Plaque Reduction / CVD
Statins - HELPFUL
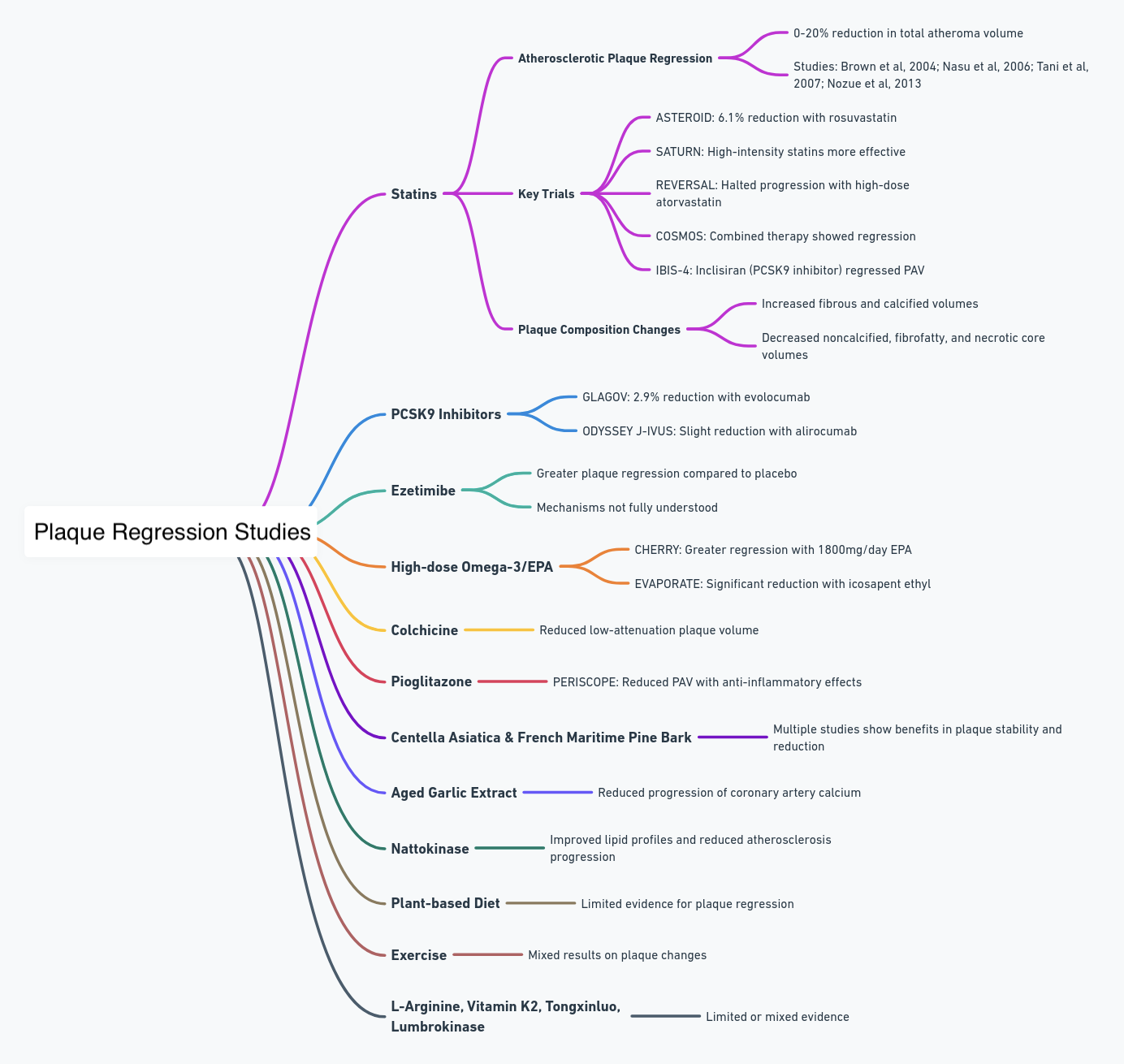
Multiple studies have indicated that statins can lead to atherosclerotic plaque regression, achieving a reduction in total atheroma volume ranging from 0-20%, compared to around a 10% plaque progression observed in control groups. This has been evidenced in studies by Brown et al, 2004; Nasu et al, 2006; Tani et al, 2007; and Nozue et al, 2013.
