L-Carnitine
Mitochondrial dysfunction due to a relative lack of micronutrients and substrates is implicated in the development of many chronic diseases.
L-carnitine is one of the key nutrients for proper mitochondrial function. It helps cellular energy production by transporting fatty acids into the mitochondria and acting as an ROS scavenger. It plays a major part in protecting cellular membranes, preventing fatty acid accumulation and in the elimination of toxic metabolites (2022).
Extended the lifespan in C. elegans (2021). Decreased the mortality in rats (1990).
Resulted in minor reductions in body weight, BMI, and fat mass compared to controls (2020).
Strong anti-inflammatory effects (HS-CRP, IL-6, TNF-α) (2020)
Interleukin 6 (IL-6) (WMD: -1.87; 95% CI: -2.80, -0.95)
Tumor necrosis factor-α (TNF-α) levels (WMD: -1.43; 95% CI: -2.03, -0.84)
C-reactive protein (CRP) (WMD: -0.10; 95% CI: -0.14, -0.06)
Impacts blood lipids favorably (2019)
TC (56 arms-MD: -8.53 mg/dl, 95% CI: -13.46, -3.6, I2: 93%)
Low-density lipoprotein-cholesterol (LDL-C) (47 arms-MD: -5.48 mg/dl, 95% CI: -8.49, -2.47, I2: 94.5)
Triglyceride (TG) (56 arms-MD: -9.44 mg/dl, 95% CI: -16.02, -2.87, I2: 91.8).
High density lipoprotein-cholesterol (HDL-C) (51 arms-MD:1.64 mg/dl, 95% CI:0.54, 2.75, I2: 92.2)
Reduced mortality by 27% and ventricular arrhythmias by 65% in secondary prevention (2013).
Seems helpful for liver disease (2020)
Multiple human studies show L-carnitine lowers ALT, AST, liver fat, and fibrosis in NAFLD and NASH. It also improves glycemic control and insulin sensitivity.
Proposed mechanisms include increased fatty acid oxidation, reduced inflammation, improved PDH flux, and glucose/insulin metabolism.
May reduce the general fatigue of cancer patients during chemotherapy.
Meta-analysis found ALCAR 1-3 g/day reduced depressive symptoms compared to placebo (2018).
A cocktail of four dietary supplements (L-carnitine, L-serine, NAC, and NR) showed a 29% improvement in cognitive function in Alzheimer's patients over a period of nearly three months, compared to a 14% improvement with placebo (2023). Generally the results in dementia were mixed (2020).
Extended the lifespan of a mouse model of ALS (2006).
Large doses may increase TMAO production which raises cardiovascular disease risk.
L-Carnitine Supplementation is Beneficial to the Liver (2020)
Role of Carnitine in Non-alcoholic Fatty Liver Disease and Other Related Diseases: An Update (2021)
Carnitine may play an important role in NAFLD based on the "multiple hit" hypothesis. The three main factors carnitine can improve are:
Inhibition of β-oxidation: Carnitine supplements may promote mitochondrial β-oxidation of fatty acids, thereby reducing liver fat accumulation.
Mitochondrial dysfunction: Carnitine can improve mitochondrial dysfunction by reducing ROS production and preventing mitochondrial membrane damage.
Insulin resistance: Carnitine enhances oxidation of long-chain acyl-CoAs which impairs insulin signaling. It also regulates the acetyl-CoA/CoA ratio and activates the IGF-1 signaling cascade to reduce insulin resistance.
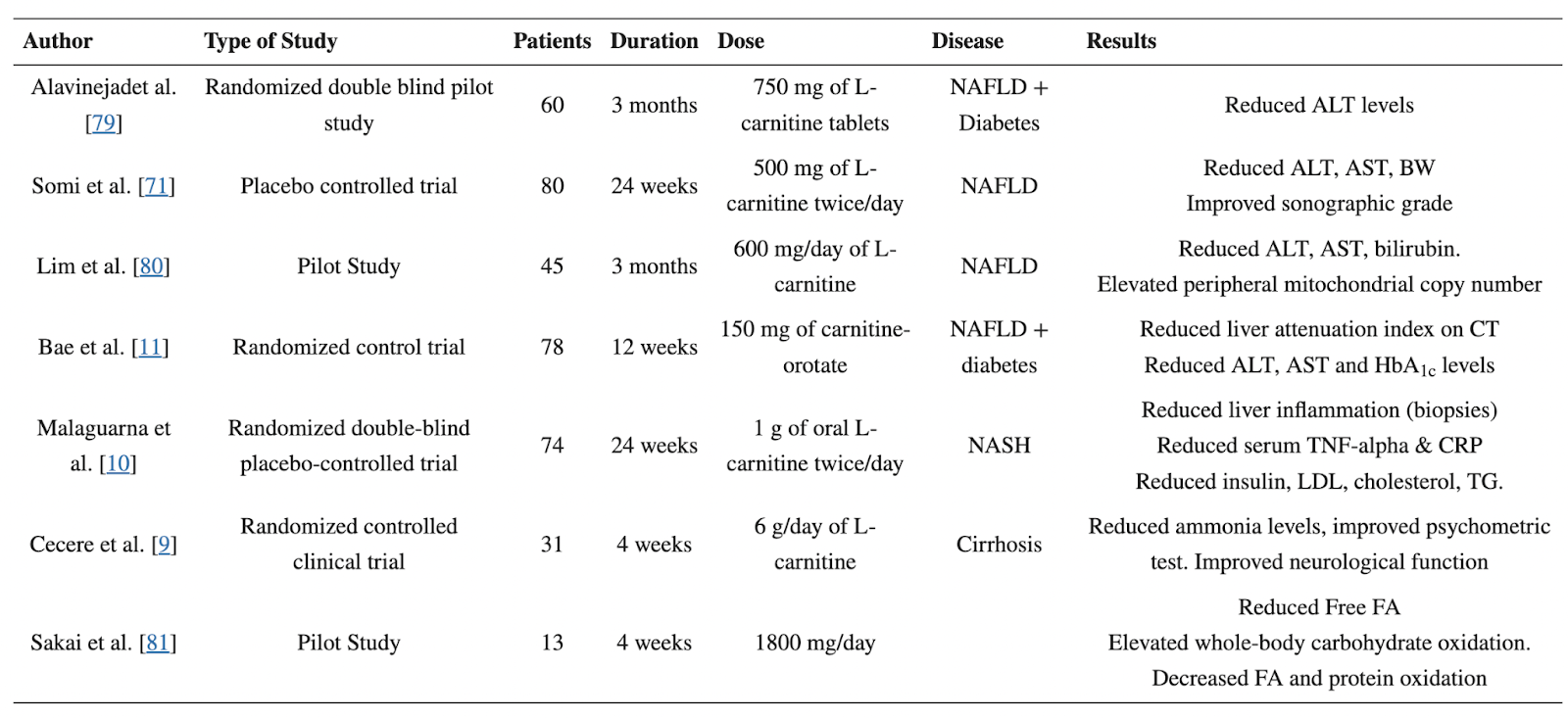
L-carnitine supplements may help treat and reduce progression of NAFLD-related diseases like non-alcoholic steatohepatitis (NASH), cirrhosis, and hepatitis based on improvements in oxidative stress, inflammation, and liver function.
