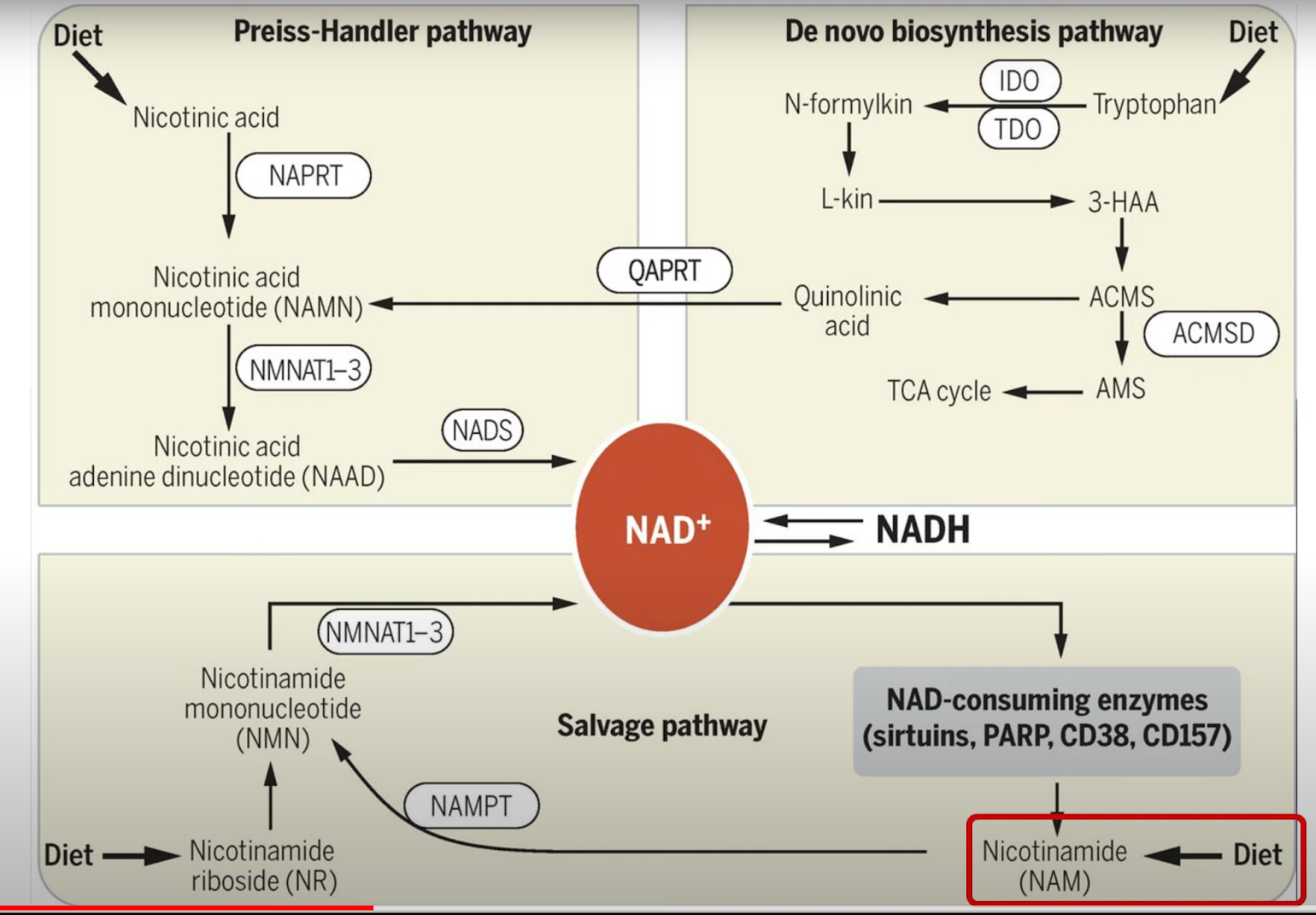
NAD+ Boosters
Niacin
Niacin extended release 2g/day reduced liver fat by 47% and visceral fat by 6.3% in a human study with 39 adults with hypertriglyceridemia.
Niacin inhibits and reverses hepatic steatosis and inflammation in animals and liver cell cultures. It prevents liver fibrosis in animals and decreases collagen in cultured human stellate cells.
Boosts muscle and blood NAD+.
Deficiency of NAD+ creates genomic instability (or rather leads to downgrading of p53 DNA repair enzymes)
5yrs niacin treatment extended human lifespan by ~1 yr (a delayed effect was seen).
Niacin may increase glucose and insulin levels.
[Fixes fatty liver; makes your body as it should. Lowers platelets by 10-20%. Increases fasting insulin, wonder if that’s because of Glycine depletion]
Niacin for treatment of nonalcoholic fatty liver disease (NAFLD): novel use for an old drug? 2019
Hu et al examined the effect of niacin extended-release (Niacin ER, trade name: Niaspan) on liver fat content in 39 adult patients with hypertriglyceridemia in an uncontrolled clinical trial. All patients were treated with niacin ER, gradually increasing the dose to 2 g/d for a total of 23 weeks (5.3 months). There were significant (P < .001) reductions in liver fat content (−47.2 ± 32.8%) and visceral fat (−6.3 ± 15.8%, P < .05) after niacin treatment. Mean body weight decreased by 1.46% of baseline during the study. The liver fat decrease remained statistically significant after adjustment for age, gender, and body weight changes. Statistically significant decreases from the baseline in liver enzymes ALT, GGT, alkaline phosphatase, and C-reactive protein (CRP) were observed.
Niacin inhibits and reverses hepatic steatosis and inflammation in animals and liver cell cultures. It prevents liver fibrosis in animals and decreases collagen in cultured human stellate cells.


Great summary of Niacin research.
https://www.youtube.com/watch?v=u6Iy5eK02s0
Cancer (link)
Studies of cultured cells (in vitro) provide evidence that NAD content influences mechanisms that maintain genomic stability. Loss of genomic stability, characterized by a high rate of damage to DNA and chromosomes, is a hallmark of cancer (42). The current understanding is that the pool of NAD is decreased during niacin deficiency and that it affects the activity of NAD-consuming enzymes rather than redox and metabolic functions (43). Among NAD-dependent reactions, poly ADP-ribosylations catalyzed by PARP enzymes (ARTDs) are critical for the cellular response to DNA injury. After DNA damage, PARPs are activated; the subsequent poly ADP-ribosylations of a number of signaling and structural molecules by PARPs were shown to facilitate DNA repair at DNA strand breaks (44). Cellular depletion of NAD has been found to decrease levels of the tumor suppressor protein p53, a target for poly ADP-ribosylation, in human breast, skin, and lung cells (45). The expression of p53 was also altered by niacin deficiency in rat bone marrow cells (46). Impairment of DNA repair caused by niacin deficiency could lead to genomic instability and drive tumor development in rat models (47, 48). Both PARPs and sirtuins have been recently involved in the maintenance of heterochromatin, a chromosomal domain associated with genome stability, as well as in transcriptional gene silencing, telomere integrity, and chromosome segregation during cell division (49, 50). Neither the cellular NAD content nor the dietary intake of NAD precursors necessary for optimizing protective responses following DNA damage has been determined, but both are likely to be higher than that required for the prevention of pellagra.
Bone marrow
Cancer patients often suffer from bone marrow suppression following chemotherapy, given that bone marrow is one of the most proliferative tissues in the body and thus a primary target for chemotherapeutic agents. Niacin deficiency was found to decrease bone marrow NAD and poly-ADP-ribose levels and increase the risk of chemically induced leukemia in rats (51). Conversely, a pharmacologic dose of either nicotinic acid or nicotinamide was able to increase NAD and poly ADP-ribose in bone marrow and decrease the development of leukemia in rats (52). It has been suggested that niacin deficiency often observed in cancer patients could sensitize bone marrow tissue to the suppressive effect of chemotherapy. However, little is known regarding cellular NAD levels and the prevention of DNA damage or cancer in humans. One study in two healthy individuals involved elevating NAD levels in blood lymphocytes by supplementation with 100 mg/day of nicotinic acid for eight weeks. Compared to non-supplemented individuals, the supplemented individuals had reduced DNA strand breaks in lymphocytes exposed to free radicals in a test tube assay (53). However, nicotinic acid supplementation of up to 100 mg/day for 14 weeks in 21 healthy smokers failed to provide any evidence of a decrease in cigarette smoke-induced genetic damage in blood lymphocytes compared to placebo (54). More recently, the frequency of chromosome translocation was used to evaluate DNA damage in peripheral blood lymphocytes of 82 pilots chronically exposed to ionizing radiation, a known human carcinogen. In this observational study, the rate of chromosome aberrations was significantly lower in subjects with higher (28.4 mg/day) compared to lower (20.5 mg/day) dietary niacin intake (55). Higher availability of NAD+ in X-irradiated peripheral blood lymphocytes was found to favor DNA repair by enhancing survival, particularly through SIRT-mediated p53 deacetylation (56).
Upper digestive tract
Generally, relationships between dietary factors and cancer are established first in epidemiological studies and followed up by basic cancer research at the cellular level. In the case of niacin, research on biochemical and cellular aspects of DNA repair has stimulated an interest in the relationship between niacin intake and cancer risk in human populations (57). A large case-control study found increased consumption of niacin, along with antioxidant nutrients, to be associated with decreased incidence of oral (mouth), pharyngeal (throat), and esophageal cancers in northern Italy and Switzerland. An increase in daily niacin intake of 6.2 mg was associated with about a 40% decrease in cases of cancers of the mouth and throat, while a 5.2 mg increase in daily niacin intake was associated with a similar decrease in cases of esophageal cancer (58, 59).
Skin
Niacin deficiency can lead to severe sunlight sensitivity in exposed skin. Given the implication of NAD-dependent enzymes in DNA repair, there has been some interest in the effect of niacin on skin health. In vitro and animal experiments have helped gather information, but human data on niacin/NAD status and skin cancer are very limited. One study reported that niacin supplementation decreased the risk of ultraviolet light (UV)-induced skin cancers in mice, despite the fact that mice convert tryptophan to NAD more efficiently than rats and humans and thus do not get severely deficient (60). Hyper-proliferation and impaired differentiation of skin cells can alter the integrity of the skin barrier and increase the occurrence of pre-malignant and malignant skin conditions. A protective effect of niacin was suggested by topical application of myristyl nicotinate, a niacin derivative, which successfully increased the expression of epidermal differentiation markers in subjects with photodamaged skin (61). The activation of the nicotinic acid receptors, GPR109A and GPR109B, by pharmacologic doses of niacin could be involved in improving skin barrier function. Conversely, differentiation defects in skin cancer cells were linked to the abnormal cellular localization of defective nicotinic acid receptors (62). Nicotinamide restriction with subsequent depletion of cellular NAD was shown to increase oxidative stress-induced DNA damage in a precancerous skin cell model, implying a protective role of NAD-dependent pathways in cancer (63). Altered NAD availability also affects sirtuin expression and activity in UV-exposed human skin cells. Along with PARPs, NAD-consuming sirtuins could play an important role in the cellular response to photodamage and skin homeostasis (64).
A pooled analysis of two large US prospective cohort studies that followed 41,808 men and 72,308 women for up to 26 years suggested that higher versus lower intake of niacin (from diet and supplements) might be protective against squamous-cell carcinoma but not against basal-cell carcinoma and melanoma (65). A phase III, randomized, double-blind, placebo-controlled trial in 386 subjects with a history of nonmelanoma skin cancer recently examined the effect of daily nicotinamide supplementation (1 g) for 12 months on skin cancer recurrence at three-month intervals over an 18-month period (66). Nicotinamide effectively reduced the rate of premalignant actinic keratose (-11%), squamous-cell carcinoma (-30%), and basal-cell carcinoma (-20%) compared to placebo after 12 months, yet this protection was not sustained during the six-month post-supplementation period (66). Larger trials are needed to assess whether nicotinamide could reduce the risk of melanomas, which are not as common as other skin cancer but are more deadly (67).
Niacin Cures Systemic NAD+ Deficiency and Improves Muscle Performance in Adult-Onset Mitochondrial Myopathy (link)
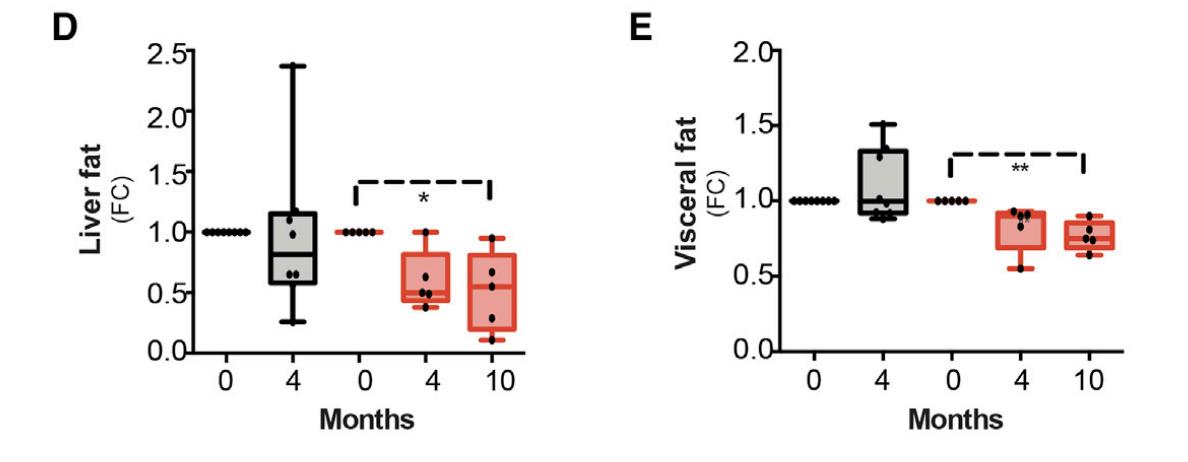
We administered an increasing dose of NAD+ booster niacin, a vitamin B3 form (to 750–1,000 mg/day) for patients and their matched controls for 10 or 4 months, respectively. Blood NAD+ increased in all subjects, up to 8-fold, and muscle NAD+ of patients reached the level of their controls. In patients, muscle metabolome shifted toward controls and liver fat decreased even 50%.