The ASTEROID trial (2006) demonstrated a 6.1% reduction in total atheroma volume with rosuvastatin 40mg over 24 months in 507 patients. Further evidence of plaque regression with statin therapy was shown in the SATURN (2011), COSMOS (2009), and IBIS-4 (2015) trials. Notably, high-intensity statins such as atorvastatin and rosuvastatin were more effective in reducing plaque than lower doses, as observed in the REVERSAL (2004), SATURN, and JAPAN-ACS (2009) trials.
Additionally, statin therapy has been found to increase fibrous and calcified plaque volumes while decreasing noncalcified, fibrofatty, and necrotic core volumes, as assessed by VH-IVUS and CCTA in multiple studies. These treatments also led to an increase in fibrous cap thickness.
Key numerical results (Percent atheroma volume – PAV):
The SATURN trial (Nicholls et al., 2011) showed high-dose atorvastatin (80mg) regressed PAV by -0.99% compared to -0.31% with low-dose atorvastatin (10mg) over 24 months in 1039 patients (p=0.001).
The REVERSAL trial (Nissen et al., 2004) found high-dose atorvastatin (80mg) halted progression of PAV (0.4% increase) compared to low-dose pravastatin (40mg; +2.7% increase) over 18 months in 502 patients (p=0.02).
The ASTEROID trial (Nissen et al., 2006) showed high-dose rosuvastatin (40mg) regressed PAV by -0.98% compared to baseline over 24 months in 507 patients (p<0.001).
The COSMOS trial (Puri et al., 2016) found rosuvastatin (40mg) + canakinumab (anti-inflammatory) regressed PAV by -0.95% compared to -0.05% with placebo over 52 weeks in 418 patients (p<0.001).
The PROSPECT trial (Stone et al., 2011) showed patients on statins had a lower rate of plaque progression (24.6%) compared to those not on statins (38.5%) over 3.4 years (p=0.008).
The JAPAN-ACS trial (Hiro et al., 2009) found strong statins reduced plaque volume by -5.1% compared to -0.7% with non-statin therapy over 8-12 months in 252 patients (p=0.015).
Beyond regressing plaque volume, statins have also been shown to stabilize plaque by increasing fibrous tissue and reducing lipid content:
The SATURN trial found high-dose atorvastatin increased fibrous tissue by +2.4% compared to +0.6% with low-dose atorvastatin (p=0.01).
The REVERSAL trial showed atorvastatin increased fibrous tissue by +0.6% compared to a -2.2% decrease with pravastatin (p<0.001).
The ESTABLISH trial (Nozue et al., 2015) found pitavastatin + ezetimibe reduced lipid volume by -17.1% compared to -7.1% with pitavastatin alone over 12 months in 104 patients (p=0.01).
A meta-analysis by Ozaki et al. (2019) concluded statins significantly increased fibrous cap thickness by 27-62μm in coronary plaques.
PCSK9 inhibitors - HELPFUL
The GLAGOV trial (2016) demonstrated that the PCSK9 inhibitor evolocumab reduced total atheroma volume by 2.9%, as compared to a 0.4% reduction with placebo over a period of 76 weeks. Meanwhile, the ODYSSEY J-IVUS trial (2019) showed a slight but non-significant reduction in total atheroma volume with alirocumab over 36 weeks. These findings suggest that such agents may have significant benefits for plaque regression, highlighting the need for longer-term studies to fully demonstrate their efficacy.
