Phosphatidylcholine
The body makes a chemical called acetylcholine from phosphatidylcholine. Acetylcholine is important for memory and other functions in the body. Phosphatidylcholine might help to protect the liver and the wall of the large intestine.
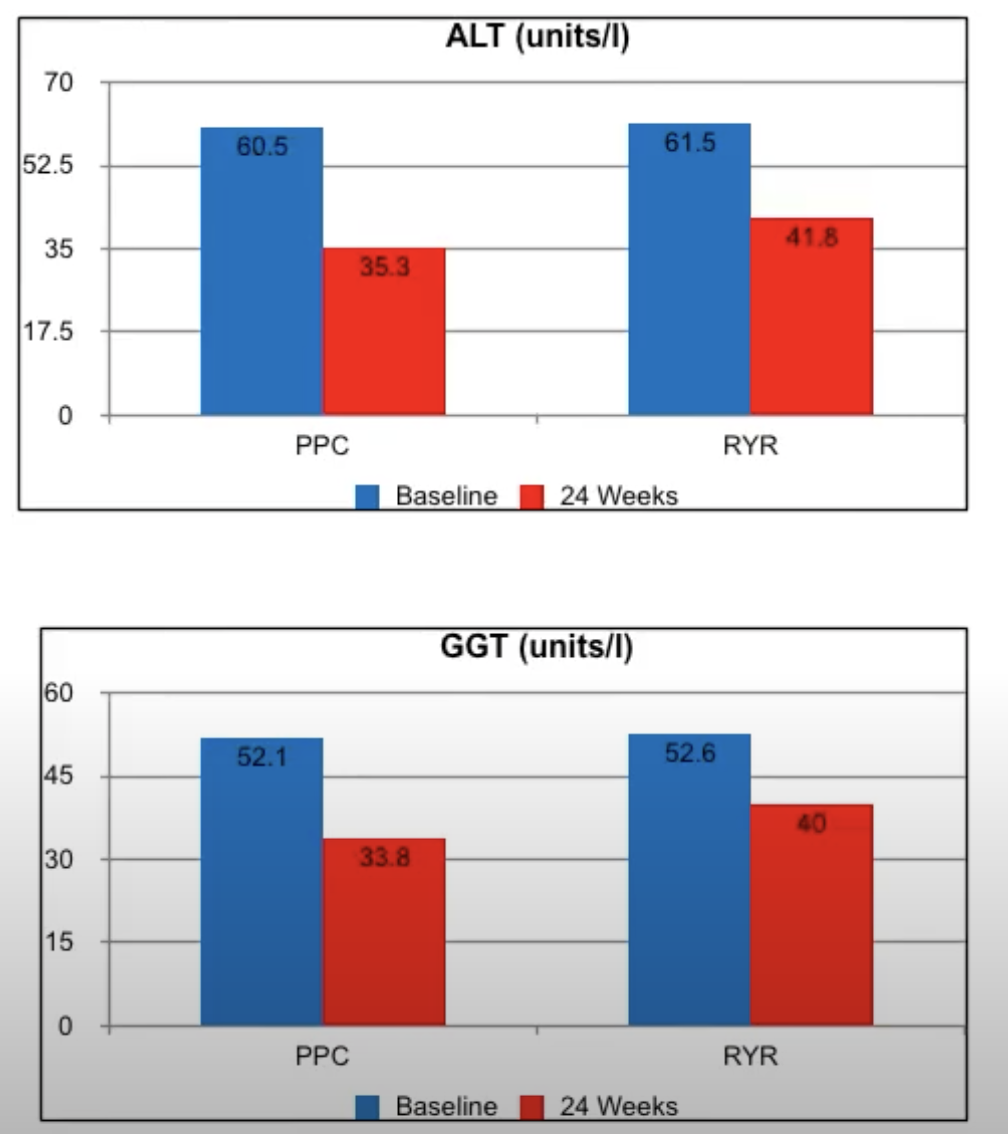
Effectiveness of phosphatidylcholine as adjunctive therapy in improving liver function tests in patients with non-alcoholic fatty liver disease and metabolic comorbidities: real-life observational study from Russia, 2020
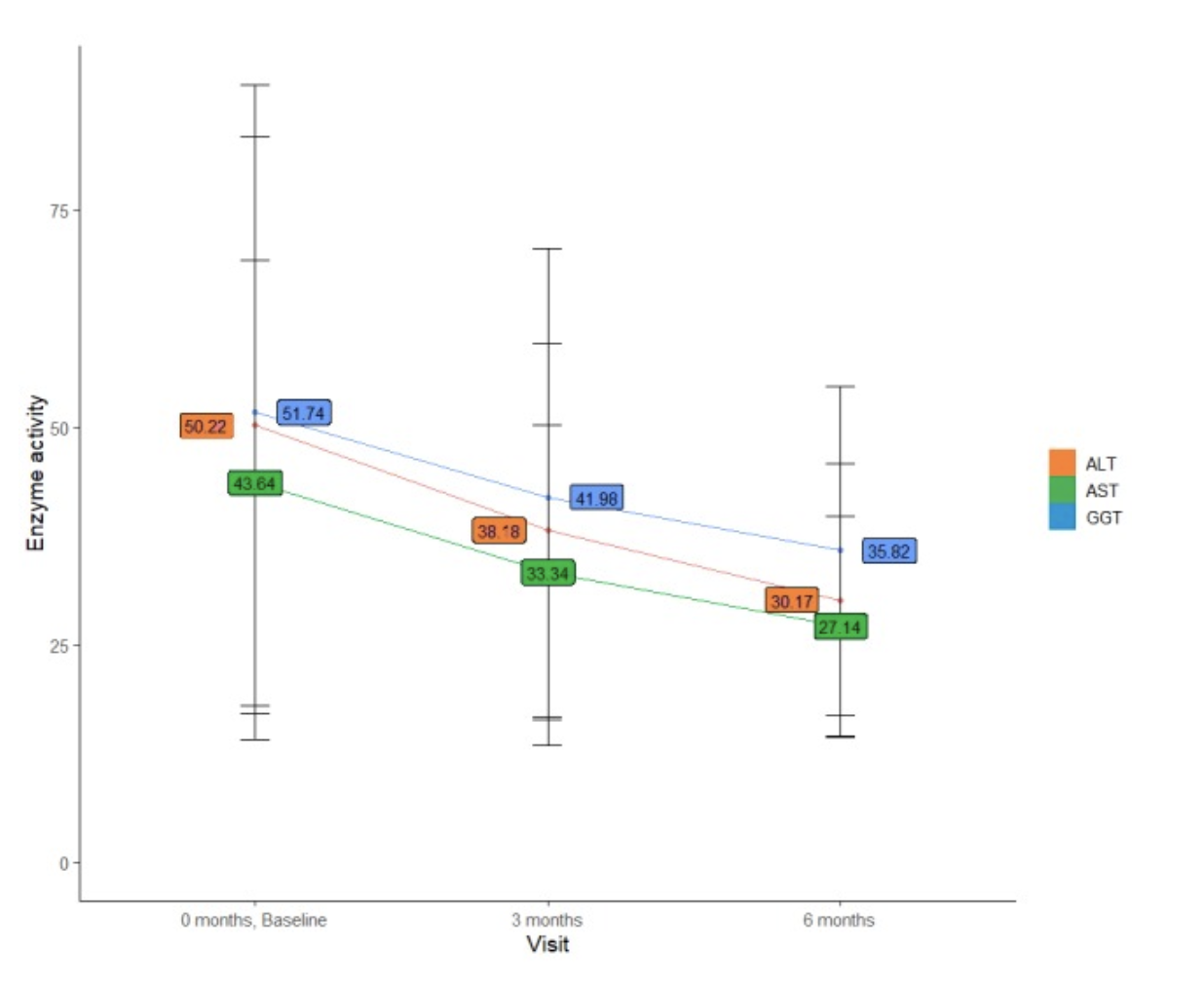
A total of 2843 adult patients with newly diagnosed NAFLD, who had a least one of four comorbidities, namely, overweight/obesity, hypertension, type 2 diabetes mellitus, and hypercholesterolaemia, and who were prescribed 1.8 g/day of PPC as an adjunctive treatment to standard care, were enrolled during 2015–2016. Laboratory data were collected at baseline and 12 and 24 weeks of the study, and included liver function tests (aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT)), fasting plasma glucose, and lipid profile.
