MPN & Longevity Research
What is Polycythemia Vera (PV)? 2
What are the most promising treatments for PV / MPN today? 3
Current and emerging therapies 14
Phenotypes and blood markers for management of PV and MPNs 20
Molecular pathogenesis of the myeloproliferative neoplasms (2021) 22
Inflammation and Oxidation in MPNs 24
MPN ⇔ Endothelial Cell Connection 41
Mediterranean diet for MPNs 46
Interferon-alpha for MPNs (Pegasys / Besremi) 58
Treatments in the Clinical Pipeline for PV & MPNs 126
Idasanutlin (MDM2 Inhibitor) 143
Off-label Drugs and Supplements for PV & MPNs 145
Leukotriene Inhibitors (Singulair / Zileuton) 151
Dipyridamole + Simvastatin + Alendronate 177
Apigenin (Celery / Parsley) 189
H1-Antihistamines / Loratadine (Claritin) / Desloratadine 213
Other JAK2/STAT3 Inhibitors 246
How to eliminate senescent blood cancer cells? 259
Rhodiola inhibits JAK2/STAT3 260
Pulmonary Hypertension (common in MPNs) 260
Epstein-Barr (EBV) present in Bone Marrow 265
Niacin May Lower Blood Counts 268
Does Aspartame cause blood cancer? 270
Comprehensive Blood Testing for MPNs 270
Antioxidant and Nutrient Testing 272
Herpes Virus / HSV / CMV Cancer 283
Basics of PV & MPN
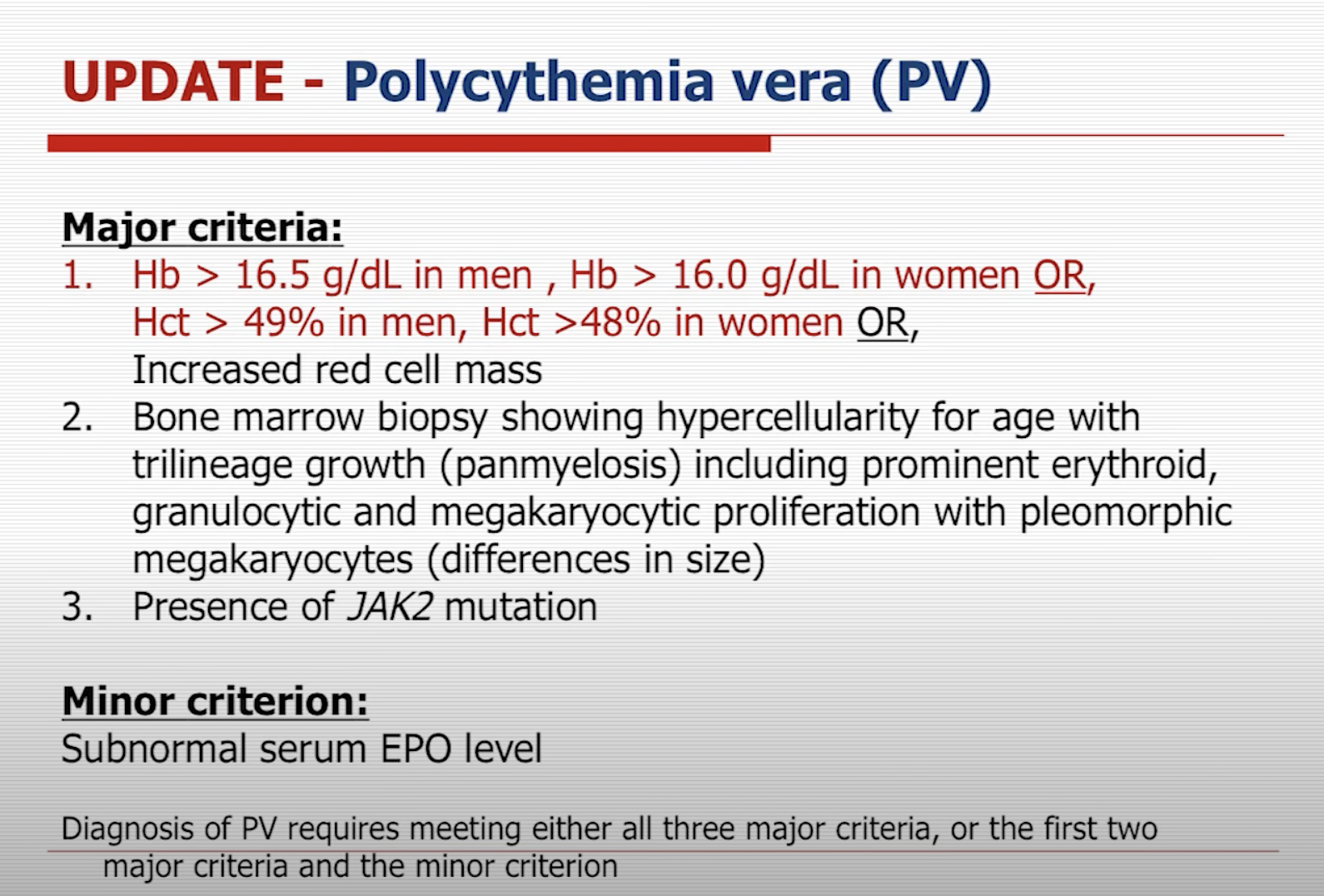
What is Polycythemia Vera (PV)?
Polycythemia Vera (PV) is a rare and chronic blood cancer marked by an excessive production of red blood cells within the bone marrow. As a myeloproliferative neoplasm (MPN), PV involves the abnormal proliferation of blood-forming cells in the bone marrow. The heightened number of red blood cells thickens the blood, reducing blood flow and elevating the risk of blood clots. This can lead to severe health complications, such as strokes, heart attacks, or deep vein thrombosis (DVT).
In over 95% of cases, the root cause of PV is a mutation in the JAK2 gene of blood stem cells, a gene instrumental in controlling blood cell production. This mutation triggers the continuous activation of the JAK2 protein, resulting in the overproduction of red blood cells, white blood cells, and platelets.
Over time, PV may evolve into a more aggressive blood cancer known as myelofibrosis (MF), characterized by the replacement of bone marrow with fibrous scar tissue. This condition can give rise to severe anemia, a weakened immune response, and heightened bleeding risks. Additionally, a small percentage of individuals with PV may eventually develop acute leukemia.
What are the most promising treatments for PV / MPN today?
COMBINE PHLEBOTOMY AND ASPIRIN
In Polycythemia Vera (PV), an increased red blood cell mass raises the risk of thrombosis and cardiovascular death. Reducing the risk of blood clots (thrombosis) can be achieved by taking aspirin and maintaining hematocrit levels within the range recommended by your physician (<45 or <42).
Phlebotomy: The study, conducted by Marchioli et al., examined the effects of different treatment intensities in patients with JAK2-positive polycythemia vera. A total of 365 adults were randomly assigned to receive either more intensive treatment (target hematocrit <45%) or less intensive treatment (target hematocrit 45-50%). The study concluded that patients with a hematocrit target of less than 45% had significantly lower rates of cardiovascular death and major thrombosis than those with a hematocrit target of 45-50%.
Aspirin: A double-blind, placebo-controlled, randomized trial involving 518 patients with polycythemia vera assessed the safety and efficacy of low-dose aspirin (100 mg daily) for preventing thrombotic complications. The study found that aspirin reduced the risk of the combined end point of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes (relative risk, 0.41; 95 percent confidence interval, 0.15 to 1.15; P=0.09) and the risk of the combined end point of nonfatal myocardial infarction, nonfatal stroke, pulmonary embolism, major venous thrombosis, or death from cardiovascular causes (relative risk, 0.40; 95 percent confidence interval, 0.18 to 0.91; P=0.03). However, overall mortality and cardiovascular mortality were not significantly reduced.
Evidence from other cancers: Aspirin has shown promise in generally improving cancer outcomes and reducing metastatic spread, particularly for localized or regional tumors. Studies have found that post-diagnosis aspirin use is associated with improved survival in various cancers, particularly before any metastasis.
UTILIZE INTERFERON TREATMENT
Interferon-alpha drugs, such as Pegasys or Besremi, can help eliminate PV cancer stem cells, may improve life expectancy in PV patients, reduce the risk of myelofibrosis (MF) and clots, especially when started early. (ref, ref, ref)
Healthy hematopoietic stem cells are necessary to sustain healthy immunity and a healthy life. Interferon is currently our best chance to maintain a healthy hematopoietic stem cell population. Interferon in PV is disease modifying; it leads to bone marrow improvement & complete normalization in a subset of users. Interferon treatment results in a significant reduction of JAK2V617F mutated clone in a majority of PV patients. Normal lifespan with PV is possible, when interferon is started early.
ADOPT A MEDITERRANEAN OR LOW-CARB DIET
Based on studies, the Mediterranean diet is ideal for PV patients, involving the consumption of ample olive oil or nuts, fish every other day, and limited refined carbohydrates & saturated fat. Based on my personal experience, a low-carb (keto) diet is very effective for controlling blood counts and symptoms if followed consistently.
CONSUME DAILY GREEN TEA FOR CONTROLLING JAK2
Daily consumption of hot green tea or its extract, epigallocatechin-3-gallate (EGCG), has been reported to inhibit JAK/STAT pathway across multiple blood cancers and autoimmune conditions. A 2018 study found that EGCG reduces JAK2 expression in chronic myeloid leukemia (CML) cells. A 2013 clinical trial showed that 69% of patients with asymptomatic CLL had a biological response to EGCG. EGCG supplementation induced complete molecular remission in a chronic lymphocytic leukemia case. Furthermore, EGCG has been found to inhibit specific IFN-γ pathways and JAK2 in alopecia areata (an autoimmune disorder that causes hair loss) patients (2018). It also demonstrated potential in vitiligo (an autoimmune skin condition) treatment by inhibiting JAK2 kinase activity (2015) A clinical trial sponsored by the National Cancer Institute showed that 69% of patients with asymptomatic CLL had a biological response to EGCG, encouraging the use of green tea for various indolent low-grade B-cell lymphomas.
I drink 1 large coffee mug of Green Tea and Hibiscus Tea daily, brewed together. I find the combination essential to improve my mood and help resolve the depressive side effects of Pegasys.
CONSUME OTHER JAK2-INHIBITING DRINKS AND FRUITS
Fruits like strawberry, blackberry, pomegranate which contain JAK2-inhibiting anthocyanins, may be highly beneficial for PV patients. Consuming several portions per day, berry powders in hot water, or pomegranate supplements may be beneficial.
MAINTAIN A HEALTHY BODY WEIGHT & CONSIDER METFORMIN
To effectively reduce the risk of cardiovascular complications associated with PV, it’s crucial to maintain a healthy body weight. If you are obese and cannot lose weight, consider medication. Metformin helps with weight loss if you have insulin resistance. Plus, Metformin has been shown to have strong anti-cancer effects. Other recent drugs, too, work extremely well for weight loss: Tirzepatide 22.5%, Semaglutide 17%.
Metformin: A 2018 study investigated the effects of metformin, a biguanide with selective antineoplastic activity, on JAK2V617F-positive myeloproliferative neoplasms (MPN) and compared it with the JAK1/2 inhibitor ruxolitinib. Metformin treatment significantly reduced cell viability, proliferation, clonogenicity, and cellular oxygen consumption in JAK2V617F-expressing cell lines. Metformin also reduced cyclin D1 expression and phosphorylation of several proteins. Combining metformin with ruxolitinib resulted in greater reduction of cell viability and increased apoptosis compared to monotherapy. Metformin effectively reduced tumor burden and splenomegaly in MPN mice models and spontaneous erythroid colony formation in primary cells from polycythemia vera patients. The study concluded that metformin has multitarget antileukemia activity in MPN, including downregulation of JAK2/STAT signaling and mitochondrial activity, and may offer alternative or complementary therapeutic strategies for MPN.
A 2019 open-label phase II trial studied the effects of metformin on primary myelofibrosis (PMF) patients, focusing on bone marrow fibrosis, inflammation mediators, and JAK-STAT pathway activation. Eleven non-diabetic adult PMF patients received metformin for a median of 10 months. Preliminary results showed a trend in bone marrow collagen reduction and downregulation of genes associated with MPN phenotype, but the results were not statistically significant. Metformin was found to be safe and well-tolerated.
I personally found off-label Metformin very helpful against MPN and Tirzepatide very helpful for weight loss.
MANAGE CHOLESTEROL LEVELS & CONSIDER A STATIN
If your LDL cholesterol is high, consider taking a cholesterol-lowering medication. Statins have been shown to be associated with longer life in PV. They’re also associated with improved hematocrit control. A remarkable hematological and molecular response was seen in a patient with polycythemia vera during a combination therapy with simvastatin and alendronate. Try a different statin drug or dose if the first one you tried didn’t work for you.
CONTROL BLOOD PRESSURE & CONSIDER AN ACE INHIBITOR
For blood pressure at or above 130/85, consider blood pressure medication, as some drugs (ACE inhibitors) have been shown to prevent spleen enlargement and fibrosis in MF in mice.
CONSIDER SUPPLEMENTING WITH ANTIOXIDANTS
Antioxidant supplements like NAC and astaxanthin may help control blood values and alleviate fatigue symptoms. Sources: (ref, ref, ref, ref)
SUPPORT ANTI-INFLAMMATORY PROCESSES & CONSIDER A LEUKOTRIENE INHIBITOR
Managing inflammation through interferon, statins, and supplements like Curcumin, NFR2 activators, and fish oil may improve disease control in PV patients. Resveratrol has been shown to specifically inhibit JAK2v617F cells. Leukotriene Inhibitors like Montelukast may work wonderfully against MPNs. Sources: (ref, ref, ref)
AVOID THE FOLLOWING
Iron supplements & Vitamin C supplements (increases the absorption of iron).
Always consult with your doctor before making any changes to your drugs or supplements.
PV Icin en ideal tedaviler
PV ICiN EN IDEAL TEDAViLER HANGiSi?
1) Aspirin + Kan verme
2) Interferon
3) Akdeniz diyeti ve diğer düşük karbonhidrat diyetleri
4) JAK2'yu durduran meyveler ve ebegümeci çayı
5) Kilo kontrolü artı Metformin (insülin direncini kırmak)
6) Kolesterol ilacı
7) Tansiyon ilacı
8 ) Yeşil çay
9) Antioksidan desteği (NAC, Astaxanthin vs)
10) Antienflamatuar desteği (Zerdeçal, vs)
11) Uzak durulacaklar
Aspirin alın ve hematokrit'i doktorunuzun uygun gördüğü aralıkta tutun (<45 veya <42). Bu pıhtı (thrombosis) şansını minimize eder. Kaynaklar: (ref, ref, ref)
Interferon, yani Pegasys veya Besremi, denen ilaçlar PV kanser kök hücrelerini yok etme özelliğine sahip. PV hastalarında yaşamı uzatma olasılığı en yüksek ilaç. Eğer doktorunuz uygun görürse, maddi imkanınız el verirse, tanıdan kısa süre sonra başlanan interferon'un MF'i, pıhtı’yı ve ölümleri önlediği gösterilmiş. Kaynaklar: (ref, ref, ref, ref)
PV için en ideal diyet Akdeniz diyeti. Bu bol zeytinyağı veya kuruyemiş yemeği gerektiriyor. iki günde bir balık. Az karbonhidrat. Sıfır karbonhidrat (keto) diyeti de eğer yapabiliyorsanız kan değerlerini kontrol etmekte çok faydalı. Ne kadar az karbonhidrat, o kadar iyi denebilir, mantıklı bir sınır dahilinde (yağdan alınan kalorileri artımak gerekiyor). Kaynaklar: (ref, ref, ref)
PV için en faydalı meyveler Nar, Çilek, Böğürtlen,Yabanmersini, Ahududu ve Dut (ingilizce berries). Bu meyvelerde JAK2'yu inhibe eden "anthocyanins" bulunuyor. Günde 1 kg'a kadar bunları yemek olası (her gün bu kadar yiyen bir tanıdığım var). Hibiscus tea (ebegümeci çayı) bu meyvelerin yerini tutabilir. Günde 1 hatta 2 kupa beni çok iyi hissetiriyor. Kaynaklar: (ref, ref)
Kilonuzu muhafaza edin. PV'de yaşanan kalp damar sorunlarını minimize etmek için yapabileceğiniz en iyi şey kilo vermek. Eğer kilo veremiyorsanız (obezseniz) ilaca başvurmaktan çekinmeyin. İnsülin direnci varsa Metformin yardımcı oluyor. Metforminin MF'de fibröz'u azalttığı görülmüş. Kaynaklar: (ref, ref, ref, ref)
Kolesterolünüzü kontrol altında tutun. Eğer yüksekse kolesterol ilacı (statin) almaktan çekinmeyin. Statinlerin PV'de ömrü uzattığı görülmüş. Aynı zamanda hematokrit kontrolünde de yardımcı oluyorlar. Birden fazla statin ilacı veya dozunu denemekten çekinmeyin. Kaynaklar: (ref, ref, ref, ref)
Tansiyonunuzu kontrol altına tutun. Eğer 13 veya üzeri ise ilaç almaktan çekinmeyin. Bazı tansiyon ilaçlarının (ACE inhibitör) MF'de dalak büyümesini ve fibrozu önlediği fare deneylerinde gösterilmiş. Kaynaklar: (ref, ref)
PV için en faydalı içecek yeşil çay. Her gün 1 veya 2 kupa içmeye çalışın. Ben Ebegümeci (hibiscus) ile karıştırıp demliyorum, en faydalı kombinasyon oluyor. JAK2'yu inhibe ediyor. Kaynaklar: (ref, ref, ref, ref)
PV'de antioksidan tükenmesi oluyor. Antioksidan almaktan çekinmeyin. Ben NAC aldığım zaman kan değerlerini daha iyi kontrol ediyorum. Kaynaklar: (ref, ref, ref)
PV'de çok fazla yangı (inflammation) oluyor, JAK2 mutasyonunundan ötürü. Yangı'yi kontrol edebilirseniz hastalığı kontrol etmede başarı şansı artıyor. Bunun için Zerdeçal ve diğer NFR2 aktivatorleri alınabilir (Zerdeçal + Zencefil + Boswellia + Ashwaganda ...). Balık yağının da yardımcı olması olası. Interferon ve Statin'de yangıyı kontrol etmekte çok yardımcı. Resveratrol’un JAK2’yu durdurduğu görülmüş. Kaynaklar: (ref, ref, ref, ref, ref)
Uzak durulacaklar:
1) Demir hapı
2) C Vitamini hapı
3) D vitamini hapı da şüpheli (ref, ref)
Bu tamamen benim deneyimlerimden ve araştırmalarından ortaya çıkmış bir liste. Her zaman doktorunuza danışarak hareket edin. Araştırmalar herkese uygun sonuç vermeyebilir. Vücudunu dinlemek de önemli. Doktorunuza da.
Science of PV
Polycythemia Vera: Risk Assessment (video)
Original Error (link)
When does a cancer first arise?
At least in some cases, the original cancer-causing mutation could have appeared as many as 40 years ago, according to a new study by researchers at Harvard Medical School and the Dana-Farber Cancer Institute.
Reconstructing the lineage history of cancer cells in two individuals with a rare blood cancer, the team calculated when the genetic mutation that gave rise to the disease first appeared. In a 63-year-old patient, it occurred at around age 19; in a 34-year-old patient, at around age 9.
Reconstructing the Lineage Histories and Differentiation Trajectories of Individual Cancer Cells in Myeloproliferative Neoplasms (link)
Some cancers originate from a single mutation event in a single cell. Blood cancers known as myeloproliferative neoplasms (MPNs) are thought to originate when a driver mutation is acquired by a hematopoietic stem cell (HSC). However, when the mutation first occurs in individuals and how it affects the behavior of HSCs in their native context is not known. Here we quantified the effect of the JAK2-V617F mutation on the self-renewal and differentiation dynamics of HSCs in treatment-naive individuals with MPNs and reconstructed lineage histories of individual HSCs using somatic mutation patterns. We found that JAK2-V617F mutations occurred in a single HSC several decades before MPN diagnosis—at age 9 ± 2 years in a 34-year-old individual and at age 19 ± 3 years in a 63-year-old individual—and found that mutant HSCs have a selective advantage in both individuals. These results highlight the potential of harnessing somatic mutations to reconstruct cancer lineages.
Current applications of therapeutic phlebotomy (2014)
Patients with PV tend to develop thrombotic events such as cardiovascular and cerebrovascular accidents, and arterial and venous thromboembolism; moreover, the course of the disease can be complicated by myelofibrosis and/or evolution into acute myeloid leukaemia/ myelodysplastic syndrome12. One of the major goals of treatment is to reduce these thrombotic events; the median survival for treated patients is currently over 10 years. Several trials have investigated the outcomes of various therapeutic combinations and they all concluded on the importance of therapeutic phlebotomy. The most important one was the PVSG prospective trial in which 400 patients were randomly assigned to receive either phlebotomy alone or chlorambucil with phlebotomy as needed or radioactive phosphate (32P) with phlebotomy as needed and were then followed for 20 years. The median survival was 13, 11 and 9 years for patients randomly assigned to treatment with phlebotomy alone, radioactive phosphate and chlorambucil, respectively13,14. The study also showed an increased incidence of thrombosis among the group treated with phlebotomy alone, especially during the first 3 years (23% compared to 16% in the 32P treatment arm). However, compared to patients given myelosuppressive therapy, patients who were treated with phlebotomy alone had a lower incidence of haematological malignancies and solid tumours. The authors concluded that phlebotomy provides the best overall survival but at an expense of increased risk of thrombosis during the first 3 years13,14. To resolve the issue of thrombosis, another trial was conducted in which patients were given high-dose aspirin and dipyridamole in addition to phlebotomy, but it was found that this addition of high doses of anticoagulants increased the incidence of gastrointestinal haemorrhages15. However, low-dose aspirin (81 mg) decreased the risk of various thrombotic events.
Hydroxyurea can be used for maintenance therapy in patients who are at high risk of thrombosis or in those who cannot tolerate therapeutic phlebotomy16. Other therapeutic options include treatment with interferon-alpha, or with anagrelide, which is used for essential thrombocythaemia.
Phlebotomy is now considered to be the mainstay of PV treatment. Side effects that may occur following therapeutic phlebotomy are identical to those after any blood donation. The difference is that phlebotomy is done more frequently than voluntary blood donation and therefore patients often report being fatigued and dizzy after several sessions. Iron deficiency may develop but it is usually a mild self-limiting anaemia and iron supplementation is not required unless it become symptomatic. In one study that involved 1,000 blood donors who were interviewed 3 weeks after whole blood donations, the most common reported adverse events were arm bruises, followed by arm soreness, fatigue, vasovagal reactions, haematoma, nausea and vomiting17. Therapeutic phlebotomy has some limitations: patients may be intolerant, or have a low acceptance of it and it may be difficult to gain peripheral vein access. There are no absolute contraindications; the relative contraindications include severe heart disease and anaemia. At our institution, during each session, 450 mL of blood are withdrawn daily until the haematocrit drops below 40%; this is usually followed by maintenance phlebotomy at regular intervals every 1 to 2 months according to the haematocrit level. However, the interval between phlebotomies varies widely and may be much longer than every 2 months.
There are no true guidelines concerning the optimal haematocrit level in patients with PV. Some studies suggested maintaining haematocrit at a level below 45% to reduce the risk of vascular occlusive episodes18. Thomas and his colleagues showed that a reduction of the haematocrit to a mean of 45.5% was associated with a decrease in whole blood viscosity with a great improvement of cerebral blood flow (73%; P<0.001)19. However a recent study conducted by Di Nisio et al. found no correlation between haematocrit levels and thrombotic episodes or mortality in patients with PV20. In order to determine the optimal cut-off for haematocrit level, a large trial (CYTO-PV trial) was conducted in Italy21. This trial showed that patients maintained at a target haematocrit of less than 45% had a significantly lower rate of cardiovascular death and major thrombosis compared to those maintained at a haematocrit greater than 45%, which contrasts with the findings of Di Nisio et al. In this large trial, 182 adults with JAK2-positive PV were randomly assigned to the low-haematocrit group (haematocrit <45%) and 183 adults with JAK2-positive PV to the high-haematocrit group (haematocrit >45%). Some patients received phlebotomy every other day or twice a week until the target haematocrit was reached, some were administered hydroxyurea and some were treated with both therapies. Cardiovascular events occurred in 4.4% of patients in the low-haematocrit group and 10.9% of those in the high haematocrit group (hazard ratio, 2.69; 95% CI: 1.19 to 6.12; P=0.02) while the incidence of death from cardiovascular causes or major thrombosis was 1.1 per 100 person-years in the low-haematocrit group and 4.4 per 100 person-years in the high-haematocrit group. This trial showed that a haematocrit less than 45% is associated with a lower rate of thrombotic events22.
The WHO Updated Diagnostic Criteria for MPN, 2016
Blast Transformation in Myeloproliferative Neoplasms: Risk Factors, Biological Findings, and Targeted Therapeutic Options, 2019
Myeloproliferative neoplasms represent a heterogenous group of disorders of the hematopoietic stem cell, with an intrinsic risk of evolution into acute myeloid leukemia. The frequency of leukemic evolution varies according to myeloproliferative neoplasms subtype. It is highest in primary myelofibrosis, where it is estimated to be approximately 10–20% at 10 years, following by polycythemia vera, with a risk of 2.3% at 10 years and 7.9% at 20 years <depends on age?>. In essential thrombocythemia, however, transformation to acute myeloid leukemia is considered relatively uncommon. Different factors are associated with leukemic evolution in myeloproliferative neoplasms, but generally include advanced age, leukocytosis, exposure to myelosuppressive therapy, cytogenetic abnormalities, as well as increased number of mutations in genes associated with myeloid neoplasms. The prognosis of these patients is dismal, with a medium overall survival ranging from 2.6–7.0 months. Currently, there is no standard of care for managing the blast phase of these diseases, and no treatment to date has consistently led to prolonged survival and/or hematological remission apart from an allogeneic stem cell transplant. Nevertheless, new targeted agents are currently under development. In this review, we present the current evidence regarding risk factors, molecular characterization, and treatment options for this critical subset of myeloproliferative neoplasms patients.
Biomarkers / JAK2 (link)
Data-driven analysis of JAK2V617F kinetics during interferonalpha2 treatment of patients with polycythemia vera and related neoplasms (2020)
Treatment with PEGylated interferon-alpha2 (IFN) of patients with essential thrombocythemia and polycythemia vera induces major molecular remissions with a reduction in the JAK2V617F allele burden to undetectable levels in a subset of patients. A favorable response to IFN has been argued to depend upon the tumor burden, implying that institution of treatment with IFN should be as early as possible after the diagnosis. However, evidence for this statement is not available. We present a thorough analysis of unique serial JAK2V617F measurements in 66 IFN-treated patients and in 6 untreated patients. Without IFN treatment, the JAK2V617F allele burden increased exponentially with a period of doubling of 1.4 year. During monotherapy with IFN, the JAK2V617F allele burden decreased mono- or bi-exponentially for 33 responders of which 28 patients satisfied both descriptions. Bi-exponential description improved the fits in 19 cases being associated with late JAK2V617F responses. The decay of the JAK2V617F allele burden during IFN treatment was estimated to have half-lives of 1.6 year for the monoexponential response and 1.0 year in the long term for the bi-exponential response. In conclusion, through data-driven analysis of the JAK2V617F allele burden, we provide novel information regarding the JAK2V617F kinetics during IFN-treatment, arguing for early intervention.
The Long, Slow Process of Carcinogenesis (link)
The team studies twelve MPN patients, whose tissue samples provided over a thousand different clones of malignant blood cells. Sequencing these turned up over 580,000 mutations (!), and the paper puts these into a phylogenetic framework to reconstruct the sequence of what the key mutations were and when they might have taken place. Using rates of mutation as a clock, some of them appear to go back even to before birth - the key JAK2V617F mutation, long associated with these malignancies, is estimated to have shown up anywhere from the 33rd week of gestation up to the age of 11. The DNMT3 mutation, similarly, seems to have appeared from the 8th week of gestation (!) out to about the age of 8. Additional driver mutations layer on top of these early events over the years to come - the mean latency between the JAK2 mutation and diagnosis of cancer, for example, was about thirty years.
[Bu kanser degil adeta hayat boyu suren kronik bir hastalik. kanser tanisindan 30 yil once vucudunda var]
Phylogenetic reconstruction of myeloproliferative neoplasm reveals very early origins and lifelong evolution (link)
The study used phylogenetic analysis of somatic mutations in hematopoietic colonies to reconstruct the evolutionary history and timing of driver mutations in 10 patients with myeloproliferative neoplasms (MPNs).
In 5 patients where JAK2V617F was the first driver mutation, it was acquired very early in life - between 6.2 weeks post-conception to 11.4 years of age. The mean latency between acquiring JAK2V617F and MPN diagnosis in these patients was 34 years (range 20-54 years).
DNMT3A mutations, commonly associated with age-related clonal hematopoiesis, were also acquired early - between in utero to 7.8 years of age.
The rate of clonal expansion after acquiring JAK2V617F was variable between patients. The slowest growing clone had a selection coefficient of 0.18 per year, while the fastest had 0.68 per year. Faster expanding clones had shorter latency to MPN diagnosis.
Additional driver mutations led to increased clonal expansion rates, with the fastest clones expanding at 2.33 per year after acquiring multiple drivers.
Modeling showed JAK2V617F would have been detectable 10 to 40 years before clinical diagnosis using sensitive assays detecting 0.01% mutant cells.
The results demonstrate MPNs originate from early life driver mutations with variable lifelong clonal expansion, providing opportunities for early detection and intervention. The long latencies between initial mutation and malignancy reveal a new model of stepwise cancer evolution over decades.
Anti-Cancer Agents as Frontline Treatment of MPNs Lead to Higher Probability of Non-Melanoma Skin Cancers (2020)
Exposure to ruxolitinib (Jakafi), hydroxyurea (Hydrea), and pipobroman (Vercyte) as first-line treatment of Philadelphia-negative myeloproliferative neoplasms (MPNs) alone or in combination with other cytoreductive treatment may increase the probability of patients developing non-melanoma skin cancer, highlighting a need for active dermatological surveillance of these patients, according to findings from the MPN-K study (NCT03745378), published inLeukemia.
Higher risk of primary cancers after polycythaemia vera and vice
versa (link)

Current and emerging therapies
Novel and emerging therapies for the treatment of polycythemia vera (2014)
Treatment and clinical endpoints in polycythemia vera: seeking the best obtainable version of the truth (2022)
This perspective article by Gotlib provides an overview of the current treatment landscape and remaining gaps in polycythemia vera (PV), a Philadelphia chromosome-negative myeloproliferative neoplasm. Key points:
Treatment planning in PV involves continual reassessment of traditional risk factors (age, prior thrombosis) to determine need for cytoreduction beyond foundational therapy with aspirin and phlebotomy.
Hydroxyurea has been the mainstay of cytoreduction for decades, but recent phase 3 trials of ruxolitinib and ropeginterferon-alpha-2b provide new options. However, limitations exist in trial data.
Achieving tight hematocrit control and reducing thrombotic events are clear treatment goals, but assessing impact on longer-term outcomes like myelofibrosis/leukemia evolution and survival is challenging in clinical trials. Thus, reliance on real-world data is needed.
Symptom burden in PV is heterogeneous but undertreated. Patient-reported outcomes like the MPN-SAF TSS provide valuable metrics.
Novel agents in development include inhibitors of MDM2, LSD1, HDAC, and modulators of iron homeostasis, but their long-term disease-modifying potential remains unknown.
Key Trial Results:
CYTO-PV trial: Maintaining hematocrit <45% vs 45-50% led to 4-fold lower rate of thrombosis and cardiovascular death.
ECLAP trial: Aspirin reduced thrombosis by 60%. High WBC count was a risk factor.
Pegylated IFN trials: Achieved superior hematologic control and molecular responses vs hydroxyurea, but statistically similar CR rates. Discontinuation rates 10-30%.
CONTINUATION-PV: 5-yr ropeginterferon data showed high hematologic and molecular response durability vs hydroxyurea.
RESPONSE trial: Ruxolitinib achieved hematocrit control in 60% of hydroxyurea-resistant/intolerant patients vs 20% with standard therapy. Spleen responses seen.
MPN-RC 112: Hydroxyurea had higher bone marrow response rates than pegylated IFN, contrasting with molecular responses favoring IFN.
Limitations:
No RCTs powered to show cytoreductives like hydroxyurea reduce thrombosis vs phlebotomy alone.
Progression and survival endpoints cannot be assessed within trial timeframes. Real-world data is needed to address this gap.
In summary, this perspective reviews the evidence for current and emerging therapies in PV, highlighting remaining gaps in assessing their impact on clinically meaningful endpoints like thrombosis, progression, and survival. Ongoing research is still needed to optimize and individualize management in this chronic myeloproliferative neoplasm.
Phase 2/3 randomized trials of IFNs
MPD-RC 112 Trial
Phase 3 trial comparing pegylated IFN-α-2a (PEG) to hydroxyurea (HU) in 168 treatment-naive, high-risk PV and ET patients.
Primary endpoint: Complete response (CR) rate at 12 months per ELN criteria.
Results:
CR rates: 37% for HU vs 35% for PEG (p=0.80), not statistically significant.
In PV patients, 12-month CR rates were 30% for HU vs 28% for PEG.
Hematocrit control was achieved in 43% on HU vs 65% on PEG (p=0.04) in PV patients.
Median JAK2V617F allele burden reductions were -5.3% for HU vs -10.7% for PEG at 12 months.
Histopathologic responses were higher with HU (23%) than PEG (5%) at 12 months (p=0.01).
Grade 3/4 adverse events more common with PEG (46%) than HU (28%).
Limitations: Trial closed early after 168 patients (out of target 300) due to drug supply issues.
PROUD-PV/CONTINUATION-PV Trials
Compared ropeginterferon-α-2b (roPEG) to HU in PV patients.
PROUD-PV: roPEG non-inferior to HU after 12 months (CR rates 21.3% vs 27.6%).
CONTINUATION-PV: At 60 months, CR rates were 56% for roPEG vs 44% for HU (p=0.0974).
JAK2V617F burden decreased through 60 months with roPEG but increased after 12 months with HU.
roPEG discontinuation due to adverse events 8% vs 4% for HU at 36 month follow-up.
Low-Risk PV Trial
Randomized PV patients to roPEG plus standard therapy vs standard therapy (phlebotomy & aspirin) alone.
roPEG arm had superior hematocrit control, reduced phlebotomies, normalized counts vs standard therapy at 12 months.
Adverse events higher with roPEG but low grade 3+ rates in both arms.
Showed potential benefits of adding IFN in low-risk PV patients.
Key Conclusions:
MPD-RC 112: No difference in 12-month CR rates between HU and PEG in high-risk ET/PV. Longer treatment with PEG appeared better for count/mutation control, while HU had higher histopathologic responses. Both limited thrombotic events and progression.
PROUD-PV/CONTINUATION-PV: Showed higher and more durable cytogenetic and molecular responses with roPEG vs HU over 60 months in PV patients.
Low-risk PV trial: Suggests benefits to adding roPEG to standard therapy in low-risk PV patients regarding hematocrit control, reduced phlebotomies, normalized counts.
Overall, the peginterferon trials demonstrate these agents can achieve high hematologic and molecular response rates compared to standard hydroxyurea therapy in both high and low-risk PV patients. Responses may take >12 months to fully emerge. Discontinuation rates are higher than hydroxyurea but overall peginterferons are well tolerated. These results support consideration of peginterferon therapy in appropriate PV patients. Additional randomized data is still needed to fully define optimal treatment strategies and sequencing.
Ruxolitinib
Ruxolitinib (RUX) is a JAK1/JAK2 inhibitor that has been evaluated in several clinical trials for treatment of patients with polycythemia vera (PV). The key results from these studies are:
RESPONSE Trial
Phase 3 trial of RUX vs standard therapy in 222 phlebotomy-dependent PV patients with splenomegaly who were resistant/intolerant to hydroxyurea.
RUX starting dose 10 mg twice daily, titrated to balance efficacy and cytopenias.
Primary endpoint: Hematocrit control and ≥35% spleen volume reduction at week 32.
Results at 32 weeks:
Primary endpoint achieved in 21% on RUX vs 1% on standard therapy.
Hematocrit control in 60% on RUX vs 20% on standard therapy.
≥35% spleen volume reduction in 38% on RUX vs 1% on standard therapy.
50% symptom score reduction in 49% on RUX vs 5% on standard therapy.
Herpes zoster occurred in 6% on RUX vs 0% on standard therapy.
At 5 years:
74% probability of maintaining primary endpoint response on RUX.
Thromboembolism rates 1.2 per 100 patient-years on RUX vs 8.2 per 100 patient-years on standard therapy.
RUX discontinuation rate 15%.
Similar survival between RUX and standard therapy arms.
Supported FDA approval of RUX as second-line therapy for PV.
RESPONSE-2 Trial
Similar PV population as RESPONSE but without splenomegaly.
Hematocrit control achieved in 62% on RUX vs 19% on standard therapy.
Further supported RUX efficacy for PV.
RELIEF Trial
PV patients with symptoms on stable hydroxyurea therapy randomized to RUX vs continuing hydroxyurea.
Trend toward improved symptoms with RUX but not statistically significant.
Suggested RUX may provide additional symptom benefit for some PV patients with residual symptoms despite hydroxyurea therapy.
In summary, the key efficacy results from these randomized trials demonstrate:
In hydroxyurea-resistant/intolerant PV patients, RUX led to significantly higher hematocrit control, spleen volume reductions, and symptom improvement compared to standard therapies.
Hematocrit control was achieved in 60-62% of patients on RUX compared to only 19-20% on standard therapy.
Spleen volume reductions of ≥35% occurred in 38% on RUX compared to 1% on standard therapy.
RUX also showed a trend for improved thromboprotection with lower thromboembolism rates vs standard therapy, although studies were not powered for this endpoint.
Discontinuation rates due to adverse events were low at 15%, but risks of herpes zoster and other infections were higher with RUX.
In conclusion, RUX demonstrates efficacy in achieving hematologic, splenic, and symptom control in hydroxyurea-resistant/intolerant PV patients, supporting its regulatory approval as a second-line treatment option for these patients. Some benefits were also suggested for symptom management in hydroxyurea-treated patients with residual symptoms. Further evaluation of long-term thrombosis rates and survival remains needed.
Updates in Therapy (2019)
Hydroxyurea (HU) remains first-line cytoreductive therapy in high risk PV and ET, based on PT-1 trial showing superiority over anagrelide for arterial events and myelofibrosis in high risk ET (Harrison et al, 2005).
Recombinant interferon alfa has high hematologic and molecular response rates in PV and ET (Kiladjian et al, 2008; Quintas-Cardama et al, 2009). It represents an alternative to HU, especially in young patients.
MPD-RC 112 trial found no difference between pegylated interferon alfa-2a and HU for hematologic or molecular response rates at 12-24 months in high risk PV or ET (Mascarenhas et al, 2018). Responses took time to develop with interferon.
DALIAH trial showed higher hematologic and molecular response rates at 36 months for interferon versus HU in PV (Knudsen et al, 2018). Discontinuation was more frequent with interferon.
Ropeginterferon alfa-2b had high hematologic and molecular response rates in PV in phase I/II study (Gisslinger et al, 2015). PROUD-CONTI phase III trial showed noninferiority to HU at 12 months and superiority for sustained hematologic and molecular responses at 2-3 years (Gisslinger et al, 2016; 2018). It was recently recommended for approval by EMA for PV.
Ruxolitinib was superior to best available therapy for hematocrit control, spleen volume reduction, symptoms, and trend for lower thrombosis in RESPONSE trial in HU-resistant/intolerant PV with splenomegaly (Vannucchi et al, 2015). Durable responses were maintained over 5 years of follow-up (Kiladjian et al, 2018).
In RESPONSE-2 trial in PV without splenomegaly, ruxolitinib significantly improved hematocrit control vs best available therapy (Passamonti et al, 2017). Durable hematologic response rates were higher with ruxolitinib at 80 weeks (Griesshammer et al, 2018).
Ruxolitinib showed efficacy after interferon use in RESPONSE studies and was superior to interferon as best available therapy (Kiladjian et al, 2018).
RELIEF study did not show significant benefit for ruxolitinib over HU for symptoms in PV patients with controlled blood counts (Mesa et al, 2017).
In MAJIC-ET, ruxolitinib did not improve hematologic response rate at 1 year vs best available therapy in HU-resistant/intolerant ET but improved symptoms (Harrison et al, 2017).
Ruxolitinib normalized blood counts and improved symptoms in HU-resistant/intolerant ET (Verstovsek et al, 2017).
Investigational Approaches
The HDM2 inhibitor idasanutlin showed efficacy in heavily pretreated PV and ET, including molecular responses, as monotherapy and combined with pegylated interferon alfa-2a (Mascarenhas et al, 2017). Phase II and novel agents are in development.
HDAC inhibitors like vorinostat have preclinical efficacy in PV (Akada et al, 2012) and clinical activity (Finazzi et al, 2013; 2016) but toxicity concerns exist.
Telomerase inhibitor imetelstat had high hematologic and molecular response rates in ET (Baerlocher et al, 2015) but development focuses on myelofibrosis.
JAK inhibitor momelotinib showed limited benefit in PV and ET (Verstovsek et al, 2017). Development focuses on myelofibrosis.
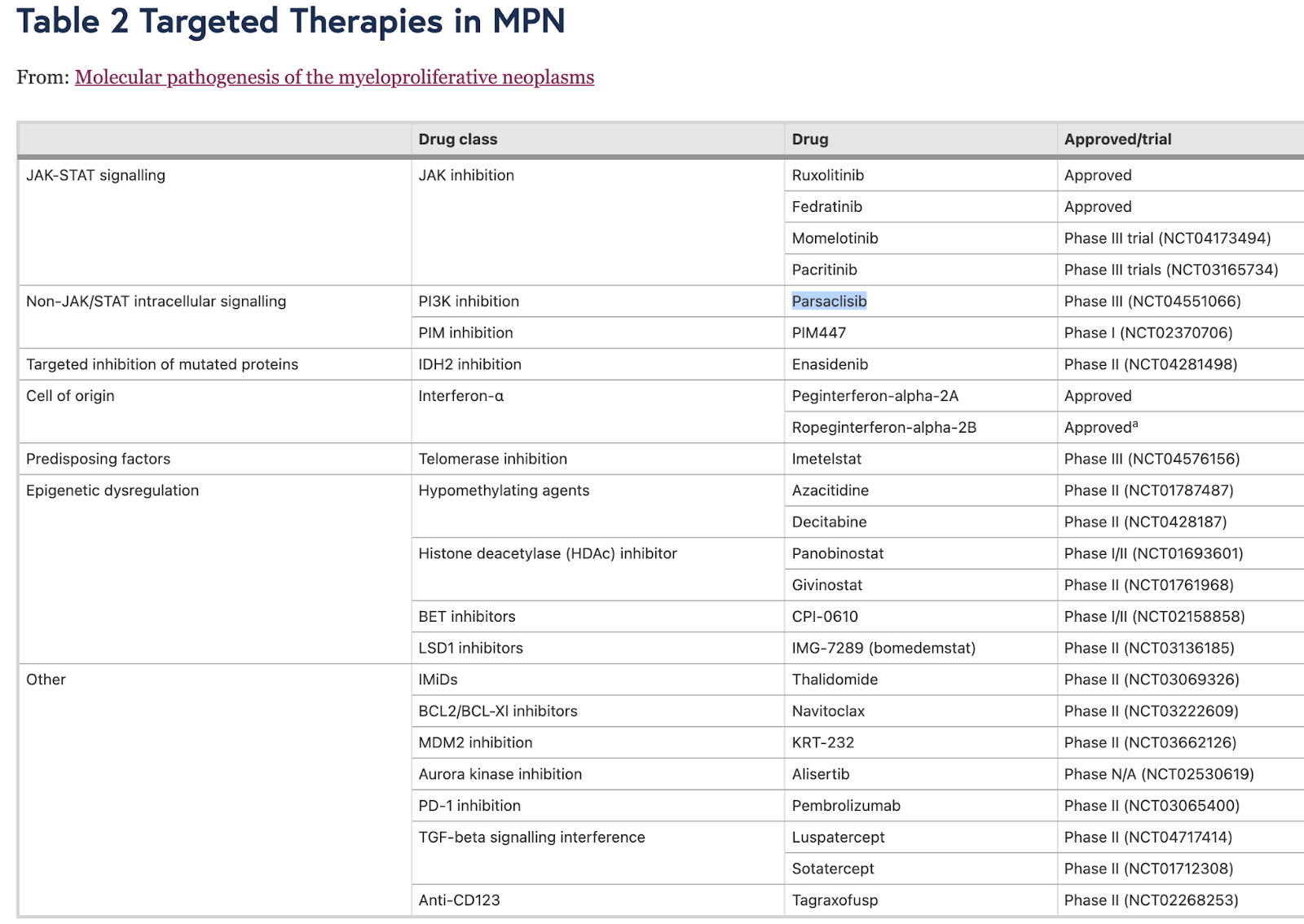
Targeted Therapies in MPN
Phenotypes and blood markers for management of PV and MPNs
Commonly Recognized Markers:
Complete blood count (CBC) to check HCT, PLT, WBC and other related metrics
JAK2 mutation testing
Bone marrow morphology
Lesser-Known Markers:
Blood Trombaxone Levels: Related to clotting mechanisms.
To normalize Trombaxone, some publications suggest twice daily aspirin is more appropriate (vs once daily). My hematologist has been strongly recommending that but I didn't follow his advice consistently. I might go back to Aspirin x 2. Check out these publications for further insights: 2022, 2020, Ref
Histamine Levels: Elevated levels can cause itching (pruritus) and may indicate mast cell activation.
To control histamine levels, we have plenty of safe anti-histamine drugs (e.g. loratadine). Might be worth considering if you have issues with histamine. As an added bonus, h1 antihistamines have nice anti cancer effects. Impressive evidence coming from other cancers. Dive deeper into this topic: My Longevity Journey Blog
Various inflammatory markers (e.g. TNF alpha, IL6, TGF-beta)...
Inflammation is a whole topic by itself. Supplements like Curcumin, Boswellia, Resveratrol... stand out towards beneficial effects for MPNs. But other anti-inflammatory drugs are actively being explored in clinical trials.
Identification of Serum Lactate Dehydrogenase (LDH) As an Independent Prognostic Biomarker in Polycythemia Vera, 2016
Background The International Working Group for Myeloproliferative Neoplasms (MPN) Research and Treatment (IWG-MRT) has previously identified older age, leukocytosis, venous thrombosis and abnormal karyotype as risk factors for overall survival (OS) in polycythemia vera (PV), and older age, abnormal karyotype and leukocytes ≥15 × 109/l as risk factors for leukemia-free survival (LFS) (Leukemia2013;27:1874). Serum lactate dehydrogenase (LDH) is a surrogate quantitative measure of cell turnover and tumor burden. We hypothesized that, compared to leukocyte count, serum LDH might be a biologically more accurate indicator of tumor aggression and sought to examine its potential utility as a prognostic biomarker in PV. Methods Study patients were selected from our institutional database of MPN based on their meeting the 2008 or 2016 World Health Organization criteria for diagnosis of PV (Blood. 2009;114:937; Blood 2016 127:2391) and availability of serum LDH level, obtained within six months of diagnosis. Information on karyotype and targeted next-generation sequencing was available in a subset of the patients (Blood 2015 126:354). Statistical analyses considered clinical and laboratory parameters obtained at time of diagnosis. Age and leukocyte count prognostic categories were based on previously published IWG-MRT study (Leukemia2013;27:1874). Results Patient characteristics: A total of 216 patients (50% females) met the above-outlined criteria: median (10th-90th percentile) levels were for age 63 years (38-81), hemoglobin 18 g/dL (16.6-20.7), platelets 467 x 10(9)/L (237-833), leukocyte count 11.7 x 10(9)/L (7.2-20.3) and spleen size 0 cm (0-2). Pruritus was documented in 28%, microcirculatory symptoms in 31%, erythromelalgia in 6%, hypertension in 45%, diabetes in 7%, active tobacco use in 13%, hyperlipidemia in 25%, palpable spleen in 26% and abnormal karyotype in 15% of informative cases. Grading for bone marrow reticulin fibrosis was documented for 144 patients: 50% grade "0", 42% grade "1", 7% grade "2" and 1 grade "3". Thrombosis history at diagnosis was documented in 26% of patients and occurred after diagnosis in 19%. Mutation analysis was available in 72 patients and revealed TET2 mutations in 18 (25%), ASXL1 in 5 (7%), SRSF2 in 2 (3%) and IDH2 in one (1.4%). Serum LDH levels and correlates: Median serum LDH level was 226 U/L (range 71-1008); the upper normal limit (UNL) for Mayo Clinic was 222 U/L. Increased serum LDH was recorded in 110 (51%) patients that included 26 (12%) patients with LDH ≥1.5 x UNL. A significant correlation was demonstrated between increased serum LDH and older age (p=0.007), female sex (p=0.04), leukocytosis (p=0.01), venous thrombosis history (p=0.005) and, interestingly, absence of active tobacco use (p=0.003); no correlation was noted for bone marrow reticulin fibrosis, presence of palpable splenomegaly, abnormal karyotype or ASXL1 mutation. Survival analysis: After a median follow-up of 77 months, 82 (38%) deaths, 8 (3.7%) leukemic transformations, 13 (6%) fibrotic progressions and 41 (19%) thrombotic events were documented. In univariate analysis, the following adversely affected OS: advanced age (P<0.0001), increased LDH as a continuous variable (p=0.0006), LDH ≥1.5 x UNL (p<0.0001), leukocyte count ≥15 x 10(9)/L (p=0.02) and arterial thrombosis history (p=0.001). In multivariable analysis, only age and LDH remained significant; multivariable HR (95% CI) were 5.4 (2.8-10.4) for age ≥67 years, 3.2 (1.8-6.0) for LDH ≥1.5 x UNL and 2.4 (1.2-4.7) for age 57 to 66 years. In the subset of patients with available information on karyotype and non-JAK2 mutations (n=72), advanced age, LDH ≥1.5 x UNL and ASXL1 mutations remained significantly associated with inferior survival. Serum LDH also predicted leukemic transformation (HR 17.8, 95% CI 4.1-78) and fibrotic progression (HR 11.6, 95% CI 25-53.7); in multivariable analysis, only serum LDH ≥1.5 x UNL (HR 22.3, 95% CI 2.1-234.6) and abnormal karyotype (HR 9.5, 95% CI 1.2-74.7) predicted leukemic transformation and only the former predicted fibrotic progression. Conclusions Serum LDH is a simple and inexpensive biomarker that might supersede leukocyte count as an independent predictor of overall, leukemia-free and myelofibrosis-free survival in PV; advanced age and ASXL1 mutations also retained significance for OS and abnormal karyotype for LFS.
Molecular pathogenesis of the myeloproliferative neoplasms (2021)
The JAK/STAT pathway is an evolutionarily conserved pathway that mediates extracellular protein-cell surface receptor interactions. It plays a crucial role in many metabolic, immune cell functions, and hematopoiesis. In myeloproliferative neoplasms (MPN), constitutive activation of the JAK/STAT signaling pathway is a key factor in disease pathogenesis, with driver mutations in JAK2, CALR, and MPL genes found in most patients.
Abnormal JAK/STAT signaling is implicated in various hematological malignancies and solid tumors. In MPN, the JAK2 V617F mutation drives constitutive activation of the JAK/STAT pathway, affecting 95% of polycythemia vera (PV) patients and approximately 50% of essential thrombocythemia (ET) and primary myelofibrosis (PMF) patients. Other mutations in JAK2, MPL, and CALR genes also contribute to the disease.
A small group of patients does not have detectable mutations in these genes and are considered "triple negative." However, additional genetic tests can identify other markers of clonality. Activating JAK/STAT mutations alone are sufficient to generate an MPN phenotype in murine models, and JAK1/2 inhibitor ruxolitinib is effective across all mutant driver backgrounds.
Despite the initial discovery of the JAK2 V617F mutation as a key driver in most MPN patients, various factors determine the overall disease phenotype, prognosis, and development of the disease. Factors include additional pathogenic mutations, order of acquisition, cellular context, germline predisposition, balance of STAT protein signaling, epigenetic dysregulation, and extrinsic influences. Genetic complexity and heterogeneity pose significant diagnostic and therapeutic challenges in MPN.
STAT PROTEINS IN MPN
In MPNs (myeloproliferative neoplasms), STAT proteins, particularly STAT1, STAT3, and STAT5, play significant roles in oncogenesis and tumor suppression. STAT5 activation is a key mediator in MPN pathogenesis, as it has been shown to generate the MPN phenotype. In ET and PV patients, STAT5A targets were enriched and nuclear phosphorylation of STAT5A was identified in JAK2 V617F positive colonies. Mouse models have also demonstrated the importance of STAT5 in generating the PV phenotype.
STAT1 signaling has been suggested as a mediator of differential molecular response between ET and PV. Phosphorylated STAT1 was detectable in ET patients but not PV patients. Mouse models showed that the loss of STAT1 resulted in a phenotype favoring erythropoiesis and reduced fibrosis. The balance between STAT1 and STAT5 signaling might contribute to phenotype determination in MPN.
Constitutive activation of STAT3 has been identified in MPN patients, with higher levels of STAT3 tyrosine phosphorylation found in JAK2 V617F positive individuals. A murine model with STAT3 hyperactivity developed myeloproliferative and lymphoproliferative pathology. STAT3 deletion led to altered MPN phenotype in JAK2 V617F mice.
NON-JAK/STAT SIGNALING IN MPN
Activation of STAT-independent phosphoinositide 3-kinase (PI3K) and mitogen-activated protein kinase (MAPK) signaling pathways is crucial in the disease pathogenesis of JAK2 V617F positive MPN. CALR mutations have also been observed to activate MAPK signaling pathways. Both PI3K/mTOR and MAPK pathways may remain active even in the presence of the JAK inhibitor ruxolitinib. Combining JAK inhibition with either PI3K or mTOR inhibitors has shown enhanced efficacy in some cases. Activated MAPK, PI3K/AKT, and JAK/STAT signaling are also observed in various myeloid malignant phenotypes. Improving the understanding of dysregulated signaling cascades in MPN patients could lead to more efficacious treatments.
NEGATIVE REGULATION OF INTRACELLULAR SIGNALING IN MPN
Negative regulation of intracellular signaling in MPN involves phosphatases or proteins targeting ubiquitination and proteasome-mediated degradation. SOCS proteins are critical negative regulators for JAK/STAT signaling, with conflicting evidence on their role in regulating mutant JAK2. CBL mutations, driving myeloproliferation and activating JAK/STAT and PI3K/AKT signaling, have been identified in many malignancies, including MPN. Loss of phosphatase activity in PTEN can drive an MPN phenotype, while higher expression of DUSP1 may be required in the JAK2 V617F context to protect cells by moderating JNK/P38 MAPK signaling.
ADDITIONAL MUTATIONS
Secondary mutations in genes such as TET2, ASXL1, and DNMT3A have been identified in some patients with PV. These mutations are thought to contribute to disease progression and the development of more aggressive forms of the disease, such as myelofibrosis or acute myeloid leukemia.
TET2 mutations and their clinical correlates in polycythemia vera, essential thrombocythemia and myelofibrosis
High-throughput DNA sequence analysis was used to screen for TET2 mutations in bone marrow-derived DNA from 239 patients with BCR-ABL-negative myeloproliferative neoplasms (MPNs). Thirty-two mutations (19 frameshift, 10 nonsense, 3 missense; mostly involving exons 4 and 12) were identified for an overall mutational frequency of approximately 13%. Specific diagnoses included polycythemia vera (PV; n=89), essential thrombocythemia (ET; n=57), primary myelofibrosis (PMF; n=60), post-PV MF (n=14), post-ET MF (n=7) and blast phase PV/ET/MF (n=12); the corresponding mutational frequencies were approximately 16, 5, 17, 14, 14 and 17% (P=0.50). Mutant TET2 was detected in approximately 17 and approximately 7% of JAK2V617F-positive and -negative cases, respectively (P=0.04). However, this apparent clustering of the two mutations was accounted for by an independent association between mutant TET2 and advanced age; mutational frequency was approximately 23% in patients > or =60 years old versus approximately 4% in younger patients (P<0.0001). The presence of mutant TET2 did not affect survival, leukemic transformation or thrombosis in either PV or PMF; a correlation with hemoglobin <10 g per 100 ml in PMF was noted (P=0.05). We conclude that TET2 mutations occur in both JAK2V617F-positive and -negative MPN, are more prevalent in older patients, display similar frequencies across MPN subcategories and disease stages, and hold limited prognostic relevance.
Inflammation and Oxidation in MPNs
Inflammation:
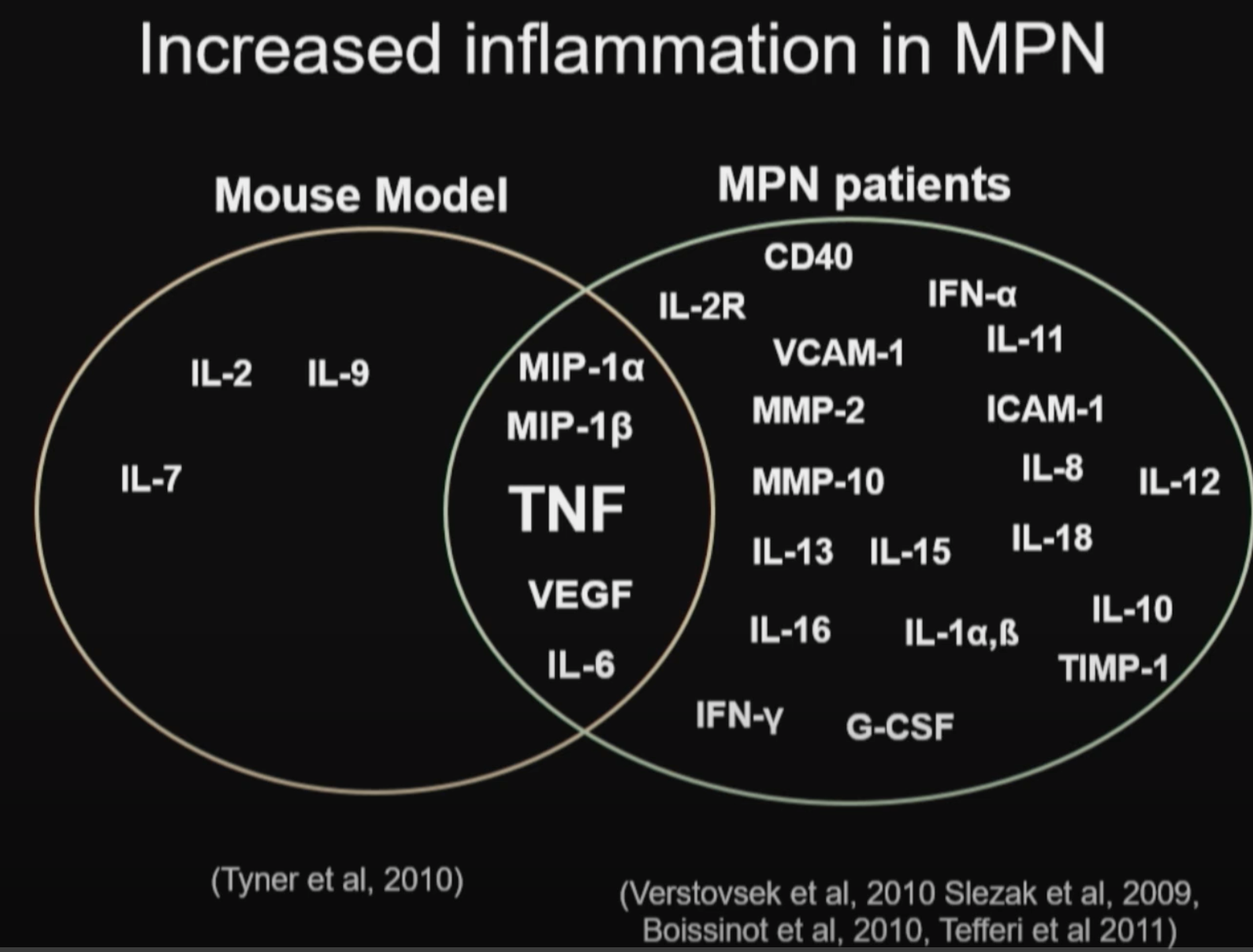
Abnormal expression and activity of a number of proinflammatory cytokines are implicated in MPNs (ref):
IL-1β, TNF-α, IL-6, IL-8, VEGF, PDGF, TGF-β and IFNs.
Chronic inflammation may be an important driving force for clonal evolution and disease progression in MPNs.
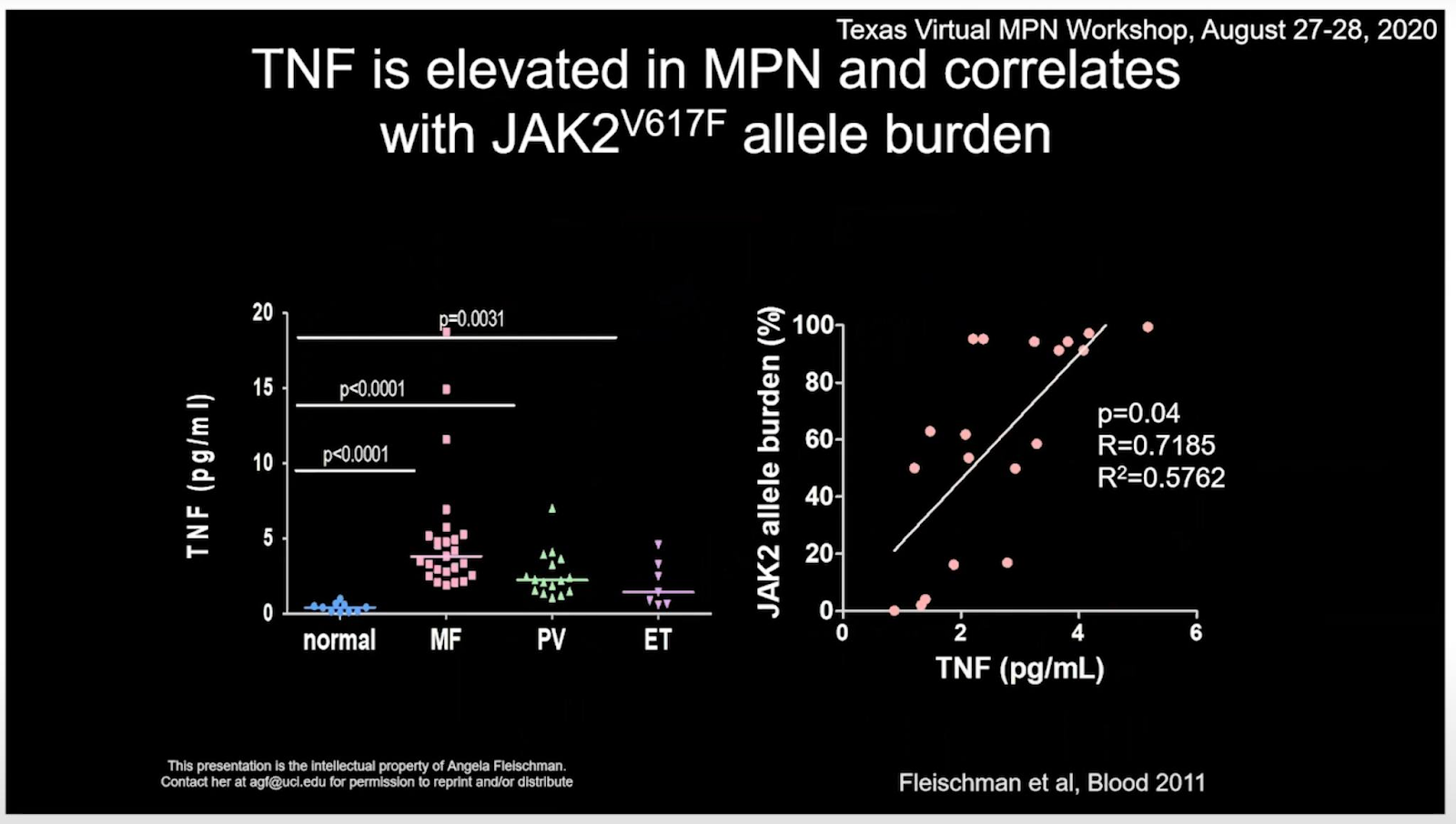
Tumor necrosis factor (TNFα), may underlie malignant clonal dominance in MPN based on results from mouse models. (ref)
In MF, bone marrow fibrosis itself is thought to be mediated heavily by the cytokine TGF-β, and possibly other cytokines produced as a result of hyperactivated JAK2 kinase in the malignant clone. (ref)
Treatment of MF with the TGF-β 1/3 Inhibitor AVID200 (MPN-RC 118) (ref)
Successful case report of controlling MF via TGF-β inhibiting supplements (ref)
Successful MPN treatments (INF-alpha, Ruxolitinib, Aspirin, Statins etc) also tend to be powerful anti-inflammatories.
Oxidation:
Reactive oxygen species (ROS) have a major role in carcinogenesis and disease progression in MPNs, where the malignant clone itself produces excess of ROS thereby creating a vicious self-perpetuating circle in which ROS activate proinflammatory pathways (NF-κB) which in turn create more ROS. (ref)
Targeting ROS via NF-κB inhibition may be a therapeutic option, which could possibly prevent genomic instability and ultimately myelofibrotic and leukemic transformation.
BET inhibitor, Pelabresib, being clinical trialed in MF is also a NF-KB inhibitor (ref).
Pevonedistat targets malignant cells in MPNs via NFκB inhibition (ref).
Aspirin and ibuprofen are least potent, while resveratrol, curcumin, celecoxib, and tamoxifen are the most potent anti-inflammatory and antiproliferative agents of NF-kB. (ref)
The gene NRF2 is significantly downregulated in all MPNs (ref). Activating NRF2 is a viable strategy to fight MPNs.
NAC and Astaxanthin may be promising for controlling oxidation.
MPNs as Inflammatory Diseases: The Evidence, Consequences, and Perspectives (link)
Chronic inflammation may be an important driving force for clonal evolution and disease progression in MPNs. Abnormal expression and activity of a number of proinflammatory cytokines are associated with MPNs, in particular MF, in which immune dysregulation is pronounced as evidenced by dysregulation of several immune and inflammation genes. In addition, chronic inflammation has been suggested to contribute to the development of premature atherosclerosis and may drive the development of other cancers in MPNs, both nonhematologic and hematologic. The MPN population has a substantial inflammation-mediated comorbidity burden. Early intervention with interferon-alpha2, which as monotherapy has been shown to be able to induce minimal residual disease, in combination with potent anti-inflammatory agents such as JAK-inhibitors is foreseen as the most promising new treatment modality in the years to come.
Module 1: Pre-MPN, Atypical MPNs, and Inflammation? 2020