Key numerical results:
The GLAGOV trial (Nicholls et al., 2016) showed that evolocumab on top of statins significantly regressed atherosclerotic plaque volume compared to statins alone in 968 patients. Evolocumab reduced percent atheroma volume (PAV) by 0.95% compared to 0.05% increase with statins alone (p<0.001).
The IBIS-4 trial (Puri et al., 2018) found that adding inclisiran, a PCSK9 inhibitor, to statins regressed PAV by 1.01% compared to 0.26% increase with placebo over 18 months in 505 patients (p<0.001).
The PRECISE-IVUS trial (Tsujita et al., 2017) showed that adding evolocumab to statins regressed PAV by -0.5% compared to +0.1% increase with statins alone over 52 weeks in 329 patients (p=0.011).

Ezetimibe - HELPFUL
At least six trials employing Intravascular Ultrasound (IVUS) have explored the effects of adding ezetimibe 10mg to optimal medical therapy. These trials mostly demonstrated numerically greater plaque regression when compared to placebo, with reductions in total atheroma volume ranging from -2.9% to -13.9%. However, not all of these trials reached statistical significance.
Ref: https://www.jacc.org/doi/10.1016/j.jacc.2021.10.035
PRECISE-IVUS (Tsujita et al, 2015): Reduction in plaque volume with ezetimibe added to statin therapy.
Conclusion: Ezetimibe contributes to coronary plaque regression when combined with statins.
Ref: https://pubmed.ncbi.nlm.nih.gov/26227186/
M. Hougaard et al., "Influence of ezetimibe in addition to high-dose atorvastatin therapy on plaque composition in patients with ST-segment elevation myocardial infarction assessed by serial: intravascular ultrasound with iMap: the OCTIVUS trial," Cardiovasc Revasc Med (2017)
Conclusions: Ezetimibe in addition to atorvastatin therapy was associated with regression of coronary atherosclerosis.
Ref: https://pubmed.ncbi.nlm.nih.gov/27919638/
Ezetimibe RCT (n=89) showing 0.4% reduction with combination versus 1.4% increase in percent atheroma volume over 12 months (Kovarnik et al., 2012).
Ref: https://pubmed.ncbi.nlm.nih.gov/22076422/
High-dose omega-3/EPA - LIKELY HELPFUL
The CHERRY trial (2020) demonstrated greater plaque regression over a 6-month period with the administration of 1800mg/day of EPA compared to a control group. Additionally, various other trials have shown that EPA treatment leads to an increase in fibrous volume and a decrease in lipid volume within coronary plaques. Utilizing OCT imaging, multiple studies have found significant increases in fibrous cap thickness when EPA is administered. Furthermore, the EVAPORATE trial (2020) revealed a markedly greater plaque regression with icosapent ethyl at a dose of 4g/day compared to placebo over an 18-month period.
Key numerical results:
The EVAPORATE trial (Budoff et al., 2020) found that in 80 patients with coronary artery disease on statins, icosapent ethyl (IPE, a highly purified EPA ethyl ester) 4 g/day significantly reduced low-attenuation plaque (LAP) volume by 17% over 18 months compared to placebo which increased LAP volume by 109%. IPE also reduced fibrofatty and fibrous plaque volume while dense calcium was unchanged.
Serial coronary CT scans in 210 ACS patients (Motoyama et al., 2022) found high-dose EPA (icosapent ethyl or EPA ethyl esters) significantly reduced coronary plaque progression compared to no EPA (5.6% vs 20.3%). EPA reduced lipid-rich plaque volume and macrophages.
A randomized trial in 80 patients (Sekimoto et al., 2023) found those with higher baseline EPA/AA ratios (0.41) had more stable plaque features like layered plaque and calcification compared to those with lower ratios.
In 369 patients who underwent PCI (Asakura et al., 2023), those with lower EPA/AA ratios (<0.4) had a higher prevalence of vulnerable plaque features like lipid-rich plaque and macrophages compared to those with ratios ≥0.4.