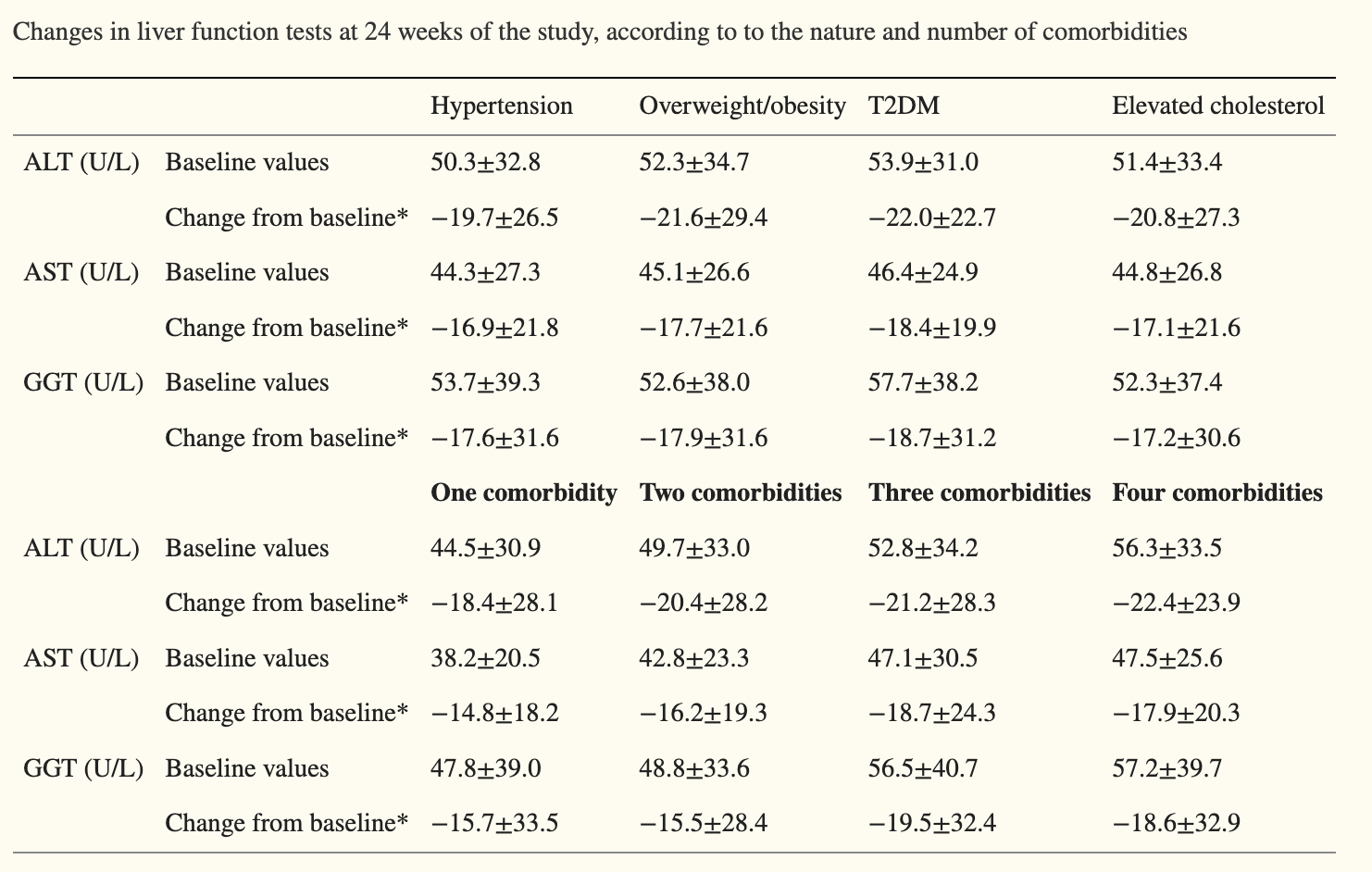
Overall, 2263 patients (79.6%) had at least two metabolic comorbidities associated with NAFLD, and overweight/obesity was the most common comorbidity reported in 2298 (80.8%) patients. At 24 weeks, there was a significant decrease in liver enzyme levels (all p<0.001 compared with baseline). Across the four comorbidity subgroups, there was a mean drop of ALT levels ranging from 19.7 to 22.0 U/L, AST from 16.9 to 18.4 U/L, and GGT from 17.2 to 18.7 U/L. Similar findings were reported in subgroups with either one, two, three, or four comorbidities, with a significant decrease in liver enzyme levels ranging from 18.4 to 22.4 U/L for ALT, 14.8 to 18.7 U/L for AST, and 15.5 to 19.5 U/L for GGT.
Conclusions
Adjuvant treatment with PPC resulted in consistent improvements in liver enzymes in patients with newly diagnosed NAFLD and associated metabolic comorbidities.
γ-Glutamyl Transferase Is Associated with Mortality Outcomes Independently of Fatty Liver
Methods: In an occupational cohort (n = 278 419), causes of death (International Statistical Classification of Diseases and Related Health Problems, 10th revision) were recorded over 7 years. Liver function tests and liver fat [measured by ultrasonographic standard criteria or fatty liver index (FLI)] were assessed at baseline. We used Cox proportional hazards models to estimate adjusted hazard ratios (HRs) and 95% CIs of all-cause, cancer, and CVD mortality for GGT quartiles (with lowest GGT quartile as reference).
Results: There were 136, 167, 265, and 342 deaths across increasing GGT quartiles. After adjusting for liver fat (by ultrasound diagnosis) in the fully adjusted model, all-cause and cancer mortality were increased in the highest GGT quartile [HR 1.50 (95% CI 1.15-1.96) and 1.57 (1.05-2.35), respectively]. For CVD mortality, the hazard was attenuated: HR 1.35 (95% CI 0.72-2.56). After adjusting for FLI in the fully adjusted model, HRs for all-cause, cancer, and CVD mortality were 1.46 (0.72-2.56), 2.03 (1.02-4.03), and 1.16 (0.41,3.24), respectively.
Conclusions: There were similar hazards for all-cause and cancer mortality and attenuated hazards for CVD mortality for people in the highest GGT quartile, adjusting for fatty liver assessed by either ultrasound or FLI.
Effectiveness of phosphatidylcholine in alleviating steatosis in patients with non-alcoholic fatty liver disease and cardiometabolic comorbidities (MANPOWER study)
Design This 24-week, observational, prospective study was carried out in 174 medical sites across 6 federal districts of Russia. A total of 2843 adult patients with newly diagnosed NAFLD, who had a least one of four comorbidities, namely overweight/obesity, hypertension, type 2 diabetes mellitus and hypercholesterolaemia, and who received PPC as an adjunctive treatment to standard care, were enrolled. The assessment of liver ultrasonography was qualitative.
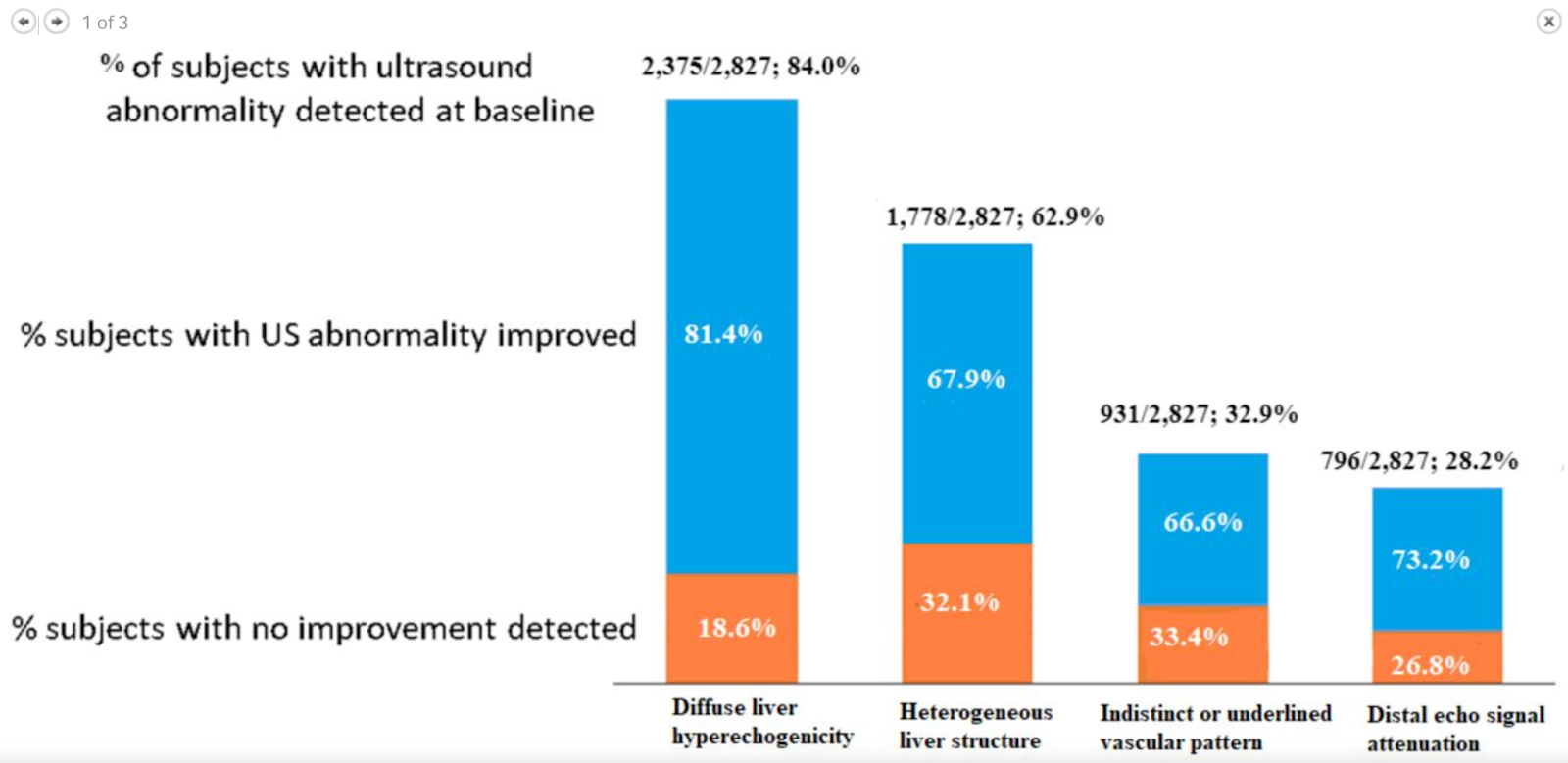
Results Overall, 2263 (79.6%) patients had at least two metabolic comorbidities associated with NAFLD, and overweight/obesity was the most common comorbidity reported in 2298 (80.8%) patients. Almost all study participants (2837/2843; 99.8%) were prescribed 1.8 g of PPC administered three times daily. At baseline, the most frequently identified abnormalities on ultrasound were liver hyperechogenicity (84.0% of patients) and heterogeneous liver structure (62.9%). At 24 weeks, a significant (p<0.05) improvement in liver echogenicity and in liver structure was observed in 1932/2827 (68.3%) patients (95% CI 66.6% to 70.1%) and in 1207/2827 (42.7%) patients (95% CI 40.9% to 44.5%), respectively. The analysis of ultrasonographic signs by number of comorbidities revealed similar findings—liver echogenicity improved in 67.2%–69.3% and liver structure in 35.6%–45.3% of patients depending on the number of comorbidities.