JAK2 The Future_ Updates in the Biology and Treatment of Myeloproliferative Neoplasms, 2020
Stephen Oh, MD, PhD
JAK2 The Future_ Updates in the Biology and Treatment of Myeloproliferative Neoplasms, 2021
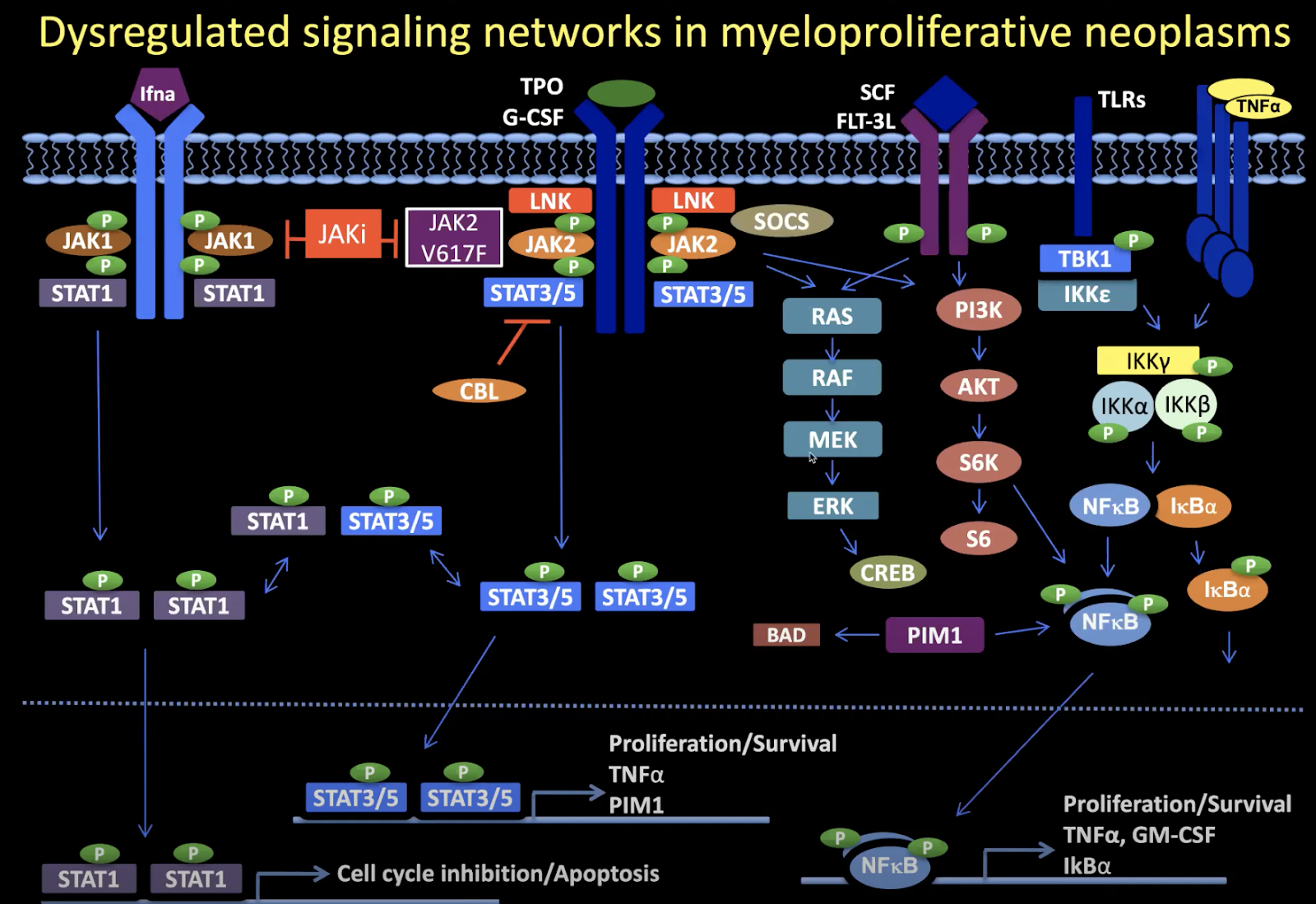
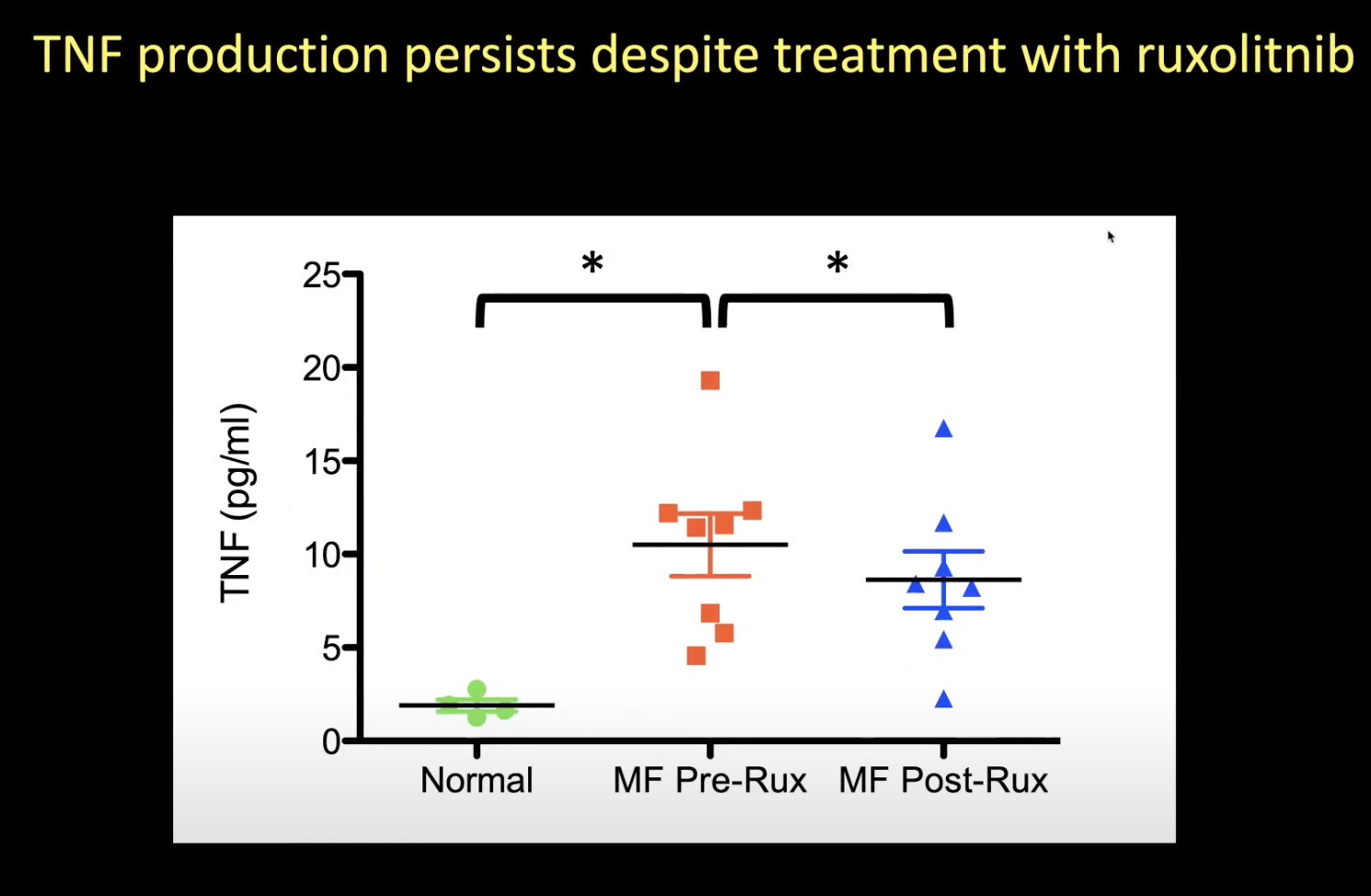
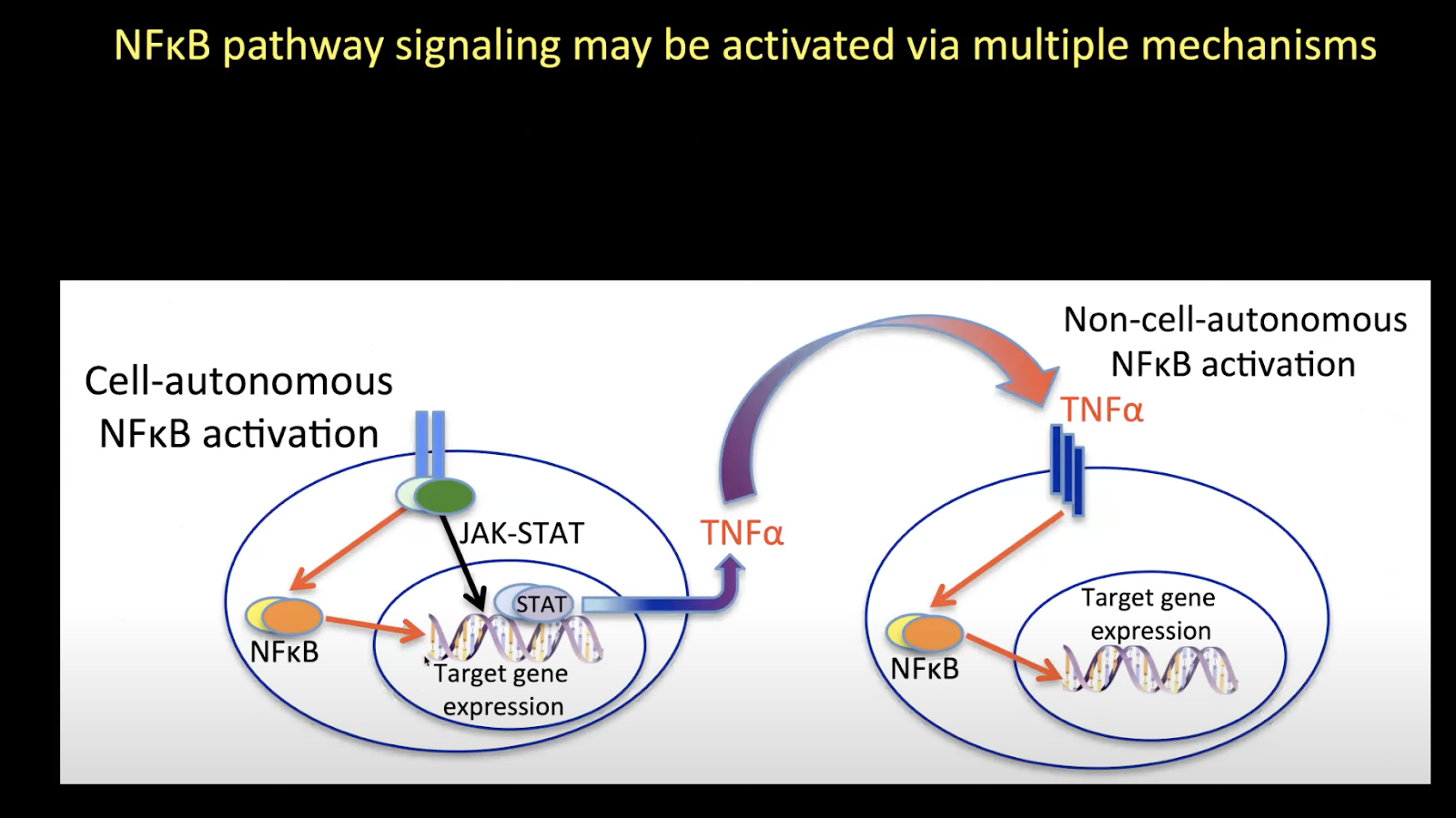
TNFalpha is overproduced in MF. This activates NFKb pathway. Jakafi inhibits JAK2, but it doesn’t reduce TNF-alpha or inhibit NFKb.
Inflammatory Pathophysiology as a Contributor to Myeloproliferative Neoplasms, 2021
Myeloid neoplasms, including acute myeloid leukemia (AML), myeloproliferative neoplasms (MPNs), and myelodysplastic syndromes (MDS), feature clonal dominance and remodeling of the bone marrow niche in a manner that promotes malignant over non-malignant hematopoiesis. This take-over of hematopoiesis by the malignant clone is hypothesized to include hyperactivation of inflammatory signaling and overproduction of inflammatory cytokines. In the Ph-negative MPNs, inflammatory cytokines are considered to be responsible for a highly deleterious pathophysiologic process: the phenotypic transformation of polycythemia vera (PV) or essential thrombocythemia (ET) to secondary myelofibrosis (MF), and the equivalent emergence of primary myelofibrosis (PMF). Bone marrow fibrosis itself is thought to be mediated heavily by the cytokine TGF-β, and possibly other cytokines produced as a result of hyperactivated JAK2 kinase in the malignant clone. MF also features extramedullary hematopoiesis and progression to bone marrow failure, both of which may be mediated in part by responses to cytokines. In MF, elevated levels of individual cytokines in plasma are adverse prognostic indicators: elevated IL-8/CXCL8, in particular, predicts risk of transformation of MF to secondary AML (sAML). Tumor necrosis factor (TNF, also known as TNFα), may underlie malignant clonal dominance, based on results from mouse models. Human PV and ET, as well as MF, harbor overproduction of multiple cytokines, above what is observed in normal aging, which can lead to cellular signaling abnormalities separate from those directly mediated by hyperactivated JAK2 or MPL kinases. Evidence that NFκB pathway signaling is frequently hyperactivated in a pan-hematopoietic pattern in MPNs, including in cells outside the malignant clone, emphasizes that MPNs are pan-hematopoietic diseases, which remodel the bone marrow milieu to favor persistence of the malignancy. Clinical evidence that JAK2 inhibition by ruxolitinib in MF neither reliably reduces malignant clonal burden nor eliminates cytokine elevations, suggests targeting cytokine mediated signaling as a therapeutic strategy, which is being pursued in new clinical trials. Greater knowledge of inflammatory pathophysiology in MPNs can therefore contribute to the development of more effective therapy.
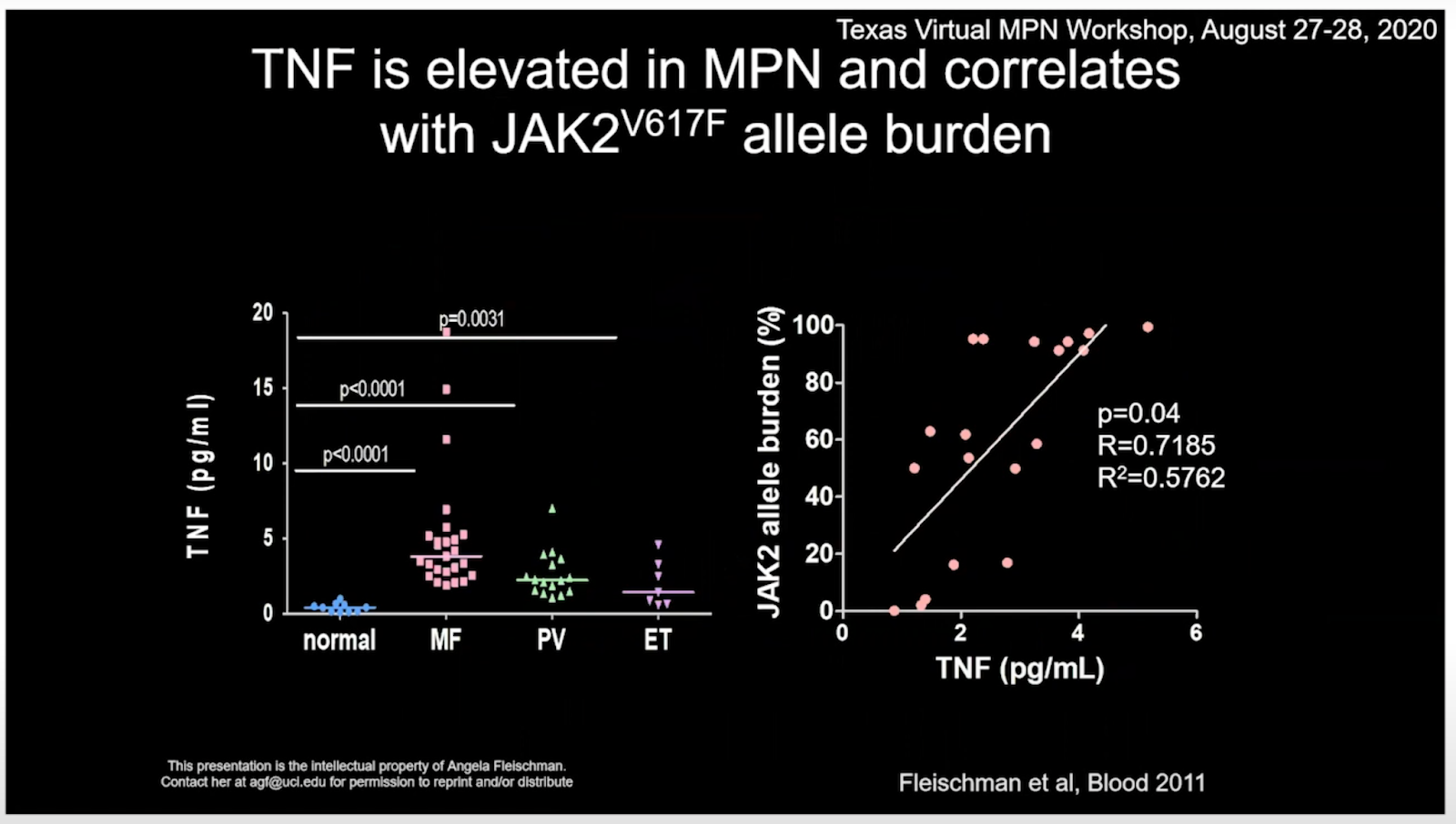
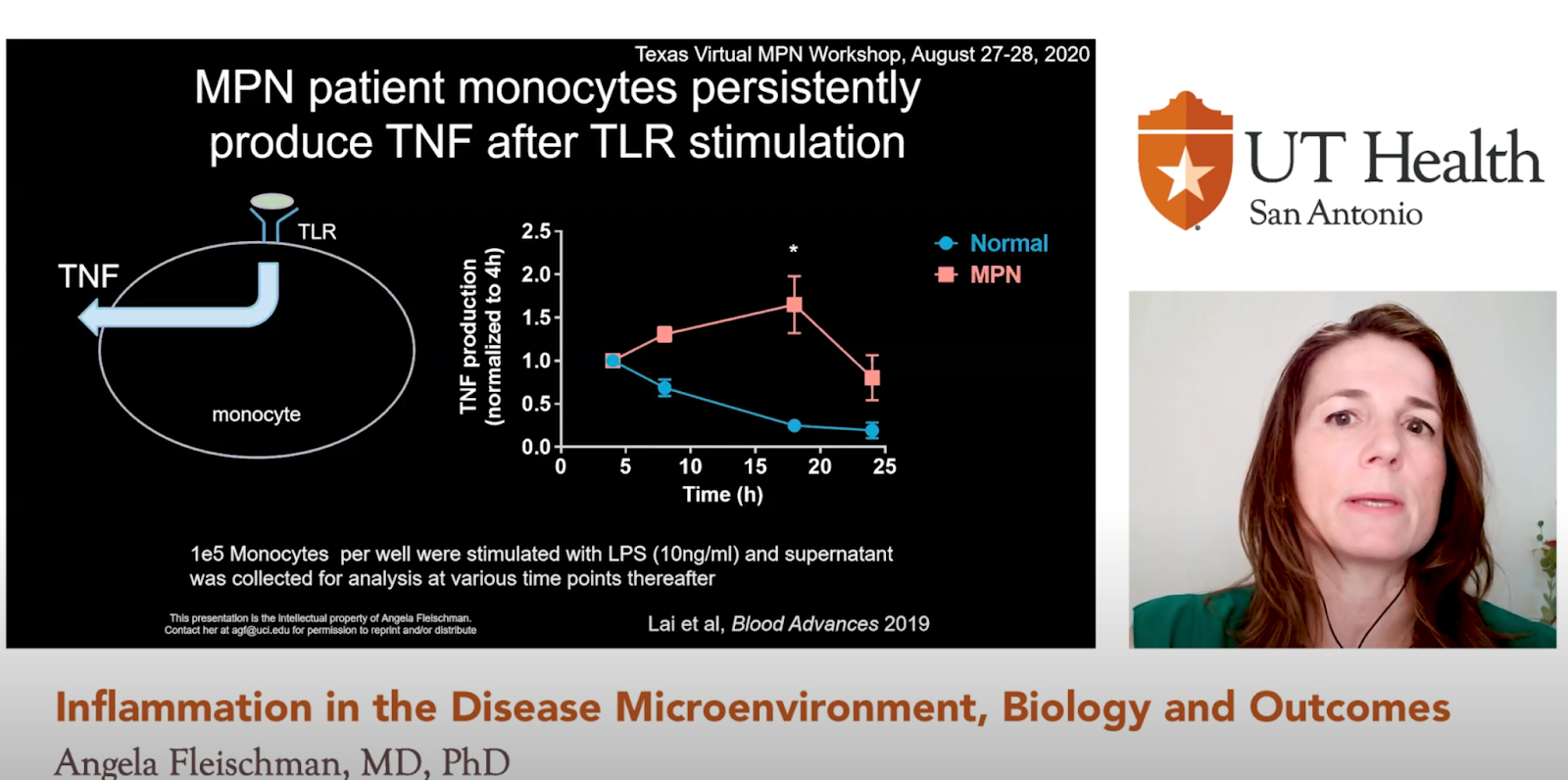
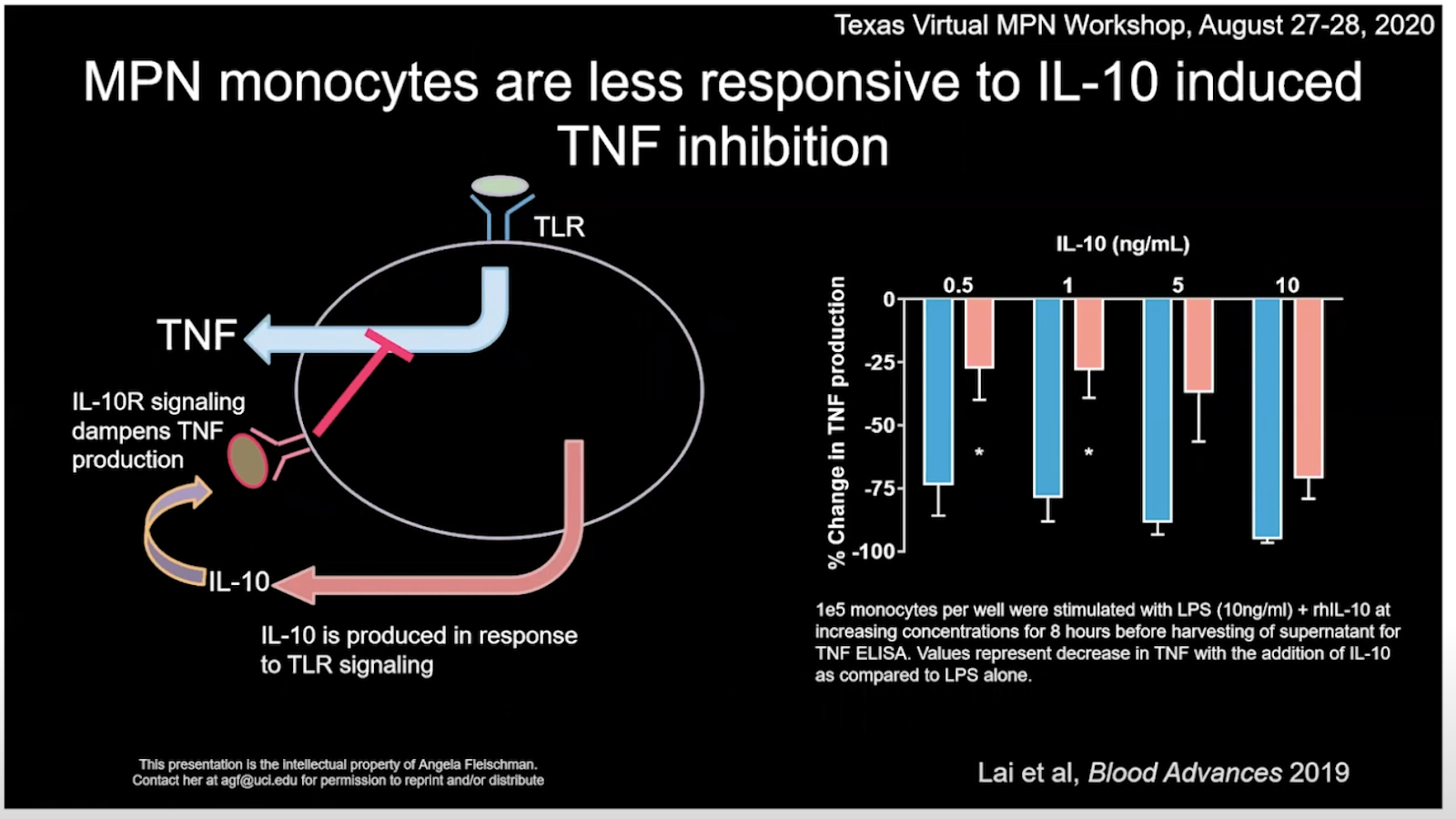
Angela Fleischman, MD, PhD-Chronic Inflammation in MPNs (link)
TNFα facilitates clonal expansion of JAK2V617F positive cells in myeloproliferative neoplasms (link)
Proinflammatory cytokines such as TNFα are elevated in patients with myeloproliferative
neoplasms (MPN), but their contribution to disease pathogenesis is unknown. Here we
reveal a central role for TNFα in promoting clonal dominance of JAK2V617F expressing …
Chronic inflammation: is it the driver or is it paving the road for malignant transformation? (link)
Chronic inflammation in well-defined mouse models such as Giα2 knock out mouse has
been shown to trigger formation and expansion of hypoxic niches and also leads to up
regulation of NFĸB, offering cells which have adapted their genetic machinery to hypoxia a …
The Role of Reactive Oxygen Species in Myelofibrosis and Related Neoplasms, 2015
Reactive oxygen species (ROS) have been implicated in a wide variety of disorders ranging between traumatic, infectious, inflammatory, and malignant diseases. ROS are involved in inflammation-induced oxidative damage to cellular components including regulatory proteins and DNA. Furthermore, ROS have a major role in carcinogenesis and disease progression in the myeloproliferative neoplasms (MPNs), where the malignant clone itself produces excess of ROS thereby creating a vicious self-perpetuating circle in which ROS activate proinflammatory pathways (NF-κB) which in turn create more ROS. Targeting ROS may be a therapeutic option, which could possibly prevent genomic instability and ultimately myelofibrotic and leukemic transformation. In regard to the potent efficacy of the ROS-scavenger N-acetyl-cysteine (NAC) in decreasing ROS levels, it is intriguing to consider if NAC treatment might benefit patients with MPN. The encouraging results from studies in cystic fibrosis, systemic lupus erythematosus, and chronic obstructive pulmonary disease warrant such studies. In addition, the antioxidative potential of the widely used agents, interferon-alpha2, statins, and JAK inhibitors, should be investigated as well. A combinatorial approach using old agents with anticancer properties together with novel JAK1/2 inhibitors may open a new era for patients with MPNs, the outlook not only being “minimal residual disease” and potential cure but also a marked improvement in inflammation-mediated comorbidities.
A case of myelofibrosis controlled, 2017
“Fibrosis” begins with excessive deposition of extracellular matrix. That can evolve to fibrosis/scar tissue & considered cause of most organ failure
It is driven by excessive transforming growth factor beta and can involve genetic and epigenetic factors in the action pathway. The condition can be reversed, if TGF-beta production is decreased.
Initial thought was to treat myelofibrosis as fibrosis problem because of the failure from other therapy
Agents that lower TGF-β
Epigallocatechin gallate (EGCG) - Taurine
Metformin - Berberine
Curcumin - Quercetin
N-acetylcysteine - Lycopene
Silymarin - Glycyrrhiza
Cod liver oil - Ascorbic acid
Boswellic acids - Astaxanthin
Vitamin D - Hesperetin
Caffeine - Hesperidin
Phytolacca - Vitamin B6
References are available on PubMed
Treatment program
From physical signs of malabsorption and the low immune system, patient placed on GFD w/o test
Metformin-ER 500 mg bid – several anti-malignant actions, including in the hematopoietic area, can decrease cell proliferation encouraged by mTOR, and attenuate organ fibrosis
Berberine 500 mg bid - contributes to lowering the mTOR pathway implicated in myelofibrosis.
Quercetin 1000 mg bid – (Note: Transfusion frequency dramatically decreased after replacement by a highly absorbed form [caged molecule by Tesseract], approx. 100% delivery of 105 mg) Quercetin has many anti-cancer mechanisms. Known to lower TGFbeta and reduce fibrosis. Quercetin can inhibit the JAK/STAT cascade of inflammation and cell proliferation
Astaxanthin, 12 mg bid – quenches hydroxyl radical and possibly slows further DNA mutation
Vitamin K2 (15 mg daily as MK4) for sub-skin bleeding, due to platelets of 70
PubMed search - this seems the 1st report controlling myelofibrosis with refractory anemia (other than stem cell transplantation) and by mostly non-Rx agents.
See also link for the full paper.
Surprising results of a supportive integrated therapy in myelofibrosis, 2014
Objectives: Myelofibrosis (MF) is characterized by shortened survival and a greatly compromised quality of life. Weight loss and cachexia seem to be the most important factors influencing survival in patients with MF. The aim of this study was to assess the efficacy of an integrated supportive therapy in improving cachexia and MF-related symptoms.
Methods: We reported on a case of a patient with MF who presented with weight loss and cachexia associated with severe anemia, fatigue, fever, and bone pain. The circulating levels of inflammatory, oxidative stress parameters, hepcidin, and erythropoietin were evaluated and were above normal ranges. The patient was treated with a multitargeted approach specifically developed for cachexia including oral l-carnitine, celecoxib, curcumin, lactoferrin, and subcutaneous recombinant human erythropoietin (EPO)-α.
Results: Surprisingly, after 1 y, cachexia features improved, all MF symptoms were in remission, and inflammatory and oxidative stress parameters, hepcidin, and EPO were reduced.
Conclusions: Because our protocol was targeted at inflammation and the metabolic state, its effectiveness may emphasize the role of inflammation in the pathogenesis of MF symptoms and demonstrates a need for the study of new integrated therapeutic strategies.

Curcumin Downregulates NF-kB and Related Genes in Patients with Multiple Myeloma: Results of a Phase I/II Study, 2007
High dose curcumin inhibiting Stat3 by 69% in blood mononuclear cells.
Long-term stabilisation of myeloma with curcumin, 2017
60 months stabilization of multiple myleloma with 8g/day curcumin (very high dose!)
Oxidative stress is increased in primary and post-polycythemia vera myelofibrosis, 2010
Abstract
Objective: To determine if increased cell turnover in chronic myeloproliferative disorders can lead to hyperhomocysteinemia as a result of folate and/or cobalamin depletion, and contribute to oxidative stress.
Materials and methods: The clinical role of oxidative stress was investigated by measuring reactive oxygen species (ROS), total antioxidant capacity (TAC), and total homocysteine (tHcy), folate, cobalamin, and holotranscobalamin (HoloTC) levels in 51 chronic myeloproliferative disorders patients (male-to-female ratio: 1.1; median age: 64 years; range, 40-84 years), including 42 with primary myelofibrosis and 9 with post-polycythemia vera myelofibrosis.
Results: Myelofibrotic patients had higher tHcy (p = 0.0201) and an unbalanced oxidative status (higher ROS and lower TAC levels; p < 0.0001) than controls. Presence of diabetes or another neoplasia was associated with higher ROS levels (p < 0.05), splenomegaly, hepatomegaly, and peripheral blasts with lower HoloTC levels (p < 0.005). The most severe forms of myelofibrosis (2-3) were associated with lower TAC (p = 0.045) and HoloTC levels (p = 0.017). Patients with Janus kinase-2 mutations had lower HoloTC levels (p = 0.0059). HoloTC deficiency was more frequently associated with Janus kinase-2 homozygosity (p < 0.0003).
Conclusions: Our findings suggest that the determination of HoloTC, tHcy, ROS concentrations, and TAC, can identify latent cobalamin deficiency and provide a rational basis for correcting the increased oxidation associated with disease progression.
The thrombotic events in polycythemia vera patients may be related to increased oxidative stress, 2014
Objective: This study was designed to compare the oxidative stress parameters of patients with polycythemia vera (PV) to those of healthy volunteers and to investigate the probable relationship between vascular events and parameters of oxidative status such as total oxidative status (TOS), total antioxidant status, oxidative stress index (OSI) and malondialdehyde (MDA) in PV patients.
Material and methods: Thirty-five PV patients (20 males and 15 females) and 20 healthy volunteers (11 males and 9 females) were enrolled. The oxidative status parameters of the patients were measured by spectrophotometric analyses at the time of diagnosis and at 6 months after treatment which consisted of phlebotomy and 100 mg/day acetyl salicylic acid with or without hydroxyurea for the high- and low-risk disease group, respectively. These parameters were compared both to healthy controls and to each other, in order to obtain the values before and after treatment. In addition, during diagnosis, the oxidative status parameters of patients with PV and a history of a vascular event were compared with those of patients with no history of a vascular event.
Results: The TOS, OSI and MDA values were significantly higher in the patients than in the control group at the time of diagnosis. At 6 months after phlebotomy and 100 mg/day acetyl salicylic acid therapy, the TOS, OSI and MDA values were significantly lower in the patients when compared to the pretreatment values. The TOS and OSI levels were notably higher in the patients with a vascular-event history than in those without this history.
Conclusion: Oxidative stress parameters were increased in PV patients.
What are the biggest molecules and pathways associated with inflammation?
Inflammation is a complex process that involves a variety of molecules and pathways. Here are some of the biggest molecules and pathways associated with inflammation:
Cytokines: These are small proteins that act as messengers between cells, signaling inflammation and recruiting immune cells to the site of injury or infection. Examples of cytokines involved in inflammation include interleukins, tumor necrosis factor-alpha (TNF-α), and interferons.
Prostaglandins: These are lipid molecules that are involved in various physiological processes, including inflammation. Prostaglandins are produced by the action of cyclooxygenase (COX) enzymes on arachidonic acid, which is released from cell membranes during inflammation. Nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen work by inhibiting COX enzymes and reducing prostaglandin production.
Leukotrienes: These are lipid molecules that are involved in inflammation and are produced by the action of lipoxygenase enzymes on arachidonic acid. Leukotrienes are involved in the recruitment of immune cells to the site of inflammation and the promotion of vascular permeability.
Toll-like receptors (TLRs): These are a family of pattern recognition receptors that recognize specific microbial molecules and activate the immune response. TLRs are involved in the initiation of inflammation and the recruitment of immune cells to the site of infection.
Nuclear factor kappa B (NF-κB) pathway: NF-κB is a transcription factor that is involved in the regulation of immune and inflammatory responses. NF-κB is activated in response to various stimuli, including cytokines and TLR ligands, and activates the expression of genes involved in inflammation.
Janus kinase/signal transducer and activator of transcription (JAK/STAT) pathway: JAK/STAT signaling is involved in the regulation of immune and inflammatory responses. Cytokines such as interferons and interleukins activate JAK/STAT signaling, leading to the activation of inflammatory gene expression.
Overall, inflammation is a complex process involving multiple pathways and molecules. The above are some of the major players in inflammation, but there are many others that are also involved.
Pathogenesis of Myeloproliferative Neoplasms: Role and Mechanisms of Chronic Inflammation (2015)
Myeloproliferative neoplasms (MPNs) are a heterogeneous group of clonal diseases characterized by the excessive and chronic production of mature cells from one or several of the myeloid lineages. Recent advances in the biology of MPNs have greatly facilitated their molecular diagnosis since most patients present with mutation(s) in the JAK2, MPL, or CALR genes. Yet the roles played by these mutations in the pathogenesis and main complications of the different subtypes of MPNs are not fully elucidated. Importantly, chronic inflammation has long been associated with MPN disease and some of the symptoms and complications can be linked to inflammation. Moreover, the JAK inhibitor clinical trials showed that the reduction of symptoms linked to inflammation was beneficial to patients even in the absence of significant decrease in the JAK2-V617F mutant load. These observations suggested that part of the inflammation observed in patients with JAK2-mutated MPNs may not be the consequence of JAK2 mutation. The aim of this paper is to review the different aspects of inflammation in MPNs, the molecular mechanisms involved, the role of specific genetic defects, and the evidence that increased production of certain cytokines depends or not on MPN-associated mutations, and to discuss possible nongenetic causes of inflammation.
2.1. Molecular Pathways Activated in Chronic Inflammation
During inflammation, cytokines are released which signal cells such as T-lymphocytes and monocytes-macrophages to travel to the site of injury. In turn, activated immune cells increase their production of inflammatory cytokines, chemokines, hematopoietic cytokines, and other growth factors, hereby stimulating numerous cell types from their environment (fibroblasts and endothelial cells), which further increases the production of inflammatory cytokines. In this context, the nuclear factor kappa-B (NF-κB) and JAK1/STAT1 pathways are the two main molecular pathways activated to enhance the production of inflammation cytokines [12, 21, 38]. In case of inflammation linked to hypoxia, which may occur after thrombosis or because of cell accumulation, the production of inflammatory cytokines and growth factors by the cells exposed to hypoxia is upregulated via the HIF-1α pathway [39, 40]. As shown in Figure 3, the NF-κB, HIF-1α, and JAK/STAT pathways interact closely. They act in synergy, NF-κB activating the HIF-1α pathway, which in turn leads to increased activation of several signaling pathways, including JAK2/STAT5 (via the production of erythropoietin (EPO)), STAT3 (via inflammation cytokines from the IL-6 family or via EPO, hepatocyte growth factor (HGF), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF)), and STAT1 (via type I and type II inflammatory cytokines) (Figure 4). Moreover, the level of JAK activity affects the expression of transcription factors HIF-1 and HIF-3 [13, 41]. In the context of malignancy, the genetic mutations associated with the tumor may or may not induce the production of inflammation cytokines in mutated cells. This aspect is particularly important in the context of blood cancers since the mutated cells are involved in the immune response or/and are major sources of production of inflammatory cytokines.

Main molecular pathways activated for the production of inflammatory cytokines. Three main transcription factors control the production of inflammatory cytokines and subsequently cell survival and proliferation: (i) HIF-1α, activated in hypoxic tissues, regulates the transcription of multiple genes including numerous inflammatory cytokines and growth factors that promote cell survival, fibrosis, and neoangiogenesis [12, 13]; (ii) NF-κB induces the expression of many inflammation cytokines and growth factors, as well as HIF-1α mRNA; (iii) STAT1, like NF-κB, induces the expression of several inflammation cytokines. To a lesser degree, STAT3 also regulates cytokine transcription, notably of IL-6. STAT1 and STAT3 are activated by JAK kinases, essentially JAK1, but other kinases also activate STAT transcription factors (e.g., MET, the HGF receptor). In addition, cancer-associated mutations may affect the expression (TET2 and IDH1/2 mutations) or signaling (JAK2-V617F, CBL, or LNK mutations) of cytokines or cytokine receptors. Certain growth factors (TGF-β) and other molecules such as liposaccharide (LPS), a component of Gram-negative bacteria, can also activate the NF-κB pathway and subsequently the HIF and JAK/STAT pathways. Red arrows represent pathways that directly lead to increased production of inflammatory cytokines.
Hypoxia-inducible factor 1 (HIF-1) is a new therapeutic target in JAK2V617F-positive myeloproliferative neoplasms, 2019
Targeting NF-κB in hematologic malignancies (2006)
The transcription factor nuclear factor kappa B (NF-κB) can intervene in oncogenesis by virtue of its capacity to regulate the expression of a plethora of genes that modulate apoptosis, and cell survival as well as proliferation, inflammation, tumor metastasis and angiogenesis. Different reports demonstrate the intrinsic activation of NF-κB in lymphoid and myeloid malignancies, including preneoplastic conditions such as myelodysplastic syndromes, underscoring its implication in malignant transformation. Targeting intrinsic NF-κB activation, as well as its upstream and downstream regulators, may hence constitute an additional approach to the oncologist's armamentarium. Several small inhibitors of the NF-κB-activatory kinase IκB kinase, of the proteaseome, or of the DNA binding of NF-κB subunits are under intensive investigation. Currently used cytotoxic agents can induce NF-κB activation as an unwarranted side effect, which confers apoptosis suppression and hence resistance to these drugs. Thus, NF-κB inhibitory molecules may be clinically useful, either as single therapeutic agents or in combination with classical chemotherapeutic agents, for the treatment of hematological malignancies.
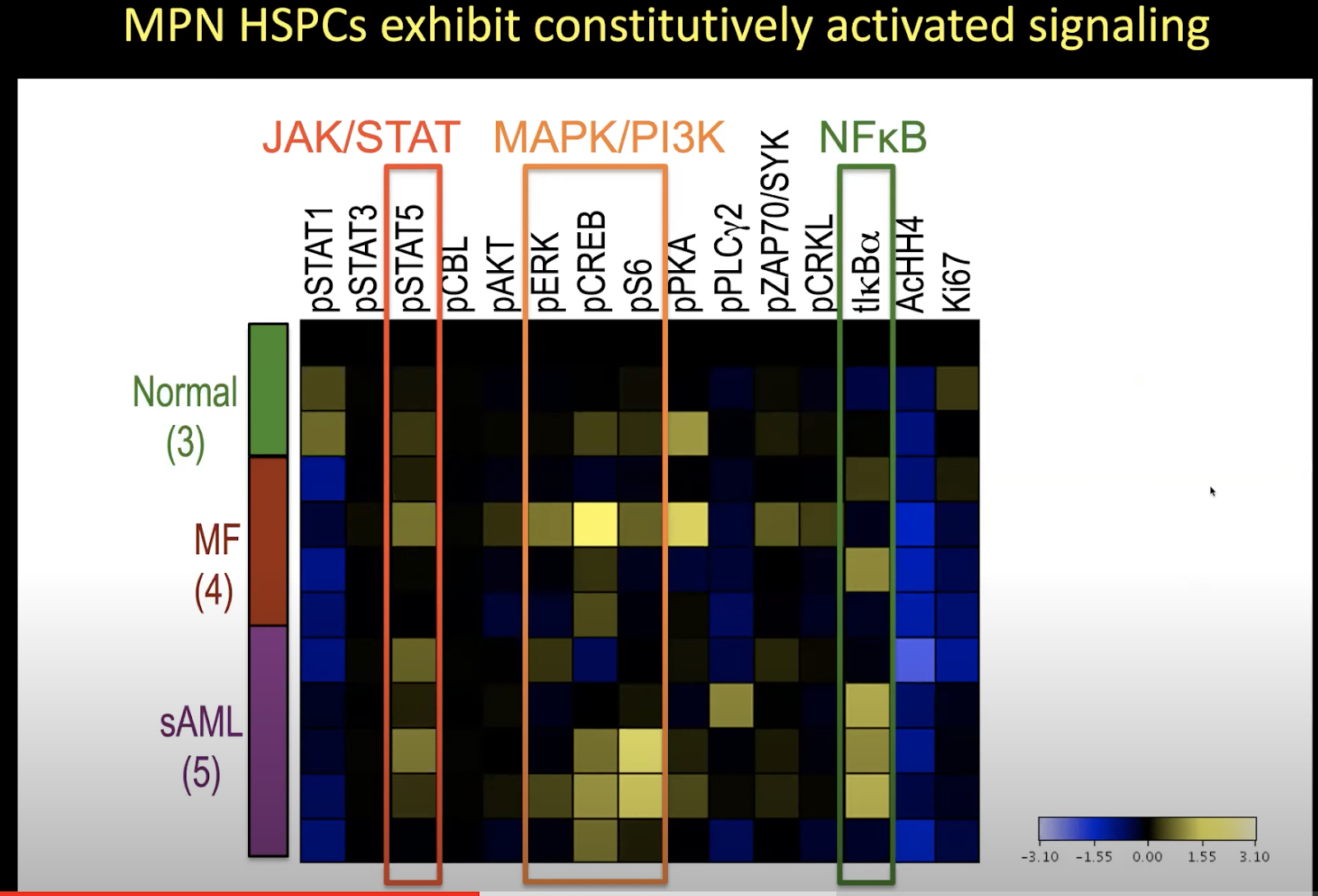
Mass Cytometry Analysis Reveals Hyperactive NF Kappa B Signaling in Myelofibrosis and Secondary Acute Myeloid Leukemia (2017)
Myeloproliferative neoplasms (MPNs) feature a malignant clone containing the JAK2 V617F mutation, or another mutation causing dysregulated JAK2 kinase activity. The multiple disease phenotypes of MPNs, and their tendency to transform phenotypically, suggest pathophysiologic heterogeneities beyond a common phenomenon of JAK2 hyperactivation. JAK2 has the potential to activate multiple other signaling molecules, either directly through downstream effectors, or indirectly through induction of target gene expression. We have interrogated myeloproliferative signaling in myelofibrosis (MF) and secondary acute myeloid leukemia (sAML) patient samples using mass cytometry, which allows the quantitative measurement of multiple signaling molecules simultaneously at the single cell level, in cell populations representing a nearly complete spectrum of hematopoiesis. MF and sAML malignant cells demonstrated a high prevalence of hyperactivation of the JAK-STAT, MAP kinase, PI3 kinase, and NFκB signaling pathways. Constitutive NFκB signaling was evident across MF and sAML patients. A supporting GSEA analysis of MF showed many NFκB target genes to be expressed above normal levels in MF patient CD34+ cells. NFκB inhibition suppressed colony formation from MF CD34+ cells. This study indicates that NFκB signaling contributes to human myeloproliferative disease and is abnormally activated in MF and sAML.
MPN ⇔ Endothelial Cell Connection
Is MPN not confined to your bone marrow?
Emerging research reveals that endothelial cells lining blood vessels can harbor disease-causing mutations thought to originate only in hematopoietic stem cells in myeloproliferative neoplasms (MPNs). A 2009 study first detected the JAK2V617F mutation in liver endothelial cells of two polycythemia vera patients with Budd-Chiari syndrome, suggesting endothelial involvement in a subset of patients. As reviewed by Farina et al. in 2021, subsequent work indicates the mutation likely arises in endothelial progenitor cells that share a common precursor with hematopoietic cells. Beyond their mutant origins, these endothelial cells exhibit a pro-thrombotic phenotype, directly enhancing MPN vascular complications. Additionally, they can promote expansion of mutated hematopoietic cell clones by creating a supportive vascular niche. Though many questions remain regarding their origins and varied roles in MPN heterogeneity, the discovery of mutated endothelial cells provides a new pathogenic mechanism linking vascular dysfunction to hematologic abnormalities in MPNs. Ongoing research aims to further elucidate how these aberrant endothelial cells contribute to thrombosis and inform improved therapeutic strategies.
The presence of JAK2V617F mutation in the liver endothelial cells of patients with Budd-Chiari syndrome (2009)
The possible role of mutated endothelial cells in myeloproliferative neoplasms (2021)

