Testosterone Replacement Therapy (TRT)
TRT:
The most impactful FDA approved therapy for life extension in hypogonadal men (compared to Statin, Metformin, BP meds, Aspirin).
Strongly associated with reduced all cause mortality by 47%-56% (ref), (53%, 61%, 79%) for the normal weight, overweight, obese respectively (ref)
Helps achieve sustained weight loss over the course of 5-10 years.
Improves insulin resistance, glycaemic control, visceral adiposity, hypercholesterolaemia, liver function, metabolic syndrome.
Clomid:
Another option to raise declining hormone levels for males. Doesn’t raise hematocrit to abnormal levels — a common problem with TRT injections (ref).
Works by binding to the receptors in your brain that would typically bind with estrogen. As a result, your brain thinks your estrogen levels are low and compensates by producing more FSH, or follicle-stimulating hormone and LH, which can boost estrogen, testosterone.
Lowers BMI (~1 unit / year or ~8 lbs/year), improves the symptoms of Testosterone Deficiency (-2 to -3 ADAM) when the drug is dosed to achive >550 ng/dl total test.
Significantly lowers IGF1 amongst hypogonadal men, women with PCOS & men with acromegaly.
Effects on cancer:
TRT is a metabolic therapy. RCC is a metabolic disease. It appears that long term testosterone treatment should help deal with RCC, lower the chances of adverse outcomes. Short term data from RCC is positive, def. not negative. Care oncology MD said it should be fine. Dr McGlynn doesn’t see anything wrong with it.
TRT may slow recurrence of low-risk prostate cancer.
Testosterone Replacement for Men with Low Testosterone Improves Liver Function, Metabolic Syndrome (link)
The study included 122 testosterone-deficient men, ages 36 to 69 years (mean age: 59.5). Results showed that restoring testosterone to normal levels led to major and progressive improvements in many features of the metabolic syndrome over the 2 years of treatment. Specifically, the men's weight, waist line and body mass index (a measure of body fat) continued to decline over the full study period. The other metabolic risk factors also significantly improved during the first year of testosterone treatment. Of the 47 men who met the criteria for a diagnosis of the metabolic syndrome at the beginning of the study, 36 (77 percent) no longer had the diagnosis after 2 years of treatment, the authors reported.
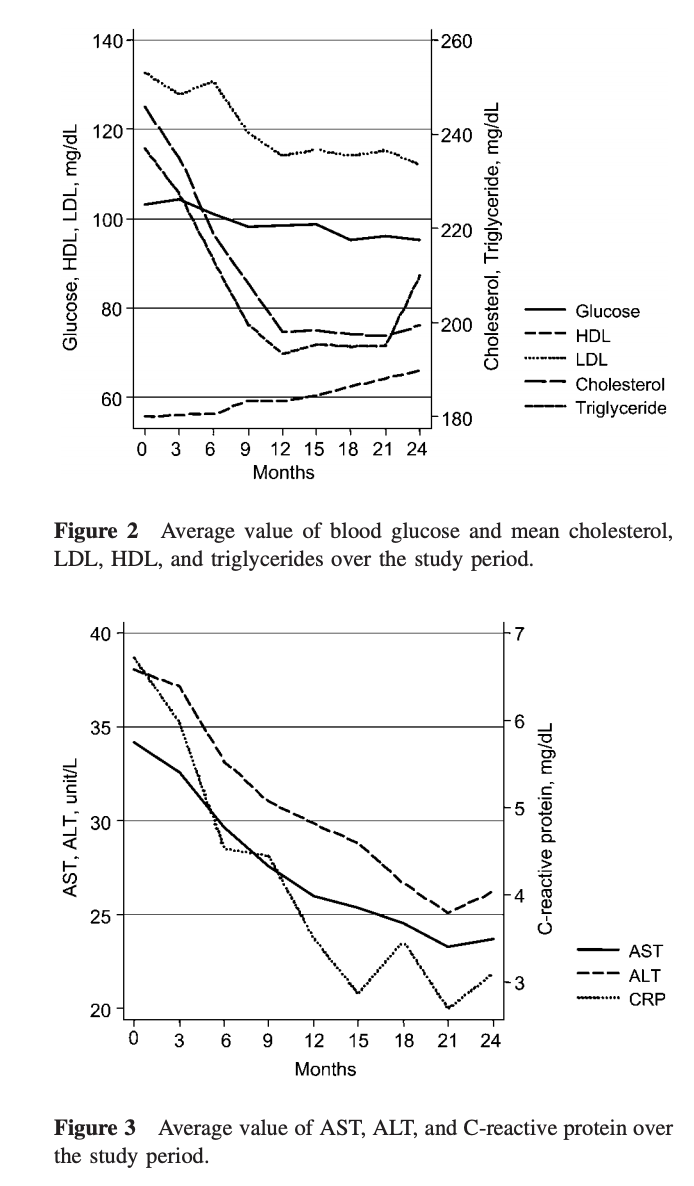
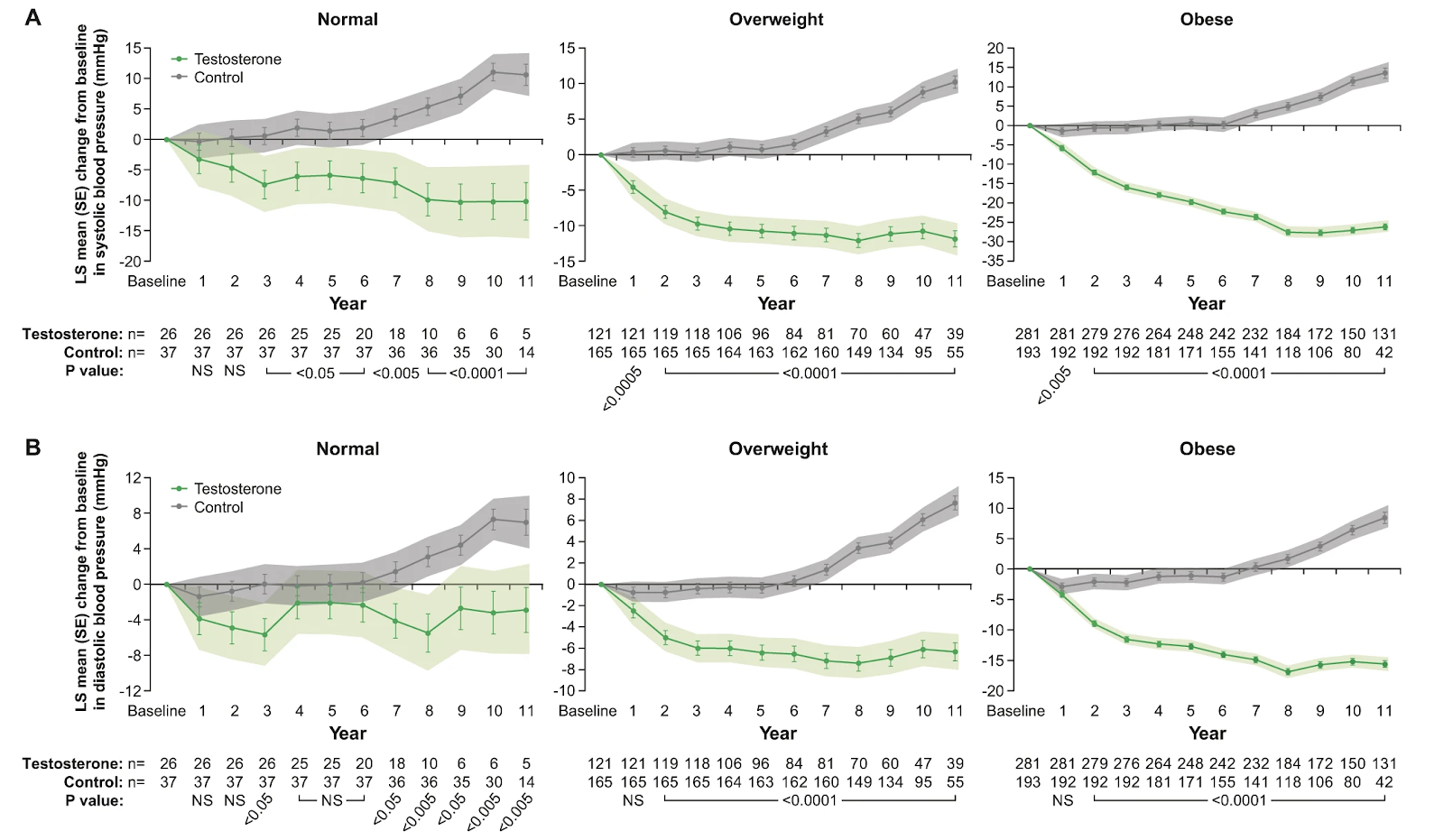
Furthermore, liver function significantly improved during the first 12 to 18 months of therapy and stabilized for the remainder of the study period. Treatment also greatly decreased blood levels of C-reactive protein, a measure of inflammation that is linked to increased risk of cardiovascular disease.
Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes, 2006
Design: This was a double-blind placebo-controlled crossover study in 24 hypogonadal men (10 treated with insulin) over the age of 30 years with type 2 diabetes.
Methods: Patients were treated with i.m. testosterone 200 mg every 2 weeks or placebo for 3 months in random order, followed by a washout period of 1 month before the alternate treatment phase. The primary outcomes were changes in fasting insulin sensitivity (as measured by homeostatic model index (HOMA) in those not on insulin), fasting blood glucose and glycated haemoglobin. The secondary outcomes were changes in body composition, fasting lipids and blood pressure. Statistical analysis was performed on the delta values, with the treatment effect of placebo compared against the treatment effect of testosterone.
