Cialis (Tadalafil) / PDE5 inhibitors
General health:
Tadalafil lowered BP by -3/-3 mm Hg upon daily use amongst obese (ref). A smaller BP lowering effect was seen with the general population (ref).
Extended mice & rat lifespan in a non-statistically significant fashion in safety studies (ref).
Men with prior MI or revascularization treated with PDE5 inhibitors had a 12% lower risk for all cause mortality compared with those on alprostadil (adjusted HR = 0.88; 95% CI, 0.79-0.98). (ref)
In males with T2D, there was a reduced risk of death (HR, 0.54; P = .002) associated with PDE5 inhibitors (ref)
In 40 men with metabolic syndrome, total testosterone: 360 ng/dL → 520 ng/dL after 3 months of daily 5mg tadalafil (ref).
Administration of sildenafil to 140 low-testosterone males was associated with mean total testosterone increase of 3.6 nmol/L (103 ng/dL; p < 0.001). (ref)
In 56 hypogonadal males, daily use of sildenafil and tadalafil increased testosterone blood level but the effect was greater with tadalafil than with sildenafil. (ref)
Daily tadalafil did NOT improve testosterone in nonobese and mixed men (two studies, N=43 and N=253). (ref, ref)
Cancer:
PDE5 inhibitors were shown to be effective in vivo and in vitro against most cancer types. They have immune enhancing effects against cancer (increased TIL). (ref)
Post-diagnostic use of PDE5 inhibitors is associated with a decreased risk of CRC-specific mortality (adjusted HR = 0.82, 95% CI 0.67-0.99) as well as a decreased risk of metastasis (adjusted HR = 0.85, 95% CI 0.74-0.98). (ref)
In a clinical trial, PDE-5 inhibitor tadalafil improved clinical outcome of advanced melanoma patients by enhancing antitumor immunity and showed potential application in combination with immunotherapy. (ref)
Phosphodiesterase type 5 and cancers: progress and challenges
In human renal carcinoma cell lines, suppression of PDE5 gene expression by PDE5 siRNA reduced cell proliferation and induced apoptosis through cGMP-PKG activation [273].
Phosphodiesterase-5 inhibitors use and risk for mortality and metastases among male patients with colorectal cancer, 2020
Phosphodiesterase-5 (PDE5) inhibitors are suggested to have anti-tumor effects and to inhibit surgery-induced immunosuppression. We aimed to explore whether post-diagnostic use of PDE5 inhibitors was associated with a better prognosis among male patients with colorectal cancer (CRC) and the role of open surgery in the association. Here we show that post-diagnostic use of PDE5 inhibitors is associated with a decreased risk of CRC-specific mortality (adjusted HR = 0.82, 95% CI 0.67-0.99) as well as a decreased risk of metastasis (adjusted HR = 0.85, 95% CI 0.74-0.98). Specifically, post-operative use of PDE5 inhibitors has a strong anti-cancer effect. The reduced risk of metastasis is mainly due to distant metastasis but not regional lymphatic metastasis. PDE5 inhibitors have the potential to be an adjuvant drug for patients with CRC to improve prognosis, especially those who have undergone open surgery.
PDE5 inhibition eliminates cancer stem cells via induction of PKA signaling
Cancer stem cells (CSCs) are involved in metastasis and resistance development, thus affecting anticancer therapy efficacy. The underlying pathways required for CSC maintenance and survival are not fully understood and only a limited number of treatment strategies to specifically target CSCs have been identified. To identify novel CSC targeting compounds, we here set-up an aldehyde dehydrogenase (ALDH)-based phenotypic screening system that allows for an automated and standardized identification of CSCs. By staining cancer cells for ALDH activity and applying high-content-based single-cell population analysis, the proportion of a potential CSC subpopulation with significantly higher ALDH activity (ALDHhigh) can be quantified in a heterogeneous cell population. We confirmed high ALDH activity as surrogate marker for the CSC subpopulation in vitro and validated Wnt signaling as an essential factor for the maintenance of CSCs in SUM149 breast cancer cells. In a small molecule screen, we identified phosphodiesterase type 5 (PDE5) inhibition as potential strategy to target CSC maintenance and survival in multiple cancer cell lines. CSC elimination by PDE5 inhibition was not dependent on PKG signaling, and we suggest a novel mechanism in which PDE5 inhibition leads to elevated cGMP levels that stimulate cAMP/PKA signaling to eliminate CSCs.