The presence of JAK2V617F mutation in the liver endothelial cells of patients with Budd-Chiari syndrome (2009)
This study by Sozer et al. (2009) found the JAK2V617F mutation in endothelial cells (ECs) lining the hepatic venules in 2 out of 3 patients with Budd-Chiari syndrome (BCS) and polycythemia vera (PV). The mutation was not detected in ECs of the third PV patient or non-PV patients. Using laser capture microdissection and PCR, the authors showed the mutant ECs expressed endothelial markers and not hematopoietic markers. Blood cells from PV patients were positive for JAK2V617F. The authors conclude that ECs are involved in the malignant process in a subset of PV patients, which may relate to thrombotic tendency. Overall the study provides evidence for endothelial involvement by the myeloproliferative neoplasm in some PV patients, suggesting a possible common hemangioblast precursor for endothelial and hematopoietic cells.
The authors of the study do not definitively show how the mutated endothelial cells with JAK2V617F arose in the liver vasculature of the PV patients with Budd-Chiari syndrome. However, they offer some hypotheses:
The mutation originated in a hemangioblast stem cell precursor that gives rise to both hematopoietic and endothelial cell lineages. This would allow the JAK2V617F mutation to be present in both cell types.
The mutation arose in a hematopoietic stem cell and was transferred to endothelial cells via endothelial progenitor cells of myeloid origin that can differentiate into mature endothelial cells.
The endothelial cells acquired the mutation from exposure to circulating JAK2V617F positive hematopoietic cells in the bloodstream of PV patients.
The mutation occurred independently in both hematopoietic and endothelial cell precursors due to a susceptible genetic background.
The variability in endothelial involvement between the PV patients suggests there may be multiple mechanisms leading to JAK2V617F endothelial cells in some patients. More research is needed to further elucidate the origins of the mutated endothelial cells and their implications for PV pathogenesis and thrombosis development. The study provides initial evidence that the mutation can be present in endothelial cells in certain PV patients, adding to our understanding of this heterogeneous disease.
The possible role of mutated endothelial cells in myeloproliferative neoplasms (2021)
Here are the key points and conclusions from the review article by Farina et al. (2021):
Myeloproliferative neoplasms (MPNs) like polycythemia vera, essential thrombocythemia, and primary myelofibrosis are clonal hematopoietic stem cell disorders characterized by overproduction of blood cells and a high risk of vascular complications including thrombosis and bleeding. The mechanisms underlying these vascular events are not fully understood.
Endothelial cells (ECs) line blood vessels and maintain vascular integrity. Evidence suggests EC dysfunction contributes to vascular events in MPNs:
MPN driver mutations like JAK2V617F have been detected in ECs and their progenitors in some MPN patients, suggesting a link between mutated ECs and vascular events.
Mutated ECs may originate from a common precursor cell ("hemangioblast") that gives rise to both ECs and hematopoietic cells during development. This could explain the shared mutations in some patients.
Assays used to study EC biology include detection of circulating endothelial progenitor cells (EPCs) and mature circulating ECs (CECs). Each has limitations in specificity.
Studies indicate JAK2V617F+ ECs have a pro-adhesive, pro-thrombotic phenotype due to increased endothelial P-selectin exposure and degranulation of Weibel-Palade bodies containing P-selectin and von Willebrand factor. This effect is enhanced by inflammation.
JAK2V617F+ ECs promote expansion of mutated hematopoietic cells over normal cells, suggesting they provide a supportive niche.
In mouse models, JAK2V617F expression in ECs alone led to increased thrombosis. Dual expression in ECs and hematopoietic cells caused cardiomyopathy and sudden death.
The evidence suggests mutated ECs play multiple roles in MPN pathogenesis by creating a pro-thrombotic vascular niche and supporting mutant hematopoietic cell growth. More research is needed to fully establish their contribution.
Vascular endothelial cell expression of JAK2V617F is sufficient to promote a pro-thrombotic state due to increased P-selectin expression (2019)
Thrombosis is the main cause of morbidity and mortality in patients with JAK2V617F myeloproliferative neoplasms. Recent studies have reported the presence of JAK2V617F in endothelial cells of some patients with myeloproliferative neoplasms. We investigated the role of endothelial cells that express JAK2V617F in thrombus formation using an in vitro model of human endothelial cells overexpressing JAK2V617F and an in vivo model of mice with endothelial-specific JAK2V617F expression. Interestingly, these mice displayed a higher propensity for thrombus. When deciphering the mechanisms by which JAK2V617F-expressing endothelial cells promote thrombosis, we observed that they have a pro-adhesive phenotype associated with increased endothelial P-selectin exposure, secondary to degranulation of Weibel-Palade bodies. We demonstrated that P-selectin blockade was sufficient to reduce the increased propensity of thrombosis. Moreover, treatment with hydroxyurea also reduced thrombosis and decreased the pathological interaction between leukocytes and JAK2V617F-expressing endothelial cells through direct reduction of endothelial P-selectin expression. Taken together, our data provide evidence that JAK2V617F-expressing endothelial cells promote thrombosis through induction of endothelial P-selectin expression, which can be reversed by hydroxyurea. Our findings increase our understanding of thrombosis in patients with myeloproliferative neoplasms, at least those with JAK2V617F-positive endothelial cells, and highlight a new role for hydroxyurea. This novel finding provides the proof of concept that an acquired genetic mutation can affect the pro-thrombotic nature of endothelial cells, suggesting that other mutations in endothelial cells could be causal in thrombotic disorders of unknown cause, which account for 50% of recurrent venous thromboses.
is there a blood test can measure a metric correlated with the propensity of JAK2+ endothelial cells?
There is currently no definitive blood test that can directly measure the propensity of JAK2-mutated endothelial cells in patients with myeloproliferative neoplasms (MPNs). However, there are some blood markers and tests that may provide indirect evidence of endothelial involvement and dysfunction in MPNs:
Elevated circulating endothelial cells (CECs) - Levels of CECs, which are mature endothelial cells shed from vessel walls, are often elevated in MPN patients. Higher CEC levels may indicate more endothelial cell turnover and damage.
Von Willebrand factor (VWF) - Some studies have found increased VWF levels in MPN patients, which could reflect endothelial cell activation or dysfunction. VWF is stored in Weibel-Palade bodies within endothelial cells.
Thrombomodulin - This endothelial cell membrane protein involved in coagulation may be elevated in the blood of MPN patients in some studies, potentially signaling endothelial injury.
Angiogenic factors like VEGF - Factors promoting angiogenesis can be increased in the blood of MPN patients and may reflect endothelial abnormalities.
Endothelial microparticles - Small particles shed from activated or apoptotic endothelial cells are increased in MPNs and correlate with coagulation abnormalities.
Genetic studies - A few reports have detected JAK2 mutations in endothelial colonies grown from MPN patient blood samples, suggesting the mutation is present in endothelial progenitors.
So in summary, while there is no definitive singular blood test for mutated endothelial cells in MPNs, measures of endothelial cell activation, damage and angiogenesis may provide useful surrogate information about the state of endothelial dysfunction that likely contributes to the thrombotic tendencies of these diseases. More research is still needed in this area.
Increased von Willebrand factor levels in polycythemia vera and phenotypic differences with essential thrombocythemia (2020)
In 48 patients with polycythemia vera (PV), levels of von Willebrand factor antigen (VWF:Ag) and VWF activity (VWF:Act) were significantly higher compared to 48 healthy controls matched for age, sex and blood group.
VWF:Ag and VWF:Act levels in PV patients were predicted independently by JAK2-V617F allelic burden (positively), erythrocyte count (inversely), and male sex.
VWF:Act levels were significantly higher in PV patients with previous thrombosis compared to those without.
The study concludes that increased VWF and Factor VIII levels in PV may contribute to the thrombotic risk and represent potential biomarkers for risk stratification.
The VWF phenotype differs substantially between PV and ET and appears disease specific. Further studies on the mechanisms linking JAK2 mutation, erythrocyte mass, and VWF levels in PV are warranted.
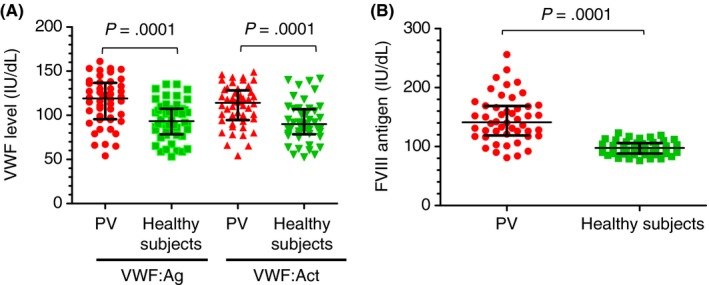
What does it mean to have a higher VWF activity (VWF:Act) level?
Higher VWF:Act levels suggest increased VWF function and activity. This could potentially promote excessive platelet aggregation and adhesion, which may contribute to an increased risk of thrombosis, as suggested by the findings in polycythemia vera patients in this study.
However, VWF:Act levels alone do not provide a complete picture of VWF status or thrombotic risk. Multiple factors regulate VWF activity in vivo. The relationship between VWF:Act and thrombosis risk is complex and needs further research.
Mediterranean diet for MPNs
Mendez et al. explored the feasibility of a Mediterranean diet intervention in patients with MPN in two randomized clinical trials. In the first trial, 75% of participants in the Mediterranean diet (MED) group maintained a MEDAS score of ≥8 throughout the 10-week intervention, indicating successful adoption of the diet with registered dietician (RD) counseling. Approximately half of the MED group experienced a ≥50% reduction in MPN-Total Symptom Score (MPN-TSS) at weeks 9-15, while only 31% in the USDA arm achieved the same reduction at 15 weeks. No significant changes in cytokines or hsCRP were found, and the MPN subtype played a more significant role in microbiome diversity than the diet intervention. In the second trial, participants in the MED group had a 43% chance of achieving a ≥50% reduction in MPN-TSS, compared to 29% in the DASH group. The study concluded that MPN patients can adopt a Mediterranean diet with RD counseling, and a remotely administered intervention is feasible. The Mediterranean diet, which is rich in anti-inflammatory foods, may help manage symptom burden in MPN patients, and the researchers plan to conduct larger randomized studies to further explore its impact.
The Mediterranean diet do’s and don’ts
The Mediterranean diet is a heart-healthy eating plan that emphasizes whole, minimally processed foods, rich in healthy fats, lean proteins, and fiber. It has been associated with numerous health benefits, such as reduced risk of chronic diseases and improved mental health. Here are some general do's and don'ts for following the Mediterranean diet:
Do's:
Prioritize fruits and vegetables: Aim for a colorful variety, as they provide essential vitamins, minerals, and fiber. Aim for at least five servings per day.
Craving sweets? Eat berries in low sugar such as blueberries, blackberries, raspberries and strawberries.
Choose whole grains: Opt for whole grain bread, pasta, rice, and other grains, as they provide more nutrients and fiber than refined grains.
Treat white bread, regular pasta, potatoes as if they’re deserts. Mainly eat whole grains.
Include healthy fats: Focus on monounsaturated and polyunsaturated fats found in olive oil, nuts, seeds, and fatty fish like salmon, mackerel, and sardines.
Minimize foods with saturated fat and pure saturated fats such as butter, cream etc.
Hungry between meals? Consider snacking on portion-controlled nuts.
Eat lean proteins: Incorporate fish, poultry, beans, and legumes as your primary protein sources. Limit red meat to a few times a month.
Make legumes such as beans and lentils a regular part of your diet.
Consume dairy in moderation: Choose low-fat or fat-free options for yogurt, cheese, and milk.
Use herbs and spices: Flavor your food with fresh herbs and spices instead of relying on salt for taste.
Enjoy moderate amounts of red wine (optional): If you drink alcohol, a moderate consumption of red wine (up to one glass per day for women, two for men) is allowed.
Stay physically active: Regular exercise complements the Mediterranean diet and supports overall health.
Don'ts:
Don't consume excessive amounts of red and processed meat: These can be high in unhealthy fats and are associated with increased risk of chronic diseases.
Don't rely on processed and refined foods: Limit consumption of sugary beverages, snacks, and pastries, as they often contain added sugars, unhealthy fats, and excess sodium.
Don't use unhealthy fats: Avoid trans fats found in some margarines, fried foods, and packaged snacks.
Don't overindulge in alcohol: Stick to the recommended guidelines or avoid alcohol entirely if you have a history of alcohol abuse or certain medical conditions.
Remember, the Mediterranean diet is more than just a list of do's and don'ts; it's a lifestyle that encourages enjoying meals with family and friends, being mindful of portion sizes, and staying active. Always consult with a healthcare professional before making significant changes to your diet.
The Mediterranean Diet Checklist (aim for MEDAS score ≥ 8)

Source: Wikipedia
Mediterranean diet macros (ref):
Fats – 35% to 40% (61 grams)
Carbohydrates – 50% (195 grams)
Proteins – 15% to 20% (59 grams)
Fibre – 32 grams
Calories – 1,527 kcal
Saturated fats – less than 10%
Sugars – 20%
Food ideas:
Chipotle salad with beans + chicken + salsa without cheese and cream
Bibibimbop with brown rice
Tuna sandwich from Jersey Mike’s
Veggie pattie from Subway
Lentil dish at home
Mixed veggies at home + low fat yogurt
Salad at home + sardines
MPN SAF TSS (ref, 2012)
Anyone can use this questionnaire to track how well they’re doing with MPN symptoms and track this score over time.
Prognosis with MPNs
Normal life expectancy for polycythemia vera (PV) patients is possible, 2021
We obtained demographics and survival data of adult PV pts from our Weill Cornell Medicine (WCM) Research Database Repository (PV-WCM) diagnosed from 1974-2020 as previously described (Abu-Zeinah et al. Leukemia 2021); and from the National Cancer Institute's Surveillance, Epidemiology and End Results (SEER) Program, 2001-2017. PV-WCM thrombosis and MF progression data were available.
Results: We identified 470 PV-WCM and 16,492 PV pts from SEER. The median OS of the PV-WCM cohort and the SEER population was 26.6 and 12.8 years, respectively, but the groups differed by age and sex (Fig 1A). PV-WCM and matched PV-SEER, however, were well balanced by age, sex, and race (standardized mean difference <0.1). The median OS of PV-WCM was 10.8 years longer than PV-SEER (p<0.001, Fig 1B). MVA confirmed 65% lower mortality in the PV-WCM group relative to the PV-SEER population (p<0.001, Fig 1C). PV-SEER OS was shorter than actuarial OS of the US population (mortality HR 2.47, p<0.001), whereas PV-WCM OS was not significantly different than expected (mortality HR 1.15, p=0.136). Excess late mortality was observed in PV-WCM after 17 years, potentially due to increased incidence of MF progression, affecting almost 50% of PV pts after 25 years (Fig 1D).
PV-WCM pts treated with rIFNα (n=137), previously shown to have improved MF-free survival and OS (Abu-Zeinah et al. Leukemia 2021), had an OS similar to the matched US population (p=0.33, Fig 1F); whereas pts not treated with rIFNα had modestly shortened OS (HR 1.26, p=0.03). Because PV progression is among the leading causes of late morbidity and mortality, and available therapy can mitigate this, it may be time to reconsider and improve upon PV risk stratification and treatment.
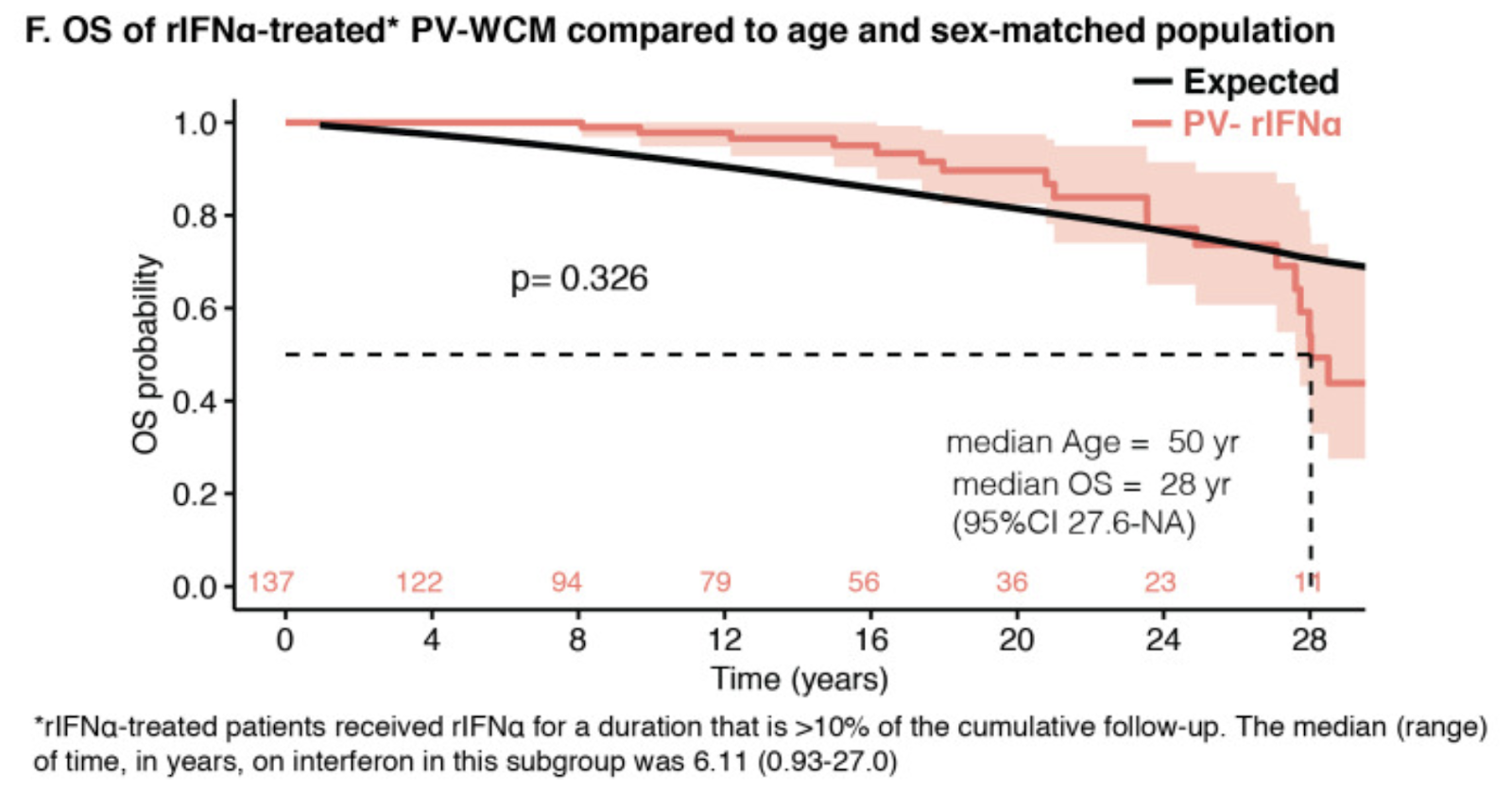
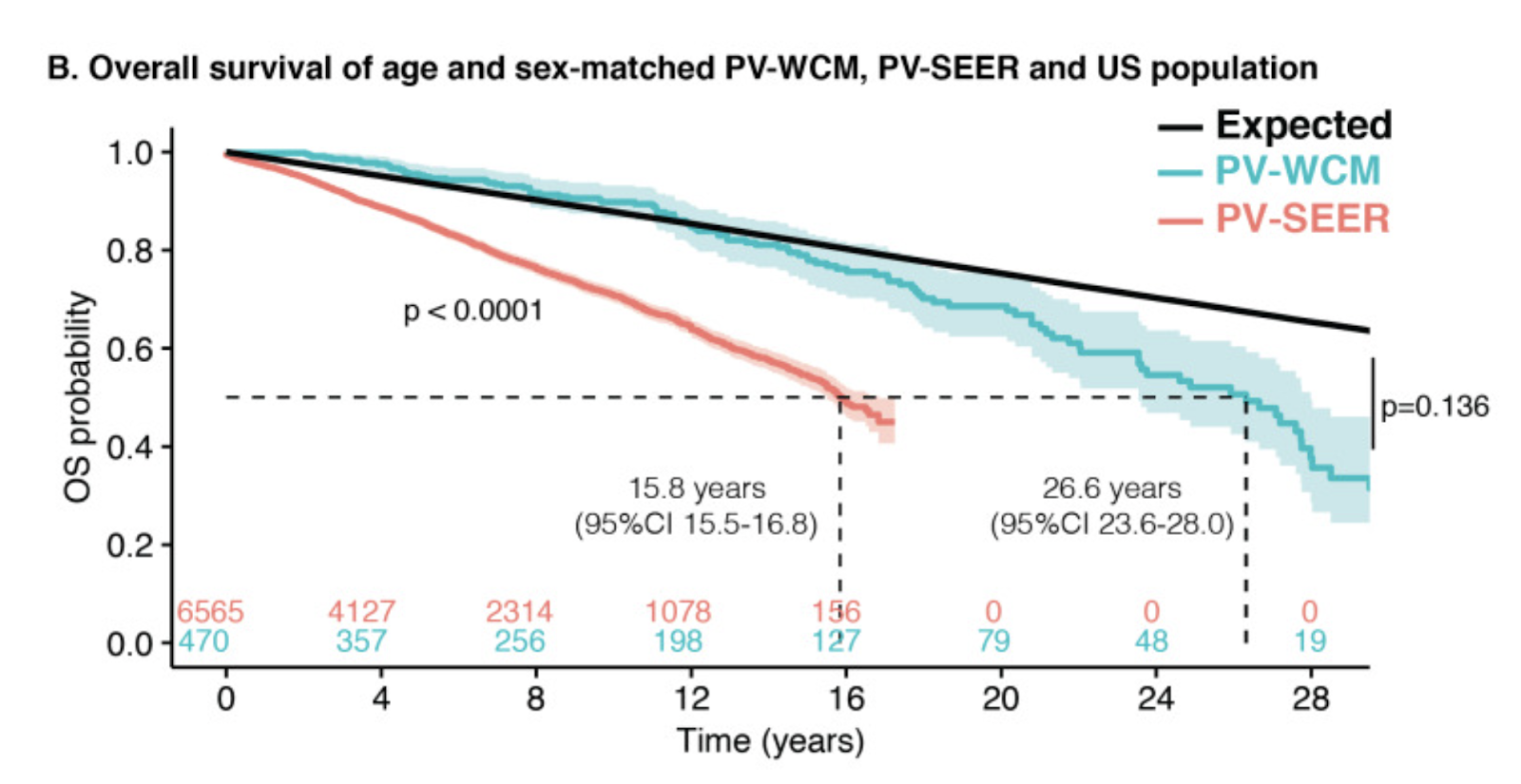
3023 Mayo Clinic Patients With Myeloproliferative Neoplasms: Risk-Stratified Comparison of Survival and Outcomes Data Among Disease Subgroups (2019)
Objective: To document the Mayo Clinic decades-long experience with myeloproliferative neoplasms (MPNs) and provide mature risk-stratified survival data and disease complication estimates.
Patients and methods: All Mayo Clinic patients with World Health Organization-defined MPNs constituted the core study group and included those with polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF).
Results: A total of 3023 consecutive patients (median age, 62 years; range, 18-96 years) were considered: 665 PV, 1076 ET, and 1282 PMF. From October 27, 1967, through December 29, 2017, 1631 deaths (54%), 183 leukemic transformations (6%), 244 fibrotic progressions (14%), and 516 thrombotic events (17%) were recorded. Median overall survival (OS) was 18 years for ET, 15 years for PV, and 4.4 years for PMF (P<.05 for all intergroup comparisons). Inferior survival was documented in patients with ET diagnosed more recently (post-1990) (P<.001), whereas survival data were time independent in PV and PMF. After conventional risk stratification, OS in low-risk ET and low-risk PV were superimposed (P=.89) but each differed significantly from that of age- and sex-matched controls (P<.001). Leukemia-free survival was similar for ET and PV (P=.22) and significantly worse with PMF (P<.001). Compared with ET, PV was associated with higher risk of fibrotic progression (P<.001). Thrombosis risk after diagnosis was highest in PV and lowest in PMF (P=.002 for PV vs ET; P=.56 for ET vs PMF; and P=.001 for PV vs PMF).
Conclusion: This study provides the most mature survival and outcomes data in MPNs and highlights MPN subgroup risk categorization as key in appraising disease natural history. The OS was only marginally better in ET compared with PV, and PV displayed a higher risk of thrombosis and fibrotic progression.
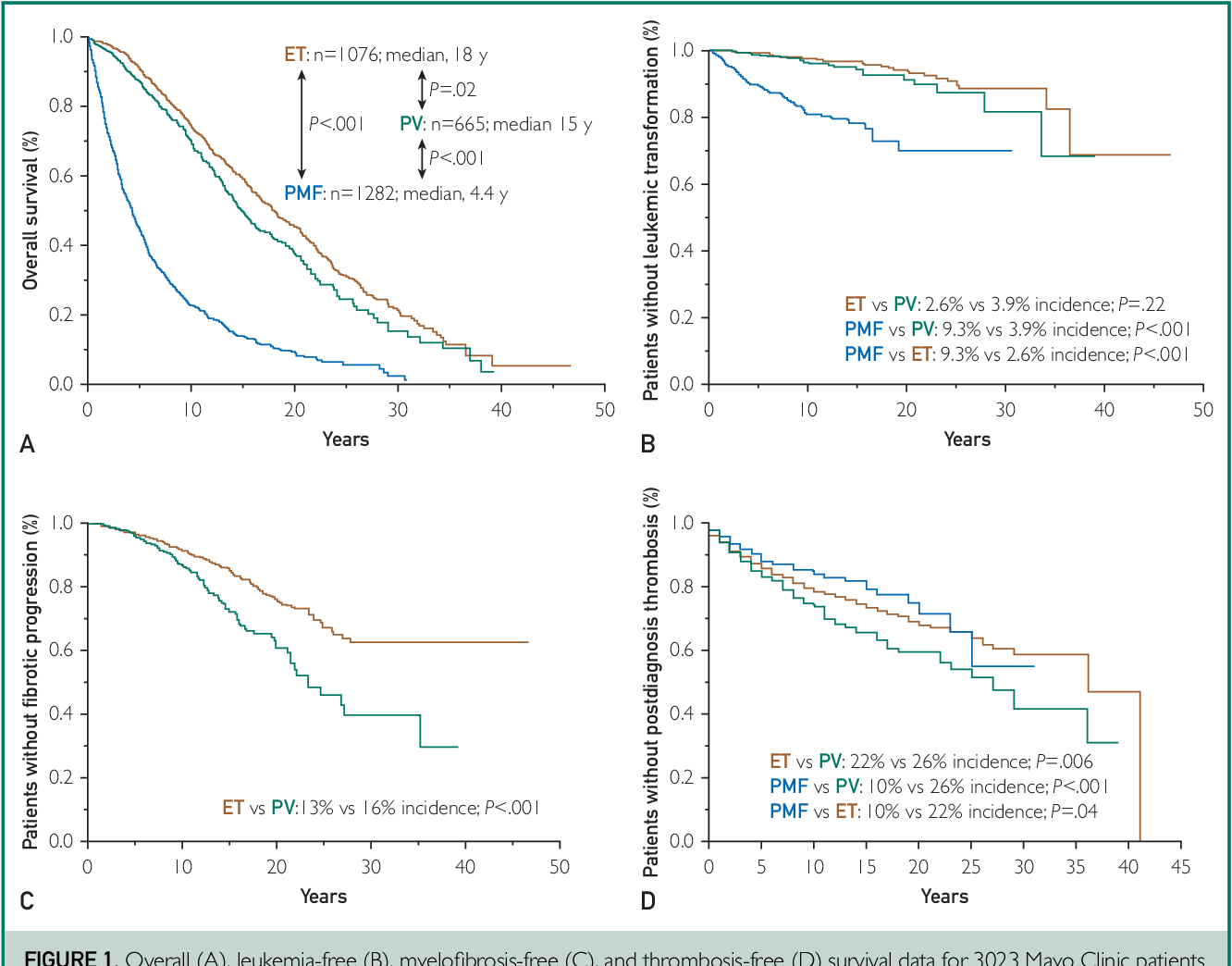
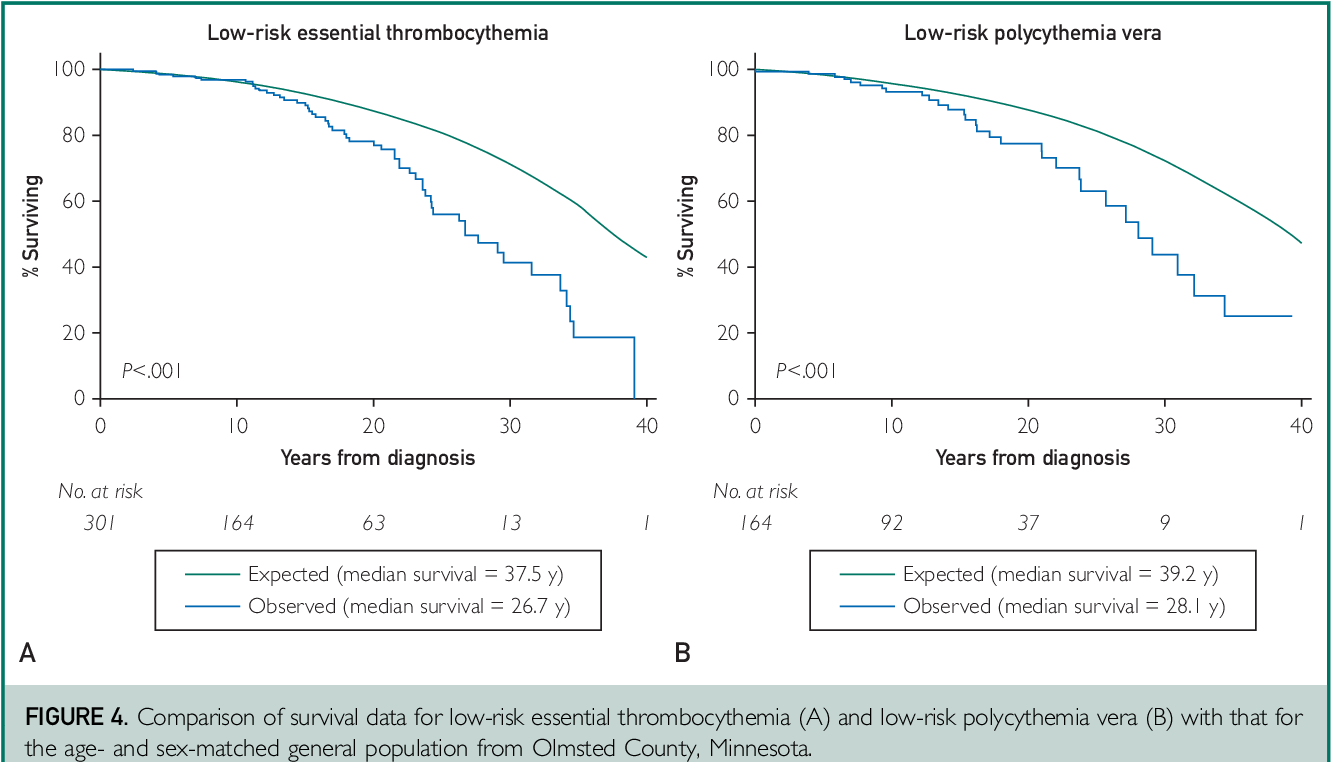

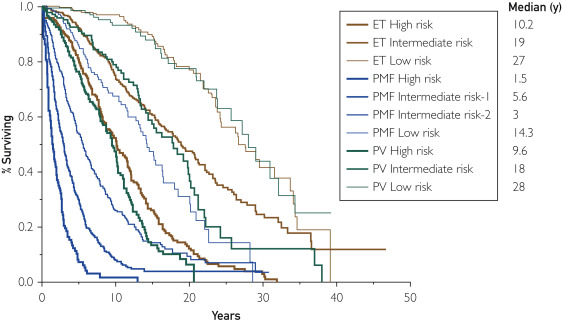
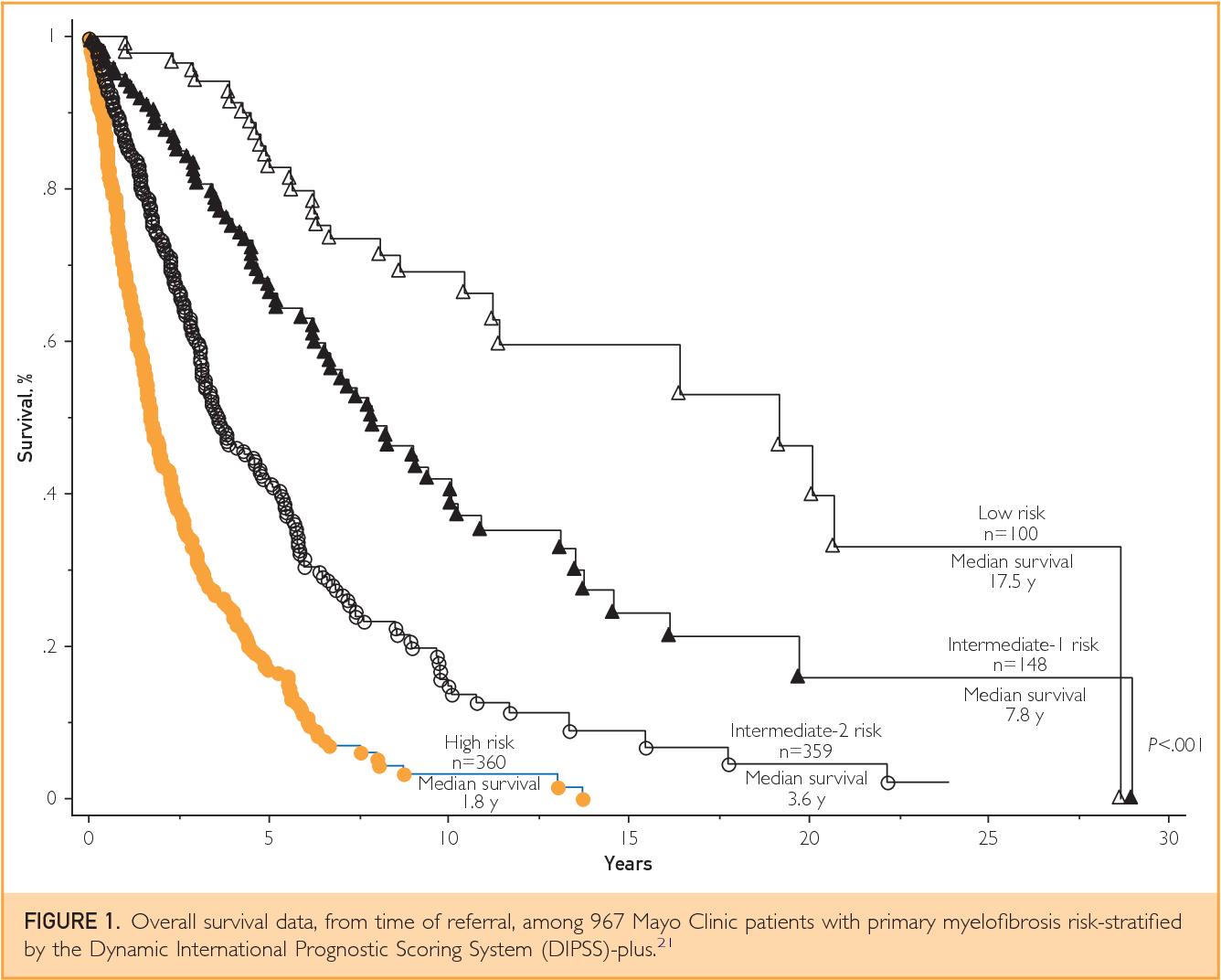
Updates in the management of polycythemia vera and essential thrombocythemia (2019)
Updates in Prognostication
In a large PV cohort (Tefferi et al, 2013), overall median survival was 18.9 years. When restricted to patients with mature data, it was 14.1 years. Older age, leukocytosis, thrombosis, abnormal karyotype predicted worse survival. A prognostic model using these was developed.
An Italian ET study (Passamonti et al, 2004) found no impact on survival vs general population. Thrombosis history and male sex predicted death.
At Mayo Clinic (Tefferi et al, 2014), PV median survival was 13.5 years, ET 19.8 years. Driver mutation status did not impact survival. PV had higher myelofibrosis progression risk.
The IPSET model for ET incorporates age, thrombosis history, leukocytosis into prognostic model predicting survival (Passamonti et al, 2012).
Molecularly annotated patients at Mayo Clinic (Tefferi et al, 2016) had mutations in >50% beyond driver mutations. Some mutations were "adverse" for survival.
The MIPSS models incorporate clinical factors and mutation data into prognostic systems for PV and ET (Tefferi et al, 2018).
A large European study (Grinfeld et al, 2018) sequenced 2035 MPN patients and identified 8 genomic subgroups with a personalized prognostic model.
Updates in Thrombosis Risk Stratification
In PV, age >60 years and thrombosis history remain basis of stratification. Patients with either are "high risk."
In ET, driver mutation status contributes. Four risk categories per IPSET-thrombosis: very low, low, intermediate, high (Barbui et al, 2015).
CALR-mutated ET patients have lower thrombotic risk. Mutation status doesn't modify IPSET model (Finazzi et al, 2014).
Growing data suggest leukocytosis increases thrombosis risk in both PV and ET:
Subanalyses of CYTO-PV data showed increased thrombosis risk above certain leukocyte thresholds (Barbui et al, 2015).
Similar findings in a US Veterans Affairs PV cohort (Parasuraman et al, 2018).
ECLAP study found leukocytosis significantly increased thrombosis risk in PV (Landolfi et al, 2007).
PT-1 study associated abnormal leukocyte counts over time with thrombosis and bleeding in ET (Campbell et al, 2012).
Conclusion
Recent approval of ruxolitinib and upcoming European approval of ropeginterferon alfa-2b represent important advances in PV treatment.
Growing awareness of leukocytosis impact on outcomes may influence clinical practice.
Symptom burden is increasingly recognized as underappreciated, especially in ET, and may spur research.
New agents are needed to modify underlying disease biology and prevent progression to advanced phases.
Treatments for PV & MPN
Interferon-alpha for MPNs (Pegasys / Besremi)
BACKGROUND ON MPNs:
Healthy hematopoietic stem cells are essential for maintaining a robust immune system and overall well-being. These stem cells give rise to various blood cells, including red blood cells, white blood cells, and platelets, which contribute to efficient oxygen transport, protection against infections and malignancies, and proper blood clotting and tissue repair (2020).
In myeloproliferative neoplasms (MPNs), JAK2-pathway overactivation results in the proliferation of an abnormal clone that dominates the bone marrow, outcompeting healthy hematopoietic stem cells.
The hyperactivation of JAK2 and excessive production of inflammatory cytokines by MPN cells contribute to chronic inflammation (2021).
As the cancerous mass increases, the likelihood of acquiring additional mutations also rises, further promoting the disease's progression and exacerbating the decline in healthy stem cell function (2010).
MPNs can be recognized as a disease of accelerated aging through the loss of stem cell function (2013) and chronic inflammation that causes damage to tissues, promote cellular senescence, and impair the function of other organ systems (2022).
HOW TO DEAL WITH MPNs?
These strategies emerge from our understanding of basic biology of MPNs:
Minimize the tumor mass to minimize the chances of progression and the chronic inflammation that comes with a large tumor mass.
Maintain a healthy stem cell function for as long as possible to minimize the effects of accelerated aging.
Interferon-alpha (INF-alpha) is an immunomodulatory and antiviral drug with both anti-tumor and anti-inflammatory properties (2013):
Enhances the immune response: INF-alpha activates the immune system and boosts the body's natural defenses, enabling it to better recognize and eliminate cancer cells or viral infections.
Inhibits viral replication: INF-alpha has antiviral properties, effectively reducing viral replication in infected cells, and helping to control and clear viral infections.
Modulates cell growth and differentiation: INF-alpha can influence the growth and differentiation of various cell types, including MPN cells, potentially inhibiting their proliferation and promoting apoptosis (programmed cell death).
Interferon-alpha is effective in patients with Polycythemia Vera (PV) and other MPNs with deep and durable responses (2011, 2015, 2010):
INF-alpha maintains a healthy stem cell function as long as possible by minimizing the MPN cancer clone in hematopoietic niche.
By normalizing elevated leukocyte and platelet counts, INF-alpha helps minimize the sustained release of inflammatory cytokines and chemokines and concurrently improves immune cell function which is important for intact tumor immune surveillance (2021).
Hydroxyurea is typically used as first-line cytoreduction in MPN patients. Although no difference has been found in secondary cancer rates between interferon and hydroxyurea [66], there are still concerns for hydroxyurea’s long-term effects [44, 67, 68]. Interferon’s potential for durable responses and disease modification makes it a more appealing choice for younger patients given that treatment can last for decades (2020).
INTERFERON-ALPHA for PV:
The 5-year CONT-PV study showed the effectiveness of ropeginterferon alfa-2b in reducing symptoms in patients with high-risk polycythemia vera (PV), showing that only 15.7% of patients reported symptoms by the sixth year compared to 20.7% in the control group, and only 18.6% required phlebotomy compared to 40% in the control group; it also demonstrated significantly lower disease progression or thromboembolic events (5.3% versus 16.2%) and a higher reduction in JAK2V617F allele burden (20.7% achieved less than 1% compared to 1.4% in the control group), suggesting improved quality of life and potential to reduce myelofibrosis risk.
Interferon-alfa treatment significantly improved myelofibrosis-free survival (27 years) and overall survival (28 years) compared to hydroxyurea (18 and 26 years) and phlebotomy-only (14 and 25 years) in patients with polycythemia vera, supporting its earlier use in treatment plans, even for younger, low-risk patients, according to a retrospective study presented in 2019.
A 2021 Weill Cornell retrospective study of 470 polycythemia vera (PV) patients found that treatment with Interferon-alpha (rIFNα) improved myelofibrosis-free survival (MFS) and overall survival (OS) rates in both low and high-risk patients compared to hydroxyurea (HU) and phlebotomy-only (PHL-O).
Normal life expectancy for polycythemia vera (PV) patients is possible with interferon-alpha treatment (2021); the study found a 65% lower mortality rate in the Weill Cornell Medicine (WCM) cohort compared to a national-database population, and PV-WCM patients treated with rIFNα had similar overall survival to the matched healthy US population.
A 2017 prospective clinical trial involving 58 patients with ET and PV found that long-term therapy with peg-interferon α-2a could normalize bone marrow morphology and reverse bone marrow fibrosis after a median of 7 yrs of therapy. 50% of patients experienced a bone marrow response with 22% achieving Complete Bone Marrow Response (BM-CR) and 28% achieving partial bone marrow response (BM-PR). BM response took on average 4 yrs with BM improvement continuing all the way to 6 yrs of therapy in some patients.
A 2020 study analyzed the kinetics of JAK2V617F allele burden in 66 interferon-alpha2 (IFN) treated patients and 6 untreated patients with essential thrombocythemia and polycythemia vera, finding that without IFN treatment, the JAK2V617F allele burden doubled every 1.4 years, while IFN treatment reduced the burden with half-lives of 1.6 years indicating the importance of early intervention.
Pegylated interferon has improved tolerability compared to standard interferon but still has a significant side effect profile, with discontinuation rates of 15-20% in clinical trials.
Combination therapy of interferon with JAK2 inhibitors, such as ruxolitinib, may improve tolerability and enhance interferon signaling, with Phase II COMBI and RUXOPEG trials showing rapid decreases in spleen size, JAK2 V617F allele burden, and improvement in hematologic parameters.
Interferon-alpha for treating polycythemia vera yields improved myelofibrosis-free and overall survival, 2021
Interferon-alpha (rIFNα) is the only disease-modifying treatment for polycythemia vera (PV), but whether or not it prolongs survival is unknown. This large single center retrospective study of 470 PV patients compares the myelofibrosis-free survival (MFS) and overall survival (OS) with rIFNα to two other primary treatments, hydroxyurea (HU) and phlebotomy-only (PHL-O). The median age at diagnosis was 54 years (range 20–94) and the median follow-up was 10 years (range 0–45). Two hundred and twenty-nine patients were women (49%) and 208 were high-risk (44%). The primary treatment was rIFNα in 93 (20%), HU in 189 (40%), PHL-O in 133 (28%) and other cytoreductive drugs in 55 (12%). The treatment groups differed by ELN risk score (p < 0.001). In low-risk patients, 20-year MFS for rIFNα, HU, and PHL-O was 84%, 65% and 55% respectively (p < 0.001) and 20-year OS was 100%, 85% and 80% respectively (p = 0.44). In high-risk patients, 20-year MFS for rIFNα, HU, and PHL-O was 89%, 41% and 36% respectively (p = 0.19) and 20-year OS was 66%, 40%, 14% respectively (p = 0.016). In multivariable analysis, longer time on rIFNα was associated with a lower risk of myelofibrosis (HR: 0.91, p < 0.001) and lower mortality (HR: 0.94, p = 0.012). In conclusion, this study supports treatment of PV with rIFNα to prevent myelofibrosis and potentially prolong survival.
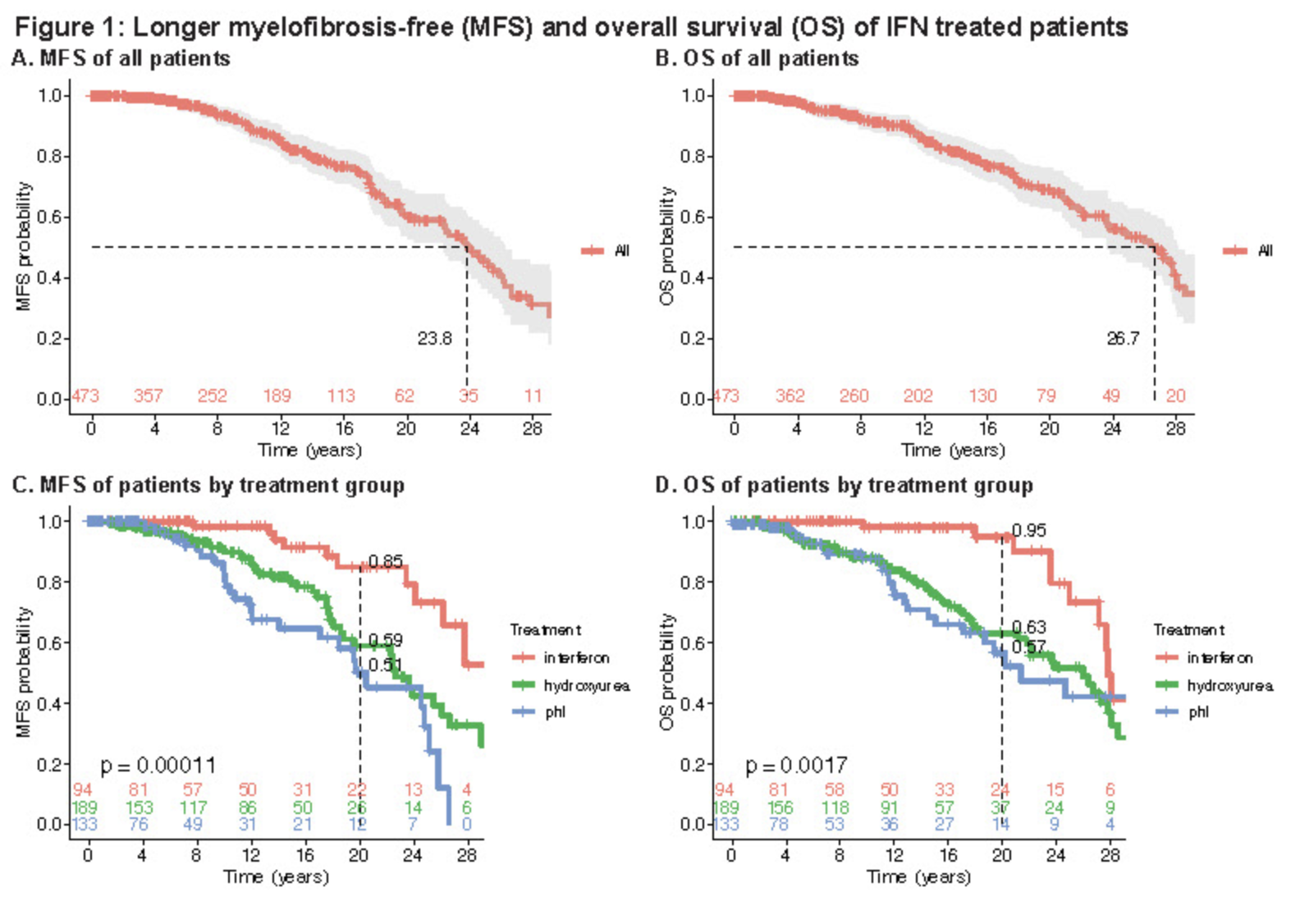
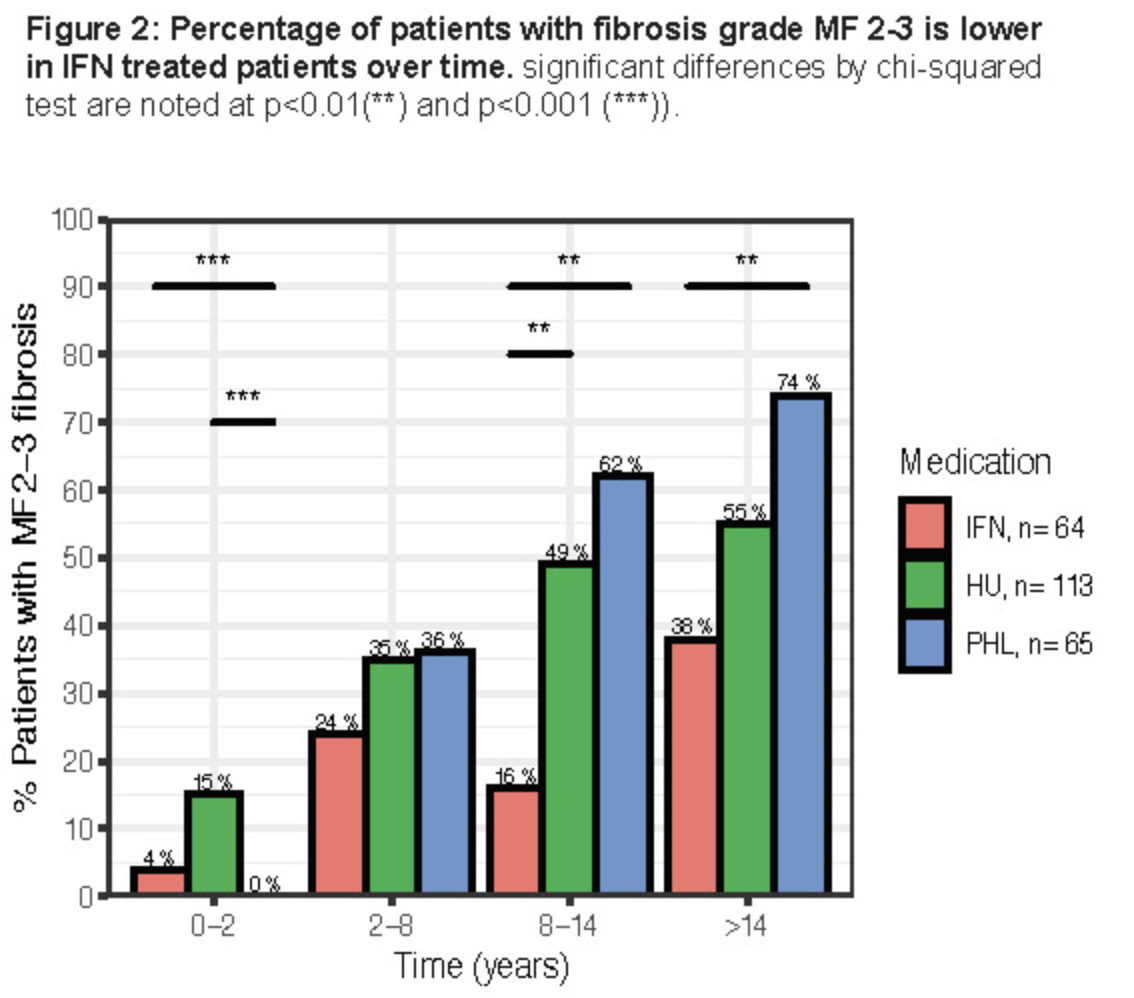
5-year results from the PROUD-PV and CONTINUATION-PV studies (link)
This analysis included all patients enrolled in the CONTINUATION-PV (NCT02218047) study:
89.6% of patients (n = 95) treated with ropeginterferon alfa-2b in the PROUD-PV study entered in the CONTINUATION-PV extension study, and 73.7% of these patients (n = 70) continued their treatment until Month 60
Similarly, 68.5% of patients (n = 76) treated with hydroxyurea in the PROUD-PV study enrolled in the CONTINUATION-PV extension study to receive best available treatment, where 88% of these were treated with hydroxyurea and 75% (n = 57) were treated up to Month 60
Complete hematologic response (CHR, defined as hematocrit [HCT] < 45% and no phlebotomy for at least 3 months, platelets < 400 × 109/L, and white blood cells < 10 × 109/L) is reported in Table 3 (LOCF).