Conclusion This study showed that PPC adjunctive therapy may be useful in improving the ultrasonographic features of NAFLD in patients with associated cardiometabolic comorbidities. It also supports evidence regarding the role of PPC in the complex management of NAFLD.
One of the first clinical trials to show that EPL lead to improvement in histological steatosis was a randomised, placebo-controlled, double-blind study from Poland by Gonciarz et al 37 in 29 patients with NAFLD with T2DM. EPLs, given at 600 mg three times per day for 6 months, were associated with a marked histological improvement in 4/15 (26.7%) patients in the EPL group versus 1/14 (7.1%) in the placebo group. In addition, EPLs were significantly effective in reducing liver size (mean measurement of the right liver lobe: 14.6 cm at baseline vs 14.4 cm at 6 months of therapy in the placebo group, as compared with 14.9 cm at baseline vs 14.0 cm at 6 months in the EPL group; p<0.05), probably as a result of reducing liver fat content.37 Our study results were also in line with other randomised controlled trials. A placebo-controlled, double-blind study38 conducted in 36 Chinese patients with NAFLD with obesity reported about the positive influence of 1.8 g of EPL/day administered for 3 months on total cholesterol (which was decreased by 10%), TG (decreased by 9%) and transaminases (normalised in 87.5% of patients), supported by a significant (p<0.05) improvement of the fatty liver (as seen from CT).38 In another randomised, open-controlled study39 from China of 68 patients with NAFLD with T2DM (of which 34 received 500 mg of metformin +600 mg of EPL both administered thrice daily vs 34 treated with metformin only for 3 months), ultrasonographic appearance and total effective rate were significantly better (p<0.05) in the EPL+ metformin arm compared with the metformin only arm (total effective rate: 78.4% vs 54.1%, respectively).39 Likewise, in an open-label, controlled study by Yin and Kong,40 in which 185 patients were treated with standard diet +oral anti-diabetics+physical exercise, and 125 of these were additionally treated with 1.8 g of EPL per day administered for 3 months, the total effective rate, which was reflected by improvements of ultrasound findings and of lipid and liver panels, was 90.2% in EPL-treated patients versus 51.0% in the control group (p<0.05).40 In a more recent long-term trial from Russia conducted in 215 diabetic patients with NASH who were randomly allocated to either a basic treatment scheme including metformin taken at 1000 mg per day or the basic treatment scheme +1368 mg of PPC per day, ultrasonography performed after 6 months of treatment revealed that hepatic echotexture significantly improved in 101/152 (66.4%) patients in the PPC group (p=0.02).41 Seven years of PPC treatment led to a decrease in ultrasound signs of fatty liver in 93/114 (81.6%) and a more effective control of T2DM in 98/114 (86.0%) patients. Fibrosis progression also appeared significantly slower in those treated with PPC compared with the control group (p=0.03).41
The findings of this study were also similar to those of real-world studies. In an open-label study by Koga et al 42 from Japan in which 51 patients with NAFLD (including 39 with NAFLD due to obesity) received 500 mg of EPL given three times per day for 6 months, the continuous, EPL-induced improvement or normalisation of the ultrasonic picture was observed in 51% of patients (p<0.001 compared with baseline). Bright liver was reduced, and decrement of backward echocardiogram and the obscurity of the intrahepatic venogram were decreased.42 In another open-label, single-centre, 6-month study from India conducted in 28 patients with NAFLD and T2DM, liver ultrasonography revealed that the hepatic echotexture improved after PPC adjunctive therapy (700 mg three times per day) in 12/22 (54.5%) study subjects.43 More recently, in a prospective, multicentre, open-label study17 evaluating EPL (1.8 g per day given for 24 weeks, followed by 0.9 g per day for 48 weeks), in a cohort of 324 patients with NAFLD from the United Arab Emirates, as an adjuvant nutrient to the treatment of primary NAFLD (n=113) or NAFLD with comorbid disease (T2DM in 107 patients and hyperlipidaemia in 104 patients), improvement of ultrasonography findings (complete or partial) occurred in 29.2%, 23.4% and 20.2% of patients with NAFLD only, NAFLD with T2DM, and NAFLD with hyperlipidaemia, respectively.17
Essential phospholipids for nonalcoholic fatty liver disease associated with metabolic syndrome: A systematic review and network meta-analysis, 2020
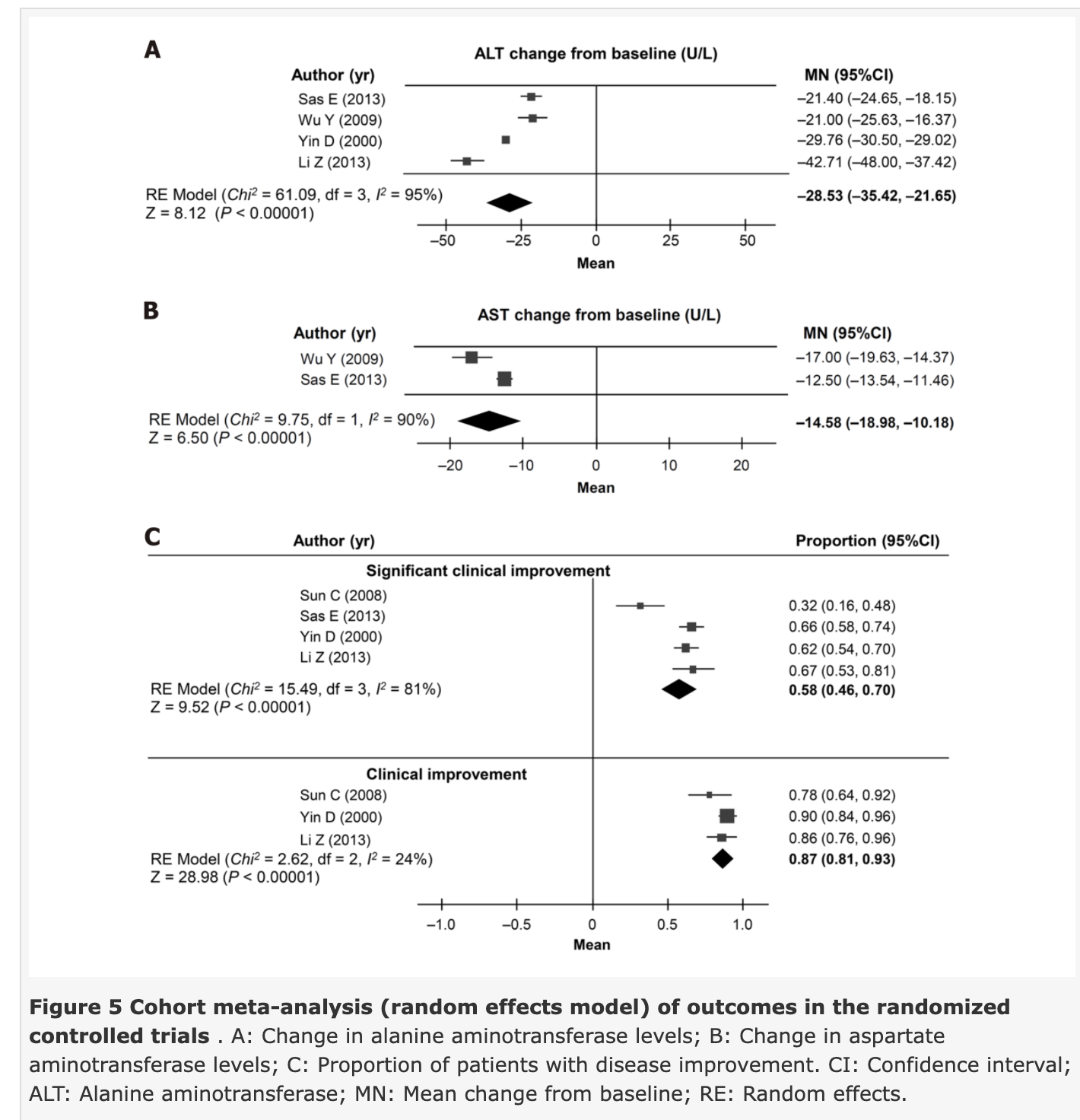
Ten studies met the inclusion criteria (n = 22-324). EPL treatment duration ranged from 4 to 72 wk. In the direct meta-analysis (four randomized controlled trials), compared with antidiabetic therapy alone, EPL plus antidiabetic therapy was associated with a significantly greater reduction in [alanine aminotransferase (ALT); MD: 11.28 U/L (95%CI: -17.33, -5.23), P = 0.0003], triglyceride [MD: -49.33 mg/dL (95%CI: -66.43, -32.23), P < 0.0001] and total cholesterol levels [MD: -29.74 mg/dL (95%CI: -38.02, -21.45), P < 0.0001]. There was also a significant increase in the rate of overall improvement [relative risk 1.50 (95%CI: 1.26-1.79), P < 0.0001], and risk of no disease (P = 0.0091), and a reduction in moderate disease (P = 0.0187); there were no significant differences in severe disease, mild disease, or significant improvement. In the cohort meta-analysis of three non-randomized clinical trials, the MD in ALT levels was -16.71 U/L (95%CI: -24.94, -8.49) and 23% of patients had improved disease. In the cohort meta-analysis of five randomized trials, MD in ALT levels was –28.53 U/L (95%CI: -35.42, -21.65), and 87% (95%CI: 81%, 93%) and 58% (95%CI: 46%, 70%) of patients showed clinical improvement and significant clinical improvement.