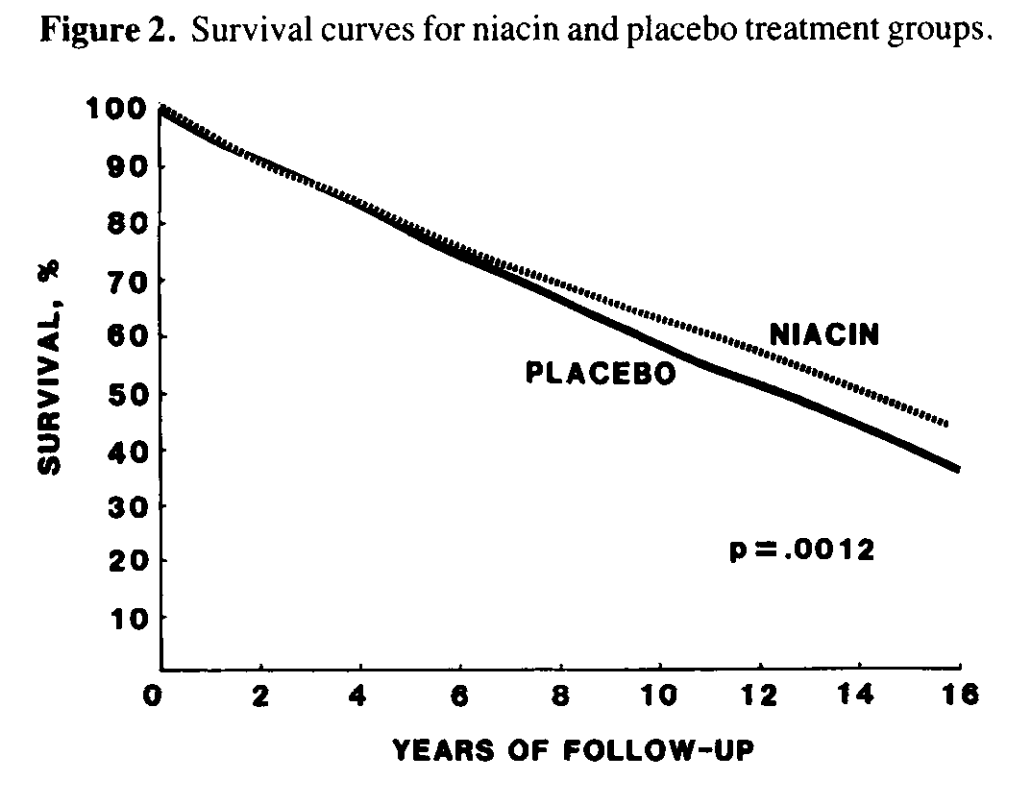
Fifteen Year Mortality in Coronary Drug Project Patients: Long-Term Benefit With Niacin (link)
The Coronary Drug Project was conducted between 1966 and 1975 to assess the long-term efficacy and safety of five lipid-influencing drugs in 8,341 men aged 30 to 64
years with electrocardiogram-documented previous myocardial infarction. The two estrogen regimens and dextrothyroxine were discontinued early because of adverse effects. No evidence of efficacy was found for the clofibrate treatment. Niacin treatment showed modest benefit in decreasing definite nonfatal recurrent myocardial infarction but did not decrease total mortality. With a mean follow-up of 15 years, nearly 9 years after termination of the trial, mortality from all causes in each of the drug groups, except for niacin, was similar to that in the placebo group. Mortality in the niacin group was 11% lower than in the placebo group (52.0 versus 58.2%; p =0.0004). This late benefit of niacin, occurring after discontinuation of the drug, may be a result of a translation into a mortality benefit over subsequent years of the early favorable effect of niacin in decreasing nonfatal reinfarction or a result of the cholesterol-lowering effect of niacin, or both.
Niacin for cholesterol (link)
In the doses needed to improve cholesterol, niacin is a drug and a potent drug at that. On average, it can lower LDL ("bad") cholesterol levels by 10%-25%. The statins and other lipid-lowering drugs can do even better, but niacin outshines them all for lowering triglyceride levels (down 20%-50%) and raising HDL ("good") cholesterol levels (up 15%-35%).
Niacin is actually the granddaddy of cholesterol-lowering drugs. It was the first medication to lower cholesterol levels (1955), the first to reduce heart attacks (1984), and the first to lower long-term mortality rates (1986).
Avoid "no-flush" preparations; they don't cause flushing, but they don't lower cholesterol, either. Best of all, perhaps, ask your doctor to prescribe Niaspan, the only FDA-approved, intermediate-release, prescription brand of niacin. It is much more expensive than over-the-counter niacin, but it's usually covered by prescription drug insurance plans. Doctors usually start with a single 500-mg tablet at bedtime, then double or triple the bedtime dose if necessary.
The Lifespan Extension Ability of Nicotinic Acid Depends on Whether the Intracellular NAD+ Level Is Lower than the Sirtuin-Saturating Concentrations
Calorie restriction can extend lifespan by increasing intracellular nicotinamide adenine dinucleotide (NAD+), thereby upregulating the activity of sirtuins (Caenorhabditis elegans Sir-2.1; human SIRT1). Nicotinic acid (NA) can be metabolized to NAD+; however, the calorie restriction mimetic (CRM) potential of NA is unclear. This study explored the ability and mechanism of NA to extend the lifespan of human Hs68 cells and C. elegans. We found that NA can efficiently increase the intracellular NAD+ levels in Hs68 cells and C. elegans; however, NA was only able to extend the lifespan of C. elegans. The steady-state NAD+ level in C. elegans was approximately 55 µM. When intracellular NAD+ was increased by a mutation of pme-1 (poly (ADP-ribose) metabolism enzyme 1) or by pretreatment with NAD+ in the medium, the lifespan extension ability of NA disappeared. Additionally, the saturating concentration of NAD+ required by SIRT1 was approximately 200 µM; however, the steady-state concentration of NAD+ in Hs68 cells reached up to 460 µM. These results demonstrate that the lifespan extension ability of NA depends on whether the intracellular level of NAD+ is lower than the sirtuin-saturating concentration in Hs68 cells and in C. elegans. Thus, the CRM potential of NA should be limited to individuals with lower intracellular NAD+.
Niacin causes insulin resistance
https://examine.com/supplements/vitamin-b3/
Likely Ineffective: Heart Disease
Multiple older studies have indicated the potential of niacin – alone or in combination with other treatment options – to prevent heart disease and reduce related mortality [27, 28, 29, 30].
However, more recent trials and comprehensive clinical reviews (over 39,000 patients included) failed to confirm these findings [12, 13, 31, 32].
Niacin improves muscle NAD+ levels, reduces visceral fat & other effects:
https://www.youtube.com/watch?v=u6Iy5eK02s0
NMN & NR Don’t Work In Humans? Alarming Research (i.e. they don’t increase tissue NAD+, while Niacin does!!)
https://www.youtube.com/watch?v=Q9U33Vqg3a4
Niacin Cures Systemic NAD + Deficiency and Improves Muscle Performance in Adult-Onset Mitochondrial Myopathy
https://pubmed.ncbi.nlm.nih.gov/32386566/
NAD+ is a redox-active metabolite, the depletion of which has been proposed to promote aging and degenerative diseases in rodents. However, whether NAD+ depletion occurs in patients with degenerative disorders and whether NAD+ repletion improves their symptoms has remained open. Here, we report systemic NAD+ deficiency in adult-onset mitochondrial myopathy patients. We administered an increasing dose of NAD+-booster niacin, a vitamin B3 form (to 750-1,000 mg/day) for patients and their matched controls for 10 or 4 months, respectively. Blood NAD+ increased in all subjects, up to 8-fold, and muscle NAD+ of patients reached the level of their controls. Some patients showed anemia tendency, while muscle strength and mitochondrial biogenesis increased in all subjects. In patients, muscle metabolome shifted toward controls and liver fat decreased even 50%. Our evidence indicates that blood analysis is useful in identifying NAD+ deficiency and points niacin to be an efficient NAD+ booster for treating mitochondrial myopathy.
Niacin May Slow Chronic Kidney Disease (CKD) Progression
A team led by Csaba P. Kovesdy, MD, of the Memphis Veterans Affairs Medical Center and the University of Tennessee Health Science Center in Memphis, found that niacin treatment was associated with a significant decrease in the proportion of patients with rapid decline in estimated glomerular filtration rate (eGFR) and a significant decrease in all-cause mortality, after adjusting for baseline demographic and comorbidity factors.
Dysfunctional high-density lipoprotein (HDL), increased reactive oxygen species, inflammation, endothelial dysfunction, hypertriglyceridemia, and hyperphosphatemia have been associated with rapid eGFR decline and increased adverse events, the researchers noted.
The cohort had normal baseline eGFR in 2005–2006. Of the 3,353,461 veterans in the cohort, 119,891 were prescribed niacin during 2005–2006. The researchers examined baseline use of niacin with slopes of eGFR over a median follow-up of 7.7 years.
In the total cohort, 9.3% of patients had rapid decline in kidney function (eGFR decline less than −5 mL/min/1.73 m2 per year). In a fully adjusted model, the niacin group had a significant 10% decreased odds of an eGFR slope less than −5 mL/min/1.73 m2 per year.
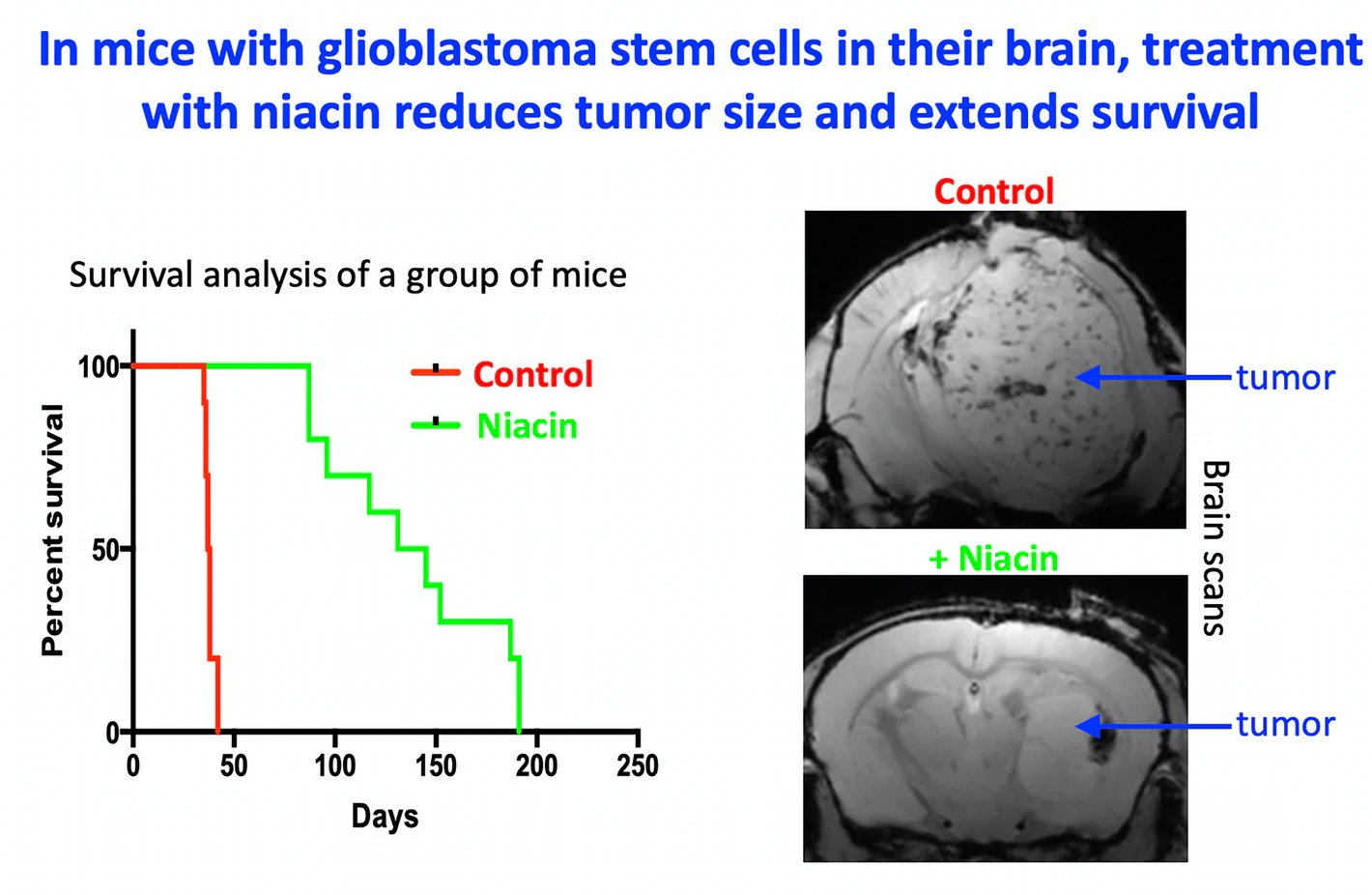
Study: Niacin may help immune system battle a deadly brain tumor
A new study by members of the Cumming School of Medicine (CSM) at the University of Calgary finds niacin, commonly called vitamin B3, combined with chemotherapy can help immune cells attack glioblastoma (a type of brain tumor), dramatically slowing progression of the disease, in mice. The results published in Science Translational Medicine found the lifespan of mice with glioblastoma that received combination therapy tripled, increasing to 150 days from 40 days.