Human trials show L-carnitine supplementation (doses around 1000-2000 mg/day) can reduce liver enzymes like ALT and AST, improve blood lipids, glucose control, and ultrasound-based NAFLD grade.
Animal studies also demonstrate that L-carnitine reduces hepatic lipid accumulation, oxidative stress, and fibrosis progression in NAFLD models. Proposed mechanisms involve modulation of NF-kB, PPARγ, and mitochondrial beta-oxidation enzymes.
Adverse effects of L-carnitine supplements are minimal, but high doses can cause diarrhea or fishy odor. Monitoring plasma levels can help determine optimal dosing.
Carnitine is an amino acid-derived substance that has several biological functions:
Transport of long-chain fatty acids (LCFAs) into the mitochondrial matrix for β-oxidation. This occurs through the "carnitine shuttle" which requires carnitine palmitoyltransferase I (CPT I), carnitine acylcarnitine translocase (CACT), and carnitine palmitoyltransferase II (CPT II).
Regulation of the acetyl-CoA/CoA ratio by buffering excess mitochondrial acetyl-CoA and forming acetyl-carnitine.
Facilitating transfer of acetyl-CoA from peroxisomes to mitochondria for complete oxidation.
Reduction of oxidative stress through free radical scavenging, inhibiting reactive oxygen species (ROS) production, and upregulating antioxidant enzymes.
The Importance of the Fatty Acid Transporter L-Carnitine in Non-Alcoholic Fatty Liver Disease (NAFLD) (2020)
Overview of L-Carnitine
L-carnitine is an amino acid derivative that transports fatty acids into mitochondria for oxidation. It also buffers excess acetyl-CoA out of mitochondria.
It is obtained from the diet (mainly meat) and synthesized endogenously. Levels are highest in muscle.
Absorption is 54-86% from food but only 5-25% from supplements.
It requires active transport into cells by the organic cation/carnitine transporter OCTN2.
Inside cells, it binds to fatty acids via carnitine palmitoyltransferase 1 (CPT1) to form acyl-carnitines that can enter mitochondria.
It is essential for fatty acid oxidation and ketogenesis. It also regulates the acetyl-CoA/CoA ratio and pyruvate dehydrogenase (PDH) flux.
L-Carnitine Deficiency and Liver Disease
Primary carnitine deficiency (PCD), due to defects in OCTN2, can present with fatty liver disease. L-carnitine treatment improves outcomes.
Inhibiting CPT1 with etomoxir also causes fatty liver in mice.
Patients with chronic liver disease and cirrhosis have reduced L-carnitine levels.
Shorter acyl-carnitine chains are elevated in liver disease compared to controls.
Long-chain acyl-carnitines are reduced in worsening NAFLD severity.
L-Carnitine Supplementation for NAFLD
Multiple human studies show L-carnitine lowers ALT, AST, liver fat, and fibrosis in NAFLD and NASH.
It also improves glycemic control and insulin sensitivity.
Proposed mechanisms include increased fatty acid oxidation, reduced inflammation, improved PDH flux, and glucose/insulin metabolism.
However, large doses may increase TMAO production which raises cardiovascular disease risk.
Animal studies show it stimulates ketogenesis when fatty acids are available.
Effects on insulin levels are inconsistent between studies. May improve insulin resistance by increasing glucose disposal.
Conclusions
L-carnitine is critical for fat metabolism and acetyl-CoA buffering relevant to NAFLD.
Liver disease inhibits L-carnitine synthesis, further impairing fat oxidation.
Multiple small studies show oral supplementation benefits NAFLD parameters.
Acylcarnitine profiling may have biomarker potential for diagnosing and monitoring NAFLD severity.
Larger comprehensive human studies are still needed on L-carnitine supplementation for NAFLD.
Evaluation of L-carnitine efficacy in the treatment of non-alcoholic fatty liver disease among diabetic patients: A randomized double blind pilot study. J. Gastroenterol. Hepatol. Res. (2016)
AIM: Non-alcoholic fatty liver disease (NAFLD) is one of the most common liver diseases worldwide and while its pathophysiology is still unverified, most of the present theories are based on Insulin resistance and oxidative stress as key factors. According to role of L-Carnitine in the process of fatty acid oxidation and glucose metabolism, it seems that this drug could be potentially effective in the treatment of diabetic patients suffering from NAFLD. This study has been designed to evaluate this potential therapeutic effect.
METHOD: 60 type 2 diabetic patients with NAFLD based on sonographic findings and elevated serum transaminases randomly divided into 2 groups. The intervention group (A) treated with L-Carnitine 750mg TDS while the control group (B) received placebo. After 3 months intervention the level of liver transaminases and sonographic degree of fatty liver compared between 2 groups.
RESULT: After three months of intervention, in group A the level of AST decreased from 122.7 ± 13.6 to 96.3 ± 7 while in group B raised from 125 ± 14 to 126 ± 11 (p < 0.001). The level of ALT in group A declined from 124.5 ± 11.3 to 82.1 ± 5.2 and in placebo group decreased from 120 ± 10.8 to 115.1 ± 6.3 (p < 0.001) In comparison of average level of AST and ALT between 2 groups, we found a meaningful decline in the serum level of liver transaminases in group A (p < 0.001) while there were no significant reduction in serum level of Cholesterol, TG and FBS (p > 0.05) and also the sonographic degree of fatty liver didn't change among 2 groups.