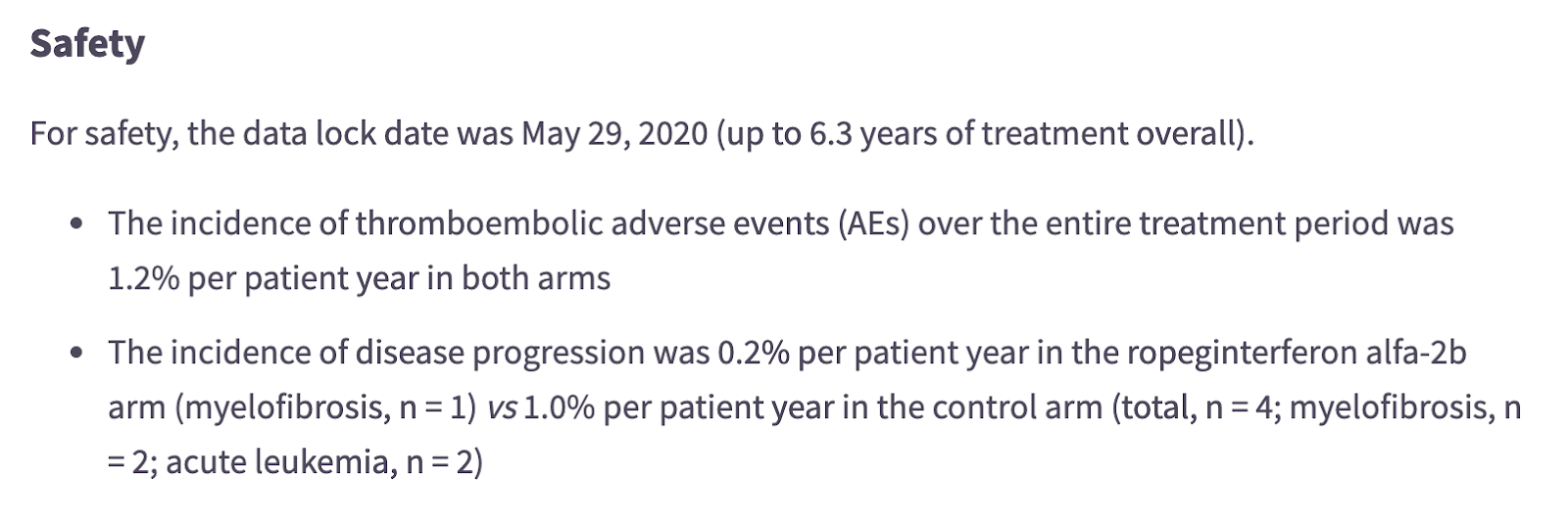
Normal life expectancy for polycythemia vera (PV) patients is possible, 2021
We obtained demographics and survival data of adult PV pts from our Weill Cornell Medicine (WCM) Research Database Repository (PV-WCM) diagnosed from 1974-2020 as previously described (Abu-Zeinah et al. Leukemia 2021); and from the National Cancer Institute's Surveillance, Epidemiology and End Results (SEER) Program, 2001-2017. PV-WCM thrombosis and MF progression data were available.
Results: We identified 470 PV-WCM and 16,492 PV pts from SEER. The median OS of the PV-WCM cohort and the SEER population was 26.6 and 12.8 years, respectively, but the groups differed by age and sex (Fig 1A). PV-WCM and matched PV-SEER, however, were well balanced by age, sex, and race (standardized mean difference <0.1). The median OS of PV-WCM was 10.8 years longer than PV-SEER (p<0.001, Fig 1B). MVA confirmed 65% lower mortality in the PV-WCM group relative to the PV-SEER population (p<0.001, Fig 1C). PV-SEER OS was shorter than actuarial OS of the US population (mortality HR 2.47, p<0.001), whereas PV-WCM OS was not significantly different than expected (mortality HR 1.15, p=0.136). Excess late mortality was observed in PV-WCM after 17 years, potentially due to increased incidence of MF progression, affecting almost 50% of PV pts after 25 years (Fig 1D).
PV-WCM pts treated with rIFNα (n=137), previously shown to have improved MF-free survival and OS (Abu-Zeinah et al. Leukemia 2021), had an OS similar to the matched US population (p=0.33, Fig 1F); whereas pts not treated with rIFNα had modestly shortened OS (HR 1.26, p=0.03). Because PV progression is among the leading causes of late morbidity and mortality, and available therapy can mitigate this, it may be time to reconsider and improve upon PV risk stratification and treatment.
Managing Polycythemia Vera in 2021 - Dr. Richard T. Silver
https://www.youtube.com/watch?v=Qi1MSJjTxgk
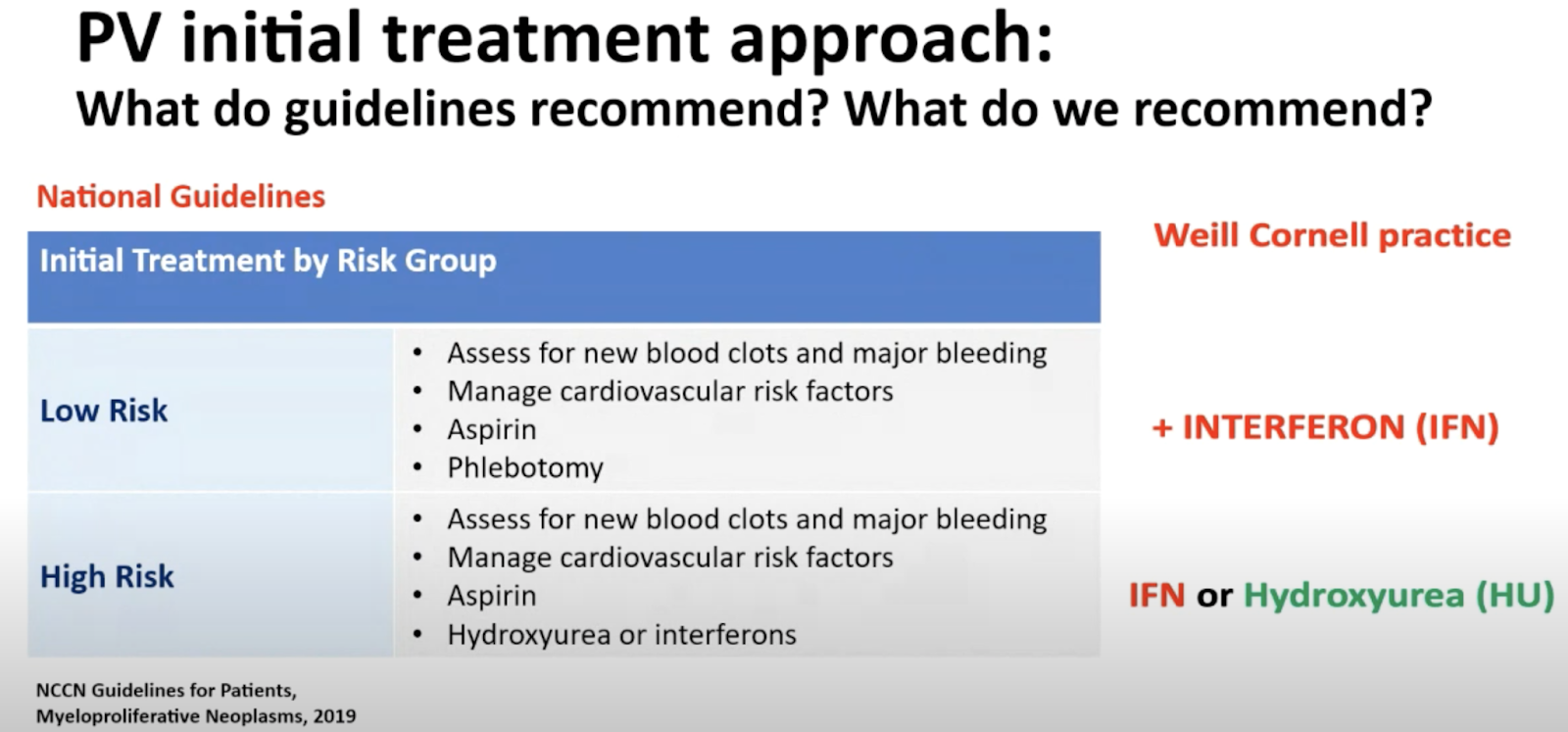

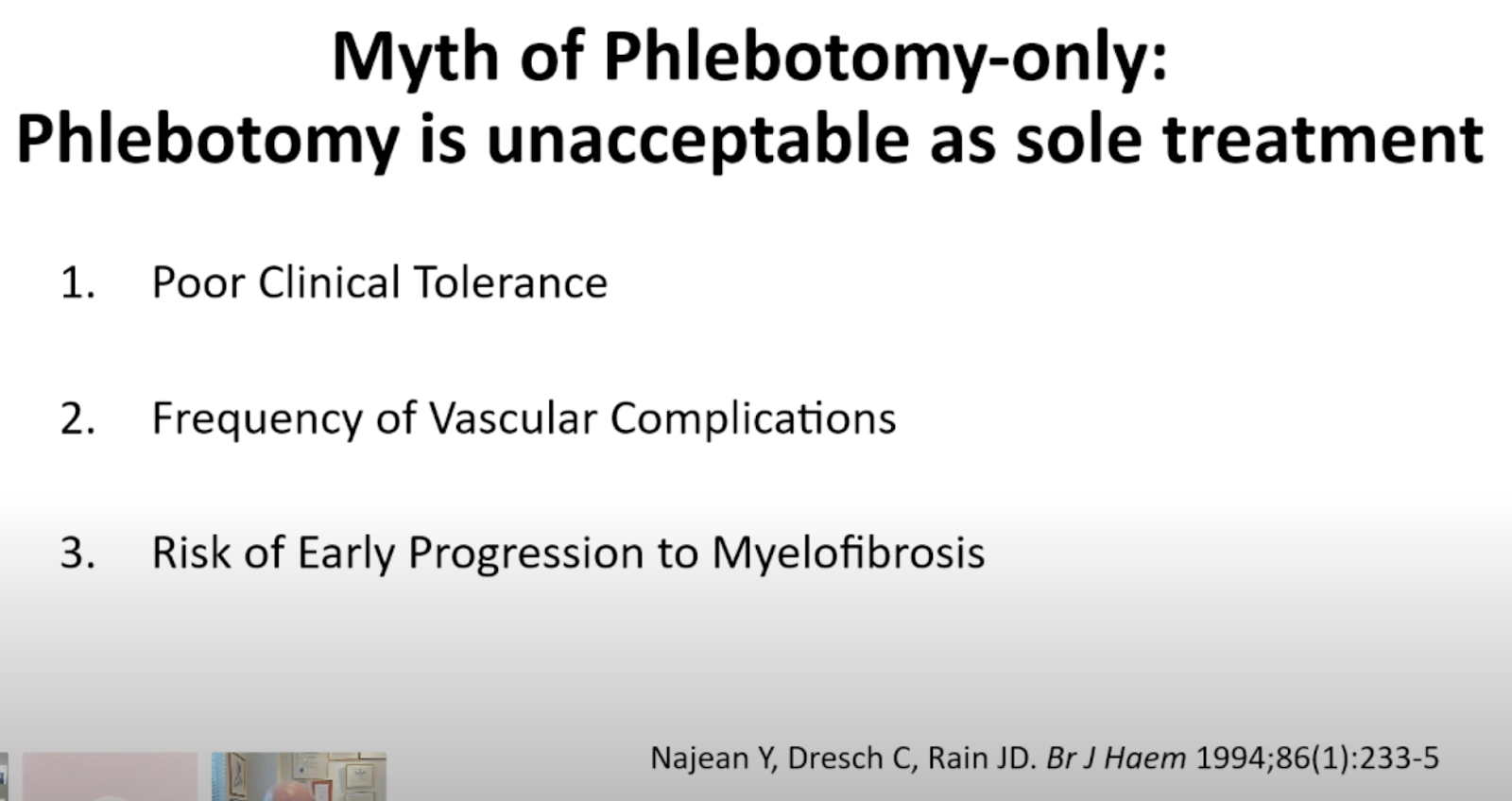
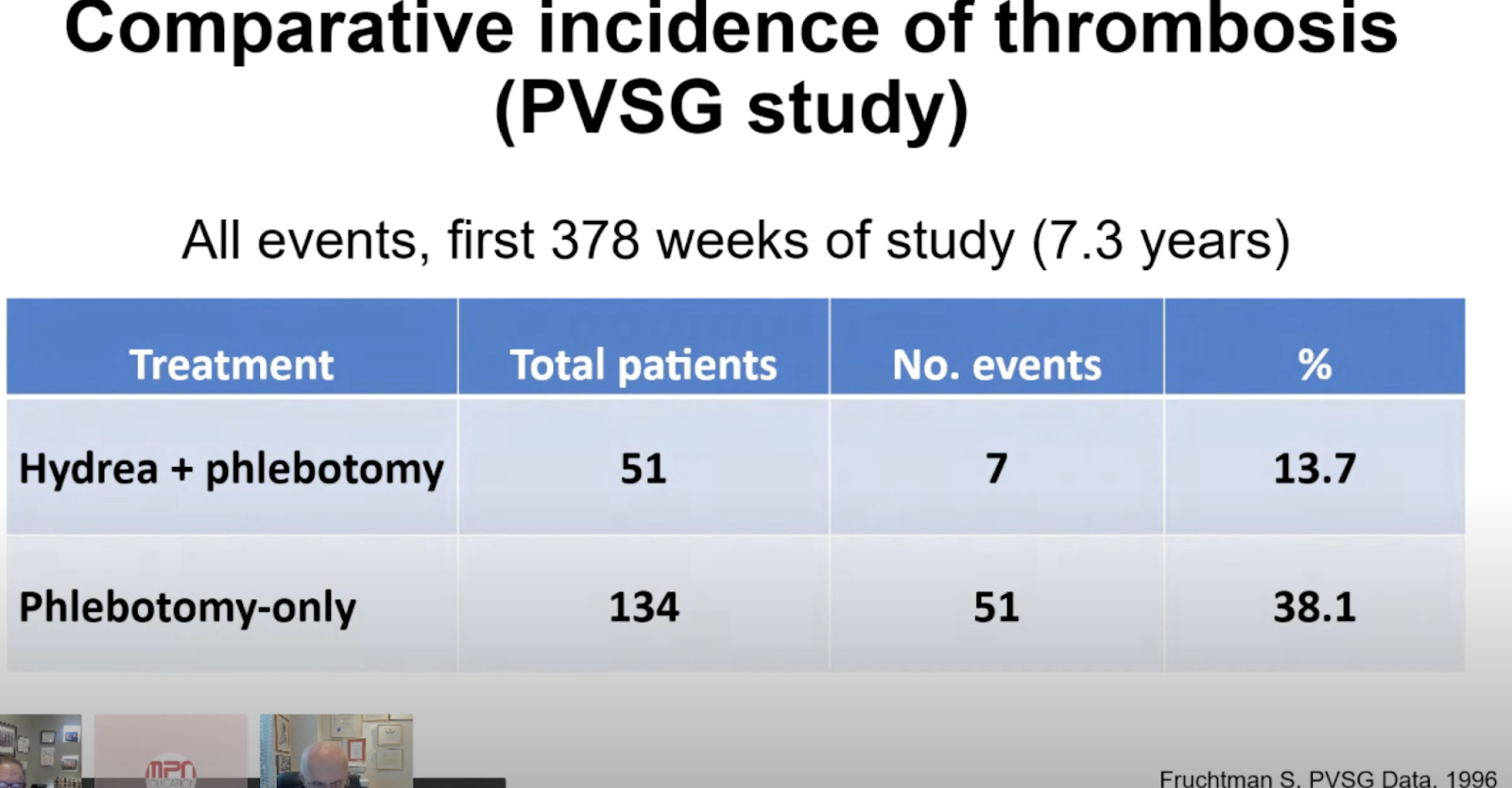
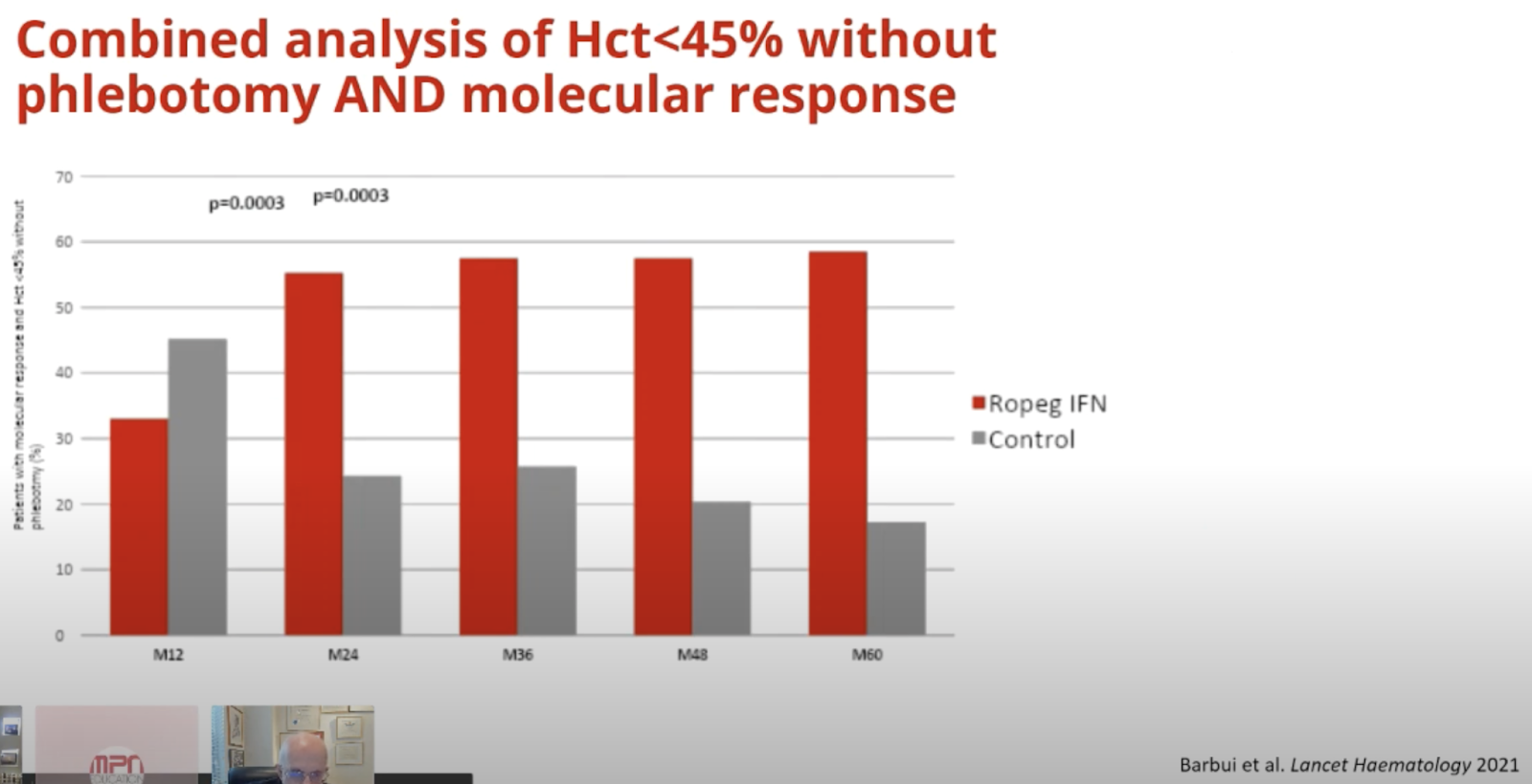

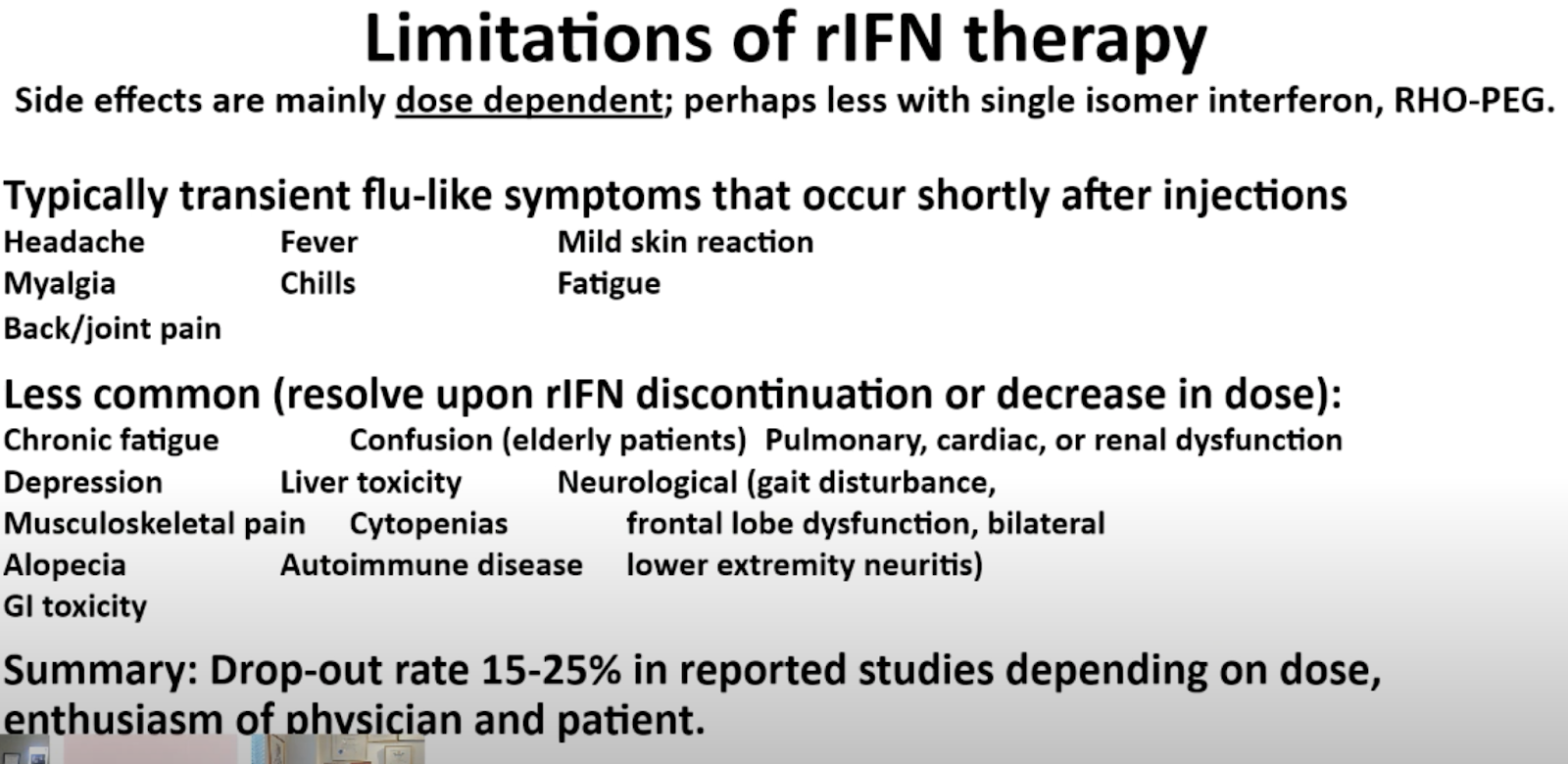
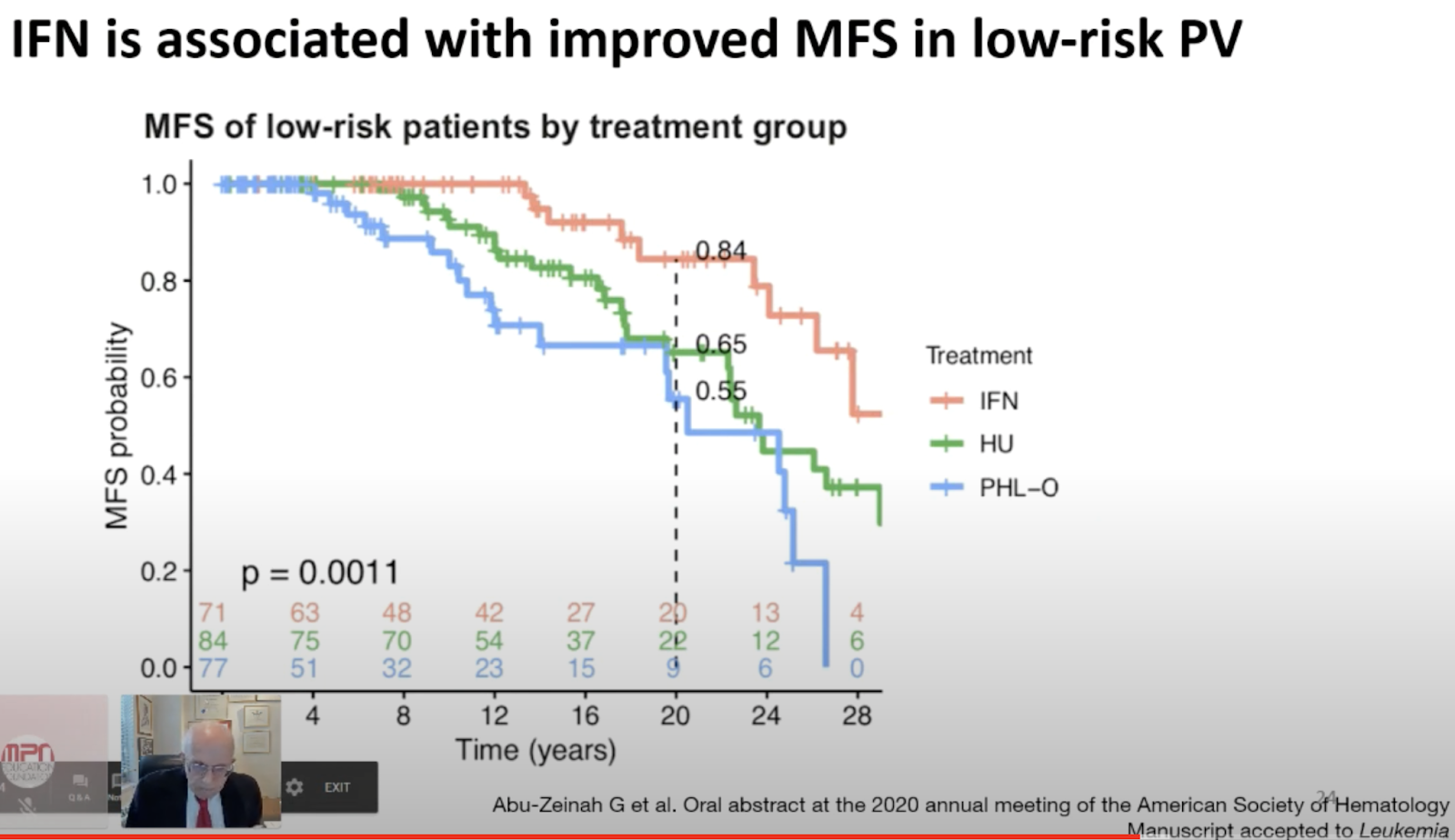

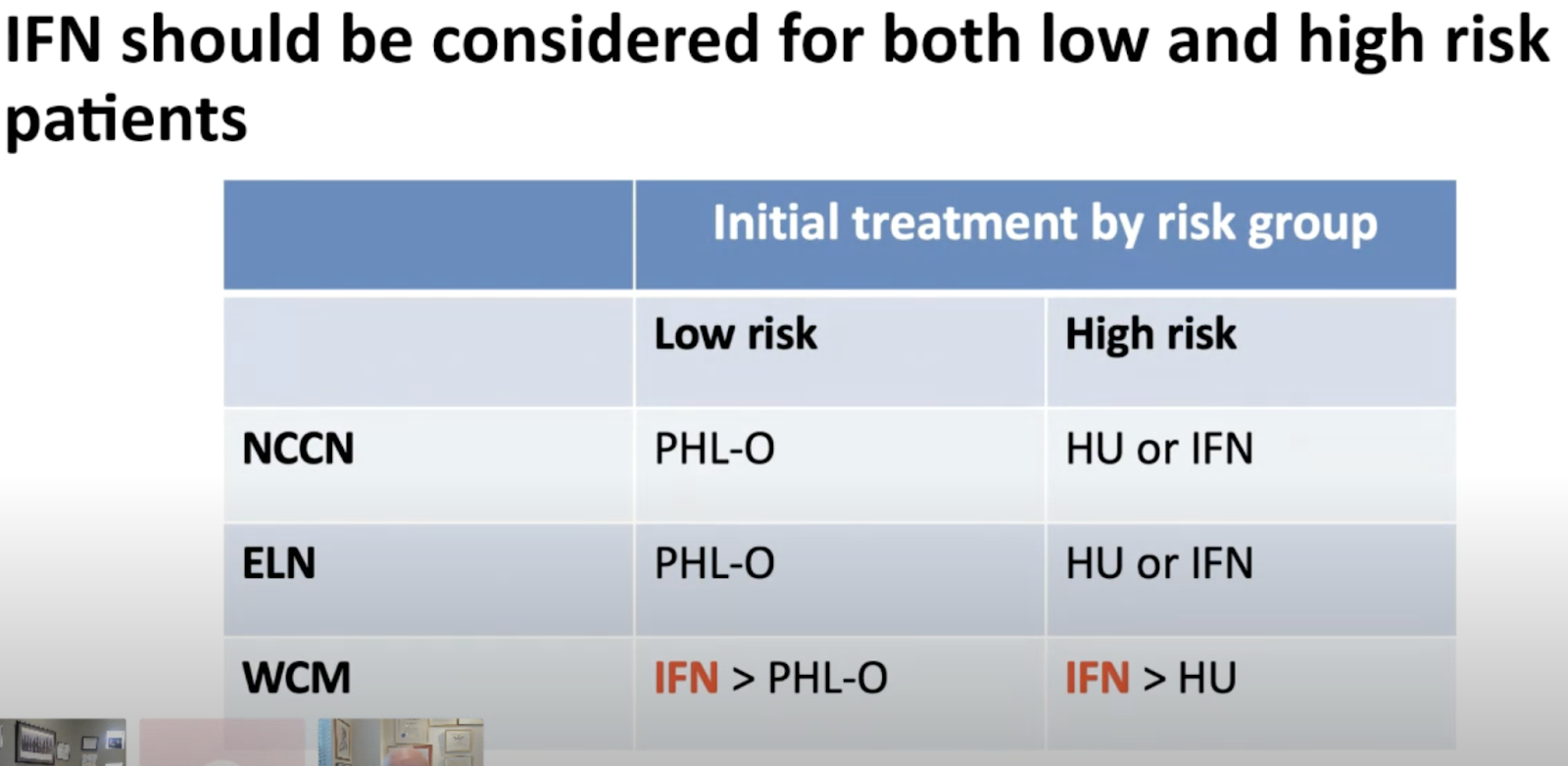
Histomorphological responses after therapy with pegylated interferon α-2a in patients with essential thrombocythemia (ET) and polycythemia vera (PV), 2017
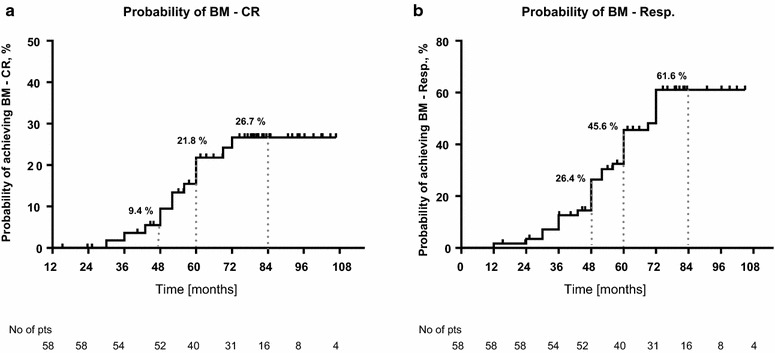
ASH 2019: Interferon-Alfa Treatment Offers Best Outcomes in Polycythemia Vera
Study findings provide evidence for earlier use, even in younger, healthier patients, 2019
Significant improvements in outcomes were seen when recombinant interferon-alfa was used for treatment of patients with polycythemia vera in a study with a follow-up period that lasted up to 45 years. The findings were presented here at the 61st American Hematology Society Annual Meeting & Exposition, which took place from December 7 to 10.
The improvements, which were independent of age, support the view that the early use of interferon-alpha should be a routine aspect of polycythemia vera treatment, “especially in younger patients, who should not be deprived of a disease-modifying therapy for being ‘low-risk’ by consensus criteria,” lead author Richard T. Silver, MD, of New York-Presbyterian Weill Cornell Medical Center in New York, told Elsevier’s PracticeUpdate. “For years, there has been argument whether patients should be treated with phlebotomy only or, if cytoreduction therapy is needed, should it be [hydroxyurea] or interferon?” said Dr. Silver. “We believe the latter, as do many others, since interferon has biologic reasons for its use in polycythemia vera. It is not a nonspecific cell poison like [hydroxyurea].”
The retrospective study focused on 306 polycythemia vera patients whose median age was 54 years (range 20–91 years), and 49% of whom were women. Most patients (82%) were white, 42% were judged high-risk, 28% had cardiovascular risk factors, and 13% had a history of thrombosis.
First-line treatment was interferon-alpha in 75 patients (25%), hydroxyurea in 134 (44%), or other cytoreductive regimens in 37 (12%). Treatment by phlebotomy only was conducted in 60 patients (20%). Alternate second-line treatment was subsequently used in 82 patients (27%). This involved a shift from hydroxyurea to other therapy in 34% or to interferon-alpha in 24%; a shift from interferon-alpha to hydroxyurea in 6% or to a therapy other than hydroxyurea in 15%; or a shift from a cytoreductive regimen to interferon-alpha in 2%, hydroxyurea in 5%, or other therapy in 13%. Treatment arms differed by age at diagnosis with a median of 50, 59 and 52 years for interferon-alpha, hydroxyurea, and phlebotomy only groups, respectively (P < .01).
The findings were presented by Ghaith Abu-Zeinah, MD, a fellow at Weill Cornell.
After a median follow-up period of 11 years (range 1–45 years), the overall median myelofibrosis-free survival (MFS) was 19.5 years. Median overall survival (OS) was 26.3. When evaluating outcomes based on treatment type, median MFS and OS were, respectively, 27 and 28 years for the interferon-alpha arm, 18 and 26 years for the hydroxyurea arm, and 14 and 25 years for the phlebotomy only arm (log-rank P < .01 for MFS and P = .01 for OS).
A multivariate analysis that included age revealed lower risks of post-polycythemia vera myelofibrosis (hazard ratio 0.43, P = .003) and death (hazard ratio 0.44 P = .004) in patients treated with interferon-alpha arm, compared with hydroxyurea. A similar pattern was seen when comparing interferon-alpha treatment with phlebotomy only, with a hazard ratio of 0.22 (P < .01) for myelofibrosis and a hazard ratio of 0.35 (P = .03) for death.
Accounting for crossover, 138 patients received interferon-alpha at any time. This treatment was associated with an 8% relative risk reduction in post-polycythemia vera myelofibrosis, with an age-adjusted hazard ratio of 0.92 (P < .01) as well as a 7% risk reduction in all-cause mortality, with an age-adjusted hazard ratio of 0.93 (P = .01).
“This is the first time that interferon has been shown to improve survival in patients with polycythemia vera, compared with phlebotomy only or [hydroxyurea], as well as significantly increasing the time to develop myelofibrosis,” said Dr. Silver “The limitations to the study are that it is a single institution and retrospective. Nevertheless, this is a new observation of significance.”
Final Results of Prospective Treatment with Pegylated Interferon Alfa-2a for Patients with Polycythemia Vera and Essential Thrombocythemia in First and Second-Line Settings (2019)
Background
Interferons are recognized as active agents in the treatment of patients with high risk essential thrombocythemia (ET) or polycythemia vera (PV), both in the upfront setting as well as beyond. Several trials have shown high rates of hematologic and molecular responses with the use of interferons, however, data on direct comparison of interferon activity in patients with early disease in comparison to patients refractory or resistant to prior therapies, such as hydroxyurea (HU) are lacking. We conducted a controlled analysis of the activity of pegylated interferon alfa-2a (PEG) in two prospective parallel clinical trials conducted in these two unique patient populations.
Methods
The MPD-RC 111 (NCT01259817) was an international, multicenter, phase 2 open-label clinical trial that evaluated PEG therapy in patients with high risk PV and high-risk ET who were either refractory or intolerant (R/I) to HU by modified ELN criteria. The MPD-RC 112 trial (NCT01258856) enrolled patients with high risk ET/PV who were treatment-naïve (TN) (HU <3 months) and randomized them (1:1) to PEG or HU. All patients randomized to PEG were included in this analysis. Both protocols were conducted concurrently at the MPD-RC member institutions and utilized a similar primary endpoint of overall response rate (complete and partial response rates) by ELN Criteria at 12 months confirmed by the same blinded central review committee. Both studies utilized the same PEG starting dose of 45 mcg weekly and was titrated for response to a maximum of 180 mcg weekly. Secondary endpoints included safety information, impact on disease biomarkers, bone marrow (BM) response, and quality of life data.
Results
Patients
ET: 39 TN and 65 R/I ET patients were available for this analysis. Median disease duration was 2.9 months in TN and 37.3 months in R/I patients. Baseline characteristics and demographics were similar in the two cohorts except lower baseline hemoglobin level in RI patients. (Table1A)
PV: 43 TN and 50 R/I PV patients were included. Median disease duration was 2.5 months in TN and 54.8 months in R/I patients. Baseline characteristics only differed by lower frequency of phlebotomy rate in R/I patients. (Table1B) Baseline symptoms scores and quality of life were similar in TN and RI groups (Table 2)
Response
ET: CR/PR/ORR at 12 months were observed in 43.1%/26.2%/69.2% in R/I ET patients and in 43.6%/25.6%/69.2% in TN ET patients (p=0.99 for ORR). (Table 3, Figure 1)
PV: CR/PR/ORR at 12 months were observed in 22%/38%/60% in R/I PV patients, and in 27.9%/58.1%/86% in TN PV patients (p=0.005 for ORR). (Table 3, Figure 1)
Safety
PEG was equally well tolerated throughout both treatment groups with treatment discontinuation due to adverse events occurring in 14.6% in TN patients and 13.9% in R/I patients. The mean (SD) dose of PEG was 102.7 (52.3) mcg in R/I ET patients and 128.7mcg (46.4) in R/I PV patients. For TN patients, mean dose was 85.7mcg (59.7) in ET and 93.5 mcg (44.0) in PV. Adverse events were consistent with historic reports of PEG use and the distribution of events was similar in R/I and TN patients. (Table 4)
Conclusion
This intention to treat response analysis included TN and R/I ET and PV patients with balanced baseline characteristics who received prospective therapy with PEG. Patients with ET had a higher overall response rate at 12 months that was equivalent in patients who were treatment-naïve and in patients who were intolerant or refractory to HU. By contrast, patients with PV who were treatment-naïve had a higher ORR than patients those intolerant or refractory to HU. We conclude that treatment with PEG is an effective therapeutic option both treatment naïve PV and ET as well as those previously treated with HU, however PEG as a second line agent is especially effective in ET patients.
Update on Long-acting Interferons for MPN, 2016

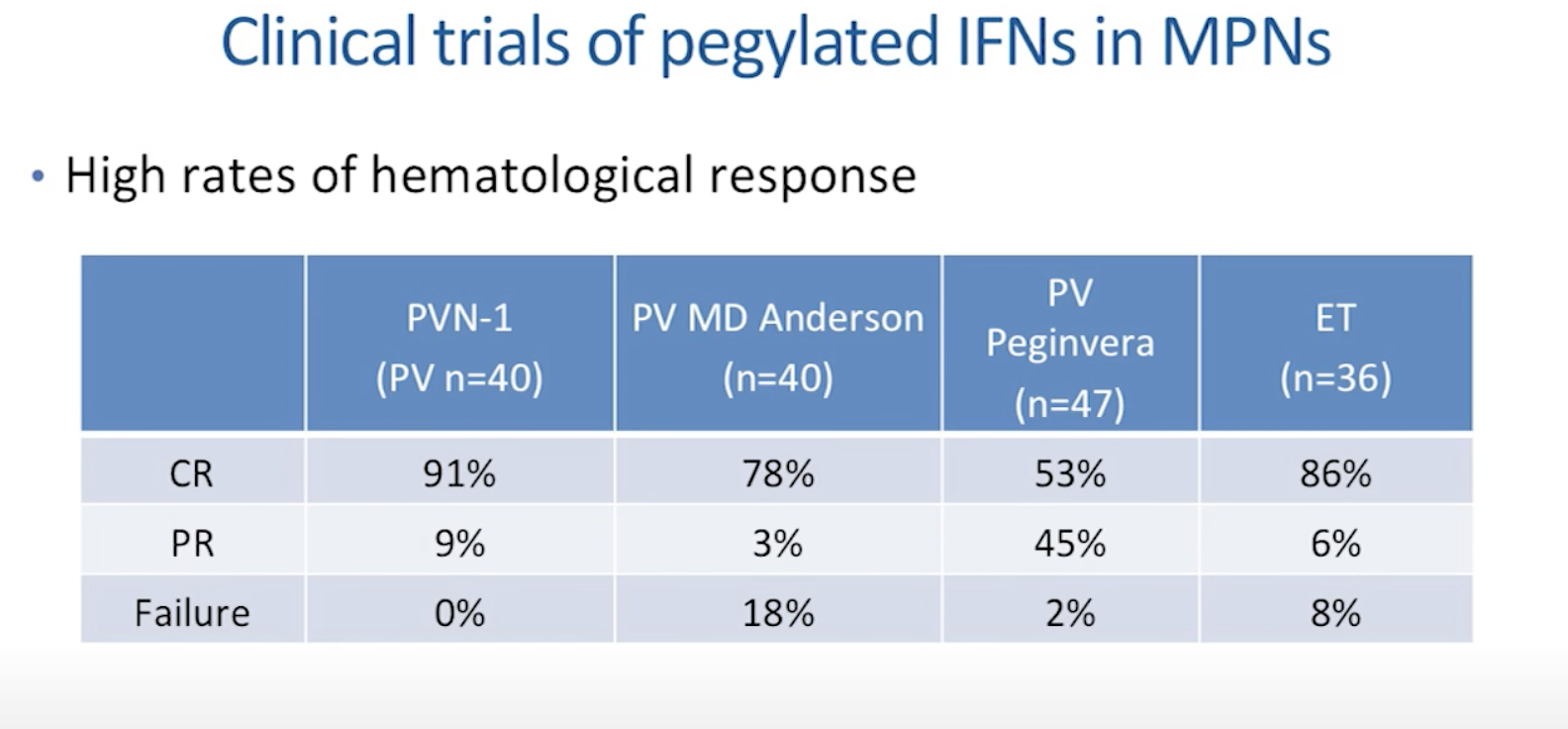
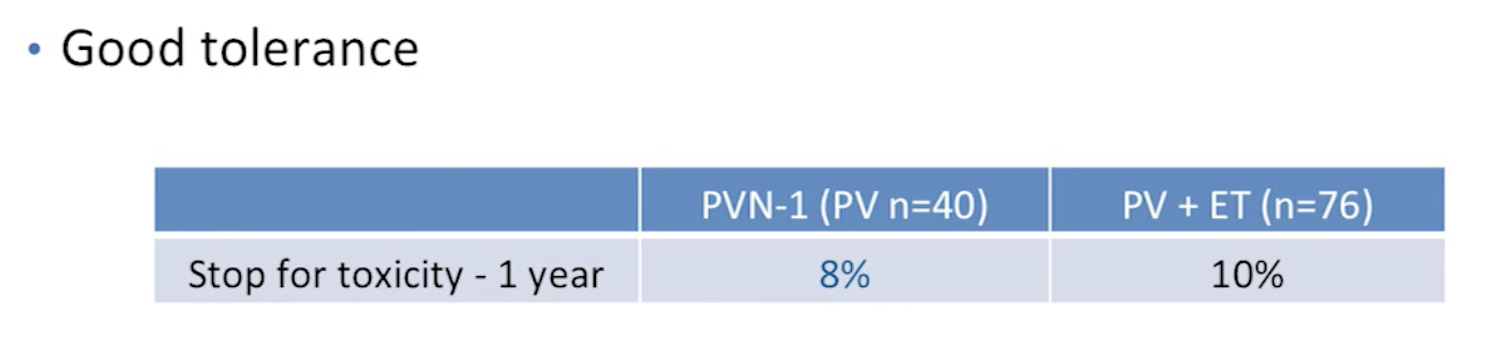
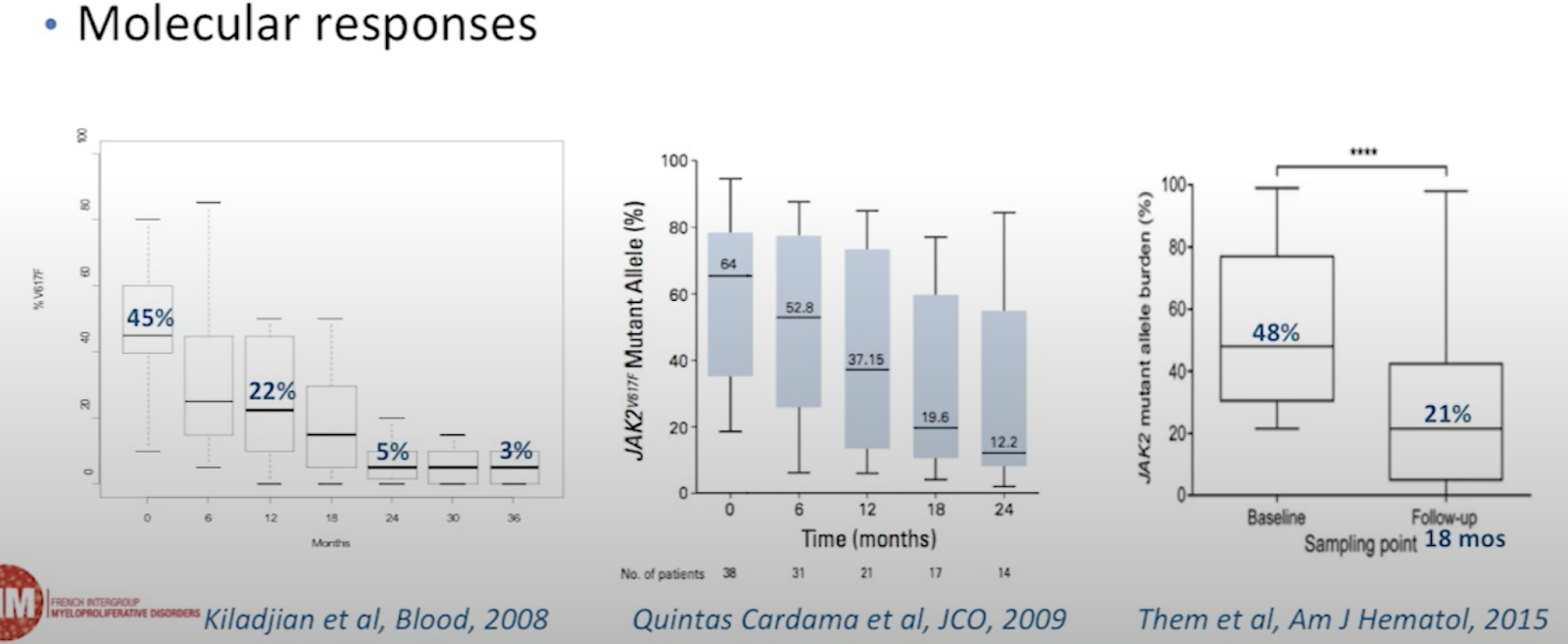
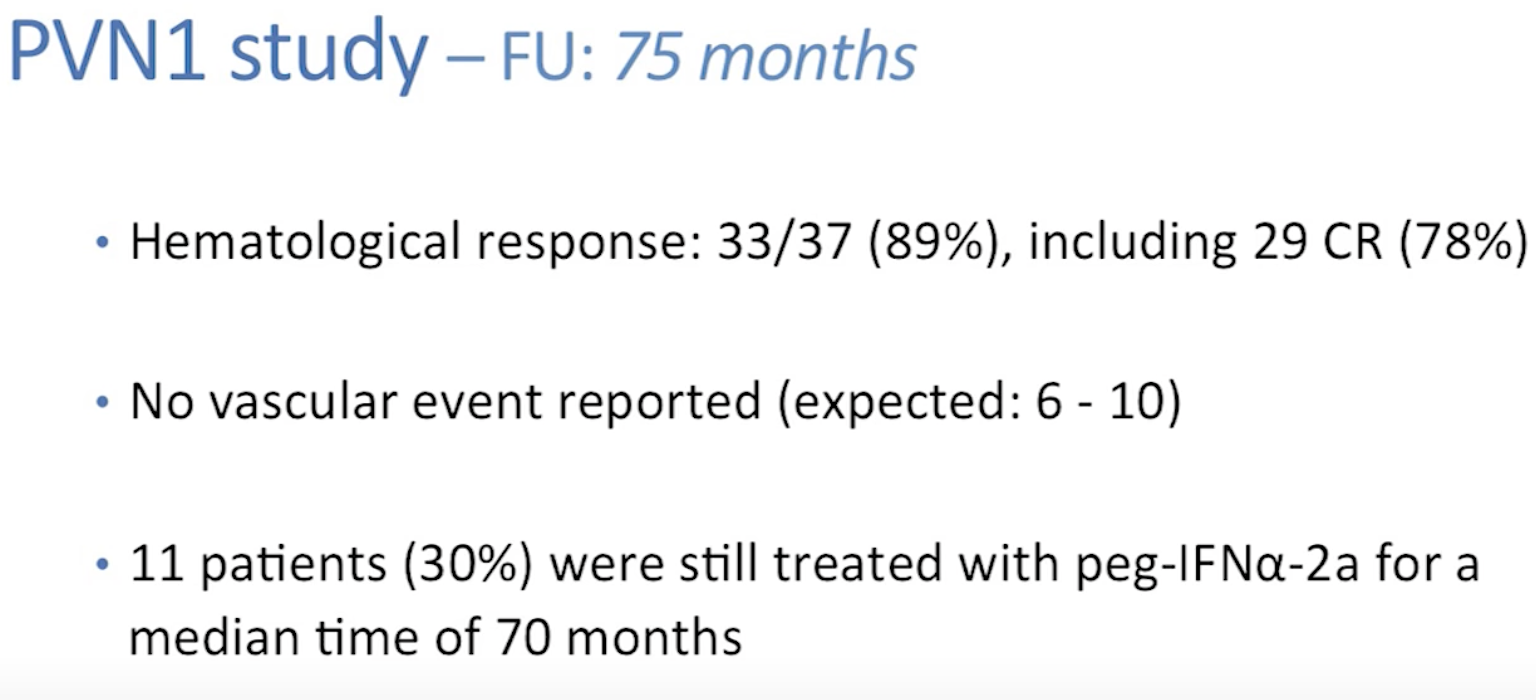
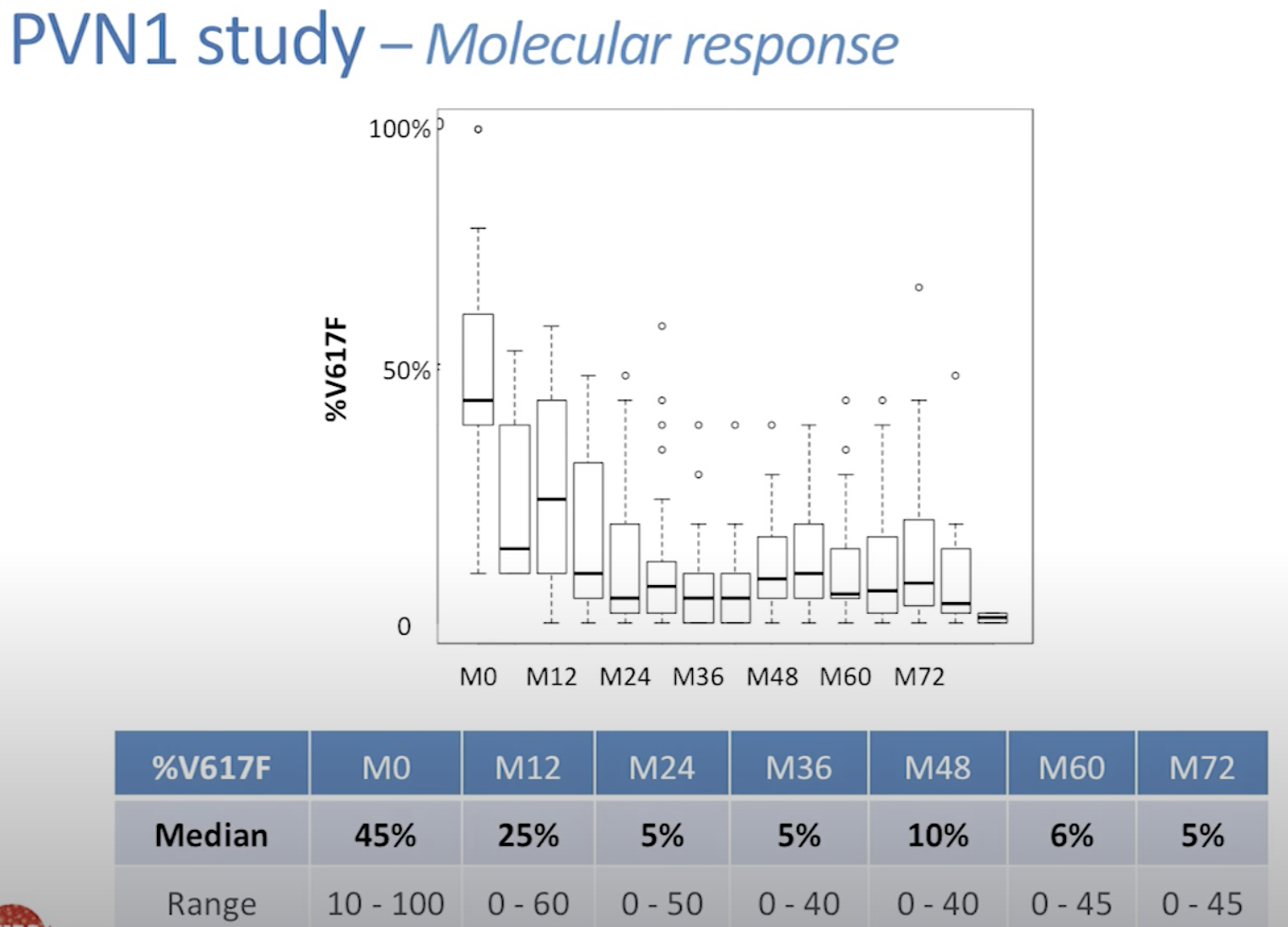

Ropeginterferon effective for treating PV (link)
Data-driven analysis of JAK2V617F kinetics during interferon-alpha2 treatment of patients with polycythemia vera and related neoplasms, 2020
Treatment with PEGylated interferon-alpha2 (IFN) of patients with essential thrombocythemia and polycythemia vera induces major molecular remissions with a reduction in the JAK2V617F allele burden to undetectable levels in a subset of patients. A favorable response to IFN has been argued to depend upon the tumor burden, implying that institution of treatment with IFN should be as early as possible after the diagnosis. However, evidence for this statement is not available. We present a thorough analysis of unique serial JAK2V617F measurements in 66 IFN-treated patients and in 6 untreated patients. Without IFN treatment, the JAK2V617F allele burden increased exponentially with a period of doubling of 1.4 year. During monotherapy with IFN, the JAK2V617F allele burden decreased mono- or bi-exponentially for 33 responders of which 28 patients satisfied both descriptions. Bi-exponential description improved the fits in 19 cases being associated with late JAK2V617F responses. The decay of the JAK2V617F allele burden during IFN treatment was estimated to have half-lives of 1.6 year for the monoexponential response and 1.0 year in the long term for the bi-exponential response. In conclusion, through data-driven analysis of the JAK2V617F allele burden, we provide novel information regarding the JAK2V617F kinetics during IFN-treatment, arguing for early intervention.
Thrombotic risk
In this interferon vs Hydrea trial. Thrombosis risk was only 1.2% per year for both interferon and hydrea arms. These folks are also on Aspirin. Link
Thrombosis rate of 2-3% was reported for those diagnosed after 2005.
Patterns of presentation and thrombosis outcome in patients with polycythemia vera strictly defined by WHO-criteria and stratified by calendar period of diagnosis (Link)
ECLAP study. Aspirin arm had 2.4% major or minor thrombosis per year (2.8yrs of study, 6.7% rate of thrombosis during this period).
Efficacy and Safety of Low-Dose Aspirin in Polycythemia Vera (Link)
Histomorphological responses after therapy with pegylated interferon α-2a in patients with essential thrombocythemia (ET) and polycythemia vera (PV) (2017)
We report on histomorphological BM responses in 58 patients with ET/PV treated with PEG-IFN-α-2a in a prospective, single-center, phase 2 clinical trial after a therapy for a median of 84 months (7 yrs).
Our current research substantiates existing data showing that long-term therapy with PEG-IFN-α-2a is not only able to induce CHR and CMR, but could also lead to complete normalization of BM morphology in a subset of patients. Moreover, PEG-IFN-α-2a was capable to completely reverse BM fibrosis in up to 22% of patients, which is higher than previously observed by other investigators [23, 26]. BM responses were achieved after median time on therapy of 48 months, confirming the observation that a long treatment duration is necessary to achieve such a response.
Our study also reports a few novel observations. In contrast to previously published results [21], we have noticed significant reduction in BM cellularity in patients with PV who achieved CMR. Patients with BM-CR seemed to derive the most benefits from the therapy with longest duration of initial responses (CHR and CMR), higher rates of CMR, and the fewest disease-related complications. Importantly, none of the patients who had achieved BM-CR progressed to overt MF, and majority of patients who had lost their initial BM-CR have maintained their hematologic and molecular responses. BM-CR was durable, as 69% of them were sustained at the time of last follow-up. Furthermore, 5 of 6 (83%) patients who continued to have BM evaluations after treatment discontinuation, have maintained their BM-CR after a median duration off therapy of 48 months. However, 2 of them have lost their best MR at the time of last follow-up, and one patients has lost his hematologic response.
Study population:
58 MPN patients (27 PV, 31 ET)
Median age of 52 yrs old
72% are JAK2 positive
median allele burden of 34%
Median WBC of 9
Median platelets of 721
62% previously treated with other drugs, 75% of them with hydroxyurea
60% had reticulin fibrosis of grade MF-1 or MF-2
Treatment:
Pegylated interferon α-2a
90mcg weekly or higher as the initial dose.
The dose was modified throughout the study based on toxicity or lack of efficacy.
Hematologic response
Initial HR was achieved in 54 (93%) patients, and it was sustained in 33% of them (n = 18) throughout the entire follow-up on a study with a median response duration of 92 months (range 58–101 +). The remaining 36 patients lost their HR after a median duration of 55 months (range 10.4–91). Sixteen patients who lost their HR, are still on study, 14 of them actively treated, as they continue to derive clinical benefit (no clinical symptoms and organomegaly) with good tolerance.
Molecular response
MR rate was 72% (n = 32) among 44 patients who were JAK2V617F-positive.
9 (20%) experienced Complete MR [undetectable JAK2V617F allele burden].
19 (43%) experienced Partial MR [ 50% reduction in JAK2V617F allele burden].
4 (9%) experienced Minor MR [mMR; 20–49% reduction in JAK2V617F allele burden].
Pre-treatment allele burden did not differ among patients with CMR, PMR and mMR.
The response duration was similar in patients with CMR (68 months; range 21–94), PMR (53 months; range 7–79) and mMR (50 months; range 12–60).
Bone marrow response
29 patients (50%) had BM response
13 patients (22%) with BM-CR (Table 3, Fig. 1)
16 patients (28%) with BM-PR [12]
Furthermore, 13 patients (22%) had complete resolution of bone marrow reticulin fibrosis (MF-0), including 3 patients with initial grade 2.
Table 3 (BM-Complete Response)


