Bisphosphonates
Osteoporosis and Fracture Prevention:
Bisphosphonates are the most widely used medications for osteoporosis. Alendronate, risedronate, ibandronate, and zoledronic acid are the most common.
Alendronate reduces vertebral fractures by 50% and non-vertebral fractures by 50% in women with prevalent vertebral fractures. It reduces hip fracture risk by 34% in the oldest old patients (Black et al., 1996; Cummings et al., 1998; Axelsson et al., 2017).
Yearly IV zoledronic acid reduces vertebral fractures by 70% and hip fractures by 40% in postmenopausal women. It also reduces fracture risk when given after a hip fracture (Black et al., 2007; Lyles et al., 2007).
A 2017 meta-analysis found bisphosphonates significantly reduced overall osteoporotic fracture risk (OR 0.62), vertebral fractures (OR 0.55), and non-vertebral fractures (OR 0.73) compared to placebo. Zoledronic acid showed the greatest reduction in overall fracture risk (OR 0.61) (Tan et al., 2017).
Muscle Mass and Strength:
Some evidence suggests bisphosphonates may have positive effects on muscle mass and strength, but data are limited.
A retrospective study found alendronate use was associated with increases in skeletal muscle mass index (+0.137 kg/m2), appendicular skeletal muscle mass (+514 g), and lower limb muscle mass (+319 g) at 1 year compared to no treatment, after adjusting for confounders (Ito et al., 2015).
A retrospective study of osteoporosis patients found 4 years of zoledronic acid treatment increased appendicular skeletal muscle mass by 841 g and skeletal muscle mass index by 0.35 kg/m2, while the control group decreased (Kaneko et al., 2021).
In a mouse model of Duchenne muscular dystrophy, pamidronate treatment increased muscle strength and suppressed muscle damage markers compared to placebo (Yoon et al., 2016).
In Caenorhabditis elegans, bisphosphonates delayed age-related muscle decline and improved neuromuscular function across the lifespan (Hughes et al., 2023).
In analyses of postmenopausal women and bariatric surgery patients, oral bisphosphonates showed modest lean mass preservation effects compared to placebo (Cain et al., 2022).
Bisphosphonates and Mortality:
Several observational studies have reported 25-60% lower overall mortality in osteoporosis patients receiving bisphosphonates, particularly alendronate, that is too large to be solely attributed to fracture reduction (Bliuc et al., 2016).
However, a 2019 meta-analysis of 38 clinical trials (101,642 participants) found no significant association between all bisphosphonate treatments and overall mortality (risk ratio 0.98; 95% CI, 0.91-1.05). Trials of zoledronate showed no association with overall mortality but evidence of heterogeneity existed (I2 = 48.2%) (Cummings et al., 2019).
A 2019 retrospective cohort study using propensity score matching found a 15% lower mortality rate in bisphosphonate users vs controls (hazard ratio 0.85, 95% CI 0.79–0.91) over median 2.8 year follow-up. The risk reduction occurred within days of treatment, suggesting potential confounding (Bergman et al., 2019).
A systematic review and meta-analysis found bisphosphonate use, especially zoledronic acid, reduced post-fracture mortality among osteoporosis patients, particularly after hip/vertebral fractures, compared to non-use (Lin et al., 2021).
Bisphosphonates and Cardiovascular Disease:
A 2016 meta-analysis of 61 trials found bisphosphonates reduced arterial calcification (mean difference -11.52%; 95% CI -16.51 to −6.52) but not arterial stiffness. No effect on cardiovascular events was seen overall (RR 1.03; 95% CI 0.91–1.17). Bisphosphonates tended to reduce cardiovascular mortality (RR 0.81; 95% CI 0.64–1.02) and significantly reduced all-cause mortality (RR 0.90; 95% CI 0.84–0.98) (Kranenburg et al., 2016).
Observational studies show mixed results on bisphosphonates and cardiovascular benefits. Some found lower cardiovascular events/mortality with bisphosphonate use, especially after hip fracture, while others found no effect (Sing et al., 2018; Rodríguez et al., 2020; Casula et al., 2020).
Zoledronic acid may increase atrial fibrillation risk based on post-hoc analyses of some trials, but most observational studies found no increased risk overall with bisphosphonates. Caution is still advised in high-risk patients (Cipriani et al., 2022).
Current evidence is insufficient to recommend bisphosphonates solely for cardioprotection, but they appear safe in patients with CVD and may provide some cardiovascular benefits (Cipriani et al., 2022).
Bisphosphonates and Cancer:
In vitro and animal studies suggest bisphosphonates, especially zoledronic acid, have anti-cancer effects through inducing tumor cell apoptosis, disrupting the bone microenvironment, and stimulating anti-tumor immunity (Modi & Lentzsch, 2012).
Clinical trials in multiple myeloma found adding zoledronic acid to chemotherapy improved survival (Aviles et al., 2007), and zoledronic acid improved overall and progression-free survival vs clodronate (Morgan et al., 2010). However, meta-analyses found no significant survival benefit overall, possibly due to differences in bisphosphonates and populations studied (Modi & Lentzsch, 2012).
A 2015 meta-analysis of adjuvant bisphosphonates in early breast cancer (18,766 women) found highly significant reductions in bone recurrence (28%), distant recurrence (18%), and breast cancer mortality (18%) in postmenopausal women only (Early Breast Cancer Trialists' Collaborative Group, 2015).
A pharmacoepidemiologic study found the combination of statins and bisphosphonates was associated with significantly increased overall cancer survival compared to no treatment (HR 0.60; 95% CI, 0.45 to 0.81) (Babcook et al., 2019).
A remarkable hematological and molecular response pattern was observed in a patient with polycythemia vera during combination therapy with simvastatin and alendronate.
In lymphoma patients receiving glucocorticoids, oral alendronate prevented chemotherapy-induced bone mineral density loss at 1 year compared to placebo (Westin et al., 2022).
Other Key Points:
Bisphosphonates are widely used to treat osteoporosis and reduce fracture risk. They have a long half-life in bone (>10 years for alendronate) and effects can persist for years after discontinuation (Papapoulos, 2005).
Serious adverse effects like osteonecrosis of the jaw are rare (<1-3 per 10,000 patient-years with oral bisphosphonates for osteoporosis). Preventive dental care and avoiding invasive dental procedures during treatment can reduce risk (Cremers & Farooki, 2011).
A remarkable hematological and molecular response pattern in a patient with polycythemia vera during combination therapy with simvastatin and alendronate
https://www.sciencedirect.com/science/article/pii/S2213048916300127
Fascinating case report. The patient was on:
Aspirin 75 mg/day
Dipyramidole 200 mg 2 times/day
Simvastatin 40 mg/day
Alendronate 70 mg/week
JAK2 burden spontaneously dropped from 64% to 10-20% and the patient stayed in hematological remission for 56 months.
Lack of clinical benefit of zoledronic acid in myelofibrosis: results of a prospective multi-center phase II trial (2015)
Based on the results of this prospective multi-center phase II trial reported by Delforge et al. (2015), zoledronic acid does not appear to provide significant clinical benefit in the treatment of myelofibrosis.
The study evaluated the effects of zoledronic acid, administered as a standard regimen of 3-weekly doses of 4mg, in 16 patients with myelofibrosis. It was inspired by pre-clinical data suggesting zoledronic acid may have disease-modifying effects and by three prior case reports documenting beneficial effects of bisphosphonates on peripheral blood counts in myelofibrosis patients.
However, with the exception of one patient who experienced normalization of hemoglobin and a significant increase in platelet count after 12 infusions, the study was unable to document therapeutic effects on:
Blood counts: The mean hemoglobin level decreased by 0.05 g/dL per 3-week interval, constituting a significant decrease over the study period (p=0.03). The probability of needing red blood cell transfusions did not decrease. Leukocyte and platelet counts did not change significantly.
Hepato-/splenomegaly: Mean spleen size increased significantly at visit 7 (p=0.01) and this persisted at visit 13 (p=0.03). Liver size did not change significantly.
Degree of marrow fibrosis: Bone biopsy examinations did not reveal a significant change (p=0.37).
Constitutional symptoms: There was no significant change in the ECOG performance score or constitutional symptoms, except an improvement in night sweats (p=0.006).
A significant reduction in night sweats was noted, but given the multifactorial etiology of this symptom and lack of improvement in any other symptoms, this was considered a non-specific effect.
Although the study overall showed significant deterioration of anemia and splenomegaly, the authors note a subtle disease-slowing effect of zoledronic acid cannot be excluded, but remains speculative without a randomized comparison.
In the one patient who responded, a consistent beneficial effect on blood counts became apparent only after the 12th infusion, suggesting a considerable cumulative dose may be required for a biological effect to occur. This contrasts with a previous case report showing a more rapid response.
The safety profile was considered favorable overall. One patient developed osteonecrosis of the jaw, a known complication of prolonged nitrogen-containing bisphosphonate treatment, which resolved spontaneously after 18 months.
In conclusion, while a clear hematologic response in a single patient supports the hypothesis that zoledronic acid may have some disease-modifying effect in myelofibrosis, the authors state that in an era where JAK inhibitors and novel targeted therapies are drastically changing the treatment paradigm, this study of 16 patients provides insufficient evidence to support a role for zoledronic acid in myelofibrosis treatment. Larger randomized trials would be needed to definitively evaluate any potential benefit.
Clodronate in myelofibrosis: a case report (2002)
Agnogenic myeloid metaplasia (AMM) is an older term for primary myelofibrosis, a chronic myeloproliferative disorder (MPD):
AMM: Also known as chronic idiopathic myelofibrosis, this disease is characterized by bone marrow fibrosis and progressive anemia. The spleen and liver enlarge, and blood is produced in these organs instead of the bone marrow.