CONCLUSION: It seems that L-Carnitine is effective in treatment of NAFLD among diabetic patients and could be a potential therapeutic approach in such patients. We recommend these findings to further be verified in future studies
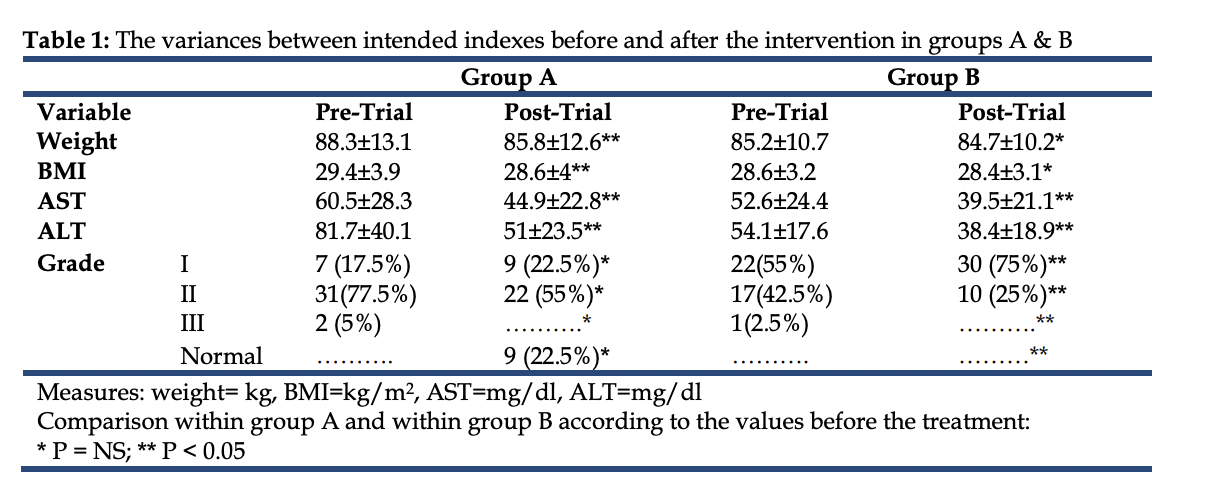
Data from a randomized and controlled trial of LCarnitine prescription for the treatment for Non-Alcoholic Fatty Liver Disease. Bioinformation. (2014)
Non-alcoholic fatty liver disease (NAFLD) consists of a range of complication. The disease describes clinical , para clinical and pathological conditions from simple steatosis in non-alcoholic steato hepatitis (NASH) to fibrosis, cirrhosis and hepato cellular carcinoma. Therefore, it is of interest to evaluate the grade of fatty liver and Liver Function Test in NAFLD patients. We collected samples and data from 80 patients referred to gastrointestinal clinic of Emam Reza hospital with sonography diagnosed NAFLD and were evaluated in two groups in a randomized clinical trial. The effects of L-Carnitine (500 mg) prescription twice a day on liver enzymes and echogenicity changes in case group was documented and compared with the control group. The mean age of the patients was 40.7±8 in the age range of 25 to 62 years old with 66 (82.5%) male and 14 (17.5%) female patients. Data show that fatty liver changes were not significantly different in the two groups (P=0.23). It is observed that the ALT was the only enzyme with significant changes (P=0.01) after a 24-week interval. It is also noted that the difference in fatty liver sonographic grading was also significant in the two groups (P=0.0001). Thus, proper therapeutic protocols can be adopted beside diet and weight loss to control the disease trend in consideration to the significant changes observed both in enzymatic levels and sonographic grading between the two groups of patients with NAFLD.
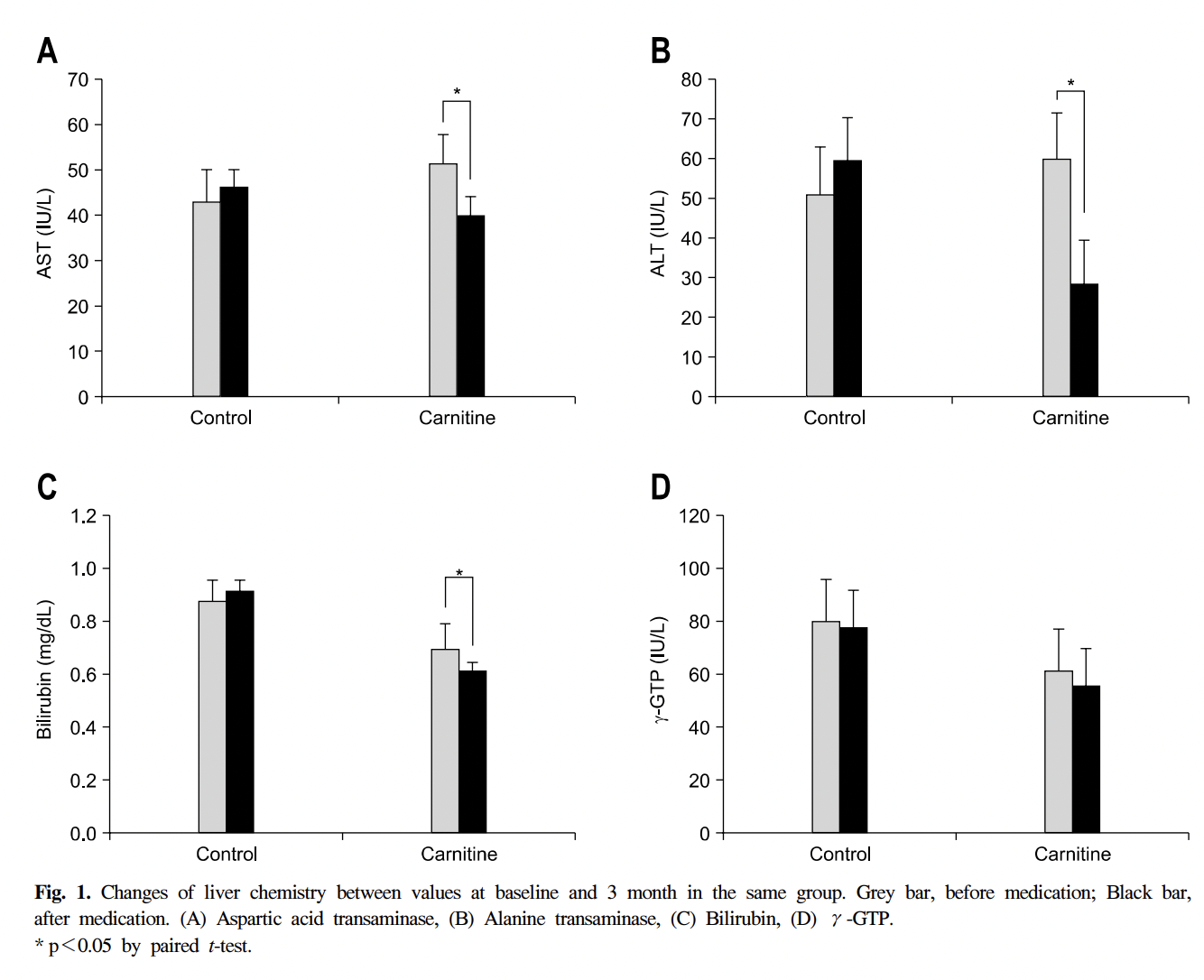
Effects of carnitine on peripheral blood mitochondrial DNA copy number and liver function in non-alcoholic fatty liver disease. Korean J. Gastroenterol. (2010)
In NAFLD, the carnitine improved liver profile and peripheral blood mitochondrial DNA copy number. This results suggest that carnitine activate the mitochondria, thereby contributing to the improvement of NAFLD.