[SEEMS NEUTRAL] Metabolomics in renal cell carcinoma: from biomarker identification to pathomechanism insights
Moreover, choline metabolism was implicated in RCC treatment. The conversion of lysophosphatidylcholine to phosphatidylcholine imparted by lysophosphatidylcholine acyltransferase devoted much to tumorigenesis in 30 RCC patients, while lysophosphatidylcholine acyltransferase knockdown could deplete phosphatidylcholine and inhibit RCC proliferation [86] (Table 1). Of note, this is the first time that lysophosphatidylcholine acyltransferase has been studied in RCC tissues. Unfortunately, the individual efficiency of choline and choline-containing metabolites in RCC detection remains a tremendous challenge since choline is not unique to RCC, but the result of any malignancy.
Delayed-Release Phosphatidylcholine Is Effective for Treatment of Ulcerative Colitis: A Meta-Analysis
Background: Phosphatidylcholine (PC) is intrinsically missing in intestinal mucus of patients with ulcerative colitis. Topical supplementation with delayed intestinal release PC formulations is assumed to compensate this lack. Three monocenter randomized controlled trials (RCTs) with a 30% PC-containing lecithin were successful, whereas 1 trial with >94% PC-containing lecithin failed. Objectives: Evaluation of 30% PC-containing lecithin provided in a delayed intestinal release formulation for treatment efficacy of ulcerative colitis was evaluated by meta-analysis of 3 RCTs. Methods: Meta-analysis of 3 studies was performed using RevMan 5.3 software. Odds ratio (OR) and 95% Cl were calculated for remission, clinical and endoscopic improvement, histology, and life quality. p values <0.05 were accepted as significant. Results: The meta-analysis of 3 RTCs with 160 included patients with ulcerative colitis verified that PC improved the rate of remission (OR = 9.68), as well as clinical (OR = 30.58) and endoscopic outcomes (OR = 36.73). Within the available patient population, also histology and quality of life became better. All effects were significant over placebo. Achieved remission was maintained in a higher percentage of patients under intestinal-release PC formulation than placebo. The profile of adverse events was identical to the placebo population. Conclusions: A 30% PC-containing lecithin in delayed intestinal release formulation improves clinical and endoscopic outcomes, histologic activity, and quality of life in patients with ulcerative colitis. For the patients, lack of adverse events is an important consideration.
Choline
https://lpi.oregonstate.edu/mic/other-nutrients/choline
7) Fat Breakdown (Lipolysis)
Fat breakdown involves the breakdown of triglyceride into glycerol and free fatty acids. Phosphatidylcholine (PC) increases the production of PPAR-gamma receptor, responsible for the breakdown of fats [52, 53].
Judging by the clinical experience of some doctors, PC injections directly into the fat deposits can cause fat breakdown and may be used as an alternative to surgery. In the lack of controlled trials, we can’t tell if this treatment is safe and effective [54, 55].
PC injections reduced fat in the eyelids of 30 patients, acting as an alternative to eyelid surgery [56].
According to limited preliminary evidence, they may also help with lipomas, benign tumors caused by fat buildup. However, the researchers emphasized the need for further well-designed studies [57].
PPAR-γ Agonists As Antineoplastic Agents in Cancers, 2017
Activation of PPAR-γ plays an inhibitory role in cell growth and proliferation by favoring cell differentiation (4).
User Experiences
One user reported that using phosphatidylcholine for a few years reversed his fatty liver and returned his high liver enzymes back to normal.
Another user reported that over a period of nearly two months their belly fat “decreased tremendously.”
One user who took phosphatidylcholine for three years had outstanding results. They said that the difference for memory boost and overall health.
3. It may help protect against medication side effects
Some medications, such as nonsteroidal anti-inflammatory drugs (NSAIDs), can cause severe gastrointestinal side effects with extended use. This includes stomach pain, gastric bleeding, and intestinal perforation.
According to a 2012 studyTrusted Source, long-term NSAID use may disrupt a phospholipid layer of the gastrointestinal tract. This may cause gastrointestinal injury. Research has shown that PC may help prevent NSAID-related gastrointestinal damage.
Lecithin Supplements and Breast Cancer Risk
Commercially made lecithin supplements, frequently derived from soy beans, contain phosphatidylcholine, and the terms phosphatidylcholine and lecithin are often used synonymously.2 Phosphatidylcholine is one of the primary forms of choline and is an essential component of cell membranes, important for cell-membrane signaling.3 Phosphatidylcholine is endogenously produced in the liver and converted to choline, but additional choline is needed from dietary sources (eg, egg yolk, liver). In 1998, an Adequate Intake (Dietary Reference Intake) for choline was recommended at 425 mg/d for adult women.2 Laboratory studies suggest that choline deficiency may promote carcinogenesis through uncontrolled apoptosis and DNA damage.3 Recent epidemiologic studies found that choline intake from foods is associated with reduced breast cancer risk4 and mortality,5 although findings are inconsistent.6,7 To the best of our knowledge, no previous studies have evaluated lecithin supplement use and breast cancer risk.
Ever-use of lecithin supplements was associated with reduced breast cancer risk (age-adjusted OR = 0.77 [95% CI = 0.62–0.97]) (Table). Although the association appeared stronger in postmenopausal women (age-adjusted OR = 0.71 [0.55–0.92]) than premenopausal women (0.96 [0.62–1.49]) (Table)
Choline and betaine intake is inversely associated with breast cancer risk: a two-stage case-control study in China (link)
Choline and Betaine Intake and Colorectal Cancer Risk in Chinese Population: A Case-Control Study
Total choline intake was inversely associated with colorectal cancer risk after adjustment for various lifestyle and dietary factors. The multivariate-adjusted OR was 0.54 (95%CI = 0.37-0.80, Ptrend <0.01) comparing the highest with the lowest quartile.