A 59-year-old man had well-documented agnogenic myeloid metaplasia (AMM) with pancytopenia. Frequent blood transfusions were required over a 10-month period. Androgen therapy was not beneficial and treatment with interferon resulted in severe thrombocytopenia with no decrease in transfusion requirements. Treatment with clodronate at a daily oral dose of 30 mg/kg resulted in a marked decrease in bone marrow fibrosis, and gradual normalization of blood counts over an 8-month period. He has been transfusion independent for the last 33 months. We support the findings of a previous case report that oral bisphosphonate therapy may be of value in patients with AMM.
Zoledronate-induced remission of acute panmyelosis with myelofibrosis (2004)
Acute panmyelosis with myelofibrosis is a rare and aggressive form of acute myeloid leukemia. We describe a new case with a huge proliferation of megakaryocytes, blast cells and reticulin fibers. The patient was treated with zoledronate, a third-generation bisphosphonate, and a gradual recovery from pancytopenia was observed. A new bone marrow biopsy performed 4 months later showed a surprising disappearance of the leukemic infiltration. Ten months after the diagnosis, the patient is still in healthy condition. This may support the recently described anti-tumor activity of zoledronate.
Clinical and haematological improvement induced by etidronate in a patient with idiopathic myelofibrosis and osteosclerosis (1994)
We report a patient with agnogenic myeloid metaplasia (AMM) associated with debilitating bone pain due to increased bone turnover and osteosclerosis. Treatment with etidronate at a dose of 6 mg/kg per day on alternate months resulted in a complete recovery of bone symptoms and normalization of metabolic parameters of bone turnover; unexpectedly, a sustained haematological improvement was also observed after several months of therapy, suggesting that bone marrow microenvironment improvement was able to restore a nearly normal haemopoiesis. We suggest that diphosphonate therapy may be of value in patients with AMM and increased bone turnover.
Osteoporosis and bone fractures: Learn More – What are the pros and cons of medication to prevent bone fractures? (link)

There are differences in how the various medications are used, though:
Alendronate: once a day or once a week as a tablet or an effervescent (fizzy) tablet to be dissolved in water
Ibandronate: once a month as a tablet or every three months through a drip
Risedronate: as a tablet taken daily, weekly or monthly, depending on the dosage
Zoledronic acid: once a year through a drip
Alendronate is by far the most commonly used bisphosphonate.
Alendronate all cause mortality
Alendronate is a commonly prescribed medication for osteoporosis, primarily aimed at reducing fracture risk. However, research has also explored its potential impact on all-cause mortality. Here's what we know:
Evidence suggests a potential link between alendronate use and reduced all-cause mortality, particularly in individuals with osteoporosis and a history of fractures. This association may be attributed to several factors:
Fracture prevention: By reducing fractures, alendronate can prevent complications and disability that contribute to mortality. Hip fractures, in particular, are associated with a significant increase in mortality risk.
Potential cardiovascular benefits: Some studies have suggested that alendronate may have a protective effect against cardiovascular disease, a leading cause of death. However, more research is needed to confirm this link.
Anti-inflammatory effects: Alendronate may have anti-inflammatory properties that could contribute to overall health and longevity.
However, it's important to note that:
The evidence is not conclusive. While several studies have shown a positive association, more research is needed to establish a definitive causal link between alendronate and reduced mortality.
Individual factors vary. The impact of alendronate on mortality may differ depending on factors such as age, overall health, and adherence to treatment.
Potential side effects exist. Alendronate can have side effects, including gastrointestinal issues and rare cases of jawbone problems.
Bisphosphonates: Mechanism of Action and Role in Clinical Practice (2009)
Bisphosphonates are the primary pharmacological agents used to treat conditions characterized by excessive osteoclast-mediated bone resorption, such as osteoporosis, Paget's disease, and malignancies metastatic to bone. They work by selectively inhibiting osteoclast activity.
Mechanism of Action:
Bisphosphonates have a high affinity for bone mineral, allowing them to achieve a high local concentration in the skeleton.
Nitrogen-containing bisphosphonates (alendronate, risedronate, ibandronate, pamidronate, zoledronic acid) work by inhibiting farnesyl pyrophosphate synthase, a key enzyme in the mevalonic acid pathway. This disrupts protein prenylation and leads to osteoclast apoptosis.
Non-nitrogen containing bisphosphonates are metabolized to cytotoxic ATP analogues in osteoclasts.
Pharmacology:
Oral bioavailability is low (<1%) due to poor absorption.
50% of absorbed dose is taken up by the skeleton, the rest is excreted unchanged in urine.
Half-life: Alendronate exhibits a notably protracted terminal half-life of approximately 10 years within bone tissues.
Skeletal retention depends on renal function, bone turnover rate, and the specific bisphosphonate. More potent ones have higher skeletal retention.
Oral dosing frequencies have been reduced to once weekly or monthly, which improves adherence compared to daily dosing.
IV formulations (ibandronate, zoledronic acid) allow less frequent dosing. Zoledronic acid has an annual dosing regimen.
Clinical Uses:
Osteoporosis:
Alendronate, risedronate, and zoledronic acid reduce vertebral, hip and non-vertebral fractures in postmenopausal women with osteoporosis. 3-year relative risk reductions:
Vertebral: 41-62%
Hip: 40-51%
Non-vertebral: 20-39%
Ibandronate reduces vertebral fractures only.
Effects are seen within 3 months, before changes in BMD, suggesting anti-fracture efficacy is due to reduction in bone turnover.
Optimal duration of therapy is unclear. Some data suggest therapy can be stopped after 5 years.
Also effective in men and glucocorticoid-induced osteoporosis.
Malignancy:
Reduce skeletal complications, bone pain in breast cancer, prostate cancer, and multiple myeloma. Pamidronate, zoledronic acid and ibandronate are used.
May have adjuvant anti-tumor effects in early stage breast cancer.
Used to prevent bone loss from hormonal therapies like aromatase inhibitors, androgen deprivation.
Adverse Effects:
Osteonecrosis of the jaw: Occurs in 1-10 per 100 oncology patients on high-dose IV therapy, lower risk with oral therapy for osteoporosis (1 in 10,000 to 1 in 100,000 patient-treatment years).
Atrial fibrillation: Slight increase seen with zoledronic acid and possibly alendronate. Mechanism unknown.
Acute phase reaction: Fever, flu-like symptoms in 10-30% after first IV dose.
Hypocalcemia: Can occur especially in patients with high bone turnover, vitamin D deficiency.
Severe musculoskeletal pain: Rare.
Esophageal irritation with oral bisphosphonates.
Renal function deterioration with IV bisphosphonates if underlying renal insufficiency.
Calcium and vitamin D adequacy is important for maximizing the efficacy of bisphosphonate therapy.
In summary, bisphosphonates are highly effective agents for reducing fractures in osteoporosis and skeletal complications of malignancy. Potential adverse effects require judicious patient selection and monitoring. More research is needed on the optimal duration of therapy.
Alendronate (statpearls)
The efficacy of bisphosphonates for prevention of osteoporotic fracture: an update meta-analysis (2017)
An approach “using systematic reviews” on PubMed and Cochrane Library was taken. Twenty-four RCTs investigating the effects of bisphosphonates for the prevention of osteoporotic fracture were included in final analysis. A pairwise meta-analysis was conducted with a random effects model. Subgroup analysis was performed according to the type of bisphosphonate.
The use of bisphosphonate decrease the risk of overall osteoporotic fracture (odds ratio [OR] 0.62; P<0.001), vertebral fracture (OR 0.55; P<0.001) and non-vertebral fracture (OR 0.73; P<0.001). Subgroup analysis indicated that zoledronic acid showed the lowest risk reduction (OR 0.61; P<0.001) for overall osteoporotic fractures but no significance was observed for etidronate (OR 0.34; P=0.127).
This update meta-analysis re-confirmed that bisphosphonate use can effectively reduce the risk of osteoporotic fracture. However, there is a lack of evidence regarding etidronate for the prevention of osteoporotic fracture.
Myelosuppressive Therapies Significantly Increase Pro-Inflammatory Cytokines and Directly Cause Bone Loss (2014)
Hence, myelosuppressive therapies increase inflammation and directly contribute to bone loss. Administration of an osteoclast inhibitor before the initiation of cancer therapy is likely to have the best outcome in preventing bone loss in patients with cancer.
Bisphosphonate Treatment Ameliorates Chemotherapy-Induced Bone and Muscle Abnormalities in Young Mice (2019)
Mice received cisplatin alone or combined with zoledronic acid (ZA; 5 μg/kg), a bisphosphonate routinely used for the treatment of osteoporosis. We found that cisplatin resulted in progressive loss of body weight (−25%), in line with reduced fat (−58%) and lean (−17%) mass. As expected, microCT bone histomorphometry analysis revealed significant reduction in bone mass following administration of chemotherapy, in line with reduced trabecular bone volume (BV/TV) and number (Tb.N), as well as increased trabecular separation (Tb.Sp) in the distal femur. Conversely, trabecular bone was protected when cisplatin was administered in combination with ZA. Interestingly, while the animals exposed to chemotherapy presented significant muscle wasting (~-20% vs. vehicle-treated mice), the administration of ZA in combination with cisplatin resulted in preservation of muscle mass (+12%) and strength (+42%). Altogether, these observations support our hypothesis of bone factors targeting muscle and suggest that pharmacological preservation of bone mass can benefit muscle mass and function following chemotherapy.
Effect of alendronate on muscle mass: Investigation in patients with osteoporosis (2015)
Many osteoporosis drugs reliably increase bone mass in the elderly; if these drugs also had a positive effect on muscle, their benefit would be even greater. We examined the effect of alendronate monotherapy on muscle mass in patients with osteoporosis.
Methods
In this retrospective cohort, case-control study, patients from an osteoporosis database were divided into 2 groups: alendronate-treated patients (group A; n = 199) and a control group receiving no drug treatment (group C; n = 233). Appendicular skeletal muscle mass (ASM) and skeletal muscle mass index (SMI) measured by dual-energy X-ray absorptiometry were assessed at approximately 1 year. The change in muscle mass was compared between the groups.