Improvement of nonalcoholic fatty liver disease with carnitine-orotate complex in type 2 diabetes (CORONA): A randomized controlled trial. Diabetes Care. (2015)
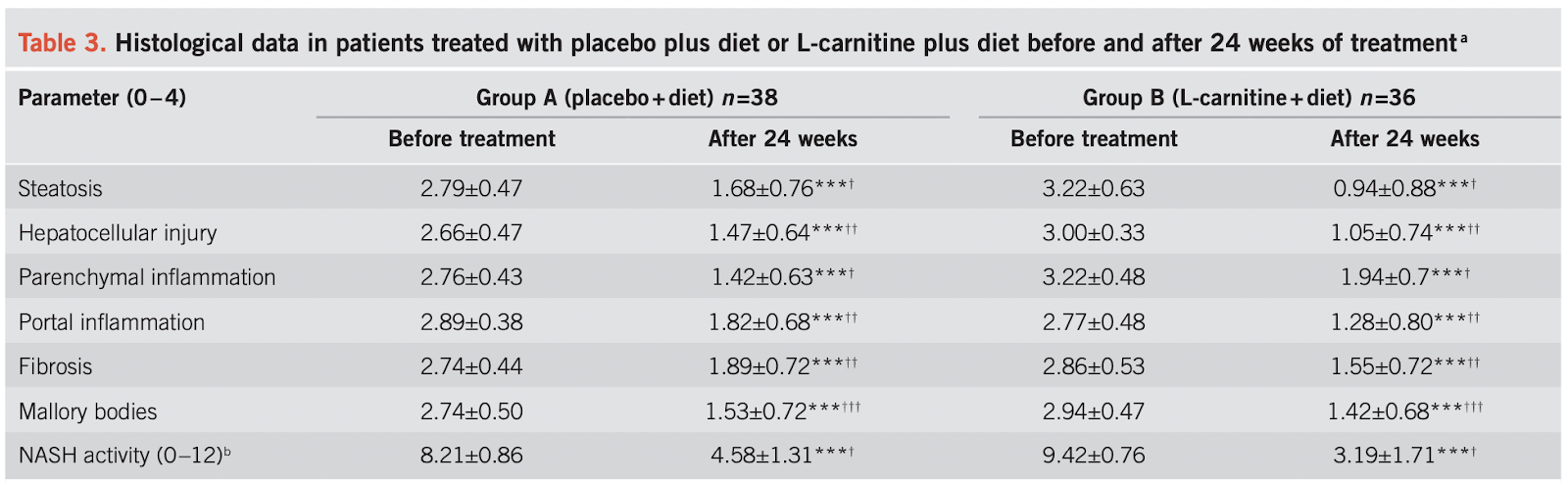
L-Carnitine supplementation to diet: A new tool in treatment of nonalcoholic steatohepatitis—A randomized and controlled clinical trial. Am. J. Gastroenterol. (2010) (Italian study)
OBJECTIVES:
Nonalcoholic steatohepatitis (NASH) is a known metabolic disorder of the liver. No treatment has been conclusively shown to improve NASH or prevent disease progression. The function of L-carnitine to modulate lipid profile, glucose metabolism, oxidative stress, and inflammatory responses has been shown. The aim of this study was to evaluate the effects of L-carnitine's supplementation on regression of NASH.
