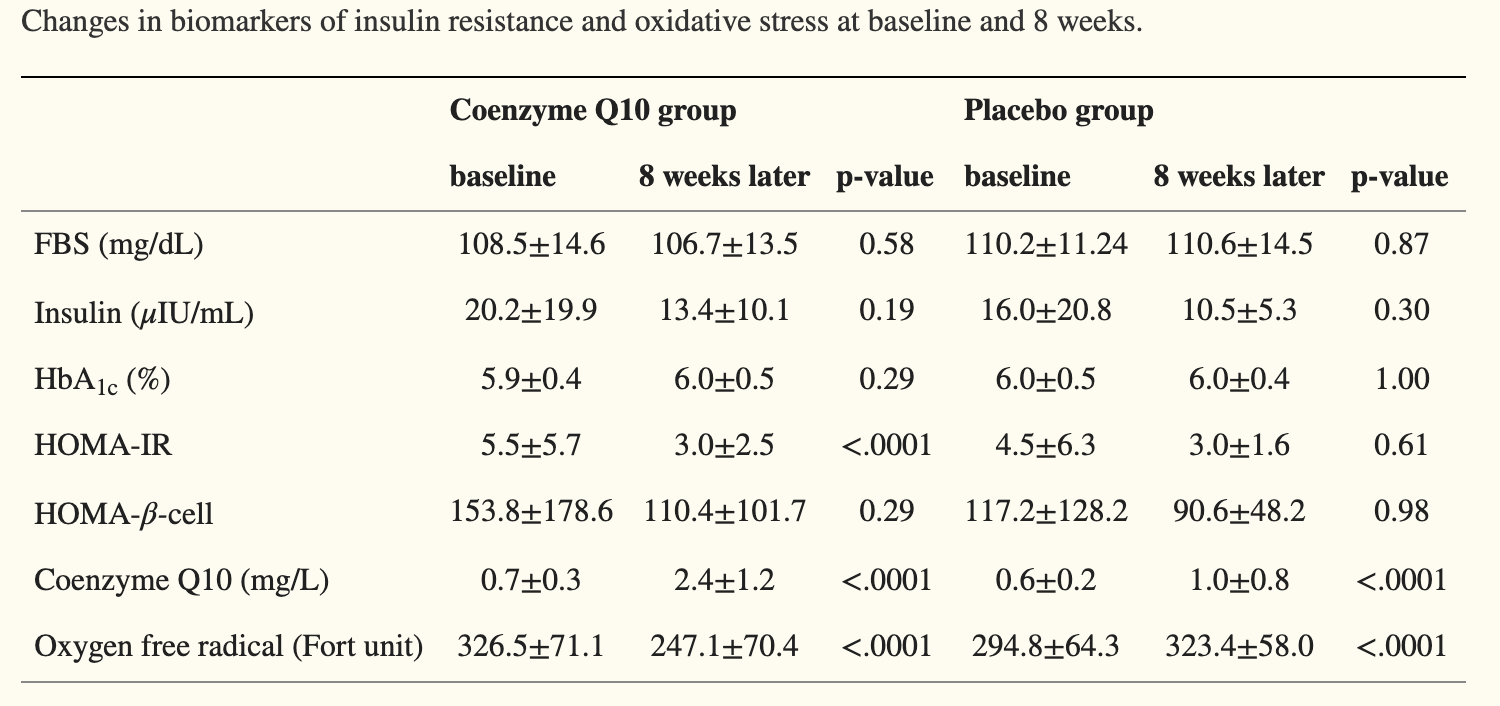
Effect of Coenzyme Q10 on Insulin Resistance in Korean Patients with Prediabetes: A Pilot Single-Center, Randomized, Double-Blind, Placebo-Controlled Study (2018)
The experimental group received coenzyme Q10 (200 mg/day) for 8 weeks, while the placebo group received a placebo via the same schedule.