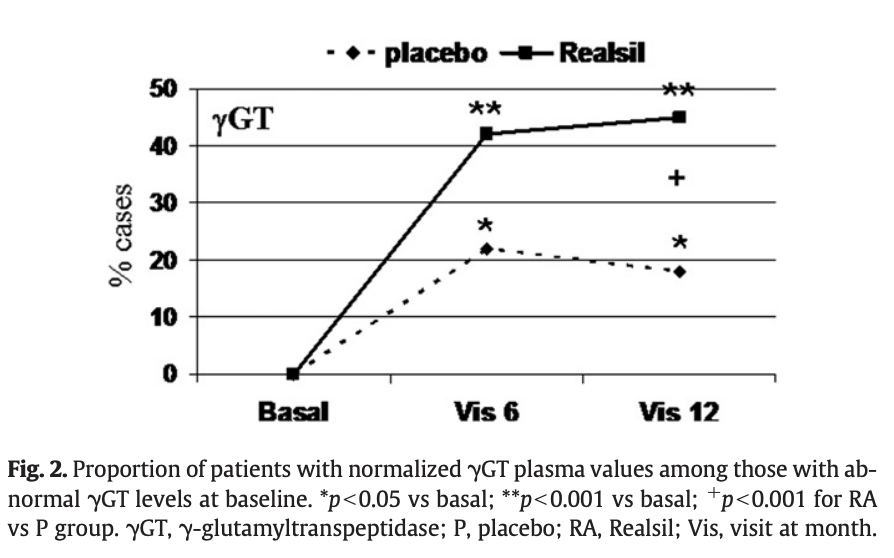
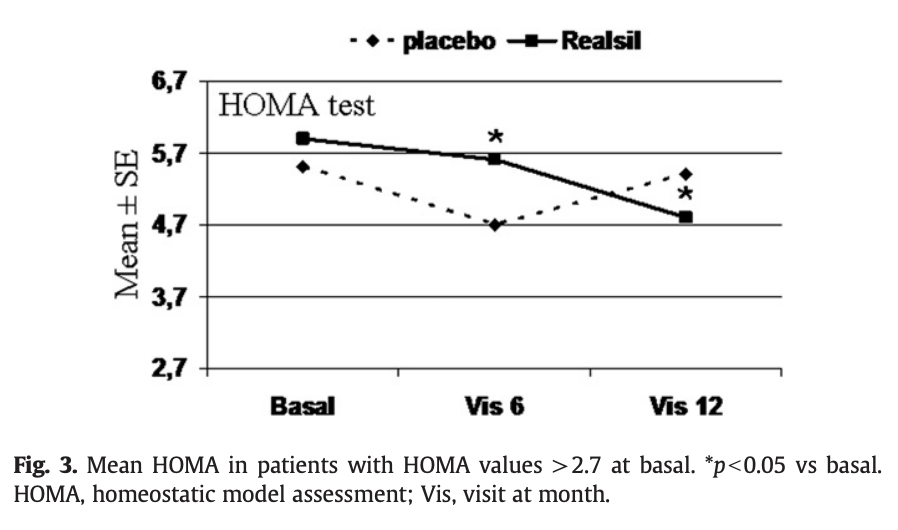
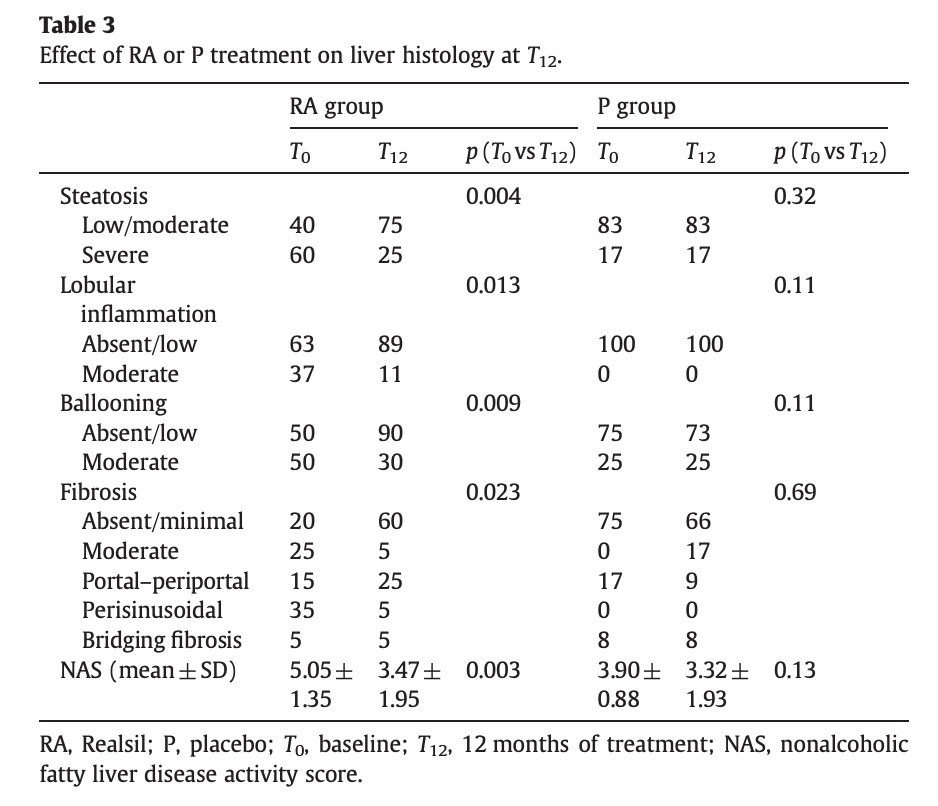
Silybin combined with phosphatidylcholine and vitamin E in patients with nonalcoholic fatty liver disease: a randomized controlled trial (link)
The only currently recommended treatment for nonalcoholic fatty liver disease (NAFLD) is lifestyle modification. Preliminary studies of silybin showed beneficial effects on liver function. Realsil (RA) comprises the silybin phytosome complex (silybin plus phosphatidylcholine) coformulated with vitamin E. We report on a multicenter, phase III, double-blind clinical trial to assess RA in patients with histologically documented NAFLD. Patients were randomized 1:1 to RA or placebo (P) orally twice daily for 12 months. Prespecified primary outcomes were improvement over time in clinical condition, normalization of liver enzyme plasma levels, and improvement of ultrasonographic liver steatosis, homeostatic model assessment (HOMA), and quality of life. Secondary outcomes were improvement in liver histologic score and/or decrease in NAFLD score without worsening of fibrosis and plasma changes in cytokines, ferritin, and liver fibrosis markers. We treated 179 patients with NAFLD; 36 were also HCV positive. Forty-one patients were prematurely withdrawn and 138 patients analyzed per protocol (69 per group). Baseline patient characteristics were generally well balanced between groups, except for steatosis, portal infiltration, and fibrosis. Adverse events (AEs) were generally transient and included diarrhea, dysgeusia, and pruritus; no serious AEs were recorded. Patients receiving RA but not P showed significant improvements in liver enzyme plasma levels, HOMA, and liver histology. Body mass index normalized in 15% of RA patients (2.1% with P). HCV-positive patients in the RA but not the P group showed improvements in fibrogenesis markers. This is the first study to systematically assess silybin in NAFLD patients. Treatment with RA but not P for 12 months was associated with improvement in liver enzymes, insulin resistance, and liver histology, without increases in body weight. These findings warrant further investigation.