Results
At baseline, group A included more women and had lower height, weight, bone mineral content, and muscle mass than group C. A comparison of changes after 1 year—adjusted for age, sex, observation period, body mass index and initial values—revealed that the muscle mass in group A showed increases by 0.137 kg/m2 in SMI, 514 g in ASM, and 319 g in lower limb muscle mass (LLM). Group C showed no changes in muscle mass. A significant difference in the amount of change in ASM and LLM was found between the groups after adjustment: 2.5 times and 4.4 times higher, respectively, in groups A and C. However, the difference in SMI disappeared after adjustment.
Conclusions
This is the first study to show that alendronate may have a positive effect not only on bone, but on muscle as well.
Retrospective Study of the Effects of Zoledronic Acid on Muscle Mass in Osteoporosis Patients (2021)
Purpose: Several osteoporosis drugs can continuously improve bone mass, but the impact on muscle mass is still unknown. This study aims to investigate how zoledronic acid monotherapy affected muscle mass in osteoporosis patients.
Patients and Methods: Patients from an osteoporosis database were divided into two groups in this retrospective cohort, case–control study: zoledronic acid-treated patients (n = 113) and a control group without osteoporosis treatment (n = 118). At four years, appendicular skeletal muscle mass (ASM) and appendicular skeletal muscle mass index (ASMI) were calculated using dual-energy X-ray absorptiometry. The differences in muscle mass between the groups were compared.
Results: At baseline, there was no difference in sex, ASM, ASMI, and bone mineral density between the zoledronic acid treatment group and the control group. The treatment group’s skeletal muscle mass increased by 841 g in ASM and 0.35 kg/m2 in ASMI after three years, while decreased in the control group.
Conclusion: This study for the first time demonstrated that that zoledronic acid is beneficial not only to the bone but also to muscle.
Positive effects of bisphosphonates on bone and muscle in a mouse model of Duchenne muscular dystrophy (2016)
We treated growing Mdx mice with pamidronate for 2 weeks.
Pamidronate treatment increased cortical bone mineral density and bone strength.
Pamidronate treatment suppressed trabecular bone remodeling.
Pamidronate treatment improved muscle strength and suppressed serum and muscle creatine kinase levels.
Bisphosphonates attenuate age‐related muscle decline in Caenorhabditis elegans (2023)
Despite lacking an endoskeleton, ZA delays Caenorhabditis elegans sarcopenia, which translates to improved neuromuscular function across the life course. Bisphosphonates might, therefore, be an immediately exploitable anti‐sarcopenia therapy.
Feasibility and Efficacy of Bisphosphonate Use for the Prevention of Bone and Muscle Loss (2022)
Loss of bone and muscle mass often occurs in tandem, increasing the risk of fragility fractures. Whereas many drugs are approved for the treatment of bone loss, there are few treatments available for the concomitant loss of bone and muscle. Identification of a treatment to mitigate pathologic bone and muscle atrophy has the potential to impact countless populations and influence approaches for healthy aging. Bisphosphonates have emerged as a potential treatment for both bone and muscle loss in cellular, murine, and observational human studies. Our findings of modest weight maintenance in postmenopausal women treated with 12-months of risedronate, relative to control, corroborates this evidence, suggesting oral bisphosphonates have the potential to mitigate menopause-related bone and body composition changes. Likewise, our analysis of participants randomized to 6 months of oral bisphosphonate or placebo following sleeve gastrectomy, demonstrated lean mass sparing, particularly at the appendicular sites. These results support the potential use of the medication for populations at high risk of concurrent bone and lean mass loss due to rapid weight loss. We hypothesize our ongoing clinical trial investigating an intravenous bisphosphonate, zoledronic acid, for prevention of bone and muscle loss following sleeve gastrectomy will substantiate our findings and offer an effective therapy for coexistent bone and muscle loss in high-risk groups.
Bisphosphonates (link)
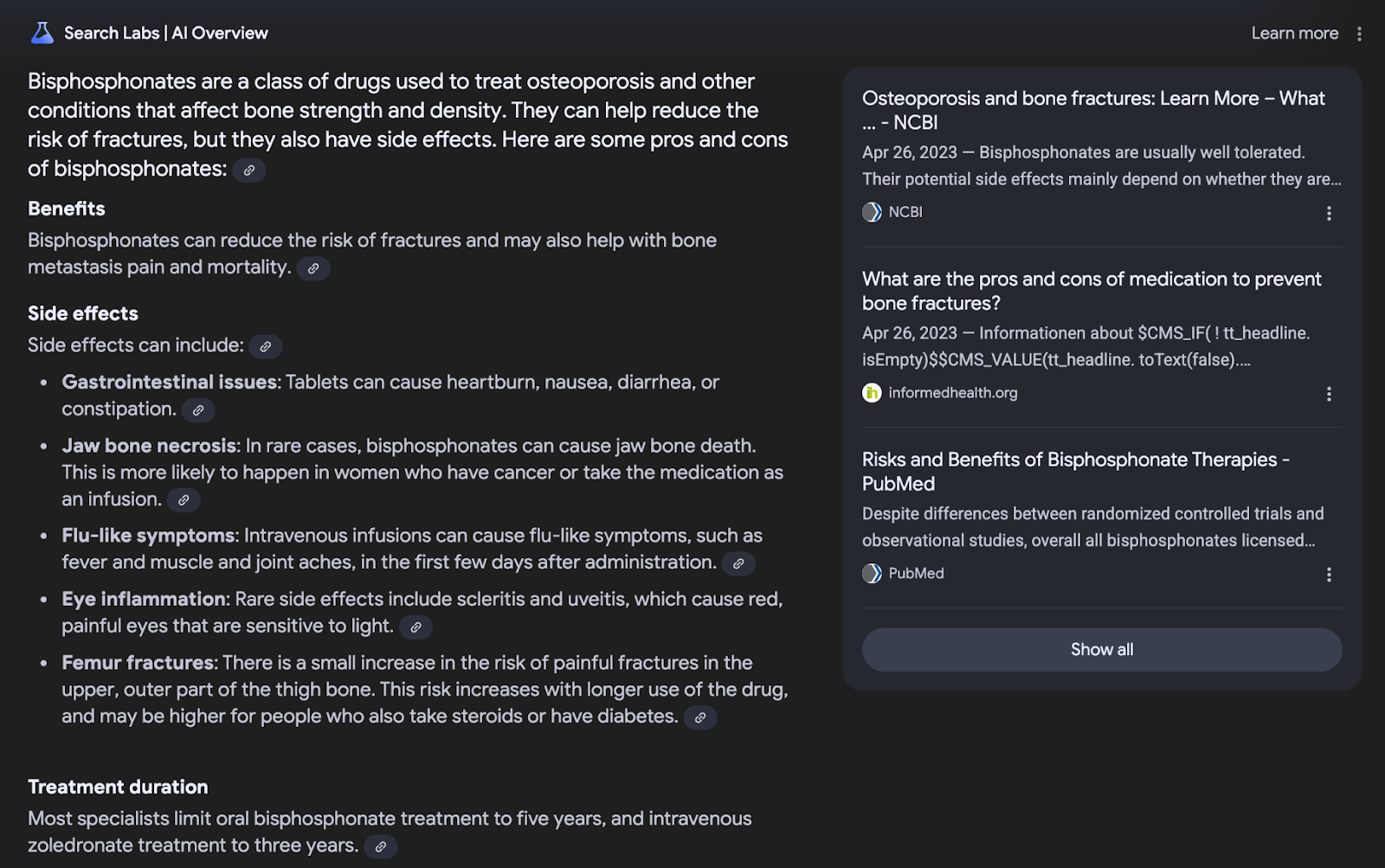
Bisphosphonates are a group of drugs that can be used to help protect bones against the effects of some cancers and to treat some bone conditions. Sometimes bisphosphonates are called bone strengthening or bone hardening treatments.
Bisphosphonates may be used to treat multiple myeloma and bone metastases.
How bisphosphonates work
Bisphosphonates slow down the action of bone cells (osteoclasts) that dissolve small bits of bones to help remodel them and keep them strong. When cancer spreads to the bone (metastasizes), these cells become overactive, causing the bone to be destroyed faster than it’s rebuilt. When this happens, the damage can cause bones to become thinner and weaker causing:
pain in the affected bones
high calcium levels in the blood (hypercalcemia)
an increased risk of bones breaking (fracturing)
Uses of bisphosphonates
Bisphosphonates slow down the breakdown of bones. They may be used to:
reduce bone pain caused by bone metastases or multiple myeloma
reduce high levels of calcium in the blood
help strengthen bone and reduce the risk of breaks caused by cancer, bone metastases or osteoporosis
Bone pain
Most cancers that affect the bones have started in another part of the body and have spread to the bone. The most common types are breast cancer, prostate cancer and lung cancer. Cancer pain is often linked to bone metastases.
Multiple myeloma is a cancer of abnormal plasma cells (a type of white blood cell) that collect in the bone marrow. These abnormal cells make a substance that leads to bone damage and bone pain.
Hypercalcemia
When bone metastases and multiple myeloma cause bones to break down, calcium moves out of the bones and into the bloodstream. This can cause calcium levels in the blood to rise. A high level of calcium in the blood is called hypercalcemia. This can also cause bones to become weak and fragile so that they break easily.
Osteoporosis
A loss of bone mass (or bone density) is called osteoporosis. This condition causes bone to become weak and more likely to break. Some cancer treatments, such as long-term
corticosteroid use, hormonal therapies
and some chemotherapy drugs can increase the risk of osteoporosis. Osteoporosis can also happen because of factors not related to cancer. Bisphosphonates may be used to prevent and treat osteoporosis.
Types of bisphosphonates
The type of bisphosphonate used can depend on the type of cancer being treated. Common bisphosphonates used to treat bone metastases and multiple myeloma include:
clodronate (Bonefos) given by mouth or by an intravenous (IV) infusion (through a vein)
pamidronate (Aredia) given by an IV infusion
zoledronic acid (Zometa) given by an IV infusion
Bisphosphonates used to prevent and treat osteoporosis include alendronate (Fosamax), risedronate (Actonel) and etidronate (Didrocal, Didronel).