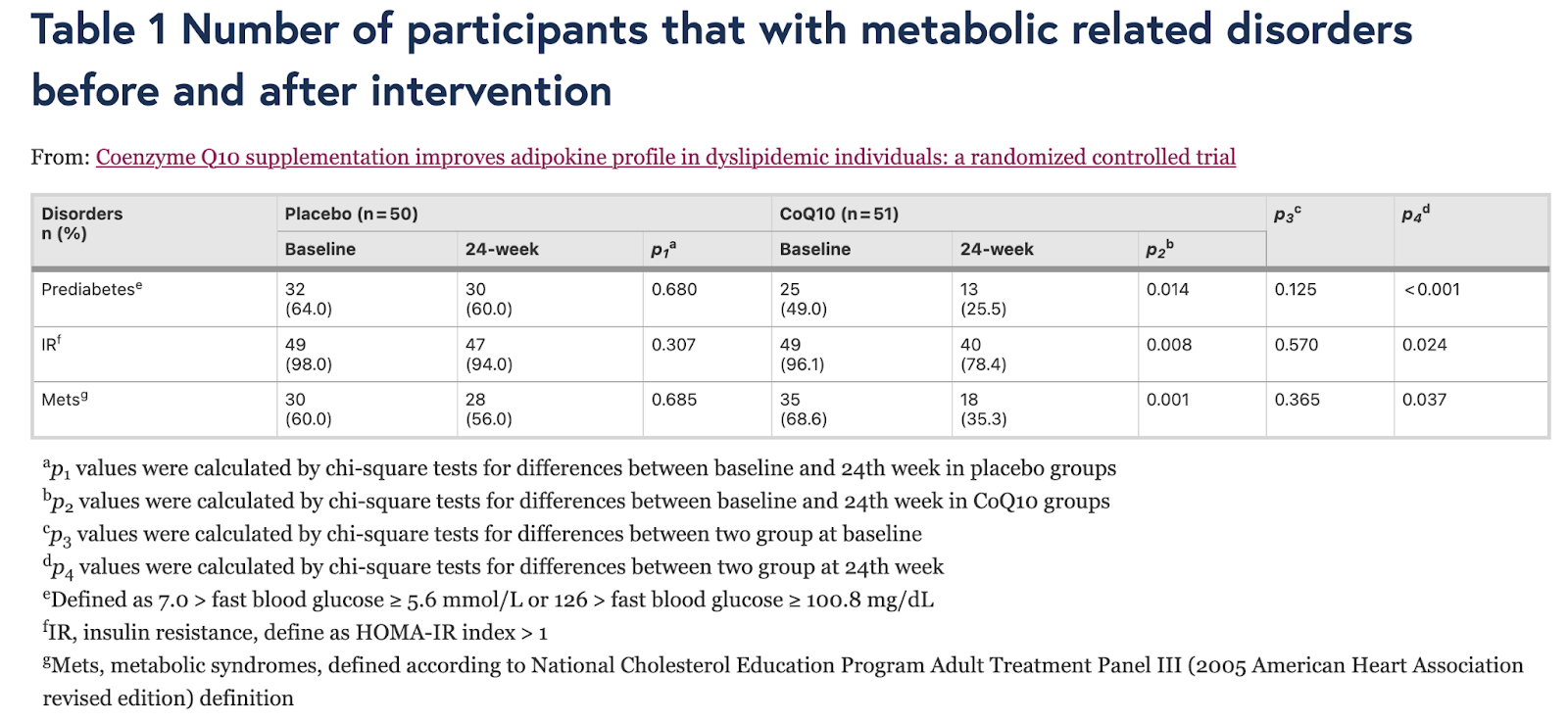
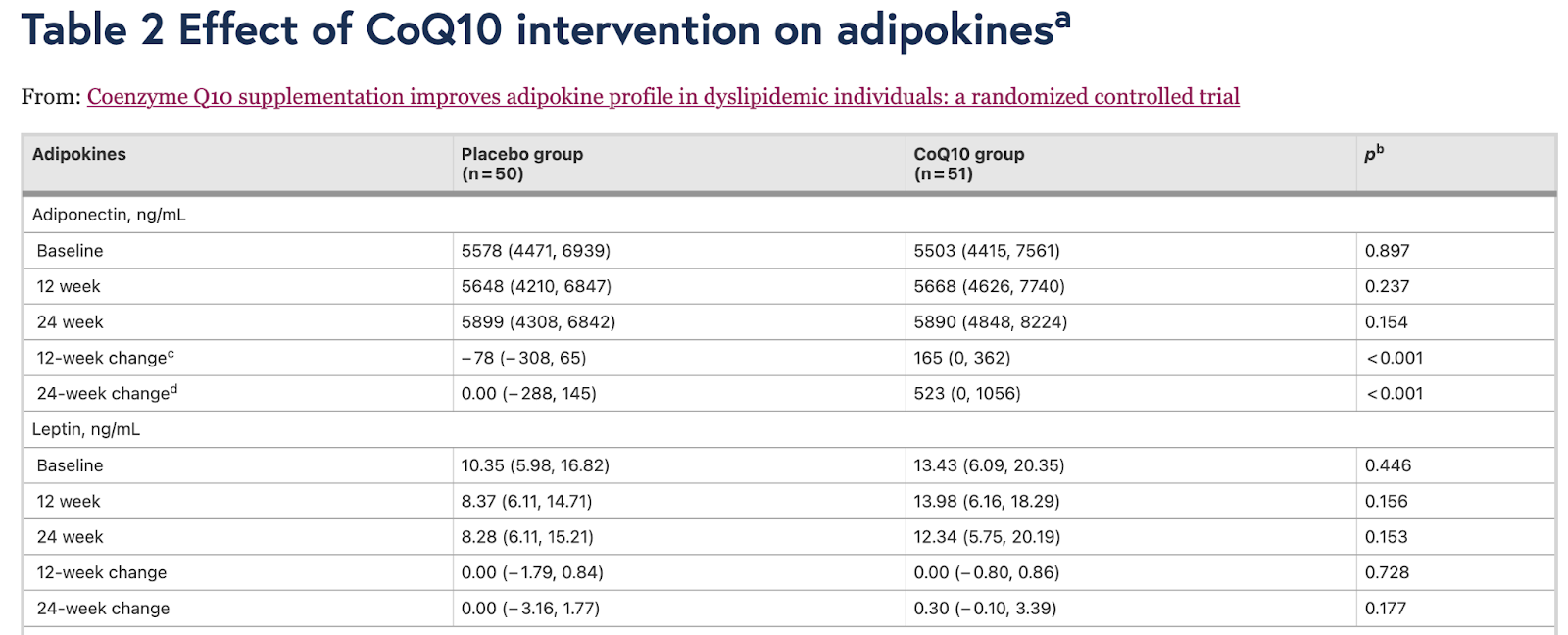
Coenzyme Q10 supplementation improves adipokine profile in dyslipidemic individuals: a randomized controlled trial (2022)
In this randomized, double-blinded, placebo-controlled trial, 101 dyslipidemic individuals were administrated to 120 mg CoQ10 or placebo for 24 weeks. Anthropometric parameters, glucolipid profile, serum total adiponectin, leptin, and resistin were evaluated at baseline, week 12 and week 24.