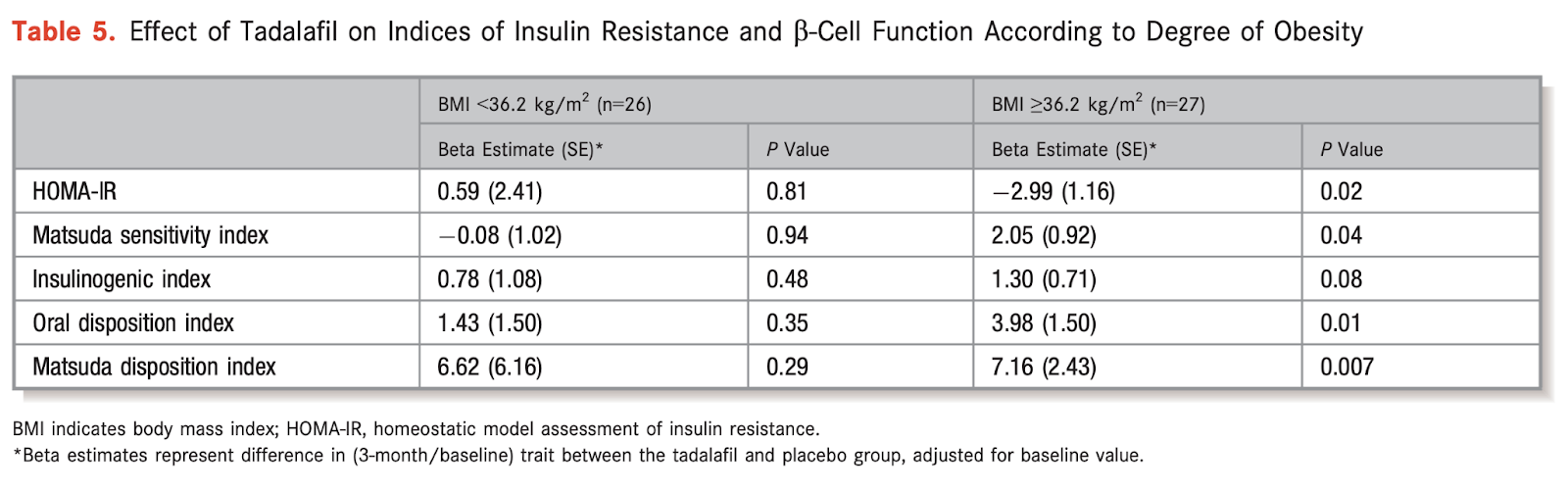
Effect of Phosphodiesterase Inhibition on Insulin Resistance in Obese Individuals
Background: Obesity is associated with cardiometabolic disease, including insulin resistance (IR) and diabetes. Cyclic guanosine monophosphate (cGMP) signaling affects energy balance, IR, and glucose metabolism in experimental models. We sought to examine effects of phosphodiesterase-5 inhibition with tadalafil on IR in a pilot study of obese nondiabetic individuals.
Methods and results: We conducted a randomized, double-blinded, placebo-controlled trial of adults age 18 to 50 years with obesity and elevated fasting insulin levels (≥10 μU/mL). Participants were randomized to tadalafil 20 mg daily or placebo for 3 months. Oral glucose tolerance tests were performed, and the effect of tadalafil on IR was examined. A total of 53 participants (mean age, 33 years; body mass index [BMI], 38 kg/m(2)) were analyzed, 25 randomized to tadalafil and 28 to placebo. In the overall sample, measures of IR did not differ between tadalafil and placebo groups at 3 months. However, in individuals with severe obesity (BMI ≥36.2 kg/m(2)), tadalafil use was associated with improved IR (homeostatic model assessment for IR), compared to placebo (P=0.02, respectively). Furthermore, one measure of β-cell compensation for IR (oral disposition index) improved with tadalafil in the overall sample (P=0.009) and in the subgroup with severe obesity (P=0.01).