Taking bisphosphonates
Bisphosphonates can be taken as pills or by an IV infusion.
Pills are usually taken once or twice per day on an empty stomach.
IV infusions are usually given every 3 to 4 weeks. They can take anywhere from 15 minutes to 4 hours, depending on which bisphosphonate is given. They can be given at the hospital or at home by a homecare nurse.
Follow-up after bisphosphonates
Follow-up when bisphosphonates are given includes:
checking to see if bone pain has lessened
blood chemistry tests to check how the kidney is working and calcium level
Side effects
Side effects can happen with any type of treatment, but everyone’s experience is different. Some people have many side effects. Other people have few or none at all.
If you develop side effects, they can happen any time during, immediately after or a few days or weeks after bisphosphonate therapy. Most side effects go away on their own or can be treated, but some side effects may last a long time or become permanent.
Side effects of bisphosphonate therapy will depend mainly on the type of bisphosphonate, the dose, how the drug is given and your overall health. Tell your healthcare team if you have these side effects or others you think might be from bisphosphonates. The sooner you tell them of any problems, the sooner they can suggest ways to help you deal with them.
The following are some side effects of bisphosphonate therapy.
Fatigue
Fatigue is a general lack of energy and tiredness that can happen during bisphosphonate therapy. Fatigue makes a person feel more tired than usual and can interfere with daily activities and sleep. It tends to be worse when you are also having other treatments, such as chemotherapy or radiation therapy.
Increased bone pain
Sometimes bone pain can temporarily become worse when you first take bisphosphonates. This side effect is often temporary. You may be given stronger pain relievers until this side effect goes away.
Digestive problems
Digestive problems can happen, especially when the bisphosphonate is taken as pills. Digestive problems include:
heartburn
abdominal cramps or pain
Flu-like symptoms
Flu-like symptoms can happen shortly after bisphosphonates are given. They include fever, chills, muscle and joint aches or pain and headaches. These side effects do not usually happen and are often temporary. They are more likely to happen after bisphosphonates are given by an IV infusion.
Low calcium levels
Bisphosphonates can lower blood calcium to below normal levels. This side effect does not usually happen and is often temporary. Calcium levels in the blood are often checked when you are given bisphosphonates.
Change in how the kidney works
Bisphosphonates can affect how the kidney works. It does not often cause any symptoms. Blood tests to check the kidney are done while you are taking bisphosphonates.
Osteonecrosis
Osteonecrosis is the death of bone caused by poor blood supply to the area. Osteonecrosis of the jaw bone underneath the teeth is a rare side effect of some bisphosphonates if they are taken for over a year. It is sometimes seen when a tooth is pulled in someone who is taking bisphosphonates. Osteonecrosis is not usually seen in people who take bisphosphonates as pills.
Osteonecrosis can cause loosening of the teeth and tooth loss and infection or open sores of the jaw bone that don’t heal. These sores are often hard to treat.
You may be advised by your doctor to get a dental check-up and have tooth or jaw problems treated before starting to take bisphosphonates. Maintaining good oral hygiene, making sure your dentures are well fitted and having regular dental check-ups might help prevent osteonecrosis of the jaw.
Bisphosphonates for cardiovascular risk reduction: a systematic review and meta-analysis (2016)
Pubmed, Embase and the Cochrane Library were systematically reviewed by two independent investigators for randomized controlled studies published up to January 2016, in which the effect of bisphosphonates on arterial wall disease, cardiovascular events, cardiovascular mortality or all-cause mortality were reported. There was no restriction for the type of population used in the trials. Random-effects models were used to calculate the pooled estimates.
61 trials reporting the effects of bisphosphonates on the outcomes of interest were included. Bisphosphonates had beneficial effects on arterial wall disease regarding arterial calcification (pooled mean percentage difference of 2 trials −11.52 (95% CI -16.51 to −6.52, p < 0.01, I2 13%), but not on arterial stiffness (pooled mean percentage difference of 2 trials −2.82; 95% CI -10.71–5.07; p = 0.48, I2 59%). No effect of bisphosphonate treatment on cardiovascular events was found (pooled RR of 20 trials 1.03; 95% CI 0.91–1.17, I2 16%), while a lower risk for cardiovascular mortality was observed in patients treated with bisphosphonates (pooled RR of 10 trials 0.81; 95% CI 0.64–1.02; I2 0%) although not statistically significant. Patients treated with bisphosphonates had a reduced risk of all-cause mortality (pooled RR of 48 trials 0.90; 95% CI 0.84–0.98; I2 53%).
Conclusions
In this systematic review and meta-analysis it is shown that bisphosphonates reduce arterial wall calcification but have no effect on arterial stiffness or on cardiovascular events. Bisphosphonates tend to reduce the risk of cardiovascular mortality and reduce all-cause mortality in various patient groups, including osteoporosis and cancer patients.
Cardiovascular Safety and Effectiveness of Bisphosphonates: From Intervention Trials to Real-Life Data (2022)
Introduction and Epidemiology:
Osteoporosis with fragility fractures and cardiovascular diseases (CVDs) are rapidly increasing worldwide, especially in the elderly population.
In Europe in 2015, 15.8 million women and 4.2 million men had osteoporosis. In 2017, there were an estimated 2.7 million fragility fractures in Europe.
The number of fragility fractures in Europe is projected to rise 23.3% from 2.7 million in 2017 to 3.3 million in 2030.
The lifetime risk of hip fracture at age 50 is comparable to the lifetime risk of stroke - around 20% for women and 14% for men in Europe. The lifetime risk of major osteoporotic fracture is similar to that of CVD.
Common risk factors and pathophysiological mechanisms may link osteoporosis and CVDs.
Cardiovascular Morbidity and Mortality After Fragility Fractures:
The risk of cardiovascular events is increased after fragility fractures, especially hip fractures. Hip fracture is independently associated with a 29% higher risk of myocardial infarction (Chiang et al. 2013) and a 1.55 times higher risk of stroke in the following year (Kang et al. 2011).
Mortality risk remains high for up to 9 months after a hip fracture, with cardiovascular diseases being a major cause of death (Cameron et al. 2010).
In the year after a first fracture, mortality risk is over 3-fold higher compared to the general population. Major causes of death are neoplasms, respiratory diseases and cardiovascular diseases (Klop et al. 2017).
Conversely, women with cardiovascular disease have an increased risk of fragility fractures (Chen et al. 2011).
Bisphosphonates in Fracture Prevention:
Bisphosphonates are the most widely used osteoporosis medications. Alendronate, risedronate, ibandronate and zoledronic acid are the most common.
Alendronate reduces vertebral fractures by 50% and non-vertebral fractures by 50% in women with prevalent vertebral fractures (Black et al. 1996, Cummings et al. 1998). It reduces hip fracture risk by 34% in the oldest old patients (Axelsson et al. 2017).
Risedronate reduces vertebral fractures by 40-50%, non-vertebral fractures by 30-36%, and hip fractures by 30%, especially in women age 70-79 (Harris et al. 1999, Reginster et al. 2000, McClung et al. 2001).
Oral ibandronate reduces vertebral fractures by 50-60% (Reginster et al. 2006).
Yearly IV zoledronic acid reduces vertebral fractures by 70% and hip fractures by 40% in postmenopausal women (Black et al. 2007). It also reduces fracture risk when given shortly after a hip fracture in both sexes (Lyles et al. 2007).
Despite the ability of bisphosphonates to reduce fracture risk, only around 20% of patients with a fragility fracture receive proper osteoporosis treatment. Adherence to oral bisphosphonates is low.
Bisphosphonates and Mortality:
Some studies suggest bisphosphonates may reduce mortality in addition to fracture risk, but evidence is mixed.
The HORIZON-Recurrent Fracture Trial found yearly IV zoledronic acid after a hip fracture reduced deaths by 28% over a median 1.9 year follow-up, in addition to reducing new fractures by 35% (Lyles et al. 2007).
A meta-analysis of 8 trials up to 2008 found antiresorptive treatments reduced mortality by 11% in frail older adults at high fracture risk, with a similar mortality benefit when restricted to just bisphosphonates (Bolland et al. 2010).
Many observational studies show lower mortality rates with bisphosphonate use, especially after hip fracture (Brozek et al. 2016, Beaupre et al. 2011, Sambrook et al. 2011).
However, a recent meta-analysis of 27 trials with over 56,000 participants concluded there was no significant association between bisphosphonates and overall mortality (Cummings et al. 2019).
While there is insufficient evidence to recommend bisphosphonates solely to increase lifespan, the data provides reassurance that mortality is not increased with these medications.
Bisphosphonates and Cardiovascular Disease:
Preclinical animal studies suggest bisphosphonates may reduce atherosclerotic plaques, improve arterial elasticity, and decrease vascular resistance and intimal thickness. Potential mechanisms include FPPS inhibition attenuating cardiac hypertrophy and decreasing γδ T-cells that promote atherosclerosis.
However, these studies used higher bisphosphonate doses than used in humans for osteoporosis. Clinical trial and real-world evidence is needed to determine effects on cardiovascular disease.
Post-hoc analyses of the HORIZON-PFT trial found yearly IV zoledronate did not affect progression of abdominal aortic calcification over 3 years (Cai et al. 2020).
Observational studies show mixed results on whether bisphosphonates affect vascular calcification. A meta-analysis of 61 trials found bisphosphonates may reduce arterial calcification but not stiffness (Kranenburg et al. 2016).
In a retrospective cohort study, alendronate use after hip fracture was associated with lower cardiovascular mortality and incident myocardial infarction at 1 year and longer-term (Sing et al. 2018). This was also seen for other nitrogen-containing bisphosphonates.
In the 10-year prospective Odense Bisphosphonate Safety Study, bisphosphonate users had a 33% lower risk of cardiovascular events compared to matched controls (Rodríguez et al. 2020).