CoQ10 treatment significantly increased serum adiponectin levels at week 12 (165 [0, 362] ng/mL, p < 0.001) and at week 24 (523 [0, 1056] ng/mL, p < 0.001]), which was significant different compared with placebo (p < 0.001). The increase of adiponectin was negative associated with decrease in index of homeostasis model assessment of insulin resistance (HOMA-IR, r = − 0.465, p = 0.001), triglyceride (TG, r = − 0.297, p = 0.047), and low-density lipoprotein cholesterol (LDL-c, r = − 0.440, p = 0.002) at week 24 only in CoQ10-treated group. Resistin was reduced by CoQ10 only at week 24 (− 1.19 [− 4.35, 0.00] ng/mL, p < 0.001), which was significant different compared with placebo (p < 0.001). Reduction of resistin was positively correlated with the change in HOMA-IR (r = 0.343, p = 0.021) and TG (r = 0.323, p = 0.030) at week 24 in CoQ10-treated group but not placebo group. Leptin was not influenced by CoQ10 treatment. Mediation analysis indicated that the improvement of HOMA-IR, TG and LDL-c by CoQ10 was mediated by adiponectin but not resistin.
Our study shows that CoQ10 ameliorates glucolipid profile and adipokines dysfunction in dyslipidemic patients in 24 weeks’ intervention. The beneficial effect of CoQ10 on glucolipid profile was mediated by adiponectin.
Functions of Coenzyme Q10 Supplementation on Liver Enzymes, Markers of Systemic Inflammation, and Adipokines in Patients Affected by Nonalcoholic Fatty Liver Disease: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial (2016)
Background: Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disorder related to inflammation. Coenzyme Q10 (CoQ10) is a natural compound that has recently been considered as an anti-inflammatory factor. In the current study we aimed to evaluate the effects of CoQ10 supplementation on liver enzymes, inflammation status, and adipokines in patients with NAFLD.
Methods: Forty-one subjects with NAFLD participated in the current randomized, double-blind, placebo-controlled trial. The participants were randomly divided into 2 groups: one group received CoQ10 capsules (100 mg once a day) and the other received placebo for 12 weeks. Blood samples of each patient were taken before and after the 12-week intervention period for measurement of liver aminotransferases, inflammatory biomarkers, and adipokines (adiponectin and leptin).
Results: Taking 100 mg CoQ10 supplement daily resulted in a significant decrease in liver aminotransferases (aspartate aminotransferase [AST] and gamma-glutamyl transpeptidase [GGT]), high-sensitivity C-reactive protein (hs-CRP), tumor necrosis factor α, and the grades of NAFLD in the CoQ10 group in comparison to the control group (p < 0.05). In addition, patients who received CoQ10 supplement had higher serum levels of adiponectin (p = 0.016) and considerable changes in serum leptin (p = 0.053). However, no significant changes occurred in serum levels of interleukin-6 in both groups.
Conclusion: The present study suggested that CoQ10 supplement at a dosage of 100 mg could be effective for improving the systemic inflammation and biochemical variables in NAFLD.
Reduction in blood viscosity by treatment with coenzyme Q10 in patients with ischemic heart disease (1990)
Coenzyme Q10 (CoQ10): Can this antioxidant help protect RBCs from oxidative damage and improve their flexibility?
Coenzyme Q10 (CoQ10) is a naturally occurring compound that plays a crucial role in energy production within cells. It is known for its antioxidant properties and potential health benefits. Here's how CoQ10 may help protect red blood cells (RBCs) and improve their flexibility:
1. Antioxidant protection: CoQ10 acts as a powerful antioxidant, neutralizing harmful free radicals that can cause oxidative stress and damage to cell membranes, including those of RBCs. By reducing oxidative damage, CoQ10 may help maintain the integrity and function of RBCs.
2. Improved RBC flexibility: RBCs need to be flexible to effectively navigate through small blood vessels and deliver oxygen to tissues. Oxidative stress can impair RBC flexibility, making it harder for them to pass through narrow capillaries. CoQ10's antioxidant properties may help preserve RBC flexibility by reducing oxidative damage to cell membranes.
3. Enhanced energy production: CoQ10 is a vital component of the mitochondrial electron transport chain, which is responsible for generating ATP (cellular energy) through a process called oxidative phosphorylation. By supporting efficient energy production within RBCs, CoQ10 may help these cells maintain their normal function and shape.