Conclusion: Results of this pilot study did not show improvements in IR with tadalafil, compared to placebo. However, tadalafil may have favorable effects on β-cell compensation, particularly in individuals with severe obesity. Future studies evaluating the potential metabolic benefits of cGMP modulation in obesity are warranted.

Phosphodiesterase-5 inhibitors and their hemodynamic effects, 2006
Erectile dysfunction occurs commonly in untreated and treated hypertensive patients, impairing adherence to treatment and quality of life. Furthermore, it is a marker for enhanced risk for cardiovascular disease. Phosphodiesterase type 5 (PDE5) inhibitors, sildenafil, vardenafil, and tadalafil, provide effective treatment of erectile dysfunction. They reduce blood pressure in healthy patients: sildenafil 100 mg, -3.7/-3.6 mm Hg; vardenafil 20 mg, -7.5/-8 mm Hg; and tadalafil 20 mg, -1.6/-0.8 mm Hg. Greater declines in blood pressure with a PDE5 inhibitor may be observed in treated and untreated hypertensive patients. The additive effect of PDE5 inhibitors with one or multiple antihypertensive drugs is modest. alpha(1)-Blockers, except tamsulosin, may result in larger declines in blood pressure and cause orthostatic hypotension. Thus, caution should be exercised by using the lowest doses of proportional, variant(1)-blockers and PDE5 inhibitors in combination. Nitrates in combination with PDE5 inhibitors cause a profound decline in blood pressure and are contraindicated.
Repurposing drugs in oncology (ReDO)—selective PDE5 inhibitors as anti-cancer agents (link)
Commercially available and widely used PDE5 inhibitors sildenafil, vardenafil and tadalafil are very strong candidates for repurposing as anticancer agents. These low-cost, low-toxicity drugs show potential to be included with current and emerging standard of care treatments in oncology. The combination with immune checkpoint inhibitors or possible use as perioperative therapies are particularly compelling strategies with the potential to positively improve survival outcomes.
Summary of evidence by cancer type.
Phosphodiesterase 5 inhibitor acts as a potent agent sensitizing acute myeloid leukemia cells to 67-kDa laminin receptor-dependent apoptosis
Sildenafil prevents HDACi-induced Epstein-Barr virus reactivation through the PKG pathway in NK/T cell lymphoma; potential implications for HDACi-mediated fatal complications (link)
Tadalafil has biologic activity in human melanoma. Results of a pilot trial with Tadalafil in patients with metastatic Melanoma (TaMe), 2017
Myeloid-derived suppressor cells (MDSCs) are known to play a critical role in the suppression of T cell antitumor responses. Our preclinical data showed that the phosphodiesterase (PDE)-5 inhibitor sildenafil impaired MDSC functions, enhanced intratumoral T cell activity and prolonged survival of melanoma-bearing mice. In this study, we evaluated biologic effects, safety and efficacy of palliative treatment with the PDE-5 inhibitor tadalafil in metastatic melanoma patients. We conducted an open-label, dose de-escalation trial with tadalafil in pretreated metastatic melanoma patients. Tumor and peripheral blood samples were taken before and 4 weeks after the start of treatment. Samples were investigated by immunohistochemistry and FACS analysis, for different immune subsets with numbers of CD8+ tumor-infiltrating lymphocytes (TIL) as primary end point. Stable disease was achieved in 3/12 patients (25%). Median progression-free survival was 4.6 mo (range 0.7–7.1), median overall survival (OS) 8.5 mo (range 2.7–23.7). The treatment was well tolerated. Stable patients displayed significantly higher numbers of CD8+ TIL in the center of metastases before treatment as compared with progressive patients. Upon the therapy, they showed increased expression of ζ-chain (used as a marker of T cell activation) in CD8+ and CD4+TILs and CD8+T cells in the peripheral blood as compared with baseline. Our study suggests that the PDE-5 inhibitor tadalafil can improve clinical outcome of advanced melanoma patients by enhancing antitumor immunity and highlights its potential application in combined melanoma immunotherapy.