In the study, the researchers found that niacin therapy alone extended survival and that the combination therapy with temozolomide (a chemotherapy drug commonly used against glioblastoma) markedly prolonged survival by stimulating and re-educating immune cells to stop helping the cancer and instead, destroy it.
"We were able to help immune cells do what they're supposed to do, attack and kill cancer cells," says Dr. Susobhan Sarkar, Ph.D., first author on the study. "We screened 1,040 compounds and found niacin had the properties needed to activate immune cells, specifically myeloid cells, and inhibit the growth of brain tumor initiating stem cells."
https://medicalxpress.com/news/2020-04-niacin-immune-deadly-brain-tumor.html
Control of brain tumor growth by reactivating myeloid cells with niacin (link)
An old vitamin’s new tricks
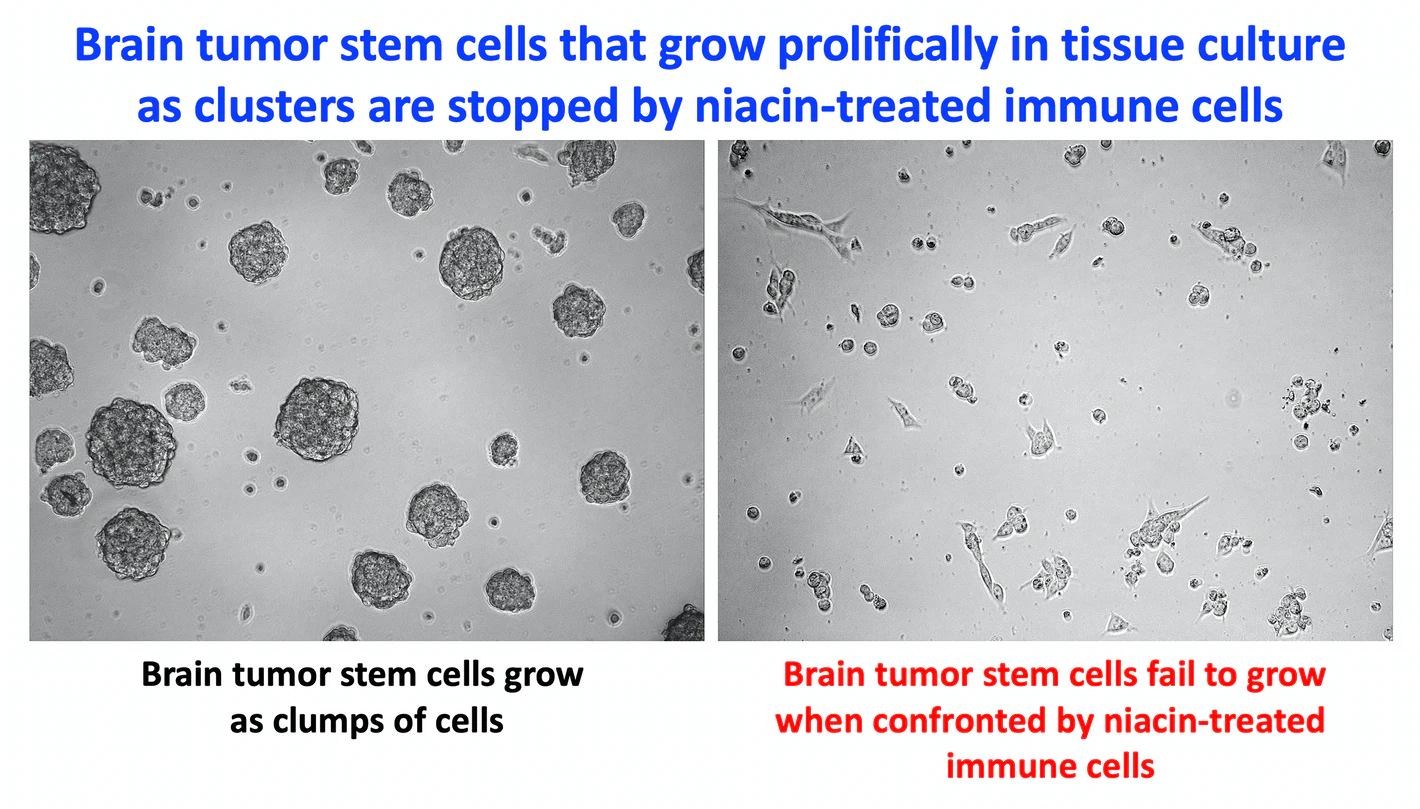
Although innate immune cells are typically present inside tumors, they often have an inactive phenotype such that they are ineffective at killing the cancer cells or even promote tumor growth. Sarkar et al. discovered that it may be possible to reprogram these cells to a more active type using niacin (vitamin B3). The authors showed that niacin-exposed monocytes can inhibit the growth of brain tumor–initiating cells. Moreover, niacin treatment of intracranial mouse models of glioblastoma increased monocyte and macrophage infiltration into the tumors, stimulated antitumor immune responses, and extended the animals’ survival, especially when combined with the chemotherapeutic drug temozolomide.
Abstract
Glioblastomas are generally incurable partly because monocytes, macrophages, and microglia in afflicted patients do not function in an antitumor capacity. Medications that reactivate these macrophages/microglia, as well as circulating monocytes that become macrophages, could thus be useful to treat glioblastoma. We have discovered that niacin (vitamin B3) is a potential stimulator of these inefficient myeloid cells. Niacin-exposed monocytes attenuated the growth of brain tumor–initiating cells (BTICs) derived from glioblastoma patients by producing anti-proliferative interferon-α14. Niacin treatment of mice bearing intracranial BTICs increased macrophage/microglia representation within the tumor, reduced tumor size, and prolonged survival. These therapeutic outcomes were negated in mice depleted of circulating monocytes or harboring interferon-α receptor–deleted BTICs. Combination treatment with temozolomide enhanced niacin-promoted survival. Monocytes from glioblastoma patients had increased interferon-α14 upon niacin exposure and were reactivated to reduce BTIC growth in culture. We highlight niacin, a common vitamin that can be quickly translated into clinical application, as an immune stimulator against glioblastomas.
* A “REMARKABLE” FINDING LINKS A COMMON VITAMIN TO FIGHTING BRAIN CANCER (link)
WHY GLIOBLASTOMA IS SO AGGRESSIVE — What makes glioblastoma so good at resisting treatment is thought to be attributable to a subpopulation of cells, called brain tumor-initiating cells, or BTICs. These cells possess “stem cell-like” properties, and are extremely adept at regrowing.
Additionally, when immune cells, such as macrophages, microglia, and monocytes, enter the tumor to try and take it down, these stem cell-like cells overthrow them – and the immune cells ultimately end up promoting tumor growth.
In a cell culture experiment, the research team found that, when treated with niacin, monocytes that had been taken from glioblastoma patients were spurred back into action – they were once again able to quash the growth of the BTICs. With the help of niacin, these immune cells regained the ability to fight off the cancer-generating potential of the brain tumor stem cells.
Using mouse models that had been implanted with BTICs derived from human patients to form glioblastomas, they tested how effective niacin worked in vivo. When they treated the mice with the vitamin compound, they found that the growth of the brain tumor was brought under control, and the lifespan of the mice greatly extended. When temozolomide — chemotherapy used to treat brain tumors — was used in combination with the niacin, these effects were enhanced even more.
{Wee Yong says the realization that niacin works in mice serves as a step forward towards finding a way to control cancer. He hopes that other advances will build upon the discovery, “so as to overcome the incurable glioblastoma”.
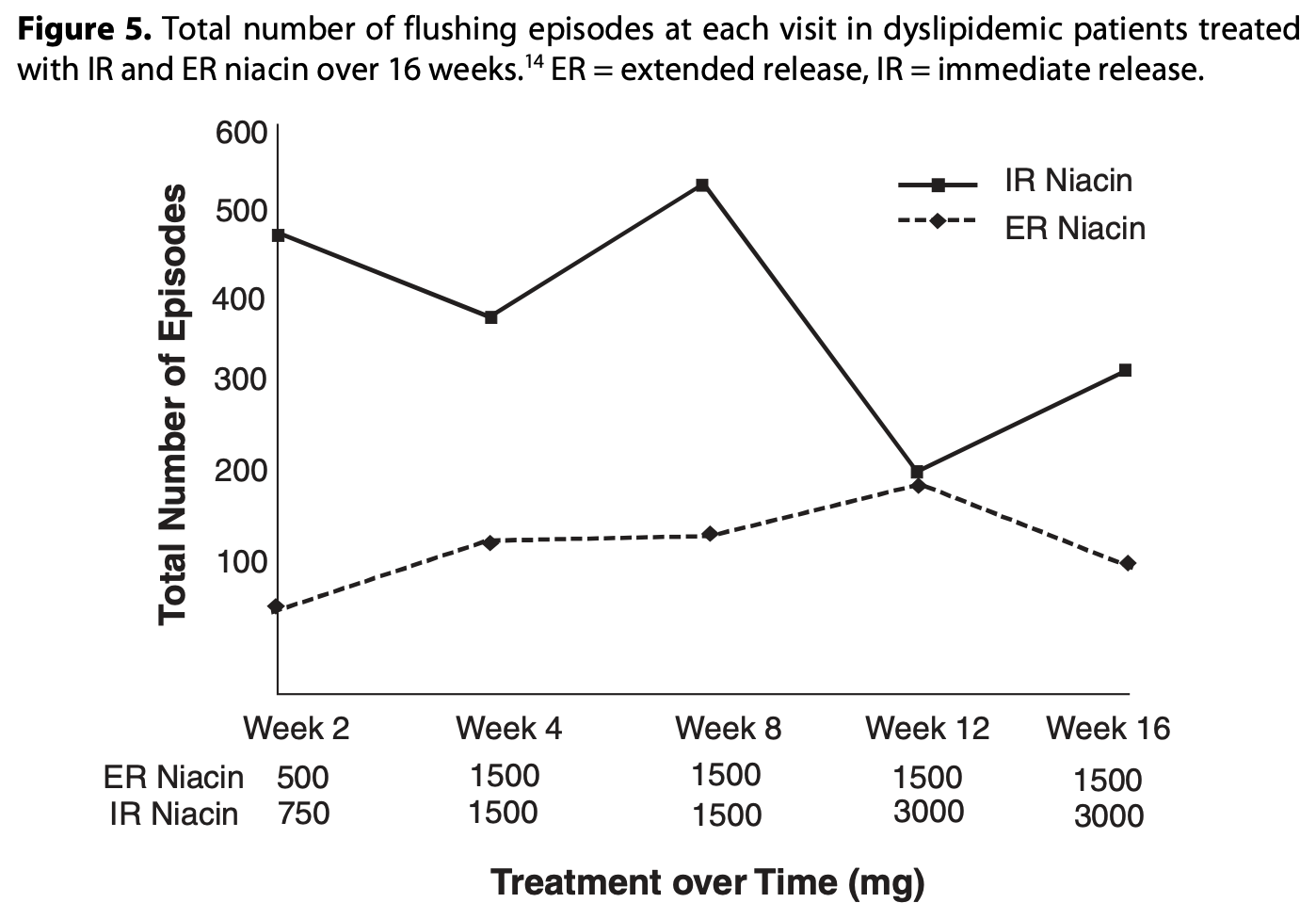
Effects of Niacin on Glucose Control in Patients With Dyslipidemia
Niacin (nicotinic acid), the most effective available pharmacotherapy for increasing high-density lipoprotein cholesterol, also lowers triglycerides and hence may be useful, alone or in combination with hydroxymethylglutaryl coenzyme A reductase inhibitors (statins), to offset residual cardiovascular risk in patients with mixed or diabetic dyslipidemia. We conducted a review of published consensus guidelines since 2000 and an English-language PubMed search of prospective, randomized controlled trials and open-label studies from January 1, 1990, through December 31, 2007, concerning the effects of niacin, alone or in combination with statins, on glycemic regulation in dyslipidemic patients (with or without diabetes mellitus). For search terms, we used the title words niacin or nicotinic acid and key words including diabetes, diabetic, dyslipidemia, glucose, glycemic, HbA1c, hemoglobin, hyperglycemia, human, insulin, postprandial, and safety. Retrospective and observational studies, case reports, and case studies were excluded. On the basis of our analysis, the effects of niacin (< or =2.5 g/d), alone or in combination with statins, on fasting glucose (an increase of 4%-5%) and hemoglobin A1c levels (an increase of < or =0.3%) are modest, transient or reversible, and typically amenable to adjustments in oral hypoglycemic regimens without discontinuing niacin. Niacin therapy was infrequently associated with incident diabetes or the need for new insulin prescriptions. Studies showed important clinical benefits of niacin or niacin-statin regimens despite modest effects on glucose control. On a population basis, significant reductions in incidences of cardiovascular events and the degree of atherosclerotic progression associated with long-term niacin (or niacin-statin) therapy in patients with diabetic dyslipidemia outweigh the typically mild effects of this therapy on glycemic regulation. Consensus guidelines recommend monitoring glycemic control after initiating niacin treatment or increasing its dosage.