Results: Testosterone therapy reduced the HOMA index (-1.73 +/- 0.67, P = 0.02, n = 14), indicating an improved fasting insulin sensitivity. Glycated haemoglobin was also reduced (-0.37 +/- 0.17%, P = 0.03), as was the fasting blood glucose (-1.58 +/- 0.68 mmol/l, P = 0.03). Testosterone treatment resulted in a reduction in visceral adiposity as assessed by waist circumference (-1.63 +/- 0.71 cm, P = 0.03) and waist/hip ratio (-0.03 +/- 0.01, P = 0.01). Total cholesterol decreased with testosterone therapy (-0.4 +/- 0.17 mmol/l, P = 0.03) but no effect on blood pressure was observed.
Beneficial effects of 2 years of administration of parenteral testosterone undecanoate on the metabolic syndrome and on non-alcoholic liver steatosis and C-reactive protein, 2009
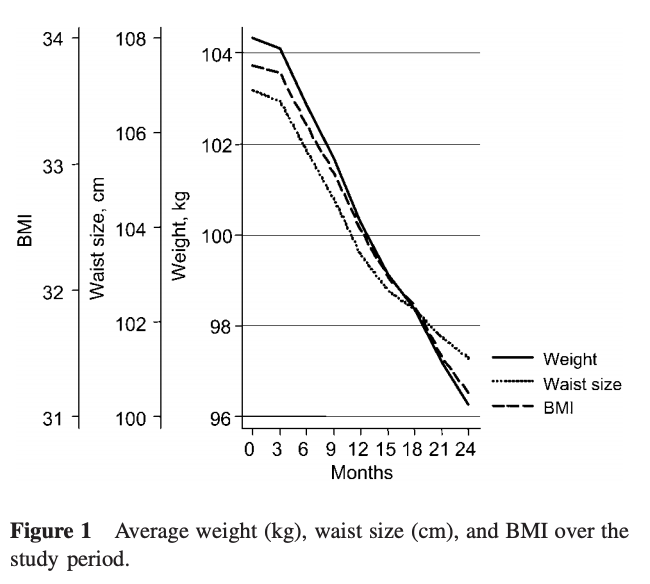
Materials and methods: A total of 122 hypogonadal men (18–83 years, mean 59.6+-8.0 years; n=11<45 years, n=25<55 years, n=53<65 years) were included in the study. Their baseline testosterone levels were between 14 and 451 ng/dL (normal = 490 ng/dL) and were treated with parenteral testosterone undecanoate for 2 years as the sole intervention (administration at 0 and 6 weeks, and thereafter every 12 weeks).
Results: Plasma testosterone increased from 330 +- 190 ng/dL to 401 +- 150 ng/mL (p=0.01) at 3 months, and then stabilized at 680+-130 ng/mL after the first 6 months. There was a remarkable progressive linear decline in body weight, body mass index, and waist circumference over the entire study period. Plasma cholesterol decreased significantly over the first 12 months, and then stabilized. Plasma glucose, triglycerides, low-density lipoprotein cholesterol, and C-reactive protein decreased significantly and high-density lipoprotein cholesterol increased significantly over the 24-month study period in a non-linear manner. There was a significant decrease in aspartate aminotransferase and alanine aminotransferase levels over the first 9 and 12 months, and then values leveled off. Changes in variables were largely correlated with changes in testosterone levels.
At baseline, 47 out of 122 male subjects fulfilled the metabolic syndrome criteria as defined by the NCEP (29), and