Cialis mice safety data (link)
PDE5 inhibition may better improve survival, outcomes in stable CAD vs. alprostadil, 2021
During a mean follow-up of 5.8 years, 26% of participants on alprostadil to treat erectile dysfunction and 14% on PDE5 inhibitors died.
Researchers observed that men with prior MI or revascularization treated with PDE5 inhibitors had a 12% lower risk for mortality compared with those on alprostadil (adjusted HR = 0.88; 95% CI, 0.79-0.98).
PDE5 inhibition for erectile dysfunction was also associated with a 19% lower risk for MI (aHR = 0.81; 95% CI, 0.7-0.93) and a 25% lower risk for HF hospitalizations compared with alprostadil (aHR = 0.75; 95% CI, 0.64-0.88).
Treatment with PDE5 inhibition compared with alprostadil only affected CV-related mortality (aHR for CV mortality = 0.83; 95% CI, 0.7-0.98; aHR for non-CV mortality = 0.92; 95% CI, 0.79-1.07), according to the study.
Phosphodiesterase-5 Inhibitors and Survival in Men With Coronary Artery Disease, 2021
Reality could be more profane. Deteriorating general health is associated with a decrease in sexual desire and activity (12,13). Therefore, a high cumulative exposure to PDE5i may have identified healthier and, therefore, sexually more active patients.
All-Cause Mortality Reduction Associated WIth Use of PDE5 Inhibitor in Type 2 Diabetes, 2016
TAKE-HOME MESSAGE
The authors evaluated 5956 men with type 2 diabetes over the course of 6.9 years in a UK retrospective cohort study to determine if on-demand PDE5 inhibitors (n = 1359) were associated with lower mortality rates. After adjusting for variables, there was a reduced risk of death (HR, 0.54; P = .002) associated with PDE5 inhibitors. There was also a reduced risk of incident myocardial infarction (P < .0001).
In this UK retrospective cohort study of type 2 diabetic men, on-demand use of PDE5 inhibitors was associated with a significant reduction in mortality and myocardial infarction.
OBJECTIVE
Experimental evidence has shown potential cardioprotective actions of phosphodiesterase type-5 inhibitors (PDE5is). We investigated whether PDE5i use in patients with type 2 diabetes, with high-attendant cardiovascular risk, was associated with altered mortality in a retrospective cohort study.
RESEARCH DESIGN AND METHODS
Between January 2007 and May 2015, 5956 men aged 40-89 years diagnosed with type 2 diabetes before 2007 were identified from anonymised electronic health records of 42 general practices in Cheshire, UK, and were followed for 6.9 years. HRs from multivariable survival (accelerated failure time, Weibull) models were used to describe the association between on-demand PDE5i use and all-cause mortality.
RESULTS
Compared with non-users, men who are prescribed PDE5is (n=1359) experienced lower percentage of deaths during follow-up (19.1% vs 23.8%) and lower risk of all-cause mortality (unadjusted HR=0.69 (95% CI: 0.64 to 0.79); p<0.001)). The reduction in risk of mortality (HR=0.54 (0.36 to 0.80); p=0.002) remained after adjusting for age, estimated glomerular filtration rate, smoking status, prior cerebrovascular accident (CVA) hypertension, prior myocardial infarction (MI), systolic blood pressure, use of statin, metformin, aspirin and β-blocker medication. PDE5i users had lower rates of incident MI (incidence rate ratio (0.62 (0.49 to 0.80), p<0.0001) with lower mortality (25.7% vs 40.1% deaths; age-adjusted HR=0.60 (0.54 to 0.69); p=0.001) compared with non-users within this subgroup.
CONCLUSION
In a population of men with type 2 diabetes, use of PDE5is was associated with lower risk of overall mortality and mortality in those with a history of acute MI.
Serum testosterone, testosterone replacement therapy and all-cause mortality in men with type 2 diabetes: retrospective consideration of the impact of PDE5 inhibitors and statins, 2016
Background: Low testosterone levels occur in over 40% of men with type 2 diabetes mellitus (T2DM) and have been associated with increased mortality. Testosterone replacement together with statins and phosphodiesterase 5 inhibitors (PDE5I) are widely used in men with T2DM.
Purpose: To determine the impact of testosterone and testosterone replacement therapy (TRT) on mortality and assess the independence of this effect by adjusting statistical models for statin and PDE5I use.