Fatty fish intake providing EPA+DHA was associated with less coronary plaque progression compared to non-fish intake in 272 patients (Puri et al., 2022).
Higher erythrocyte EPA levels were associated with plaque regression and lower CV events in 240 patients randomized to EPA+DHA versus no EPA/DHA (Alfaddagh et al., 2019). An omega-3 index ≥4% was optimal.
In summary, human studies utilizing coronary imaging, plaque histology, and clinical periodontal outcomes provide evidence that the omega-3 fatty acid EPA can regress or stabilize atherosclerotic plaque when used as an adjunct to statins. Reduced plaque volume, lipid content, macrophages, and increased collagen are observed with EPA supplementation. Higher erythrocyte EPA levels and EPA/AA ratios are associated with more stable plaque phenotypes and improved clinical outcomes. The anti-inflammatory and antioxidant properties of EPA are likely key mechanisms underlying plaque stabilization.
Colchicine - LIKELY HELPFUL
An open-label CCTA study in 80 ACS patients (2017) showed colchicine 0.5mg/day reduced low-attenuation plaque volume by 15.9mm3 versus 6.6mm3 with optimal medical therapy alone over 12 months. Total atheroma volume changes were similar. Further RCTs are required given promising outcome data with colchicine.
Pioglitazone - LIKELY HELPFUL
The PERISCOPE was a double-blind, randomized, multicenter trial that sought to evaluate plaque changes with pioglitazone vs glimepiride using IVUS, results showed PAV reduction in the pioglitazone group (Mean PAV decreased 0.16%, 95% CI, vs increased 0.73%, 95% CI, P = 0.002), inhibition of inflammation might be the mechanism involved (Nissen et al, 2008).
Pioglitazone reduces the necrotic-core component in coronary plaque in association with enhanced plasma adiponectin in patients with type 2 diabetes mellitus (Ogasawara et al, 2009)
Effects of the PPARγ agonist pioglitazone on coronary atherosclerotic plaque composition and plaque progression in non-diabetic patients: a double-center … (Christoph, 2015)
Pioglitazone induces regression of coronary atherosclerotic plaques in patients with type 2 diabetes mellitus or impaired glucose tolerance: a randomized prospective … (Nakayama et al, 2010)
Pioglitazone induces regression and stabilization of coronary atherosclerotic plaques in patients with impaired glucose tolerance (Yang et al, 2012)
Regression and shift in composition of coronary atherosclerotic plaques by pioglitazone: insight from an intravascular ultrasound analysis (Clementi et al, 2009)
Pioglitazone reduces neointima volume after coronary stent implantation: a randomized, placebo-controlled, double-blind trial in nondiabetic patients (Marx et al, 2005)
Rapid improvement of carotid plaque echogenicity within 1 month of pioglitazone treatment in patients with acute coronary syndrome (Hirano et al, 2009)
Pioglitazone decreases coronary artery inflammation in impaired glucose tolerance and diabetes mellitus: evaluation by FDG-PET/CT imaging (Nitta et al, 2013
Pioglitazone attenuates atherosclerotic plaque inflammation in patients with impaired glucose tolerance or diabetes: a prospective, randomized, comparator-controlled … (Mizoguchi et al, 2011)
Benefit of adding pioglitazone to successful statin therapy in nondiabetic patients with coronary artery disease (Sugamura et al, 2008)
Centella Asiatica (Gotu Kola) and French Maritime Pine Bark - LIKELY HELPFUL
Multiple studies have demonstrated the potential benefits of Centella asiatica and French maritime pine bark extracts in improving plaque stability, reducing progression, and decreasing calcifications in arterial plaques:
A 1-year study by L Incandela et al, 2001, involving 60 patients, found that Centella extract prevented an increase in plaque size and increased firm plaque compared to placebo.
A 3-year study by Gianni Belcaro et al, 2020, involving over 300 patients, showed substantially lower plaque progression with the combined use of pine bark and Centella extracts.