after 1 year of testosterone treatment this number had declined to 17 out of 122 male subjects, with a further decline to 11 out of 122 male subjects after 24 months.
Effect of 2 Years of Testosterone Replacement on Insulin Secretion, Insulin Action, Glucose Effectiveness, Hepatic Insulin Clearance, and Postprandial Glucose Turnover in Elderly Men, 2007
RESEARCH DESIGN AND METHODS—55 elderly men with relative testosterone deficiency ingested a labeled mixed meal and underwent a frequently sampled labeled intravenous glucose tolerance test before and after either placebo or treatment with testosterone patch (5 mg/day) for 2 years.
RESULTS—Despite restoring bioavailable testosterone to values observed in young men, the change (24 months minus baseline values) in fasting and postprandial glucose, insulin, and C-peptide concentrations and meal appearance, glucose disposal, and endogenous glucose production were virtually identical to those observed after 2 years of placebo. The change over time in insulin and C-peptide concentrations post–intravenous glucose injection also did not differ. Furthermore, the change over time in insulin action and glucose effectiveness (measured with the unlabeled and labeled “oral” and “intravenous” minimal models), as well as insulin secretion and hepatic insulin clearance (measured with the C-peptide model), did not differ in the testosterone and placebo groups.
CONCLUSIONS—We conclude that 2 years of treatment with testosterone in elderly men does not improve carbohydrate tolerance or alter insulin secretion, insulin action, glucose effectiveness, hepatic insulin clearance, or the pattern of postprandial glucose metabolism. Thus, testosterone deficiency is unlikely the cause of the age-associated deterioration in glucose tolerance commonly observed in elderly men.
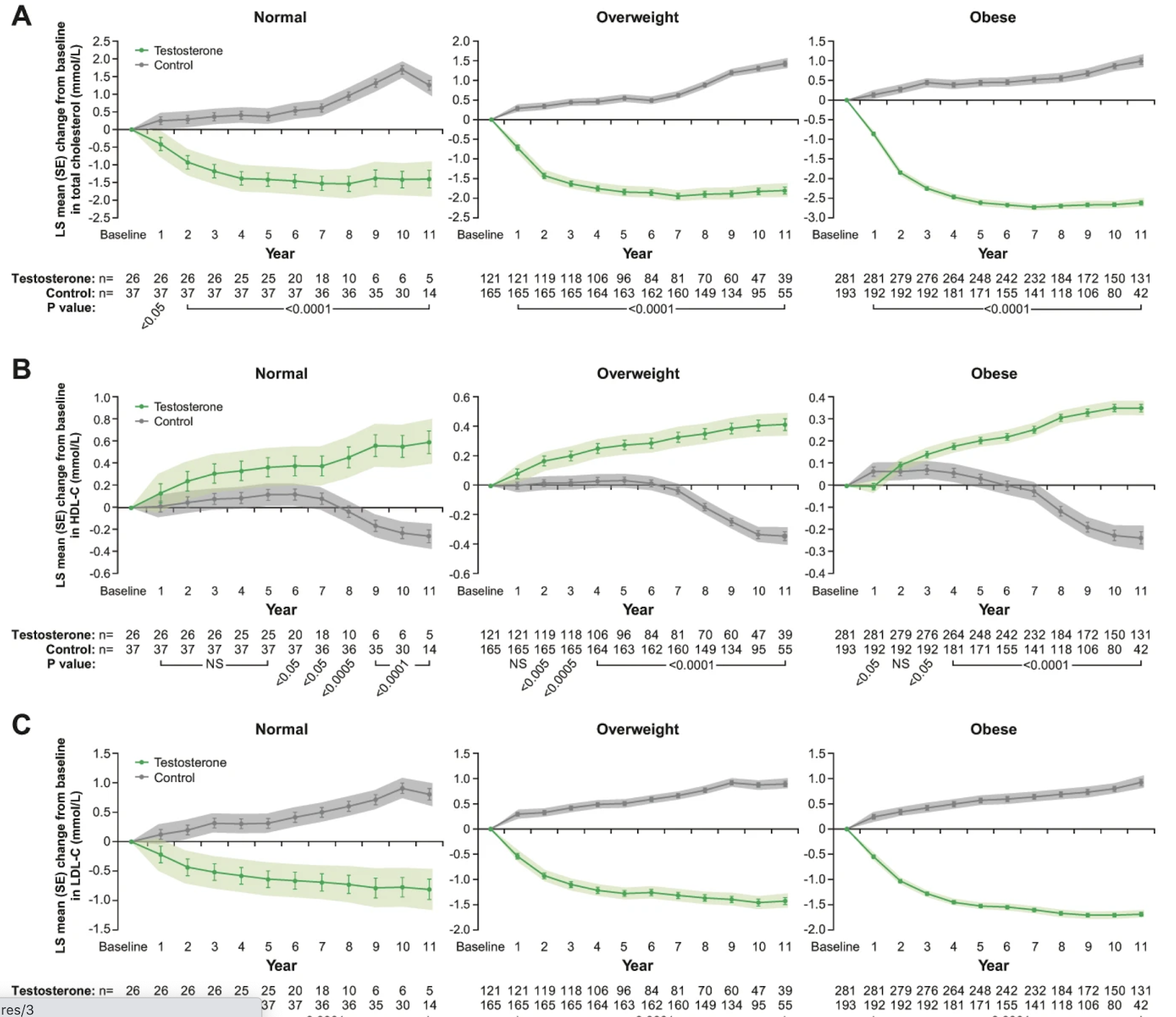
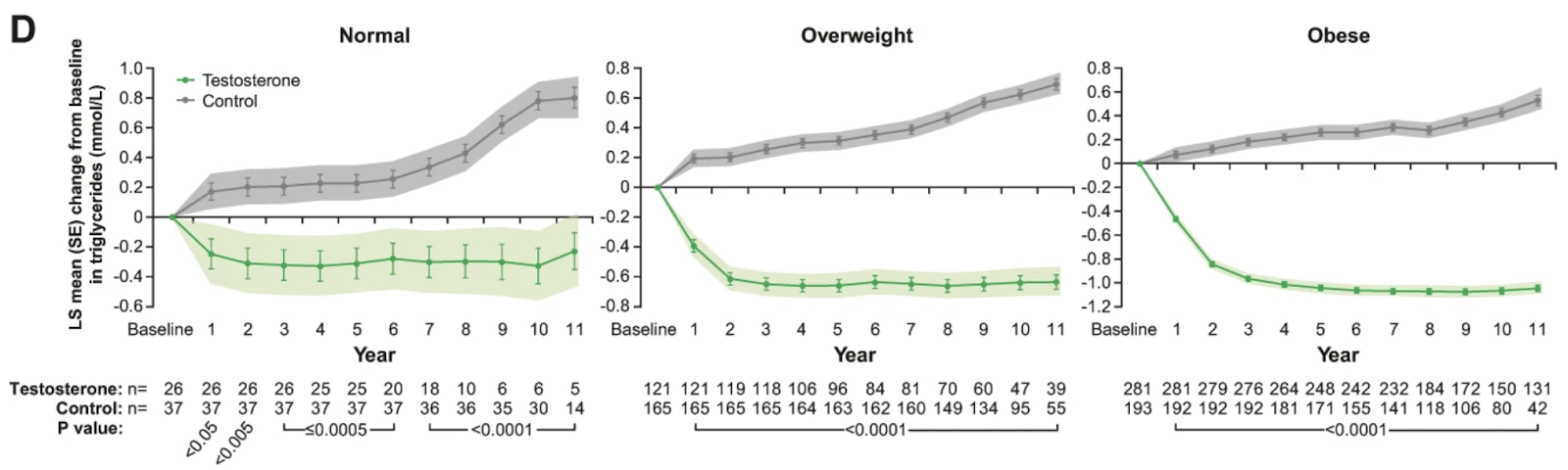
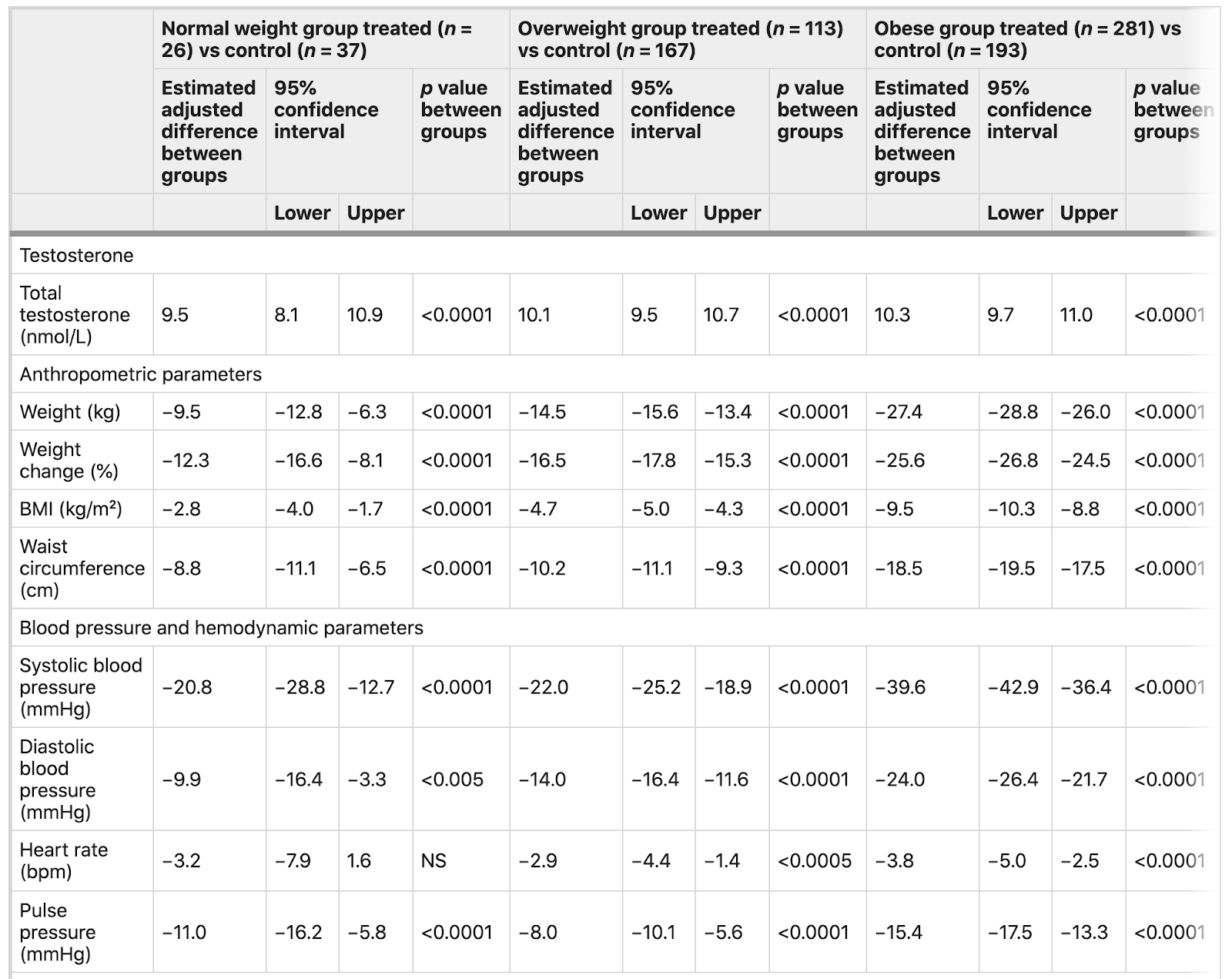
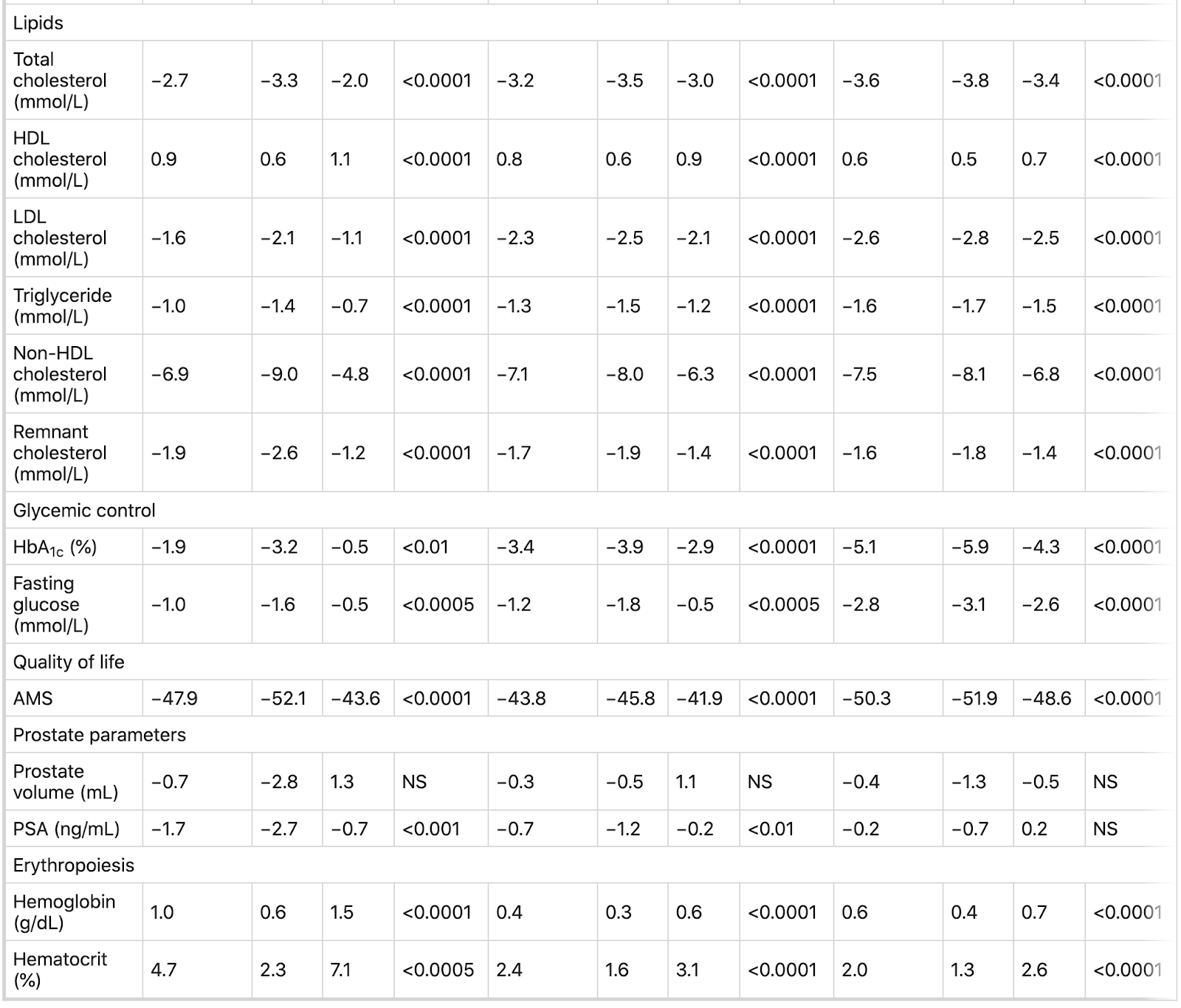
Differential effects of 11 years of long-term injectable testosterone undecanoate therapy on anthropometric and metabolic parameters in hypogonadal men, 2020
Hypogonadal men (n = 823) with total T ≤ 12.1 nmol/L = 350 (age: 60.6 ± 7.0 years). . T undecanoate 1000 mg injections (TU) were administered every 12 weeks following an initial 6-week interval.