Methods: We studied 857 men with T2DM screened from five primary care practices during April 2007-April 2009. Of the 857 men, 175/637 men with serum total testosterone ≤ 12 nmol/l or free testosterone (FT) ≤ 0.25 nmol/l received TU for a mean of 3.8 ± 1.2 (SD) years. PDE5I and statins were prescribed to 175/857 and 662/857 men respectively. All-cause mortality was the primary end-point. Cox regression models were used to compare survival in the three testosterone level/treatment groups, the analysis adjusted for age, statin and PDE5I use, BMI, blood pressure and lipids.
Results: Compared with the Low T/untreated group, mortality in the Normal T/untreated (HR: 0.62, CI: 0.41-0.94) or Low T/treated (HR: 0.38, CI: 0.16-0.90) groups was significantly reduced. PDE5I use was significantly associated with reduced mortality (HR: 0.21, CI: 0.066-0.68). After repeating the Cox regression in the 682 men not given a PDE5I, mortality in the Normal T/untreated and Low T/treated groups was significantly lower than that in the reference Low T/untreated group. Mortality in the PDE5I/treated was significantly reduced compared with the PDE5I/untreated group (OR: 0.06, CI: 0.009-0.47).
Conclusions: Testosterone replacement therapy is independently associated with reduced mortality in men with T2DM. PDE5I use, included as a confounding factor, was associated with decreased mortality in all patients and, those not on TRT, suggesting independence of effect. The impact of PDE5I treatment on mortality (both HR and OR < 0.25) needs confirmation by independent studies.
How are PDE5 inhibitors metabolized?
Each PDE5 inhibitor undergoes metabolism predominantly through the hepatic isoenzyme cytochrome P450 (CYP) 3A4 pathway. Minor pathways include CYP2C9 for sildenafil, CYP3A5 and CYP2C for vardenafil, and CYP2C for avanafil.
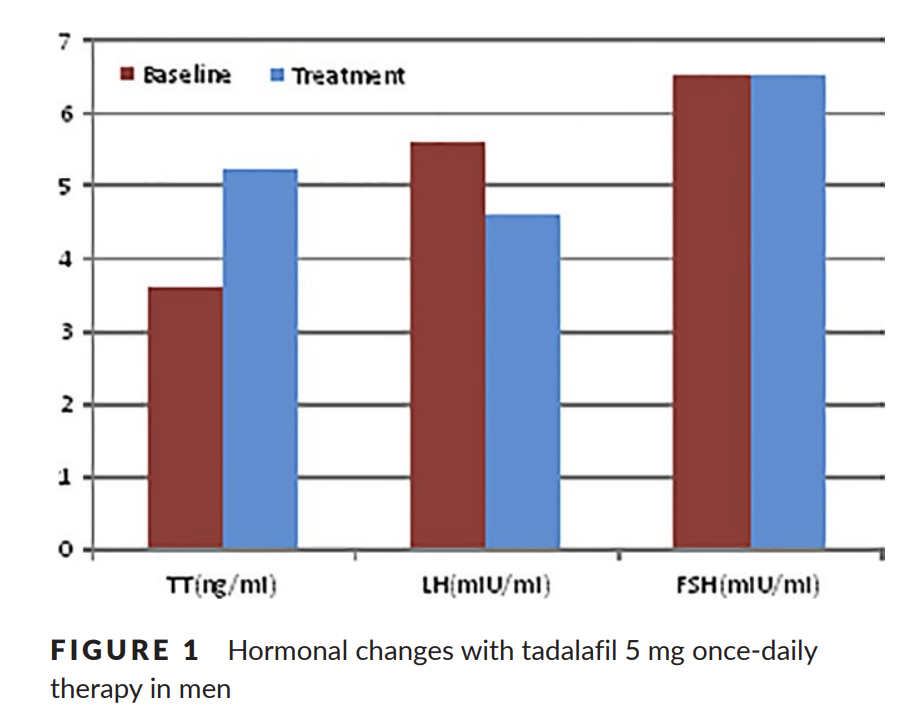
Effects of taking tadalafil 5 mg once daily on erectile function and total testosterone levels in patients with metabolic syndrome, 2017
We aimed to evaluate the efficacy of tadalafil 5 mg once-daily treatment on testosterone levels in patients with erectile dysfunction (ED) accompanied by the metabolic syndrome. A total of 40 men with metabolic syndrome were evaluated for ED in this study. All the patients received 5 mg tadalafil once a day for 3 months. Erectile function was assessed using the five-item version of the International Index of Erectile Function (IIEF) questionnaire. Serum testosterone, follicle-stimulating hormone and luteinising hormone levels were also evaluated, and blood samples were taken between 08.00 and 10.00 in the fasting state. All participants have three or more criteria of metabolic syndrome. At the end of 3 months, mean testosterone values and IIEF scores showed an improvement from baseline values (from 3.6 ± 0.5 to 5.2 ± 0.3, from 11.3 ± 1.9 to 19 ± 0.8 respectively). After the treatment, serum LH levels were decreased (from 5.6 ± 0.6 to 4.6 ± 0.5). There was significantly difference in terms of baseline testosterone and luteinising hormone values and IIEF scores (p < .05). Based on our findings, we recommend tadalafil 5 mg once daily in those men with erectile dysfunction especially low testosterone levels accompanied by metabolic syndrome.