An Italian cohort study of over 82,000 elderly bisphosphonate users found high adherence (>80% proportion of days covered) was associated with a lower risk of hospitalization for atherosclerotic cardiovascular events, with a hazard ratio of 0.75 (Casula et al. 2020).
In a post-hoc analysis of an RCT, IV zoledronate every 18 months in older osteopenic women resulted in fewer cardiovascular events compared to placebo (Reid et al. 2020).
Bisphosphonates and Atrial Fibrillation:
Some evidence suggests bisphosphonates, especially IV zoledronic acid, may increase risk of atrial fibrillation, but data are conflicting.
This concern arose from post-hoc analyses of the HORIZON-PFT trial showing a higher atrial fibrillation rate with yearly IV zoledronate (6.9% vs 5.3% with placebo) (Black et al. 2007). Re-analysis of the FIT trial also showed higher atrial fibrillation risk with alendronate.
However, no increased atrial fibrillation risk was seen in trials of risedronate or the HORIZON-RFT trial of zoledronate after hip fracture.
Most case-control studies have found no increased atrial fibrillation risk with bisphosphonates overall. Results are conflicting between meta-analyses and observational studies.
Given the inconsistent evidence, caution is still advised in using bisphosphonates in patients at high risk for atrial fibrillation. Other osteoporosis medications can be considered in this population.
Conclusions:
Observational data suggest bisphosphonate users may have lower mortality, delayed vascular calcification progression, and lower atherosclerotic burden. However, discrepancies exist between meta-analyses of RCTs and observational studies on cardiovascular benefits of bisphosphonates.
There is currently insufficient evidence to recommend bisphosphonates to reduce cardiovascular mortality or morbidity. Fracture prevention remains the main indication.
Osteoporosis guidelines do not specifically address cardiovascular safety of bisphosphonates, especially in patients with concomitant cardiovascular disease.
Despite conflicting data, bisphosphonates should be used cautiously in patients at high atrial fibrillation risk.
The antifracture benefits of bisphosphonates outweigh potential risks in patients with bone fragility. Treating osteoporosis should be prioritized given the morbidity and mortality associated with fractures.
In summary, while bisphosphonates are not currently recommended solely for cardioprotection, they appear to be safe in patients with cardiovascular disease and may even provide some cardiovascular benefits, though more research is needed. Concerns about atrial fibrillation risk remain with IV bisphosphonates in particular. Overall, the fracture prevention effects of bisphosphonates provide a net benefit in patients with osteoporosis despite potential cardiovascular risks. Optimizing treatment of this large and growing population is important to reduce the burden of fractures and their consequences.
Alendronate all cause mortality
Association Between Drug Treatments for Patients With Osteoporosis and Overall Mortality Rates: A Meta Analysis (2019)
Main Outcomes and Measures
Associations of all drug treatments, particularly bisphosphonate and zoledronate treatments, with overall mortality.
Results
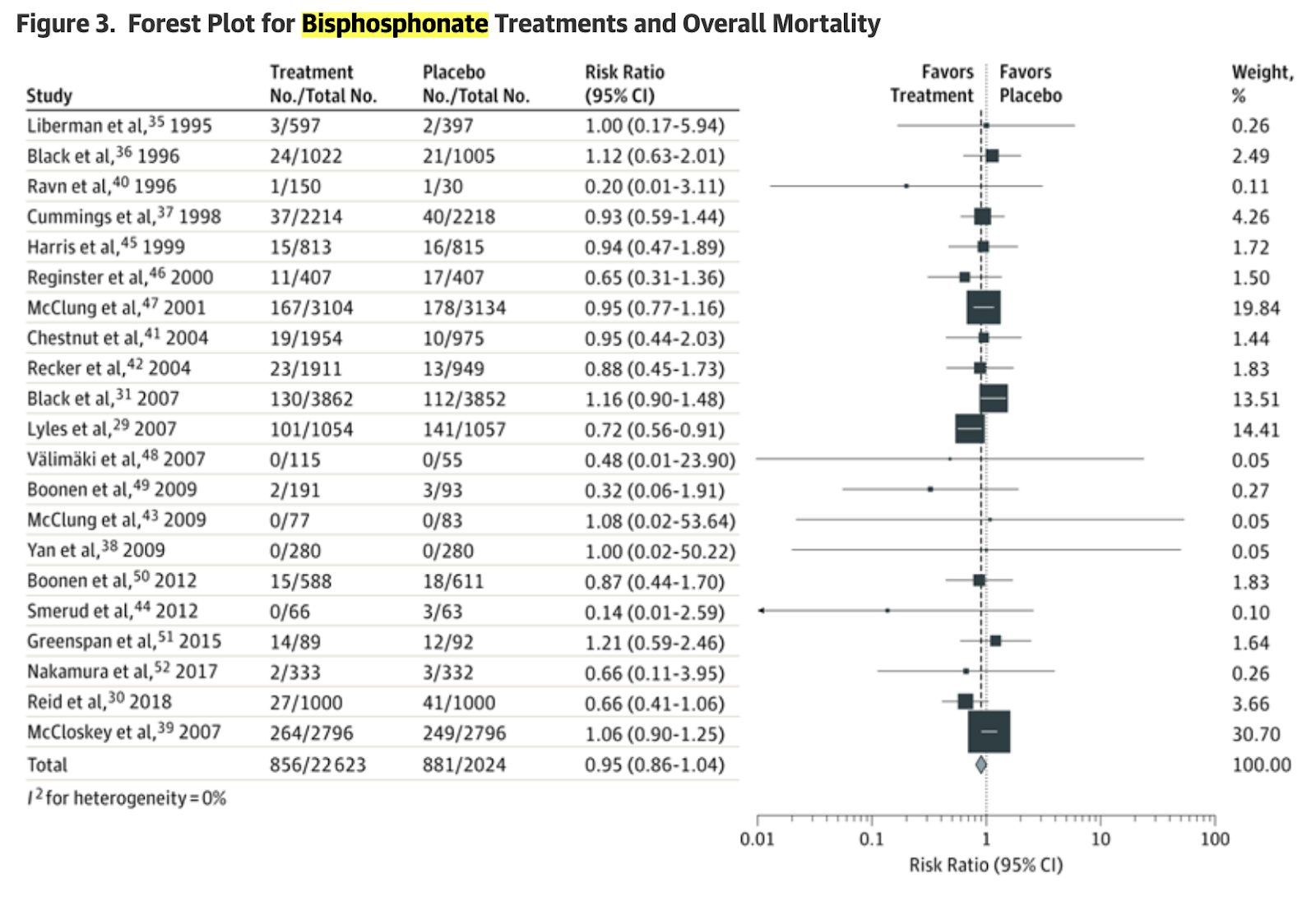
Of 38 clinical trials that included 101 642 unique participants, 38 were included in the meta-analyses of all drug treatments (45 594 participants randomized to placebo; 56 048 to treatment); 21 clinical trials, of bisphosphonate treatments (20 244 participants randomized to placebo; 22 623 to treatment); and 6 clinical trials, of zoledronate treatments (6944 participants randomized to placebo; 6926 to treatment). No significant association was found between all drug treatments for osteoporosis and overall mortality rate (risk ratio [RR], 0.98; 95% CI, 0.91-1.05; I2 = 0%). Clinical trials of bisphosphonate treatment (RR, 0.95; 95% CI, 0.86-1.04) showed no significant association with overall mortality. Also, clinical trials of zoledronate treatment (RR, 0.88; 95% CI, 0.68-1.13) showed no association with overall mortality rate; however, evidence existed for heterogeneity of the results (I2 = 48.2%).
Conclusions and Relevance
Results of this meta-analysis suggest that bisphosphonate treatment may not be associated with reduced overall mortality rates in addition to decreased fracture risk and should only be recommended to reduce fracture risk. Additional trials are needed to clarify whether treatment with zoledronate reduces mortality rates.
—----------
The purpose of treating patients with medications for osteoporosis is to reduce the risk of fracture and the subsequent pain and disability.1-3 Preventing fractures may also lessen the increased risk of mortality owing to fractures. Hip and vertebral fractures are often followed by increased overall mortality,4-12 and some studies have reported that most types of fractures are associated with increased mortality.12-15 However, much of the increased risk for both fracture and mortality may be owing to the patients’ poor health or other factors; thus, it is not clear whether or to what degree mortality following fractures could be reduced by preventing fractures.16-18 Studies have estimated that less than 30% of the mortality following hip and vertebral fractures may be attributed to the fracture itself and, therefore, potentially avoidable by preventing the fracture.19,20
Some studies have suggested that treatments for osteoporosis may directly reduce overall mortality rates in addition to decreasing fracture risk. Several observational studies have reported that patients with osteoporosis who have received drug treatments, particularly bisphosphonates (largely oral versions, such as alendronate sodium), experienced 25% to 60% lower overall mortality that is too large to be attributed to a reduction in fractures and may have been owing to the direct effect of the drug treatments. This substantially lower overall mortality rate has been reported among patients with several different characteristics, including those living in communities,21 living in institutional care,22 admitted to intensive care units,23 prescribed treatments after a fracture,23-25 or receiving treatments from a fracture liaison service as part of an osteoporosis management program.26,27 It seems unlikely that bisphosphonate treatments substantially reduce all-cause mortality in addition to reducing fracture risk because these drugs bind almost exclusively to bone, are cleared from the blood to extremely low or undetectable levels within 24 hours of administration, and are only detectable in extremely low concentrations in tissues other than bone.28 Although the association between drug treatments for osteoporosis and reduced mortality rates remained significant after adjusting for several potential confounders and matching propensity scores, it is possible that these associations were owing to other confounding factors that were not measured; for example, those who took drug treatments for the prevention of fracture may have had better health and nutrition, exercised more frequently, or used other preventive measures more often than those who did not.