Results
Long-term TTh in hypogonadal men, irrespective of weight at baseline, produced improvements in body weight, waist circumference (WC) and body mass index (BMI). Furthermore, TTh decreased fasting blood glucose and HbA1c and improved lipid profiles. Gradual decreases in blood pressure (systolic and diastolic) and pulse pressure occurred in men treated with T in each group. Marked reductions in mortality and major cardiovascular events were recorded in men receiving TTh (HR=(0.47, 0.39, 0.21) for the normal weight, overweight, obese respectively.
Conclusions
Our findings demonstrate that TTh produces reductions in weight, WC, and BMI. There were 77 (19.5%) deaths in the untreated groups and 23 (5.4%) in the T-groups. Based on these findings we suggest that long-term TTh in overweight and obese hypogonadal men produces progressive and sustained weight loss and that TTh may contribute to reductions in mortality and incident major adverse cardiovascular events.

c Changes in BMI (kg/m²) in hypogonadal men with normal weight, overweight or obesity at baseline treated with or without testosterone therapy. d Changes in waist circumference in hypogonadal men with normal weight, overweight or obese at baseline treated with or without testosterone therapy. Data are shown as least squares means ± standard errors. Shaded areas represent 95% confidence intervals. P values indicate statistical significance between groups for each year.

Effects of long-term treatment with testosterone on weight and waist size in 411 hypogonadal men with obesity classes I-III: observational data from two registry studies (link) (testosterone undecanoate)
Background/Objectives:
Long-term testosterone replacement therapy (TRT) up to 5 years has been shown to produce progressive and sustainable weight loss (WL) in hypogonadal men. This study investigated effects of long-term TRT up to 8 years in hypogonadal men with different obesity classes.
Results:
In all three classes of obesity, T therapy produced significant WL, decrease in waist circumference (WC) and body mass index (BMI). In patients with class I obesity, mean weight decreased from 102.6±6.4 to 84.1±4.9 kg, change from baseline: −17.4±0.5 kg and −16.8±0.4%. WC in this group of patients decreased from 106.8±7.4 to 95.1±5.3 cm, change from baseline: −10.6±0.3 cm. BMI decreased from 32.69±1.4 to 27.07±1.57, change from baseline: −5.52±0.15 kg m−2. In patients with class II obesity, weight decreased from 116.8±6.9 to 91.3±6.3 kg, change from baseline: −25.3±0.5 kg and −21.5±0.4%. WC decreased from 113.5±7.5 to 100.0±5.4 cm, change from baseline: −13.9±0.4 cm. BMI decreased from 37.32±1.45 to 29.49±1.71, change from baseline: −8.15±0.17 kg m−2. In patients with class III obesity, weight decreased from 129.0±5.6 to 98.9±4.8 kg, change from baseline: −30.5±0.7 kg and −23.6±0.5%. WC decreased from 118.5±5.6 to 103.8±4.9 cm, change from baseline: −14.3±0.4 cm. BMI decreased from 41.93±1.48 to 32.46±1.59, change from baseline −9.96±0.29 kg m−2.
Conclusions:
Testosterone therapy appears to be an effective approach to achieve sustained WL in obese hypogonadal men irrespective of severity of obesity. Based on these findings we suggest that T therapy offers safe and effective treatment strategy of obesity in hypogonadal men.
Clomiphene citrate is safe and effective for long-term management of hypogonadism, 2011

Patients were commenced on CC 25 mg every other day and were titrated to 50 mg every other day based on the treatment serum T level. The target total T level was arbitrarily set at 550 ± 50 ng/dL.
Patients were free of side-effects, suggesting that CC is effective in the long-term management of HG.
Long-Term Safety and Efficacy of Clomiphene Citrate for the Treatment of Hypogonadism, 2019
A total of 400 patients underwent clomiphene citrate treatment for a mean ± SD of 25.5 ± 20.48 months (range 0 to 84). Of the patients 280 received clomiphene citrate for 3 years or less (mean 12.75 ± 9.52 months) and 120 received it for more than 3 years (mean 51.93 ± 10.52 months). Of men on clomiphene citrate for more than 3 years 88% achieved eugonadism, 77% reported improved symptoms and 8% reported side effects. Estradiol was significantly increased following clomiphene citrate treatment. Results did not significantly differ between patients treated for more than 3, or 3 or fewer years. The most common side effects reported by patients treated more than 3 years included changes in mood in 5, blurred vision in 3 and breast tenderness in 2. There was no significant adverse event in any patient treated with clomiphene citrate.
A Comparison of Secondary Polycythemia in Hypogonadal Men Treated with Clomiphene Citrate versus Testosterone Replacement: A Multi-Institutional Study, 2017
Overall, men on testosterone replacement therapy were older than clomiphene citrate treated men (age 51.5 vs 38 years). Men on testosterone replacement had longer treatment duration than clomiphene citrate treated men (19.6 vs 9.2 months). For testosterone replacement therapy and clomiphene citrate the mean change in hematocrit was 3.0% and 0.6%, and the mean change in serum testosterone was 333.1 and 367.6 ng/dl, respectively. The prevalence of polycythemia in men on testosterone replacement was 11.2% vs 1.7% in men on clomiphene citrate (p = 0.0003). This significance remained on logistic regression after correcting for age, site, smoking history and pretreatment hematocrit.
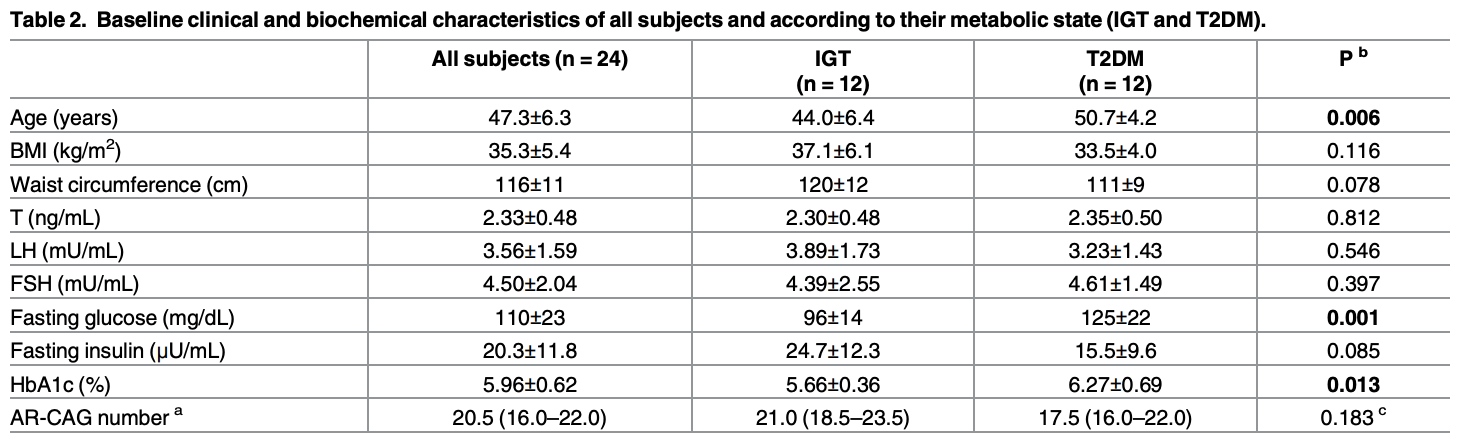
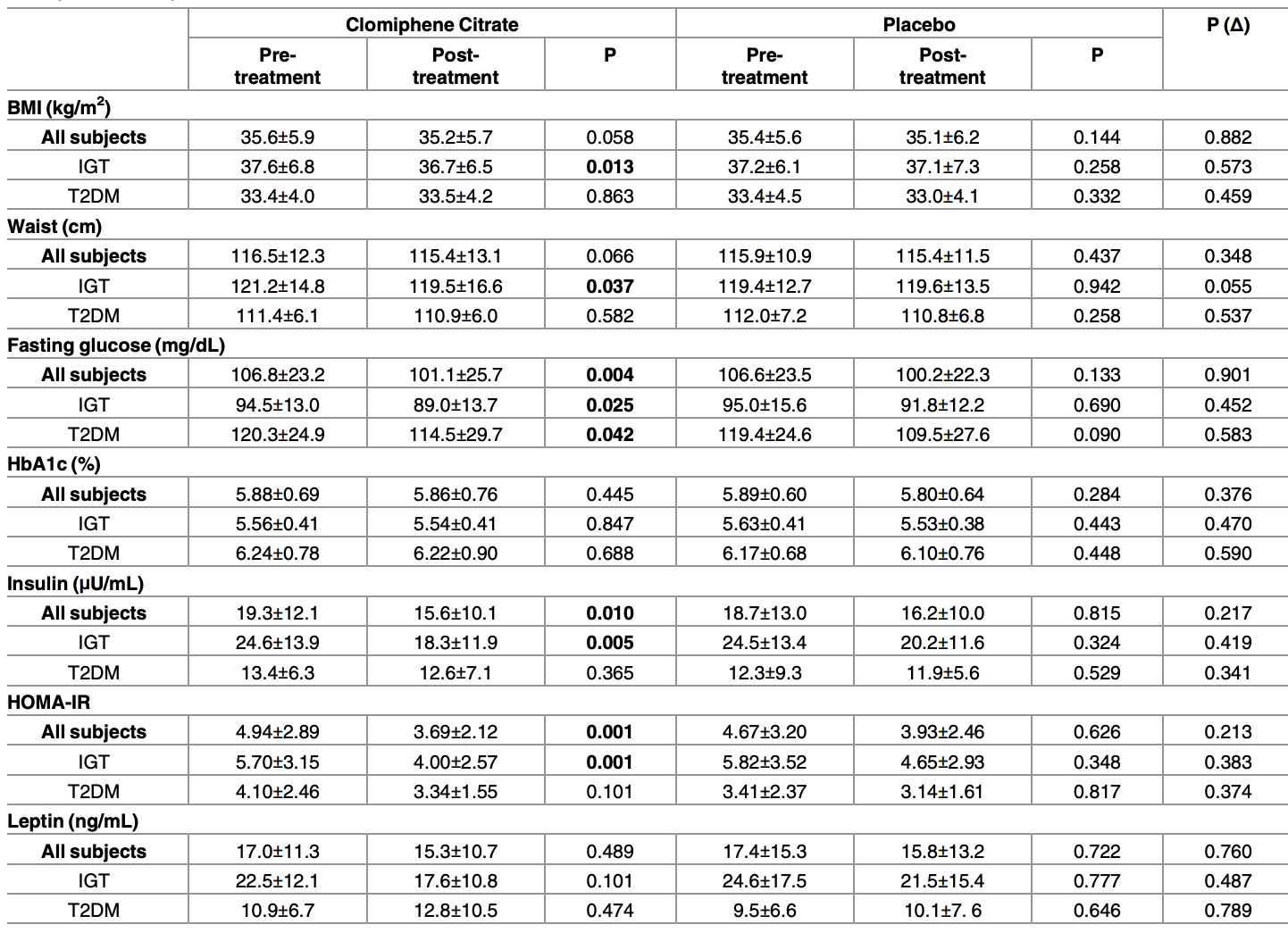
Clomiphene citrate (Clomid) effect in obese men with low serum testosterone treated with metformin due to dysmetabolic disorders, 2017
[Clomid lowers HOMA-IR and fasting insulin.]