In 40 men with metabolic syndrome, TT: 360 ng/dL → 520 ng/dL after 3 months of daily 5mg tadalafil.
Sildenafil increases serum testosterone levels by a direct action on the testes, 2018
Phosphodiesterase-5-inhibitors, such as sildenafil, increase intracavernosal cyclic guanosine monophosphate levels, which results in corporal smooth muscle relaxation and penile erection. Here, we determined the effects of sildenafil administration on the hypo-thalamic-pituitary-gonadal axis in men with erectile dysfunction and low testosterone levels. The Testosterone and Erectile Dysfunction trial (ClinicalTrials.gov # NCT00512707) initially administered an optimized dose of sildenafil to 140 men, aged 40–70 years with erectile dysfunction, low serum total testosterone (<11.4 nmol/L; 330 ng/dL) and/or free testosterone (<173 pmol/L; 50 pg/mL) over 3–7 weeks. Sex steroids and gonadotropins were measured at baseline and after sildenafil optimization in a longitudinal study without a separate control group. Serum testosterone, dihydrotestosterone (DHT) and oestrogens were measured using liquid chromatography-tandem mass spectrometry. Administration of an optimized dose of sildenafil was associated with mean increases of 3.6 nmol/L (103 ng/dL; p < 0.001) and 110 pmol/L (31.7 pg/mL; p < 0.001) in total and free testosterone levels respectively. This was accompanied by parallel increases in serum DHT (0.17 nmol/L; 4.9 ng/dL; p < 0.001) and oestradiol (14 pmol/L; 3.7 pg/mL; p < 0.001) and significant suppression of luteinizing hormone (change −1.3 units/L; p = 0.003) levels, suggesting a direct effect at the testicular level. Androstenedione and oestrone increased by 1.3 nmol/L (38 ng/dL; p = 0.011) and 10.7 pmol/L (2.9 pg/mL; p = 0.012), respectively, supporting a possible effect of sildenafil on adrenal steroidogenesis. In conclusion, sildenafil administration was associated with increased testosterone levels likely ascribable to a direct effect on the testis.

Evaluation of the effect of sildenafil and tadalafil on testosterone blood level, 2016
Objective
The aim of this study was to evaluate and compare the effect of sildenafil and tadalafil on testosterone blood level.
Patients and methods
Fifty-six married male patients with ED and age range 40–70 years with low–normal total testosterone level were included. Patients were randomly allocated into two groups: group I included 28 patients with ED who received 25 mg sildenafil once daily oral dose for 2 months, and group II included 28 patients with ED who received 5 mg tadalafil once daily oral dose for 2 months. Serum testosterone and luteinizing hormone (LH) levels were evaluated before starting the treatment and after 2 months of treatment.
Results
There was increased total testosterone level, a significant decrease in LH and increased post-treatment International Index of Erectile Function values in both groups. There was a significant increase in values of post-treatment total testosterone level and International Index of Erectile Function and a significant decrease in post-treatment LH in group II compared with group I.