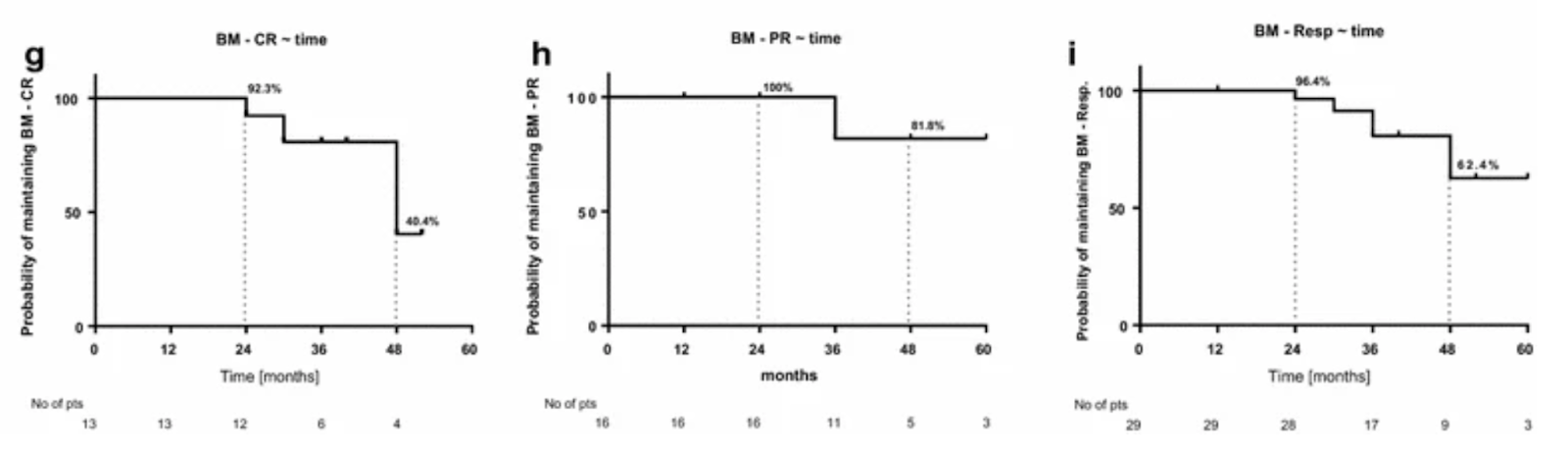

Vascular complications
Overall, 6 (10%) patients experienced unprovoked vascular complications (5 thrombotic and one bleeding event): one while having BM-CR, 2 BM-PR, and 3 BM-NR. The incidence rate of major unprovoked thromboembolic event in enrolled patients during the entire study follow-up was 1.37 per 100 person years.
Disease progression
Progression to overt MF and AML occurred in 5 patients (9%; 4 MF and 1 AML), and none of these patients had a BM response.
Patients after therapy discontinuation
Among patients with a BM response who discontinued therapy, 6 continued to have BM biopsies performed, with a median of 4 samples per patient (range 3–6). Four stopped therapy while in BM-CR and 2 while in BM-PR.
Two patients (#1 and #11, Figs. 4, 5), who had achieved a BM-PR at the time of treatment discontinuation, continued to show improvements in their BM despite being off therapy. Remarkably, both achieved a BM-CR after being off therapy for 32 and 36 months, and maintained their BM-CR for 30 and 24 months, still off therapy, respectively. One of these patients (#1, Fig. 5) has lost his CHR and best MR while still remaining in BM-CR; the other one continues to be in CHR (MR not evaluable for JAK2 negativity). Among those 4 patients who stopped therapy at the time of BM-CR (#9, #10, #12, and #13, Fig. 4), 3 remain in sustained BM-CR. One of them has lost his best MR (#10, Fig. 4), one remains in CMR (#9, Fig. 4) and one is JAK2 negative (#12, Fig. 4). All three patients maintain their initial CHR. Only one patient has lost his BM-CR after being off therapy for 24 months, he has also lost his CHR and best MR (#13, Fig. 6).
At present, therefore, 5 of 6 evaluable patients are in BM-CR after stopping therapy, and are maintaining their BM-CR for a median time of follow-up after therapy discontinuation of 48 months (range 32–68).
New Perspectives of Interferon-alpha2 and Inflammation in Treating Philadelphia-negative Chronic Myeloproliferative Neoplasms, 2021
In recent years, the use of recombinant interferon-alpha (rIFNα) as the initial treatment of the myeloproliferative neoplasms (MPNs), essential thrombocythemia, polycythemia vera and myelofibrosis, has been increasing. In a subset of patients, treatment with rIFNα for approximately 5 years may result in minimal residual disease (MRD) characterized by hematologic remission, a low JAK2V617F allele burden, and normal bone marrow morphology. The important role of chronic inflammation as the driving force for clonal evolution and disease progression and the impact of chronic inflammation upon symptom burden have been substantiated. Here, we highlight timely research questions regarding the use of rIFNα in the future MPN landscape and underscore the importance of early diagnosis and treatment with it to achieve MRD. Based upon the highly encouraging results from combination therapy of stem cell-targeted therapy with rIFNα and the potent anti-inflammatory drug, ruxolitinib, we also place in perspective studies of combinations with older, inexpensive agents (eg, statins, N-acetylcysteine, and colchicine), which have well-established anti-inflammatory and antithrombotic capabilities. Mathematical modeling studies have substantiated the concept that chronic inflammation is a trigger and driver of MPN development, and stress the importance of initiating rIFNα treatment as early as possible. Studies of the impact of rIFNα in individuals carrying the JAK2V617F or the CALR mutation as clonal hematopoiesis of indeterminate potential (CHIP) are urgently needed to determine whether rIFNα treatment at this early CHIP stage may eradicate the malignant clone. We foresee a bright future for patients with an MPN, in whom early intervention with stem cell-targeted therapy, rIFNα, alone or in combination with drugs targeting the chronic inflammatory state, may allow many to achieve MRD, thus becoming candidates for clinical trials employing vaccines leading to the possibility of cure.
Interferon alpha therapy in essential thrombocythemia and polycythemia vera—a systematic review and meta-analysis (2020)
This meta-analysis included 44 studies with a total of 1359 patients (730 with essential thrombocythemia (ET) and 629 with polycythemia vera (PV)) treated with interferon-alpha (IFN).
The overall response rate (ORR) was 80.6% (95% CI 76.6-84.1%) for ET patients. The complete hematologic response (CHR) rate was 59.0% (95% CI 51.5-66.1%).
For PV patients, the ORR was 76.7% (95% CI 67.4-84.0%) and the CHR rate was 48.5% (95% CI 37.8-59.4%).
Response rates were similar for pegylated IFN versus non-pegylated IFN, and between studies with follow-up <24 months versus ≥24 months.
The rate of thromboembolic events was low at 1.2% per patient-year for ET and 0.5% per patient-year for PV.
The rate of treatment discontinuation due to adverse events was 8.8% per patient-year for ET and 6.5% per patient-year for PV.
Flu-like symptoms were the most common adverse effects, but serious adverse events were rare.
Molecular responses, defined as ≥50% reduction in JAK2 V617F allele burden, occurred in up to 57% of PV patients.
The authors concluded that both pegylated and non-pegylated IFN are effective and safe long-term treatments for ET and PV, with durable molecular responses suggesting potential disease-modifying effects.
Limitations include heterogeneity in outcome definitions and reporting between studies, and limited data directly comparing IFN to standard treatments like hydroxyurea.
Overall, this meta-analysis provides strong evidence that IFN is an effective treatment option for ET and PV, with low rates of thromboembolic events, manageable side effect profiles, and potential disease-modifying benefits compared to other cytoreductive therapies.
Symptomatic Diffs between PEG and HU (2022)
What are the biggest symptomatic differences between Pegasys and Hydroxyurea? I downloaded the symptom (AE) data in this paper and ranked by the difference. Topmost elements = higher symptom burden with Pegasys. Bottommost elements = higher symptom burden with Hydroxurea. Rows marked with * are p<0.05 (statistically significant differences). The rest might be due to chance.
A word of caution: The timeframe for this study is 3-12 months after starting treatment. This makes the comparison somewhat unfair to Pegasys. We know that you get the best results with interferon after 3-5 years. Many users even reduce the frequency of injections, reducing the sides. Hydrea only becomes less effective over time. Pegasys becomes more effective over time, allowing dose reductions and providing symptom relief even at the same dose.
—-------------
Pegylated Interferon Alfa-2b Treatment for Patients With Solid Tumors: A Phase I/II Study (2002)
PURPOSE: The efficacy of interferon alfa has been established in treating advanced melanoma and renal cell carcinoma (RCC) patients. We conducted a phase I/II study to determine the maximum-tolerated dose (MTD), the safety and tolerability, and the preliminary efficacy of once-weekly pegylated interferon alfa-2b (IFNα-2b) in patients with advanced solid tumors (primarily RCC).
RESULTS: The MTD for pegylated IFNα-2b at 12 weeks was 6.0 μg/kg/wk. One year of 6.0 μg/kg/wk was well tolerated with appropriate dose modification; no grade 3 or 4 fatigue occurred, and safety was comparable with that with nonpegylated IFNα-2b. The most common nonhematologic adverse events included mild to moderate nausea, anorexia, and fatigue. Six patients had grade 3 or 4 hematologic toxicity. Twenty-nine patients continued on the extension protocol. Four patients had a complete response, and five patients had a partial response. Among 44 previously untreated RCC patients, the objective response rate was 14%. Median survival for all RCC patients was 13.2 months.
CONCLUSION: Pegylated IFNα-2b was active and well tolerated in patients with metastatic solid tumors, including RCC, at doses up to 6.0 μg/kg/wk.
Interferon alfa-2a in advanced renal cell carcinoma: treatment results and survival in 159 patients with long-term follow-up
[Not pegylated interferon alpha2-a]
Purpose: Three trials were conducted to define the efficacy and toxicity of interferon alfa-2a in the treatment of metastatic renal cell cancer. Univariate and multivariate analyses were performed to identify prognostic factors for survival.
Patients and methods: Prospectively, 159 patients were treated with interferon alfa-2a.
Results: The overall response proportion was 10% (two complete and 14 partial responses). The median response duration was 12.2 months. The median survival duration was 11.4 months, with 3% of patients alive at 5 or more years. A univariate statistical analysis showed that a Karnofsky performance status > or = 80, prior nephrectomy, and interval from diagnosis to treatment of longer than 365 days were significant prognostic factors for survival. In a multivariate analysis, only prior nephrectomy and Karnofsky performance status > or = 80 were shown to be independent predictors of survival.
Improvement of glucose and lipid metabolism with pegylated interferon-α plus ribavirin therapy in Chinese patients chronically infected with genotype 1b hepatitis C virus
https://www.annsaudimed.net/doi/10.5144/0256-4947.2015.293
Shows improvements in Trigs, FB, HA1C, TC at week 72, and much less at week 48
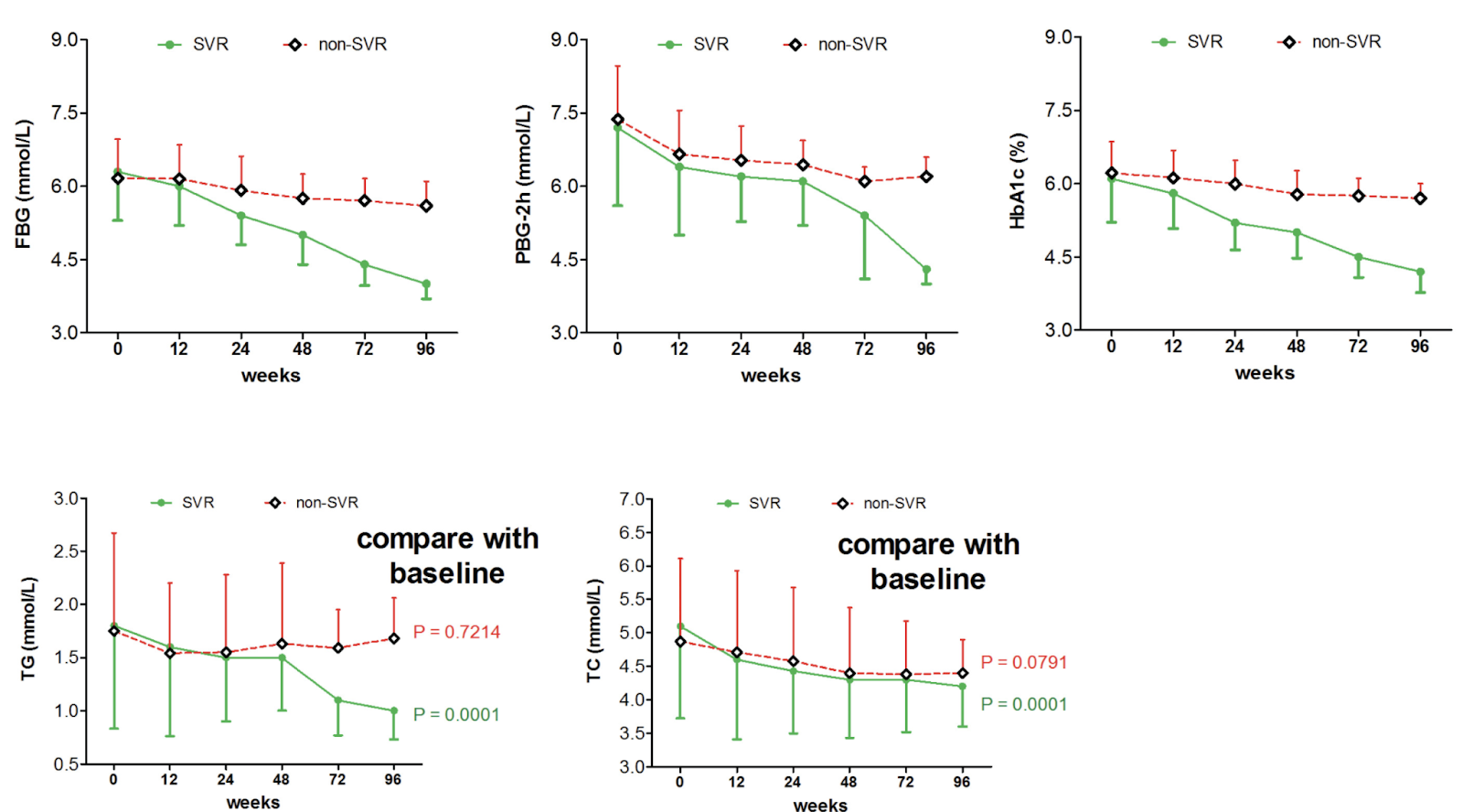
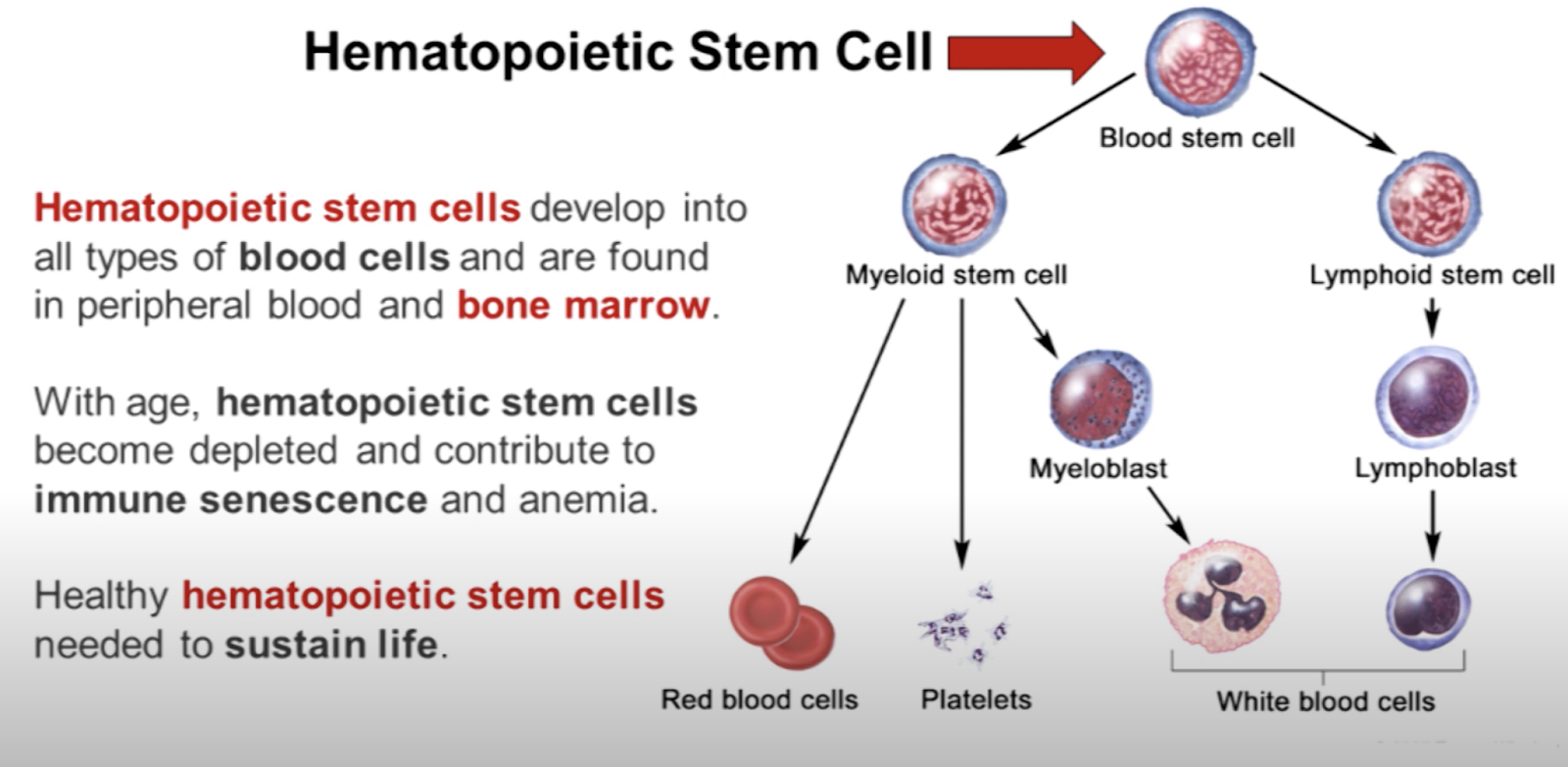
Histomorphological responses after therapy with pegylated interferon α-2a in patients with essential thrombocythemia (ET) and polycythemia vera (PV), 2017
Background
Pegylated interferon alfa-2a (PEG-IFN-α-2a) is a potent immunomodulating agent capable of inducing high rate of hematologic and even complete molecular remission in patients with essential thrombocythemia (ET) and polycythemia vera (PV). We recently reported results of a phase 2 trial of PEG-IFN-α-2a in 83 patients with ET and PV after a median follow-up of 83 months. Here we report an analysis of bone marrow (BM) responses in these patients.
Methods
Among 83 patients, 58 (70%, PV 25, ET 31) had evaluable BM samples. BM responses and fibrosis grading were defined according to the International Working Group for Myeloproliferative Neoplasms Research and Treatment, and the European Consensus on grading of BM fibrosis, respectively. BM was assessed prior to enrollment, and every 6–24 months while on therapy in all patients, and after therapy discontinuation in some patients.
Results
The median age of analyzed 58 patients was 52 years, and 29% were males. After a median follow-up of 84 months, 32 patients are still on study. Hematologic (HR) and molecular responses (MR) were seen in 93 and 69% patients, respectively. Twenty-nine patients (50%) had a BM response, including 13 (22%) with a complete BM response (BM-CR). Moreover, 13 patients (22%) have experienced complete resolution of bone marrow reticulin fibrosis. Patients with BM response had higher duration of HR and MR, and lower discontinuation rate. Furthermore, patients with BM-CR had a higher probability of complete MR. The median duration of BM-CR was 30 months, and 9 patients have maintained their BM-CR (69%), including five who have maintained their response after discontinuation of therapy. Despite this observation, the pattern of HR, MR and BM response, their durability and interrelation was heterogeneous.
Conclusions
Our results show the ability of PEG-IFN-α-2a to induce complete BM responses in a subset of ET and PV patients, but its correlation with durable clinically relevant treatment benefit warrants further investigation.
Perspectives on interferon-alpha in the treatment of polycythemia vera and related myeloproliferative neoplasms: minimal residual disease and cure? 2019
The first clinical trials of the safety and efficacy of interferon-alpha2 (IFN-alpha2) were performed about 30 years ago. Since then, several single-arm studies have convincingly demonstrated that IFN-alpha2 is a highly potent anti-cancer agent in several cancer types but unfortunately not being explored sufficiently due to a high toxicity profile when using non-pegylated IFN-alpha2 or high dosages or due to competitive drugs, that for clinicians at first glance might look more attractive. Within the hematological malignancies, IFN-alpha2 has only recently been revived in patients with the Philadelphia-negative myeloproliferative neoplasms—essential thrombocytosis, polycythemia vera, and myelofibrosis (MPNs)—and in patients with chronic myelogenous leukemia (CML) in combination with tyrosine kinase inhibitors. In this review, we tell the IFN story in MPNs from the very beginning in the 1980s up to 2018 and describe the perspectives for IFN-alpha2 treatment of MPNs in the future. The mechanisms of actions are discussed and the impact of chronic inflammation as the driving force for clonal expansion and disease progression in MPNs is discussed in the context of combination therapies with potent anti-inflammatory agents, such as the JAK1–2 inhibitors (licensed only ruxolitinib) and statins as well. Interferon-alpha2 being the cornerstone treatment in MPNs and having the potential of inducing minimal residual disease (MRD) with normalization of the bone marrow and low-JAK2V617F allele burden, we believe that combination therapy with ruxolitinib may be even more efficacious and hopefully revert disease progression in many more patients to enter the path towards MRD. In patients with advanced and transforming disease towards leukemic transformation or having transformed to acute myeloid leukemia, “triple therapy” is proposed as a novel treatment modality to be tested in clinical trials combining IFN-alpha2, DNA-hypomethylator, and ruxolitinib. The rationale for this “triple therapy” is given, including the fact that even in AML, IFN-alpha2 as monotherapy may revert disease progression. We envisage a new and bright future with many more patients with MPNs obtaining MRD on the above therapies. From this stage—and even before—vaccination strategies may open a new horizon with cure being the goal for some patients.
Interferon α-induced Apoptosis in Tumor Cells Is Mediated through the Phosphoinositide 3-Kinase/Mammalian Target of Rapamycin Signaling Pathway (link)
Interferon (IFN) α induces a caspase-dependent apoptosis that is associated with activation of the proapoptotic Bak and Bax, loss of mitochondrial membrane potential, and release of cytochrome c. In addition to the onset of the classical Jak-STAT pathway, IFNα also induced phosphoinositide 3-kinase (PI3K) activity. Pharmacological inhibition of PI3K activity by Ly294002 disrupted IFN-induced apoptosis upstream of mitochondria. Inhibition of mTOR by rapamycin or by overexpression of a kinase dead mutant of mTOR, efficiently blocked IFNα-induced apoptosis. A PI3K and mTOR-dependent phosphorylation of p70S6 kinase and 4E-BP1 repressor was induced by IFNα treatment of cells and was strongly inhibited by Ly294002 or rapamycin. The activation of Jak-STAT signaling upon IFNα stimulation was not affected by abrogating PI3K/mTOR pathway. Neither was the expression of several IFNα target genes affected, nor the ability of IFNα to protect against virus-induced cell death affected by inhibition of the PI3K/mTOR pathway. These data demonstrate that an intact PI3K/mTOR pathway is necessary for the ability of IFNα to induce apoptosis, whereas activation of the Jak-STAT pathway alone appears to be insufficient for this specific IFNα-induced effect.
The fact that IFNα acts as a potent inducer of apoptosis in a number of malignant cell lines and in primary tumor cells (6, 7, 8, 9, 10, 44) allows the suggestion that the induction of programmed cell death may be one of the actual mechanism for the anti-tumor effects of IFN. One could draw a parallel with the cytotoxic drugs used for chemotherapy, the major mechanism of action of which is induction of apoptosis of tumor cells (45). As with cytotoxic drugs, many tumor types are resistant to IFN therapy for unknown reasons. Therefore the knowledge of the signaling pathways responsible for the apoptosis induction is extremely important for understanding of the variability in cellular responses to IFN treatment.
The Effect Of Antioxidants On The Side Effects Of Pegylated Interferon/Ribavirin Combination Therapy In Patients With Chronic Hepatitis C, 2013
Abstract
Background and study aim:: Combined anti-hepatitis C therapy with pegylated interferon and ribavirin is associated with numerous side effects that affect both patients’ compliance and response rates. These side effects are believed to be, in part, due to oxidative stress induced by ribavirin. In the present work, we tried to evaluate if antioxidants can ameliorate the side effects of this therapy in patients with chronic hepatitis C (CHC).
Patients and methods: Two hundred selected patients with CHC were randomized to receive either the standard antiviral combination therapy (Peginterferon and Ribavirin) plus antioxidant mixture (slow release vitamin C 500 mg daily, vitamin E 400 mg daily, silymarin 420 mg daily and N-acetylcystein 600 mg daily) for 48 weeks (study group, group I) or to receive the standard combination therapy only for 48 weeks (control group, group II). Patients were followed up during the whole treatment course to assess the occurrence of subjective and laboratory side effects of the combined antiviral therapy.
Results :The results of our study revealed statistically significant difference between both groups regarding changes in hemoglobin concentration along therapy from week one onwards as reduction in hemoglobin concentration along therapy was significantly lower in group I; p = 0.001. The frequency of significant anemia (Hb < 10 gm/dl) in group I was significantly lower than Group II from week twelve onwards; p value ranged from 0.013 to 0.001. Moreover, the frequency of fatigue was significantly lower in group I from week two onwards till the end of therapy; p value ranged from 0.027 to < 0.001. On the other hand, all other checked side effects either subjective or laboratory revealed a non significant statistical difference between both groups.
Conclusion : The use of an antioxidant mixture with antiviral combination therapy in patients with CHC can improve treatment associated anemia and fatigue but has no effect on other treatment associated side effects.
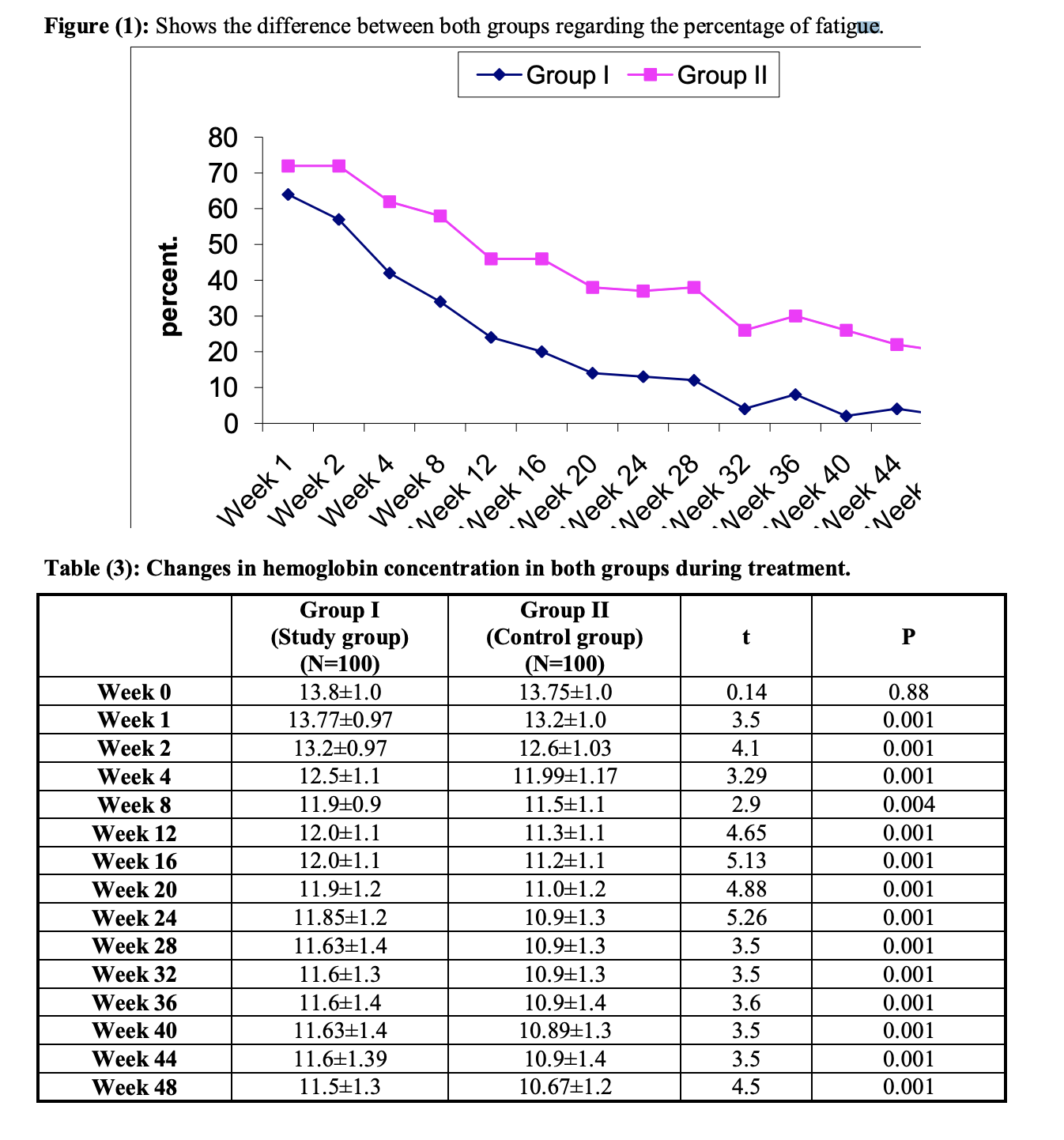
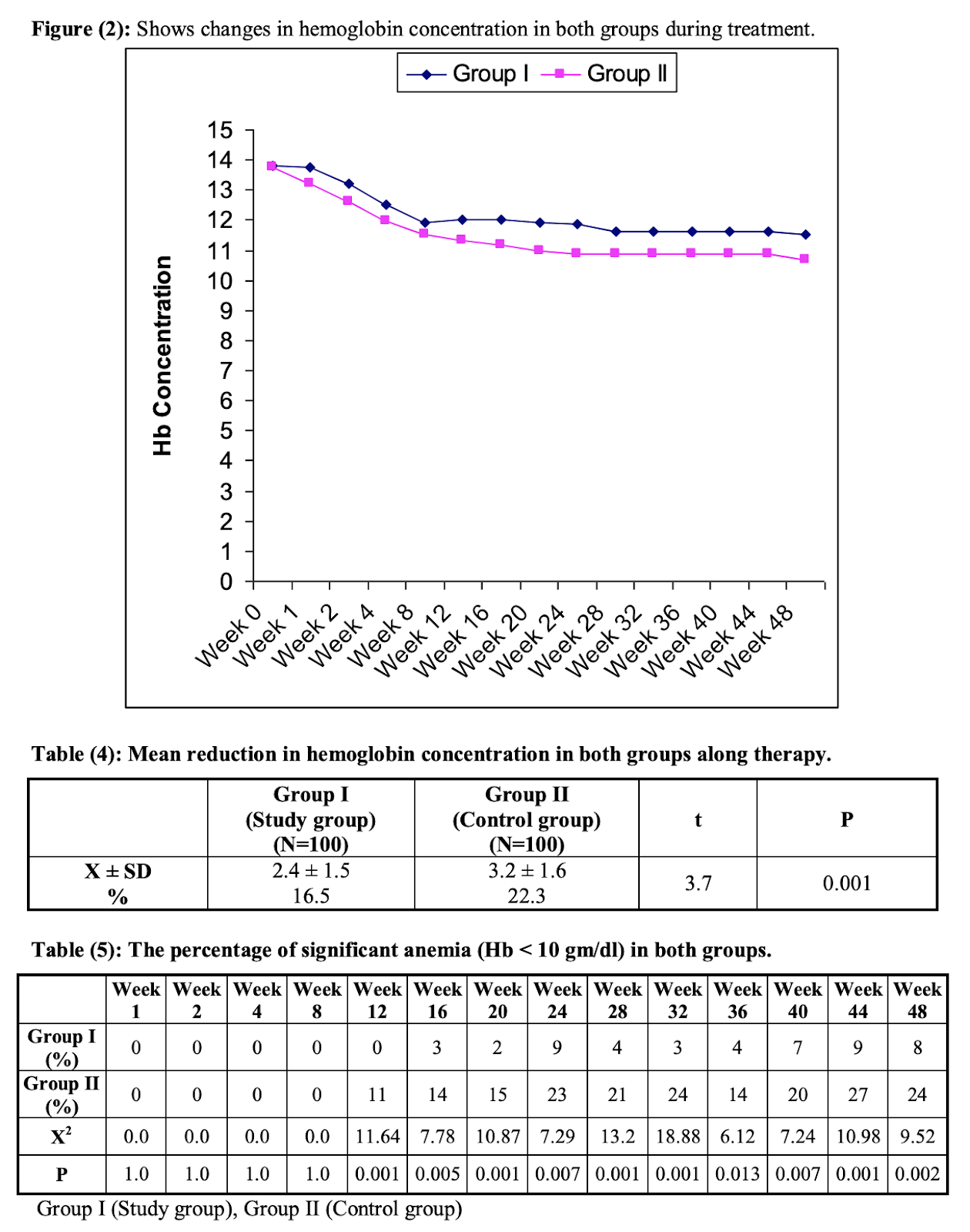
N-Acetyl Cysteine Enhances the Response to Interferon-α in Chronic Hepatitis C: A Pilot Study
Hepatitis C virus (HCV) is an RNA virus that replicates in both the liver and lymphoid cells. Interferon-α (IFN-α) is a useful treatment of chronic hepatitis C (CHC) although resistance to this drug occurs frequently. The mechanisms underlying resistance to IFN remain unknown. In this work, we have measured the levels of glutathione in plasma and peripheral lymphoid cells from 15 healthy controls and 24 CHC patients, 10 of whom were without treatment and 14 showed high serum alanine aminotransferase (ALT) values despite therapy with lymphoblastoid IFN for more than 4 months. In all patients, glutathione levels in plasma and in mononuclear cells were depressed in comparison to controls. In IFN-unresponsive patients, the addition of 600 mg tid of oral N-acetyl cysteine (NAC), a glutathione precursor, resulted in a steady decrease of ALT values in all patients, with complete normalization in 41 % of cases after 5–6 months of combined therapy. Administration of NAC alone for 1 month was without effect in the 10 patients that were not receiving IFN. Supplementation of IFN with NAC induced a near normalization of intralymphocytic glutathione, but plasma levels were only moderately increased. HCV replication was markedly inhibited in lymphocytes and viremia was cleared in one of the 8 patients tested. In conclusion, NAC enhances the response to IFN in CHC. Controlled studies are needed to ascertain whether antioxidant therapy might act in synergy with IFN in chronic viral hepatitis.
Genomic Profiling of a Randomized Trial of Interferon-α versus Hydroxyurea in MPN Reveals Mutation-Specific Responses, 2021
Background Although somatic mutations influence the pathogenesis, phenotype, and outcome of myeloproliferative neoplasms (MPN), little is known about their impact on molecular response to cytoreductive treatment. Methods We performed targeted next-generation sequencing (NGS) on 202 pre-treatment samples obtained from patients with MPN enrolled in the DALIAH trial (randomized controlled phase III clinical trial, NCT01387763) and 135 samples obtained after 24 months of therapy with recombinant interferon-alpha (IFNα) or hydroxyurea (HU). The primary aim was to evaluate the association between complete clinicohematologic response (CHR) at 24 months and molecular response through sequential assessment of 120 genes using NGS. Results Among JAK2-mutated patients treated with IFNα, those with CHR had a greater reduction in the JAK2 variant allele frequency (VAF) (median 0.29 to 0.07; p<0.0001) compared with those not achieving CHR (median 0.27 to 0.14; p<0.0001). In contrast, the CALR VAF did not significantly decline in neither those achieving CHR nor those not achieving CHR. Treatment-emergent mutations in DNMT3A were observed more commonly in patients treated with IFNα compared with HU, p=0.04. Furthermore, treatment-emergent DNMT3A-mutations were significantly enriched in IFNα treated patients not attaining CHR, p=0.02. A mutation in TET2, DNMT3A, or ASXL1 was significantly associated with prior stroke (age-adjusted OR=5.29 [95% CI, 1.59-17.54]; p=0.007) as was a mutation in TET2 alone (age-adjusted OR=3.03 [95% CI, 1.03-9.01]; p=0.044). Conclusion At 24 months, we found mutation-specific response patterns to IFNα: (1) JAK2- and CALR-mutated MPN demonstrated distinct molecular responses and (2) DNMT3A-mutated clones/subclones emerged on treatment.
Influence of pegylated interferon and ribavirin on insulin resistance and metabolic factors in chronic hepatitis C (link)
Insulin seems to have dropped by 20-25% by week 48.
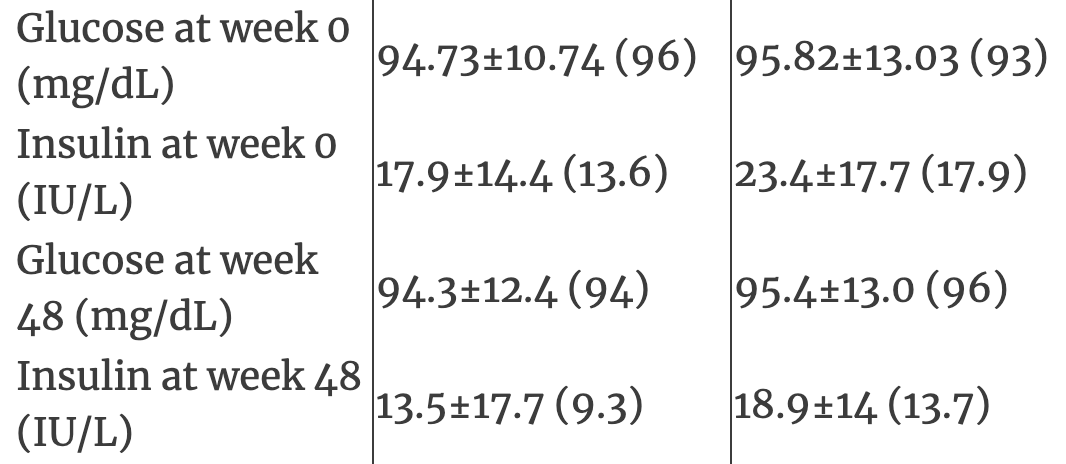
Shows very little change in Homa-IR, Glucose by week 48
Serum hs-CRP was correlated with treatment response to pegylated interferon and ribavirin combination therapy in chronic hepatitis C patients (link)
Hs-CRP level was significantly decreased in 83 patients after peginterferon/ribavirin combination therapy (0.24 vs. 0.62 mg/L, P < 0.001)
Mechanism of Action of Interferon, 2020
Both Type I and II interferons exert their effects through human interferon alfa receptor chains, which activate signaling via the Janus kinase (JAK)-signal transducer and activator of transcription (STAT) pathway [21,22]. The anti-viral properties of interferon have led to its successful use in diseases such as hepatitis B and C and Kaposi sarcoma. Interferon’s mechanism of action in MPNs is less clear. Numerous studies have demonstrated an apoptotic effect on hematopoietic progenitors, with a preference for the mutated clone [23,24]. Colony unit megakaryocyte proliferation is also directly targeted, which likely accounts for interferon’s effects on thrombocytosis. In addition, there is evidence that interferon inhibits thrombopoietin (TPO) activation via suppression of JAK2 substrate phosphorylation [25]. Mouse models have shown that interferon can directly activate dormant hematopoietic stem cells in vivo [26], and specifically can induce differentiation in JAK2 V617F mutated quiescent stem cells [27]. This results in potential long-term depletion of the mutant clone via direct targeting of progenitor cells.
However, interferon also induces broader stimulatory effects on the immune system, enhancing surveillance and targeting of the mutant clone. Studies have demonstrated that interferon augments T-cell, macrophage, and natural killer cell activity, and increases expression of tumor-associated and major histocompatibility complex antigens [28,29,30].
Mechanisms of action of IFN-alpha2 (link)
Weight loss during pegylated interferon and ribavirin treatment of chronic hepatitis C*, 2005
Treatment of hepatitis C virus (HCV) infection with interferon (IFN)-alpha, as monotherapy or in combination with ribavirin, is associated with significant side-effects including weight loss. The aim of our study was to describe the evolution of body weight during combination antiviral treatment and to examine the possible determinants of weight loss. This was a retrospective analysis of 126 patients who received combination therapy of pegylated IFN-alpha-2b and ribavirin at our unit. Body weight was recorded at each outpatient attendance during treatment and follow-up, and was expressed as a percentage of baseline value. We observed a decline of body weight during treatment. Median (range) weight values at 4, 12, 24, and 48 weeks (expressed as percentage of baseline weight) were 97.7 (91.5-110.2), 95.4 (84.4-109.4), 93.7 (80.8-106.5), and 91.1 (80.1-103.6) respectively. There was no significant association of increased weight loss with age, gender, pretreatment weight, ethnicity, pretreatment histological stage, cumulative IFN dose (adjusted for body weight), HCV genotype or treatment outcome. Median body weight returned to baseline within 6 months of stopping treatment. Patients experience significant weight loss during combination therapy. Those experiencing greater weight losses during therapy did not benefit from improved antiviral response.
White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study, 2015

https://ash.confex.com/ash/2020/webprogram/Paper141796.html
Update on Long-acting Interferons for MPN, 2016
https://www.youtube.com/watch?v=lp58hdmZTIE
Managing Polycythemia Vera in 2021 - Dr. Richard T. Silver
https://www.youtube.com/watch?v=Qi1MSJjTxgk
https://www.practiceupdate.com/content/ash-2019-interferon-alfa-treatment-offers-best-outcomes-in-polycythemia-vera/94020
Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study
https://pubmed.ncbi.nlm.nih.gov/32014125/
Based on this publication, the sooner you get on it the better. It will help you control your JAK2 allele %, which has a doubling time of 1.4 yrs or so:
https://onlinelibrary.wiley.com/doi/full/10.1002/cam4.2741
[1] Interferon in Polycythemia Vera (PV) Yields Improved Myelofibrosis-Free and Overall Survival (Dec 2020 conference publication)
[2] Final Results of Prospective Treatment with Pegylated Interferon Alfa-2a for Patients with Polycythemia Vera and Essential Thrombocythemia in First and Second-Line Settings (Nov 2019)
[3] Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study (link)
[4] Can pegylated interferon improve the outcome of polycythemia vera patients? (2017 journal article)
[5] Update on Long-acting Interferons for MPN, 2016 (link)
[6] Managing Polycythemia Vera in 2021 - Dr. Richard T. Silver (link)
[7] Long-Term Efficacy and Safety of Recombinant Interferon Alpha-2 Vs. Hydroxyurea in Polycythemia Vera: Preliminary Results from the Three-Year Analysis of the Daliah Trial - a Randomized Controlled Phase III Clinical Trial (2018)
[8] Use of Interferon Alfa in the Treatment of Myeloproliferative Neoplasms: Perspectives and
Review of the Literature
Based on [1], Interferon was superior to Hydrea in terms of overall survival and progression-free survival. (Small study, but this is what you get with a rare disease.)
Based on [3], another peg-interferon formulation was shown superior to control disease blood markers over 1+ yr time horizon over Hydrea. This formulation recently applied for FDA approval.
Based on all of the above, a significant percentage (20-30%) of interferon treated PV patients go into deep molecular remission, where the disease practically disappears. It's more targeted. Hydrea never does that.
From what I read Interferon is considered a valid option especially for younger patients. I'm on 90mcg weekly (not the full 180mcg Hep C dose).
Here's a snippet (2020 summary article). Basically, I was naturally concerned about being on a chemo pill (Hydrea) for decades. A targeted option looked a bit more appealing.
I finally got a report from the doctor on my Jak2 mutation, and upon reading it I noticed that it says 78% of my cells have this mutation. I'm just wondering if that means it's more advanced or progressive? Does anyone here have any ideas? I will ask my doctor too at my next appointment.
Shannon Chen
We have a lot of patients in this group experiencing encouraging results from interferon/Pegasys. I’m personally one of them. Make sure you see a good MPN specialist who actually has patients on interferon. It’s all about managing the dosages well and this should be the least scary treatment for us among all. In fact, in the last ASH conferences, Drs published their 10+ years research concluding that interferon is the only drug that lowers mutation AB, and with a possibility of reversing progression. I’m 36 and have been using it for 3 years even through my pregnancies. It saved my life.
-----------
Ianthe Lycos
Wondering if I should stop taking this actually. I have been injecting Pegasys for about 6 months now, 90 mcg once a week as I have been diagnosed by hematologist with Polycythemia Vera ( rare form of blood cancer). The hematologist said there are no side effects. I suspect there are some, because I feel really weak and my lungs are feeling like I have pneumonia all the time. Even so the positive aspect is my blood counts are now normal, the itching skin and massive headache from high blood pressure has stopped. Though I am concerned in that the lung problem and weakness is a side effect of the pegasys drug, and is my body warning me to have a break from it ? :
Marcy Worthington
I, also, suggest you ask about lowering your dose. I, and a number of people I know, only inject 45mcg. Pegasys is actually known for producing adverse effects, but they are often minimized at lower doses. Please also ask your doctors to look for other possible causes of your weakness and lung issues.
Jill Zaitchick
45mcg for 4 plus years --no difficult side effects . Maybe a lower dose would suit you better--ask your Physician . This will possibly reduce your side effects . I have avoided bad side effects--although it has taken me a bit longer to achieve great results --but I have --after the first year on the drug.
Soledad Yukis
You must start for a low doses and growing slowly. This is hormesis training. The body needs time to adapt.
Shelley Herman-Sonnenberg
The starting dose is 45mcg/week. I hope that you are seeing an MPN specialist.
Tammy Bagley
Please speak with your doctor as soon as possible and let them know you are having some issues with your lungs and see if they will reduced your dose to 45 mcg or even 30 mcg for a couple months then increase to 45. If you read the literature from the maker of the drug, Genentech, included with the drug, you will see that some patients have lung issues from taking Pegasys. I too had this side effect when I first started Pegasys at 45 mcg. My doctor reduced the dose to 30 mcg for 2 months, then increased 45 mcg and I no longer had issues with the drug.
https://www.gene.com/patients/medicines/pegasys
Inhibitors of PI3K/Akt and/or mTOR Inhibit the Growth of Cells of Myeloproliferative Neoplasms and Synergize with JAK2 Inhibitor and Interferon (link, patent)
Interferon-α enhances the susceptibility of renal cell carcinoma to rapamycin by suppressing mTOR activity (link)
Combination of valproic acid, everolimus and low dosed interferon alpha provides amplified antineoplastic effects on prostate cancer cells (link)
7th Annual Women & MPN Conference- Dr. Ruben Mesa (link)
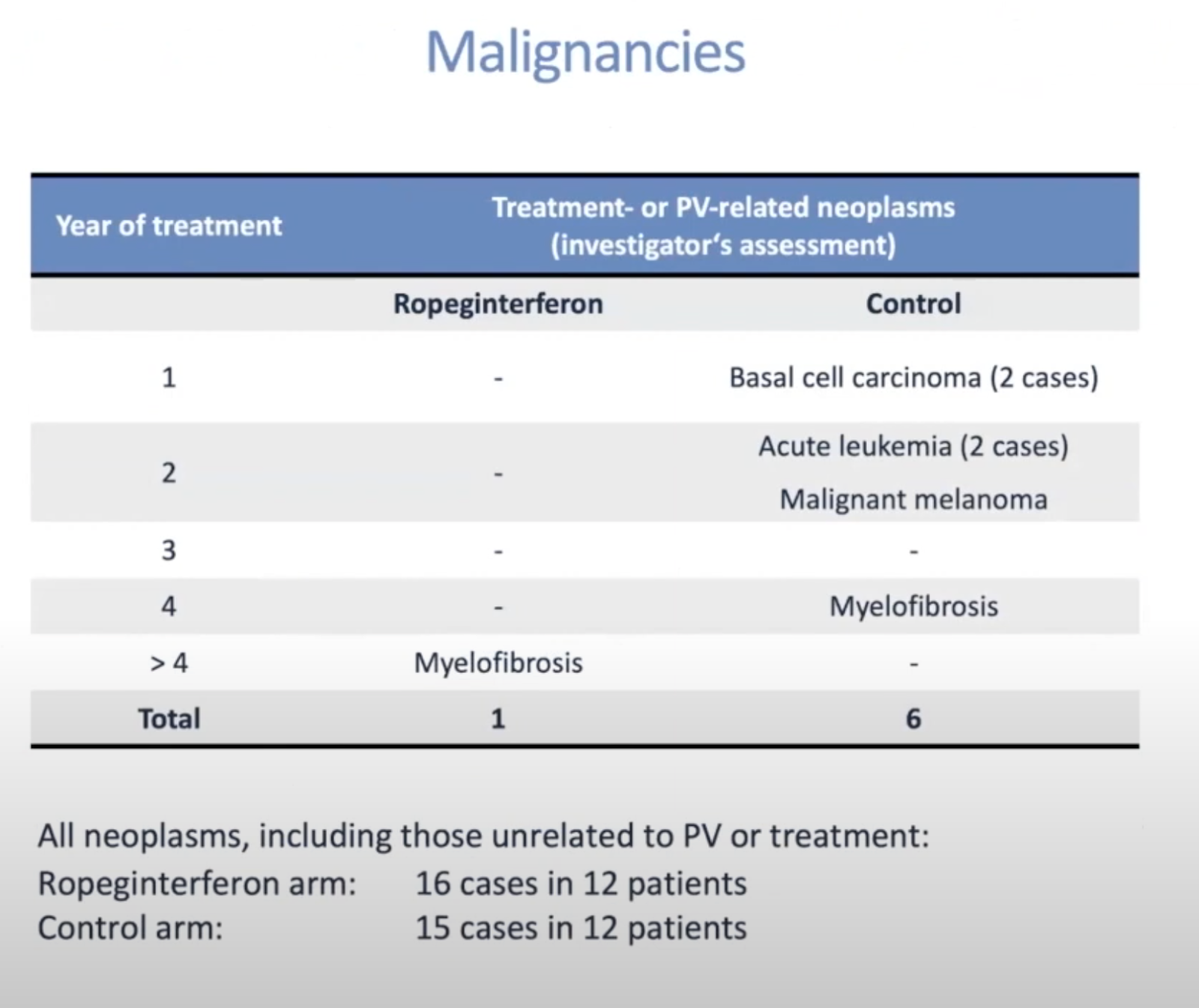

Depletion of Jak2V617F myeloproliferative neoplasm-propagating stem cells by interferon-α in a murine model of polycythemia vera (2013)
Abstract
Interferon-α (IFNα) is an effective treatment of patients with myeloproliferative neoplasms (MPNs). In addition to inducing hematological responses in most MPN patients, IFNα reduces the JAK2V617F allelic burden and can render the JAK2V617F mutant clone undetectable in some patients. The precise mechanism underlying these responses is incompletely understood and whether the molecular responses that are seen occur due to the effects of IFNα on JAK2V617F mutant stem cells is debated. Using a murine model of Jak2V617F MPN, we investigated the effects of IFNα on Jak2V617F MPN-propagating stem cells in vivo. We report that IFNα treatment induces hematological responses in the model and causes depletion of Jak2V617F MPN-propagating cells over time, impairing disease transplantation. We demonstrate that IFNα treatment induces cell cycle activation of Jak2V617F mutant long-term hematopoietic stem cells and promotes a predetermined erythroid-lineage differentiation program. These findings provide insights into the differential effects of IFNα on Jak2V617F mutant and normal hematopoiesis and suggest that IFNα achieves molecular remissions in MPN patients through its effects on MPN stem cells. Furthermore, these results support combinatorial therapeutic approaches in MPN by concurrently depleting dormant JAK2V617F MPN-propagating stem cells with IFNα and targeting the proliferating downstream progeny with JAK2 inhibitors or cytotoxic chemotherapy.
Hydrea / Hydroxyurea
A reappraisal of the benefit-risk profile of hydroxyurea in polycythemia vera: A propensity-matched study (2017)
Here are the key points and conclusions from the research article by Barbui et al. (2017):
The study compared outcomes of phlebotomy (PHL) versus hydroxyurea (HU) for treatment of polycythemia vera (PV) using data from the European Collaborative Low-dose Aspirin (ECLAP) study.
1042 PV patients were selected who received only PHL or HU to maintain hematocrit <45% during follow-up.
Propensity score matching was used to create balanced groups receiving PHL (n=342) or HU (n=681).
Over median 29.9 months (PHL) vs 34.7 months (HU), HU significantly reduced rate of cardiovascular events (5.8 vs 3.0 per 100 person-years, p=0.002), hematologic transformations (1.1 vs 0.1 per 100 person-years, p=0.006) and overall mortality (0.32 vs 0.11 per 100 person-years, p<0.001) compared to PHL.
HU reduced risk of cardiovascular events by 50% (HR 0.50, 95% CI 0.35-0.72) and overall mortality by 67% (HR 0.33, 95% CI 0.20-0.57) versus PHL.
In high-risk patients (age >60 years or prior thrombosis), HU significantly reduced cardiovascular events (8.7 vs 4.8 per 100 person-years), hematologic transformation (1.5 vs 0.1 per 100 person-years) and overall mortality (0.5 vs 0.1 per 100 person-years) compared to PHL.
Higher proportion of HU patients achieved hematocrit <45% and leukocytes <12 x 10^9/L compared to PHL during follow-up.
No difference in outcomes between HU and PHL for low-risk patients.
HU did not increase risk of leukemic transformation versus PHL.
In conclusion, HU significantly reduced cardiovascular events, hematologic transformation, and mortality compared to PHL in high-risk polycythemia vera patients. HU provided superior hematologic control. These results support use of HU as first-line therapy for high-risk polycythemia vera patients.
Different effect of hydroxyurea and phlebotomy on prevention of arterial and venous thrombosis in Polycythemia Vera (2018)
The study by Barbui et al (2019) investigated whether hydroxyurea (HU) or phlebotomy (PHL) is more effective for preventing arterial and venous thrombosis in patients with polycythemia vera (PV). The study was a retrospective analysis of 1042 PV patients from the ECLAP trial who received either HU or PHL as cytoreductive therapy to maintain hematocrit <45%.
A propensity score matching analysis was done to create comparable groups receiving HU (n=634) or PHL (n=317). Groups were well balanced for baseline characteristics like age, gender, cardiovascular risk factors, prior thrombosis, leukocyte count, hematocrit level, etc. During a median follow-up of 2 years, HU significantly reduced non-fatal arterial thrombosis compared to PHL (2.4% vs 6.3%, p=0.002). The rate of arterial thrombosis was 3-fold lower with HU (0.84 per 100 person-years) versus PHL (2.62 per 100 person-years, p=0.001). However, HU and PHL showed comparable efficacy for reducing venous thromboembolism (p=0.574).
The cumulative incidence curves showed the benefit of HU over PHL for lowering arterial thrombosis was observed both in patients with and without prior thrombosis history. But no difference was seen between HU and PHL for cumulative incidence of venous thrombosis.
The key numerical results from Barbui et al are:
634 PV patients received hydroxyurea with median treatment duration of 24 months
317 PV patients received phlebotomy alone with median treatment duration of 25.8 months
Arterial thrombosis occurred in 2.4% of HU patients versus 6.3% of PHL patients (p=0.002)
Rate of arterial thrombosis was 0.84 per 100 person-years on HU versus 2.62 per 100 person-years on PHL (p=0.001)
No difference in venous thromboembolism between HU (10.1%) and PHL (9.5%), p=0.574
Cumulative incidence of arterial thrombosis at 4 years was 2.8% with HU versus 8.5% with PHL (p<0.001)
Cumulative incidence of venous thrombosis at 4 years was 11.4% with HU versus 10.6% with PHL (p=0.715)
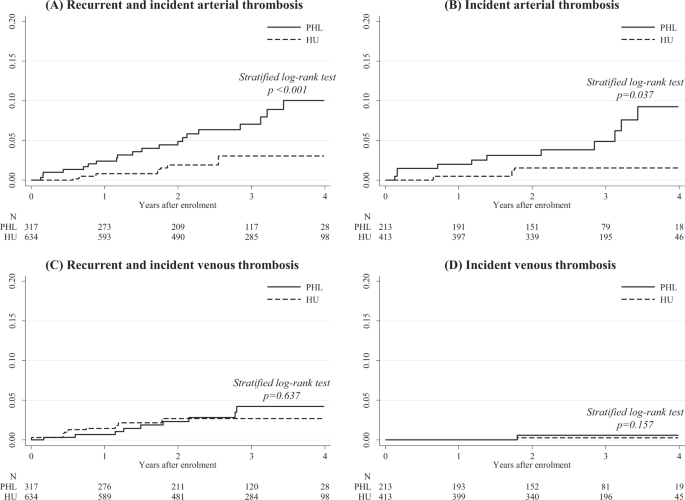
The impact of phlebotomy and hydroxyurea on survival and risk of thrombosis among older patients with polycythemia vera (2018)
The article (Podoltsev et al, 2018) was a retrospective cohort study using data from the SEER-Medicare database to evaluate the real-world effectiveness of phlebotomy and hydroxyurea (HU) for older patients diagnosed with polycythemia vera (PV) from 2007-2013. The study included 820 patients aged 66-99 years at PV diagnosis who were followed for a median of 2.75 years. The main outcomes were overall survival and risk of thrombosis after PV diagnosis.
Key findings:
41.1% of patients received both phlebotomy and HU, 23% received only phlebotomy, 19.6% received only HU, and 16.3% received neither treatment. The median number of phlebotomies was 7 and median HU adherence (percent of days covered) was 61.6%.
37.2% of patients died during follow-up. Median survival was significantly longer for phlebotomy users (6.29 years) vs nonusers (4.5 years) and for HU users (6.02 years) vs nonusers (5.25 years).
In multivariable Cox models adjusting for demographics, comorbidities, and healthcare access:
Phlebotomy use was associated with a 35% lower mortality risk compared to nonuse. Each additional phlebotomy per year was associated with a 29% lower mortality risk.
Each 10% increase in HU adherence was associated with an 8-9% lower mortality risk.
36.1% of patients experienced a thrombotic event. The rate was significantly lower for phlebotomy users (29.3%) vs nonusers (46%) and for HU users (27.6%) vs nonusers (45.4%).
In multivariable competing risk models:
Phlebotomy use was associated with a 48% lower risk of thrombosis compared to nonuse. More phlebotomies per year was associated with lower thrombosis risk.
Each 10% increase in HU adherence was associated with an 8% lower thrombosis risk.
Older age, male sex, ≥2 comorbidities, and no flu shot were associated with higher mortality. ≥2 comorbidities and low income were associated with higher thrombosis risk.
The authors conclude that phlebotomy and HU were associated with improved survival and lower thrombosis risk in older PV patients, but appear to be underutilized in real-world practice. They suggest improved guideline dissemination and implementation could improve outcomes.
Phlebotomy and Hydroxyurea Are Underused in Patients With Polycythemia Vera, 2018
Real-world treatments and thrombotic events in polycythemia vera patients in the USA (2023)
This real-world retrospective study by Verstovsek et al. (2023) examined treatment patterns, hematocrit control, and thrombotic event rates in 28,306 patients diagnosed with polycythemia vera (PV) in the United States. The study cohort was identified using medical and pharmacy claims data from 2011-2019. Patients were stratified into high-risk (age ≥60 years or history of thrombosis) and low-risk groups.
The key findings and conclusions were:
60% of high-risk and 83% of low-risk patients initiated PV treatment with phlebotomy monotherapy. During the median follow-up of 808 days, most patients retained their original therapy (74% high-risk, 81% low-risk).
Only 25% of high-risk patients achieved the hematocrit (HCT) target of <45% recommended by guidelines. Among high-risk patients on phlebotomy monotherapy, just 16% maintained HCT <45%, compared to 29% on hydroxyurea and 40% on combination therapy.
64% of low-risk patients on phlebotomy monotherapy had HCT levels above 50% at some point, versus 14% who always maintained HCT <45%. Low-risk patients on hydroxyurea or combination therapy had better HCT control.
16% of all patients experienced a thrombotic event after PV treatment initiation, including 20% of high-risk and 8% of low-risk patients. Stroke (36%) and deep vein thrombosis (35%) were the most common events.
Among the high-risk patients who had a thrombotic event, 45% were treated with phlebotomy monotherapy and never switched therapies.
In summary, the study found suboptimal HCT control in both high- and low-risk PV patients, with phlebotomy monotherapy being associated with the poorest control. A significant proportion of patients, especially high-risk, experienced thrombotic events despite access to recommended therapies.
The authors conclude that available PV treatments may not be utilized to their full potential in real-world practice. The heavy reliance on phlebotomy monotherapy likely contributes to the suboptimal HCT control and ongoing risk of thrombotic complications seen in this cohort.
A randomized phase 3 trial of interferon-α vs hydroxyurea in polycythemia vera and essential thrombocythemia (2022): MPD-RC 112 Trial
This randomized phase 3 trial compared pegylated interferon-alpha-2a (PEG) to hydroxyurea (HU) in 168 treatment-naive, high-risk patients with essential thrombocythemia (ET) or polycythemia vera (PV).
Key eligibility criteria:
High-risk ET or PV per WHO criteria
High-risk factors included age ≥60 years, history of thrombosis, high platelet count, symptoms, or comorbidities requiring treatment
Treatment arms:
PEG: 45 μg weekly subcutaneous injections, titrated up to 180 μg weekly (n=82)
HU: 500 mg twice daily oral, with dose adjustments as needed (n=86)
Primary endpoint:
Complete response (CR) rate at 12 months, defined by ELN criteria
Key Results:
CR rates at 12 months were 37% for HU vs 35% for PEG (p=0.80), not statistically significant.
Overall response rates (CR + PR) were 70% for HU vs 78% for PEG at 12 months (p=0.22).
In PV patients, 12-month CR rates were 30% for HU vs 28% for PEG; hematocrit control was achieved in 43% vs 65%, respectively (p=0.04).
Platelet control rates in ET patients were similar between HU (45%) and PEG (46%) at 12 months.
At 24 months, CR rates were 20% for HU vs 29% for PEG; overall response rates were 41% vs 60% (p=0.045).
Median JAK2V617F allele burden reductions were -5.3% for HU vs -10.7% for PEG at 12 months. Burden decreased further through 24 months with PEG but increased after 12 months with HU.
Histopathologic responses were more frequent with HU (23%) than PEG (5%) at 12 months (p=0.01).
Serious adverse events were more common with PEG (46%) than HU (28%) (p=0.01).
Limitations:
Trial closed early after enrolling 168 out of target of 300 patients due to lack of drug availability.
Limited power to detect differences in thrombosis rates between arms.
Short follow-up time of maximum 3 years.
Conclusions:
At 12 months, no significant difference in CR rates between HU and PEG in high-risk ET/PV patients.
Longer treatment with PEG appeared more effective in controlling counts and reducing mutation burden, while HU had higher histopathologic response rates.
Both agents limited thrombotic events and progression despite these differences.
PEG had a less favorable toxicity profile than HU.
Results support both drugs as effective options requiring individualized choice.
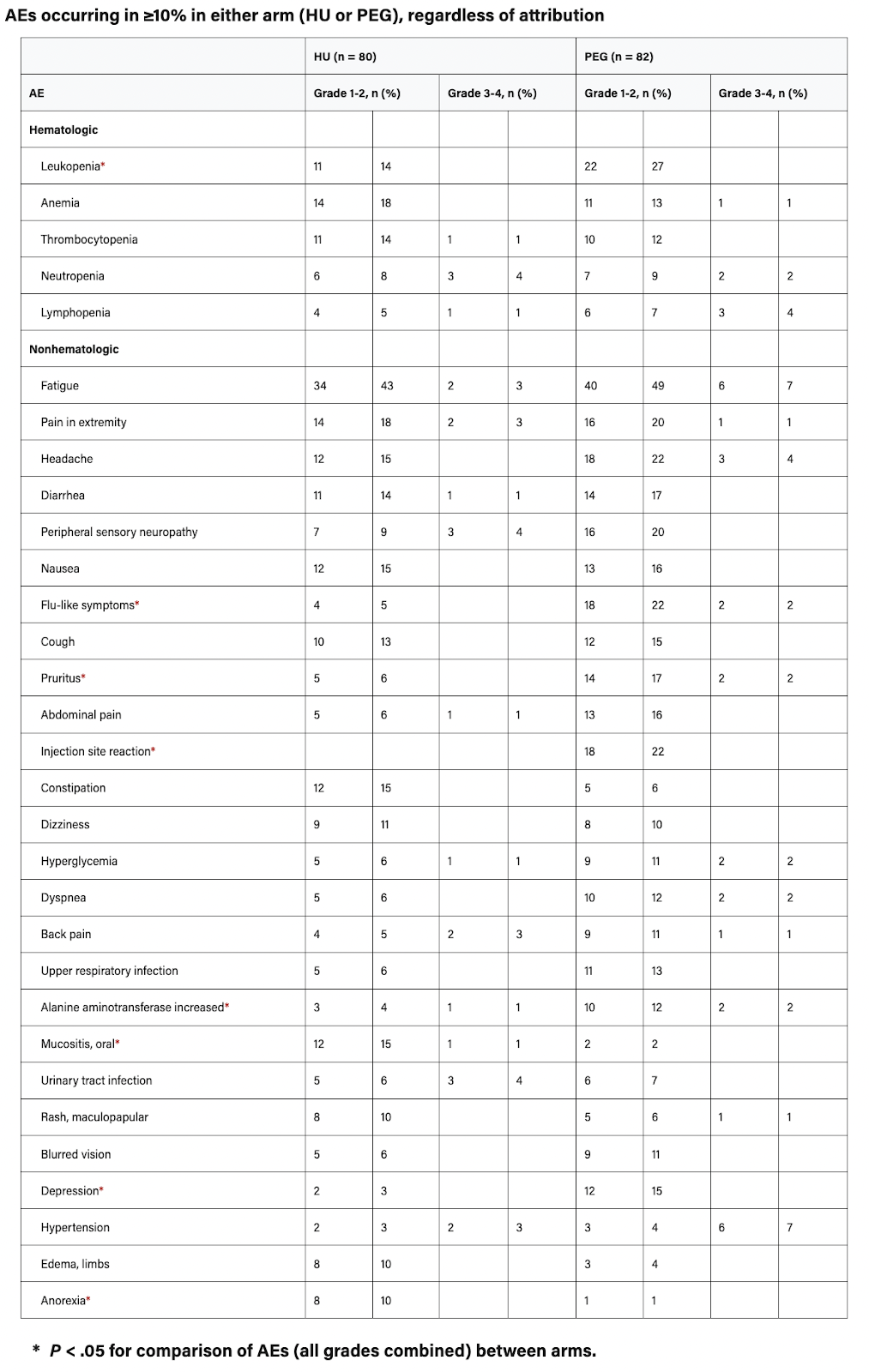
Low doses of DNA damaging agents extend Saccharomyces cerevisiae (yeast) chronological lifespan by promoting entry into quiescence, 2018
Recent research has shown that mild stresses, through a process called hormesis, can extend lifespan in various species. The specific stresses that induce hormesis vary by genotype, and the mechanisms are not fully understood. A new study found that low doses of DNA damaging or replication stress agents like hydroxyurea, methyl methanesulfonate, 4-nitroquinoline 1-oxide, and Zeocin lengthened lifespan in yeast if exposure occurred during growth but not stationary phase. These treatments did not affect mitochondrial activity, increase general stress resistance, or induce mitohormesis. Instead, they increased the proportion of quiescent cells in stationary phase populations. Further, deleting genes influencing quiescence prevented the lifespan extension, suggesting mild DNA damage promotes longevity by enhancing quiescence, elucidating a new hormetic mechanism relevant to healthy aging.
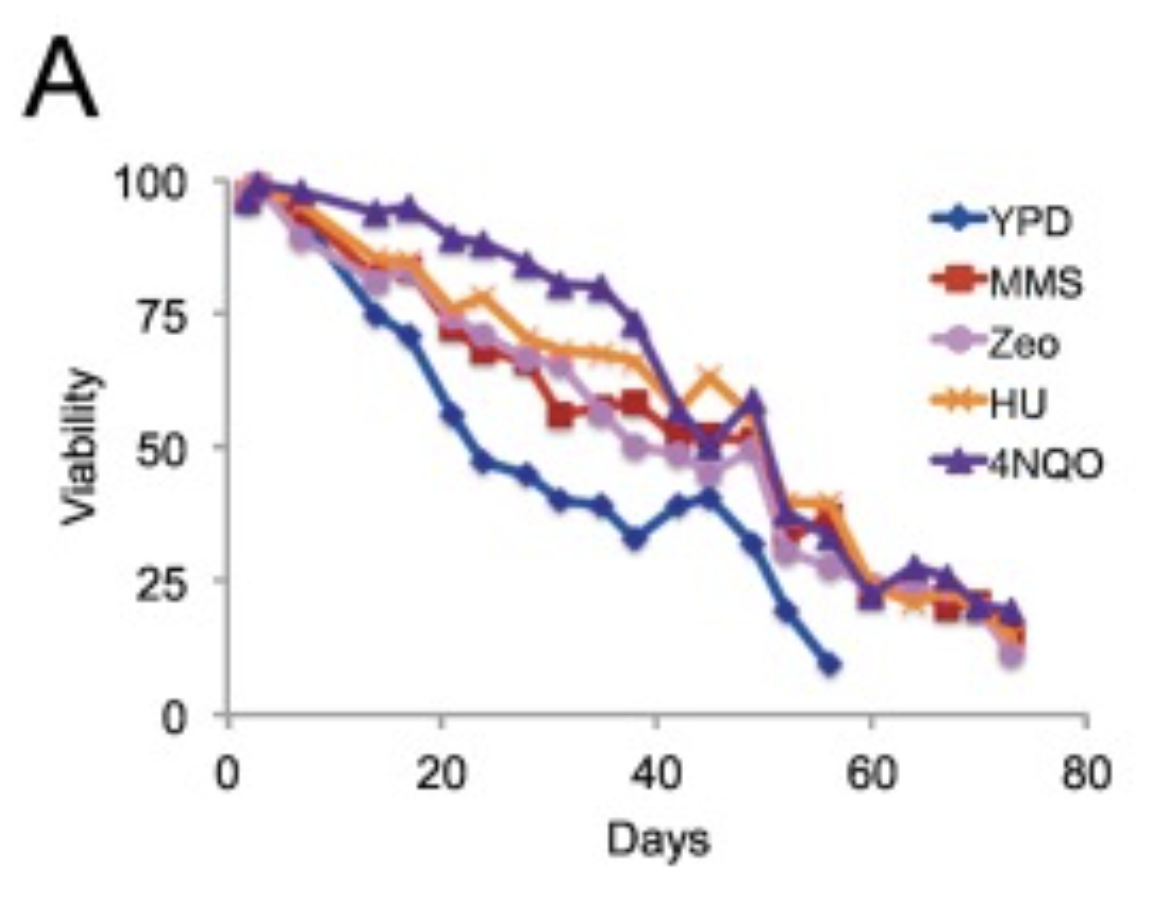
Chemotherapy With Hydroxyurea (NSC-32065) in Renal Cell Carcinoma. (1968)
Eighteen patients with metastatic renal cell carcinoma were treated with hydroxyurea. Of 14 patients who received more than 50 Gm total dose, five have shown objective responses lasting two to five months. Drug-induced toxicity con- sisted of bone marrow depression and mild to moderate gastrointestinal toxicity and was readily reversible upon drug withdrawal. Further clinical studies with hydroxyurea in kidney carcinoma are indicated to assess its antineoplastie effect in a larger number of patients with this type of tumor.