Methods
24 obese men, aged 47.3 ±. 6.3 (range 35–55 years), with low T level (≤3 ng/mL) and naïve diagnosis of IGT or T2DM were included. Subjects were randomized to CC 25 mg/day or placebo (Plac) with MET 2 g/day for 3 months. After a 6-week wash-out period, subjects were moved to the alternative arm for additional 3 months. Clinical evaluation and blood exams performed prior to and at the end of treatment.
Results
Of 24 randomized, 21 were evaluable, classified as IGT (n = 11) or T2DM (n = 10). Compared to baseline levels, T levels increased significantly after 3 months of CC treatment (3.03±0.80 to 5.99±1.67 ng/mL P<0.001) but not after the Plac treatment (2.87±0.78 to 3.09±0.84 ng/mL P<0.001 between the treatments). T changes were similar in IGT and T2DM subjects. Gonadotropins as well raised significantly after CC treatment (LH 3.83±1.45 to 8.53±6.40 mU/mL; FSH 4.84±1.67 to 10.15±5.08 mU/mL P<0.001 respectively), whereas no changes for LH (3.51±1.59 to 3.63±1.39 mU/mL) but a smooth increased for FSH (4.61±2.49 to 5.39±2.65 mU/mL; P = 0.004) were shown after Plac treatment (LH P = 0.001 and FSH P = 0.002 between treatments). Furthermore, fasting glucose (106.8±23.2 to 101.1±25.7 mg/dL; P = 0.004), insulin (19.3±12.1 to 15.6±10.1 μU/mL; P = 0.010) and HOMA-IR (4.94±2.89 to 3.69±2.12; P = 0.001) decreased significantly during the CC treatment period, whereas no significant changes were observed in any of these parameters in the Plac treatment.
Clomiphene for hypogonadism complicated by polycythemia (link)
At the first visit, the patient’s hemoglobin was 18.5 g/dL; hematocrit, 55% (normal range 38.8%–50%); and serum creatinine, 1.4 mg/dL (normal range 0.6–1.2 mg/dL). The testosterone was discontinued due to secondary polycythemia. Six weeks after discontinuing testosterone therapy, his hemoglobin was 16.1 g/dL and hematocrit was 49.5%. His follicle-stimulating hormone level was 8.6 mIU/mL; luteinizing hormone, 7.7 mIU/mL; prolactin, 10.5 ng/mL; and prostate-specific antigen, 1.3 ng/mL. He had a low total testosterone of 219 pg/mL (2.29 nmol/L) and a low free testosterone of 23.5 pg/mL (0.14 nmol/L).
Two months later, the patient was doing well off testosterone but still continued to have some sexual dysfunction. Magnetic resonance imaging with contrast of the head revealed no pituitary lesions. His hemoglobin was 15.8 g/dL and hematocrit was 46.7%. The patient was started on clomiphene 25 mg daily, increasing after a few weeks to 50 mg daily based on suggested treatment guidelines. On clomiphene, his serum total testosterone level was 388 ng/dL (13.46 nmol/L) and free testosterone was 41.5 pg/mL (0.25 nmol/L) with an improvement in his libido and erectile dysfunction associated with hypogonadism.
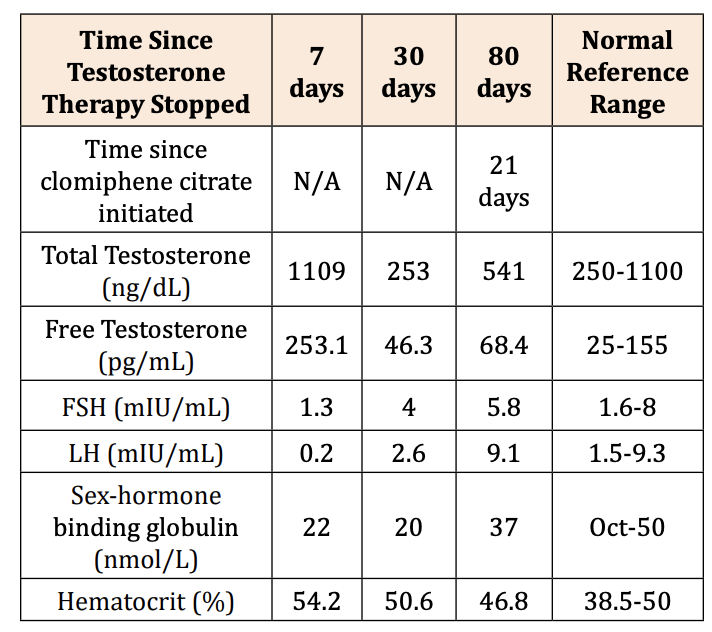
Effective Treatment of Secondary Hypogonadism with Clomiphene Citrate in a Male Patient with Secondary Polycythemia and History of Transient Ischemic Attack, 2020
Due to no improvement in clinical status with lifestyle improvements and a decreasing AM testosterone level from 283ng/dl to 253ng/dl and free testosterone decreasing to 49pg/ml, the decision was made to start the patient on clomiphene citrate 25 mg daily. Repeat laboratory testing after the patient had been on clomiphene citrate for four weeks, and off of testosterone replacement therapy for approximately 80 days showed significant improvement in testosterone levels, FSH, and LH (Table 2). Hematocrit had also normalized to 46.8 % indicating resolution of polycythemia. The patient reported satisfactory outcomes with normalization of his libido, morning erections and ability to have sexual intercourse.
Metformin and/or Clomiphene Do Not Adversely Affect Liver or Renal Function in Women with Polycystic Ovary Syndrome, 2011
Six hundred twenty-six infertile women with PCOS with serum liver function parameters less than twice the upper limit of normal were included. Clomiphene citrate (n = 209), MET (n = 208), or combined (n = 209) were given for up to 6 months.
Renal function improved in all treatment arms with significant decreases in serum blood urea nitrogen levels (range, −14.7 to −21.3%) as well as creatinine (−4.2 to −6.9%). There were similar decreases in liver transaminase levels in the clomiphene citrate and combined arms (−10% in bilirubin, −9 to −11% in transaminases) without significant changes in the MET arm. When categorizing baseline bilirubin, aspartate aminotransferase, and alanine aminotransferase into tertiles, there were significant within-treatment arm differences between the tertiles with the highest tertile having the largest decrease from baseline regardless of treatment arm.
Conclusion:
Women with PCOS can safely use metformin and clomiphene even in the setting of mildly abnormal liver function parameters, and both result in improved renal and liver function.

Safety and Efficacy of Clomiphene Citrate in the Treatment of Secondary Hypogonadism. A Retrospective Study, 2021
Data was obtained from the Veterans Administration Data Warehouse through the Veterans Administration Informatics and Computing Infrastructure. 405,824 male patients with a diagnosis of hypogonadism (87.1%)and infertility (12.9%). nationally at the VA. Of these, 9566 patients have been treated with clomiphene citrate and 232,123 with various testosterone therapy. The two groups were then matched by propensity method to controls at a ratio of about 1:1 for Age, race, BMI and time for follow-up as potential confounding factors hat could have affected inclusion in the study controls.
Results: Clomid treatment normalized testosterone levels in 53.2% versus 46.8% in the testosterone group (OR 1.32 P<0.005). All-cause mortality was in the clomid group 0.16% and 1.62%in the testosterone group (OR 0.16 P<0.001). The incidence of new Osteoporosis for clomid was 3.9 % versus 5.9% for testosterone (OR 0.65 P<0.001)
Conclusion: This is a retrospective study comparing the efficacy and side effects of clomiphene versus testosterone for treatment of hypogonadism. The study showed that clomiphene is more effective than testosterone to treat secondary hypogonadism. We also found decreased overall mortality and incidence of polycythemia and osteoporosis.