Niacin increased glucose, insulin, and C-peptide levels in sedentary nondiabetic postmenopausal women
The current study examined the effects of niacin and a single bout of aerobic exercise on plasma glucose, insulin, and C-peptide in sedentary, nondiabetic postmenopausal women. As a crossover design, 17 participants underwent four different trials: rest during the no-niacin condition (R), exercise during the no-niacin condition (E), rest during the with-niacin condition (RN), and exercise during the with-niacin condition (EN). All participants took 1,000 mg/day of extended-release niacin for 4 weeks during the with-niacin conditions (RN and EN). The exercise treatment consisted of a single bout of treadmill walking at 60% heart rate reserve until 400 kcal were expended. Blood samples were collected at 24 hours after each trial and analyzed for changes in plasma glucose, insulin, and C-peptide. A two by two analysis of variance was used to examine the changes in dependent variables, and the Bonferroni adjustment was employed as the post hoc test. The level of statistical significance was set at P<0.05. There was no significant interaction between exercise and niacin, nor was there a main effect of exercise for changes in glucose, insulin, or C-peptide. However, there was a significant main effect for niacin as mean glucose, insulin, and C-peptide values significantly increased with niacin; glucose increased 10.6% (P=0.001), from 95.03±10.67 mg/dL to 105.07±13.56 mg/dL; insulin increased 61.8% (P=0.001), from 16.98±12.49 μU/mL to 27.48±14.84 μU/mL; and C-peptide increased 46.1% (P=0.001), from 1.65±0.75 ng/mL to 2.41±0.97 ng/mL. Although niacin was generally well tolerated, given its adverse effects on glucose, insulin, and C-peptide profiles, the use of niacin should be done so with caution and under medical supervision.
Effect of hypolipidemic treatment on glycemic profile in patients with mixed dyslipidemia
METHODS: This is a prespecified analysis of a prospective, randomized, open-label, blinded end point (PROBE) study (ClinicalTrials.gov identifier: NCT01010516). Patients (n = 100) with mixed dyslipidemia on a standard statin dose who had not achieved lipid targets were randomized to switch to the highest dose of rosuvastatin (40 mg/d) or to add-on-statin extended release nicotinic acid (ER-NA)/laropiprant (LRPT) or to add-on-statin micronised fenofibrate for a total of 3 mo. Fasting plasma glucose (FPG), glycosylated hemoglobin (HbA1c), homeostasis model assessment of insulin resistance (HOMA-IR) index and lipid profile were evaluated at baseline and 3 mo after treatment intervention.
RESULTS: FPG increased in add-on ER-NA/LRPT and rosuvastatin monotherapy groups by 9.7% and 4.4%, respectively (P < 0.01 between the 2 groups and compared with baseline), while it did not significantly change in the add-on fenofibrate group. Similarly, HbA1c increased by 0.3% in add-on ER-NA/LRPT group and by 0.2% in the rosuvastatin monotherapy group (P < 0.01 for all comparisons vs baseline and for the comparison between the 2 groups), while no significant change was reported in the add-on fenofibrate group. HOMA-IR increased by 65% in add-on ER-NA/LRPT and by 14% in rosuvastatin monotherapy group, while it decreased by 6% in the add-on fenofibrate group (P < 0.01 vs baseline and for all comparisons among the groups). Non-HDL-C decreased in all groups (by 23.7%, 24.7% and 7% in the rosuvastatin, ER-NA/LRPT and fenofibrate group, respectively, P < 0.01 for all vs baseline and P < 0.01 for all vs with fenofibrate group).
Nicotinamide
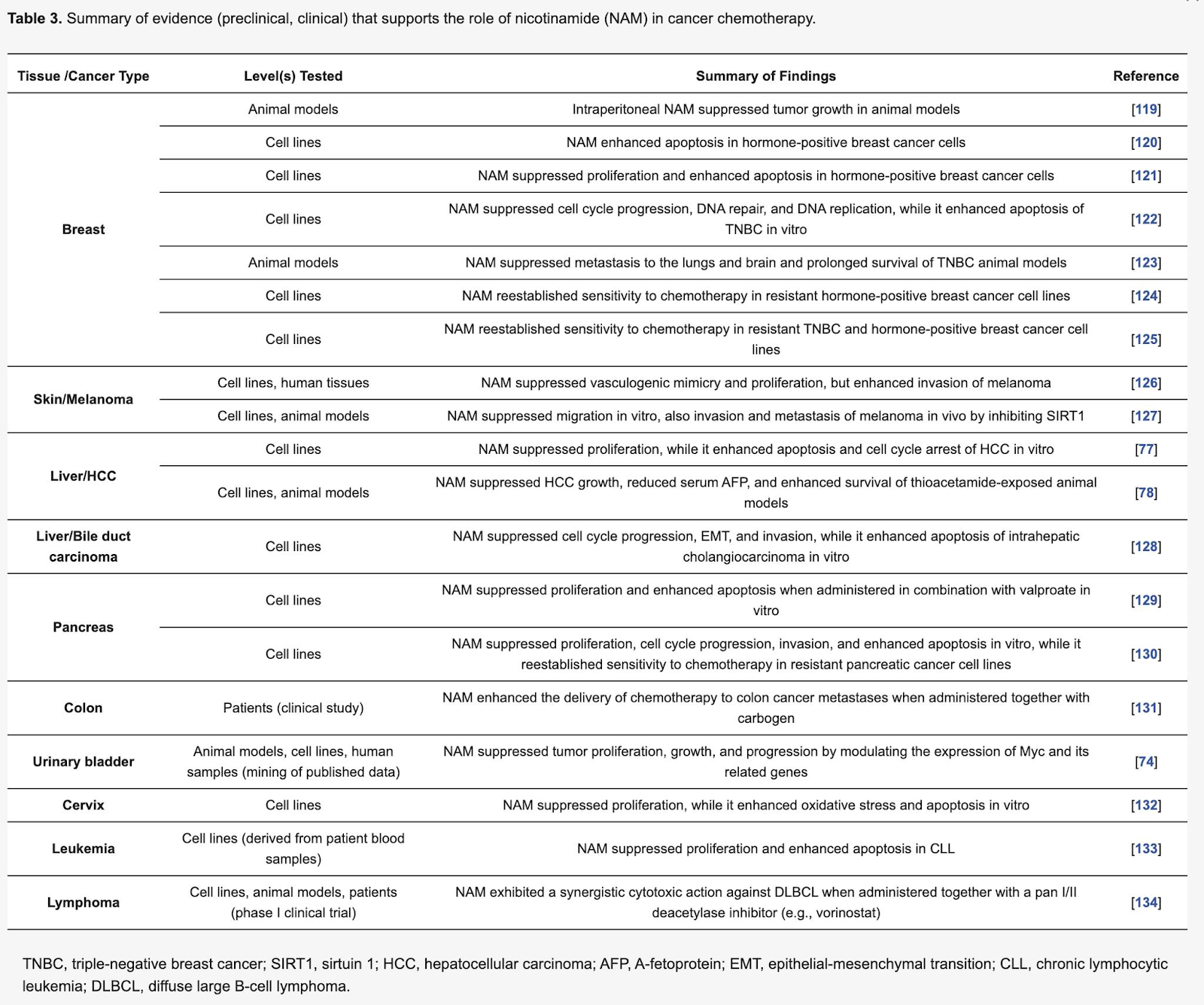
The Role of Nicotinamide in Cancer Chemoprevention and Therapy, 2020
Nicotinamide (NAM) is a water-soluble form of Vitamin B3 (niacin) and a precursor of nicotinamide-adenine dinucleotide (NAD+) which regulates cellular energy metabolism. Except for its role in the production of adenosine triphosphate (ATP), NAD+ acts as a substrate for several enzymes including sirtuin 1 (SIRT1) and poly ADP-ribose polymerase 1 (PARP1). Notably, NAM is an inhibitor of both SIRT1 and PARP1. Accumulating evidence suggests that NAM plays a role in cancer prevention and therapy. Phase III clinical trials have confirmed its clinical efficacy for non-melanoma skin cancer chemoprevention or as an adjunct to radiotherapy against head and neck, laryngeal, and urinary bladder cancers. Evidence for other cancers has mostly been collected through preclinical research and, in its majority, is not yet evidence-based. NAM has potential as a safe, well-tolerated, and cost-effective agent to be used in cancer chemoprevention and therapy. However, more preclinical studies and clinical trials are needed to fully unravel its value.
Concerning kidney tumorigenesis, NAM treatment has shown both tumor-inhibiting and promoting capacity. Rakieten et al. reported that NAM inhibited the formation of renal tumors in streptozotocin-exposed animal models [80], whereas Rosenberg et al. reported that it enhanced kidney tubular tumor development [96].
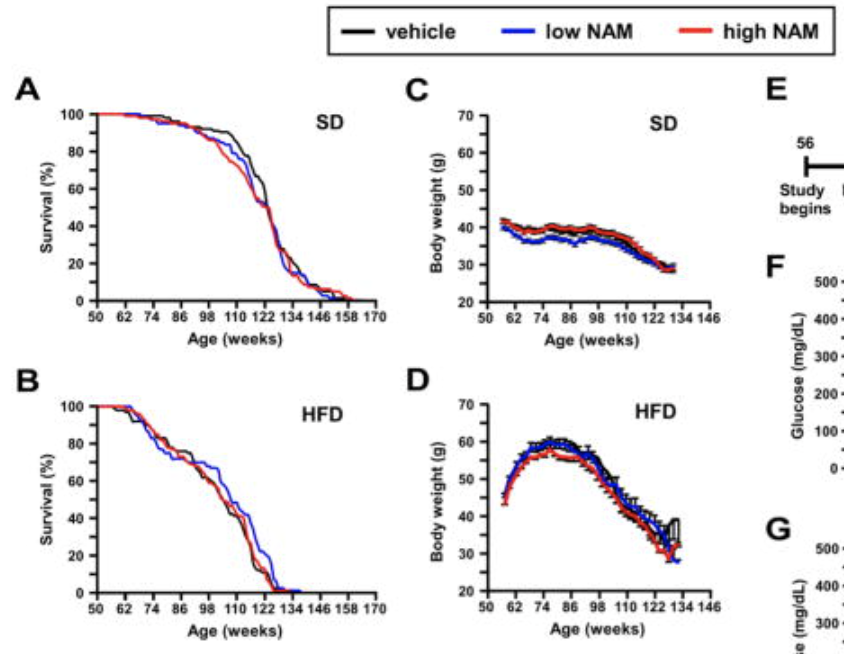
Nicotinamide improves aspects of healthspan but not lifespan in mice, 2018 (Not NR!!)
The team found that mice on the high-fat diet supplemented with NAM for over 12 months showed improved glucose metabolism, less signs of fatty liver, and better physical performance than expected for mice their age (a two-year old mouse being roughly equivalent to a 70-year old human).
Nicotinamide blocks proliferation and induces apoptosis of chronic lymphocytic leukemia cells through activation of the p53/miR-34a/SIRT1 tumor suppressor network, 2011
Because of its relatively indolent clinical course, chronic lymphocytic leukemia (CLL) offers a versatile model for testing novel therapeutic regimens and drug combinations. Nicotinamide is the main NAD(+) precursor and a direct inhibitor of four classes of enzymes, including the sirtuins. SIRT1, the main member of the sirtuin family, inactivates p53 by deacetylating a critical lysine residue. In this study, we showed that CLL cells express high levels of functional SIRT1, which is inhibited by exogenous nicotinamide. This agent blocks proliferation and promotes apoptosis selectively in leukemic cells that express wild-type (wt) p53. Nicotinamide modulates the p53-dependent genes p21, NOXA, BAX, and Mcl-1, indicating an activation of the p53 pathway and of caspase-3. DNA-damaging chemotherapeutics, such as etoposide, activate a functional loop linking SIRT1 and p53 through the induction of miR-34a. When leukemic cells are simultaneously exposed to nicotinamide and etoposide, we observe a significant increase in miR-34a levels with a concomitant inhibition of SIRT1. Furthermore, p53 acetylation levels are higher than with either agent used alone. Overall, treatment with both nicotinamde and etoposide shows strongly synergistic effects in the induction of apoptosis. We therefore concluded that nicotinamide has the dual property of inhibiting SIRT1 through a noncompetitive enzymatic block (p53 independent) and at the same time through miR-34a induction (p53 dependent). These observations suggested the therapeutic potential of nicotinamide, a novel, safe, and inexpensive drug, to be used in addition to chemotherapy for CLL patients with wt p53.
Nicotinamide Metabolism Mediates Resistance to Venetoclax in Relapsed Acute Myeloid Leukemia Stem Cells, 2020
We previously demonstrated that leukemia stem cells (LSCs) in de novo acute myeloid leukemia (AML) patients are selectively reliant on amino acid metabolism and that treatment with the combination of venetoclax and azacitidine (ven/aza) inhibits amino acid metabolism, leading to cell death. In contrast, ven/aza fails to eradicate LSCs in relapsed/refractory (R/R) patients, suggesting altered metabolic properties. Detailed metabolomic analysis revealed elevated nicotinamide metabolism in relapsed LSCs, which activates both amino acid metabolism and fatty acid oxidation to drive OXPHOS, thereby providing a means for LSCs to circumvent the cytotoxic effects of ven/aza therapy. Genetic and pharmacological inhibition of nicotinamide phosphoribosyltransferase (NAMPT), the rate-limiting enzyme in nicotinamide metabolism, demonstrated selective eradication of R/R LSCs while sparing normal hematopoietic stem/progenitor cells. Altogether, these findings demonstrate that elevated nicotinamide metabolism is both the mechanistic basis for ven/aza resistance and a metabolic vulnerability of R/R LSCs.