METHODS:
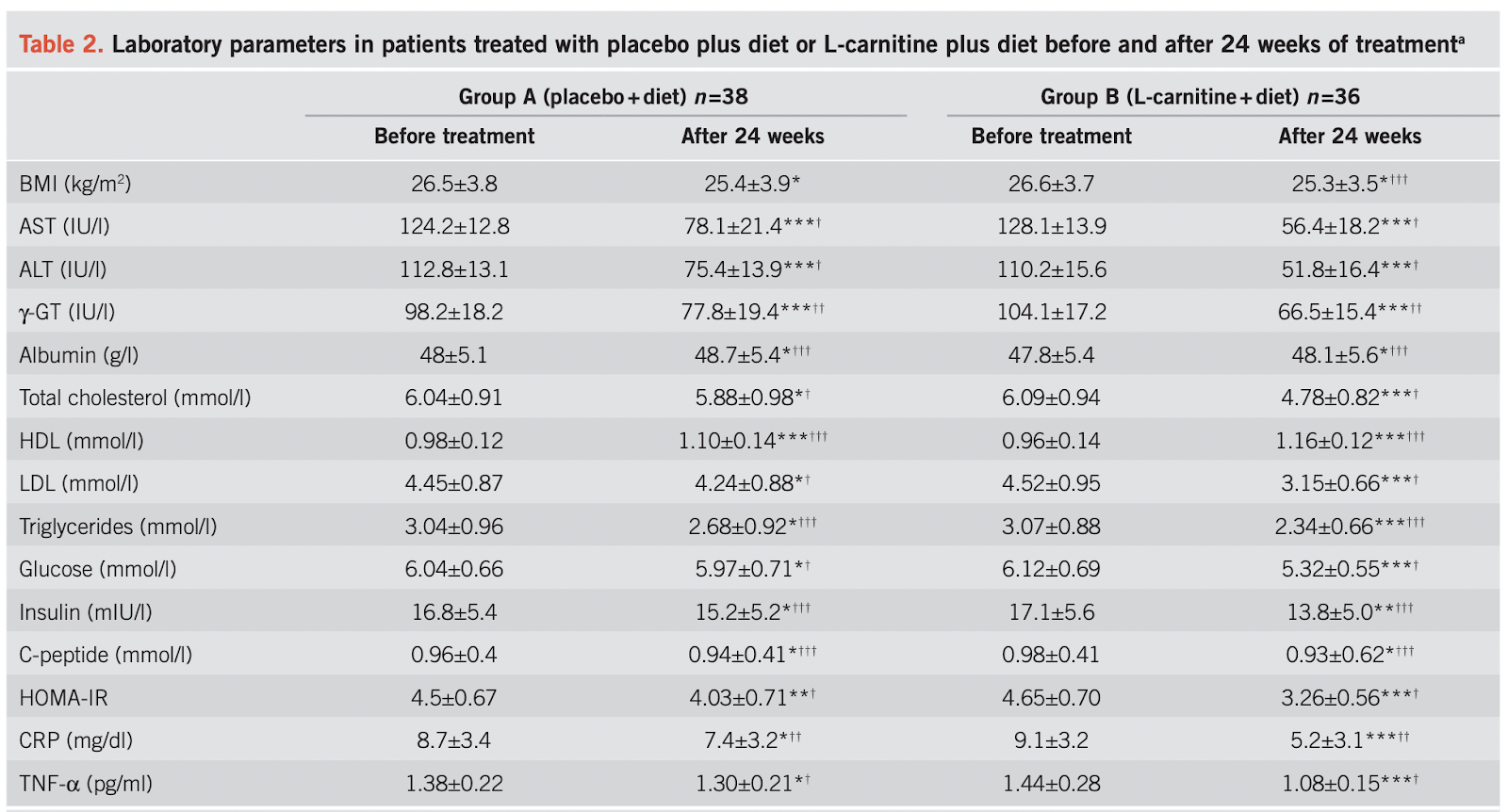
In patients with NASH and control subjects, we randomly dispensed one 1-g L-carnitine tablet after breakfast plus diet and one 1 g tablet after dinner plus diet for 24 weeks or diet alone at the same dosage and regimen. We evaluated liver enzymes, lipid profile, fasting plasma glucose, C-reactive protein (CRP), tumor necrosis factor (TNF)-α, homeostasis model assessment (HOMA)-IR, body mass index, and histological scores.
RESULTS:
At the end of the study, L-carnitine-treated patients showed significant improvements in the following parameters: aspartate aminotransferase (P=0.000), alanine aminotransferase (ALT) (P=0.000), γ-glutamyl-transpeptidase (γ-GT) (P=0.000), total cholesterol (P=0.000), low-density lipoprotein (LDL) (P=0.000), high-density lipoprotein (HDL) (P=0.000), triglycerides (P=0.000), glucose (P=0.000), HOMA-IR (P=0.000), CRP (P=0.000), TNF-α (P=0.000), and histological scores (P=0.000).
CONCLUSIONS:
L-carnitine supplementation to diet is useful for reducing TNF-α and CRP, and for improving liver function, glucose plasma level, lipid profile, HOMA-IR, and histological manifestations of NASH.
Efficacy of L-Carnitine in reducing hyperammonaemia and improving neuropsychological test performance in patients with hepatic cirrhosis results of a randomised Trial. Clin. Drug Investig. (2002)
Effect of L-carnitine in patients with liver cirrhosis on energy metabolism using indirect calorimetry: A pilot study. J. Clin. Med. Res. (2016)
L-Carnitine supplementation reduces the general fatigue of cancer patients during chemotherapy (2018)
L-Carnitine (LC) plays an important role in the metabolism of fatty acids, and LC deficiency is associated with a feeling of weakness or general fatigue. Cancer patients receiving chemotherapy often develop LC deficiency, which is considered to be a factor contributing to general fatigue. The aim of the present study was to evaluate the efficacy of LC supplementation as a treatment for general fatigue in cancer patients during chemotherapy. A total of 11 cancer patients who were suffering from general fatigue during chemotherapy in our hospital between September 2014 and December 2015 were examined (6 cases involved adjuvant chemotherapy and 5 cases involved chemotherapy for unresectable or recurrent disease). The patients were administered 1,500 mg/day of levocarnitine per os, and the change in mean daily fatigue from the baseline to 8 weeks was assessed using the Brief Fatigue Inventory. The change in the plasma levels of albumin and the lymphocyte counts from the baseline to 8 weeks were also assessed. LC supplementation reduced general fatigue in all cases. Moreover, LC supplementation maintained the plasma levels of albumin and lymphocyte counts during chemotherapy, and enabled patients to continue chemotherapy sequentially without dose reduction. Therefore, LC supplementation improved general fatigue in all the examined cancer patients during chemotherapy. This treatment may make improve the tolerability of chemotherapy in cancer patients by reducing general fatigue and improving the nutritional status.