Two randomized placebo-controlled clinical trials of zoledronate therapy suggested that patients randomized to receive zoledronate treatment experienced benefits beyond fracture prevention. One randomized clinical trial reported a statistically significant 28% lower mortality rate in patients who had a recent hip fracture.29 A recent, 6-year clinical trial of zoledronate treatment administered to older women without osteoporosis reported significant reductions in the risk of myocardial infarction and breast cancer, with a 35% lower mortality rate that was not statistically significant.30 In contrast, a larger randomized clinical trial of zoledronate treatment administered to women with osteoporosis noted no effect on mortality rate.31
A 2010 meta-analysis of clinical trials of antiresorptive drugs, including bisphosphonates, reported that those treatments reduced overall mortality by 10%.32 Another meta-analysis of 61 clinical trials of bisphosphonate treatments reported a 10% lower overall mortality rate; however, most of the studies were of patients with cancer, for whom it is known that bisphosphonate therapy reduces metastases to bone, and many of the clinical trials were not placebo-controlled.33
If drug therapies for patients with osteoporosis, particularly treatments with bisphosphonates or zoledronate, substantially reduce mortality in addition to decreasing fractures, it may be worthwhile to administer these treatments to almost all older adults, regardless of their fracture risk. Therefore, we conducted a systematic review and meta-analysis of randomized placebo-controlled clinical trials of drug treatments for osteoporosis to evaluate whether these treatments reduced overall mortality. We specifically tested the hypothesis that treatment with bisphosphonates or zoledronate reduces the overall mortality rate.
—-----
Bisphosphonates and mortality: confounding in observational studies? (2019)
Methods
This was a retrospective cohort study of hip fracture patients discharged from Swedish hospitals between 1 July 2006 and 31 December 2015. The data covered 260,574 hip fracture patients and were obtained from the Swedish Hip Fracture Register and national registers. Of the 260,574 patients, 49,765 met all eligibility criteria and 10,178 were pair matched (bisphosphonate users to controls) using time-dependent propensity scores. The matching variables were age, sex, diagnoses, prescription medications, type of hip fracture, type of surgical procedure, known or suspected dementia, and physical functioning status.
Results
Over a median follow-up of 2.8 years, 2922 of the 10,178 matched patients died. The mortality rate was 7.9 deaths per 100 person-years in bisphosphonate users and 9.4 deaths in controls, which corresponded to a 15% lower mortality rate in bisphosphonate users (hazard ratio 0.85, 95% confidence interval 0.79–0.91). The risk of death was lower in bisphosphonate users from day 6 of treatment, although the association was not significant until the second week.
Conclusion
Bisphosphonate use was associated with lower mortality within days of treatment initiation. This finding is consistent with confounding, although an early treatment effect cannot be ruled out.
Bisphosphonates Reduce All-Cause Mortality in Women and Men (medscape)
Study Details:
Study type: Prospective epidemiological cohort study (Canadian Multicentre Osteoporosis study - CaMos)
Presented at: American Society for Bone and Mineral Research 2016 Annual Meeting
Lead researcher: Dana Bliuc, PhD, Garvan Institute of Medical Research, Sydney, Australia
Participants: Women and men aged 50 years and older, enrolled between 1995 and 2012
Key Numerical Findings:
Cohort composition:
2,173 bisphosphonate users
1,265 female hormone-replacement-therapy (HRT) users (as a healthy-user group)
1,889 participants not receiving any treatment
Baseline characteristics:
35% of women in the bisphosphonate group had experienced a prior fracture
17% in the HRT group had experienced a prior fracture
Mortality risk reduction in women:
42% reduction among current bisphosphonate users
47% reduction in past bisphosphonate users
No effect on mortality risk with HRT use
Mortality risk reduction in men:
30% reduction among current bisphosphonate users
Fracture cohort analysis (women only):
Overall 35% reduction in mortality risk with bisphosphonate use
Alendronate: approximately 45% reduction in mortality risk
Risedronate: nonsignificant reduction of about 20%
Etidronate: no reduction in mortality risk
Treatment duration:
On average, participants took alendronate for about 5 years
The study concluded that bisphosphonate use, particularly alendronate, was associated with a significant reduction in all-cause mortality in both women and men, even after adjusting for important baseline variables. This protective effect was not related to a decline in subsequent fractures.
Reduced All-Cause Mortality With Bisphosphonates Among Post-Fracture Osteoporosis Patients: A Nationwide Study and Systematic Review
Patients diagnosed with osteoporosis who had been hospitalized for major fractures were identified from Taiwan's National Health Insurance Research Database 2008-2017 and followed until 2018. There were 24,390 new bisphosphonate users who were classified and compared with 76,725 nonusers of anti-osteoporosis medications in terms of survival outcomes using Cox model analysis. An inverse probability of treatment weighted Cox model and landmark analyses for minimizing immortal time bias were also performed. Bisphosphonate users vs. nonusers had a significantly lower mortality risk, regardless of fracture site (hazard ratios (95% confidence intervals) for patients with any major fracture, hip fracture, and vertebral fracture: 0.90 (0.88, 0.93), 0.83 (0.80, 0.86), and 0.86 (0.82, 0.89), respectively). Compared with nonuse, zoledronic acid (0.77 (0.73, 0.82)) was associated with the lowest mortality, followed by ibandronate (0.85 (0.78, 0.93)) and alendronate/risedronate (0.93 (0.91, 0.96)). Using bisphosphonates for ≥ 3 years had lower mortality (0.60 (0.53, 0.67)) than using bisphosphonates for < 3 years (0.98 (0.95, 1.01)). Intravenous bisphosphonates had a lower mortality than that of oral bisphosphonates. Our results are consistent with the systematic review findings among real-world populations. In conclusion, bisphosphonate use, especially persistence to intravenous bisphosphonates (e.g., zoledronic acid), may reduce post-fracture mortality among patients with osteoporosis, particularly those with hip/vertebral fractures. This supports the rational use of bisphosphonates in post-fracture care.
Long-Term Safety of Bisphosphonates (2005)
Bisphosphonates are widely used to treat osteoporosis. They reduce the incidence of new fractures in patients with established osteoporosis (1, 2). In women with osteopenia, bisphosphonates prevent bone loss, and physicians prescribe them with the hope of preventing future fractures. These medications have profound effects on bone physiology, but the long-term consequences remain unknown. The longest duration of placebo-controlled trials is 6 yr; subjects in observational studies have used the newer amino-bisphosphonates for 10 yr. Some unadvertised aspects of bisphosphonates, including their long half-life and their effects on bone physiology, are not well recognized.
Unlike most medications, bisphosphonates remain in the body for decades. These drugs are not metabolized, but are either excreted renally or deposited within the bones. The amount of drug within the bone will accumulate with use. There is no known method of removing the medication from the bones. The duration of physiological effect is still unknown. After taking alendronate for 5 yr, the bone resorption and formation markers remain suppressed for at least 5 yr after discontinuation (3).
Pros and cons of bisphosphonates
Are there any serious side effects?
In very rare cases, bisphosphonates cause the jaw bone – or parts of the jaw bone – to die (necrosis). It is estimated that up to 3 out of 10,000 women could develop this side effect after many years of treatment. Necrosis of the jaw bone is thought to be more likely in women who have cancer and those who are given the medication as an infusion.
A randomized trial of alendronate as prophylaxis against loss in bone mineral density following lymphoma treatment (2022)
Oral alendronate is a safe and effective primary prophylaxis against loss in bone mineral density in lymphoma patients.
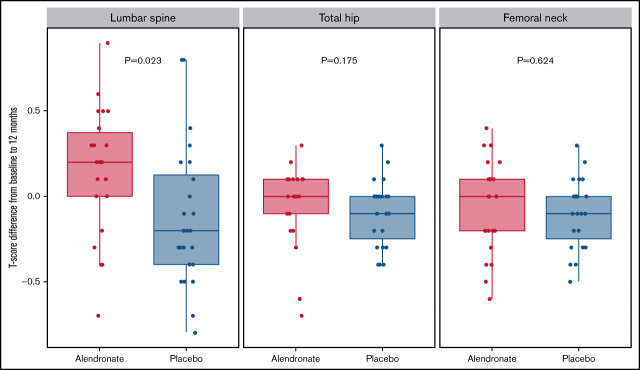
Lymphoma patients often receive high glucocorticoid doses as part of standard therapy. Observational studies have shown a substantial risk of glucocorticoid-induced osteoporosis (GIO) with associated fractures. The aim of the SIESTA trial was to determine if oral alendronate (ALN) is a safe and effective prophylaxis against GIO in lymphoma. SIESTA was a single-center, randomized, double-blinded, phase 2 study of lymphoma patients planned for glucocorticoid-containing chemotherapy. After randomization, patients received weekly ALN 70 mg or placebo for a total of 52 weeks. Bone mineral density (BMD) was assessed at baseline, after completion of chemotherapy (end of treatment [EOT]) (4 to 6 months), and at the end of the study (EOS) (12 months). Vertebral fracture and biomarkers were assessed at baseline and EOS. Patients with baseline BMD assessment and at least 1 follow-up BMD assessment were analyzed for efficacy. The primary endpoint was a change in lumbar spine T-score from baseline to EOS. Of the 59 patients enrolled, 23 of 30 in the ALN arm and 24 of 29 in the placebo arm were analyzed for efficacy. The mean change in T-score from baseline to 12 months at the lumbar spine was +0.15 for ALN and -0.12 for placebo (P = .023). The difference in ΔTEOS between the ALN and placebo groups was larger among females (ALN 0.28; placebo -0.28; P = .01). Biomarker analyses confirmed reduced bone resorption in ALN-treated patients. In conclusion, ALN is a safe and effective primary prophylaxis against loss in BMD following glucocorticoid-containing chemotherapy. Despite reduced BMD loss in the ALN arm, the treatment did not influence fracture risk in this small cohort of patients.
Bisphosphonates for myeloma (link)
Bisphosphonates are drugs that are used to strengthen and protect the bones in various conditions, including myeloma. Studies have shown that regular treatment with bisphosphonates significantly reduces myeloma bone disease and the risk of spontaneous fractures in patients with myeloma, improving mobility and quality of life and reducing the incidence of pain. Bisphosphonates work by inhibiting and destroying osteoclasts, thereby reducing the breakdown of bone, increasing bone density and preventing factures and hypercalcaemia.