[NAMPT is the rate-limiting enzyme that converts nicotinamide to nicotinamide mononucleotide in the NAD biosynthetic pathway from nicotinamide in mammals]
Role of Nicotinamide in DNA Damage, Mutagenesis, and DNA Repair
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC2915624/
Poly(ADP-Ribose) Polymerase Inhibitor Hypersensitivity in Aggressive Myeloproliferative Neoplasms
DNA repair defects have been previously reported in myeloproliferative neoplasms (MPNs). Inhibitors of poly(ADP-ribose) polymerase (PARP) have shown activity in solid tumors with defects in homologous recombination (HR). The present study was performed to assess MPN sensitivity to PARP inhibitors ex vivo.
Experimental Design
HR pathway integrity in circulating myeloid cells was evaluated by assessing formation of RAD51 foci after treatment with ionizing radiation or PARP inhibitors. Sensitivity of MPN erythroid and myeloid progenitors to PARP inhibitors was evaluated using colony formation assays.
Results
Six of 14 MPN primary samples had reduced formation of RAD51 foci after exposure to ionizing radiation, suggesting impaired HR. This phenotype was not associated with a specific MPN subtype, JAK2 mutation status or karyotype. MPN samples showed increased sensitivity to the PARP inhibitors veliparib and olaparib compared to normal myeloid progenitors. This hypersensitivity, which was most pronounced in samples deficient in DNA damage-induced RAD51 foci, was observed predominantly in samples from patients with diagnoses of chronic myelogenous leukemia, chronic myelomonocytic leukemia or unspecified myelodysplastic/MPN overlap syndromes.
Conclusions
Like other neoplasms with HR defects, MPNs exhibit PARP inhibitor hypersensitivity compared to normal marrow. These results suggest that further preclinical and possibly clinical study of PARP inhibitors in MPNs is warranted.
I Think I’ve Finally Figured Out How To Use Niacinamide | Ray Peat Forum (link)
Effects of NAD+ precursor supplementation on glucose and lipid metabolism in humans: a meta-analysis (link)
NAD- CHAMBER OF HORRORS (link)
The NAD- CHAMBER OF HORRORS tales are about some of the main things that can go horribly wrong if you don’t have enough NAD+ in your body or your NAD+/NADH ratio goes screwy. These include but are not limited to:
Inadequate production of sirtuins: SIRT1, SIRT6 and SIRT7
PARP starvation and compromised DNA repair; genomic instability
Inadequate production of key mitochrondial proteins, mitochondrial dysfunction and death,
Extensive mitochondria-originated ROS flooding
Metabolic reprogramming to Warburg metabolism
Misfolded proteins don’t get cleaned up
Compromised stress resistance
Histones don’t get adequately deacetylated
Reduced antioxidant defenses and oxidative damage to proteins
Deacetylated and inactivated tumor suppressor proteins
Microtubule railways hijacked, inflammasomes activated, and chronic destructive inflammation
Cell senescence
Impaired autophagy
Endoplasmic reticulum stress
Pharmacological Intakes of Niacin Increase Bone Marrow Poly(ADP-Ribose) and the Latency of Ethylnitrosourea-Induced Carcinogenesis in Rats, 2002
Cancer chemotherapy agents cause short-term leukopenia during treatment and the development of secondary leukemias after recovery from the original disease. We reported that niacin deficiency in rats increases the severity of nitrosourea-induced leukopenia and the subsequent development of cancers. This study was designed to test the effects of supplementing an already high quality diet with pharmacologic levels of niacin. For a period of 4 wk, nontumor-bearing weanling Long-Evans rats were pair-fed AIN-93M diets that were niacin adequate (30 mg/kg diet) or pharmacologically supplemented (4 g/kg diet) with nicotinic acid (NA) or nicotinamide (Nam). One week after the initiation of niacin feeding protocols, ethylnitrosourea (ENU) treatment began (12 doses, 30 mg/kg by gavage, every other day). ENU treatment caused leukopenia, which was not prevented by niacin supplementation. At the end of ENU treatment, all rats were switched to a niacin-adequate diet and monitored. Within 36 wk after the start of treatment, all of the ENU-treated rats either lost 5% of peak body weight or had palpable tumors > 1 cm in diameter, and were necropsied. Supplementation with NA or Nam at 4.0 g/kg diet (combined analysis) increased the latency of the ENU-induced morbidity curve, relative to niacin-adequate controls. Morbidity could be attributed in almost all cases to some form of neoplasm, with leukemias the predominant form. In short-term studies, supplementation with either NA or Nam caused dramatic increases in bone marrow NAD+ (1- to 1.5-fold), basal poly(ADP-ribose) (3- to 5-fold) and ENU-induced poly(ADP-ribose) levels (1.5-fold). These data show that supplementation of a niacin-adequate, high quality diet with pharmacologic levels of nicotinic acid or nicotinamide increases NAD+ and poly(ADP-ribose) levels in bone marrow and may be protective against DNA damage.
Nicotinamide inhibits melanoma in vitro and in vivo
07 October 2020
Background
Even though new therapies are available against melanoma, novel approaches are needed to overcome resistance and high-toxicity issues. In the present study the anti-melanoma activity of Nicotinamide (NAM), the amide form of Niacin, was assessed in vitro and in vivo.
Methods
Human (A375, SK-MEL-28) and mouse (B16-F10) melanoma cell lines were used for in vitro investigations. Viability, cell-death, cell-cycle distribution, apoptosis, Nicotinamide Adenine Dinucleotide+ (NAD+), Adenosine Triphosphate (ATP), and Reactive Oxygen Species (ROS) levels were measured after NAM treatment. NAM anti-SIRT2 activity was tested in vitro; SIRT2 expression level was investigated by in silico transcriptomic analyses. Melanoma growth in vivo was measured in thirty-five C57BL/6 mice injected subcutaneously with B16-F10 melanoma cells and treated intraperitoneally with NAM. Interferon (IFN)-γ-secreting murine cells were counted with ELISPOT assay. Cytokine/chemokine plasmatic levels were measured by xMAP technology. Niacin receptors expression in human melanoma samples was also investigated by in silico transcriptomic analyses.
Results
NAM reduced up to 90% melanoma cell number and induced: i) accumulation in G1-phase (40% increase), ii) reduction in S- and G2-phase (about 50% decrease), iii) a 10-fold increase of cell-death and 2.5-fold increase of apoptosis in sub-G1 phase, iv) a significant increase of NAD+, ATP, and ROS levels, v) a strong inhibition of SIRT2 activity in vitro. NAM significantly delayed tumor growth in vivo (p ≤ 0.0005) and improved survival of melanoma-bearing mice (p ≤ 0.0001). About 3-fold increase (p ≤ 0.05) of Interferon-gamma (IFN-γ) producing cells was observed in NAM treated mice. The plasmatic expression levels of 6 cytokines (namely: Interleukin 5 (IL-5), Eotaxin, Interleukin 12 (p40) (IL12(p40)), Interleukin 3 (IL-3), Interleukin 10 (IL-10) and Regulated on Activation Normal T Expressed and Secreted (RANTES) were significantly changed in the blood of NAM treated mice, suggesting a key role of the immune response. The observed inhibitory effect of NAM on SIRT2 enzymatic activity confirmed previous evidence; we show here that SIRT2 expression is significantly increased in melanoma and inversely related to melanoma-patients survival. Finally, we show for the first time that the expression levels of Niacin receptors HCAR2 and HCAR3 is almost abolished in human melanoma samples.
Conclusion
NAM shows a relevant anti-melanoma activity in vitro and in vivo and is a suitable candidate for further clinical investigations.
Increased plasma nicotinamide phosphoribosyltransferase is associated with a hyperproliferative phenotype and restrains disease progression in MPN-associated myelofibrosis, 2016
Abstract
Myeloproliferative neoplasm (MPN)-associated myelofibrosis is a clonal, neoplastic disorder of the hematopoietic stem cells, in which inflammation and immune dysregulation play an important role. Extracellular nicotinamide phosphoribosyltransferase (eNAMPT), also known as visfatin, is a cytokine implicated in a number of inflammatory and neoplastic diseases. Here plasma levels of eNAMPT in patients with MPN-associated myelofibrosis and their effects on disease phenotype and outcomes were examined. The concordance of eNAMPT levels with the marker of general inflammation high-sensitivity C-reactive protein (hs-CRP) was also studied. A total of 333 MPN-associated myelofibrosis patients (187 males and 146 females) and 31 age- and gender-matched normal-weight healthy subjects were enrolled in the study main body. Levels of eNAMPT and hs-CRP were simultaneously assayed in 209 MPN-associated myelofibrosis patients. Twenty-four polycythemia vera or essential thrombocythemia patients were used as controls. eNAMPT was over expressed in MPN-associated myelofibrosis, and eNAMPT expression was correlated with higher white blood cell count, higher hemoglobin, and higher platelet count, suggesting that eNAMPT is an indispensable permissive agent for myeloproliferation of MPN-associated myelofibrosis. The lack of correlation between eNAMPT and hs-CRP revealed that eNAMPT in MPN-associated myelofibrosis does not behave as a canonical inflammatory cytokine. In addition, higher levels of eNAMPT predicted longer time to blast transformation, and protected against progression toward thrombocytopenia and large splenomegaly. In conclusion, in MPN-associated myelofibrosis high levels of eNAMPT mark the myeloproliferative potential and, at variance with a high number of cancers, are protective against disease progression.
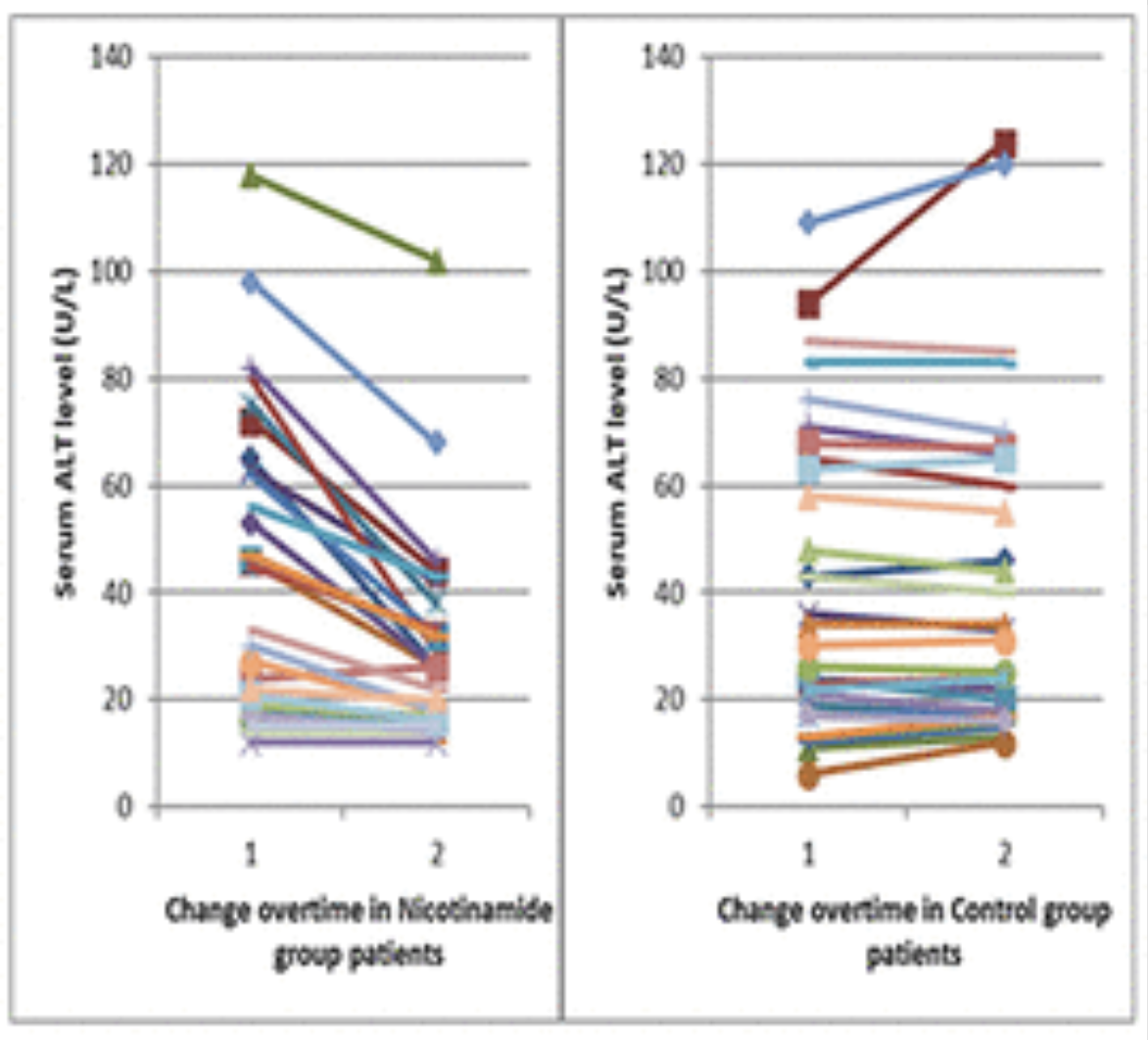
Nicotinamide supplementation in diabetic nonalcoholic fatty liver disease patients: randomized controlled trial, 2022
Background:
Nicotinamide has been reported to protect against liver steatosis and metabolic imbalances in nonalcoholic fatty liver disease (NAFLD) in animal models.
Objectives:
The objective was to investigate the efficacy and safety of nicotinamide supplementation in diabetic NAFLD patients.
Design:
This is a prospective randomized controlled open label study.
Methods:
Seventy diabetic NAFLD patients were randomly assigned either to the nicotinamide group (n = 35) who received nicotinamide 1000 mg once daily for 12 weeks in addition to their antidiabetic therapy or the control group (n = 35) who received their antidiabetic therapy only. The primary outcome was improvement in steatosis score, while secondary outcomes included assessment of liver stiffness, liver enzymes, lipid profile, insulin resistance, serum malondialdehyde, serum adiponectin, and patients’ quality of life (QOL).