4. Potential cardiovascular benefits: In addition to its effects on RBCs, CoQ10 has been studied for its potential cardiovascular benefits. It may help support healthy blood pressure levels, improve endothelial function (the lining of blood vessels), and reduce inflammation, all of which can contribute to overall cardiovascular health and better blood flow.
Coenzyme Q10 Attenuates Human Platelet Aggregation Induced by SARS-CoV-2 Spike Protein via Reducing Oxidative Stress In Vitro (2022)
Coenzyme Q10 Reduces Platelet Hyperreactivity and Attenuates Atherosclerosis via Inhibiting Platelet αIIbβ3-mediated Signaling Pathway (2018)
Influence of the disease duration on erythrocytic antioxidant defense in patients with polycythemia vera (2001)
Twelve patients with polycythemia vera (PV) were observed and assigned to two groups: group 1 had duration of the disease up to 3 years (mean duration 2.1 years); group 2 - more than 10 years (mean duration 14.6 years). 50 healthy volunteers served control. Content of hemoglobin (Hb) was determined in blood and red blood cells (RBC). Activities of superoxide dismutase (SOD), catalase (CAT), glutathione reductase (GSSG-R), glutathione peroxidase (GSH-Px), glucose-6-phosphate dehydrogenase (G-6-PD) and content of malondialdehyde (MDA) were evaluated. It was shown that RBC in patients with PV have essential changes in their antioxidant systems (AOS). In early stage of PV (group 1) activation of SOD, CAT, GSSG-R and G-6-PD has compensating characteristics. Development of the disease (group 2) leads to weakening of AOS and activation of lipid peroxidation in membranes of RBC and to reduction of Hb level. The obtained results confirm the need for correction of AOS in RBC of patients to use natural antioxidants in the routine therapy of PV.
Oxidative stress is increased in primary and post−polycythemia vera myelofibrosis (2010)
The Thrombotic Events in Polycythemia Vera Patients May Be Related to Increased Oxidative Stress (2014)
Interferon-alpha2 treatment of patients with polycythemia vera and related neoplasms favorably impacts deregulation of oxidative stress genes and antioxidative defense mechanisms (2022)
Efficacy and Optimal Dose of Coenzyme Q10 Supplementation on Inflammation-Related Biomarkers: A GRADE-Assessed Systematic Review and Updated Meta-Analysis of Randomized Controlled Trials (2023)
Based on this systematic review and meta-analysis of 30 randomized controlled trials involving 1506 participants, Hou et al. (2022) provide the following key conclusions regarding the effects of coenzyme Q10 (CoQ10) supplementation on inflammatory biomarkers:
CoQ10 supplementation significantly reduced circulating levels of C-reactive protein (CRP) (SMD: -0.41, 95% CI: [-0.69 to -0.12], p = 0.005), interleukin-6 (IL-6) (SMD: -0.67, 95% CI: [-1.01 to -0.33], p < 0.001), and tumor necrosis factor-α (TNF-α) (SMD: -1.06, 95% CI: [-1.59 to -0.52], p < 0.001) compared to control groups.
CoQ10 supplementation also significantly increased circulating CoQ10 concentrations (WMD: 0.99, 95% CI: [0.84 to 1.14], p < 0.001).
Subgroup analyses indicated that a CoQ10 dose of 300-400 mg/day achieved the greatest reductions in inflammatory markers:
CRP: SMD: -1.65, 95% CI: [-3.11 to -0.20], p = 0.026
IL-6: 200-300 mg/day dose - SMD: -0.64, 95% CI: [-1.03 to -0.25], p = 0.001
TNF-α: SMD: -1.16, 95% CI: [-1.91 to -0.41], p = 0.002
Subgroup analyses by health status showed CoQ10 significantly reduced:
CRP in healthy individuals (SMD: -4.07, 95% CI: [-5.39 to -2.75], p < 0.001)
IL-6 in healthy people, CVD patients and those with other diseases
TNF-α in dyslipidemia, NAFLD and other disease patients
CoQ10's anti-inflammatory effects did not appear to depend on supplementation duration. Significant reductions in inflammatory markers were seen with both short (<12 weeks) and long durations (≥12 weeks).