A pilot study of low dose hydroxyurea as a novel resistance modulator in metastatic renal cell cancer (2000)
Mechanisms of chemoresistance in renal cell carcinoma include P-glycoprotein, overexpression of multidrug resistance-1 (mdr1) gene, and unstable chromosomal aberrations. In vitro exposure of resistant tumor cells to low dose hydroxyurea causes loss of chromosomal aberrations, decrease in the mdr1 gene copies, and increased sensitivity to vinblastine. Patients received continuous hydroxyurea 500 mg every Monday, Wednesday and Friday. Vinblastine 5 mg/m2 was given intravenously on days 1 and 8 every 21 days. Seventeen patients with a median age of 63 (range 40-80) received a median of 3 courses of vinblastine (range 1-14). Toxicities included: > or = grade 3 non-hematologic toxicity (1) and febrile neutropenia (2). No treatment related mortality occurred. Three patients (17.6%) had partial responses. The median survival was 38.0 weeks (95% CI = 26.9-49.1 weeks). The addition of hydroxyurea given at the dose of 500 mg orally three times weekly had no major impact on the expected antitumor effect of vinblastine.
Jakafi / Ruxolitinib
Ruxolitinib (Jakafi), a Janus-associated kinase (JAK1/JAK2) inhibitor, was approved by the FDA in December 2014 for the treatment of patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea. Approval was based on data from the phase III RESPONSE trial.Aug 20, 2019
Ruxolitinib Versus Best Available Therapy for Polycythemia Vera Intolerant or Resistant to Hydroxycarbamide in a Randomized Trial (2023)
The MAJIC-PV study by Harrison et al (2023) was a randomized phase II trial evaluating the long-term efficacy and safety of ruxolitinib versus best available therapy (BAT) in patients with high-risk polycythemia vera (PV) who were resistant or intolerant to hydroxyurebamide (HC-INT/RES). 180 patients were randomized to receive ruxolitinib (n=93) or BAT (n=87), with a median follow-up of 4.8 years.
The most frequent BATs were hydroxycarbamide (32%), interferon (15%), and combination of hydroxycarbamide and interferon (12%; Data Supplement [Table S3]).
The primary endpoint was complete response (CR) rate at 1 year, defined as hematocrit <45% without phlebotomy for 3 months, platelets ≤400 x 109/L, white blood cells ≤10 x 109/L, and normal spleen size. CR at 1 year was achieved in 43% on ruxolitinib versus 26% on BAT (P=0.02). Ruxolitinib was associated with more durable CR compared to BAT. The overall response rate was 97% for ruxolitinib versus 93% for BAT.
Ruxolitinib significantly improved event-free survival (EFS) compared to BAT, with a hazard ratio (HR) of 0.58 (P=0.03). EFS was defined as time to major thrombosis, major hemorrhage, transformation to myelofibrosis/AML, or death. Patients achieving CR within 1 year also had superior EFS (HR 0.41, P=0.01). Thrombosis-free survival was improved with ruxolitinib (HR 0.56, P=0.05). Progression-free survival showed a trend favoring ruxolitinib. Overall survival did not differ between arms.
Molecular response, defined as >50% reduction in JAK2V617F variant allele fraction (VAF), was more frequent with ruxolitinib versus BAT (56% vs 25%, P<0.001). Molecular response at 12 months and at last follow-up was associated with improved EFS, PFS, and overall survival. Ruxolitinib induced substantial reduction in JAK2V617F mutant stem/progenitor cells in patients achieving deep molecular responses.
Additional somatic mutations beyond JAK2V617F were detected in 41% and associated with more events, with ASXL1 mutations conferring highest risk (adjusted HR 3.02, P=0.003). Patients on ruxolitinib had significant and durable improvement in myeloproliferative neoplasm symptom burden versus BAT.
In summary, the MAJIC-PV study demonstrated superior hematologic control, molecular responses, EFS, and symptom benefit with ruxolitinib versus BAT in HC-INT/RES PV. For the first time, attainment of molecular response was shown to correlate with improved EFS, PFS, and overall survival. The results support the use of ruxolitinib and integration of molecular monitoring in high-risk PV resistant/intolerant to hydroxyurea.
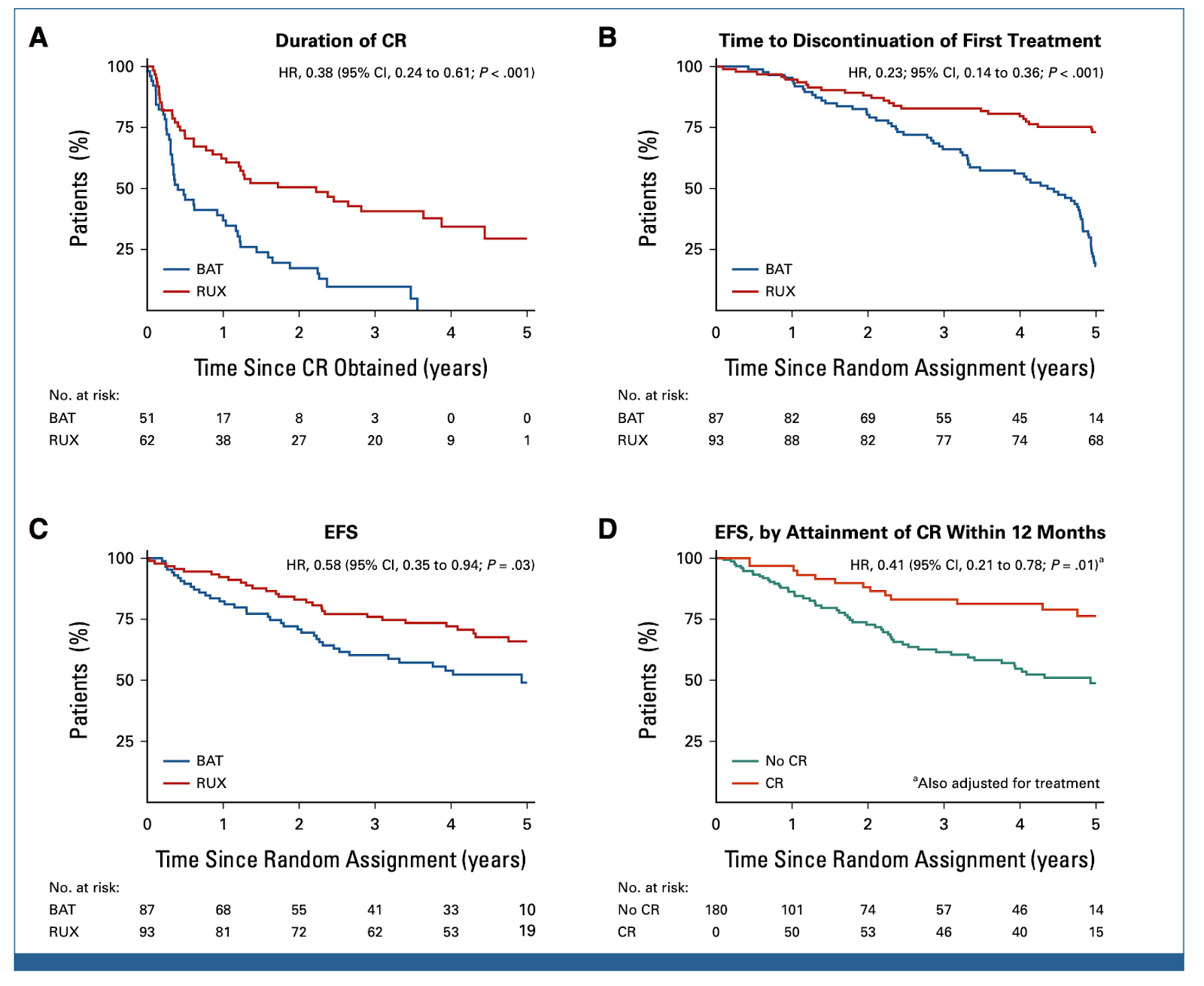
Long-term efficacy and safety of ruxolitinib versus best available therapy in polycythaemia vera (RESPONSE): 5-year follow up of a phase 3 study (2020)
This 5-year follow-up analysis of the phase 3 RESPONSE trial evaluated the long-term efficacy and safety of ruxolitinib versus best available therapy (BAT) in patients with polycythemia vera resistant to or intolerant of hydroxyurea.
At the primary analysis at week 32, 22.7% of patients on ruxolitinib achieved the primary composite endpoint of hematocrit control and ≥35% spleen volume reduction compared to only 0.9% on BAT (p<0.001).
Of the 25 primary responders to ruxolitinib, 6 had progressed by 5 years. The probability of maintaining primary response at 5 years was 0.74 (95% CI: 0.51-0.88).
26 patients achieved complete hematologic remission (CHR) with ruxolitinib at week 32, with 10 progressing by week 256. The probability of maintaining CHR at 5 years was 0.55 (95% CI: 0.32-0.73).
70 patients achieved overall clinicohaematologic response with ruxolitinib at week 32, with 21 progressing by week 256. The probability of maintaining this response at 5 years was 0.67 (95% CI: 0.54-0.77).
The probability of maintaining ≥35% spleen volume reduction at 5 years was 0.72 (95% CI: 0.34-0.91).
In the intention-to-treat analysis, overall survival at 5 years was 91.9% with ruxolitinib versus 91.0% with BAT (HR 0.95; 95% CI: 0.38-2.41).
Greater reductions in JAK2 V617F allele burden and improvements in quality of life were observed with long-term ruxolitinib treatment compared to BAT.
The safety profile of long-term ruxolitinib was consistent with previous reports, with anemia and thrombocytopenia being the most common hematologic adverse events. Rates of non-hematologic adverse events and infections were lower with ruxolitinib versus BAT.
Rates of thromboembolic events were lower with ruxolitinib compared to BAT. No new safety signals were identified.
In summary, this 5-year analysis of the RESPONSE trial showed that ruxolitinib provides durable efficacy and has an acceptable long-term safety profile in polycythemia vera patients resistant to or intolerant of hydroxyurea. The results support ruxolitinib as a viable long-term treatment option for these patients.
Long Term Survival in Myelofibrosis Improved with Early Use of Jakafi (2023)
Verstovsek et al. (2012) conducted a double-blind, placebo-controlled trial of ruxolitinib (Jakafi) in 309 patients with intermediate-2 or high-risk primary myelofibrosis, post-polycythemia vera myelofibrosis, or post-essential thrombocythemia myelofibrosis. Patients were randomized 1:1 to receive either ruxolitinib (n=155) or placebo (n=154).
Key conclusions:
A spleen response (≥35% reduction in spleen volume from baseline) occurred in 41.9% of ruxolitinib patients compared to 0.7% of placebo patients (p<0.001).
46.2% of ruxolitinib patients had a ≥50% reduction in symptom score compared to 5.3% of placebo patients (p<0.001).
After a median follow-up of 51 weeks, 8.0% of ruxolitinib patients and 13.7% of placebo patients had died (HR 0.51, 95% CI 0.27–0.99; p=0.041).
Ruxolitinib therapy was associated with anemia and thrombocytopenia but these were generally manageable with dose modifications or transfusions.
Verstovsek et al. (2013) reported 3-year efficacy and safety data from the COMFORT-II trial comparing ruxolitinib to best available therapy (BAT) in 219 patients with primary myelofibrosis, post-polycythemia vera myelofibrosis, or post-essential thrombocythemia myelofibrosis. Patients were randomized 2:1 to receive ruxolitinib (n=146) or BAT (n=73).
Key conclusions:
41.7% of ruxolitinib patients had a ≥35% spleen volume reduction from baseline at week 144 compared to 0.9% of BAT patients.
47.7% of ruxolitinib patients had a ≥50% reduction in symptom score at week 144 compared to 4.9% of BAT patients.
Estimated 3-year overall survival was 79.9% in the ruxolitinib group compared to 61.4% in the BAT group (HR 0.48, 95% CI 0.28-0.85; p=0.009).
Anemia and thrombocytopenia remained common but manageable toxicities with long-term ruxolitinib treatment.
Passamonti et al. (2014) compared survival from diagnosis in 100 patients receiving ruxolitinib from the COMFORT-2 trial to 350 patients receiving conventional therapy from the Dynamic International Prognostic Scoring System (DIPSS) cohort.
Key conclusions:
Median survival was 5 years with ruxolitinib compared to 3.5 years with conventional therapy.
8-year survival probability was 32.2% with ruxolitinib compared to 15.9% with conventional therapy.
Ruxolitinib was associated with improved survival after adjusting for age and IPSS risk category.
Cervantes et al. (2013) analyzed 5-year efficacy and safety data from COMFORT-I and COMFORT-II in patients treated with ruxolitinib.
Key conclusions:
Patients initially randomized to ruxolitinib had longer median overall survival compared to patients initially randomized to control therapies (5.3 years vs 2.3 years for COMFORT-I; not reached vs 5.3 years for COMFORT-II).
Survival advantage was greatest in patients starting ruxolitinib treatment early after diagnosis compared to later treatment.
Ruxolitinib provided durable reductions in spleen volume and symptom burden over 5 years.
No new safety signals emerged with longer-term ruxolitinib treatment.
In summary, the COMFORT-I and COMFORT-II trials demonstrated that ruxolitinib significantly reduces spleen volume, improves debilitating symptoms, and prolongs overall survival compared to placebo, best available therapy, or conventional treatments in patients with myelofibrosis. The survival advantage appears greatest when ruxolitinib is used as initial therapy soon after diagnosis rather than later in the disease course. Ruxolitinib is associated with increased risks of anemia and thrombocytopenia, but these side effects are generally manageable. The 5-year data confirm the long-term efficacy and safety of ruxolitinib in myelofibrosis patients. Based on these pivotal trials, ruxolitinib received FDA approval in 2011 as the first targeted therapy specifically for myelofibrosis.
Combining ruxolitinib with hydroxyurea yielded an 85% clinical response rate in a study of 20 myelofibrosis patients with hyperproliferative disease. (Pugliese et al., 2019)
Improved Survival of Patients with Myelofibrosis in the Last Decade (2020)
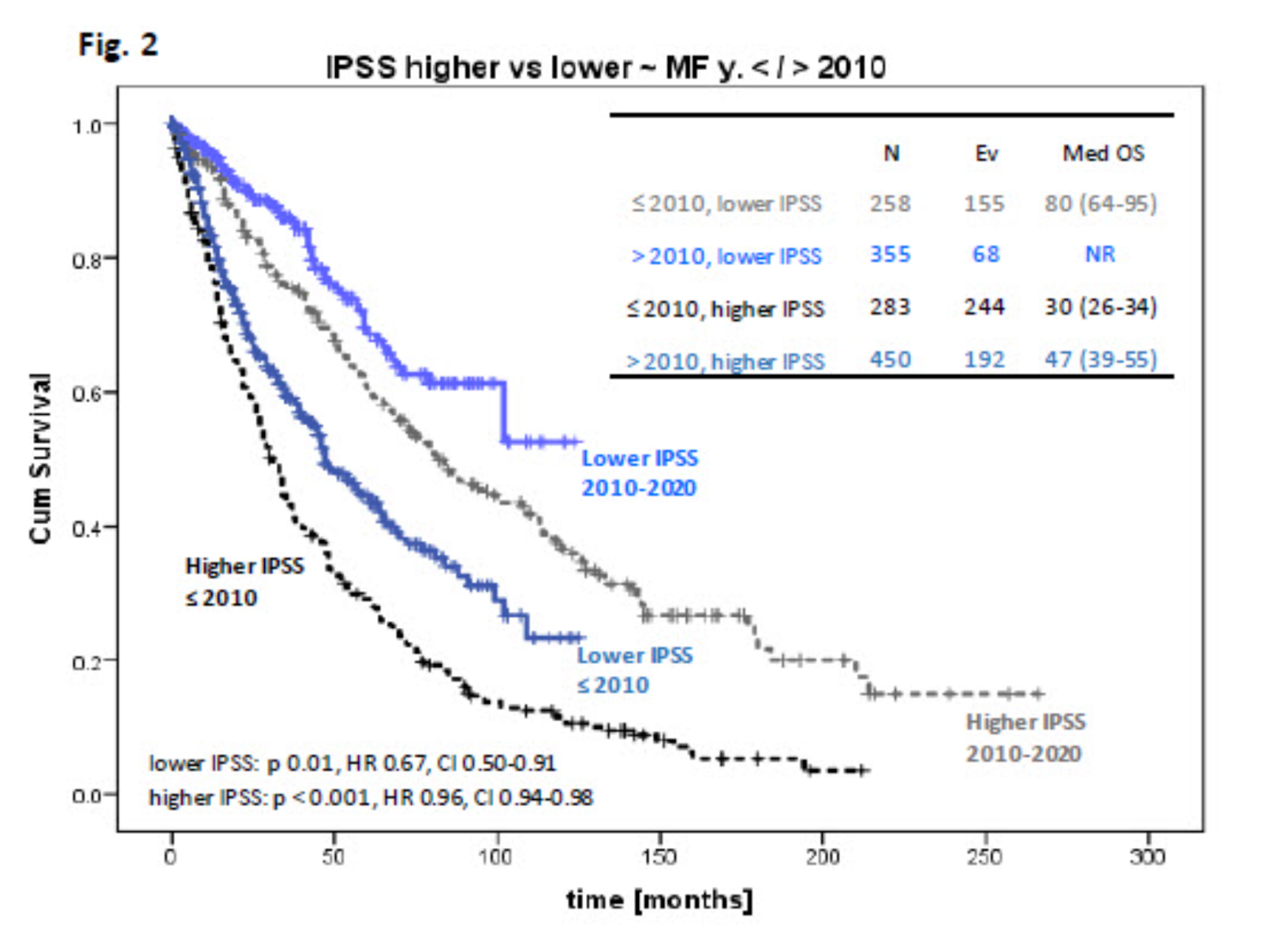
Introduction: The myeloproliferative neoplasm myelofibrosis (MF) is associated with reduced overall survival (OS) compared to the general population. In 2011, the JAK1/2 inhibitor ruxolitinib, was approved in the USA for the treatment of intermediate and high-risk MF. Long-term follow-up of patients in pivotal phase 3 studies showed survival benefit of ruxolitinib therapy.
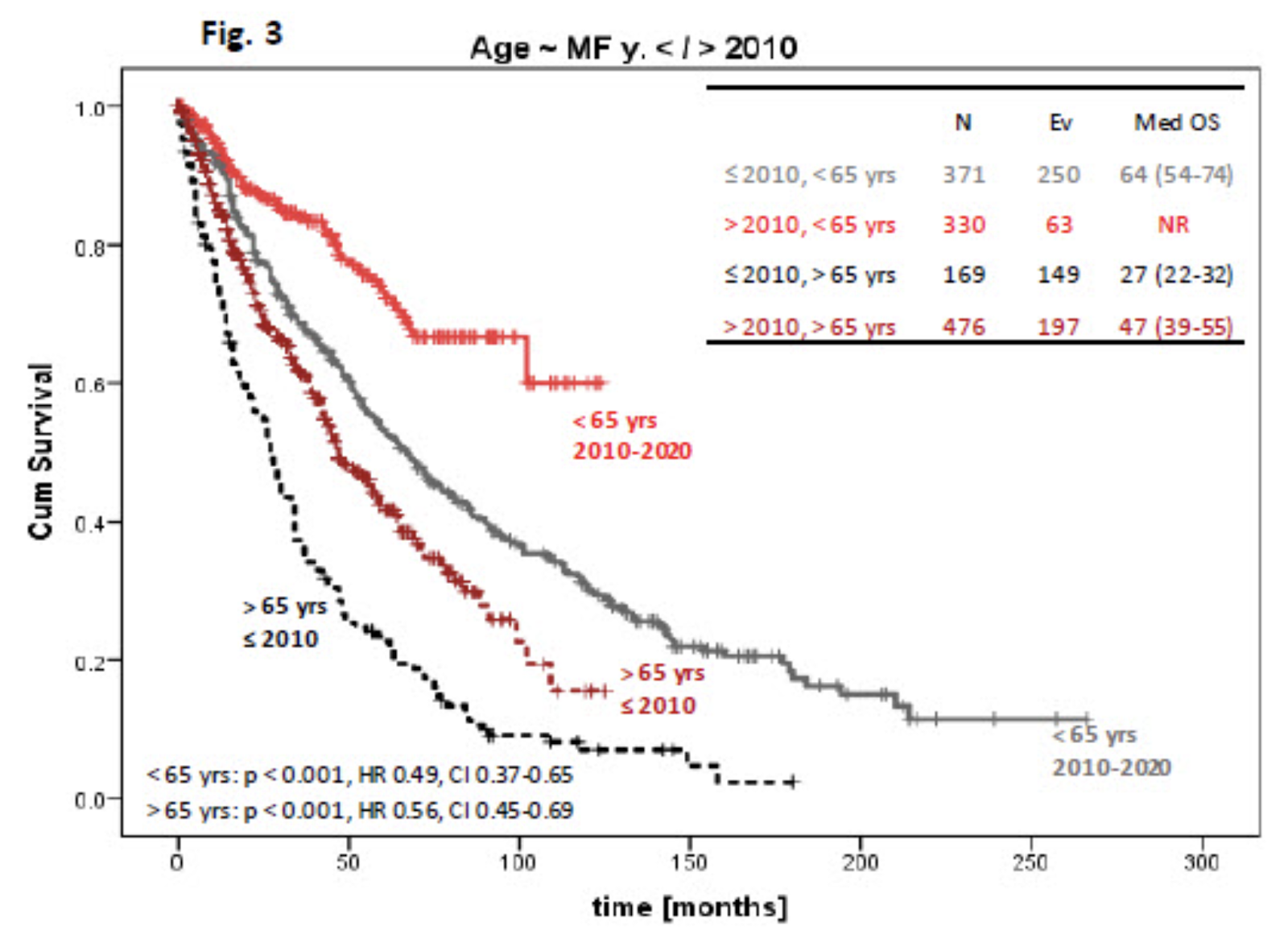
Objective: We sought to evaluate the outcome of patients with MF diagnosed before and after the year of 2010 to assess whether OS changed in the past decade in the era of ruxolitinib.
Methods: We retrospectively reviewed the charts of 1346 patients with MF who presented to our institution in the last 25 years and compared clinical parameters and outcomes between those presented before and after the year of 2010 (before / after y. 2010). Newly diagnosed MF patients and patients within 12 months from diagnosis who were previously only treated with supportive therapy (danazol, growth-factors, steroids) were included. Cytogenetics (≥10 metaphases) was classified according to Gangat, JCO, 2011. Molecular analysis (≥ 28 genes) was performed only after y. 2010 by using next generation sequencing platform. Fisher exact test and χ2 were used for analysis of categorical variables. Overall survival (OS) was estimated using the Kaplan-Meier method and comparison was done by the log-rank test.
Results: Among the 1346 patients, 806 (60%) patients were seen after y. 2010. Median age of all patients was 65 years (range, 20-94), 62% were males. Patient characteristics with comparison between groups are shown in Table 1. Patients after y. 2010 were older, with lower WBC and lower lactate dehydrogenase, but had more symptoms. The distribution of IPSS scores between groups were comparable at around 10% for low, 36% for intermediate-1, 20-25% for intermediate-2 and ~30% for high risk.
Eighty-five and 80% of patients before and after y. 2010, respectively, received therapy for MF at our institution. Overall, 78 patients (37 after y. 2010) underwent stem cell transplantation. Among treated patients at our institution, 25% (n 117) and 37% (n 241) before and after y. 2010 received ruxolitinib during their follow-up. Ruxolitinib therapy was initiated with a median time of 2 months (range, 0.2-156) from presentation to our institution, longer in those before y. 2010 (11 vs 1 months in patients after y. 2010, respectively, p = 0.001)
After a median follow-up of 30.4 months (range, 0.9-266); 659 (49%) of patients died. More deaths were noticed in those before y. 2010 (74% vs 32 %, respectively, p < 0.001); but these patients had also longer follow-up (37.5 months vs 25 months, p < 0.001). Eighty-five patients (10%) developed acute leukemia: 2 cases per 100 person-years per observation for both groups.
Patients after y. 2010 had superior OS to those before y. 2010 with HR 0.7 (95% CI: 0.59-0.82), p < 0.001, Figure 1. Superior OS was observed in all patients after y. 2010 (vs before y. 2010) when stratified by IPSS score (higher equals for combination of int -2 and high, Figure 2), or age (cutoff of 65 years, Figure 3). Patients exposed to ruxolitinib had superior OS regardless of being diagnosed before or after y. 2010, with respective medians of 98 (95% CI: 78-118) and 91 (95% CI: 73-109) months (details to be presented at the conference).
Conclusion: Our results demonstrate that survival of patients with MF has improved in the last decade. Survival has improved in younger and older patients as well as in those with more advanced disease (per IPSS risks). Many factors may have contributed to the observed improvement in outcome of MF patients, including new therapies, e.g. ruxolitinib, as well as improved supportive management and disease awareness.
Adding hydroxyurea in combination with ruxolitinib improves clinical responses in hyperproliferative forms of myelofibrosis (2019)
The study by Pugliese et al (2019) examined the efficacy and safety of adding hydroxyurea to ruxolitinib therapy in patients with myelofibrosis (MF) who had uncontrolled hyperproliferative disease manifestations such as leukocytosis and thrombocytosis while on ruxolitinib monotherapy.
MF is a clonal myeloproliferative neoplasm characterized by bone marrow fibrosis, extramedullary hematopoiesis, and splenomegaly. Patients often have symptoms like fatigue, night sweats, bone pain, and abdominal discomfort due to massive splenomegaly (Tefferi & Vainchenker, 2011). The discovery of dysregulation in the Janus kinase (JAK) pathway led to the development of JAK inhibitors like ruxolitinib which reduce splenomegaly and symptoms in MF patients (Baxter et al., 2005; Kralovics et al., 2005). However, ruxolitinib therapy is frequently limited by dose-dependent cytopenias like thrombocytopenia. Furthermore, patients may develop secondary resistance to ruxolitinib, manifested as loss of spleen response and disease progression with leukocytosis. Adding hydroxyurea, a cytoreductive agent, may help overcome hematological resistance and improve disease control.
The study was a retrospective, multicenter analysis of 20 patients with primary, post-polycythemia vera, or post-essential thrombocythemia MF. Patients had intermediate or high-risk MF per IWG criteria (Cervantes et al., 2009). All patients had received ruxolitinib monotherapy for a median of 15.9 months. 17 patients (85%) started combination therapy due to uncontrolled leukocytosis (median WBC 21.4 x 10^9/L) while 3 patients (15%) started for uncontrolled thrombocytosis (platelet counts 558-2000 x 10^9/L).
Hydroxyurea was added after a median of 6.5 months on ruxolitinib. The starting hydroxyurea dose ranged from 500 mg to >1000 mg daily. 8 patients (40%) were able to increase their ruxolitinib dose by a mean of 5.1 mg twice daily after starting combination therapy. Only 3 patients (15%) required ruxolitinib dose reduction.
After a median follow-up of 12.4 months on combination therapy, 16 of 20 patients (80%) achieved a hematological response. 14 of 17 patients (82.3%) starting for leukocytosis control attained a WBC response. 2 of 3 patients starting for thrombocytosis control attained a platelet response. 12 patients (60%) had clinical improvement in splenomegaly and/or symptoms versus only 8 patients (40%) on ruxolitinib monotherapy.
The combination was well tolerated overall. 8 patients (40%) required hydroxyurea dose reduction for cytopenias. Only 1 patient discontinued ruxolitinib due to thrombocytopenia. The most common adverse event was manageable thrombocytopenia.
In summary, the key conclusions were:
Adding hydroxyurea to ruxolitinib therapy led to high hematological response rates of 80-82% in patients with uncontrolled leukocytosis or thrombocytosis on ruxolitinib monotherapy.
Clinical improvement in splenomegaly and symptoms was seen in 60% with combination therapy versus 40% with ruxolitinib alone.
The combination allowed increased ruxolitinib exposure, with 40% of patients able to escalate ruxolitinib dose by a mean of 5.1 mg twice daily.
The combination was overall well tolerated, with thrombocytopenia being the most common side effect but manageable with dose adjustments.
Only 15% of patients required ruxolitinib dose reduction and 5% discontinued ruxolitinib on combination therapy.
In conclusion, adding hydroxyurea to ruxolitinib improves hematological, clinical, and symptom responses in patients with hyperproliferative MF resistant to ruxolitinib monotherapy. The combination is well tolerated and increases ruxolitinib exposure. Larger prospective studies are warranted to confirm these findings.
Ruxolitinib reduces JAK2 p.V617F allele burden in patients with polycythemia vera enrolled in the RESPONSE study, 2017
In patients with polycythemia vera (PV), an elevated JAK2 p.V617F allele burden is associated with indicators of more severe disease (e.g., leukocytosis, splenomegaly, and increased thrombosis risk); however, correlations between allele burden reductions and clinical benefit in patients with PV have not been extensively evaluated in a randomized trial. This exploratory analysis from the multicenter, open-label, phase 3 Randomized Study of Efficacy and Safety in Polycythemia Vera With JAK Inhibitor INCB018424 Versus Best Supportive Care trial evaluated the long-term effect of ruxolitinib treatment on JAK2 p.V617F allele burden in patients with PV. Evaluable JAK2 p.V617F-positive patients randomized to ruxolitinib (n = 107) or best available therapy (BAT) who crossed over to ruxolitinib at week 32 (n = 97) had consistent JAK2 p.V617F allele burden reductions throughout the study. At all time points measured (up to weeks 208 [ruxolitinib-randomized] and 176 [ruxolitinib crossover]), mean changes from baseline over time in JAK2 p.V617F allele burden ranged from −12.2 to −40.0% (ruxolitinib-randomized) and −6.3 to −17.8% (ruxolitinib crossover). Complete or partial molecular response was observed in 3 patients (ruxolitinib-randomized, n = 2; ruxolitinib crossover, n = 1) and 54 patients (ruxolitinib-randomized, n = 33; ruxolitinib crossover, n = 20; BAT, n = 1), respectively. Among patients treated with interferon as BAT (n = 13), the mean maximal reduction in allele burden from baseline was 25.6% after crossover to ruxolitinib versus 6.6% before crossover. Collectively, the data from this exploratory analysis suggest that ruxolitinib treatment for up to 4 years provides progressive reductions in JAK2 p.V617F allele burden in patients with PV who are resistant to or intolerant of hydroxyurea. The relationship between allele burden changes and clinical outcomes in patients with PV remains unclear.
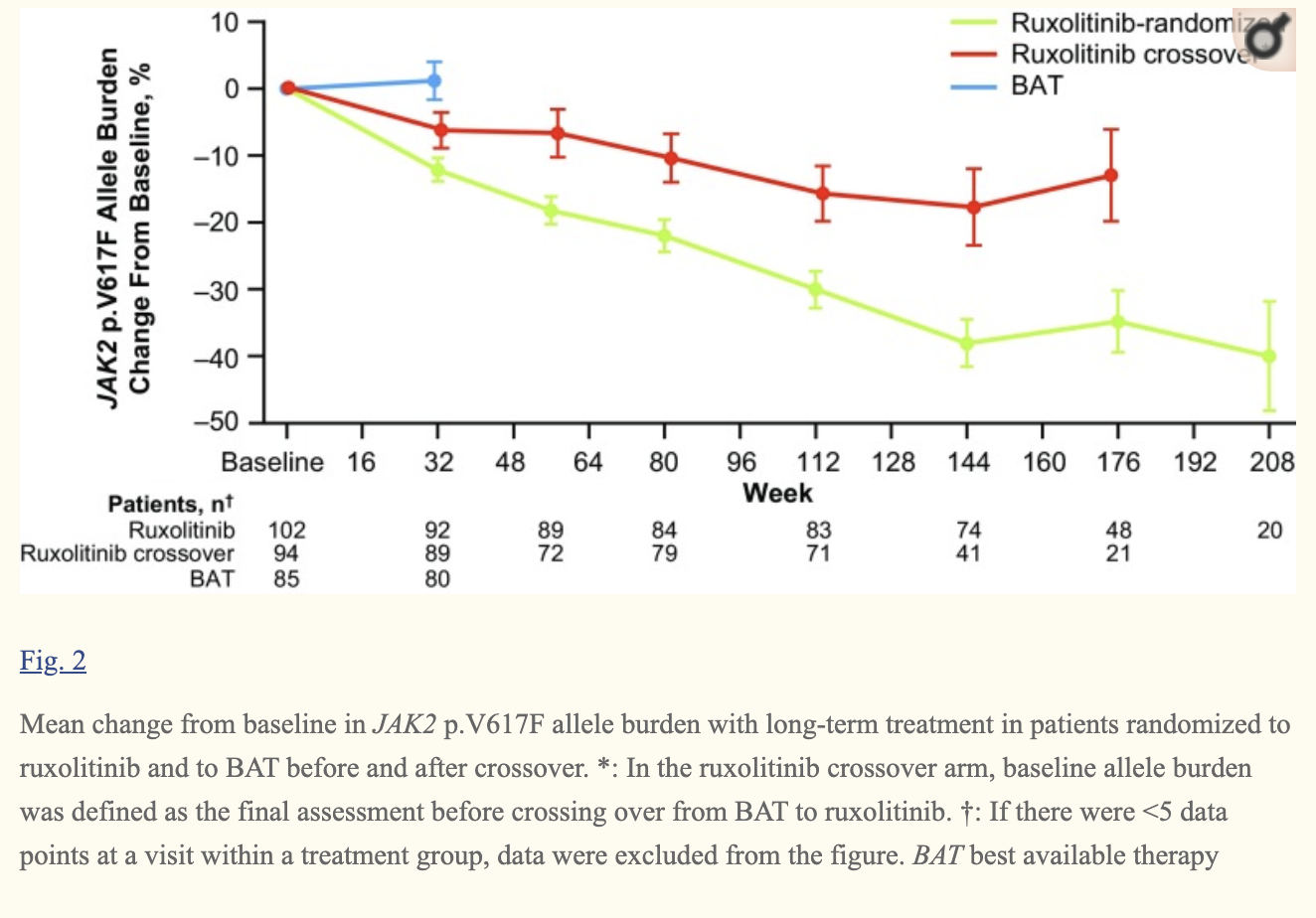
Ruxolitinib and interferon-α2 combination therapy for patients with polycythemia vera or myelofibrosis: a phase II study, 2020
We report the final 2-year end-of-study results from the first clinical trial investigating combination treatment with ruxolitinib and low-dose pegylated interferon-α2 (PEG-IFNα2). The study included 32 patients with polycythemia vera and 18 with primary or secondary myelofibrosis; 46 patients were previously intolerant of or refractory to PEGIFNα2. The primary outcome was efficacy, based on hematologic parameters, quality of life measurements, and JAK2 V617F allele burden. We used the 2013 European LeukemiaNet and International Working Group- Myeloproliferative Neoplasms Research and Treatment response criteria, including response in symptoms, splenomegaly, peripheral blood counts, and bone marrow. Of 32 patients with polycythemia vera, ten (31%) achieved a remission which was a complete remission in three (9%) cases. Of 18 patients with myelofibrosis, eight (44%) achieved a remission; five (28%) were complete remissions. The cumulative incidence of peripheral blood count remission was 0.85 and 0.75 for patients with polycythemia vera and myelofibrosis, respectively. The Myeloproliferative Neoplasm Symptom Assessment Form total symptom score decreased from 22 [95% confidence interval (95% CI):, 16-29] at baseline to 15 (95% CI: 10-22) after 2 years. The median JAK2 V617F allele burden decreased from 47% (95% CI: 33-61%) to 12% (95% CI: 6-22%), and 41% of patients achieved a molecular response. The drop-out rate was 6% among patients with polycythemia vera and 32% among those with myelofibrosis. Of 36 patients previously intolerant of PEG-IFNα2, 31 (86%) completed the study, and 24 (67%) of these received PEG-IFNα2 throughout the study. In conclusion, combination treatment improved cell counts, reduced bone marrow cellularity and fibrosis, decreased JAK2 V617F burden, and reduced symptom burden with acceptable toxicity in several patients with polycythemia vera or myelofibrosis.
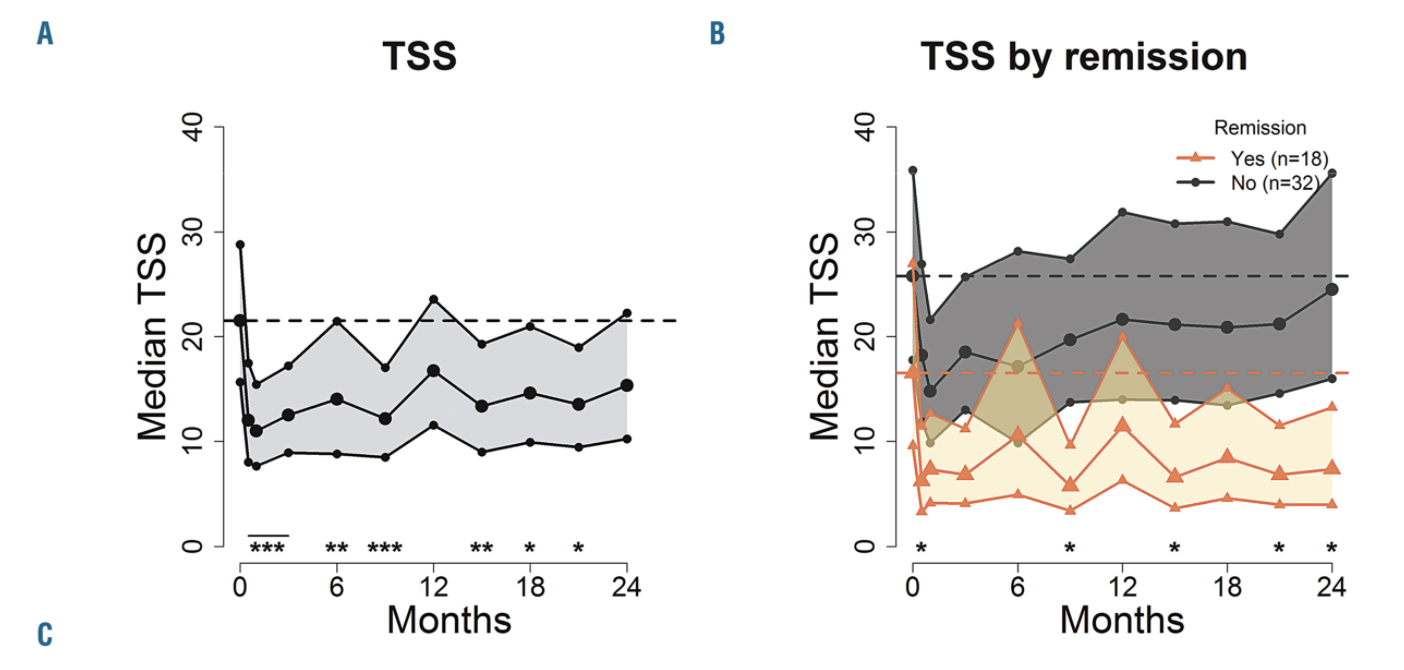