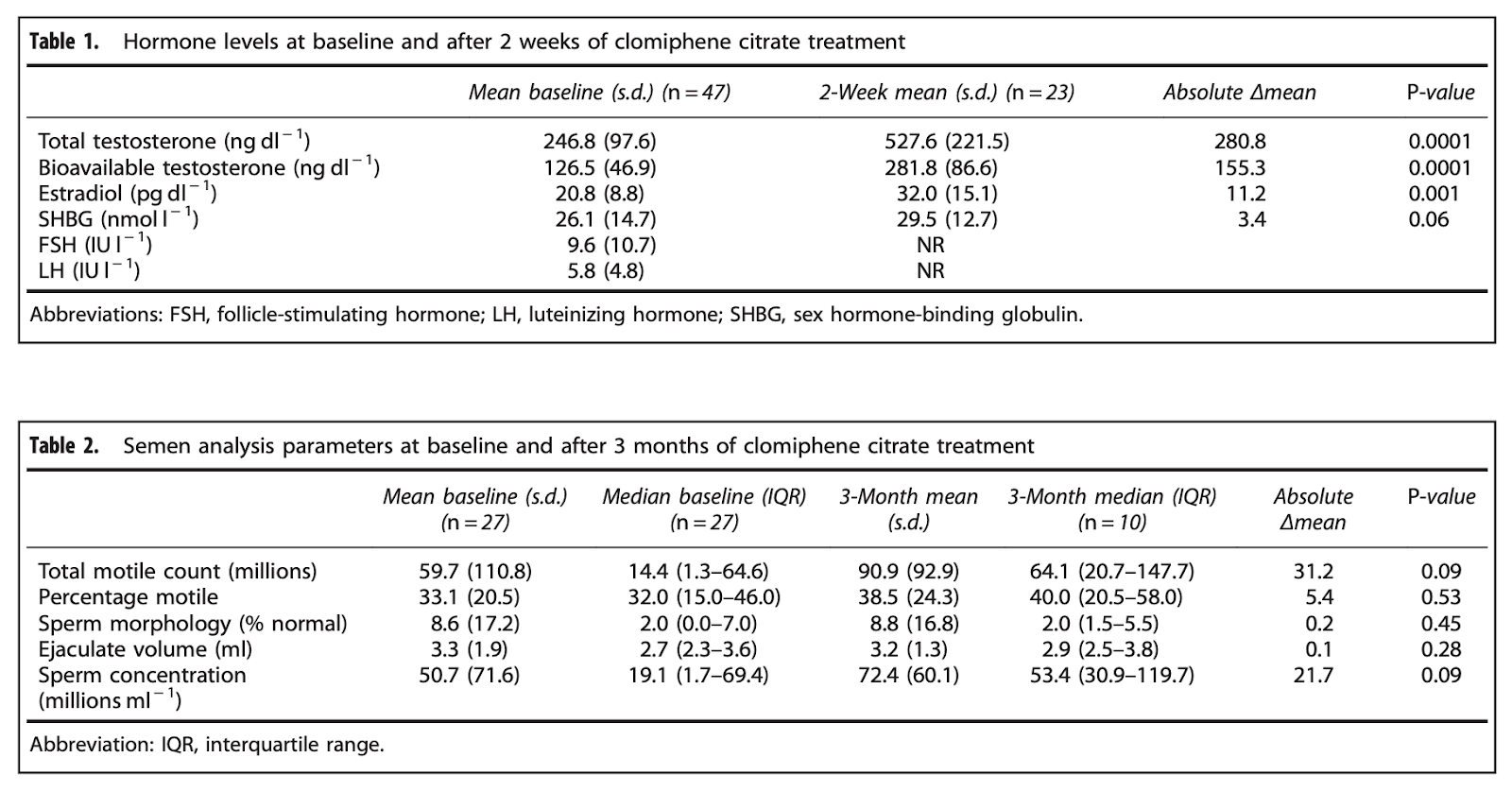
The safety and efficacy of clomiphene citrate in hypoandrogenic and subfertile men, 2015
47 men between 18 and 55 years placed on 50 mg CC every other day. We evaluated the effect of CC on testosterone after 2 weeks, rates of adverse effects and predictors of CC response.
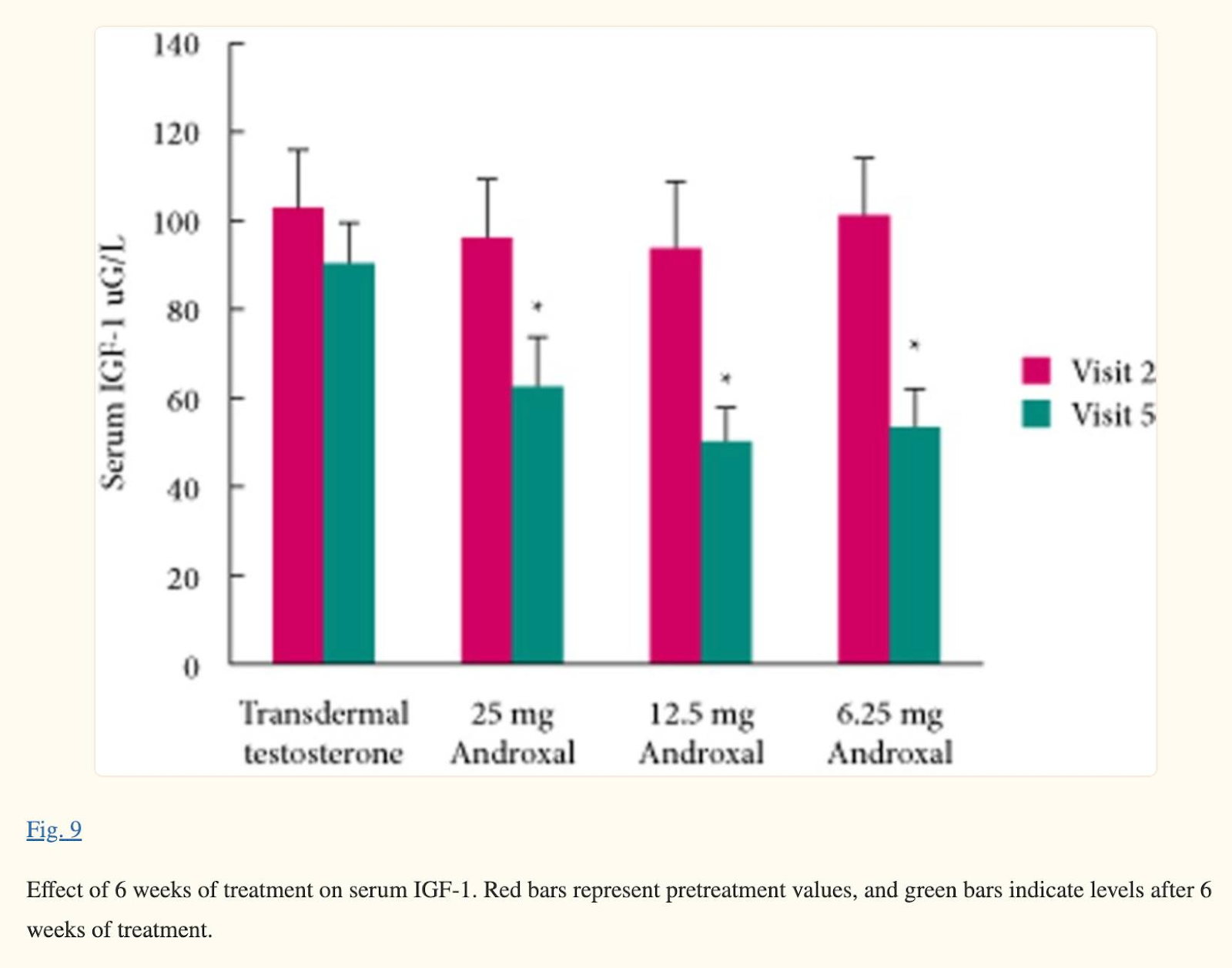
Testosterone restoration using enclomiphene citrate in men with secondary hypogonadism: a pharmacodynamic and pharmacokinetic study, 2013
One of the isomers in clomid potently lowers IGF1.
Clomiphene citrate increases insulin-like growth factor binding protein-1 and reduces insulin-like growth factor-I without correcting insulin resistance associated with polycystic ovarian syndrome, 2000
Plasma concentrations of IGF-I decreased by 31.5% (434 ± 84 versus 297 ± 71 ng/ml; P < 0.05) after 5 days of clomiphene therapy, whereas plasma concentrations of IGFBP-1 increased by ~28.1% (26.3 ± 4 versus 36.6 ± 7 ng/ml; P < 0.05). This gave a 56.5% reduction in the IGF-I:IGFBP-1 ratio (21.9 versus 9.53). No significant changes in basal plasma concentrations of fasting insulin or area under the insulin curve were observed in response to oral loading.
Decline in insulin-like growth factor I levels after clomiphene citrate does not correct hyperandrogenemia in polycystic ovary syndrome, 1998
In PCOS patients a significant increase in estradiol (110 +/- 11 to 245 +/- 58 pmol/L; P < 0.05) and estrone (301 +/- 32 to 401 +/- 90 pmol/L; P < 0.05) levels and a significant lowering of IGF-I levels (330 +/- 43 to 214 +/- 27 micrograms/L; P < 0.05) were observed after CC treatment.
Clomiphene citrate may help men with acromegaly (link)
Dr. Duarte and colleagues enrolled 16 men, ages 36 to 79, with IGF-1 above the upper limit of normal for at least one year despite medical therapies, and low testosterone levels.
The researchers measured hormone levels before and during the study. For three months, they added 50 mg/day of the selective estrogen receptor modulator (SERM) clomiphene citrate to the men's previous treatment.