The quality of evidence based on GRADE assessment was very low for the effects of CoQ10 on CRP, IL-6 and TNF-α, mainly due to heterogeneity between studies.
Potential mechanisms for CoQ10's anti-inflammatory actions include inhibiting oxidative stress, NF-κB signaling, and the NLRP3 inflammasome.
In conclusion, this meta-analysis provides evidence that CoQ10 supplementation, especially at doses of 300-400 mg/day, can significantly reduce circulating levels of the inflammatory biomarkers CRP, IL-6 and TNF-α in both healthy individuals and those with various diseases. However, the overall quality of evidence is very low, indicating a need for additional high-quality RCTs with larger sample sizes to further substantiate these findings. The authors note they are currently designing a clinical trial to further investigate the efficacy and optimal anti-inflammatory dose of CoQ10.
Coenzyme Q10 (2024)
Coenzyme Q10 (CoQ10), also known as ubiquinone, is a fat-soluble, vitamin-like molecule naturally present in every cellular membrane within our bodies (Sood et al, 2024). It is crucial for efficiently transferring electrons within the mitochondrial oxidative respiratory chain and producing adenosine triphosphate (ATP) (Sood et al, 2024). CoQ10 can potentially increase the production of vital antioxidants, such as superoxide dismutase, an enzyme that effectively mitigates vascular oxidative stress in individuals with hypertension (Sood et al, 2024). Furthermore, CoQ10 can improve blood flow and safeguard blood vessels by preserving nitric oxide (Sood et al, 2024).
Certain conditions such as fibromyalgia, diabetes, cancer, heart failure, and neurodegenerative, mitochondrial, and muscular diseases are linked to reduced circulating levels of CoQ10 (Sood et al, 2024; Du et al, 2018; Cordero et al, 2012). Statin drugs inhibit the production of an intermediate in the mevalonate pathway—a biochemical route leading to CoQ10 synthesis (Sood et al, 2024; Zaleski et al, 2018). Researchers theorize that statin drugs may contribute to CoQ10 depletion, and given that muscle pain and cramping are frequent adverse effects of statins, they attribute these symptoms to the diminished levels of CoQ10 (Sood et al, 2024; Skarlovnik et al, 2014).
According to the 2022 ACC/AHA/HFSA guidelines, supplementation with CoQ10 effectively reduced vascular mortality, all-cause mortality, and hospital stays for heart failure at 2 years, although long-term supplementation is needed (Correction to: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure, 2022). A recently published systematic review showed that supplementation with CoQ10, in addition to standard therapy in patients with moderate-to-severe heart failure, is associated with symptom reduction and reduction of major adverse cardiovascular events (Jafari et al, 2018; Bhatt et al, 2018). CoQ10 may improve functional capacity, endothelial function, and left ventricle contractility in congestive heart failure patients (Jafari et al, 2018; Belardinelli et al, 2006).
Supplementation shows promising results in improving endothelial function in several subsets of patients. CoQ10 can improve endothelial function in patients with ischemic left ventricular systolic dysfunction and heart failure (Dai et al, 2011; Zozina et al, 2018). Likewise, compared with placebo, CoQ10 improves endothelial function in the peripheral circulation of patients with type 2 diabetes mellitus and hyperlipidemia (Watts et al, 2002).
CoQ10 shows the potential to decrease pain, fatigue, and morning tiredness compared to a placebo in patients with fibromyalgia (Cordero et al, 2013; Cordero et al, 2011). Some data suggest that supplementation with moderate-to-high dose CoQ10 may influence bicycle exercise aerobic capacity in patients with mitochondrial disorders (Glover et al, 2010). Supplementation with CoQ10 in men with Peyronie disease may decrease penile plaque size, reduce penile curvature, and improve erectile function (Safarinejad, 2010).