Role of carnitine in cancer chemotherapy-induced multiple organ toxicity (2010)
In the last few years, cancer chemotherapy has been successfully employed in the treatment of different types of human tumours. Unfortunately, the optimal clinical usefulness of this important treatment modality is usually limited secondary to the development of life-threatening multiple organ toxicity. Cancer chemotherapy may cause these toxic effects by mechanisms not involved in their anticancer activity that can severely affect the life of patients and represent a direct cause of death. Several experimental and clinical studies have demonstrated that some important anticancer drugs interfere with the absorption, synthesis, and excretion of carnitine in non-tumour tissues, resulting in a secondary carnitine deficiency which is reversed by carnitine treatment without affecting anticancer therapeutic efficacy. Prototypes of anticancer drugs that alter carnitine system are doxorubicin, cisplatin, carboplatin, oxaliplatin, cyclophosphamide and ifosfamide. Furthermore, cachectic cancer patients are especially at risk for carnitine deficiency due to decreased oral intake and/or increased renal losses. Altered serum and urine carnitine levels have been reported in cancer patients with various forms of malignant diseases. Recent studies in our laboratory have demonstrated that carnitine deficiency constitute a risk factor and should be viewed as a mechanism during development of oxazaphosphorines-induced cardiotoxicity in rats. Similarly, inhibition of gene expression of heart fatty acid-binding protein and organic cation/carnitine transporter in doxorubicin cardiomyopathic rat model has been reported. In view of these facts and in view of irreplaceability of these important anticancer drugs, this review aimed to highlight the role of carnitine depletion and supplementation during development of chemotherapy-induced multiple organ toxicity.
The effects of L-carnitine supplementation on indicators of inflammation and oxidative stress: a systematic review and meta-analysis of randomized controlled trials (2020)
Objective: Several trials investigated the efficacy of L-carnitine administration on markers of inflammation and indicators of oxidative stress; however, their findings are controversial. The aim of this study was to conduct a comprehensive meta-analysis and a critical review, which would analyze all randomized controlled trials (RCTs) in order to determine the effects of L-carnitine supplementation on inflammatory markers and oxidative stress.
Methods: An electronic search was performed using Scopus, Cochrane Library, PubMed, Google scholar and Web of Science databases on publications from 1990 up to May 2020. Human RCTs conducted in healthy subjects or participants with certain disorders which investigating the efficacy of L-carnitine supplementation compared to control (placebo, usual treatment or no intervention) on inflammation and oxidative markers were included. Data were pooled applying a random-effects model and as the overall effect size, weighted mean difference (WMD) was presented. Between heterogeneity among studies was computed using Cochran's Q test and I-square (I2). Quality of studies assessed using the Jadad scale. Dose-response analysis was measured using meta-regression. The funnel plot, as well as the Egger's regression test was applied to determine the publication bias.
Results: 44 trials (reported 49 effect sizes for different outcomes of interest) met the inclusion criteria for this meta-analysis. According to the findings, L-carnitine supplementation resulted in a significant reduction in C-reactive protein (CRP) (WMD: -0.10; 95% CI: -0.14, -0.06), interleukin 6 (IL-6) (WMD: -1.87; 95% CI: -2.80, -0.95), tumor necrosis factor-α (TNF-α) levels (WMD: -1.43; 95% CI: -2.03, -0.84), and malondialdehyde (MDA) (WMD: -0.47; 95% CI: -0.76, -0.18) levels, while there was a significant increase in superoxide dismutase (SOD) (WMD: 2.14; 95% CI: 1.02, 3.25). However, no significant effects of L-carnitine on glutathione peroxidase (GPx) (WMD: 0.02; 95% CI: -0.01, 0.05) and total antioxidant capacity (TAC) (WMD: 0.14; 95% CI: -0.05, 0.33) were found.
Conclusions: L-carnitine supplementation was associated with lowering of CRP, IL-6, TNF-α, and MDA, and increasing SOD levels, but did not affect other inflammatory and oxidative stress biomarkers.
Efficacy of l-carnitine supplementation for management of blood lipids: A systematic review and dose-response meta-analysis of randomized controlled trials (2019)
Background and aim: l-carnitine has an important role in fatty acid metabolism and could therefore act as an adjuvant agent in the improvement of dyslipidemia. The purpose of present systematic review and meta-analysis was to critically assess the efficacy of l-carnitine supplementation on lipid profiles.
Methods and results: We performed a systematic search of all available randomized controlled trials (RCTs) in the following databases: Scopus, PubMed, ISI Web of Science, The Cochrane Library. Mean difference (MD) of any effect was calculated using a random-effects model. In total, there were 55 eligible RCTs included with 58 arms, and meta-analysis revealed that l-carnitine supplementation significantly reduced total cholesterol (TC) (56 arms-MD: -8.53 mg/dl, 95% CI: -13.46, -3.6, I2: 93%), low-density lipoprotein-cholesterol (LDL-C) (47 arms-MD: -5.48 mg/dl, 95% CI: -8.49, -2.47, I2: 94.5) and triglyceride (TG) (56 arms-MD: -9.44 mg/dl, 95% CI: -16.02, -2.87, I2: 91.8). It also increased high density lipoprotein-cholesterol (HDL-C) (51 arms-MD:1.64 mg/dl, 95% CI:0.54, 2.75, I2: 92.2). l-carnitine supplementation reduced TC in non-linear fashion based on dosage (r = 21.11). Meta-regression analysis indicated a linear relationship between dose of l-carnitine and absolute change in TC (p = 0.029) and LDL-C (p = 0.013). Subgroup analyses showed that l-carnitine supplementation did not change TC, LDL-C and TG in patients under hemodialysis treatment. Intravenous l-carnitine and lower doses (>2 g/day) had no effect on TC, LDL-C and triglycerides.
Conclusion: l-carnitine supplementation at doses above 2 g/d has favorable effects on patients' lipid profiles, but is modulated on participant health and route of administration.
L-Carnitine Supplement Review | Amazing Energy Benefits?

Carnitine promotes recovery from oxidative stress and extends lifespan in C. elegans, (2021)
Carnitine is required for transporting fatty acids into the mitochondria for β-oxidation. Carnitine has been used as an energy supplement but the roles in improving health and delaying aging remain unclear. Here we show in C. elegans that L-carnitine improves recovery from oxidative stress and extends lifespan. L-carnitine promotes recovery from oxidative stress induced by paraquat or juglone and improves mobility and survival in response to H2O2 and human amyloid (Aβ) toxicity. L-carnitine also alleviates the oxidative stress during aging, resulting in moderate but significant lifespan extension, which was dependent on SKN-1 and DAF-16. Long-lived worms with germline loss (glp-1) or reduced insulin receptor activity (daf-2) recover from aging-associated oxidative stress faster than wild-type controls and their long lifespans were not further increased by L-carnitine. A new gene, T08B1.1, aligned to a known carnitine transporter OCTN1 in humans, is required for L-carnitine uptake in C. elegans. T08B1.1 expression is elevated in daf-2 and glp-1 mutants and its knockdown prevents L-carnitine from improving oxidative stress recovery and prolonging lifespan. Together, our study suggests an important role of L-carnitine in oxidative stress recovery that might be important for healthy aging in humans.