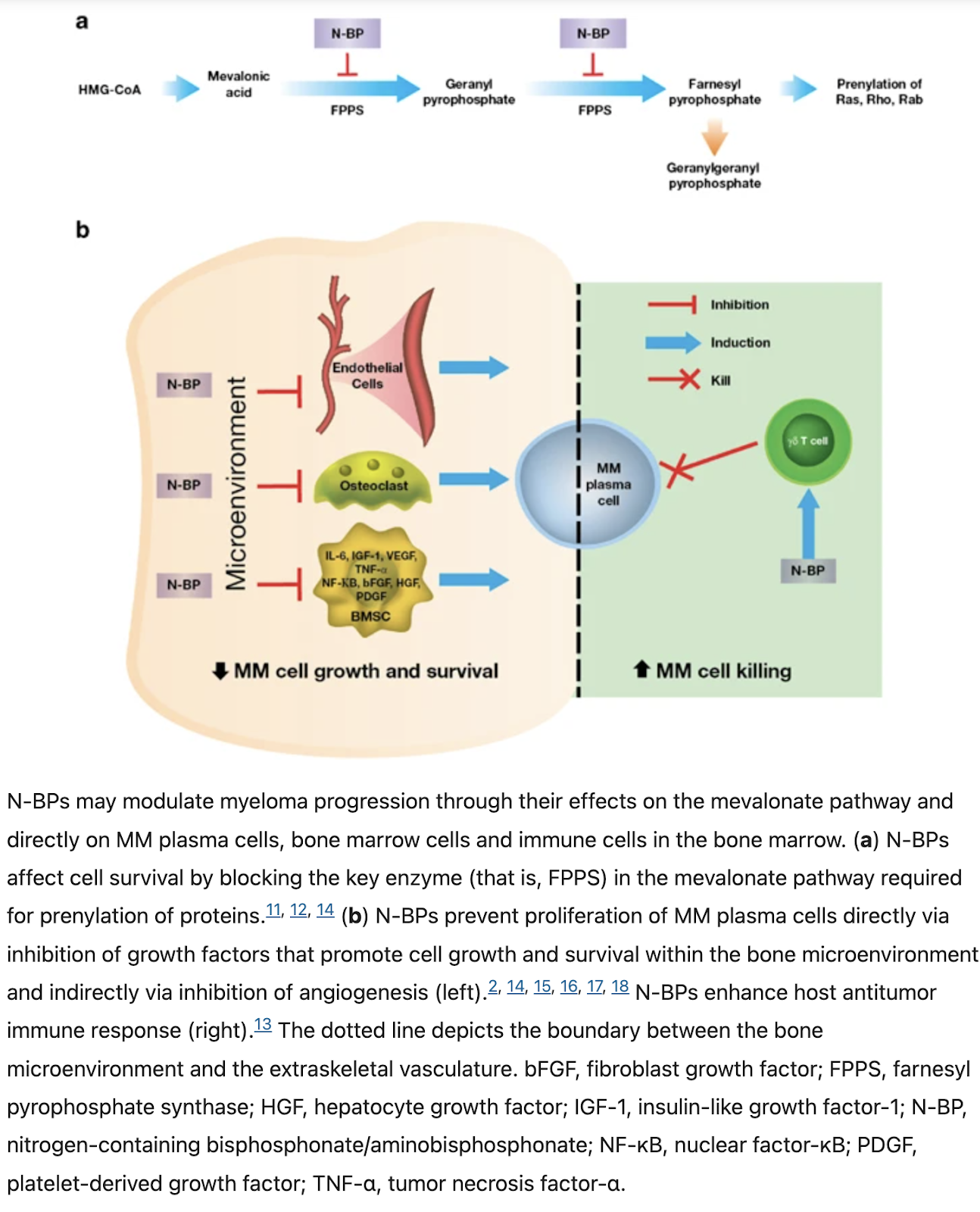
Bisphosphonates as anti-myeloma drugs (2011)
Bisphosphonates (BPs), especially newer generation nitrogen-containing BPs (N-BPs) like zoledronic acid and pamidronate, inhibit bone resorption by inducing osteoclast apoptosis and disrupting the osteoclast cytoskeleton. This occurs through inhibition of the enzyme farnesyl pyrophosphate synthase (FPPS) in the mevalonate pathway, impairing post-translational prenylation of small GTPases involved in cell signaling (Modi & Lentzsch, 2012).
However, preclinical evidence suggests BPs may also have direct and indirect anti-myeloma effects beyond just inhibiting bone resorption:
Direct effects on myeloma cells: In vitro studies show BPs, especially N-BPs like zoledronic acid, can induce apoptosis and inhibit proliferation of myeloma cell lines. This occurs through inhibition of the mevalonate pathway, leading to accumulation of isopentenyl pyrophosphate (IPP) and ApppI that have cytotoxic effects. Combining BPs with dexamethasone, thalidomide or simvastatin synergistically enhanced apoptosis of myeloma cells (Modi & Lentzsch, 2012).
Disrupting the bone marrow microenvironment: BPs may indirectly inhibit myeloma progression by preventing bone resorption which releases growth factors and cytokines that stimulate tumor growth. BPs also reduce angiogenesis and inhibit adhesion of myeloma cells to bone marrow stromal cells (Modi & Lentzsch, 2012).
Immunomodulatory effects: BPs stimulate host anti-tumor immunity by activating gamma-delta T cells through IPP accumulation. BPs also revert tumor-associated macrophages from an M2 pro-tumoral to an M1 anti-tumoral phenotype, reducing their pro-angiogenic activity (Modi & Lentzsch, 2012).
Emerging clinical evidence supports an anti-myeloma effect of BPs:
In a trial by Aviles et al (2007) of newly diagnosed myeloma patients, adding zoledronic acid to chemotherapy significantly improved 5-year event-free survival (80% vs 52%) and overall survival (80% vs 46%) compared to chemotherapy alone (Modi & Lentzsch, 2012).
The MRC Myeloma IX trial (Morgan et al, 2010) in newly diagnosed patients (n=1960) found zoledronic acid significantly prolonged overall survival (p=0.0118) and progression-free survival (p=0.0179) vs the BP clodronate. The OS benefit occurred independently of anti-myeloma response. Zoledronic acid also significantly reduced skeletal-related events (27.0% vs 35.3%, p=0.0004) (Modi & Lentzsch, 2012).
However, some studies found no mortality benefit of BPs in unselected myeloma patients overall, though subgroup analyses showed survival advantages in some cases, e.g. patients without baseline vertebral fractures (McCloskey et al, 2001). An updated meta-analysis of ~3000 patients found no significant survival benefit with BPs, but included various BPs of differing potency (Modi & Lentzsch, 2012).
In conclusion, preclinical data provide strong evidence that N-BPs like zoledronic acid have anti-myeloma effects through direct cytotoxicity on tumor cells, disrupting the tumor-promoting bone microenvironment, and stimulating host immunity. Emerging clinical trial data, especially with zoledronic acid, suggest an anti-myeloma and survival benefit, but results have been mixed potentially due to differences in BPs used and patient populations. Further clinical studies are warranted evaluating potent BPs like zoledronic acid in combination with modern anti-myeloma therapies. Optimizing BP use in myeloma must balance their potential anti-myeloma benefits with risks like osteonecrosis of the jaw (Modi & Lentzsch, 2012).
The use of bisphosphonates in multiple myeloma: recommendations of an expert panel on behalf of the European Myeloma Network (2009)
Background
Bisphosphonates (BPs) prevent, reduce, and delay multiple myeloma (MM)-related skeletal complications. Intravenous pamidronate and zoledronic acid, and oral clodronate are used for the management of MM bone disease. The purpose of this paper is to review the current evidence for the use of BPs in MM and provide European Union-specific recommendations to support the clinical practice of treating myeloma bone disease.
Design and methods
An interdisciplinary, expert panel of specialists on MM and myeloma-related bone disease convened for a face-to-face meeting to review and assess the evidence and develop the recommendations. The panel reviewed and graded the evidence available from randomized clinical trials, clinical practice guidelines, and the body of published literature. Where published data were weak or unavailable, the panel used their own clinical experience to put forward recommendations based solely on their expert opinions.
Results
The panel recommends the use of BPs in MM patients suffering from lytic bone disease or severe osteoporosis. Intravenous administration may be preferable; however, oral administration can be considered for patients unable to make hospital visits. Dosing should follow approved indications with adjustments if necessary. In general, BPs are well tolerated, but preventive steps should be taken to avoid renal impairment and osteonecrosis of the jaw (ONJ). The panel agrees that BPs should be given for 2 years, but this may be extended if there is evidence of active myeloma bone disease. Initial therapy of ONJ should include discontinuation of BPs until healing occurs. BPs should be restarted if there is disease progression.
Conclusions
BPs are an essential component of MM therapy for minimizing skeletal morbidity. Recent retrospective data indicate that a modified dosing regimen and preventive measures can greatly reduce the incidence of ONJ.
Bisphosphonate therapy for the treatment of osteoporosis (great link!)
Bisphosphonates work by being absorbed in areas of the body where there is a lot of bone remodelling. This interferes with the remodelling process, so may reduce the risk of breast cancer spreading to the bones and elsewhere in the body. From Bisphosphonates for primary breast cancer
Adjuvant bisphosphonate treatment in early breast cancer: meta-analyses of individual patient data from randomised trials (2015)
Findings
We received data on 18 766 women (18 206 [97%] in trials of 2–5 years of bisphosphonate) with median follow-up 5·6 woman-years, 3453 first recurrences, and 2106 subsequent deaths. Overall, the reductions in recurrence (RR 0·94, 95% CI 0·87–1·01; 2p=0·08), distant recurrence (0·92, 0·85–0·99; 2p=0·03), and breast cancer mortality (0·91, 0·83–0·99; 2p=0·04) were of only borderline significance, but the reduction in bone recurrence was more definite (0·83, 0·73–0·94; 2p=0·004). Among premenopausal women, treatment had no apparent effect on any outcome, but among 11 767 postmenopausal women it produced highly significant reductions in recurrence (RR 0·86, 95% CI 0·78–0·94; 2p=0·002), distant recurrence (0·82, 0·74–0·92; 2p=0·0003), bone recurrence (0·72, 0·60–0·86; 2p=0·0002), and breast cancer mortality (0·82, 0·73–0·93; 2p=0·002). Even for bone recurrence, however, the heterogeneity of benefit was barely significant by menopausal status (2p=0·06 for trend with menopausal status) or age (2p=0·03), and it was non-significant by bisphosphonate class, treatment schedule, oestrogen receptor status, nodes, tumour grade, or concomitant chemotherapy. No differences were seen in non-breast cancer mortality. Bone fractures were reduced (RR 0·85, 95% CI 0·75–0·97; 2p=0·02).