A double-blind, randomized controlled trial showed 300 mg daily to be safe and superior to a placebo for migraine prevention (Sándor et al, 2005). Another randomized, double-blind, placebo-controlled trial in adult women showed that 400 mg of supplementation decreased migraine frequency, severity, and duration (Dahri et al, 2019). One study showed that only 100 mg daily reduced the severity of headaches and the number of headaches per month in migraine sufferers (Shoeibi et al, 2017).
The meta-analysis of RCTs indicated that CoQ10 supplementation (100 to 600 mg/d) decreased the Statin-Associated Muscle Symptoms (SAMS) (Qu et al, 2018). In patients with primary CoQ10 deficiency, early treatment with high-dose supplementation (ranging from 5 to 50 mg/kg/day) can limit disease progression (Salviati et al, 2017). A recent study of CoQ10 supplementation (20 mg/kg) demonstrated promising results in patients with primary CoQ10 deficiency with nephrotic syndrome and sensorineural hearing loss (Yuruk Yildirim et al, 2020).
CoQ10 supplementation reduces systemic inflammation and biochemical parameters in nonalcoholic fatty liver disease (NAFLD) (Campisi et al, 2022). However, as mentioned in pharmacokinetics, CoQ10 is excreted in bile. Hence, use is not advised in patients with biliary obstruction (Campisi et al, 2022). According to a recent meta-analysis, supplementation with CoQ10 may benefit clinical pregnancy rates (CPR) in assisted reproductive technologies (ART) (Florou et al, 2020).
Most human studies on CoQ10 have focused on its oral supplementation. Available in various forms, such as tablets, capsules, soft gels, and liquid formulations, these oral supplements range from 30 to 600 mg per unit and are easily accessible over the counter (Sood et al, 2024). While topical over-the-counter preparations are also available, research on this mode of administration is limited (Sood et al, 2024; Knott et al, 2015).
The common adverse effects of CoQ10 are generally mild and infrequent, including stomach upset, nausea, vomiting, and diarrhea (Drugs and Lactation Database, 2021; Baggio et al, 1994). Dosages of 100 mg/d or higher have been associated with mild insomnia in some individuals (PDQ Integrative, Alternative, and Complementary Therapies Editorial Board, 2022). Liver enzyme elevation is seen in some patients taking 300 mg or more daily, but no liver toxicity is reported. Caution is required in bile duct obstruction (PDQ Integrative, Alternative, and Complementary Therapies Editorial Board, 2022). Other rare adverse effects have included dizziness, photophobia, irritability, headache, heartburn, increased involuntary movements, and fatigue (Drugs and Lactation Database, 2021; Baggio et al, 1994; Feigin et al, 1996).
CoQ10 is chemically similar to vitamin K, and some reports are available in the literature for potential warfarin and CoQ10 interaction. There are chances of warfarin treatment failure when patients are taking CoQ10 supplements with warfarin therapy. This interaction is reversible (Landbo et al, 1998; Engelsen et al, 2003; Engelsen et al, 2002).
CoQ10 is safe as a dietary supplement. Toxicity is unlikely up to a daily intake of 1200 mg/d, although typical dosages have been 100 to 200 mg/d (Hidaka et al, 2008). In preclinical studies, ubiquinol's No-Observed-Adverse-Effect Level (NOAEL) is 300 to 600 mg/kg (Sprague Dawley rats). The human supplementation dose of CoQ10 is generally 100 to 300 mg/d. Assuming the human dose is 300 mg/day (5 mg/kg body weight), the safety factor is 60 to 120 times. The study indicated that chronic use of ubiquinol as a dietary supplement in humans is safe (Deshmukh et al, 2019).