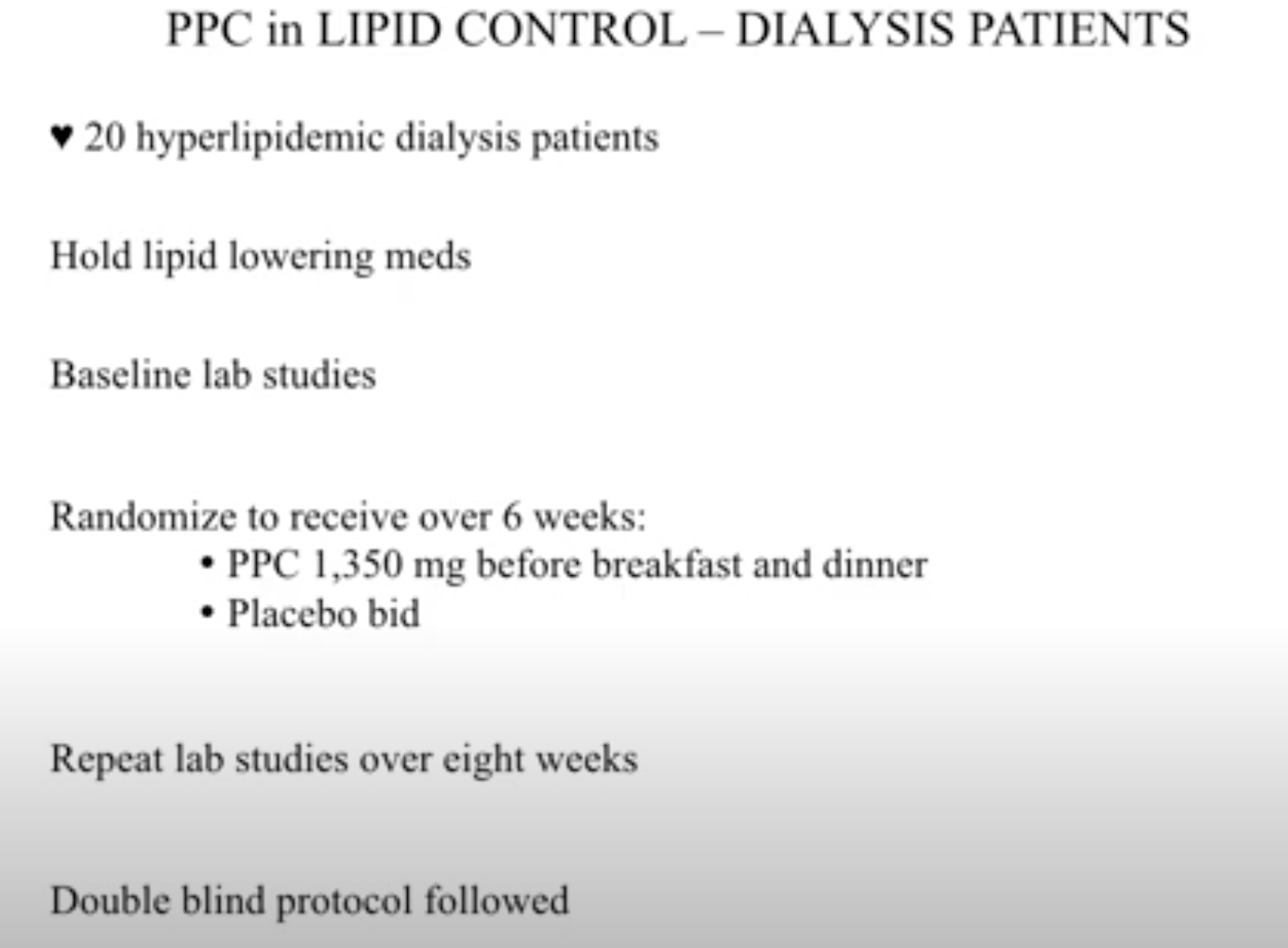
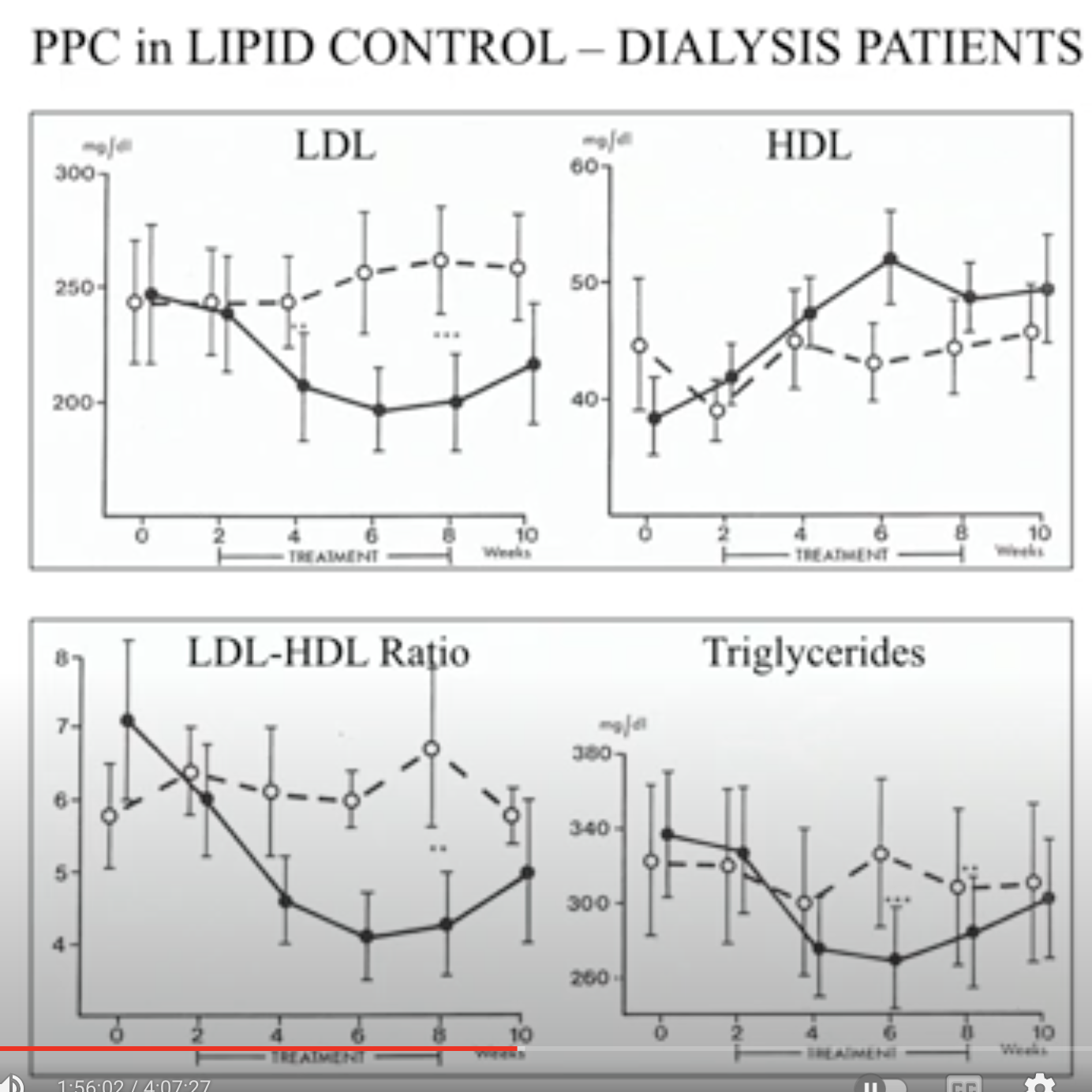
Reduction of hyperlipidemia with 3-sn-polyenyl-phosphatidylcholine in dialysis patients, 1989
Hyperlipidemia is of particular concern in dialysis patients due to the high incidence of ischemic cardiovascular complications. Two groups of 10 patients with at least one year of dialysis and a residual glomerular filtration rate less than 1 ml/min, serum cholesterol greater than 260 mg/dl, LDL cholesterol greater than 180 mg/dl and triglycerides greater than 200 mg/dl were admitted to the study. The patients received either 3 x 450 mg 3-sn-polyenyl-phosphatidylcholine (PPC) mornings and evenings (2.7 g daily, 6 capsules) or placebo during the double-blind, randomized study. Six weeks treatment was followed by a two-week wash-out phase. Lipid parameters including total cholesterol, triglycerides, HDL and LDL cholesterol were determined 14 days before treatment, at treatment begin, at 2, 4 and 6 weeks during treatment and 14 days after treatment cessation. PPC caused a significant decrease in total cholesterol (-37.8 mg/dl) two weeks after treatment begin (2 p less than 0.001). This decrease remained constant during the duration of treatment. Two weeks after PPC application a decrease in LDL-cholesterol had occurred (-32.0 mg/dl) (2 p less than 0.01) as compared to stable placebo values. Significant PPC induced decreases in triglycerides occurred four (-58.2 mg/dl; 2 p less than 0.001) and six weeks (-43.3 mg/dl; 2 p less than 0.01) after initiation of treatment, as compared to the placebo group (four weeks: +5.7 mg/dl and six weeks: -11.4 mg/dl). Side effects in the PPC group were equivalent to those reported in the placebo group. This study shows that PPC is an effective antihyperlipidemic agent in dialysis patients.