A 4-year study by G Belcaro et al, 2015, with over 200 patients, found significantly lower progression to worse plaque conditions with these extracts.
A 1-year study by Shu Hu et al, 2020, including 84 patients, observed decreased arterial calcifications with the extracts, in contrast to increased calcifications with aspirin alone.
A 6-month study by Gianni Belcaro et al, 2017, involving 40 patients, demonstrated a doubled plaque stability index with the use of these extracts.
These studies collectively suggest that Centella asiatica and French maritime pine bark extracts hold promise for improving various plaque parameters
Aged Garlic Extract - LIKELY HELPFUL
Multiple studies have demonstrated that aged garlic extract (AGE) reduces the progression of coronary artery calcium versus placebo in patients with heart disease or at high risk. Key studies include those by Budoff et al, 2004, Budoff et al, 2009, and Zeb et al, 2012. Additionally, a 2020 study also found lower coronary artery calcium (CAC) progression with AGE. Further research, specifically the 2004, 2016, and 2013 studies, showed that subjects taking AGE had reduced plaque progression and superior prevention of CAC/carotid intima-media thickness (CIMT) progression compared to placebo. Overall, these results indicate that garlic, particularly AGE, can effectively slow the progression of atherosclerosis.
Garlic and Heart Disease, 2016
Three small-scale, randomized, double-blind, placebo-controlled studies have demonstrated the positive effects of garlic on the progression of Coronary Artery Calcification (CAC), employing it as a surrogate marker for clinical endpoints (Budoff et al., 2004; Budoff et al., 2009; Zeb et al., 2012). These studies uniformly utilized the standardized Kyolic brand Aged Garlic Extract (KB AGE) at typical doses (e.g. 1.2g/day).
The first study by Budoff et al. (2004) indicated that among 23 patients with known coronary artery disease or high-risk patients (Framingham risk >20% over 10 years), KB AGE reduced the progression of CAC over a year compared to a placebo. Specifically, the progression rate was 7.5 ± 9.4% in the KB AGE group, whereas it was 22.2 ± 18.5% in the placebo group.
In a subsequent study, Budoff et al. (2009) achieved significant outcomes in a sample of 65 intermediate-risk patients (average age of 60 ± 9 years) with a Framingham risk of 10–20% and a baseline CAC greater than 30. The treatment involved KB AGE supplemented with vitamin B-12, folic acid, vitamin B-6, and L-arginine. Over a one-year follow-up period, the CAC progression was significantly lower in the treatment group compared to the placebo group (6.8% compared to 26.5%, P = 0.005).
Lastly, Zeb et al. (2012) conducted a study involving 65 asymptomatic, intermediate-risk men (average age 55 ± 6 years, baseline CAC >10), who were treated with KB AGE plus coenzyme Q10. The results after a year demonstrated a significantly lower mean CAC progression in the treatment group than in the placebo group (32 ± 6 compared with 58 ± 8, P = 0.01).
Given the connection between CAC progression and an elevated risk of Ischemic Heart Disease (IHD), and considering the evidence from these three studies indicating that garlic treatment reduces the progression rate of CAC, it is reasonable to hypothesize that garlic could help decrease IHD rates. However, it's important to highlight that while all three studies used KB AGE, two of them used additional treatments alongside KB AGE, which could potentially have influenced the outcomes.
In a 2020 study with 2.4g Aged Garlic Extract, the placebo group had a significantly increased annular CAC progression of 28% compared to the AGE supplement group (20%).
The rate of increase in coronary artery calcium scoring, a marker for atherosclerosis, was measured in subjects taking an aged garlic product or placebo (2004). The mean change of the calcium score was significantly lower in subjects taking the active garlic product along with a trend towards improved high-density lipoprotein cholesterol levels and homocysteine levels.
Since then, studies using coronary CT angiography, a more advanced imaging modality, have been completed (2016). Over the course of a year, subjects consuming aged garlic extract experienced a significantly lower change in plaque compared to subjects taking a placebo. Using a different vascular assessment, the carotid intima-media thickness (CIMT) test, a group of subjects taking garlic powder tablets or placebo were studied (2013). After 3 months of treatment, CIMT differences existed with superior prevention of progression in the garlic group.