Conclusion
In 56 hypogonadal males, daily use of sildenafil and tadalafil increased testosterone blood level but the effect was greater with tadalafil than with sildenafil.
Tadalafil improves lean mass and endothelial function in nonobese men with mild ED/LUTS: in vivo and in vitro characterization, 2017
Daily tadalafil improved lean mass content in non-obese men probably via enhanced insulin secretion, estradiol reduction, and improvement of endothelial function in vivo.
Purpose: Phosphodiesterase type-5 inhibitor administration in diabetic men with erectile dysfunction (ED) is associated with reduced waist circumference. We evaluated potential effects of daily tadalafil administration on body composition and investigated its possible mechanism(s) of action in C2C12 skeletal muscle cells in vitro.
Methods: Forty-three men on stable caloric intake (mean age 48.5 ± 7; BMI 25.5 ± 0.9 kg/m2) complaining mild ED and/or low urinary tract symptoms (LUTS) were randomly assigned to receive tadalafil (TAD) 5 mg/daily (once-a-day=OAD-TAD; n = 23) or 20 mg on-demand (on-demand=OD-TAD; n = 20) for 2 months. Primary outcomes were variations of body composition measured by Dual-energy X-ray absorptiometry; secondary outcomes were ED/LUTS questionnaire scores along with hormone (testosterone, estradiol, insulin) and endothelial function (Endopat2000) variations.
Results: OAD-TAD increased abdominal lean mass (p < 0.01) that returned to baseline after 2 months withdrawal. LUTS scores improved (p<0.01) in OD-TAD while ED scores improved (p < 0.01) in both groups. We found significant improvements in endothelial function (p < 0.05) that directly correlated with serum insulin (p < 0.01; r = 0.3641) and inversely correlated with estradiol levels (p < 0.01; r = 0.3655) even when corrected for potential confounders. Exposure of C2C12 cells upon increasing tadalafil concentrations (10-7 to 10-6 M) increased total androgen receptor mRNA and protein expression as well as myogenin protein expression after 24 and 72 h (2.8 ± 0.4-fold and 1.4 ± 0.02-fold vs. control, respectively, p < 0.05).