In summary, coenzyme Q10 is a promising dietary supplement with potential therapeutic benefits in various conditions, including heart failure, fibromyalgia, migraine prophylaxis, and mitochondrial disorders. It may also help alleviate statin-associated muscle symptoms and improve endothelial function in certain patient subsets. While generally well-tolerated, caution is advised in patients with biliary obstruction or those taking warfarin. As research continues to evolve, healthcare professionals must stay updated on the latest evidence to make informed decisions when recommending CoQ10 supplementation to their patients.
Parenteral CoQ10 Formulation (BPM31510) Significantly Improves Survival In Animal Model Of Leukemia Including The Resolution Of Paraplegia Due To Brain Metastasis (2013)
Leukemia cells exhibit alterations in intermediary metabolism similar to other cancers, wherein ATP sourcing is shunted from mitochondrial oxphos towards glycolytic preponderance (Warburg Effect) to meet oncogenic proliferative demands. A consequence of this metabolic switch is the simultaneous short-circuit of the programmed death pathways, leading to a immortalization program in cancer cells including leukemia. Delivery of high levels of CoQ10 in a lipid nanodispersion mixture (BPM31510) has been demonstrated to preferentially shift metabolic networks from glycolysis towards mitochondrial-centric oxphos and recapitulation of apoptotic pathways in various cancers in vitro and in vivo models. Given the centrality of the Bcl-2 involvement in the etiology of leukemia, this study focused on investigation of the effectiveness of BPM31510 in animal models of erythroid and myeloid leukemia. Human acute erythro-leukemia (K562) and acute myeloid leukemia (KG1) models were developed in immune-compromised mice. The mice (total n=120 for each model respectively) were randomized into four (n=30/group) treatment groups: Untreated (control); BPM31510 (75 mg/kg, once/day); chemotherapy (Adriamycin [5mg/kg; once/wk]+AraC [25mg/kg; 5 days] and BPM31510+chemotherapy. All dosing were intravenous and followed a protocol of 3wk treatment followed by 1wk rest. In both leukemia models, combination of BPM31510 with chemotherapy was associated with significant increase in survival compared to other groups. BPM31510 alone improved survival compared to chemotherapy in myeloid leukemia, not in erythroleukemia model. In a separate study, a rat (Fisher 344) chloroleukemia (MIA C51) model of CNS leukemia was developed that demonstrated paraplegia and urinary retention as a result of brain metastasis. Administration of BPM31510 (50 mg/kg/day, IP) was associated with complete resolution of limb paralysis demonstrating the ability of BPM31510 in penetrating into the CNS. Moreover, BPM31510 (50 mg/kg/day, IP) administration was associated with significant increase in survival in animals with metastasis to the lungs and liver. The data provides encouraging evidence of the potential translational use of CoQ10 containing BPM31510 in the treatment of leukemia. A Phase 1 study in relapse acute leukemia is to be started shortly.
Integrative Hematology: State of the Art (2023)
Coenzyme Q10 (CoQ10): Some evidence suggests the efficacy of CoQ10, at a dosage of 1200 mg/daily, in causing not only hematological but even cytogenetic remissions [9].
The rationale for using this substance is that plasma CoQ10 concentration decreased in an untreated MDS group compared to controls; this could be related to the mitochondrial dysfunction and systemic inflammation [10]. Furthermore, its known antioxidant action could contribute to its effectiveness.
A more recent study showed, in fact, a significant impairment of mitochondrial respiration in peripheral blood cells in low-risk MDS; the utilization of CoQ10 and carnitine improved not only mitochondrial function but also cytopenia and quality of life [11].
It is currently unclear which patient setting could benefit most from this substance but, given the lack of side effects, we believe it makes sense to use it in all patients with myelodysplastic syndrome, also in consideration of anecdotal data on marked improvement in patients with sideroblastic anemia and mitochondrial myopathy [12].


Comments