Interpretation
Adjuvant bisphosphonates reduce the rate of breast cancer recurrence in the bone and improve breast cancer survival, but there is definite benefit only in women who were postmenopausal when treatment began.
Acute myeloid leukemia (AML)
The third-generation bisphosphonate zoledronic acid (ZOL) has been shown to be cytotoxic against AML cell lines. (2007)
Adjuvant bisphosphonate treatment in early breast cancer: meta-analyses of individual patient data from randomised trials (2015)
Bisphosphonates have profound effects on bone physiology, and could modify the process of metastasis. We undertook collaborative meta-analyses to clarify the risks and benefits of adjuvant bisphosphonate treatment in breast cancer.
We sought individual patient data from all unconfounded trials in early breast cancer that randomised between bisphosphonate and control. Primary outcomes were recurrence, distant recurrence, and breast cancer mortality. Primary subgroup investigations were site of first distant recurrence (bone or other), menopausal status (postmenopausal [combining natural and artificial] or not), and bisphosphonate class (aminobisphosphonate [eg, zoledronic acid, ibandronate, pamidronate] or other [ie, clodronate]). Intention-to-treat log-rank methods yielded bisphosphonate versus control first-event rate ratios (RRs).
We received data on 18 766 women (18 206 [97%] in trials of 2–5 years of bisphosphonate) with median follow-up 5·6 woman-years, 3453 first recurrences, and 2106 subsequent deaths. Overall, the reductions in recurrence (RR 0·94, 95% CI 0·87–1·01; 2p=0·08), distant recurrence (0·92, 0·85–0·99; 2p=0·03), and breast cancer mortality (0·91, 0·83–0·99; 2p=0·04) were of only borderline significance, but the reduction in bone recurrence was more definite (0·83, 0·73–0·94; 2p=0·004). Among premenopausal women, treatment had no apparent effect on any outcome, but among 11 767 postmenopausal women it produced highly significant reductions in recurrence (RR 0·86, 95% CI 0·78–0·94; 2p=0·002), distant recurrence (0·82, 0·74–0·92; 2p=0·0003), bone recurrence (0·72, 0·60–0·86; 2p=0·0002), and breast cancer mortality (0·82, 0·73–0·93; 2p=0·002). Even for bone recurrence, however, the heterogeneity of benefit was barely significant by menopausal status (2p=0·06 for trend with menopausal status) or age (2p=0·03), and it was non-significant by bisphosphonate class, treatment schedule, oestrogen receptor status, nodes, tumour grade, or concomitant chemotherapy. No differences were seen in non-breast cancer mortality. Bone fractures were reduced (RR 0·85, 95% CI 0·75–0·97; 2p=0·02).
Adjuvant bisphosphonates reduce the rate of breast cancer recurrence in the bone and improve breast cancer survival, but there is definite benefit only in women who were postmenopausal when treatment began.
Bisphosphonates in multiple myeloma: a network meta‐analysis (2012)
Alendronate anticancer effects
Alendronate inhibits proliferation and invasion of human epidermoid carcinoma cells in vitro, 2005
Assessment of Anticancer Effect of Alendronate in Breast Cancer: An In vitro Study, 2019
Anti-Tumor Activity and Immunotherapeutic Potential of a Bisphosphonate Prodrug, 2017
Bisphosphonates have benefits in breast cancer and multiple myeloma patients and have been used with adoptive immunotherapy with γδ T cells expressing Vγ2 Vδ2 TCRs. Although treatment with γδ T cells is safe, it has shown limited efficacy. Present bisphosphonates stimulate γδ T cells but were designed to inhibit bone resorption rather than treating cancer and have limited oral absorption, tumor cell entry, and cause bone side effects. The development of phosphate and phosphonate nucleotide prodrugs has led to important drugs for hepatitis C and HIV. Using a similar approach, we synthesized bisphosphonate prodrugs and found that they efficiently limit tumor cell growth. Pivoxil bisphosphonate esters enter cells where esterases convert them to their active acids. The bisphosphonate esters stimulated γδ T cells to secrete TNF-α in response to a variety of tumor cells more efficiently than their corresponding acids. The most active compound, tetrakis-pivaloyloxymethyl 2-(thiazole-2-ylamino)ethylidene-1,1- bisphosphonate (7), specifically expanded γδ T cells and stimulated them to secrete interferon-γ and kill tumor cells. In preclinical studies, combination therapy with compound 7 and γδ T cells prolonged survival of mice inoculated with either human bladder cancer or fibrosarcoma cells. Therefore, bisphosphonate prodrugs could enhance the effectiveness of adoptive cancer immunotherapy with γδ T cells.
Tumour macrophages as potential targets of bisphosphonates, 2011
Tumour cells communicate with the cells of their microenvironment via a series of molecular and cellular interactions to aid their progression to a malignant state and ultimately their metastatic spread. Of the cells in the microenvironment with a key role in cancer development, tumour associated macrophages (TAMs) are among the most notable. Tumour cells release a range of chemokines, cytokines and growth factors to attract macrophages, and these in turn release numerous factors (e.g. VEGF, MMP-9 and EGF) that are implicated in invasion-promoting processes such as tumour cell growth, flicking of the angiogenic switch and immunosuppression. TAM density has been shown to correlate with poor prognosis in breast cancer, suggesting that these cells may represent a potential therapeutic target. However, there are currently no agents that specifically target TAM's available for clinical use.
Bisphosphonates (BPs), such as zoledronic acid, are anti-resorptive agents approved for treatment of skeletal complication associated with metastatic breast cancer and prostate cancer. These agents act on osteoclasts, key cells in the bone microenvironment, to inhibit bone resorption. Over the past 30 years this has led to a great reduction in skeletal-related events (SRE's) in patients with advanced cancer and improved the morbidity associated with cancer-induced bone disease. However, there is now a growing body of evidence, both from in vitro and in vivo models, showing that zoledronic acid can also target tumour cells to increase apoptotic cell death and decrease proliferation, migration and invasion, and that this effect is significantly enhanced in combination with chemotherapy agents. Whether macrophages in the peripheral tumour microenvironment are exposed to sufficient levels of bisphosphonate to be affected is currently unknown. Macrophages belong to the same cell lineage as osteoclasts, the major target of BPs, and are highly phagocytic cells shown to be sensitive to bisphosphonates in model studies; In vitro, zoledronic acid causes increased apoptotic cell death; in vivo the drug has been shown to inhibit the production of pro-angiogenic factor MMP-9, as well as most recent evidence showing it can trigger the reversal of the TAMs phenotype from pro-tumoral M2 to tumoricidal M1. There is thus accumulating evidence supporting the hypothesis that effects on TAMs may contribute to the anti-tumour effect of bisphosphonates. This review will focus in detail on the role of tumour associated macrophages in breast cancer progression, the actions of bisphosphonates on macrophages in vitro and in tumour models in vivo and summarise the evidence supporting the potential for the targeting of tumour macrophages with bisphosphonates.
Technical Advance: Liposomal alendronate depletes monocytes and macrophages in the nonhuman primate model of human disease (link)
Epidemiologic Analysis Along the Mevalonate Pathway Reveals Improved Cancer Survival in Patients Who Receive Statins Alone and in Combination With Bisphosphonates
Purpose
Cohort studies report associations between statin use and improved survival in patients with cancer. We used pharmacoepidemiologic methods to evaluate the survival of patients with cancer who received statins alone or in ostensibly synergistic drug combinations.
Materials and Methods
Patients with cancer who were diagnosed from 2010 to 2013 were identified in a large health care claims database. The rate of all-cause death up to 1 year after diagnosis was compared by Cox proportional hazard regression. Sensitivity analyses included age stratification, statin type and intensity, and comparison with or without bisphosphonates and dipyridamole.
Results
Among 312,907 identified patients with cancer, treatment groups included statin users (n = 65,440), nonstatin users who received medications that block cholesterol absorption (n = 9,289), and nonusers (n = 226,007). Statin use before diagnosis was associated with improved overall survival compared with no treatment (hazard ratio [HR], 0.85; 95% CI, 0.80 to 0.91) and specifically in patients with leukemia, lung, or renal cancers. Nonstatin users had increased overall survival compared with no treatment (HR, 0.73; 95% CI, 0.62 to 0.85); when stratified, this difference held true only for pancreatic cancer and leukemia. No differences were observed between statin and nonstatin groups. Bisphosphonate use alone had no effect (n = 4,528), but patients who used both statins and bisphosphonates (n = 4,090) had increased survival compared with no treatment (HR, 0.60; 95% CI, 0.45 to 0.81). The effect of the combination of dipyridamole and statin use (n = 651) was not significant compared with no treatment.
Conclusion
This study suggests that the combination of statins with drugs that affect isoprenylation, such as bisphosphonates, improves survival in patients with cancer. Consideration of pathway-specific pharmacology allows for hypotheses testing with the pharmacoepidemiologic approach. Prospective evaluation of these findings warrants clinical investigation and preclinical mechanistic studies.
Alendronate kidney disease
What is the impact of bisphosphonate therapy upon dental implant survival? A systematic review and meta‐analysis (2016)


Comments