Conclusions: Daily tadalafil improved lean mass content in non-obese men probably via enhanced insulin secretion, estradiol reduction, and improvement of endothelial function in vivo. The in vitro increased myogenin and androgen receptor protein expression in skeletal muscle cells suggests a translational action of phosphodiesterase type-5 on this receptor.

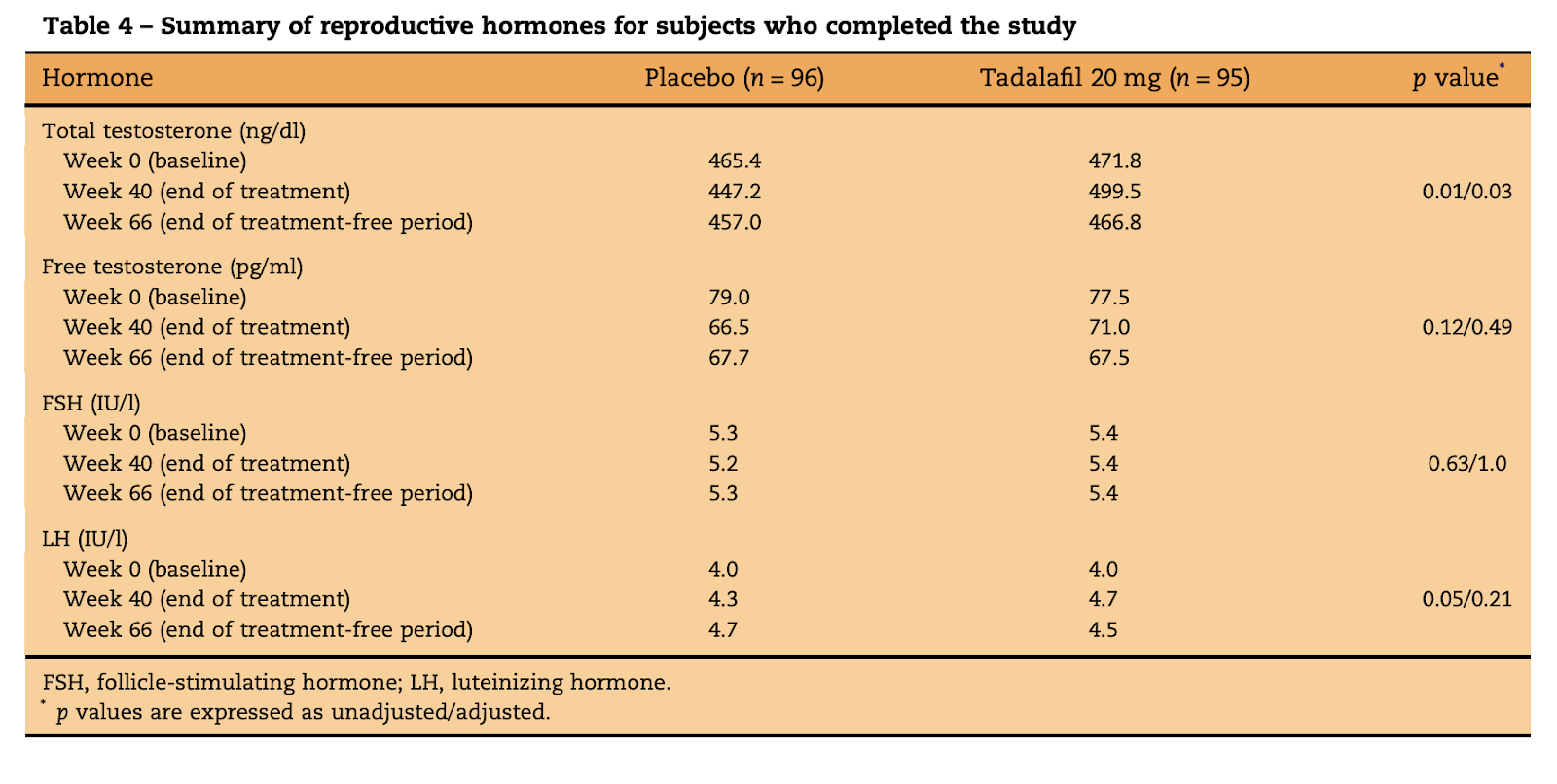
An Evaluation of Semen Characteristics in Men 45 Years of Age or Older after Daily Dosing with Tadalafil 20 mg: Results of a Multicenter, Randomized, Double-Blind, Placebo-Controlled, 9-Month Study, 2008
Objectives
Assess the effects on spermatogenesis of daily tadalafil 20 mg over three spermatogenesis cycles in men ≥ 45 yr.
Methods
In this double-blind, placebo-controlled, noninferiority study, healthy men (or with mild erectile dysfunction) were randomized to receive tadalafil 20 mg (n = 125) or placebo (n = 128) for 9 mo followed by a 6-mo, treatment-free period. Semen and serum samples were provided at baseline and every 10–12 wk. The primary outcome was the proportion of subjects with ≥ 50% reduction in sperm concentration at end point. Secondary outcomes included sperm concentration, number per ejaculate, motility and morphology; serum concentrations of testosterone, luteinizing and follicle-stimulating hormones; and tolerability.
Common treatment-emergent adverse events were headache, back pain, dyspepsia, gastroesophageal reflux disease, and myalgia. Twelve (9.6%) tadalafil and seven (5.5%) placebo subjects discontinued because of adverse events.
Conclusions
This study demonstrated no deleterious effects of 9 mo of daily tadalafil 20 mg on spermatogenesis or hormones related to testicular function in men ≥ 45 yr.
Correcting imbalance of sex hormones by a phosphodiesterase 5 inhibitor improves copulatory dysfunction in male rats with type 2 diabetes, link
After 12 weeks of tadalafil treatment, levels of testosterone were significantly increased both in OLETF-tadalafil and LETO-tadalafil groups versus vehicle groups. Tadalafil decreased estradiol levels both in OLETF and LETO rats. Furthermore, tadalafil increased serum LH levels with a reduction of proinflammatory cytokines.


Comments