Plant-based diet - LIKELY HELPFUL
The Ornish Lifestyle Heart Trial (1998) prescribed a plant-based diet without added fats and showed reductions in coronary artery narrowing at 5 years. However, this study used angiography rather than direct plaque imaging. The DISCO-CT trial (2020) found greater reductions in noncalcified plaque with a plant-based diet, but no change in percent atheroma volume. Overall, diet alone has limited evidence for plaque regression.
The Lifestyle Heart Trial (n=42) combined a very low-fat vegetarian diet with stress management and moderate exercise. Percent diameter stenosis regressed from 40% to 37.8% after 1 year in the intervention group, compared to progression from 42.7% to 46.1% in usual care. Greater regression was seen after 5 years along with fewer cardiac events (Ornish et al., 1990; Ornish et al., 1998).
An open 2-year trial (n=123) of a plant-based diet, exercise, stress management showed 6.1% average reduction in diameter stenosis. Most adherent tertile had 18.2% regression with 4-fold lower cardiac events than least adherent (38 vs 11 events) (Gupta et al., 2011).
A 2-year vegetarian diet cohort study (n=39) showed no lesion progression in 18 patients, but no regression. Lesion growth correlated with higher cholesterol/HDL ratio (Arntzenius et al., 1985).
The STARS diet trial (n=90) over 39 months reduced coronary narrowing progression to 15% and 12% with diet interventions compared to 46% with usual care (Watts et al., 1992).
Nattokinase - MIXED EVIDENCE
A retrospective study of 1,062 hyperlipidemic patients by Chen et al. (2022) found that nattokinase (NK) at 10,800 FU/day for 12 months significantly improved lipid profiles by 15.7-18.1% and reduced carotid atherosclerosis progression by 21.7-36% compared to no treatment. A lower dose of NK (3,600 FU/day) was found to be ineffective. The study also noted that lifestyle factors and co-administration of vitamin K2 or aspirin further enhanced NK's effects. This research provides evidence for NK's anti-atherosclerotic effects at higher doses.
Exercise - MIXED EVIDENCE
A meta-analysis showed that cardiac rehabilitation with exercise reduced cardiovascular (CV) mortality and hospital admissions by 26% and 18%, respectively. However, randomized controlled trials (RCTs) using intravascular ultrasound (IVUS) did not find significant plaque regression with exercise compared to control. One study found regression in patients walking more than 7000 steps per day. Observational data associating exercise with plaque changes are limited overall.
L-Arginine - MIXED EVIDENCE
A small RCT adding L-arginine to garlic extract, B vitamins and statin found reduced CAC progression versus placebo over 1 year in intermediate risk patients (Budoff et al, 2009). However, L-arginine's contribution is unclear. Another small RCT in hypercholesterolemic patients found improved endothelial function but no impact on carotid IMT after 6 months of L-arginine. Evidence is very limited overall.
Vitamin K2 - MIXED EVIDENCE
While hopes exist that Vitamin K2 could reduce coronary calcification, RCT evidence is lacking. One RCT in aortic stenosis showed no impact on CAC progression with high-dose K2. Another found no CAC progression over 3 years with K2, but had no placebo group. Overall, evidence is mixed.
Tongxinluo
This traditional Chinese combination was associated with plaque regression and reduced cardiac events in one study of over 1000 patients (Shi et al, 2016). However, exotic components like scorpion extract may limit applicability. Further studies in other populations are needed.
Lumbrokinase
A Chinese multicenter RCT (n=310) found lumbrokinase reduced fibrinogen, CRP, plaque volume and carotid IMT compared to placebo over 1 year in stroke patients (Cao et al, 2013). Side effects were minimal. Evidence remains limited to this lone trial.


Comments