Polyenylphosphatidylcholine improves the lipoprotein profile in diabetic patients, 1994
Patients with diabetes mellitus commonly exhibit pathological lipoprotein profiles and concomitant cardiovascular or peripheral atherosclerotic complications. Thirty non-insulin-dependent diabetics with secondary hyperlipidemia received 2.7 g 3-sn-polyenylphosphatidylcholine (PPC) or placebo daily, orally over a 2-month period under randomized, double-blind trial conditions, to investigate the efficacy and tolerance of the treatment. This period was followed by a one-month observation phase without investigational medication. Serum LDL cholesterol, total cholesterol, HDL cholesterol and triglycerides were determined on days 1, 14, 28, 56 and 84. After 56 days of treatment with PPC, the primary variable of effectiveness, LDL cholesterol, decreased significantly (p = 0.0174) by 17% from 191 +/- 31 to 159 +/- 36 mg/dl, whereas values did not change in the placebo group. Total cholesterol (TC) in serum decreased by 16% from 303 +/- 22 to 255 +/- 23 mg/dl with PPC. In the placebo group, only a slight decrease from 292 +/- 27 to 289 +/- 41 mg/dl occurred. Mean serum triglyceride (TG) levels fell by 9% from 194 +/- 32 to 177 +/- 27 mg/dl in the PPC group. In the control group, values increased from 193 +/- 34 to 202 +/- 41 mg/dl. The differences in LDL, TC and TG between the treatment groups were statistically significant; p = 0.0014, p = 0.0001 and p = 0.007, respectively. HDL cholesterol in serum increased 12% from 50 +/- 10 to 55 +/- 13 mg/dl after PPC application. The control group did not show any alteration of mean HDL cholesterol level at any time.(ABSTRACT TRUNCATED AT 250 WORDS)
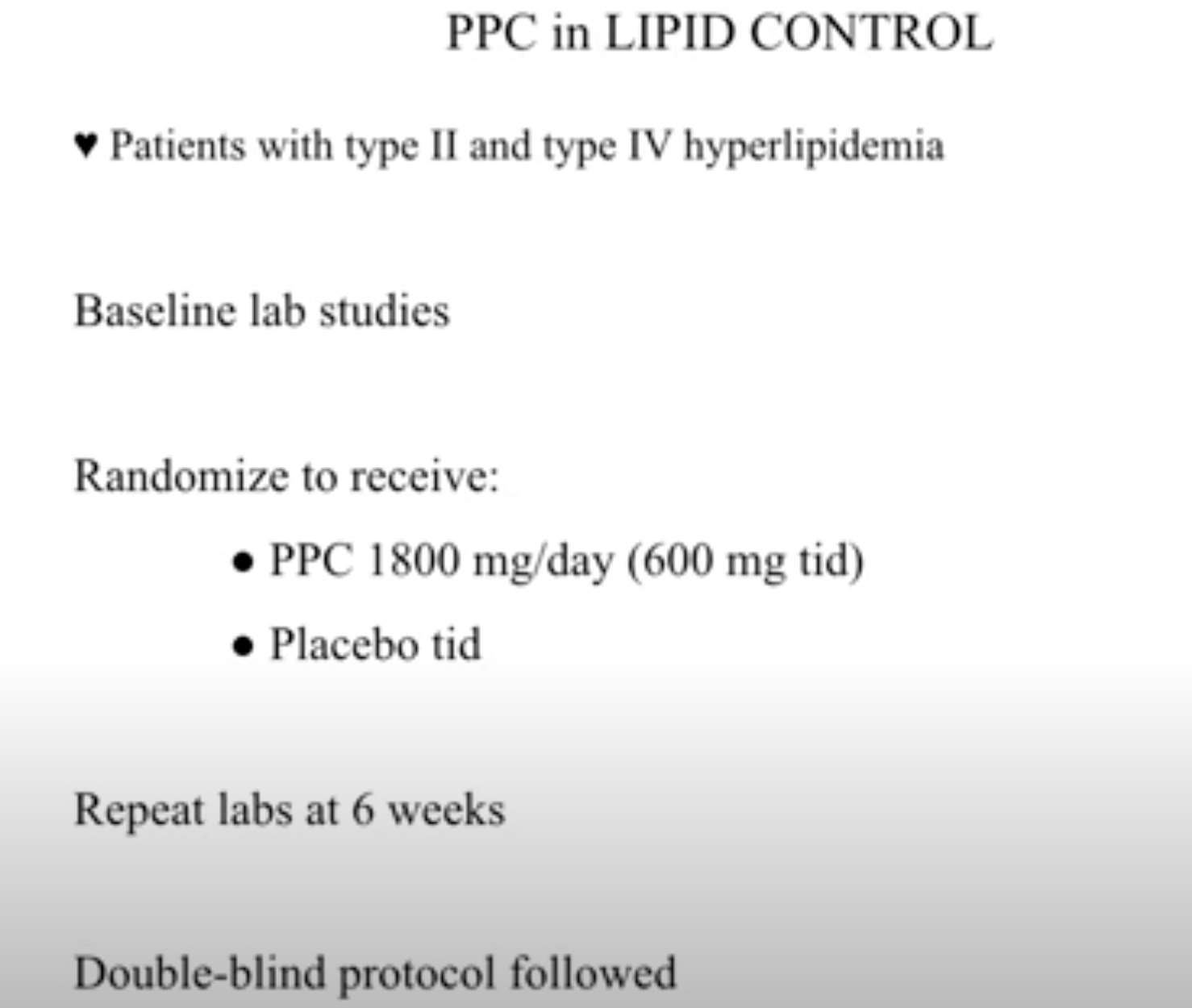
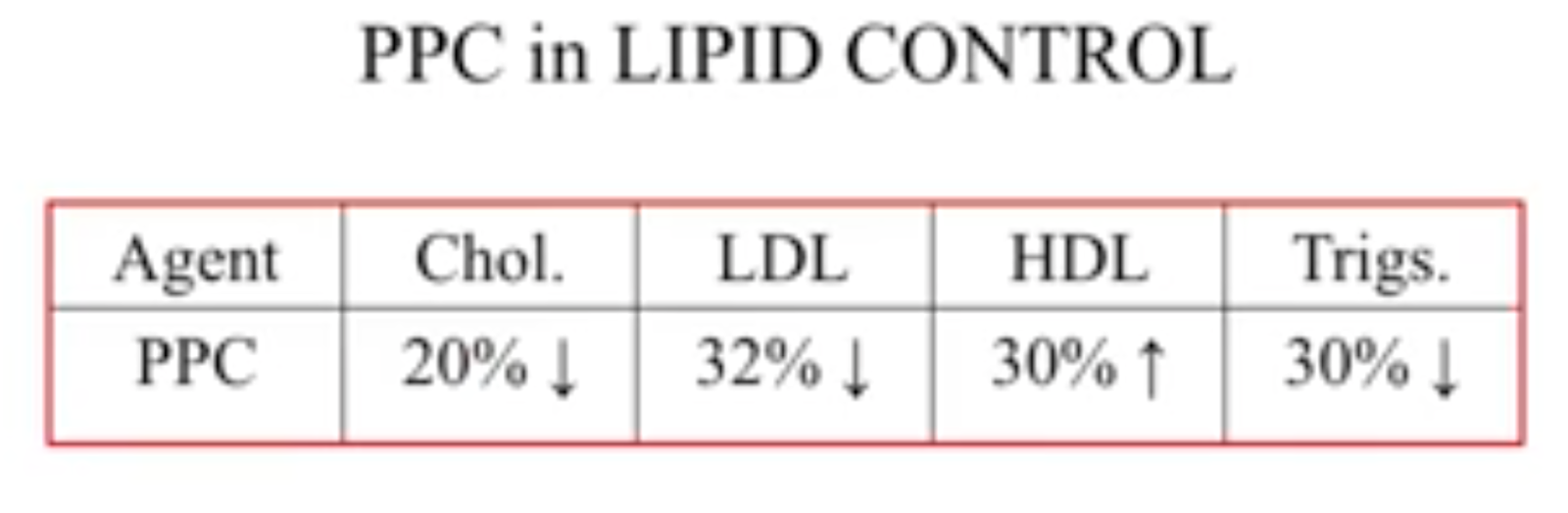
Modification of serum lipids, lipoproteins and apoproteins AI and B in patients with hyperlipidemia Type IIa and IIb using polyenylphosphatidylcholine, 1985
In a double blind study 27 patients with type II hyperlipidemia (8 IIa and 19 IIb) were treated as follows: 13 received placebo and 14 sn-polyenylphosphatidylcholin (PPC) (P 0206/1/01, Nattermann GmbH, Cologne) in a dose of three times 450 mg b.i.d. In all patients, and also in the two subclasses of patients with type IIa and type IIb hyperlipidemia, total cholesterol and LDL cholesterol were lowered significantly by PPC. The other parameters showed only minor variation. There was a downward trend in apoprotein B, triglycerides and VLDL cholesterol, and an upward trend in apoprotein AI, with virtually unchanged HDL cholesterol. None of these variations was significant compared with placebo. The fall in LDL cholesterol with unchanged HDL cholesterol caused a statistically significant decrease in the LDL cholesterol/HDL cholesterol ratio, thus supporting the hypothesis of an antiatherogenic property of PPC, as demonstrated experimentally in various animals.
Fighting Hepatitis (link)
Another study examined PPC’s effects when combined with the anti-viral medication interferon on patients with two forms of chronic hepatitis, hepatitis B and hepatitis C. Seventy-one percent of the patients treated with PPC and interferon experienced a biochemical response to therapy (as measured by a 50% or greater decrease in the liver enzyme serum alanine aminotransferase) compared to 56% of the patients treated with interferon alone. PPC was especially effective in increasing the response rate to treatment in hepatitis C patients. The researchers noted that PPC is well tolerated and may be combined with interferon therapy for chronic hepatitis.6
Dosage and Safety Concerns
A therapeutic dose of PPC ranges from 1.8 to 2.7 grams per day. PPC has no known contraindications, side effects, or interactions with medications. It also has an excellent safety profile and is generally well tolerated. The most common reported side effect is gas, which is most strongly associated with very high doses, typically 15 grams or more per day. PPC is generally considered safe in pregnancy, and choline requirements appear to be especially high in pregnant and lactating women. Pregnant and lactating women should always consult with their physicians before using PPC or other nutritional supplements.
Polyunsaturated phosphatidyl-choline and interferon alpha for treatment of chronic hepatitis B and C: a multi-center, randomized, double-blind, placebo-controlled trial, 1998
Methodology: Patients received 5 million I.U. (Hepatitis B) and 3 million I.U. (hepatitis C) interferon s.c. thrice weekly for 24 weeks, respectively, and were randomly assigned to additional oral medication with either 6 capsules of PPC (total daily dose: 1.8 g) or 6 capsules of placebo per day for 24 weeks. Biochemical response to therapy was defined as a reduction of ALT by more than 50% of pre-treatment values. The responders were treated for further 24 weeks after cessation of interferon therapy with either PPC or placebo.