Serum IGF-1 levels decreased by 41% (424 ng/mL to 250; p<0.0004) and seven patients (44%) achieved normal IGF-1 levels. Total serum testosterone levels increased by 209% (from 282 ng/dL to 497 ng/dL) and reached normal levels in four (67%) of the patients considered hypogonadal.
Testosterone Replacement Therapy Increases Longevity In Men (link, link)
The research (US Veterans study) studied data on more than 83,000 men aged 50 or above and having low testosterone levels. The study spread on the period between 1999 and 2014. The participants were divided by researchers into three different clinical groups. Some were treated until their testosterone levels returned to normal, some were untreated, and some were treated but without reaching normal levels.
The findings have shown a sharp contrast between those who were untreated and those who were treated until attained normal testosterone levels. Those aged men who had their hormone level restored to normal were 24 percent less likely to suffer a heart attack, 36 percent less likely to suffer a stroke and 56 percent less likely to die during the follow-up period.
It is still unknown for what reasons testosterone's has apparent benefits for the overall survival rate. According to the researchers, among the possible explanations are insulin sensitivity, body fat, blood platelets, lipids, inflammation and other biological pathways.
Testosterone treatment and mortality in men with low testosterone levels, 2012
An observational study of mortality in testosterone-treated compared with untreated men.
The study was conducted with a clinical database that included seven Northwest Veterans Affairs medical centers.
Patients included a cohort of 1031 male veterans, aged older than 40 yr, with low total testosterone [≤250 ng/dl (8.7 nmol/liter)] and no history of prostate cancer, assessed between January 2001 and December 2002 and followed up through the end of 2005.
Testosterone treatment was initiated in 398 men (39%) during routine clinical care. The mortality in testosterone-treated men was 10.3% compared with 20.7% in untreated men (P<0.0001) with a mortality rate of 3.4 deaths per 100 person-years for testosterone-treated men and 5.7 deaths per 100 person-years in men not treated with testosterone. After multivariable adjustment including age, body mass index, testosterone level, medical morbidity, diabetes, and coronary heart disease, testosterone treatment was associated with decreased risk of death (hazard ratio 0.61; 95% confidence interval 0.42-0.88; P = 0.008). No significant effect modification was found by age, diabetes, or coronary heart disease.
Impact of Testosterone Replacement Therapy on Myocardial Infarction, Stroke, and Death in Men With Low Testosterone Concentrations in an Integrated Health Care System, 2016
The aim of this study was to assess the effect of testosterone replacement therapy (TRT) on cardiovascular outcomes. Men (January 1, 1996, to December 31, 2011) with a low initial total testosterone concentration, a subsequent testosterone level, and >3 years of follow-up were studied. Levels were correlated with testosterone supplement use. The primary outcome was major adverse cardiovascular events (MACE), defined as a composite of death, nonfatal myocardial infarction, and stroke at 3 years. Multivariate adjusted hazard ratios (HRs) comparing groups of persistent low (<212 ng/dl, n = 801), normal (212 to 742 ng/dl, n = 2,241), and high (>742 ng/dl, n = 1,694) achieved testosterone were calculated by Cox hazard regression. A total of 4,736 men were studied. Three-year rates of MACE and death were 6.6% and 4.3%, respectively. Subjects supplemented to normal testosterone had reduced 3-year MACE (HR 0.74; 95% confidence interval [CI] 0.56 to 0.98, p = 0.04) compared to persistently low testosterone, driven primarily by death (HR 0.65, 95% CI 0.47 to 0.90). HRs for MI and stroke were 0.73 (95% CI 0.40 to 1.34), p = 0.32, and 1.11 (95% CI 0.54 to 2.28), p = 0.78, respectively. MACE was noninferior but not superior for high achieved testosterone with no benefit on MI and a trend to greater stroke risk. In conclusion, in a large general health care population, TRT to normal levels was associated with reduced MACE and death over 3 years but a stroke signal with high achieved levels suggests a conservative approach to TRT.
Testosterone treatment and cardiovascular events in prescription database studies (link)
In four studies, including 69 282 men, T treatment was associated with a decreased risk for all-cause mortality ranging from 22% to 66%.19,27,31,32 No study found an overall increased mortality risk, but one study found a transient 11% increased mortality risk with T initiation (31).
Outcomes of clomiphene citrate treatment in young hypogonadal men, 2012
We prospectively evaluated 86 men with hypogonadism (HG) as confirmed by two consecutive early morning testosterone measurements <300 ng/dL. • The cohort included all men with HG presenting to our clinic between 2002 and 2006 who, after an informed discussion, elected to have CC therapy. CC was commenced at 25 mg every other day and titrated to 50 mg every other day. The target testosterone level was 550 ± 50 ng/dL.
Results: Patients' mean (standard deviation [sd]; range) age was 29 (3; 22-37) years. Infertility was the most common reason (64%) for seeking treatment. The mean (sd) duration of CC treatment was 19 (14) months. At the last evaluation, 70% of men were using 25 mg CC every other day, and the remainder were using 50 mg every other day. All mean testosterone and gonadotropin measurements significantly increased during treatment. Subjectively, there was an improvement in all questions (except loss of height) on the ADAM questionnaire. More than half the patients had an improvement in at least three symptoms.
Clomiphene increases free testosterone levels in men with both secondary hypogonadism and erectile dysfunction: who does and does not benefit? 2003
A total of 178 men with secondary hypogonadism and ED received clomiphene citrate for 4 months. Sexual function improved in 75%, with no change in 25%
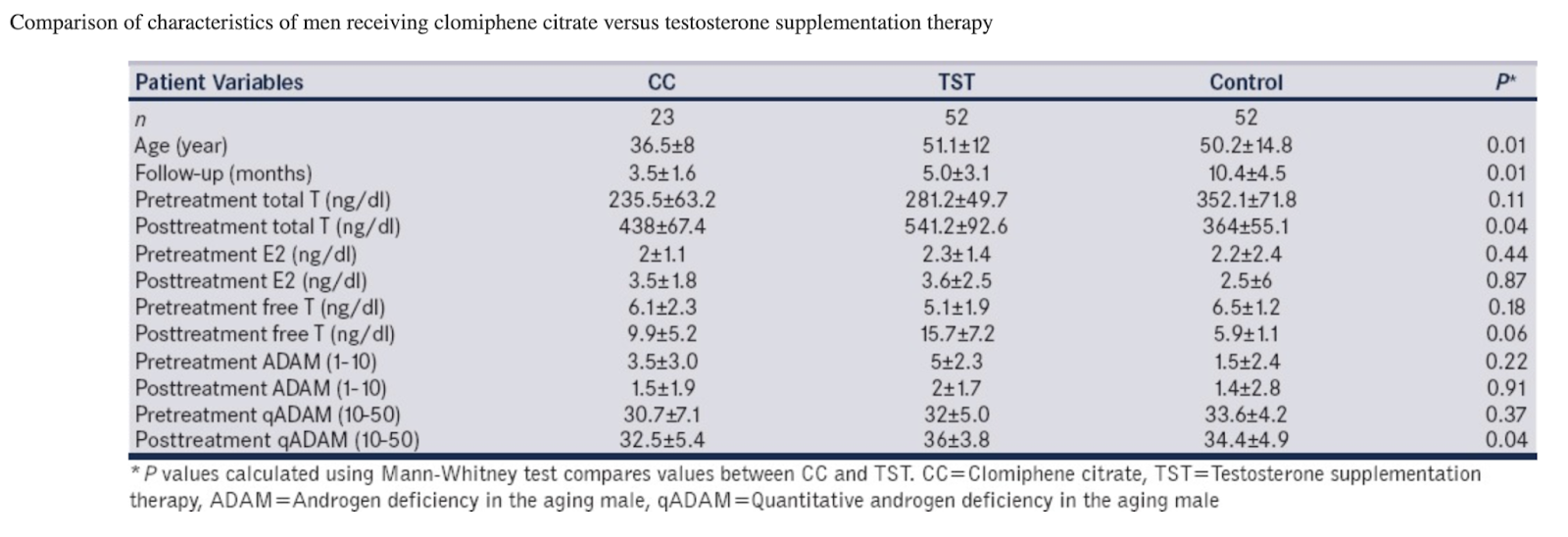
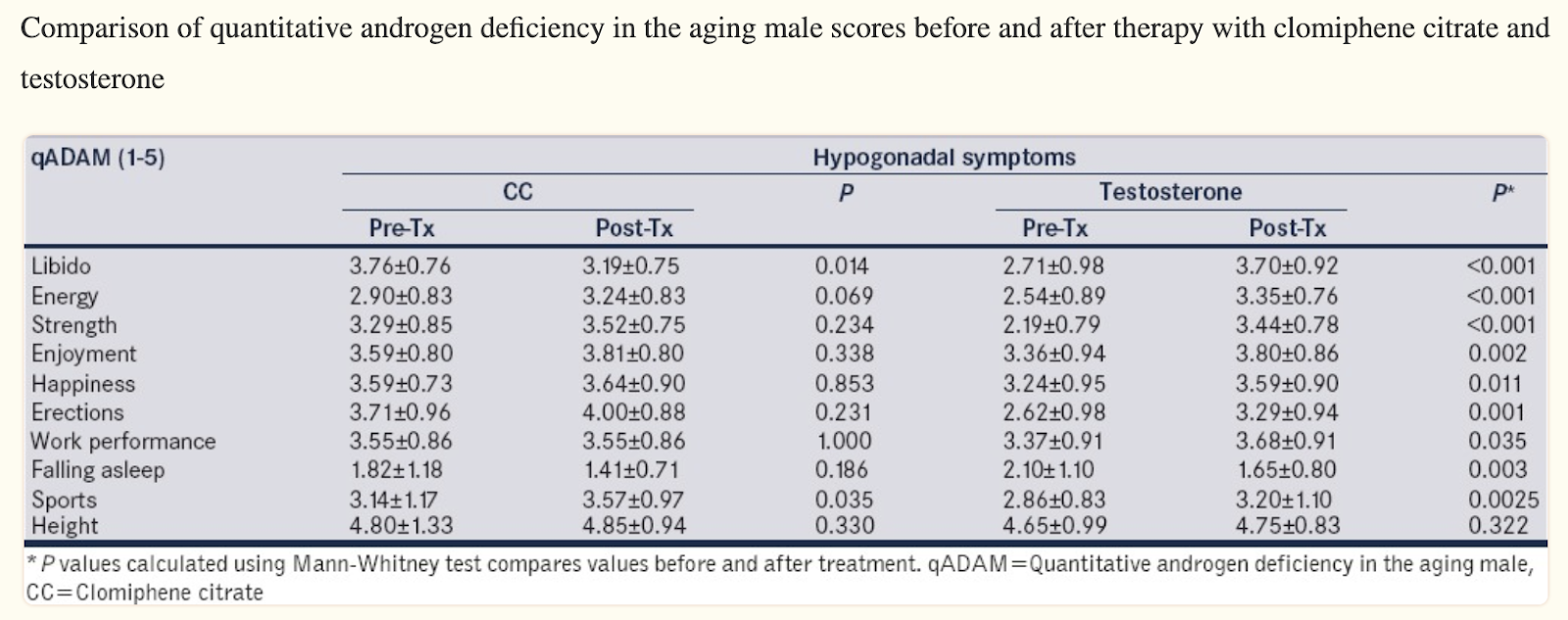
Testosterone versus clomiphene citrate in managing symptoms of hypogonadism in men, 2017
[This study can be ignored, because they don’t specify how long the treatment lasted. Over 3-5 yrs weight loss should improve nearly all sexual markers.]