Results:
Only 61 patients completed the study; 31 in the nicotinamide group and 30 in the control group. Comparisons between groups and within groups revealed nonsignificant changes in steatosis and fibrosis scores. However, significant reduction was observed in liver enzymes with a median decrease in alanine transaminase of 26.6% versus 0.74% in nicotinamide and control groups, respectively. After 12 weeks of treatment, the nicotinamide group showed significantly lower levels of low-density lipoprotein cholesterol (p value = 0.004), total cholesterol (p value = 0.006), and insulin resistance marker (p value = 0.005) compared with control. Serum triglycerides, malondialdehyde, and adiponectin levels were all comparable between the two groups. Regarding QOL, a significant improvement was detected in the total scores and the activity and fatigue domains scores.
Conclusion:
Nicotinamide at a dose of 1000 mg daily was tolerable, improved metabolic abnormalities and QOL of diabetic NAFLD patients with no effect on liver fibrosis or steatosis.
Nicotinamide and NAFLD: Is There Nothing New Under the Sun? 2019
Reduced NAD concentrations contribute to the dysmetabolic imbalance and consequently to the pathogenesis of NAFLD. The dietary supplementation or the pharmacological modulation of NAD levels appear to be an attractive strategy.
NAD + and NAFLD - caution, causality and careful optimism, 2022
Nicotinamide adenine dinucleotide (NAD+ ) has been proposed as a potential target to prevent and reverse NAFLD. NAD+ is an important redox factor for energy metabolism and is used as a substrate by a range of enzymes, including sirtuins (SIRT), which regulates histone acetylation, transcription factor activity and mitochondrial function. NAD+ is also a precursor for reduced nicotinamide adenine dinucleotide phosphate (NADPH), which is an important component of the antioxidant defense system. NAD+ precursors such as nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are available as over-the-counter dietary supplements, and oral supplementation with these precursors increases hepatic NAD+ levels and prevents hepatic lipid accumulation in pre-clinical models of NAFLD. NAD+ precursors have also been found to improve hepatic mitochondrial function and decrease oxidative stress in pre-clinical NAFLD models. NAD+ repletion also prevents NAFLD progression to non-alcoholic steatohepatitis (NASH), as NAD+ precursor supplementation is associated with decreased hepatic stellate cell activation, and decreased fibrosis. However, initial clinical trials have only shown modest effects when NAD+ precursors were administrated to people with obesity. We review the available pre-clinical investigations of NAD+ supplementation for targeting NAFLD, and discuss how data from the first clinical trials can be reconciled with observations from preclinical research.
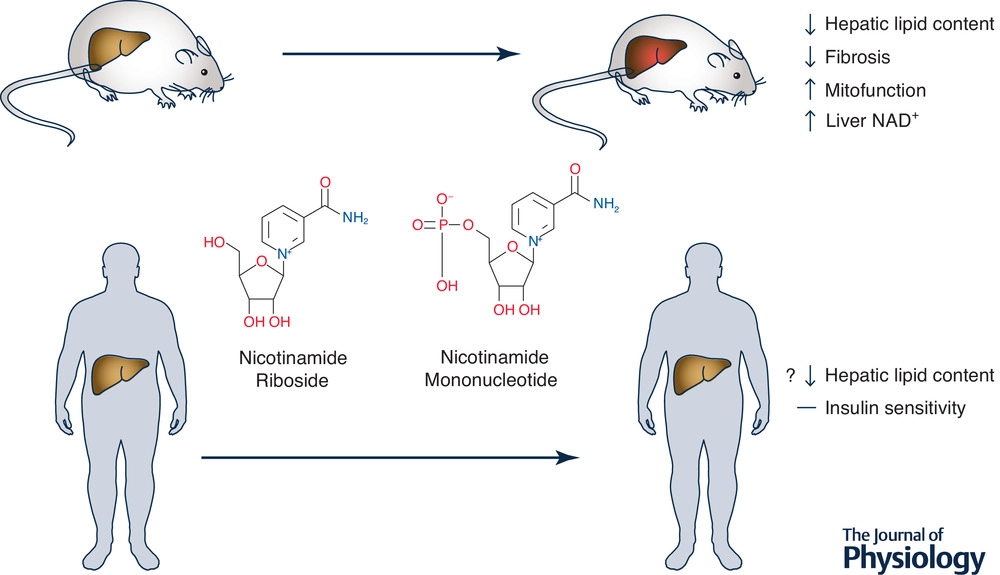
They summarise observations from preclinical and clinical studies looking at how B3 vitamins may affect fatty liver formation and liver fibrosis, and they attempt to explain why the effects of the vitamin have turned out to be more limited in humans.
For example, they say in the overview article that treatment with vitamin B3 leads to weight loss and improved liver function in mice by improving activation of the cell’s mitochondria, reducing damage from reactive oxygen compounds and inhibiting the progression from fatty liver to liver fibrosis. The latter is due to inhibition of the activity of the cells that form scar tissue in the liver when it is damaged. In overweight humans, vitamin B3 treatment led to a small reduction in the fat content of the liver, but did not affect insulin sensitivity in the liver and did not lead to weight loss.
Niacinamide = Nicotinamide = NAM: Benefits, Uses and Side Effects
Useful for Chronic Kidney Disease
Chronic kidney disease is the progressive loss of kidney function that affects your body’s ability to clean and filter blood and control blood pressure.
This can cause a harmful buildup of chemicals, such as phosphate, in your blood.
Research suggests that niacinamide may help decrease phosphate levels in people with kidney dysfunction by blocking its absorption.
Phosphate levels are otherwise typically managed through diet, medications or dialysis, depending on the severity of the buildup.
Vitamin B3 (Nicotinamide - NAM) prevents basal cell carcinoma and squamous cell carcinoma in people at high risk --
In high-risk people who have already had a non-melanoma skin cancer, i.e. a basal cell carcinoma (BCC) or a squamous cell carcinoma (SCC), taking vitamin B3 tablets daily reduces the risk of future non-melanoma skin cancer.
The largest trial of vitamin B treatment showed that it is an effective and low-risk treatment. At a dose of 500mg twice daily, taken for a year, the rate of new non-melanoma skin cancers was reduced by approximately 23 per cent:
Basal cell carcinomas were reduced by 20 per cent. Less serious superficial basal cell carcinomas were prevented more effectively than more aggressive forms of basal cell carcinoma.
Squamous cell carcinomas were reduced by 30 per cent. This reduction was the same for superficial and more aggressive squamous cell carcinomas.
Some people get better results than this. In an earlier study, nicotinamide was found to reduce non-melanoma skin cancer rates by up to 75 per cent, but these figures have not been reproduced across larger numbers of patients.
Vitamin B seems to work best in people with the highest levels of risk, i.e. those who have had many BCCs or SCCs previously.
Oral nicotinamide is now recognised as an important part of the routine treatment of people at high risk of BCC and SCC and is about to become part of the Cancer Council’s national treatment guidelines for BCC and SCC4.
Protection from vitamin B3 only lasts while it is being taken. In other words, for long term reduction of non-melanoma skin cancer, it needs to be taken indefinitely.
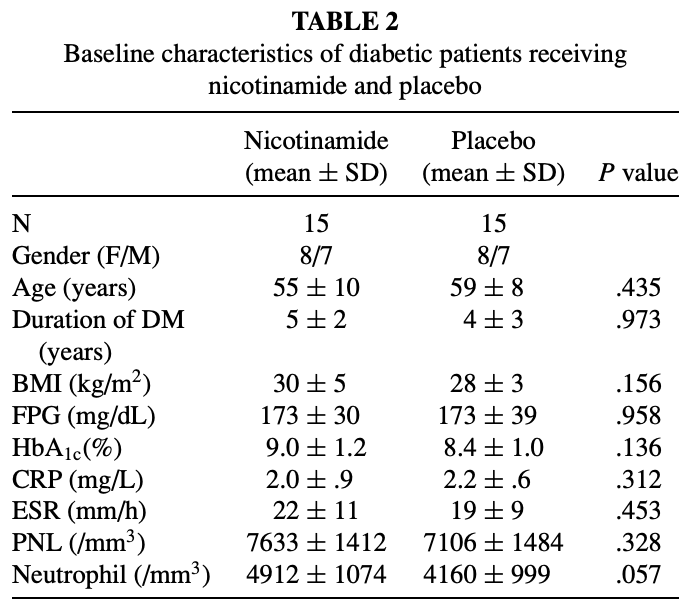
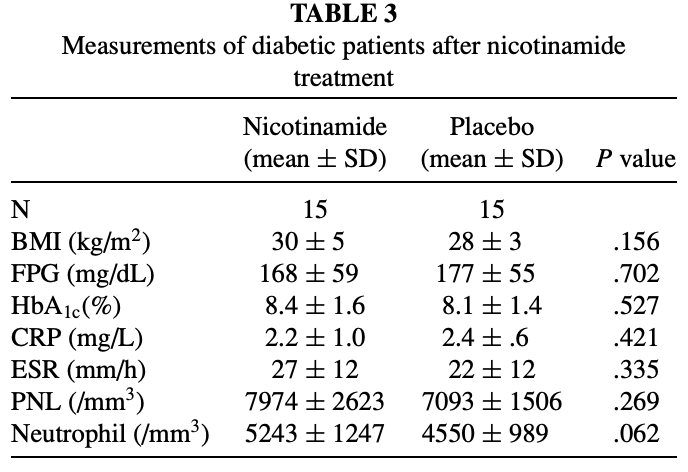
Nicotinamide Effects Oxidative Burst Activity of Neutrophils in Patients with Poorly Controlled Type 2 Diabetes Mellitus, 2003
NMN
NMN Lengthens Telomeres In Humans & Mice | Review By Modern Healthspan (link)
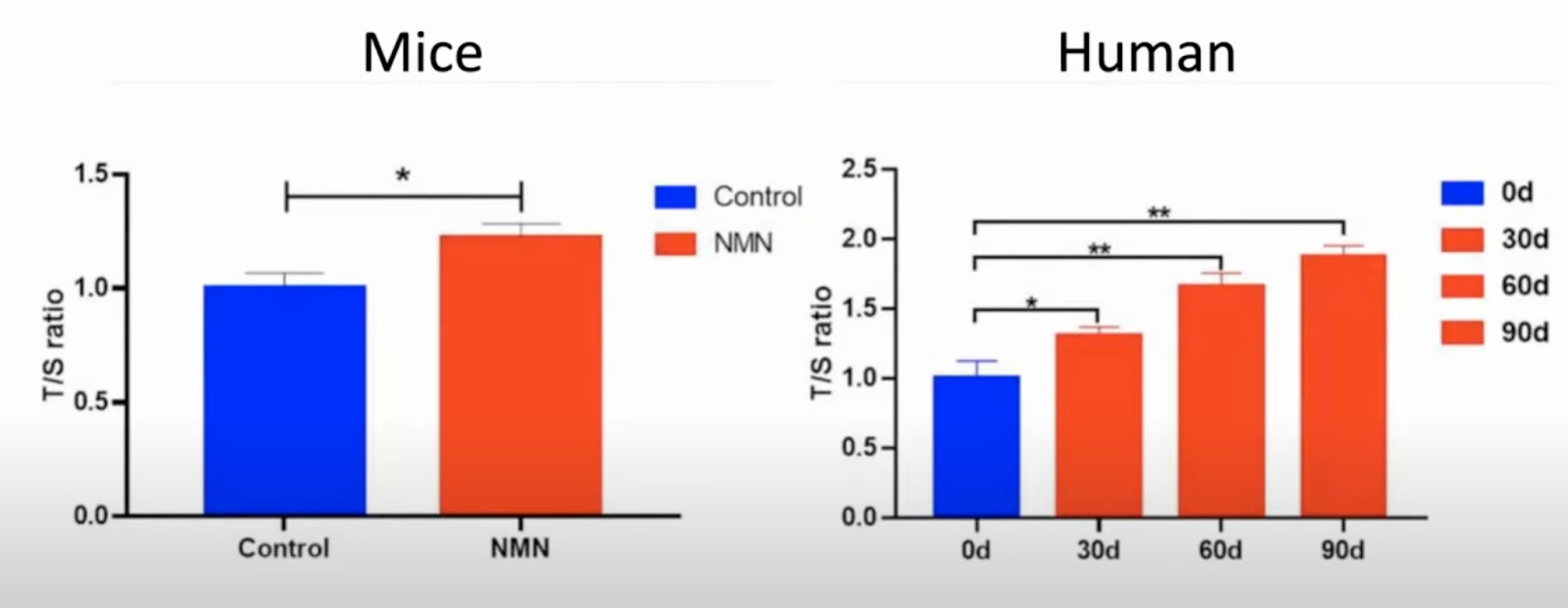
The Impacts of Short-Term NMN Supplementation on Serum Metabolism, Fecal Microbiota, and Telomere Length in Pre-Aging Phase, 2021
A non-blinded clinical trial in eight healthy men was conducted to investigate the supplementary effect of NMN on the telomere length of the peripheral blood mononuclear cell (PBMC). The male subjects enrolled in the study were selected based on the criteria based on an NMN clinical trial NCT04228640 (https://clinicaltrials.gov/ct2/show/study/NCT04228640) and a previous study (33) as follows: (1) 45–60 years old with body mass index (BMI) at a range of 18.5–30 kg/m2; (2) no allergic and metabolic diseases; (3) without any form of niacin supplement for 7 days prior to the study and for the whole test period; (4) kept consistent diet and lifestyle habits during the whole test period; (5) took NMN supplement for 90 days; (6) followed verbal and written study directions. The information of the volunteers is presented in Supplementary Table 1. All the participants were instructed to take NMN (300 mg/day/person) (34) in warm water once a day after 30 min of breakfast for a total of 90 days.