Ruxolitinib Versus Best Available Therapy for Polycythemia Vera Intolerant or Resistant to Hydroxycarbamide in a Randomized Trial (2023): MAJIC-PV
The MAJIC-PV study is a randomized phase II trial evaluating the long-term safety and efficacy of ruxolitinib versus best available therapy (BAT) in 180 patients with high-risk polycythemia vera (PV) who were intolerant or resistant to hydroxycarbamide (HC-INT/RES). The median follow-up was 4.8 years.
The primary endpoint was complete response (CR) rate within 12 months, defined as hematocrit <45% without phlebotomy for 3 months, platelets ≤400 x 109/L, white blood cells ≤10 x 109/L, and normal spleen size. CR was achieved in 43% on ruxolitinib versus 26% on BAT (P=.02). Ruxolitinib was associated with more durable CR than BAT (hazard ratio 0.38, P<.001).
Overall response rates were 97% for ruxolitinib and 93% for BAT. Ruxolitinib patients required fewer phlebotomies despite longer treatment duration (83 versus 307, P<.001). Hemoglobin and hematocrit were lower with ruxolitinib.
Thromboembolic event-free survival was improved with ruxolitinib (hazard ratio 0.56, P=.05). Event-free survival (EFS) was superior for ruxolitinib (hazard ratio 0.58, P=.03) and for those achieving CR within 12 months (hazard ratio 0.41, P=.01).
At last follow-up, larger reductions in JAK2V617F variant allele fraction (VAF) occurred with ruxolitinib (56% had >50% reduction versus 25% on BAT, P<.001). Molecular response (>50% VAF reduction) at 12 months was associated with improved EFS (P=.005). Molecular response at last sample was associated with improved PFS, EFS, and OS (P≤.01).
Additional driver mutations were present in 41% and associated with impaired EFS (hazard ratio 1.92, P=.01). Mutated ASXL1 specifically increased risk (hazard ratio 3.02, P=.003). ASXL1 mutations were over-represented in molecular non-responders.
Ruxolitinib provided durable symptom relief compared to worsening on BAT. Infections, GI disorders, and vascular events were the most frequent adverse events, with more infections on ruxolitinib.
In summary, the MAJIC-PV study demonstrates ruxolitinib provides superior hematologic control, EFS, molecular response, and symptoms in HC-INT/RES PV. Molecular response correlated with clinical outcomes and clearance of mutant stem cells. The data support targeted therapy and molecular monitoring in high-risk PV patients.
Long-term outcomes of ruxolitinib (RUX) therapy in patients (pts) with myelofibrosis (MF): 5-year update from COMFORT-I (2016)
Background: The JAK1/JAK2 inhibitor RUX has demonstrated rapid and durable improvements in splenomegaly and symptoms and improved survival in the phase 3 COMFORT studies in pts with MF. Here we report final long-term safety and efficacy results after 5 years (y) of RUX treatment in COMFORT-I. Methods: In COMFORT-I, 309 pts were randomized (1:1) to RUX or placebo (PBO). RUX starting dose was based on baseline platelet count (100–200×109/L: 15 mg BID; > 200×109/L: 20 mg BID). Pts receiving PBO could crossover to RUX after the primary analysis (when all pts completed week [wk] 24 and half completed wk 36) or at any time if they had prespecified worsening of splenomegaly. The primary endpoint was the proportion of pts achieving ≥ 35% reduction in spleen volume (SV) at wk 24. Overall survival (OS) was estimated by Kaplan-Meier analysis according to randomized treatment.
Results: Median follow-up was 268 wk at the time of this analysis. Of 154 pts randomized to PBO, 111 crossed over to RUX; median time to crossover was 41.1 wk. At wk 24, pts originally randomized to RUX had a mean SV reduction of 31.6%; this was durable for pts who continued on RUX (mean SV reduction at wk 264, 37.6%). Median duration of ≥ 35% SV reduction was 168.3 wk (range, 107.7–NE). OS favored RUX (HR 0.69; 95% CI: 0.50, 0.96; P= 0.025), with 69 and 82 deaths among pts originally randomized to RUX and PBO, respectively. Median OS has not been reached for RUX. Mean platelet count and Hgb initially decreased through 3 mo. Mean Hgb gradually increased toward baseline. After wk 24, mean Hgb and platelet count generally remain stable through 5 y. New onset grade 3 or 4 anemia was 25.2% for the RUX arm and 26.1% for PBO crossover; grade 3 or 4 thrombocytopenia occurred in 12.3% and 13.5% of pts, respectively. Notable AEs included herpes zoster (10.3% and 13.5% of RUX and PBO crossover pts, respectively); basal cell carcinoma (7.7% and 9.0%, respectively); acute myeloid leukemia (5 pts in each arm). Conclusions: After a median follow-up of 268 wk, the hazard ratio for OS favored pts randomized to RUX over those randomized to PBO, and SV reductions were sustained with long-term therapy. Collectively, these data support the durable efficacy and long-term safety of RUX in pts with MF.
Dr. Mesa - MPN Update Summer 2021 (link)
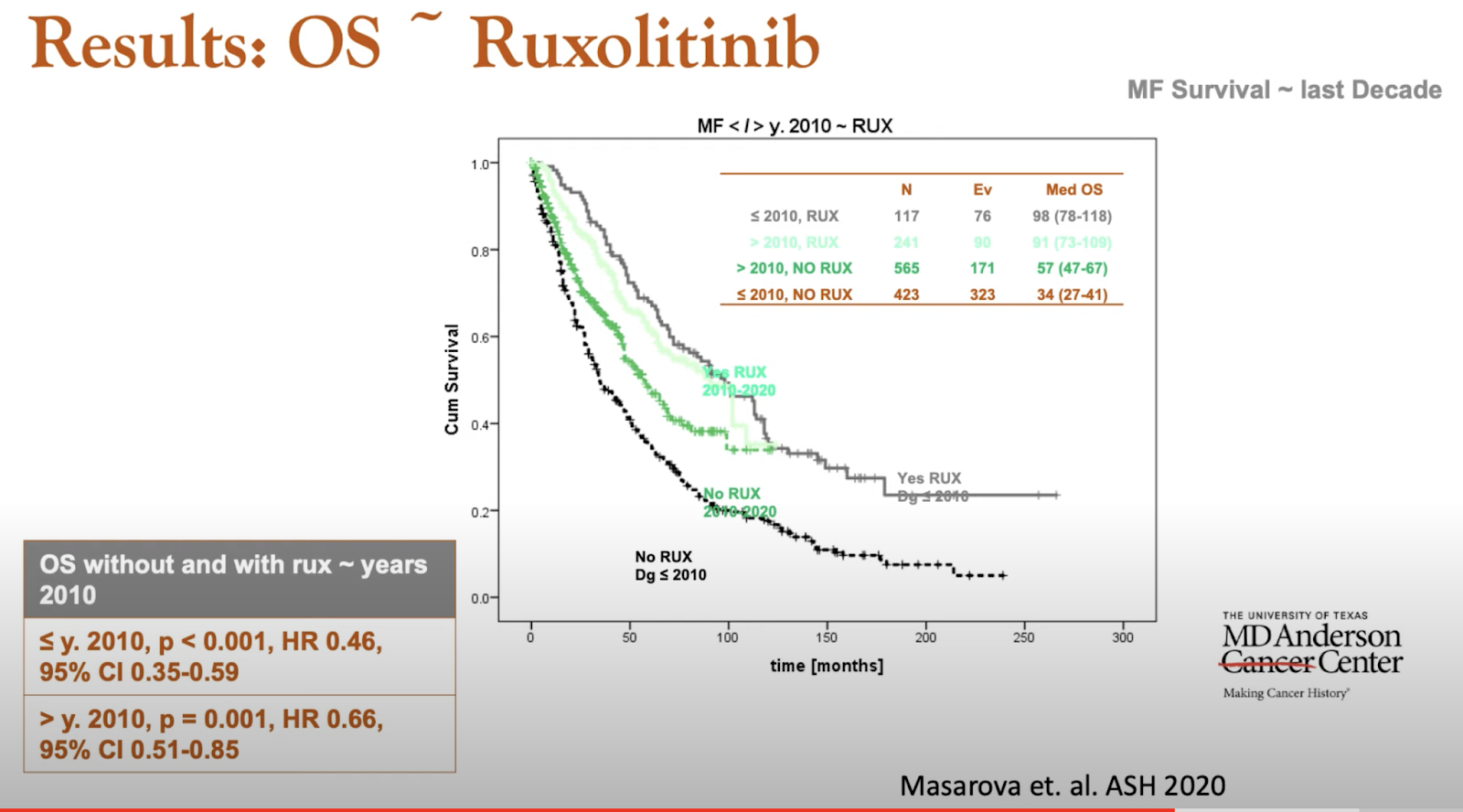
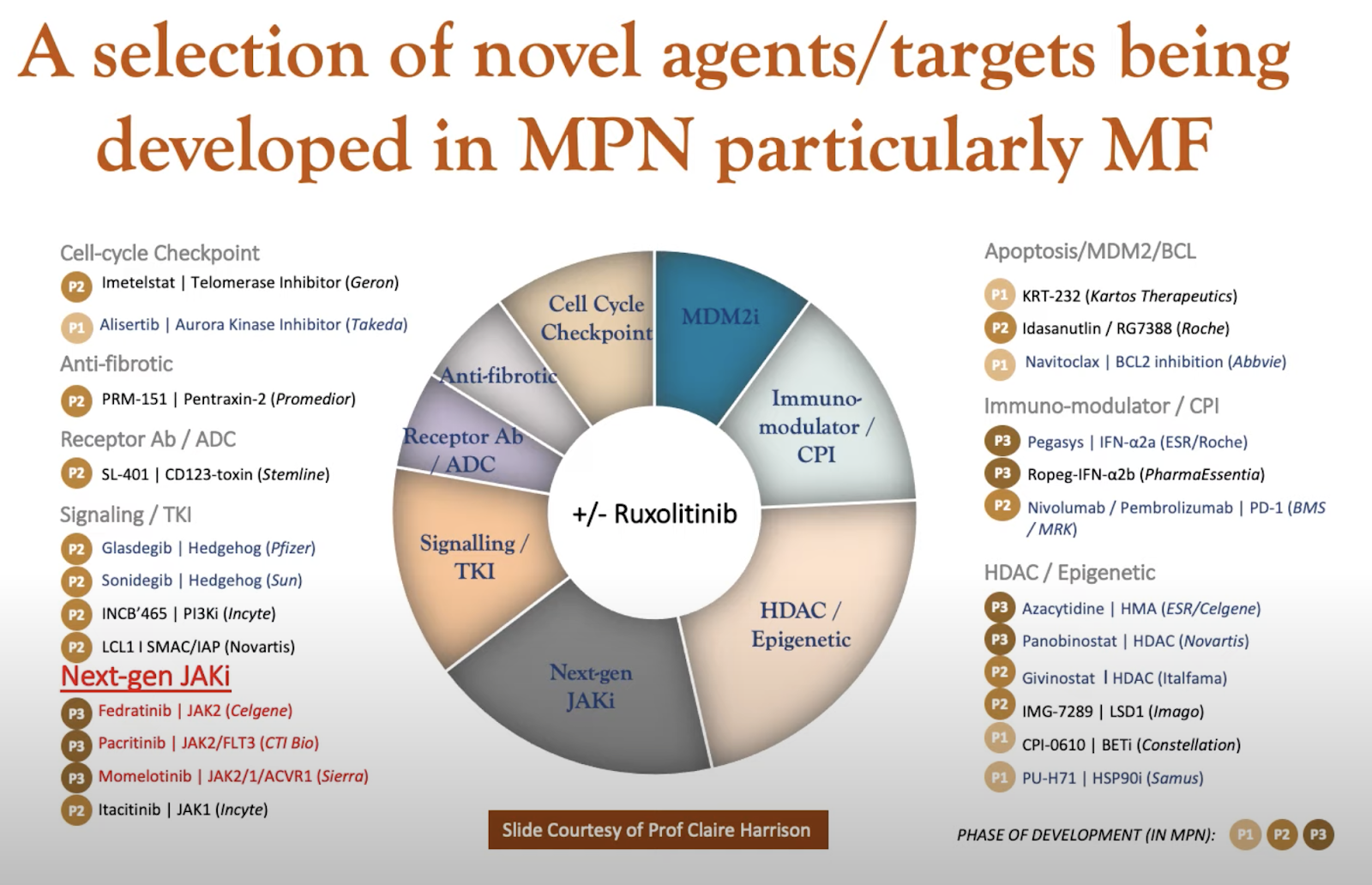
Fedratinib
The U.S. Food and Drug Administration (FDA) has approved fedratinib to treat intermediate-2 or high-risk primary or secondary (post-polycythemia vera or post-essential thrombocythemia) myelofibrosis.Dec 30, 2021
A Look at Fedratinib and the JAKARTA Trials (link)
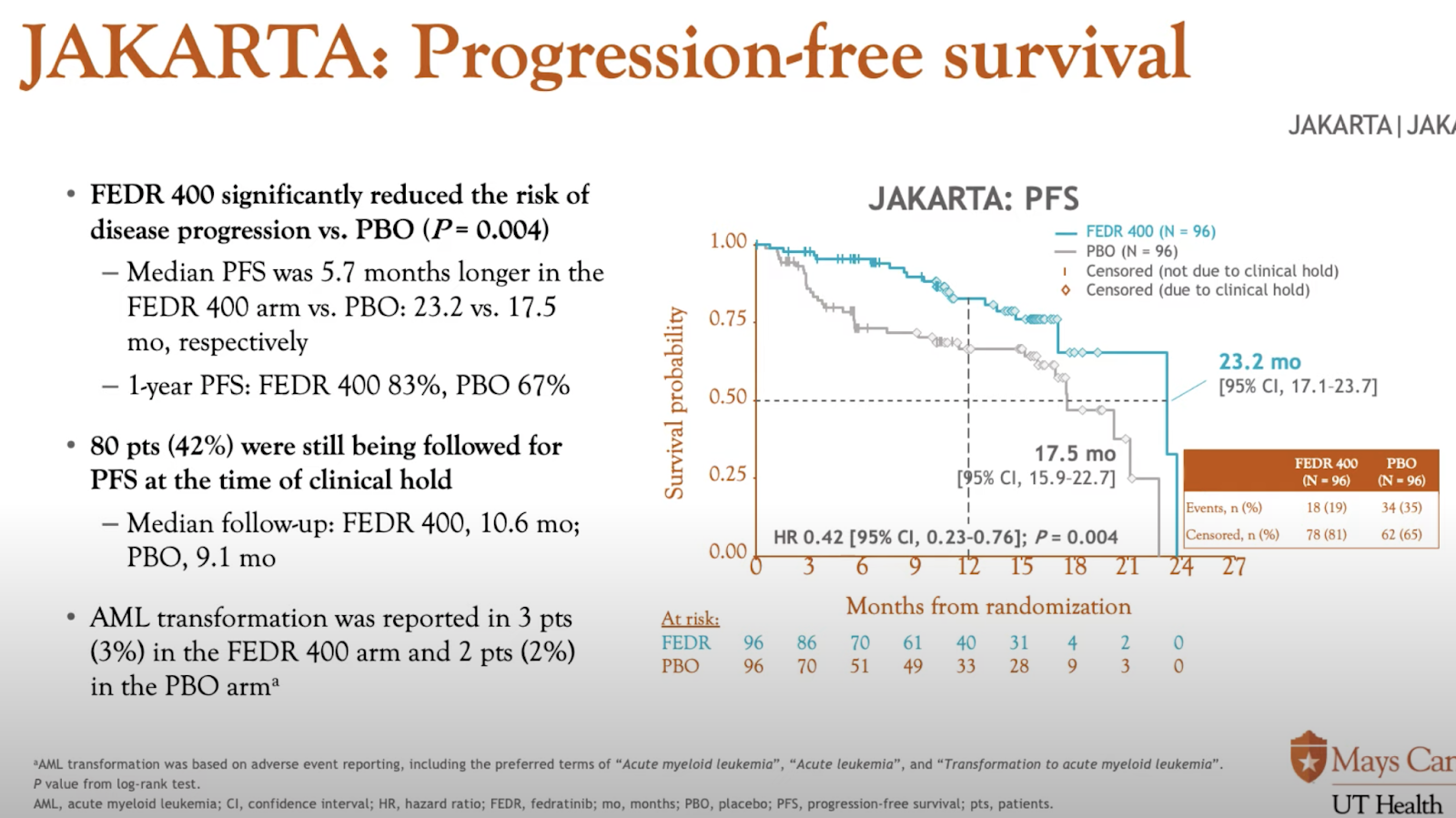
Momelotinib
On September 15 2023, the U.S. Food and Drug Administration (FDA) approved momelotinib (Ojjaara) for the treatment of intermediate- or high-risk myelofibrosis, including primary myelofibrosis or secondary myelofibrosis (post–polycythemia vera and post–essential thrombocythemia), in adults with anemia.
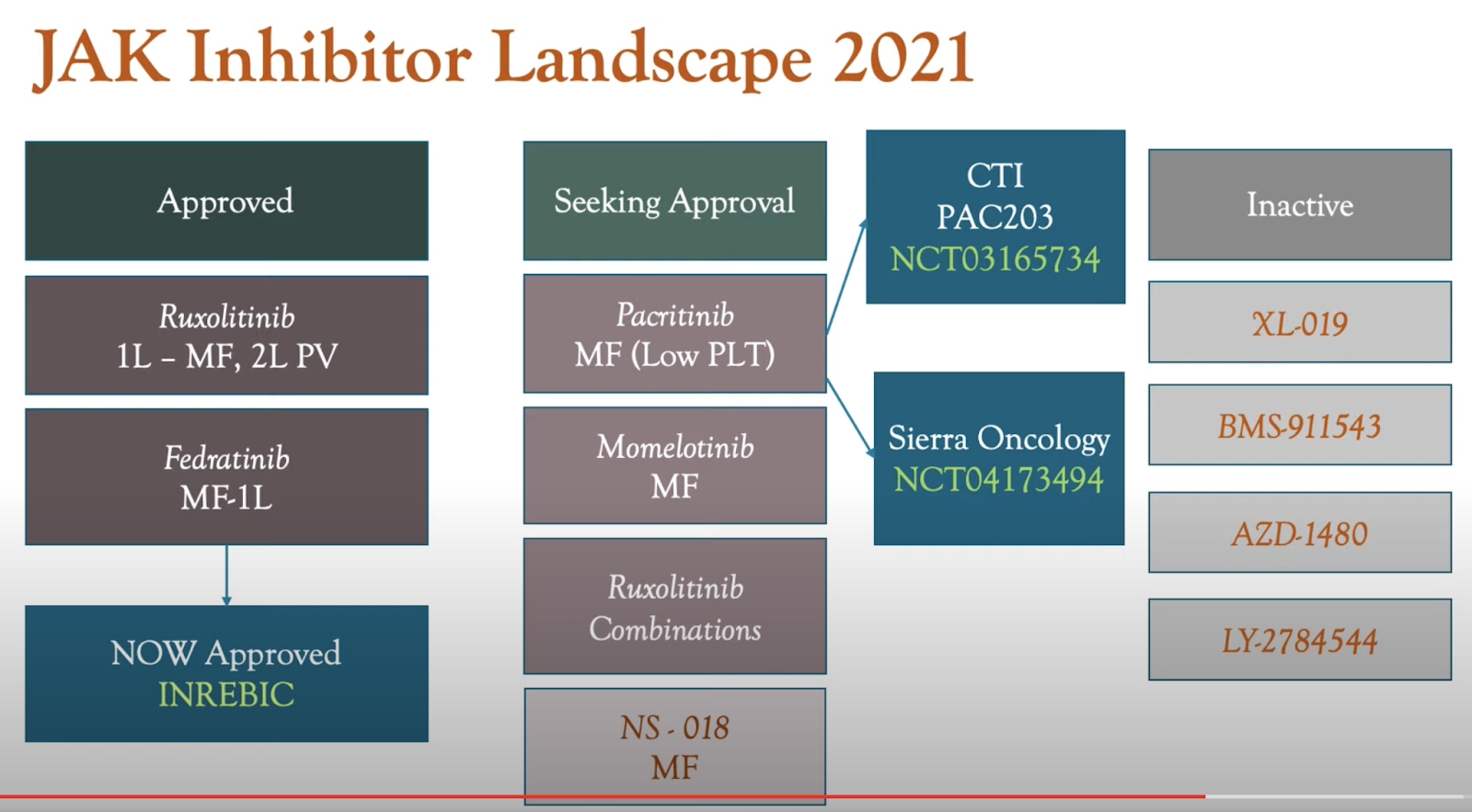
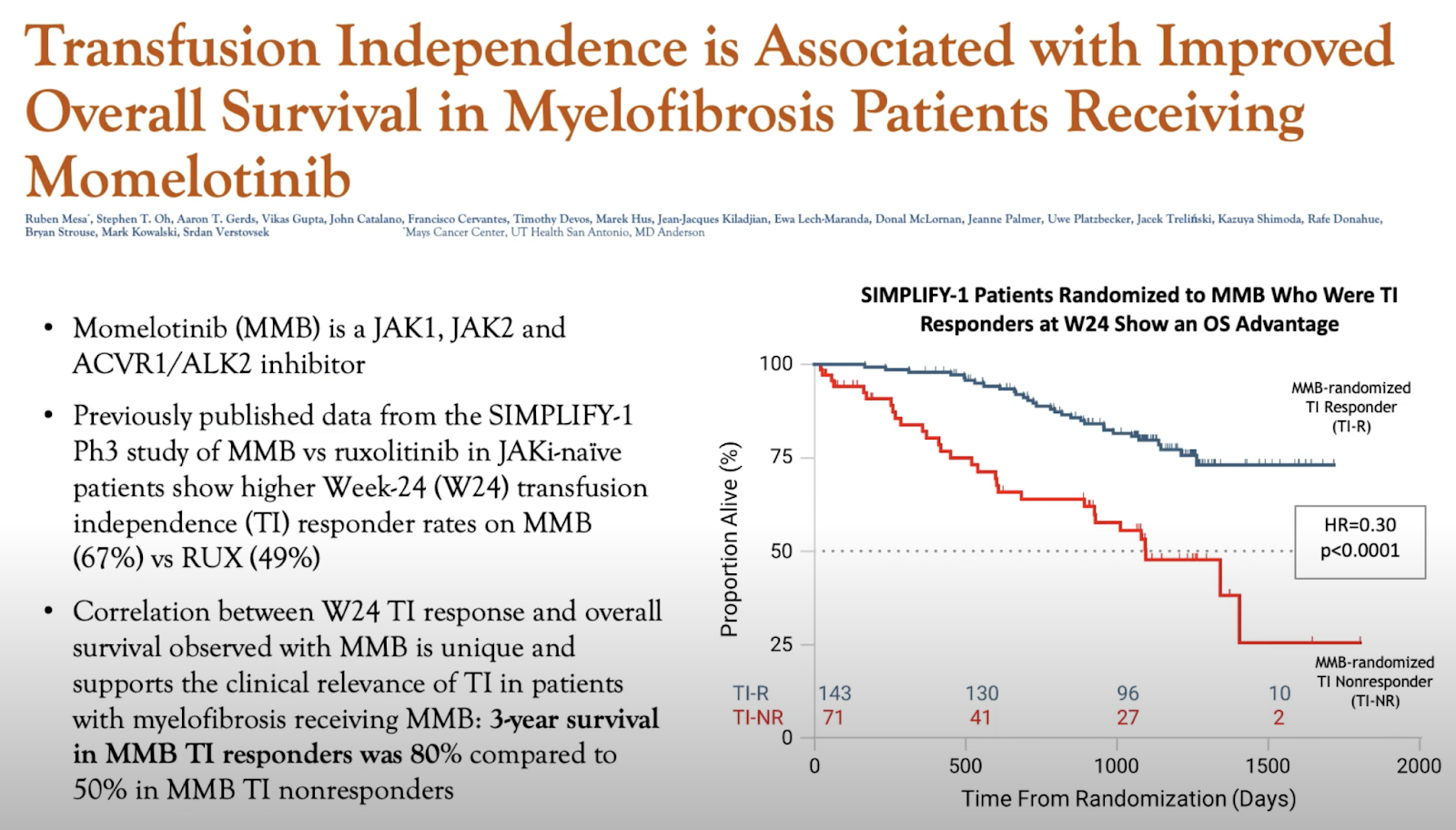
Treatments in the Clinical Pipeline for PV & MPNs
Selinexor
Selinexor (KPT-330) is a first in class nuclear transport inhibitor currently in clinical trials as an anti-cancer agent.
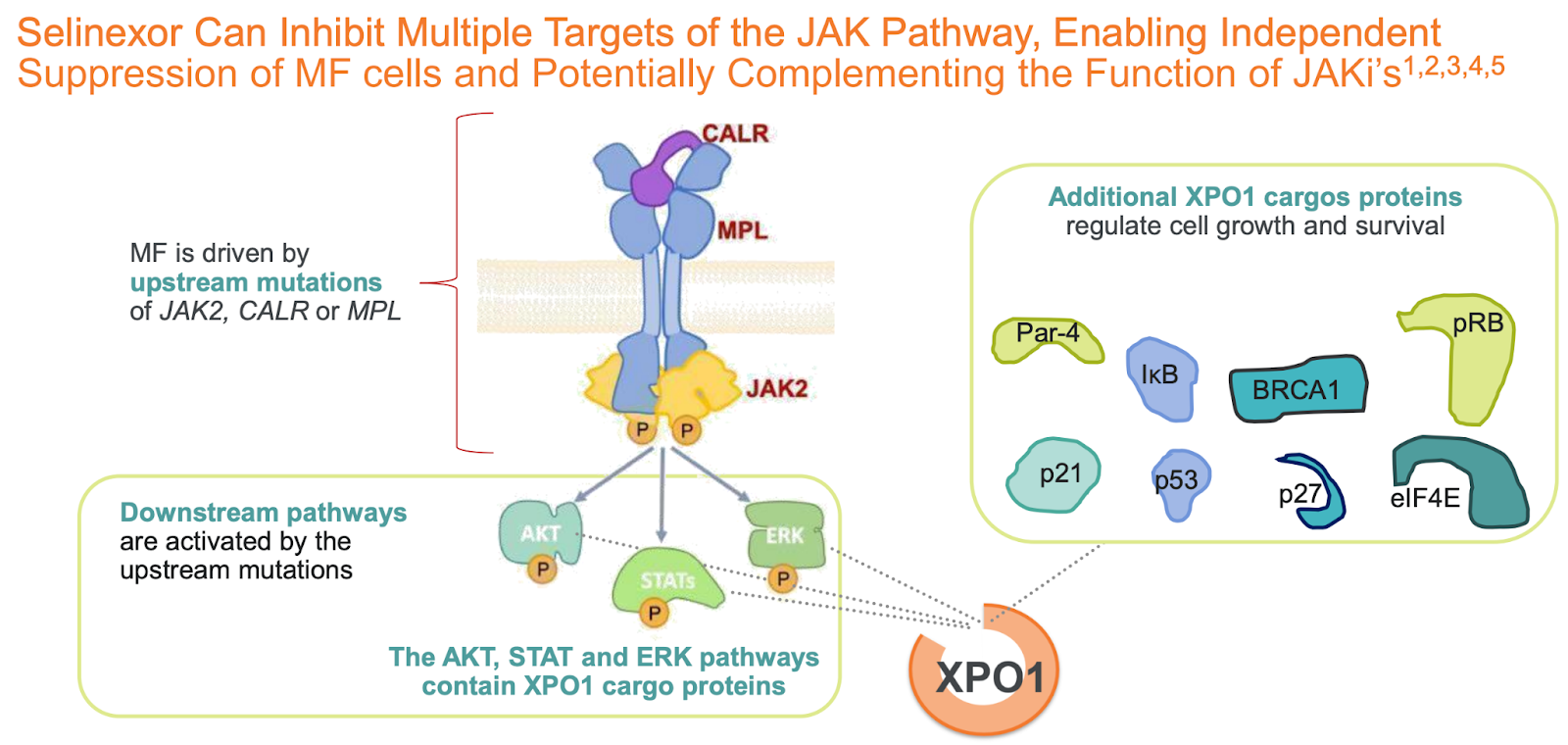
Selinexor/Ruxolitinib Combo Elicits Sustained Spleen Responses, Improves Symptoms in Myelofibrosis (2023)
The first presentation by Dr. Rangwala discussed results from the phase 1 XPORT-MF-034 trial evaluating selinexor in combination with ruxolitinib in patients with treatment-naive myelofibrosis. The trial enrolled 24 patients, with 10 receiving selinexor 40 mg weekly and 14 receiving 60 mg weekly, in combination with ruxolitinib.
Key efficacy results with the 60 mg dose of selinexor:
Rapid and deep spleen responses: In the efficacy-evaluable population, 83.3% achieved ≥35% spleen volume reduction (SVR35) at week 12 and 91.7% at week 24. In the intent-to-treat population, rates were 71.4% and 78.6% at weeks 12 and 24, respectively (Rangwala et al, 2023).
Robust symptom improvement: In the efficacy-evaluable patients, 80% achieved ≥50% reduction in total symptom score (TSS50) at week 12 and 77.8% at week 24. In the ITT population, rates were 66.7% and 58.3% at weeks 12 and 24, respectively (Rangwala et al, 2023).
SVR35 observed in 100% of evaluable patients at any time point. Responses were consistent across subgroups including males and those with low starting doses of ruxolitinib.
Improvement in spleen and cytokine-related symptoms seen across all domains of the Myelofibrosis Symptom Assessment Form (MFSAF).
Selinexor was generally well tolerated, with low rates of treatment discontinuations (7.1%). The most common grade ≥3 AEs were anemia (42.9%), thrombocytopenia (28.6%), and neutropenia (7.1%).
Evidence of disease modification was seen, with platelet normalization and stabilization of hemoglobin levels.
The efficacy and safety data support 60 mg selinexor as the recommended dose for a phase 3 study in combination with ruxolitinib.
Dr. Mascarenhas provided an overview on myelofibrosis treatment approaches and discussed the potential for selinexor to improve patient outcomes:
Myelofibrosis has a poor prognosis, with median survival of only 1.8-7.8 years depending on risk status (Mascarenhas, 2022).
JAK inhibitors like ruxolitinib are currently standard of care, but provide limited benefit. In the phase 3 COMFORT-I trial, only 42% of ruxolitinib patients achieved SVR35 at week 24 vs 0.7% with placebo (Verstovsek et al, 2012).
With ruxolitinib, the majority of discontinuations are due to side effects like cytopenias. Outcomes are poor after ruxolitinib discontinuation, with median survival of only 14 months in one study (Newberry et al, 2017).
There is a clear unmet need for more effective and tolerable treatments, particularly in the frontline setting. Selinexor has the potential to transform the treatment paradigm based on the phase 1 results showing rapid, deep, and durable spleen and symptom responses with generally manageable side effects.
The XPORT-MF-034 phase 3 trial is expected to initiate in the first half of 2023 and will evaluate selinexor plus ruxolitinib versus placebo plus ruxolitinib in 306 patients with treatment-naive myelofibrosis.
In summary, the phase 1 XPORT-MF-034 trial demonstrated impressive efficacy signals with the 60 mg dose of selinexor in combination with ruxolitinib for patients with previously untreated myelofibrosis. Selinexor induced high rates of spleen volume reduction and symptom improvement that were rapid in onset and deepened over time. Selinexor was tolerable overall with low rates of treatment discontinuation. These results support evaluation of selinexor plus ruxolitinib versus ruxolitinib alone in the upcoming phase 3 trial, which has the potential to establish a new standard of care for myelofibrosis.
Rusfertide (PTG-300)
7th Annual Women & MPN Conference- Dr. Ruben Mesa (link)
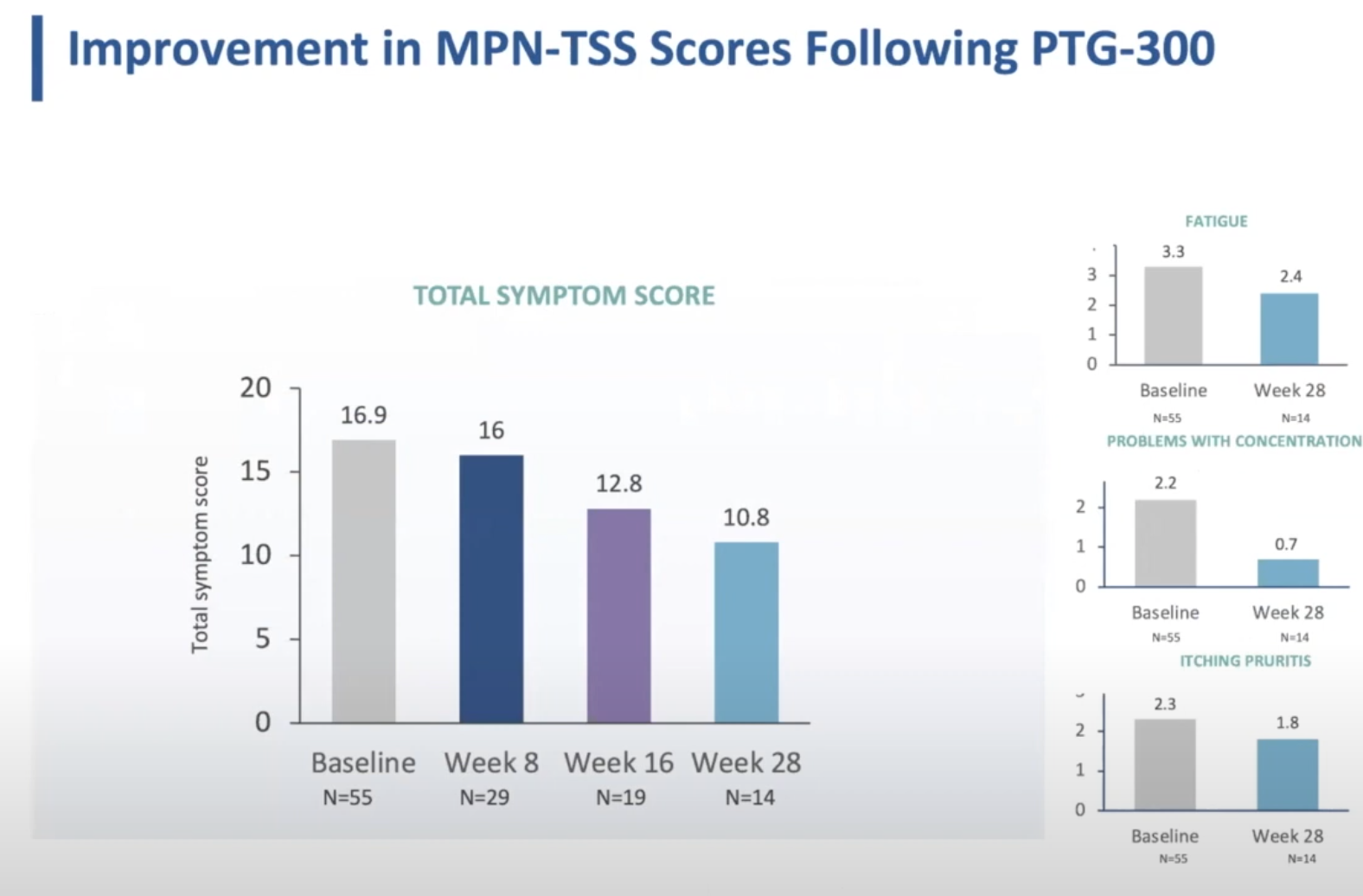