Onset of effects of testosterone treatment and time span until maximum effects are achieved, 2011
Effects on sexual interest appear after 3 weeks plateauing at 6 weeks, with no further increments expected beyond. Changes in erections/ejaculations may require up to 6 months. Effects on quality of life manifest within 3–4 weeks, but maximum benefits take longer. Effects on depressive mood become detectable after 3–6 weeks with a maximum after 18–30 weeks. Effects on erythropoiesis are evident at 3 months, peaking at 9–12 months. Prostate-specific antigen and volume rise, marginally, plateauing at 12 months; further increase should be related to aging rather than therapy. Effects on lipids appear after 4 weeks, maximal after 6–12 months. Insulin sensitivity may improve within few days, but effects on glycemic control become evident only after 3–12 months. Changes in fat mass, lean body mass, and muscle strength occur within 12–16 weeks, stabilize at 6–12 months, but can marginally continue over years. Effects on inflammation occur within 3–12 weeks. Effects on bone are detectable already after 6 months while continuing at least for 3 years.
Testosterone in Metastatic Renal Cell Carcinoma Patients (FARETES) (link)
Methods:
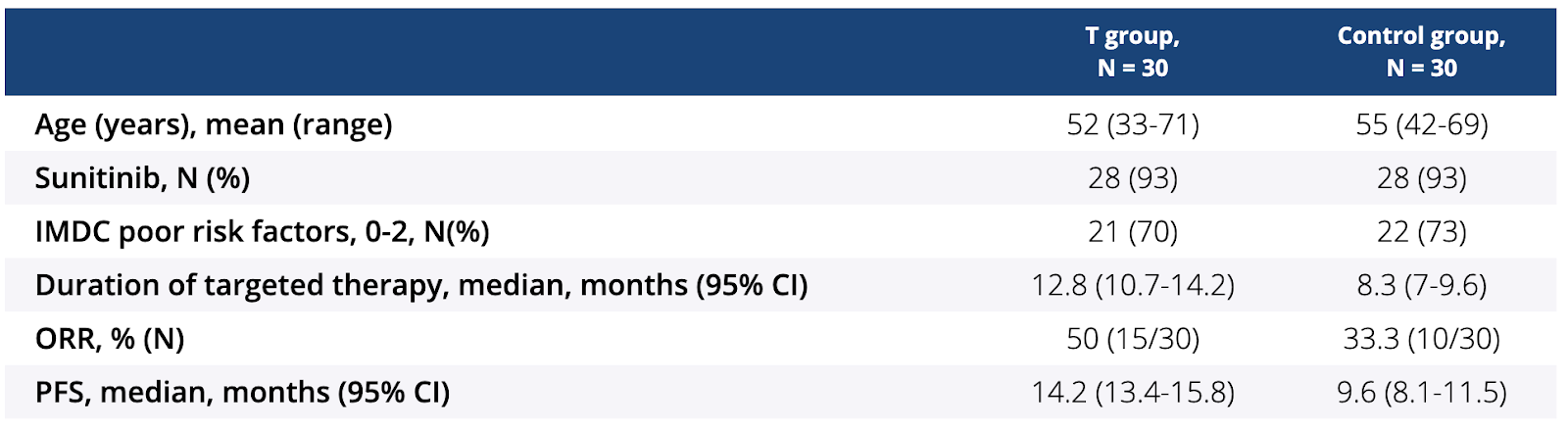
Sixty male patients with clear cell mRCC, normal PSA level, low testosterone level and no evidence of hypothyroidism receiving first-line sunitinib or pazopanib with fatigue were randomly assigned (1:1) to either T (Nebido, 1,000 mg) and targeted therapy or targeted therapy alone (control group). T was injected intramuscular deeply on Day 1 of a new treatment cycle. Exploratory endpoints included rate of adverse events (AE) of targeted therapy, duration of targeted therapy, objective response rate (ORR), progression-free survival (PFS) and overall survival (OS).
Results:
As of the data cutoff on October 17, 2018, median (range) follow-up was 15.2 (9.9 -16.5) months. No unexpected toxicity of T was observed. Grade 3-4 targeted therapy-related AE occurred in 11 (37%) and 3 (10%) patients in the control group and T group, respectively. Discontinuation due to AE was observed in 3% (1/30) of patients in the T group and in 17% (5/30) of patients in the control group. ORR and PFS were significantly better in the T group (all P < 0.05, Table). Median OS was not reached in either group
Conclusions:
T therapy could decrease rate of serious AE of targeted therapy. Male mRCC patients receiving T had longer duration of targeted therapy, better PFS and ORR. Larger trials are needed to evaluate efficacy of T in this group of patients.
Pharmacological Inhibition of Insulin Growth Factor-1 Receptor (IGF-1R) Alone or in Combination With Ruxolitinib Shows Therapeutic Efficacy in Preclinical Myeloproliferative Neoplasm Models, 2021
Even after development of the JAK1/JAK2 inhibitor ruxolitinib, myeloproliferative neoplasm (MPN) patients require novel therapeutic options. While ruxolitinib can considerably improve quality of life and prolong survival, it does not modify the natural disease course in most patients. Moreover, resistance develops with prolonged use. Therefore, various combination treatments are currently being investigated. Published data provide a compelling rationale for the inhibition of insulin growth factor-1 receptor (IGF-1R) signaling in MPN. Here we report that genetic and pharmacological inhibition of IGF-1R selectively reduced Jak2V617F-driven cytokine-independent proliferation ex vivo. Two different structurally unrelated IGF-1R inhibitors ameliorated disease phenotype in a murine MPN model and significantly prolonged survival. Moreover, in mice, low-dose ruxolitinib synergized with IGF-1R inhibition to increase survival. Our data demonstrate preclinical efficacy of IGF-1R inhibition in a murine MPN model.
EAU 2019: Testosterone Replacement Therapy May Slow Recurrence in Low-Risk Prostate Cancer
Study Background
Starting in 2008, a team of doctors from the University of California, Irvine, led by Thomas Ahlering, MD, began to carefully select patients for testosterone replacement after primary treatment of prostate cancer with robotic radical prostatectomy. They hoped this method would improve recovery of sexual function.
The team worked with 834 patients undergoing radical prostatectomy. They treated 152 low-risk patients with no evidence of disease with testosterone replacement therapy. After a median of 3.1 years following surgery, they tested the patients for biochemical recurrence of cancer, as indicated by measurement of prostate-specific antigen levels.
Study Findings
The researchers found that cancer had recurred in only approximately 5% of patients treated with testosterone, whereas cancer had recurred in 15% of the patients who did not receive testosterone. Overall, after accounting for differences between the groups, they found nearly a threefold reduction by 3 years.
Dr. Ahlering commented, “This is not what we set out to prove, so it was a big surprise: not only did testosterone replacement not increase recurrence, but it actually lowered recurrence rates. While the testosterone is not curing cancer per se, it is slowing the growth of cancer, giving an average of an extra 1.5 years before traces of cancer can be found. We already know that testosterone can help with physiological markers such as muscle mass, better cholesterol and triglyceride levels, and increased sexual activity, so this seems to be a win-win.”
He continued, “There have been smaller studies that have hinted testosterone may not be risky for certain patient groups, but this is the largest such study ever conducted. We’re not suggesting that treatment methods be changed just yet, but this puts us at the stage where we need to question the taboo against testosterone use in prostate cancer therapy—especially for low-risk patients after radical prostatectomy. We need the oncology/urology community to begin to review testosterone use.”
Testosterone supplementation after prostate cancer? (link)
NED, cancer gone => TRT appears safe, even beneficial. If residual cancer suspected, do the opposite of TRT.


Comments