Aging is a natural process with concomitant changes in the gut microbiota and associate metabolomes. Beta-nicotinamide mononucleotide, an important NAD+ intermediate, has drawn increasing attention to retard the aging process. We probed the changes in the fecal microbiota and metabolomes of pre-aging male mice (C57BL/6, age: 16 months) following the oral short-term administration of nicotinamide mononucleotide (NMN). Considering the telomere length as a molecular gauge for aging, we measured this in the peripheral blood mononuclear cells (PBMC) of pre-aging mice and human volunteers (age: 45–60 years old). Notably, the NMN administration did not influence the body weight and feed intake significantly during the 40 days in pre-aging mice. Metabolomics suggested 266 upregulated and 58 downregulated serum metabolites. We identified 34 potential biomarkers linked with the nicotinamide, purine, and proline metabolism pathways. Nicotinamide mononucleotide significantly reduced the fecal bacterial diversity (p < 0.05) with the increased abundance of Helicobacter, Mucispirillum, and Faecalibacterium, and lowered Akkermansia abundance associated with nicotinamide metabolism. We propose that this reshaped microbiota considerably lowered the predicated functions of aging with improved immune and cofactors/vitamin metabolism. Most notably, the telomere length of PBMC was significantly elongated in the NMN-administered mice and humans. Taken together, these findings suggest that oral NMN supplementation in the pre-aging stage might be an effective strategy to retard aging. We recommend further studies to unravel the underlying molecular mechanisms and comprehensive clinical trials to validate the effects of NMN on aging.
The NAD-Booster NR Potently Stimulates Hematopoiesis through Increased Mitochondrial Clearance, 2019
It has been recently shown that increased oxidative phosphorylation, as reflected by increased mitochondrial activity, together with impairment of the mitochondrial stress response, can severely compromise hematopoietic stem cell (HSC) regeneration. Here we show that the NAD+-boosting agent nicotinamide riboside (NR) reduces mitochondrial activity within HSCs through increased mitochondrial clearance, leading to increased asymmetric HSC divisions. NR dietary supplementation results in a significantly enlarged pool of progenitors, without concurrent HSC exhaustion, improves survival by 80%, and accelerates blood recovery after murine lethal irradiation and limiting-HSC transplantation. In immune-deficient mice, NR increased the production of human leucocytes from hCD34+ progenitors. Our work demonstrates for the first time a positive effect of NAD+-boosting strategies on the most primitive blood stem cells, establishing a link between HSC mitochondrial stress, mitophagy, and stem-cell fate decision, and unveiling the potential of NR to improve recovery of patients suffering from hematological failure including post chemo- and radiotherapy.
NAD+ Precursor (NR) Stimulates the Production of Blood Cells (link)
An international team of scientists discovered that dietary supplementation of nicotinamide riboside can maintain the balance within blood-making stem cells and speed up blood cell generation.
“We expect nicotinamide riboside and other mitochondrial modulators to become a complementary approach for increasing stem cell fitness and accelerating blood production, either through dietary supplementation or pharmacological administration,” says senior author Olaia Naveiras of Ecole Polytechnique Fé dé rale de Lausanne (EPFL), Switzerland, in a statement.
This study is the first to demonstrate that NR, as a dietary supplement, can boost the function of the blood stem cells, unveiling NR’s potential to prevent blood-recovery failures. The researchers also noted that the NR and other molecules with similar functions, such as nicotinamide mononucleotide, might become a supportive treatment that expands beyond blood-cancer patients. It may also help patients with blood-related autoimmune disorders in the future.
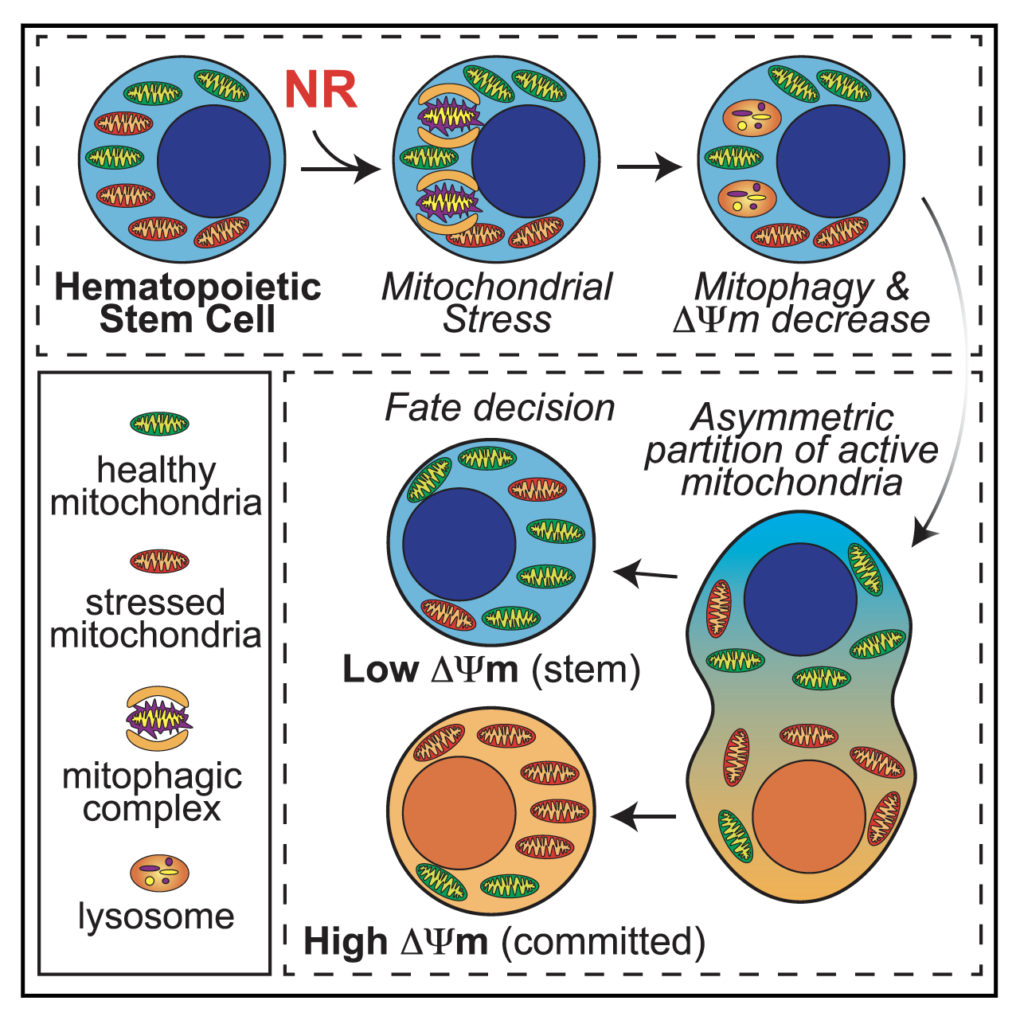
Naveiras and colleagues describe the effects of vitamin B3 derivatives in blood formation, of which they find nicotinamide riboside (NR) to most potently increase blood progenitors. Treating purified mouse or human blood stem cells with NR improved their mitochondrial quality and reduced the toxicity of bone marrow transplantation in mice. (Vannini et al., 2019)
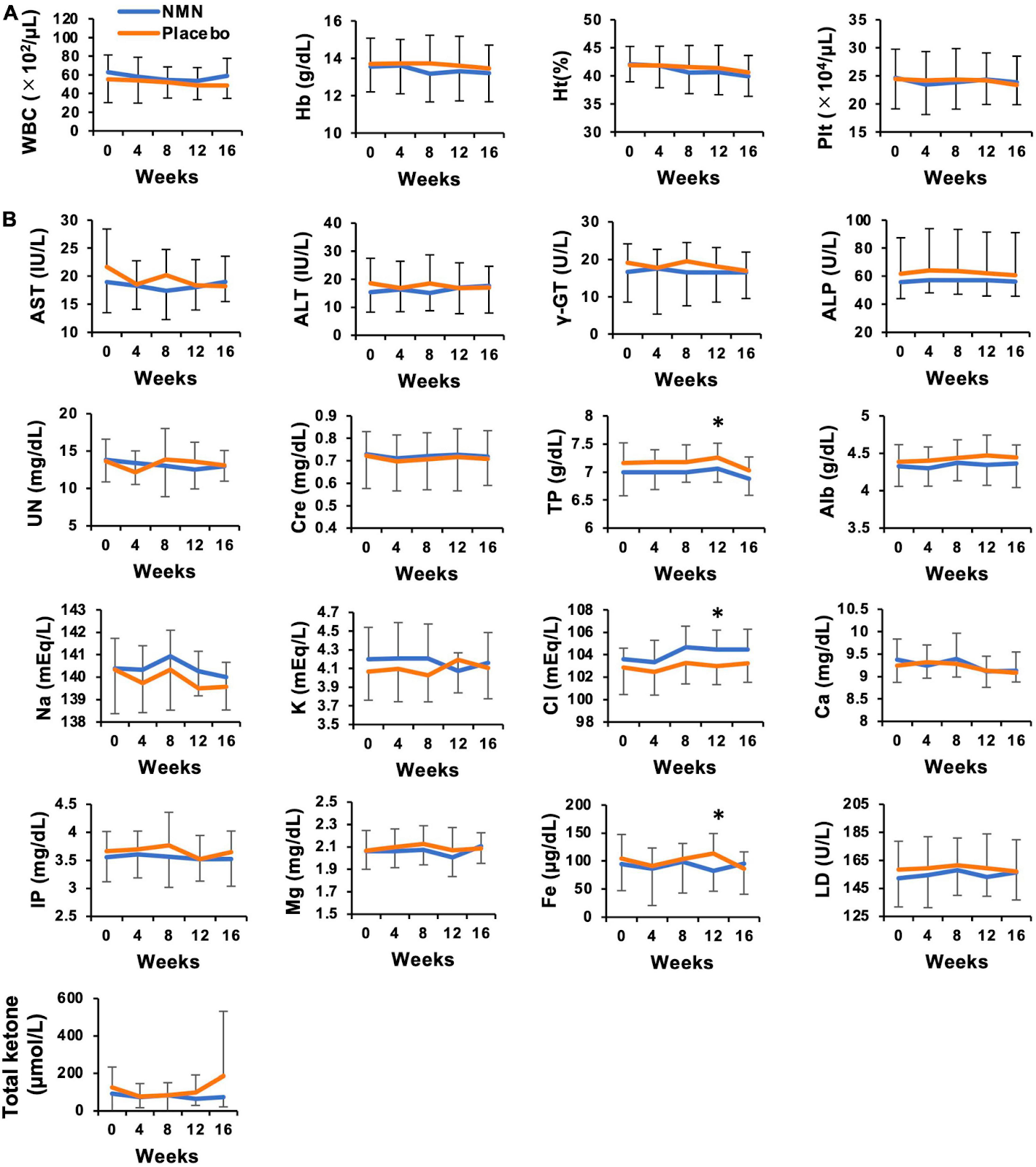
Oral Administration of Nicotinamide Mononucleotide Is Safe and Efficiently Increases Blood Nicotinamide Adenine Dinucleotide Levels in Healthy Subjects, 2022
Placebo-controlled, randomized, double blind, parallel-group trial to investigate the safety of orally administered NMN and its efficacy to increase NAD+ levels in thirty healthy subjects. Healthy volunteers received 250 mg/day of NMN (n = 15) or placebo (n = 15) for 12 weeks, and physiological and laboratory tests were performed during this period. In addition, NAD+ and its related metabolites in whole blood were examined. Oral supplementation of NMN for 12 weeks caused no abnormalities in physiological and laboratory tests, and no obvious adverse effects were observed. NAD+ levels in whole blood were significantly increased after NMN administration. We also observed the significant rise in nicotinic acid mononucleotide (NAMN) levels, but not in NMN. We also found that the increased amount of NAD+ was strongly correlated with pulse rate before the administration of NMN. These results suggest that oral administration of NMN is a safe and practical strategy to boost NAD+ levels in humans.