Acetyl-l-carnitine 1: Effects on mortality, pathology and sensory-motor performance in aging rats (1990)
Three different test sites assessed the effects of acetyl-l-carnitine (AC) on age-related changes in general health, sensory-motor skills, learning, and memory. Two groups of rats began the experiments at 16 months of age. One group (OLD-AC) was given AC, 75 mg/kg/day, beginning at 16 months. The other group (OLD-CON) was treated identically except it was not given the drug. Beginning at 22 months of age, these rats and a group of young (3–4 months old) rats (YG-CON) were given a series of sensory-motor tasks. AC decreased mortality, and had no reliable effect on body weight, fluid intake, or the general health of the rats. These data indicate that a chronic dose of AC does not interfere with food and water intake, and may increase longevity. An age-related decline of performance occurred in most of the sensory-motor tasks; locomotor activity was reduced in a novel environment and in a runwheel, and the ability to prevent falling was reduced in tests on a taut wire, rotorod, inclined screen, and several types of elevated bridges. An age-related decline of performance did not occur in grooming, or in the latency to initiate several different behaviors. AC had no effect on performance in any sensory-motor task. These data indicate that the improvements produced by AC in some tests of spatial memory may be due to the effects of AC on cognitive abilities rather than on sensory-motor skills.
l-Carnitine suppresses the onset of neuromuscular degeneration and increases the life span of mice with familial amyotrophic lateral sclerosis (ALS) (2006)
Oral administration of l-carnitine prior to disease onset significantly delayed the onset of signs of disease (log-rank P = 0.0008), delayed deterioration of motor activity, and extended life span (log-rank P = 0.0001) in transgenic ALS mice carrying a human SOD1 gene with a G93A mutation (Tg).
L-Carnitine Summary (link)
- L-carnitine is synthesized in the body from lysine and methionine. Rate of synthesis is 0.16-0.48 mg/kg body weight/day (Rebouche, 2006).
- Key functions: transports long-chain fatty acids into mitochondria via the "carnitine shuttle" involving CPT I, CACT, and CPT II (Rebouche, 2006); regulates acetyl-CoA/CoA ratio by forming acetylcarnitine (Rebouche, 2006); facilitates transfer of acetyl-CoA from peroxisomes to mitochondria (Rebouche, 2006); reduces oxidative stress through antioxidant properties (Solarska et al., 2010).
- Absorption: 54-86% absorbed from foods, 5-25% from 0.6-7 g supplemental doses (Rebouche, 2004).
- Primary systemic carnitine deficiency is an autosomal recessive disorder caused by mutations in SLC22A5 encoding carnitine transporter OCTN2 (Frigeni et al., 2017). Requires L-carnitine supplementation.
- Secondary deficiencies can result from renal disorders, valproic acid use, pivalate antibiotics, and genetic defects in fatty acid oxidation (Stanley, 2004).
Disease treatment:
1) Type 2 diabetes - Meta-analyses suggest L-carnitine may improve insulin resistance but impact on glucose control is mixed (Xu et al., 2017; Vidal-Casariego et al., 2013; Asadi et al., 2019).
2) Myocardial infarction - Meta-analysis found L-carnitine therapy reduced mortality by 27% and ventricular arrhythmias by 65% (DiNicolantonio et al., 2013).
3) Heart failure - Meta-analysis found L-carnitine improved exercise tolerance and cardiac function but not mortality (Song et al., 2017).
4) Intermittent claudication - Systematic reviews found modest benefit of propionyl-L-carnitine on walking performance (Brass et al., 2013; Delaney et al., 2013).
5) Depression - Meta-analysis found ALCAR 1-3 g/day reduced depressive symptoms compared to placebo (Veronese et al., 2018).
6) Alzheimer's disease - Older meta-analyses suggest some cognitive benefit with ALCAR but results were mixed (Montgomery et al., 2003; Hudson et al., 2003) (2020).
7) Hepatic encephalopathy - Meta-analysis found ALCAR reduced blood ammonia levels in patients with cirrhosis and encephalopathy compared to placebo (Malaguarnera et al., 2019).
8) Male infertility - Few small studies suggest 2 g/day L-carnitine may improve sperm parameters but larger trials needed (Lenzi et al., 2003; Lenzi et al., 2004).
- No proven benefit found for cancer fatigue, diabetes neuropathy, or physical performance based on systematic reviews (2017).
- Food sources: highest in meat and dairy. Intakes 23-135 mg/day in omnivores, ~1 mg/day in vegetarians (Lombard et al., 1989).
- Supplement doses: 0.5-2 g/day L-carnitine or ALCAR common. Intravenous form used for deficiency treatment.
In summary, key roles of L-carnitine are transporting fatty acids and regulating acetyl-CoA. Potential benefits seen for some conditions like MI, depression, and male infertility but larger, rigorous trials still needed. Rich food sources are meat and dairy but supplemental forms have low bioavailability.
L-Carnitine (Examine)
L-Carnitine is a naturally occurring amino acid found in animal products like meat and dairy. It can also be synthesized in the body from the amino acids lysine and methionine (Rebouche, 1982).
Origin and Composition
L-carnitine has the chemical structure C7H15NO3. The related compounds Acetyl-L-carnitine (ALCAR) and Propionyl-L-carnitine differ slightly in their chemical structures (Evans & Fornasini, 2003).
In the body, carnitine exists in free form as L-carnitine or as acetylated ALCAR. It is synthesized endogenously from lysine and methionine, a process that requires vitamin C (Rebouche et al, 1991).
Newborns and infants have lower carnitine synthesis, so rely more on mother's milk for intake (Suskind et al, 2009). Infant formulas often add carnitine.