Results: 176 patients completed the study protocol (per-protocol population: 92 in the PPC and 84 in the placebo group). A biochemical response (> 50% ALT reduction) was seen in 71% of patients who were treated with PPC, but only in 56% of patients who received placebo (p < 0.05). PPC increased the response rate in particular in patients with hepatitis C: 71% of those patients responded in the PPC group versus 51% in the placebo group (p < 0.05). Prolonged PPC therapy given to responders beyond the cessation of interferon therapy tended to increase the rate of sustained responders at week 48 in patients with hepatitis C (41% versus 15% in the control group; p = 0.064). In contrast, PPC did not alter the biochemical response to interferon in patients with hepatitis B. PPC did not accelerate elimination of HBV-DNA, HBeAg and HCV-RNA.
Conclusions: In conclusion, PPC may be recommended in patients with chronic hepatitis C in combination with interferon and after termination of interferon in order to reduce the high relapse rate. PPC may not be recommended for patients with chronic hepatitis B. In contrast to IFN and other antiviral agents PPC does not carry major risks and is tolerated very well.
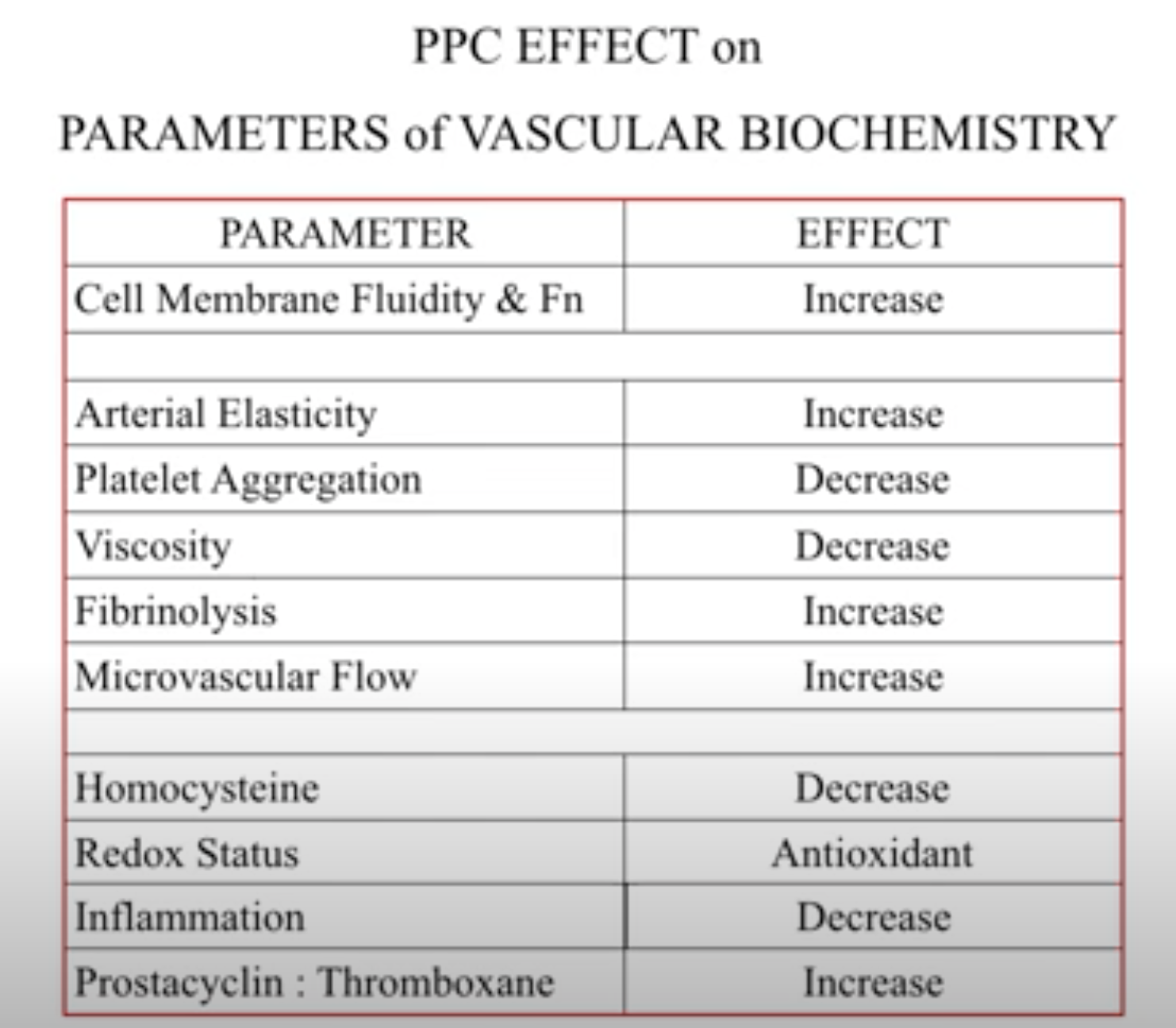
Polyenylphosphatidylcholine (PPC) in Cardiovascular Disease and Integrative Medicine - Part Two, 2018


Choline supplemented as phosphatidylcholine decreases fasting and postmethionine-loading plasma homocysteine concentrations in healthy men, 2005
Background: A high homocysteine concentration is a potential risk factor for cardiovascular disease that can be reduced through betaine supplementation. Choline is the precursor for betaine, but the effects of choline supplementation on plasma total homocysteine (tHcy) concentrations in healthy humans are unknown.
Objective: The objective was to investigate whether supplementation with phosphatidylcholine, the form in which choline occurs in foods, reduces fasting and postmethionine-loading concentrations of plasma tHcy in healthy men with mildly elevated plasma tHcy concentrations.
Design: In a crossover study, 26 men ingested ≈2.6 g choline/d (as phosphatidylcholine) or a placebo oil mixture for 2 wk in random order. Fatty acid composition and fat content were similar for both treatments. A methionine-loading test was performed on the first and last days of each supplementation period.
Results: Phosphatidylcholine supplementation for 2 wk decreased mean fasting plasma tHcy by 18% (−3.0 μmol/L; 95% CI: −3.9, −2.1 μmol/L). On the first day of supplementation, a single dose of phosphatidylcholine containing 1.5 g choline reduced the postmethionine-loading increase in tHcy by 15% (−4.8 μmol/L; 95% CI: −6.8, −2.8 μmol/L). Phosphatidylcholine supplementation for 2 wk reduced the postmethionine-loading increase in tHcy by 29% (−9.2 μmol/L; 95% CI: −11.3, −7.2 μmol/L). All changes were relative to placebo.
Conclusions: A high daily dose of choline, supplemented as phosphatidylcholine, lowers fasting as well as postmethionine-loading plasma tHcy concentrations in healthy men with mildly elevated tHcy concentrations. If high homocysteine concentrations indeed cause cardiovascular disease, choline intake may reduce cardiovascular disease risk in humans.
Skincare Benefits of Phosphatidylcholine (link)
Acne
Studies have shown PC to be very effective at treating acne. The efficacy of phosphatidylcholine from soya was evaluated in the treatment of acne vulgaris in 7 studies on 77 subjects.
77 patients with acne vulgaris grades one and two (on no other treatment for their condition) were given 1mg Phosphatidylcholine / cm2 for eight weeks. The results showed that comedones and efflorescences were significantly improved within 2 weeks and remarkably improved after 4 weeks. 64% reduction in comedones and 75% reduction of efflorescences. As well as a decrease in squalene concentration and increase linoleic acid concentration in skin surface lipids [1].
Repair Against UVB Damage
Another study found that Phosphatidylcholine helped to reduce erythema (redness) in the UVB treated skin of 31 patients skin type II and III[4]. The mechanism of action is postulated to be an effect of increasing antioxidants and the reduction of free radicals both the result of the high level of EFA’s in this liposomal material.
Wound Healing and Infections
Another study showed significantly improved life of skin grafts suggesting a nourishing skin health promoting effect of PC. Also significantly better new skin formation on wounds with PC probably due to its hydrating and skin normalising qualities. PC provides over 300% improved activity of antibacterials probably due to its penetration and protective qualities [5].
References
[1] – Ghyczy-, M, Nissen, HP & Biltz, H 1996, ‘The treatment of acne vulgaris by phosphatidylcholine from soybeans, with a high content of linoleic acid’ Journal of Applied Cosmetology, vol. 14, no. 4, pp. 137-145.
[2] – Kim C1, Shim J, Han S, Chang I. 2002, “The skin-permeation-enhancing effect of phosphatidylcholine: caffeine as a model active ingredient.” Int’l J. of Cosmetic Science, 2002 Nov-Dec;53(6):363-74.
[3] – Montenegro, L., Bonina, F., 1995 “Protective Effect Evaluation of Free radical Scavengers on UVB Induced Human Cutaneous Erythema by Skin Reflectance Spectrophotometry” Int’l J. of Cosmetic Science, 1995; 17: 91-103.
[4] – Thiele, B., Ghyczy, M., “Influence of Phospholipid Liposomes on UVB-Induced Erythema Formation”, Arch Dermatol Res, 1993; 285:428-431.
[5] – Reimer et al., “An innovative Topical Drug Formulation for Wound Healing and Infection Treatment: In vitro and in vivo Investigations of a Povidone-Iodine Liposome Hydrogel” Dermatology 2000; 201; 235-241


Comments