NIACIN & NICOTINAMIDE vs Expensive NR & NMN? 2020
NAD+ in Aging: Role of Nicotinamide Riboside and Nicotinamide Mononucleotide
https://www.youtube.com/watch?v=hggLOXhFRxc
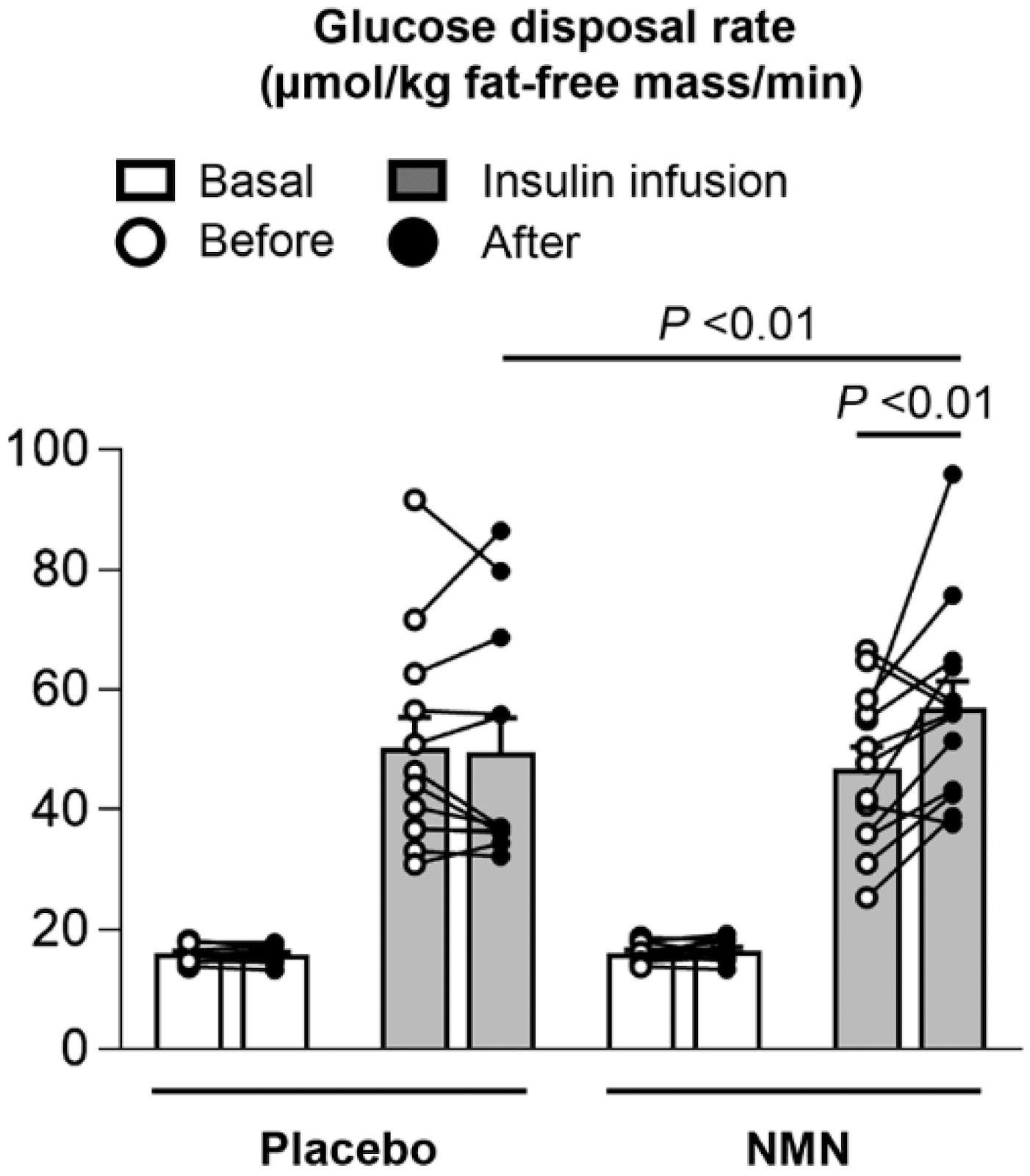
Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women, 2021
In rodents, obesity and aging impair nicotinamide adenine dinucleotide (NAD+) biosynthesis, which contributes to metabolic dysfunction. Nicotinamide mononucleotide (NMN) availability is a rate-limiting factor in mammalian NAD+ biosynthesis. We conducted a 10-week, randomized, placebo-controlled, double-blind trial to evaluate the effect of NMN supplementation on metabolic function in postmenopausal women with prediabetes who were overweight or obese. Insulin-stimulated glucose disposal, assessed by using the hyperinsulinemic-euglycemic clamp, and skeletal muscle insulin signaling (phosphorylation of AKT and mTOR) increased after NMN supplementation, but did not change after placebo treatment. NMN supplementation up-regulated the expression of platelet-derived growth factor receptor β and other genes related to muscle remodeling. These results demonstrate NMN increases muscle insulin sensitivity, insulin signaling and remodeling in women with prediabetes who are overweight or obese
Fat free mass, insulin, hba1c, HDL

Does NMN improve metabolic health in humans?
https://peterattiamd.com/does-nmn-improve-metabolic-health-in-humans/
Cancer Research Points to Key Unknowns about Popular “Antiaging” Supplements
Increased nicotinamide adenine dinucleotide pool promotes colon cancer progression by suppressing reactive oxygen species level
https://pubmed.ncbi.nlm.nih.gov/30457689/
NAD metabolism fuels human and mouse intestinal inflammation
https://gut.bmj.com/content/67/10/1813
[Relevance not strong] BRCA1 as a nicotinamide adenine dinucleotide (NAD)-dependent metabolic switch in ovarian cancer (NAD may promote ovarian cancer)
[Relevance not strong] Up-regulated NAMPT associated with worse invasive breast cancer
https://pubmed.ncbi.nlm.nih.gov/29725408/
[Relevance not strong] Prostate cancer cells up-regulate NAD+ to survive
https://cancerandmetabolism.biomedcentral.com/articles/10.1186/s40170-018-0186-3
[Relevance not strong] Brain cancer with higher NAMPT levels are more deadly
https://www.pnas.org/content/113/51/E8247
Nicotinamide Phosphoribosyltransferase in Malignancy (link)
Nicotinamide phosphoribosyltransferase (Nampt) catalyzes the rate-limiting step of nicotinamide adenine dinucleotide (NAD) synthesis. Both intracellular and extracellular Nampt (iNampt and eNampt) levels are increased in several human malignancies and some studies demonstrate increased iNampt in more aggressive/invasive tumors and in tumor metastases. Several different molecular targets have been identified that promote carcinogenesis following iNampt overexpression, including SirT1, CtBP, and PARP-1. Additionally, eNampt is elevated in several human cancers and is often associated with a higher tumor stage and worse prognoses. Here we review the roles of Nampt in malignancy, some of the known mechanisms by which it promotes carcinogenesis, and discuss the possibility of employing Nampt inhibitors in cancer treatment.
Nicotinamide riboside (NR)
17-a-estradiol late in life extends lifespan in aging UM-HET3 male mice; nicotinamide riboside and three other drugs do not affect lifespan in either sex, 2021
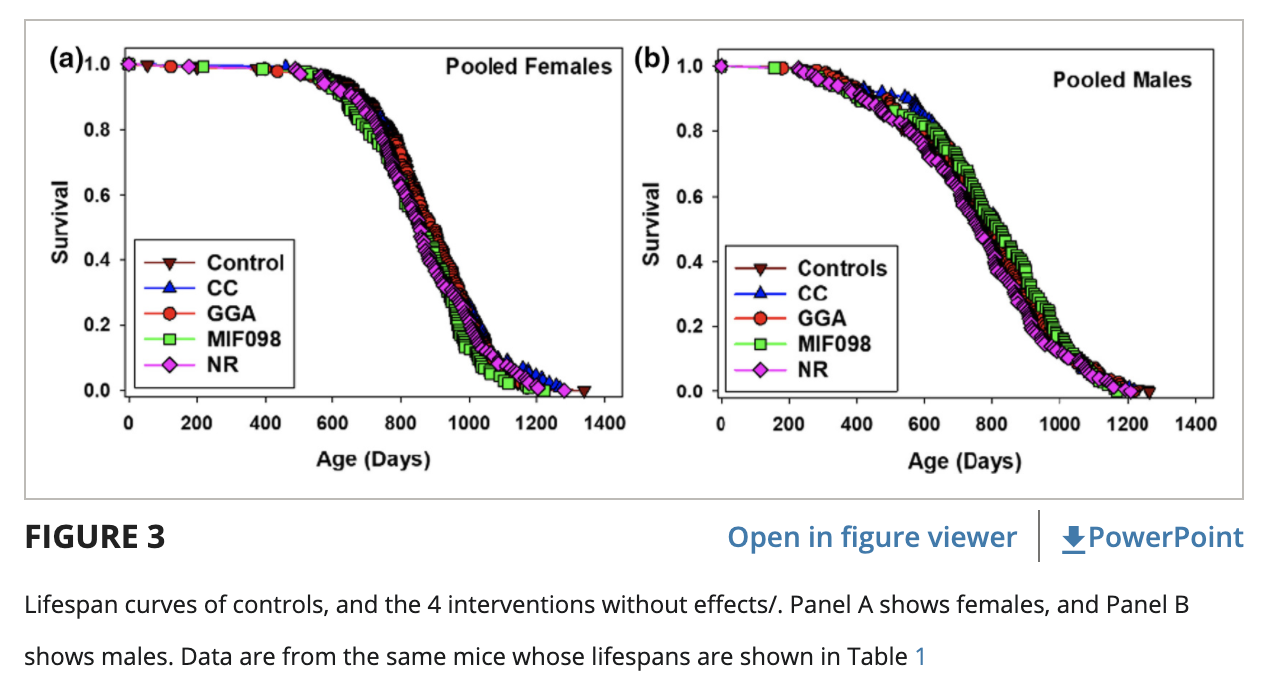
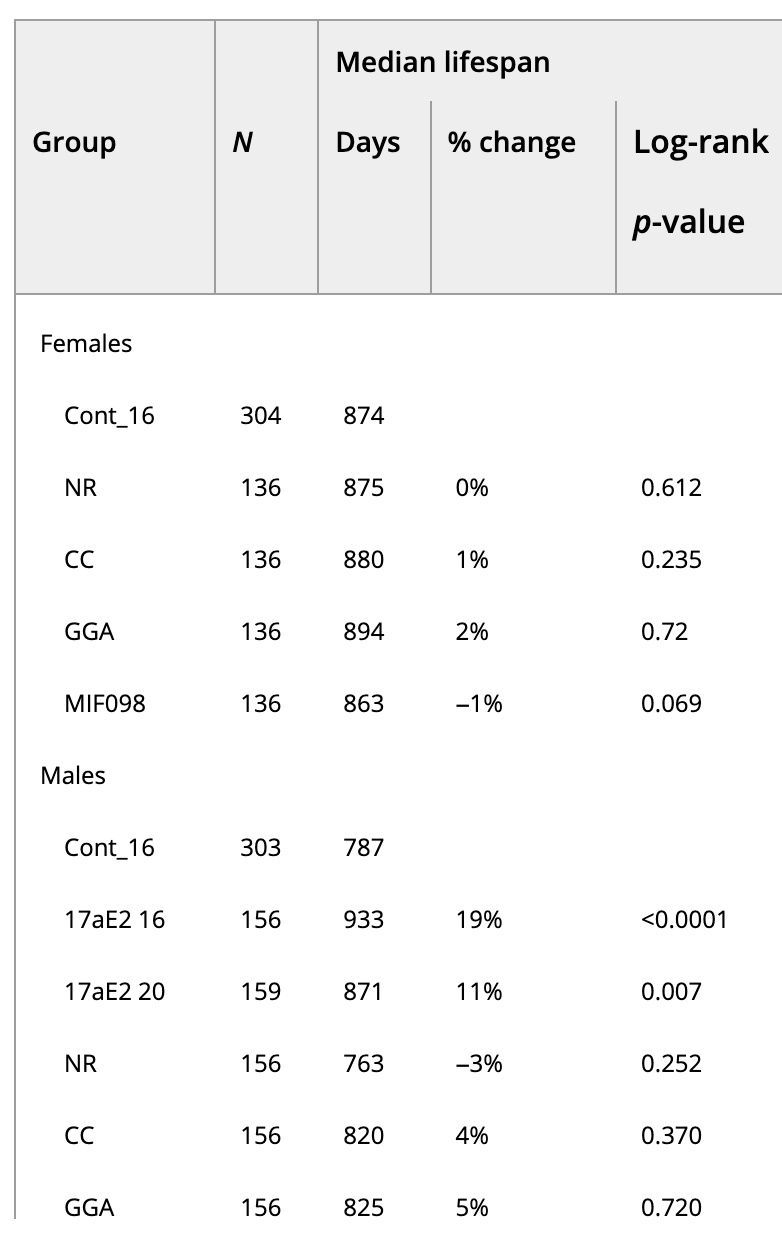
1,000 mg NR Chloride per kilogram diet (1,000 ppm). Mice were fed the NR diet continuously starting at 8 months of age. Upon assay, the amounts of NR plus nicotinamide totaled 878 ppm. Human equivalent ~20 yrs old.
NAD(+) repletion improves mitochondrial and stem cell function and enhances life span in mice. Science, 2016
Aged mice (24 months old) treated with nicotinamide riboside for 6 weeks survived, on average, 5% longer than control mice. Human equivalent ~62 yrs old.

NR improves NSC and McSC function and increases the life span of aged C57BL/6J mice.
Cohorts of 30 mice were fed with a control chow diet with or without NR (400 mg/kg/day) supplementation. 30 control + 30 NR mice. NR (400 mg/kg/day).
Nicotinamide riboside (NR): Results from human & mice studies
https://blog.insidetracker.com/nr-nmn-longevity-supplements-work-humans
Nicotinamide riboside attenuates age-associated metabolic and functional changes in hematopoietic stem cells, 2021
With age, hematopoietic stem cells (HSC) undergo changes in function, including reduced regenerative potential and loss of quiescence, which is accompanied by a significant expansion of the stem cell pool that can lead to haematological disorders. Elevated metabolic activity has been implicated in driving the HSC ageing phenotype. Here we show that nicotinamide riboside (NR), a form of vitamin B3, restores youthful metabolic capacity by modifying mitochondrial function in multiple ways including reduced expression of nuclear encoded metabolic pathway genes, damping of mitochondrial stress and a decrease in mitochondrial mass and network-size. Metabolic restoration is dependent on continuous NR supplementation and accompanied by a shift of the aged transcriptome towards the young HSC state, more youthful bone marrow cellular composition and an improved regenerative capacity in a transplant setting. Consequently, NR administration could support healthy ageing by re-establishing a more youthful hematopoietic system.
Nonalcoholic fatty liver disease: NAFLD is the most common chronic liver disorder in industrialized nations and one closely related to our obesity epidemic.9 Nicotinamide riboside was found to prevent—and even reverse—NAFLD in mice on a high-fat, high-sugar diet. This effect was due to its ability to increase sirtuin activity, which resulted in sharp increases in mitochondrial fat burning as well as increases in the energy storage molecule ATP, which all cells require to perform their functions.9


Comments