Vegetarians/vegans have lower intake from diet and lower stores, but higher bioavailability from supplements (Lombard et al, 1989).
Sources and Requirements
Omnivore intake averages 2-12 umol/kg/day. Vegetarians much lower at <1 umol/kg/day (Flanagan et al, 2010).
No RDA established since not an essential nutrient. Recommended intake is 100-400mg/kg for deficiencies. Doses up to 3000mg appear safe (Cruciani et al, 2006).
Absorption and Metabolism
Absorbed in small intestine via organic cation transporter OCTN2. Bioavailability 14-18% from supplements, higher (54-87%) from food (Sahajwalla et al, 1995).
ALCAR bioavailability similar to L-carnitine (Evans & Fornasini, 2003).
Half-life around 60 minutes. Excreted as metabolites primarily in urine (Rebouche & Seim, 1998).
Tissue Distribution
Highest concentrations in skeletal muscle (126.4 mmol/L), lesser amounts in liver, serum and extracellular fluid (Evans & Fornasini, 2003).
ALCAR crosses blood brain barrier via OCTN2 and B(0,+) transporters (Nałecz et al, 2004).
Mechanisms
Increases beta-oxidation and transport of long-chain fatty acids into mitochondria for fat burning (Bartlett & Eaton, 2004).
Involved in converting fat into energy. Works with CPT1, CPT2, and CAT enzymes (Jogl et al, 2004).
May increase mitochondrial biogenesis (Iossa et al, 2002).
Cognitive Effects
ALCAR increased acetylcholine in vitro (Dolezal & Tucek, 1981).
500 mg/kg ALCAR increased serotonin 20%, noradrenaline 25%, glucose 43-55% in mice brain regions (Smeland et al, 2012).
ALCAR improved learning in old rodents (Ando et al, 2001) and reduced cognitive decline in humans with Alzheimer's or dementia at 1-3 g/day (Malaguarnera et al, 2012).
Exercise Performance
15 g L-carnitine increased endurance in humans (Colombani et al, 1996). Smaller doses (2-3 g) ineffective (Broad et al, 2008).
1.5-2 g/day reduced muscle damage and soreness markers (Kraemer et al, 2006).
2 g/day increased androgen receptors in muscle over 3 weeks (Kraemer et al, 2006). Did not increase testosterone.
Fat Loss
Does not appear to increase fat loss in normal-weight rodents or humans (Villani et al, 2000).
May increase fat loss in deficiency states like vegetarianism (Rebouche, 1992).
Cardiovascular
3 g propionyl-L-carnitine (PLC) increased nitric oxide and blood flow in clinical studies (Bloomer et al, 2007). Reduced intermittent claudication symptoms (Brevetti et al, 1992).
2 g/day ALCAR + ALA reduced blood pressure ~10 mmHg in poor metabolizers (Ruggenenti et al, 2009).
Meta-analysis found 2 g/day reduced mortality 27% in post-MI patients (DiNicolantonio et al, 2013).
Safety
Well tolerated up to 3 g/day. Main side effect is unpleasant body odor in some people (Rubin et al, 2001).
No toxicity seen at standard supplemental doses (Rubin et al, 2001).
In summary, L-carnitine is an amino acid synthesized in the body that is also obtained from the diet. It is involved in transporting fatty acids for energy production and has roles in exercise, cognition, cardiovascular function and more. Supplement doses of 1-3 g/day appear effective for many benefits with a good safety profile. Deficiencies may occur in vegetarians/vegans, newborns and the elderly.
L-Carnitine: Benefits, Side Effects, Sources, and Dosage (healthline)
Overview of L-Carnitine
L-carnitine is an amino acid derivative that transports fatty acids into cells to be processed for energy production.
It is made in the body and also found in foods like meat and dairy. It is conditionally essential, meaning requirements may exceed production in some people.
There are several forms of carnitine supplements, including acetyl-L-carnitine (ALCAR) and L-carnitine-L-tartrate. Acetyl-L-carnitine is likely the most effective form for the brain.
L-carnitine is stored mostly in muscles and plays a key role in mitochondrial function and energy metabolism. It may support disease treatment and healthy aging.
Weight Loss Effects
A review of 37 studies found L-carnitine significantly reduced body weight, BMI, and fat mass compared to control. However, it did not affect belly fat or body fat percentage. (2020)
Another analysis of 9 studies found people taking L-carnitine lost an average of 2.9 lbs (1.3 kg) more weight than control.
A meta-analysis of 6 studies found L-carnitine reduced body weight, BMI, and belly fat in those with polycystic ovary syndrome.
More research is still needed on long-term weight loss effects. L-carnitine may complement but not replace diet and exercise.
Brain Health Benefits
Acetyl-L-carnitine may help prevent age-related mental decline and improve learning markers.
A study found 1500 mg of ALCAR per day for 28 weeks improved brain function in those with dementia.
However, other studies found no benefits on reaction time or memory in young healthy adults. More research is still needed.
Other Potential Benefits
May improve heart health markers like blood pressure, cholesterol, and symptoms of heart failure.
Could enhance exercise recovery, muscle oxygen supply, endurance, and reduce soreness, but with mixed evidence.
A review of 41 studies found it lowered blood sugar and A1c levels in those with diabetes, obesity, or overweight.
May be as effective as antidepressants for depression with fewer side effects, but more research is needed.
Safety and Side Effects
Doses of 2 grams or less per day are generally safe long-term, but can cause mild digestive upset.
However, L-carnitine may increase TMAO levels, which are linked to increased heart disease risk.
Food sources like meat and dairy are more bioavailable than supplements. Healthy adults can synthesize sufficient levels.
Recommended Dosage
Doses used in studies range from 500-4000 mg per day, divided into multiple doses.
Those with low intake like vegetarians/vegans, kidney disease, or the elderly may benefit from 500-2000 mg daily.
Acetyl-L-carnitine doses for brain health range from 500-3000 mg per day.
L-carnitine L-tartrate doses for exercise range from 1000-4000 mg per day.
In conclusion, L-carnitine is a generally safe supplement that may support weight loss, brain function, exercise performance, heart health, and disease treatment. However, food sources are sufficient for most healthy individuals. More research is still needed on its long-term efficacy and safety.



Comments