Givinostat
Long-term safety and efficacy of givinostat in polycythemia vera: 4-year mean follow up of three phase 1/2 studies and a compassionate use program (2021)
The article reports interim 4-year follow-up safety and efficacy results from an ongoing, open-label, single-arm, multicenter study evaluating long-term treatment with the histone deacetylase inhibitor givinostat in patients with polycythemia vera (PV). At the cutoff date, 54 patients with myeloproliferative neoplasms (MPNs) had enrolled, with 51 having PV.
Key eligibility criteria were adults with JAK2V617F-positive MPN who had tolerated and responded to prior givinostat treatment in 3 earlier phase 1/2 studies or compassionate use. Patients continue givinostat at their last effective and tolerated dose, either as monotherapy or with hydroxyurea if co-administered previously.
The primary objectives are to evaluate long-term safety/tolerability (adverse events) and efficacy per international response criteria. Exploratory endpoints include changes in JAK2V617F allele burden.
Of 51 PV patients enrolled, 50 received ≥1 givinostat dose (safety population) and had ≥1 post-baseline efficacy assessment (ITT population). Median treatment duration was 2.8 years (range 0.25-11 years).
Baseline demographics for PV patients: median age 65 years, 58% male, median time since PV diagnosis 7.2 years. 15 patients (30%) received concomitant hydroxyurea during the study.
Safety Results:
- 96% of PV patients had ≥1 AE; most were Grade <3 (90%).
- 26% had Grade ≥3 AEs, of which 5 patients had givinostat-related Grade 3 AEs.
- No Grade 4 or 5 AEs related to givinostat occurred.
- Most common drug-related AEs were Grade 1/2 GI disorders (32%) and blood/lymphatic disorders (16%).
- 26% had serious AEs, of which 1 was considered givinostat-related (Grade 2 multiple sclerosis).
- 10 patients (20%) withdrew due to AEs, 6 (12%) due to givinostat-related AEs.
Efficacy Results:
- In PV patients, >80% had partial or complete response maintained over follow-up.
- 4 patients were nonresponders at study entry but received compassionate givinostat use.
- Mean JAK2V617F allele burden declined over time for most annual visits.
- 6 PV patients (12%) had disease progression (1 to AML, 5 to post-PV myelofibrosis).
In subgroup analyses:
- PV patients on givinostat monotherapy had a slightly better safety profile vs. those on combination therapy.
- Overall response rates were higher for givinostat monotherapy subgroup.
Limitations include the single-arm noncomparative design, limited long-term data for some patients given varying enrollment times, and inclusion of mostly PV patients.
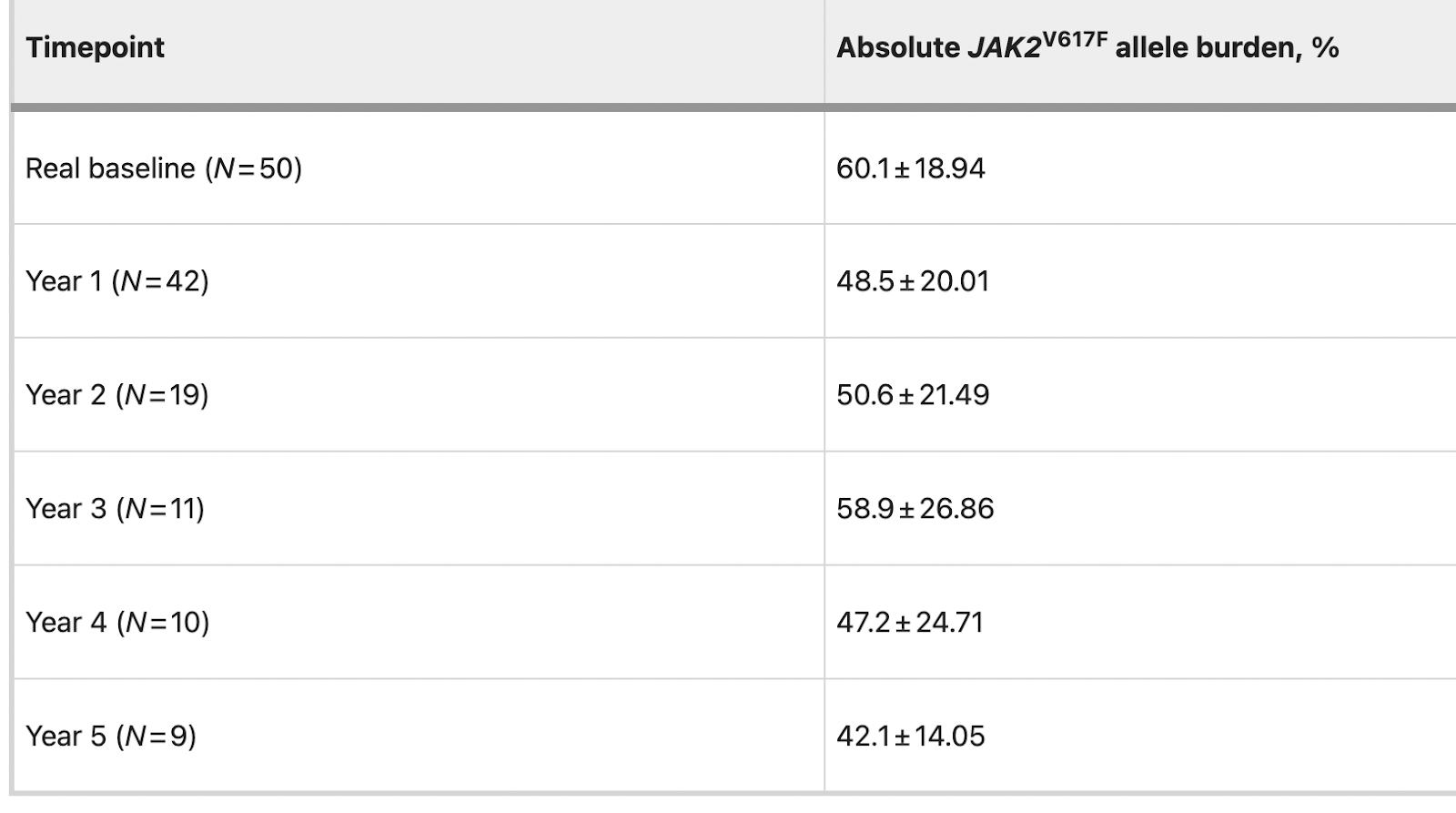
Givinostat Wiki
Givinostat (INN[1]) or gavinostat (originally ITF2357) is a histone deacetylase inhibitor with potential anti-inflammatory, anti-angiogenic, and antineoplastic activities.[2] It is a hydroxamate used in the form of its hydrochloride.
Givinostat is in numerous phase II clinical trials (including for relapsed leukemias and myelomas),[3] and has been granted orphan drug designation in the European Union for the treatment of systemic juvenile idiopathic arthritis,[4] polycythaemia vera.[5] and Duchenne muscular dystrophy. A preclinical study produced early results suggesting the molecule might help with diastolic dysfunction.[6] ITF2357 was discovered at Italfarmaco of Milan, Italy. It was patented in 1997 and first described in the scientific literature in 2005.[7][8]
Adverse effects
In clinical trials of givinostat as a salvage therapy for advanced Hodgkin's lymphoma, the most common adverse reactions were fatigue (seen in 50% of participants), mild diarrhea or abdominal pain (40% of participants), moderate thrombocytopenia (decreased platelet counts, seen in one third of patients), and mild leukopenia (a decrease in white blood cell levels, seen in 30% of patients). One-fifth of patients experienced prolongation of the QT interval, a measure of electrical conduction in the heart, severe enough to warrant temporary suspension of treatment.[9]
Mechanism of action
Givinostat inhibits class I and class II histone deacetylases (HDACs) and several pro-inflammatory cytokines. This reduces expression of tumour necrosis factor (TNF), interleukin 1α and β, and interleukin 6.[8]
It also has activity against cells expressing JAK2(V617F), a mutated form of the janus kinase 2 (JAK2) enzyme that is implicated in the pathophysiology of many myeloproliferative diseases, including polycythaemia vera.[10][11] In patients with polycythaemia, the reduction of mutant JAK2 concentrations by givinostat is believed to slow down the abnormal growth of erythrocytes and ameliorate the symptoms of the disease.[5]
The Role of Dietary Histone Deacetylases (HDACs) Inhibitors in Health and Disease
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4210916/#sec6-nutrients-06-04273
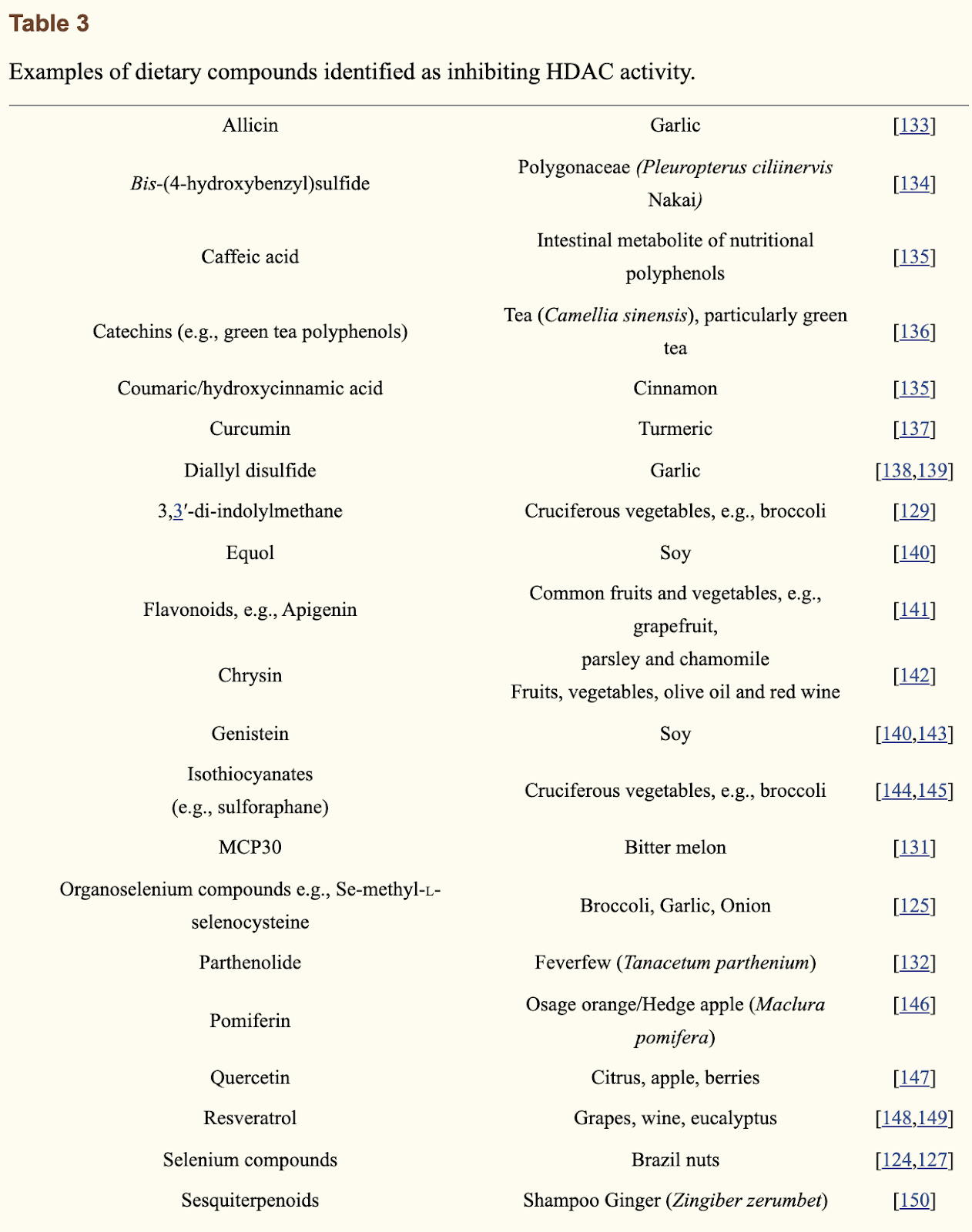
Treatment with a selective histone deacetylase (HDAC) 1 and 2 inhibitor in aged mice rejuvenates multiple organ systems (2023)
The process of aging increases the risk of developing age-related diseases, which come at great societal healthcare costs and suffering to individuals. Meanwhile, targeting the basic mechanisms of aging can reduce the risk of developing age-related diseases during aging, essentially resulting in a ‘healthy aging’ process. Multiple aging pathways exist, which over past decades have systematically been confirmed through gene knockout or overexpression studies in mammals and the ability to increase healthy lifespan. In this work, we perform transcriptome-based drug screening to identify small molecules that mimic the transcriptional profiles of long-lived genetic interventions in mammals. We identify one small molecule whose transcriptional effects mimic diverse known genetic longevity interventions: compound 60 (Cmpd60), which is a selective inhibitor of histone deacetylase 1 (HDAC1) and 2 (HDAC2). In line with this, in a battery of molecular, phenotypic, and bioinformatic analyses, in multiple disease cell and animal models, we find that Cmpd60 treatment rejuvenates multiple organ systems. These included the kidney, brain, and heart. In renal aging, Cmpd60 reduced partial epithelial-mesenchymal transition (EMT) in vitro and decreased fibrosis in vivo. For the aging brain, Cmpd60 reduced dementia-related gene expression in vivo, effects that were recapitulated when treating the APPSWE-1349 Alzheimer mouse. In cardiac aging, Cmpd60 treatment activated favorable developmental gene expression in vivo and in line with this, improved ventricular cardiomyocyte contraction and relaxation in a cell model of cardiac hypertrophy. Our work establishes that a systemic, two-week treatment with an HDAC1/2 inhibitor serves as a multi-tissue, healthy aging intervention in mammals. This holds potential for translation towards therapeutics that promote healthy aging in humans.
Pelabresib
Pelabresib (CPI-0610): An Exciting Novel Drug for the Treatment of Myelofibrosis (2023)
The review by Ferreira Gomes and Harrison (2023) provides an overview of the novel drug pelabresib (CPI-0610) and its potential as a treatment for myelofibrosis (MF). MF is a subtype of myeloproliferative neoplasms characterized by bone marrow fibrosis, abnormal megakaryopoiesis, inflammatory cytokine production, progressive cytopenias, splenomegaly, and high symptom burden. It can occur as primary MF or evolve from polycythemia vera or essential thrombocythemia. MF has a poor prognosis and current standard of care is JAK inhibitor therapy, which provides limited benefits.
Pelabresib is an oral selective BET bromodomain inhibitor that binds to BET proteins BRD2, BRD3, BRD4, and BRDT. BET proteins are epigenetic readers that regulate expression of genes involved in cell proliferation, inflammation, and fibrosis. Preclinical studies show pelabresib can downregulate aberrant NF-κB signaling, inflammatory cytokine production, megakaryopoiesis, and profibrotic pathways implicated in MF. The authors review evidence from preclinical studies and early phase clinical trials supporting pelabresib's potential as a treatment for MF.
Key conclusions:
BET inhibition with pelabresib impacts multiple pathogenic drivers in MF, including downregulation of NF-κB signaling, reduced inflammation, effects on dysregulated megakaryopoiesis, and antifibrotic activity.
Preclinical studies show synergistic effects on MF when pelabresib is combined with JAK inhibitors like ruxolitinib.
Early phase clinical trials demonstrate pelabresib is well-tolerated and has promising clinical activity in MF patients, both as monotherapy and in combination with ruxolitinib.
Results from Phase 1 Studies:
Pelabresib was evaluated in 3 Phase 1 trials in lymphoma, leukemia, MDS/MPN, and multiple myeloma patients (total N=138). Doses ranged from 6 to 400 mg daily.
Pelabresib was well tolerated up to the maximum tested dose. Most adverse events were low grade (81.4% grade 1/2). Main side effects were reversible cytopenias and GI toxicity.
Results from Phase 2 MANIFEST trial:
Arm 1: Pelabresib monotherapy in JAKi-refractory/ineligible MF patients (n=86). 11% achieved ≥35% spleen volume reduction (SVR35) at 24 weeks. 16% of transfusion-dependent patients achieved transfusion independence.
Arm 2: Pelabresib + ruxolitinib in JAKi-suboptimal responders (n=86). 20% achieved SVR35 at 24 weeks. 16% of transfusion-dependent patients achieved transfusion independence.
Arm 3: Upfront pelabresib + ruxolitinib in JAKi-naïve MF (n=84). 68% achieved SVR35 at 24 weeks compared to 42% with ruxolitinib monotherapy in historical trials. Durable symptom improvement and spleen responses were seen over time.
Pelabresib improved bone marrow fibrosis, normalized peripheral blood cell composition, reduced inflammatory cytokines, and lowered JAK2V617F mutant allele fraction, suggesting disease-modifying potential.
Combination was well tolerated. Most common AEs were cytopenias and GI toxicity.
Conclusions:
Pelabresib shows promising clinical activity in MF, both as monotherapy and combined with ruxolitinib.
Combination pelabresib + ruxolitinib induces high, durable spleen and symptom responses compared to ruxolitinib alone, especially in JAKi-naïve patients.
Pelabresib impacts potential MF disease biomarkers like fibrosis, inflammation, peripheral blood cell composition, and mutant allele burden.
MANIFEST-2 Phase 3 trial is underway comparing upfront pelabresib + ruxolitinib vs ruxolitinib + placebo in JAKi-naïve MF patients.
Pelabresib is an exciting novel drug that may address limitations of current JAKi therapy, particularly in combination treatment for MF. Further data are needed to confirm disease-modifying and survival benefits.
MANIFEST: Pelabresib in Combination With Ruxolitinib for Janus Kinase Inhibitor Treatment-Naïve Myelofibrosis (2023)
The phase II MANIFEST trial evaluated the efficacy and safety of the combination of pelabresib (a BET inhibitor) and ruxolitinib (a JAK inhibitor) in 84 JAK inhibitor-naïve patients with myelofibrosis. The primary endpoint was spleen volume reduction of ≥35% (SVR35) at 24 weeks, which was achieved in 68% of patients. The secondary endpoint of ≥50% reduction in total symptom score (TSS50) at 24 weeks was achieved in 56% of patients. These response rates are higher compared to historical rates with JAK inhibitor monotherapy of 29-42% for SVR35 and 34-46% for TSS50 (Mascarenhas et al, 2023).
At 48 weeks, SVR35 was 59.5% and median TSS reduction was -54.8%, indicating durable spleen and symptom responses over 48 weeks of treatment. The combination was well tolerated, with the most common grade 3/4 adverse events being thrombocytopenia (12%) and anemia (35%), which led to treatment discontinuation in only 4% of patients. After 2 years, 50% of patients remained on treatment.
Additional results:
SVR35 responses were consistent across risk groups, including 70% for intermediate-1 risk and 67% for intermediate-2/high risk by DIPSS.
Median spleen volume reduction was -50% at 24 weeks and -54.6% at 48 weeks.
36% of patients had improved hemoglobin levels (mean increase 1.3 g/dL).
28% of evaluable patients had ≥1 grade improvement in bone marrow fibrosis.
30% had >25% reduction in JAK2V617F mutant allele fraction, associated with SVR35 response.
Rapid and sustained reduction seen in inflammatory cytokines like TNFα, IL-6, IL-8.
Median ruxolitinib dose was 10 mg twice daily and median pelabresib dose was 125 mg once daily.
The authors conclude that the combination of pelabresib and ruxolitinib shows high clinical activity, is well tolerated, and has potential disease-modifying effects in myelofibrosis patients who are JAK inhibitor-naïve. The results support further investigation of this combination as it may improve outcomes compared to JAK inhibitor monotherapy. A phase III trial is underway comparing pelabresib+ruxolitinib to ruxolitinib alone in treatment-naïve myelofibrosis patients (MANIFEST-2 trial).
PURPOSE
Standard therapy for myelofibrosis comprises Janus kinase inhibitors (JAKis), yet spleen response rates of 30%-40%, high discontinuation rates, and a lack of disease modification highlight an unmet need. Pelabresib (CPI-0610) is an investigational, selective oral bromodomain and extraterminal domain inhibitor (BETi).
METHODS
MANIFEST (ClinicalTrails.gov identifier: NCT02158858), a global, open-label, nonrandomized, multicohort, phase II study, includes a cohort of JAKi-naïve patients with myelofibrosis treated with pelabresib and ruxolitinib. The primary end point is a spleen volume reduction of ≥ 35% (SVR35) at 24 weeks.
RESULTS
Eighty-four patients received ≥ 1 dose of pelabresib and ruxolitinib. The median age was 68 (range, 37-85) years; 24% of patients were intermediate-1 risk, 61% were intermediate-2 risk, and 16% were high risk as per the Dynamic International Prognostic Scoring System; 66% (55 of 84) of patients had a hemoglobin level of < 10 g/dL at baseline. At 24 weeks, 68% (57 of 84) achieved SVR35, and 56% (46 of 82) achieved a total symptom score reduction of ≥ 50% (TSS50). Additional benefits at week 24 included 36% (29 of 84) of patients with improved hemoglobin levels (mean, 1.3 g/dL; median, 0.8 g/dL), 28% (16 of 57) with ≥ 1 grade improvement in fibrosis, and 29.5% (13 of 44) with > 25% reduction in JAK2V617F-mutant allele fraction, which was associated with SVR35 response (P = .018, Fisher's exact test). At 48 weeks, 60% (47 of 79) of patients had SVR35 response. Grade 3 or 4 toxicities seen in ≥ 10% patients were thrombocytopenia (12%) and anemia (35%), leading to treatment discontinuation in three patients. 95% (80 of 84) of the study participants continued combination therapy beyond 24 weeks.
CONCLUSION
The rational combination of the BETi pelabresib and ruxolitinib in JAKi-naïve patients with myelofibrosis was well tolerated and showed durable improvements in spleen and symptom burden, with associated biomarker findings of potential disease-modifying activity.
Imetelstat
Telomerase Inhibitor Imetelstat in Patients with Essential Thrombocythemia (2015)
BACKGROUND
Imetelstat, a 13-mer oligonucleotide that is covalently modified with lipid extensions, competitively inhibits telomerase enzymatic activity. It has been shown to inhibit megakaryocytic proliferation in vitro in cells obtained from patients with essential thrombocythemia. In this phase 2 study, we investigated whether imetelstat could elicit hematologic and molecular responses in patients with essential thrombocythemia who had not had a response to or who had had unacceptable side effects from prior therapies.
METHODS
A total of 18 patients in two sequential cohorts received an initial dose of 7.5 or 9.4 mg of imetelstat per kilogram of body weight intravenously once a week until attainment of a platelet count of approximately 250,000 to 300,000 per cubic millimeter. The primary end point was the best hematologic response.
RESULTS
Imetelstat induced hematologic responses in all 18 patients, and 16 patients (89%) had a complete hematologic response. At the time of the primary analysis, 10 patients were still receiving treatment, with a median follow-up of 17 months (range, 7 to 32 [ongoing]). Molecular responses were seen in 7 of 8 patients who were positive for the JAK2 V617F mutation (88%; 95% confidence interval, 47 to 100). CALR and MPL mutant allele burdens were also reduced by 15 to 66%. The most common adverse events during treatment were mild to moderate in severity; neutropenia of grade 3 or higher occurred in 4 of the 18 patients (22%) and anemia, headache, and syncope of grade 3 or higher each occurred in 2 patients (11%). All the patients had at least one abnormal liver-function value; all persistent elevations were grade 1 or 2 in severity.
CONCLUSIONS
Rapid and durable hematologic and molecular responses were observed in patients with essential thrombocythemia who received imetelstat. (Funded by Geron; ClinicalTrials.gov number,
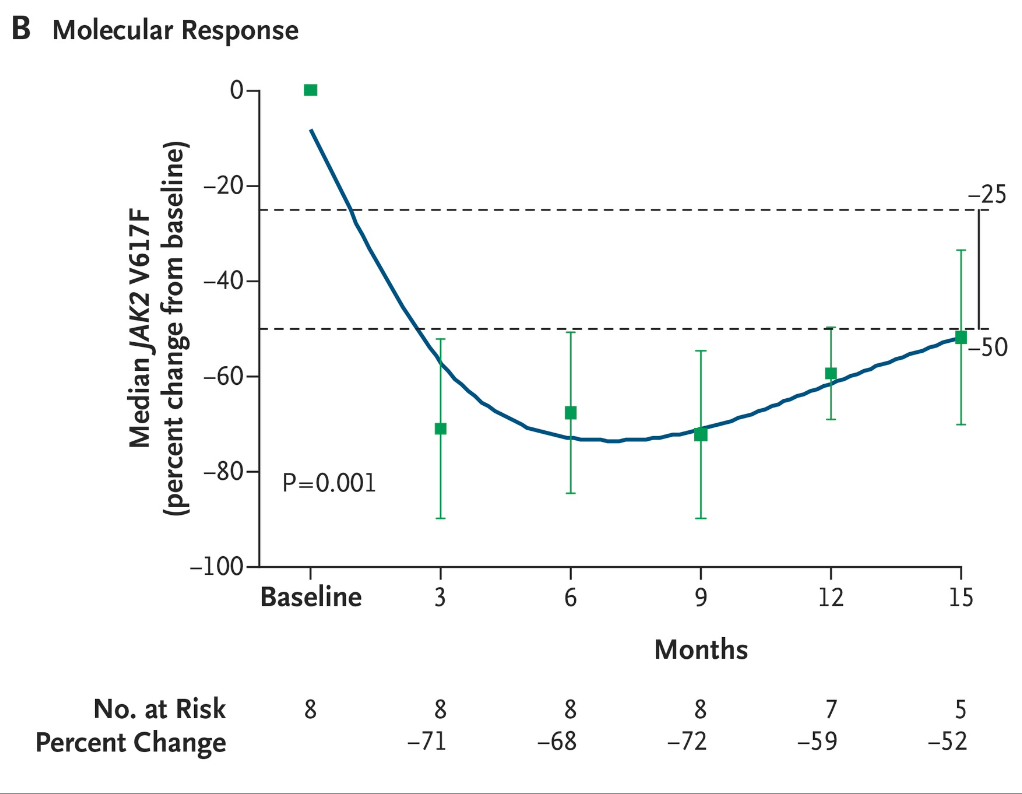
Navitoclax
Navitoclax plus ruxolitinib in JAK inhibitor-naive patients with myelofibrosis: Preliminary safety and efficacy in a multicenter, open-label phase 2 study (2022)
This is an ongoing Phase 2 trial evaluating navitoclax (NAV), a BCL-XL/BCL-2 inhibitor, in combination with ruxolitinib (RUX), a JAK 1/2 inhibitor, in patients with myelofibrosis (MF) who were JAK inhibitor-naïve.
32 patients received the NAV+RUX combination.
At 24 weeks, 52% of evaluable patients achieved the primary endpoint of ≥35% spleen volume reduction (SVR35).
76% achieved SVR35 at any time during treatment.
The combination also showed improvements in total symptom score, bone marrow fibrosis, and anemia.
The combination was generally well tolerated, with anemia, thrombocytopenia and neutropenia being the most common grade ≥3 adverse events.
In summary, this Phase 2 trial showed that the NAV+RUX combination demonstrated robust spleen volume reductions and improvements in other efficacy endpoints in JAK inhibitor-naïve MF patients. The combination was reasonably well tolerated. These results support further evaluation of this combination in MF.
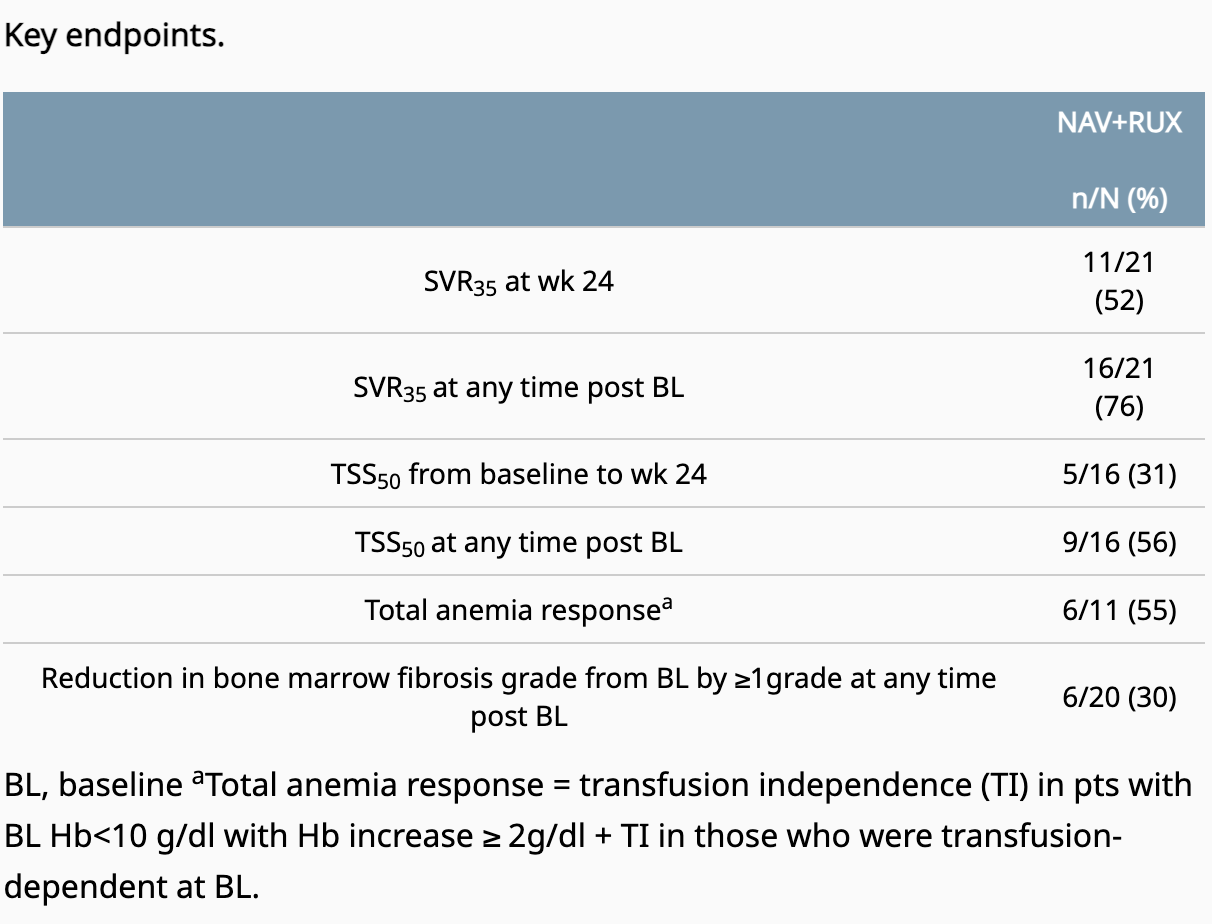
REFINE: Phase II study of navitoclax + ruxolitinib in JAK inhibitor-naive patients with MF (link)
Addition of Navitoclax to Ongoing Ruxolitinib Therapy for Patients With Myelofibrosis With Progression or Suboptimal Response: Phase II Safety and Efficacy (2022)
This was a phase 2 trial investigating adding navitoclax (a BCL-XL/BCL-2 inhibitor) to ruxolitinib in 34 myelofibrosis patients with suboptimal response or progression on ruxolitinib monotherapy.
26.5% achieved the primary endpoint of ≥35% spleen volume reduction (SVR35) at 24 weeks, increasing to 41% at any time on study. Median duration of SVR35 was 13.8 months.
30% achieved ≥50% reduction in total symptom score.
33% had improvement in bone marrow fibrosis by 1-2 grades.
64% achieved anemia response.
Median overall survival was not reached with median 21.6 months follow-up.
Navitoclax plus ruxolitinib was well tolerated, with reversible thrombocytopenia being the most common adverse event.
Purpose: Targeting the BCL-XL pathway has demonstrated the ability to overcome Janus kinase inhibitor resistance in preclinical models. This phase II trial investigated the efficacy and safety of adding BCL-XL/BCL-2 inhibitor navitoclax to ruxolitinib therapy in patients with myelofibrosis with progression or suboptimal response to ruxolitinib monotherapy (ClinicalTrials.gov identifier: NCT03222609).
Methods: Thirty-four adult patients with intermediate-/high-risk myelofibrosis who had progression or suboptimal response on stable ruxolitinib dose (≥ 10 mg twice daily) were administered navitoclax at 50 mg once daily starting dose, followed by escalation to a maximum of 300 mg once daily in once in weekly increments (if platelets were ≥ 75 × 109/L). The primary end point was ≥ 35% spleen volume reduction (SVR35) from baseline at week 24. Secondary end points included ≥ 50% reduction in total symptom score (TSS50) from baseline at week 24, hemoglobin improvement, change in bone marrow fibrosis (BMF) grade, and safety.
Results: High molecular risk mutations were identified in 58% of patients, and 52% harbored ≥ 3 mutations. SVR35 was achieved by 26.5% of patients at week 24, and by 41%, at any time on study, with an estimated median duration of SVR35 of 13.8 months. TSS50 was achieved by 30% (6 of 20) of patients at week 24, and BMF improved by 1-2 grades in 33% (11 of 33) of evaluable patients. Anemia response was achieved by 64% (7 of 11), including one patient with baseline transfusion dependence. Median overall survival was not reached with a median follow-up of 21.6 months. The most common adverse event was reversible thrombocytopenia without clinically significant bleeding (88%).
Conclusion: The addition of navitoclax to ruxolitinib in patients with persistent or progressive myelofibrosis resulted in durable SVR35, improved TSS, hemoglobin response, and BMF. Further investigation is underway to qualify the potential for disease modification.
AbbVie Presents Positive Investigational Navitoclax Combination Data in Phase 2 REFINE Study Suggesting Anti-Fibrosis Activity for Patients with Myelofibrosis (link)
This is data from a Phase 2 trial evaluating navitoclax (an investigational BCL-XL/BCL-2 inhibitor) in combination with ruxolitinib in patients with myelofibrosis
34 myelofibrosis patients who had suboptimal response or disease progression on ruxolitinib monotherapy received the combination.
Exploratory analysis showed improvements in potential biomarkers of disease modification:
38% of evaluable patients had improvement in bone marrow fibrosis (BMF)
23% had ≥20% reduction in driver gene variant allele frequency (VAF)
Median overall survival was not reached for patients with BMF or VAF responses, versus 28.5 months in those without responses.
At time of analysis with >2 year follow-up, survival estimate was 100% for patients with BMF/VAF responses.
Combination was generally tolerated, with thrombocytopenia being the most common adverse event.
In summary, this exploratory analysis suggests the navitoclax combination may show anti-fibrosis activity and extend survival in myelofibrosis patients based on effects on potential biomarkers. Larger Phase 3 trials are underway to confirm these findings.
Longevity interventions in Titan mice attenuate frailty and senescence accumulation (2023)
We treated 12-week-old Titan mice with Navitoclax for five days, followed by a 16-day break. This was repeated five times to the age of 27 weeks. The treatment resulted in 16.7 % increased median lifespan compared to the placebo group, (330 days placebo vs 385 days Navitoclax) and a significant extension of overall lifespan (Gehan-BreslowWilcoxon test, P = 0.026; Fig. 2c). Caspase-9 activity in the liver and blood cell composition, including platelet count, remained unchanged two weeks after the last transient Navitoclax treatment, whereas body weight was reduced by treatment, especially in late life (Supplementary Fig. 2b-h, Supplementary Table 1). Notably, Navitoclax-treated mice show reduced levels of SA-β-gal in the liver compared to the placebo group at the age of 26 to 27 weeks, two weeks after the last treatment (MannWhitney test, P = 0.03; Fig. 2d), confirming the results in C. elegans15
.
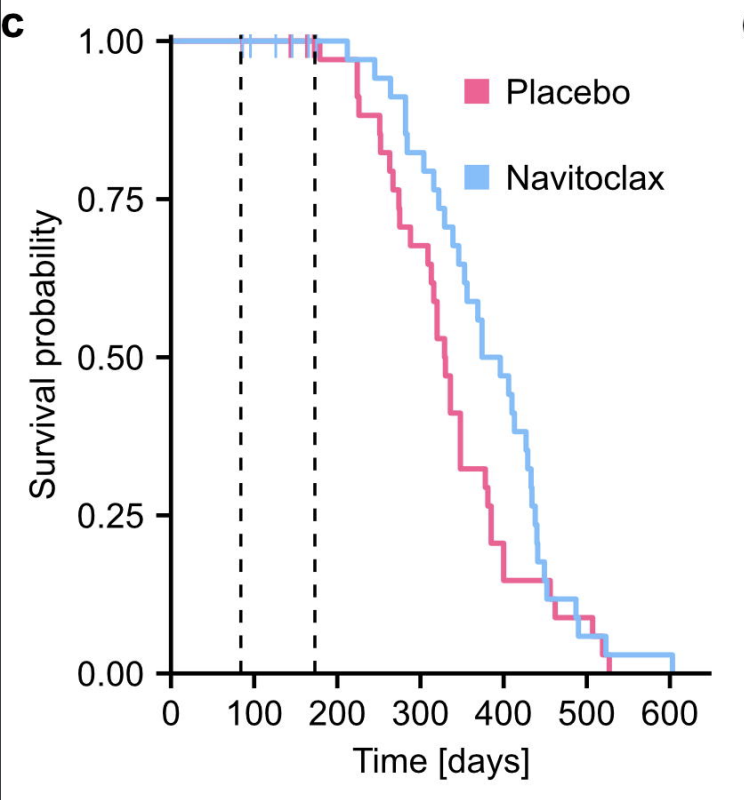
Idasanutlin (MDM2 Inhibitor)
An update on the use of idasanutlin in polycythemia vera (video)
The MDM2 antagonist idasanutlin in patients with polycythemia vera: results from a single-arm phase 2 study (2022)
This open-label single-arm phase 2 study by Mascarenhas et al. (2021) investigated the efficacy, safety, pharmacokinetics and pharmacodynamics of the MDM2 antagonist idasanutlin in 27 patients with hydroxyurea (HU)-resistant/-intolerant polycythemia vera (PV).
The study found that idasanutlin showed clinical activity in this patient population, but chronic gastrointestinal toxicity led to a high rate of treatment discontinuation.
Key conclusions:
Idasanutlin showed preliminary signs of clinical activity in patients with HU-resistant/-intolerant PV, with 56% of evaluable patients achieving the primary endpoint of hematocrit control at week 32.
69% of evaluable patients achieved an overall response per modified ELN criteria at week 32.
Hematocrit control and responses appeared durable, with 62% and 60% of responders maintaining response for ≥12 weeks beyond week 32, respectively.
A rapid reduction in JAK2 V617F variant allele frequency (VAF) was observed as early as after 3 treatment cycles, with significantly greater reductions seen in patients who achieved complete hematologic response and hematocrit control compared to non-responders. This suggests an association between early molecular response and clinical efficacy.
Bone marrow histopathological remission was attained in 2 treated patients, indicating potential disease-modifying effects.
However, low-grade gastrointestinal toxicities frequently led to treatment discontinuation in >50% of patients, compromising the overall benefit-risk profile.
Key efficacy results:
Of 16 evaluable patients, 56% (n=9) achieved the primary endpoint of hematocrit control at week 32.
In evaluable patients with baseline splenomegaly (n=13), only 1 patient (8%) achieved the primary composite endpoint of hematocrit control and ≥35% spleen volume reduction.
The overall response rate per modified ELN criteria was 69% (11/16) at week 32.
8 patients (50%) achieved complete hematologic response at week 32.
Median reduction in spleen volume was -7% at week 32, with any degree of reduction seen in 69% of evaluable patients.
Median reduction in JAK2 V617F VAF was 76% at week 32. Greater reductions were seen in responders versus non-responders.
43% of patients had a ≥50% reduction in symptom burden per MPN-SAF TSS at week 32.
Key safety and tolerability results:
Low-grade gastrointestinal toxicities like nausea (93%), diarrhea (78%) and vomiting (41%) were the most common adverse events.
11% of patients experienced grade ≥3 nausea and 4% had grade ≥3 vomiting.
Treatment was discontinued early in 41% of patients, predominantly due to gastrointestinal side effects.
In summary, idasanutlin showed preliminary signs of clinical activity and rapid molecular response in patients with HU-resistant/-intolerant PV, but poor tolerability due to gastrointestinal toxicity led to high study discontinuation rates. The MDM2 antagonist mechanism appears promising for PV, but modification of the idasanutlin regimen may be needed to improve tolerability while retaining efficacy. Further clinical evaluation of MDM2 inhibition is warranted in PV.
An open-label, global, phase (Ph) 1b/2 study adding navtemadlin (NVTM) to ruxolitinib (RUX) in patients (Pts) with primary or secondary myelofibrosis (MF) who have a suboptimal response to RUX. HemaSphere. 2023
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10428378/
The combination of nvtm and ruxolitinib showed promising efficacy in patients with myelofibrosis who had suboptimal response to ruxolitinib alone. In this phase 1b/2 study, the recommended phase 2 dose of nvtm was 240 mg daily (Days 1-7/28-day cycle) added to stable ruxolitinib dosing.
Among 24 patients treated at the phase 2 dose, 44% achieved ≥25% spleen volume reduction and 31% achieved ≥35% reduction at Week 24 by intent-to-treat analysis. Symptom improvement was also clinically meaningful, with 38% achieving ≥50% decrease in Total Symptom Score. Efficacy results were even more favorable in the subset of 11 patients reaching Week 24.
The addition of nvtm significantly reduced circulating CD34+ cells, providing evidence of disease modification. The combination demonstrated an acceptable safety profile, with only 33% of patients experiencing Grade 3/4 adverse events and no Grade 5 events.
Overall, this data indicates clinically meaningful improvements in splenomegaly and symptoms when nvtm is added to ruxolitinib in myelofibrosis patients undercontrolled with ruxolitinib monotherapy. The favorable risk-benefit profile supports further evaluation in phase 3 trials.
Off-label Drugs and Supplements for PV & MPNs
Pioglitazone
PPARγ agonists promote the resolution of myelofibrosis in preclinical models, 2021
Treatment with PPARγ agonists (including pioglitazone) counteracts MF-related anemia, represses leukocytosis, and improves BM and splenic changes related to the disease in 3 preclinical mouse models of MF. We demonstrate that PPARγ activation represses the survival and clonogenicity of cells from cell lines and PV/MF patients and slows cell proliferation in vitro and in PV (JAK2V617F) and ET (CALRdel52) mouse models. We also assess the potential effect of PPARγ agonists on TGF-β1–driven fibrosis via their antagonism of regulation of the TGF-β signaling pathway. Using genome-wide assays, we show that the effect of PPARγ agonists is mainly mediated via a competition for the transcriptional cofactor p300. Overall, these results establish that PPARγ agonists may be novel therapeutic candidates for MPNs with MF.
Pioglitazone for NAFLD Patients With Prediabetes or Type 2 Diabetes Mellitus: A Meta-Analysis, 2021
Objective: To systematically evaluate the effects of pioglitazone in the treatment of patients with prediabetes or T2DM combined with NAFLD.
Methods: The Cochrane Central Register of Controlled Trials (CENTRAL), Embase, and ClinicalTrials databases were searched until August 2020 for publications written in English. Two reviewers independently assessed study eligibility, continuous data extraction, independent assessment of bias risk, and graded the strength of evidence. Our primary outcomes were the individual number of patients with improvement of at least 1 point in each of the histological parameters. Baseline characteristic data, such as BMI, weight, total body fat, fasting plasma glucose and fasting plasma insulin, and liver biological indicators, such as triglyceride level, HDL cholesterol level, plasma AST, and plasma ALT, were used as secondary outcomes.
Results: A total of 4 studies were included. Compared with placebo, pioglitazone significantly improved steatosis grade, inflammation grade and ballooning grade, while in the fibrosis stage, there was no significant improvement in pioglitazone compared with placebo. In addition, pioglitazone can also improve blood glucose and liver function.
Conclusion: Pioglitazone can significantly improve the histological performance of the liver and insulin sensitivity. Additionally, it can significantly reduce fasting blood glucose, glycosylated hemoglobin, plasma AST, ALT and other liver biological indicators. Due to the lack of relevant randomized controlled trials and short intervention times, long-term studies are still needed to verify its efficacy and safety.
Diabetes drugs for nonalcoholic fatty liver disease: a systematic review, 2019
Three trials randomized patients without diabetes to pioglitazone or placebo [12, 13, 22]. In the first RCT, 163 patients with NASH were randomized to 30-mg pioglitazone or to placebo for 96 weeks [13]. Most patients (87%) underwent end-of-study biopsy. More patients treated with pioglitazone compared with placebo experienced improvement in liver histology (34% vs. 19%, P = 0.04), steatosis (69% vs. 31%, P < 0.001), NAFLD score (− 1.9 vs. 10.5, P < 0.001), and resolution of NASH (47% vs. 21%, P = 0.001). Liver function tests, fasting serum glucose, and insulin resistance were also significantly improved with pioglitazone versus placebo. However, weight gain was increased with pioglitazone compared with placebo (+ 4.7 kg vs. + 0.7 kg, P < 0.001). There was no difference between groups in change in liver fibrosis. Twelve patients experienced serious adverse events, with fewer events in the pioglitazone group (2.5% vs. 12%, RR 0.21, 95% CI 0.05 to 0.92).
In the second RCT, 74 patients with NASH were randomized to 30 mg of pioglitazone or placebo for 12 months [12]. All received diet and exercise counseling that was reinforced each visit. Sixty-one participants (82%) had liver biopsy at the end of treatment. A reduction in liver fat was seen with pioglitazone and placebo from baseline with no difference between groups. Pioglitazone was associated with a reduction in liver fibrosis compared with placebo (P = 0.05). Pioglitazone was also associated with greater improvement in HbA1c compared with placebo (− 0.2% vs. + 0.1%, P = 0.01), as well as greater improvement in ALT (− 37.1 vs. − 6.9 IU/L, P = 0.009). However, as above, pioglitazone treatment was associated with increase in body weight versus placebo (+ 2.6 kg vs. − 3.5 kg, P = 0.02). Withdrawals due to adverse events (18%) were similar between groups.
A third good-quality trial compared pioglitazone (15 mg/day) with placebo (n = 30 in each group) among Iranian adults with probable NAFLD by liver sonography [22]. While BMI was not different between groups (− 0.6 vs. − 0.7 kg/m2; P = 0.46), ALT (− 8.6 vs. − 0.6 IU/L; P < 0.001) and AST (− 6.7 vs. − 0.9 IU/L; P < 0.001) were significantly reduced among those receiving pioglitazone. No adverse events were reported.
Pioglitazone and risk of mortality in patients with type 2 diabetes: results from a European multidatabase cohort study, 2017
Objectives
Estimate and compare the risk of mortality in patients whose antidiabetic therapy is modified to include pioglitazone compared with an alternative antidiabetic medication at the same stage of disease progression.
Design
Retrospective cohort study.
Setting
Pooled analysis of clinical data collected from primary and/or secondary care settings in four European countries: Finland, The Netherlands, Sweden and the UK .
Participants
56 337 patients with type 2 diabetes mellitus first prescribed pioglitazone between 2000 and 2011, and 56 337 patients never prescribed pioglitazone matched by treatment stage, history of diabetes, diabetes complications and cardiovascular disease, and year of cohort entry using exact and propensity score matching. Patients were followed-up for a mean of 2.90 (SD 2.21) and 2.83 (SD 2.37) years in the pioglitazone-exposed and non-pioglitazone-exposed groups, respectively.
Outcomes
All-cause mortality ascertained from clinical or registry data. Mortality was a planned secondary outcome in a study primarily studying the association of pioglitazone use with bladder cancer risk.
Results
The crude overall mortality rate per 10 000 patient years was 206 (95% CI 199 to 213) in the pioglitazone-exposed group and 448 (95% CI 438 to 458) in the non-pioglitazone-exposed group. The crude HR comparing pioglitazone to alternative antidiabetic exposure was 0.46 (95% CI 0.45 to 0.48). This reduced in magnitude to 0.67 (95% CI 0.64 to 0.70) following further adjustment for matching variables, propensity scores, age, gender and time-dependent variables representing use of alternative antidiabetic drugs.
Conclusions
In this large observational cohort study of patients with type 2 diabetes, pioglitazone exposure was associated with a statistically significant decrease in the risk of all-cause mortality across four European countries. Results should be interpreted with caution due to the potential for residual confounding.
Pioglitazone Exposure Reduced the Risk of All-Cause Mortality in Insulin-Treated Patients with Type 2 Diabetes Mellitus, 2020
Context: The long-term safety and benefit of pioglitazone use in combination with insulin are still uncertain.
Objective: This study compared the risks of all-cause mortality and major cardiovascular (CV) events between pioglitazone users and nonusers receiving insulin therapy.
Design, setting and patients: We conducted a 13-year retrospective cohort study by using data from the population-based National Health Insurance Research Database in Taiwan. A total of 20 376 patients with type 2 diabetes mellitus (T2DM) receiving insulin therapy were enrolled during 2000 to 2012. Overall, the incidence rates of all-cause mortality and CV events were compared between 2579 pioglitazone users and 2579 matched nonusers.
Results: After adjustment for age, sex, comorbidities, Diabetes Complications Severity Index scores, and drugs used, mortality rates were 30.26 and 15.02 per 1000 person-years for pioglitazone nonusers and users, respectively. The adjusted hazard ratio (aHR) of mortality was 0.47 (95% confidence interval [CI]: 0.38-0.58, P < 0.001) for pioglitazone users compared with nonusers. The aHRs of CV and non-CV deaths were 0.78 (95% CI: 0.51-1.19) and 0.50 (95% CI: 0.38-0.66), respectively. The aHRs of hospitalized coronary artery disease, hospitalized stroke, and incident heart failure were not significantly different between pioglitazone users and nonusers.
Conclusions: This nationwide cohort study demonstrated that pioglitazone use reduced the risks of all-cause mortality and non-CV death for patients with T2DM undergoing insulin therapy.
Effects of pioglitazone on cardiovascular events and all-cause mortality in patients with type 2 diabetes: A meta-analysis of randomized controlled trials, 2022
In 2019, the Italian Society of Diabetology and the Italian Association of Clinical Diabetologists nominated an expert panel to develop guidelines for drug treatment of type 2 diabetes. After identifying the effects of glucose-lowering agents on major adverse cardiovascular events (MACEs), all-cause mortality, and hospitalization for heart failure (HHF) as critical outcomes, the experts decided to perform a systematic review and meta-analysis on the effect of pioglitazone with this respect.
Data synthesis
A MEDLINE database search was performed to identify RCTs, up to June 1st, 2021, with duration≥52 weeks, in which pioglitazone was compared with either placebo or active comparators. The principal endpoints were MACE and HHF (restricted for RCT reporting MACEs within their outcomes), all-cause mortality (irrespective of the inclusion of MACEs among the pre-specified outcomes). Mantel-Haenszel odds ratio (MH–OR) with 95% Confidence Interval (95% CI) was calculated for all the endpoints considered.
Eight RCTs were included in the analysis for MACEs and HF (5048 and 5117 patients in the pioglitazone and control group, respectively), and 24 in that for all-cause mortality (10,682 and 9674 patients). Pioglitazone neither significantly increased nor reduced the risk of MACE, all-cause mortality, and HHF in comparison with placebo/active comparators (MH–OR: 0.90, 95% CI 0.78–1.03, 0.91, 95% CI 0.77, 1.09, and 1.16, 95% CI 0.73, 1.83, respectively). Pioglitazone was associated with a significant reduction of MACE in patients with prior cardiovascular events (MH–OR 0.84, 95% CI 0.72–0.99).
Conclusions
This meta-analysis showed no significant effects of pioglitazone on incident MACE, all-cause mortality, and HHF.
Assessing the need for pioglitazone in the treatment of patients with type 2 diabetes: a meta-analysis of its risks and benefits from prospective trials, 2020
The safety and usefulness of pioglitazone (Pio) is repeatedly called into question due to the contradictory information available about it. A meta-analysis and risk benefit assessment was conducted to address the various points of debate regarding Pio. Electronic database search (Cochrane library, Embase & PubMed) resulted in 10 citations eligible for this meta-analysis (prospective, randomised studies), which was conducted using CMA software version 3 (Biostat Inc., Englewood, NJ, USA). The meta-analysis was registered with PROSPERO (ID: CRD42019122403) and compared pioglitazone with a control (anti-hyperglycemic agents without pioglitazone) in patients with either established cardiovascular disease or having high cardiovascular risk. Sensitivity and subgroup analysis were conducted to differentiate the effect of Pio against active controls and placebo. The use of Pio compared to the control group that did not use Pio resulted in a 14% and 23% significant reduction in odds of major adverse cardiac events (MACE: MH-OR, 0.86; 95% CI 0.75–0.98), and stroke (MH-OR, 0.77; 95% CI 0.60–0.99), respectively. This reduction in stroke was not significant in comparison to placebo on subgroup analysis. However, Pio significantly increased odds of heart failure (HF) (MH-OR, 1.47; 95% CI 1.26–1.71) as well as hospitalization for heart failure (hHF) (MH-OR, 1.48; 95% CI 1.21–1.81). In addition, the use of Pio was associated with a significant increase in odds of fractures in women (MH-OR, 2.05; 95% CI 1.28–3.27) and anaemia (MH-OR, 2.56; 95% CI 1.55–4.21). Pio has no significant effect on bladder cancer nor macular oedema. Pio has salutary effects on MACE. The positive effects are completely offset by the harm they seem to cause by way of heart failure, fractures, and anaemia. Pio should therefore be reserved for treatment of T2D with high CV risk or established cardiovascular (CV) disease only in selected patients where other antidiabetics are precluded and not routinely.
For years now, the balance between the safety and efficacy of pioglitazone (Pio), a peroxisome proliferator-activated receptor gamma (PPAR γ) agonist, in the treatment of patients with type 2 diabetes (T2D) has been heavily debated. Some experts have even argued that there is minimal role of this drug in treating T2D1.
PPAR γ agonists have heterogeneous cardiovascular effects2, with rosiglitazone, showing deleterious effects on the cardiovascular system, and these effects translate into a higher rate of myocardial infarction and all-cause mortality associated with its use3. In contrast, the use of Pio is associated with not only an improvement of glycaemia, but also an additional reduction of inflammatory markers like high-sensitivity C reactive protein (hs CRP), interleukin 6 (IL 6), and tumor necrosis factor alpha (TNF α) along with a suppression of adhesion molecules like soluble intercellular adhesion molecule (s I CAM), soluble vascular cell adhesion molecule-1 (s VCAM 1), and soluble sE-selectin, indicating improvement of endothelial function4. Pio has also been shown to reduce blood pressure5 and is associated with improvement of lipid abnormalities6 seen in T2D. Surrogate markers of atherosclerotic cardiovascular disease are reduced with Pio when compared to sulphonylureas7. These provide indirect evidence of the positive role of Pio in cardiovascular disease seen in T2D. On the other hand, along with these salutary effects, usage of Pio is associated with weight gain and oedema, which would intuitively have negative effects on cardiovascular outcomes. Indeed, there is a large body of evidence demonstrating an increased risk of heart failure with the use of Pio7, 8. Pio has also been implicated in fractures, anemia, and macular oedema, along with bladder cancer, creating much discourse about its continued usage9, 10.
The doubts have somewhat mellowed with the publication of a few trials highlighting its cardiovascular (CV) benefits11,12,13,14,15,16,17 including reduction of stroke in pre-diabetes and insulin resistance18.
However, with the persistent shadow of doubt on this molecule appearing from time to time, the risk–benefit assessment of this drug should be conducted objectively and scientifically. Previous systematic reviews have addressed only stroke as an outcome or have addressed observational studies only19, 20. The most detailed systematic review and meta-analysis on Pio and CV outcomes published in 2016 addressed cardiovascular outcomes in diabetes, pre-diabetes, and insulin resistance and not T2D specifically21. Another meta-analysis conducted in 2007 analyzed a spectrum of extremely heterogenous studies and obviously does not include multiple important citations which have been published since22.
Leukotriene Inhibitors (Singulair / Zileuton)
GENERAL SUMMARY:
Leukotriene inhibitors are medications that block inflammatory substances called leukotrienes, helping to alleviate and prevent asthma symptoms and allergic reactions.
Recent studies suggest potential benefits of leukotriene inhibitors in conditions such as cancer, obesity-related inflammation, diabetes, heart disease, and neurological aging.
ANTI-CANCER EFFECTS:
LTRA (Cysteinyl Leukotriene Receptor Antagonists) use in asthma patients from Taiwan demonstrated a dose-dependent decrease in cancer risk across all cancers studied, warranting further study of their chemopreventive potential (2016).
LTRA use in Korea was associated with a decreased cancer risk, especially when used in high doses and for longer durations (2022).
In a 2017 study, arachidonate 5-lipoxygenase (Alox5) was found to be a key genetic effector of JAK2V617F in driving Polycythemia Vera (PV), while combining 5-lipoxygenase (5-LOX) inhibitor zileuton with JAK2 inhibitor ruxolitinib demonstrated enhanced antitumor activity in PV mice (2021).
Pharmaxis developed PXS-5505, an oral pan-LOX inhibitor initially developed for Myelofibrosis (MF) treatment, showing positive results in a phase 2 cancer trial with significant reductions in fibrosis (2022)
Galecto's Phase 2a trial (MYLOX-1) of GB2064 for MF treatment demonstrated positive results, with a majority of patients experiencing a reduction in collagen fibrosis of the bone marrow, indicating potential disease-modifying effects (link).
Leukotriene inhibitor exposure in U.S. veterans with asthma was associated with a reduced risk of lung cancer (2021).
Montelukast, a leukotriene inhibitor, induces apoptosis in lung cancer cells, suggesting a potential therapeutic use (2017).
CysLT1R antagonists demonstrated inhibition of tumor growth in a colon cancer xenograft model (2013).
LTRAs demonstrated potential as chemoprevention candidates in colorectal cancer by reducing aberrant crypt foci formation in a nonrandomized, open-label, controlled trial (2022).
Leukotriene signaling promotes tumor growth and metastasis, suggesting potential for pharmacological targeting in tumor metastasis treatment (2020).
METABOLIC EFFECTS:
A 2011 review discussed the role of lipoxygenases, specifically 5-lipoxygenase and its derived products (leukotrienes), in exacerbating adipose tissue inflammation and related pathologies in obesity. Overexpression of the 5-lipoxygenase pathway and increased leukotriene production are common in excessive visceral fat depots, where they induce inflammation and promote insulin resistance.
A 2021 study showed that montelukast, an LTRA, led to significant improvements in liver stiffness, liver enzymes, metabolic parameters, and liver fibrosis biomarkers in patients with non-alcoholic steatohepatitis (NASH).
The 2023 study aimed to evaluate the effectiveness, tolerability, and safety of combining montelukast therapy with metformin in obese diabetic patients. After 12 weeks of treatment, the montelukast group significantly improved in all parameters compared to the placebo group.
The 2018 systematic review of 28 studies (26 animal studies and 2 human clinical trials) concluded that leukotriene inhibitors potentially reduced the risk of myocardial infarction, ischemic stroke, and atherosclerosis in both animal studies and human trials, suggesting a potential role in reducing CVD.
A 2015 study suggested that leukotriene receptor inhibition may be a druggable target to restore cognitive functions in the elderly.
A 2020 observational study using Norwegian registry data found that previous use of montelukast correlated with improved scores on cognitive or neurological functioning.
DEEPER DIVE:
Leukotriene inhibitors are commonly used to alleviate and prevent asthma symptoms as well as allergic reactions. Given the central role leukotrienes play in chronic inflammation, leukotriene inhibitors are being considered for a wide range of diseases, including osteoarthritis (2003, 2021), cancer (2020), obesity-related inflammation (2011), liver disease (2021), diabetes (2023), heart disease (2018), and neurological aging (2015, 2020).
Researchers have been investigating the role of various enzymes and inhibitors in the treatment of myeloproliferative neoplasms (MPNs) such as polycythemia vera (PV) and primary myelofibrosis (PMF). In a 2017 study, arachidonate 5-lipoxygenase (Alox5) was found to be a key genetic effector of JAK2V617F in driving PV, and its inhibition showed potential as a therapeutic target for treating MPNs. In a 2021 study, the combination of 5-lipoxygenase inhibitor zileuton and JAK2 inhibitor ruxolitinib demonstrated enhanced antitumor activity in hematopoietic progenitor cells from PV patients, providing conceptual validation for further clinical applications of this combined treatment.
TGF-beta,TNF-alpha, IL-6, hs-CRP are some inflammatory mediators and serum markers that have been observed to be significantly elevated in MPNs (2021). Montelukast has been shown to help control these markers in two separate contexts: liver disease (2021) and diabetes (2023). The 2021 study showed that montelukast led to significant improvements in liver stiffness, liver enzymes, metabolic parameters, and liver fibrosis biomarkers in patients with non-alcoholic steatohepatitis (NASH). These studies and the anti-fibrotic mechanisms involved raise the possibility that similar benefits can be expected in MPNs.
LOX (Lysyl Oxidase) is an enzyme that plays a crucial role in the formation and maintenance of the extracellular matrix (ECM) by catalyzing the cross-linking of collagen and elastin fibers. LOX is important for tissue stability and has been implicated in the development and progression of fibrosis and certain types of cancer.
A 2021 study identified lysyl oxidase (LOX) as a potential therapeutic target for PMF. LOX was found to be upregulated in PMF mice and patients, implying a role in bone marrow fibrosis progression. The development of two new small molecule LOX inhibitors, PXS-LOX_1 and PXS-LOX_2, demonstrated promise in pre-clinical studies by slowing PMF progression, offering a potential new therapeutic approach targeting ECM dysregulation in PMF.
Pharmaxis has developed an oral pan-LOX inhibitor called PXS-5505, which inhibits all lysyl oxidase family members. The compound has demonstrated significant reductions in fibrosis in in-vivo models of various fibrotic disorders and cancers with prominent stroma or fibrotic metastatic niches. Pharmaxis is initially targeting PXS-5505 for myelofibrosis. (link, 2022, 2022)
In a phase 2 cancer trial, 15 patients were enrolled, with six completing 24 weeks of treatment. PXS-5505 was well tolerated, with no serious treatment-related adverse events. Two of the six patients experienced clinically important symptom improvement, and five of the six patients had stable or improved bone marrow fibrosis scores and platelet and/or hemoglobin scores. However, no reductions in spleen volume were observed.
Galecto, a clinical-stage biotechnology company, announced positive results from an intermediate assessment of its ongoing Phase 2a trial (MYLOX-1) of GB2064 for myelofibrosis treatment. Four out of five evaluable patients receiving GB2064 monotherapy for at least six months experienced a ≥1-grade reduction in collagen fibrosis of the bone marrow, suggesting that GB2064 could impact disease progression and be disease-modifying. (link)
A 2016 study found that cysteinyl leukotriene receptor antagonists (LTRAs) significantly decreased cancer risk in asthma patients in a dose-dependent manner. Leukotrienes, which are involved in inflammatory disorders, have been found to promote tumor growth and resistance to immunotherapy. Pharmacological targeting of leukotriene signaling in tumor metastasis is an emerging possibility.
A 2021 study showed that montelukast, an LTRA, led to significant improvements in liver stiffness, liver enzymes, metabolic parameters, and liver fibrosis biomarkers in patients with non-alcoholic steatohepatitis (NASH). Montelukast was well-tolerated and did not cause depression, suggesting potential as a promising therapeutic strategy for NASH.
A 2011 review discussed the role of lipoxygenases, specifically 5-lipoxygenase and its derived products (leukotrienes), in exacerbating adipose tissue inflammation and related pathologies in obesity. Overexpression of the 5-lipoxygenase pathway and increased leukotriene production are common in excessive visceral fat depots, where they induce inflammation and promote insulin resistance. The 5-lipoxygenase pathway also plays a significant role in inflammation in hepatic tissue and is a pathogenic factor in obesity-induced nonalcoholic fatty liver disease (NAFLD). Modulation of lipoxygenases could be a novel target for preventing adipose tissue and hepatic dysfunction related to metabolic syndrome.
The 2023 study aimed to evaluate the effectiveness, tolerability, and safety of combining montelukast therapy with metformin in obese diabetic patients. After 12 weeks of treatment, the montelukast group significantly improved in all parameters compared to the placebo group. Montelukast adjuvant therapy was found to be superior to metformin-only therapy in diabetes control and weight loss, likely due to increased insulin sensitivity and anti-inflammatory properties. The combination was safe and tolerable throughout the study.
The 2018 systematic review of 28 studies (26 animal studies and 2 human clinical trials) concluded that leukotriene receptor antagonists, such as montelukast, potentially reduced the risk of myocardial infarction, ischemic stroke, and atherosclerosis in both animal studies and human trials, suggesting a potential role in reducing some cardiovascular diseases.
The 2022 nonrandomized, open-label, controlled trial studied the effect of leukotriene receptor antagonists (LTRAs) on colorectal aberrant crypt foci (ACF) formation in humans. The trial enrolled 40 patients and found a significant decrease in ACFs in the LTRA group compared to the observation group, suggesting LTRAs as potential candidates for colorectal cancer chemoprevention.
Montelukast, an approved anti-asthmatic drug, has been shown to reduce neuroinflammation, increase hippocampal neurogenesis, and improve learning and memory in old rats by inhibiting the GPR17 receptor. This suggests that leukotriene receptor inhibition may be a druggable target to restore cognitive functions in the elderly, 2015.
The suppression of the 5-lipoxygenase (5LO) pathway, including the use of montelukast, has been considered safe in chronic conditions like asthma and could potentially benefit patients with Alzheimer's disease, non-AD amyloidoses, tauopathies, oxidation-linked nervous system disorders, and inflammation-centered disease processes, 2015.
A 2020 observational study using Norwegian registry data found that previous use of montelukast correlated with improved scores on cognitive or neurological functioning. The study suggests that montelukast may alleviate degenerative neurological changes associated with human aging and potentially postpone mental aging. The findings may help initiate clinical trials to examine the effect of montelukast on aging.
Alox5 Blockade Eradicates JAK2V617F-Induced Polycythemia Vera in Mice, 2017
Myeloproliferative neoplasms such as polycythemia vera (PV), which are associated with the JAK mutation V617F, remain incurable despite progress in the use of JAK2 inhibitors for treatment of some of these diseases. In this study, we employed mice that undergo JAK2V617F-induced PV as a tool to explore new candidate targets for therapy. Our investigations focused on the lipid metabolic enzyme arachidonate 5-lipoxygenase (Alox5), which we found to be strongly upregulated by JAK2V617F in hematopoietic cells in vitro and in vivo Notably, genetic deletion of Alox5 or its inhibition in mice with a bioactive small-molecule inhibitor was sufficient to attenuate PV development. This therapeutic effect was associated with induction of a blockade in cell-cycle progression and also with apoptosis in PV cells. Genetic loss exerted an inhibitory effect on PV-initiating cells. Similarly, Alox5 inhibition was sufficient to suppress colony formation in human JAK2V617F-expressing CD34+ cells. Mechanistic investigations showed that Alox5 inhibition reduced AKT activation and decreased β-catenin expression in JAK2V617F-expressing cells. Together, our results define Alox5 as a key genetic effector of JAK2V617F in driving PV, and they identify this enzyme as a candidate therapeutic target to treat this refractory myeloproliferative neoplasm
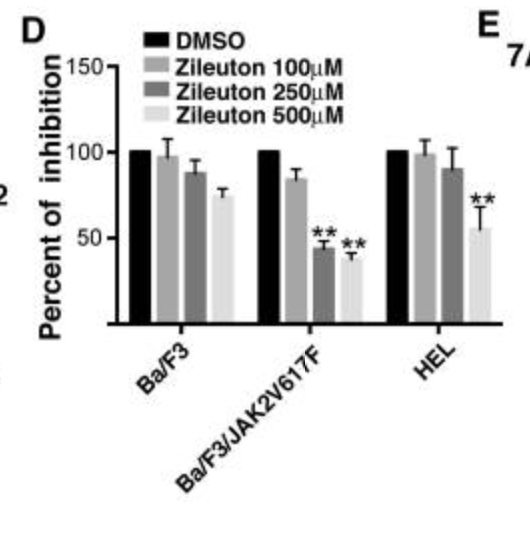
(minimal effect on normal leftmost stem cells; significant inhibition on middle and rightmost cancer cells)
Targeting cancer stem cells in JAK2V617F induced neoplasm (2020)
Project Summary/Abstract We aim to develop a new therapeutic strategy for one major form of JAK2V617F-induced myeloproliferative neoplasms (MPNs), polycythemia vera (PV), with a focus on targeting PV-initiating cells (cancer stem cells in PV). A curative therapy for PV is still lacking. The proposed studies are based on our preliminary finding that the arachidonate 5-lipoxygenase (5-LO) gene (Alox5) plays a key role in survival regulation of PV-initiating cells. The Alox5 pathway is known for producing inflammatory (asthma-causing) leukotrienes, and an FDA-approved human anti-asthma drug called Singulair (Montelukast) blocks leukotriene receptor binding to reduce the inflammatory response. We have found that Singulair inhibits the growth of JAK2-V617F-expressing cells in vitro and in mice. Thus, Singulair could be an effective new agent for treating PV. We hypothesize that leukotrienes produced in the Alox5-pathway play an essential role in survival regulation of MPN-initiating cells in PV, and Singulair antagonizes the action of leukotrienes to act as a potential new therapeutic agent for PV. Testing this hypothesis is of clinical significance and would benefit: 1) PV patients who have not progressed to acute myeloid leukemia (AML); 2) PV patients who are in clinical remission of AML with residual JAK2V617F-expressing cells and may relapse with time; 3) PV patients who had bone marrow transplantation for treating AML progressed from PV but still have residual JAK2V617F-expressing cells; and 4) the individuals who have detectable JAK2V617F transcripts in myeloid cells but have not developed clinical symptoms of PV. Because the Alox5 pathway is known to produce leukotrienes, one plausible mechanistic explanation of action of Singulair is that it eradicates PV by blocking receptor binding of leukotriens to PV-initiating cells. We also need to know the underlying molecular mechanisms by which Singulair inhibits PV-initiating cells and PV development. In fact, our preliminary studies show that JAK2V617F regulates the Alox5 pathway involving two Alox5 downstream genes, beta-catenin (as a stimulator) and Blk (as a suppressor), and it will be important to investigate whether Singuliar regulates these two genes in PV-initiating cells. Finally, it is critical to determine whether Singulair inhibits the growth of human PV-initiating cells. The specific aims are: 1) To determine whether the survival of PV-initiating cells is dependent on leukotrienes and whether a blockade of leukotrienes by Singulair reduces their effects on PV-initiating cells; 2) To determine the molecular mechanisms by which Singulair inhibits PV-initiating cells and PV development; and 3) To determine whether Singulair blocks the Alox5 pathway in human PV-initiating cells and reduces engraftment of human PV-initiating cells in immunocompromised mice. Broadly, Singulair is a potential therapeutic agent for solid tumors as Alox5 is associated with tumorigenesis in the colon, lung, pancreas, liver, esophagus, skin, etc.
A drug targeting 5-lipoxygenase enhances the activity of a JAK2 inhibitor in CD34 + bone marrow cells from patients with JAK2V617F-positive polycythemia vera in vitro, 2021
Janus kinase 2 (JAK2) inhibitors, the first targeted treatments for myeloproliferative neoplasms (MPNs), provide substantial benefits, including a marked reduction in splenomegaly and MPN-associated symptoms. However, these drugs rarely induce molecular remission in patients with MPNs. Zileuton, a 5-lipoxygenase (5-LO) inhibitor, has been demonstrated to selectively deplete hematopoietic stem cells (HSCs) expressing a JAK2 point mutation (JAK2V617F) in mouse models of JAK2V617F-induced polycythemia vera (PV). To determine the potential activity of 5-LO inhibitors in combination with JAK inhibitors against human PV HSCs, the present study first analyzed 5-LO expression in CD34+ bone marrow cells from patients with JAK2V617F-positive PV using western blotting and reverse transcription-quantitative PCR, and then examined the effect of zileuton combined with ruxolitinib on colony formation using a colony formation assay. Furthermore, cell cycle and apoptosis in CD34+ cells from patients with PV and healthy volunteers were determined by flow cytometry. In the present study, 5-LO expression was upregulated in CD34+ cells from patients with PV compared with in CD34+ cells from healthy volunteers. Higher levels of leukotriene B4, a product of the 5-LO signaling pathway, were detected in patients with PV compared with in healthy volunteers. Zileuton treatment suppressed the colony formation of CD34+ cells from patients with PV in a dose-dependent manner. Furthermore, zileuton and ruxolitinib exerted their anticancer effects by suppressing hematopoietic colony formation, inducing apoptosis and arresting the cell cycle of human CD34+ cells from patients with PV. The combination of these two drugs exerted a more beneficial effect than either agent alone. Based on these data, zileuton enhanced the antitumor activity of low-dose ruxolitinib in hematopoietic progenitor cells from patients with PV, providing conceptual validation for further clinical applications of combination treatment with ruxolitinib and zileuton for patients with PV.
5-LO expression is upregulated in numerous different types of cancer, including pancreatic, breast, prostate, esophageal and colon cancer (29–33). The products of 5-LO, such as 5-hydroxyeicosatetraenoic acid (5-HETE) and LTs, are able to promote cell proliferation, suppress apoptosis, promote angiogenesis and enhance tumor cell invasion (34–36). According to previous studies, epidermal growth factors and neurotensin are involved in the 5-LO-mediated tumor progression in individuals with prostate cancer (37,38). A study of patients with colorectal cancer revealed that 5-HETE stimulates angiogenesis by inducing the expression of VEGF (39,40). Furthermore, increased activities of 5-LO and matrix metalloproteinases are associated with extracellular matrix stiffness (41) and enhance the invasiveness of cancer cells (42,43). The enzyme 5-LO is involved in the development of not only solid malignancies but also certain forms of leukemia (44,45). Recently, the 5-LO gene was shown to be a critical regulator for mouse leukemic stem cells (LSCs) in BCR-ABL-induced chronic myeloid leukemia (CML), and the combination of zileuton and imatinib extends the survival time of mice with CML (46). This finding motivated an initial clinical trial combining zileuton with imatinib as a treatment for CML (clinicaltrials.com). Zileuton has been revealed to selectively deplete JAK2V617F-expressing HSCs, thereby preventing PV development in mice (14). The molecular mechanism of 5-LO in PV is associated with the β-catenin signaling pathway, which is required for the maintenance of both HSCs (47) and LSCs in individuals with CML (48–50).
Five-lipoxygenase inhibitors can induce apoptosis and growth arrest in human breast cancer cells through the interplay of multiple factors, including the loss of growth stimulation by 5-LO products, the induction of PPARγ, and potential activation of PPARγ by interactions with shunted endoperoxides.
5-lipoxygenase is overexpressed in colon polyps and cancer compared to normal colonic mucosa, and its inhibition can reduce colon cancer cell proliferation both in vitro and in vivo.
5-lipoxygenase and leukotriene B4 receptor are upregulated in human pancreatic cancer tissues, suggesting that lipoxygenase inhibitors could be valuable in the treatment of pancreatic cancer.
5-lipoxygenase expression is increased in esophageal cancer, and its inhibitors can induce apoptosis in esophageal cancer cells, suggesting that 5-LOX may be an effective target for esophageal cancer prevention.
5- and 12-lipoxygenase are markedly expressed in prostatic intraepithelial neoplasia and prostate cancer tissues, and their inhibitors can induce potent antiproliferative effects against prostate cancer cells, making lipoxygenase a potential new target for prostate cancer treatment.
Both 5-LOX and 12-LOX are upregulated in human pancreatic cancer cells, and their inhibitors can significantly inhibit pancreatic cancer cell proliferation, indicating that lipoxygenase inhibitors may be valuable for the treatment of pancreatic cancer.
Lipoxygenase inhibitors abolish human pancreatic cancer cell proliferation by disrupting 5-LOX and 12-LOX expression, which play critical roles in tumor cell growth.
Increased 5-LOX metabolites from hypoxic ovarian cancer cells promote tumor-associated macrophage infiltration, suggesting potential therapeutic exploitation of TAMs.
Quiescent chronic myeloid leukemia (CML) cells exhibit more transcriptional similarity to dividing cells than quiescent normal cells, with chemokines possibly playing a role in CD34+ cell mobilization.
5-lipoxygenase (5-LO) inhibitors interfere with stem cell capacity in acute myeloid leukemia (AML) through the enzymatically inactive form of 5-LO, which hinders β-catenin nuclear translocation.
Absence of the Alox5 gene impairs leukemia stem cells (LSCs) and prevents chronic myeloid leukemia development, with 5-LO inhibition potentially offering a new clinical approach for AML patients.
Lysyl oxidase inhibition in primary myelofibrosis: A renewed strategy, 2021
Primary myelofibrosis (PMF) is a type of myeloproliferative neoplasm (MPN) that portends a poor prognosis and has limited options for treatment. PMF is often driven by clonal mutations in one of three genes that regulate the JAK-STAT signaling pathway, leading to hyperactivation of this signaling pathway and over-proliferation of megakaryocytes (MKs) and their precursors. PMF presents with debilitating symptoms such as splenomegaly and weight loss. The few available treatments for PMF include a JAK2 inhibitor, ruxolitinib, which causes side effects and is not always effective. The extracellular matrix (ECM) and bone marrow (BM) microenvironment may play an important role in the pathogenesis of PMF. Lysyl oxidase (LOX), an enzyme that plays a key role in the ECM by facilitating the cross-linking of collagen and elastin fibers, has been shown to be upregulated in MKs of PMF mice and in PMF patients, suggesting its role in the progression of BM fibrosis. Recently, LOX has been identified as a potential novel therapeutic target for PMF and the development of new small molecule LOX inhibitors, PXS-LOX_1 and PXS-LOX_2, has shown some promise in slowing the progression of PMF in pre-clinical studies. Given that these inhibitors displayed an ability to target the dysregulation of the ECM via LOX inhibition, they show promise as therapeutic agents for an underappreciated aspect of PMF.
Beth K.
Hello Friends,
I am very excited to share an update regarding my recent JAK2 results— it is below .5% ! My first JAK2 test result in July 2016 was 69.9%. I was on Pegasys for 10 months, and it dropped steadily. I added in Singulair at 5th month of treatment after reading about Dr. Li’s Research. I went into molecular remission in May 2017, JAK2 was at 6.07%, and was taken off of Pegasys, as my platelets dropped to 77. I have been off Pegasys for 13 months, only on Singulair and a baby aspirin, and during this time my JAK2 continued to drop to current result of below .5%. I have had a wonderful success with Pegasys, with very little side effects. I am also vegan, and take Singulair as mentioned above. (My platelets hover around 130.)
Oral pan-LOX Inhibitor (PXS-5505) (link)
Pharmaxis has developed an oral drug inhibiting all lysyl oxidase family members. The compound has shown significant reductions in fibrosis in in-vivo models of myelofibrosis, myelodysplastic syndrome, pancreatic cancer, kidney fibrosis and lung fibrosis,. This all-encompassing LOX inhibitor is well positioned for the treatment of severe fibrosis as well as cancer with prominent stroma (connective tissue) or fibrotic metastatic niches. Pharmaxis is initially developing the compound for myelofibrosis.
PXS-5505: Pharmaxis positive interim data from myelofibrosis phase 2 cancer trial, 2022
A total of 15 patients have been enrolled in the cohort expansion phase of the study with 6 patients having completed 24 weeks of treatment (6 months). Four patients have dropped out of the study due to a lack of clinical response.
PXS-5505 has been well tolerated with no serious treatment related adverse events reported.
2/6 patients had clinically important improvement in symptoms.
5/6 patients had either stable or improved bone marrow fibrosis scores of ≥1 grade.
5/6 have stable or improved platelet and/or haemoglobin scores.
No reductions were seen in spleen volume.
“This is encouraging given the poor prognoses seen after ruxolitinib discontinuation with a median overall survival of only 11-14 months, typical of this study population. These results support further clinical investigation of PXS-5505 in myelofibrosis.”
Phase 1/2a study to evaluate safety, pharmacokinetic and pharmacodynamic dose escalation and expansion study of pxs-5505 in patients with primary, postpolycythemia vera or post-essential thrombocythemia myelofibrosis, 2022

Dr Gabriela Hobbs (Massachusetts General Hospital) on the myelofibrosis landscape and MF-101 can be seen here.
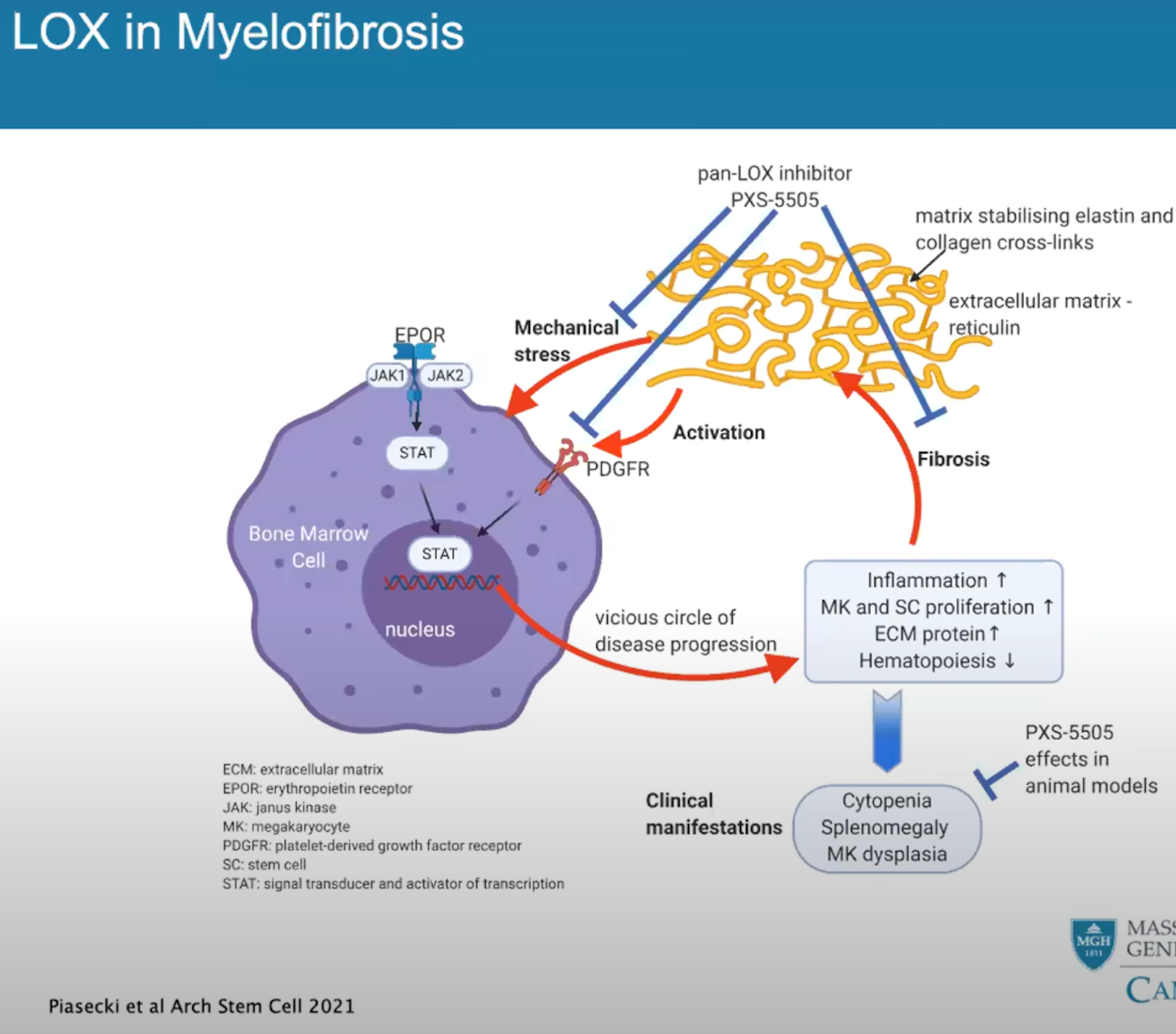
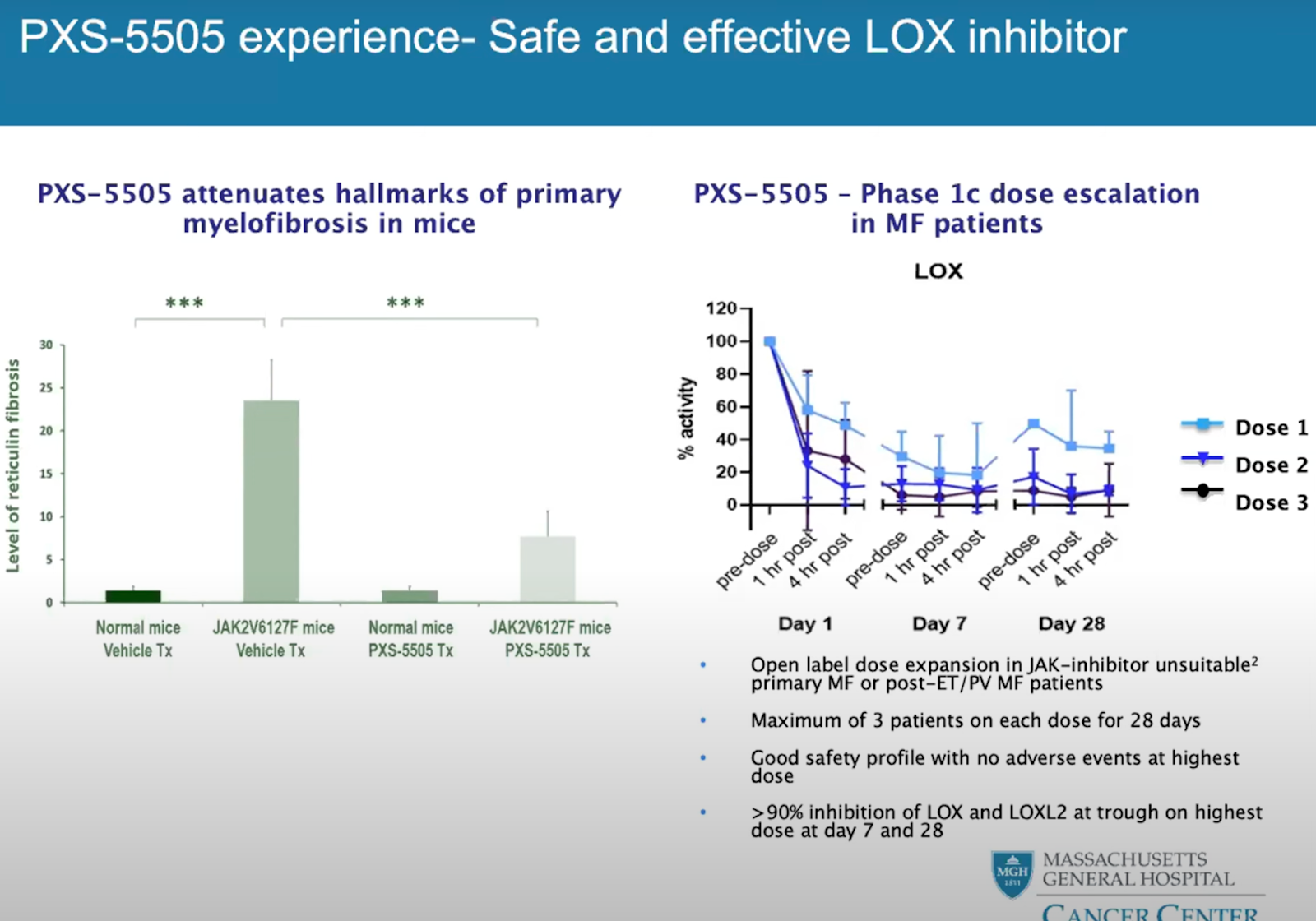
GB-2064 by Galecto (link)
Galecto, Inc. (NASDAQ: GLTO), a clinical stage biotechnology company focused on the development of novel treatments for fibrosis and cancer, today announced positive results from a planned intermediate assessment of its ongoing Phase 2a trial of GB2064 for the treatment of myelofibrosis (“MYLOX-1 trial”, NCT04679870). Fibrosis is a key disease mechanism of myelofibrosis that destroys the bone marrow function. Reducing fibrosis is required to slow the progression of the disease. Four out of five evaluable myelofibrosis patients who received GB2064 monotherapy for at least six months in the MYLOX-1 trial experienced a ≥ 1-grade reduction in collagen fibrosis of the bone marrow, an improvement suggesting that GB2064 could impact the progression of the disease and be disease modifying.
Patient Note
Just frustrated that none of the drugs that actually have reversed fibrosis are available to me. two are Lysyl Oxidase Inhibitors. PXS-5505 by Pharmaxis and GB-2064 by Galecto. Both in phase 2 trials. Dr. Mesa advised me that none of the MF trial drugs were suitable. He says that I’m still PV with some scarring(grade 2) not post PV/MF-2.
Reversing fibrosis – the ploidy connection, 2011
5 lox vs pan lox inhibitor
Lox inhibitors and pan-Lox inhibitors are types of drugs that target lipoxygenases (Lox), a family of enzymes involved in the metabolism of arachidonic acid, which is a key component in the production of inflammatory mediators called leukotrienes. Lox inhibitors are designed to specifically target one or more isoforms of the lipoxygenase enzyme, while pan-Lox inhibitors target multiple isoforms at once. The distinction between the two lies in their specificity and breadth of action.
1. Specificity: 5-Lox inhibitors are designed to selectively target the 5-lipoxygenase (5-Lox) enzyme isoform. This isoform is primarily involved in the production of leukotrienes, which contribute to inflammation and various inflammatory diseases, such as asthma, arthritis, and atherosclerosis. By inhibiting this particular isoform, 5-Lox inhibitors can help reduce inflammation and alleviate symptoms associated with these conditions.
Pan-Lox inhibitors, on the other hand, target multiple isoforms of the lipoxygenase enzyme family, rather than focusing on a specific isoform like 5-Lox inhibitors. By inhibiting several isoforms, pan-Lox inhibitors can exert broader anti-inflammatory effects, which might be beneficial in treating a wider range of inflammatory diseases or conditions.
2. Therapeutic applications: Due to their specificity, 5-Lox inhibitors are typically used to treat inflammatory conditions where the 5-lipoxygenase enzyme plays a significant role, such as asthma, arthritis, and atherosclerosis. In contrast, pan-Lox inhibitors may be utilized in a broader range of inflammatory conditions, potentially including those where multiple lipoxygenase isoforms contribute to disease progression.
3. Potential side effects: Since pan-Lox inhibitors target multiple isoforms, they may have a higher risk of causing unintended side effects compared to more targeted 5-Lox inhibitors. However, the specific side effect profile for each drug depends on its chemical structure and other factors.
What are Leukotriene receptor antagonists (LTRAs)?
Leukotriene receptor antagonists (LTRAs) are a class of drugs that work by blocking the action of leukotrienes, which are inflammatory molecules involved in the pathophysiology of asthma and allergic rhinitis. Some of the commonly prescribed LTRAs include:
Montelukast (brand name: Singulair): Montelukast is a widely used LTRA for the treatment of asthma, exercise-induced bronchoconstriction, and allergic rhinitis. It selectively blocks the cysteinyl leukotriene receptor type 1 (CysLT1) and helps to reduce bronchoconstriction, mucus production, and inflammation in the airways.
Zafirlukast (brand name: Accolate): Zafirlukast is another LTRA used in the management of asthma. Like montelukast, it also selectively blocks the CysLT1 receptor and helps to alleviate asthma symptoms by reducing airway inflammation and constriction.
Pranlukast (brand name: Onon): Pranlukast is an LTRA available in some countries, primarily in Asia, for the treatment of asthma and allergic rhinitis. It also works by blocking the CysLT1 receptor and has a similar mechanism of action as montelukast and zafirlukast.
Cysteinyl Leukotriene Receptor Antagonists Decrease Cancer Risk in Asthma Patients, 2016
Previous in vitro and in vivo studies have demonstrated the potential of using cysteinyl leukotriene receptor antagonists (LTRAs) for chemoprevention, but this has not been investigated in any clinical setting. We therefore investigated the chemopreventive effect of LTRAs in a nationwide population-based study. From the Taiwan National Health Insurance Research Database, we enrolled adults with newly-diagnosed asthma between 2001 and 2011. Among these patients, each LTRA user was matched with five randomly-selected LTRA non-users by sex, age, asthma diagnostic year and modified Charlson Comorbidity Index score. We considered the development of cancer as the outcome. Totally, 4185 LTRA users and 20925 LTRA non-users were identified. LTRA users had a significantly lower cancer incidence rate than LTRA non-users did. Multivariable Cox regression analyses adjusting for baseline characteristics and comorbidities showed LTRA use was an independent protecting factor (hazard ratio = 0.31 [95% CI: 0.24–0.39]), and cancer risk decreased progressively with higher cumulative dose of LTRAs. In conclusion, this study revealed that the LTRA use decreased cancer risk in a dose-dependent manner in asthma patients. The chemopreventive effect of LTRAs deserves further study.
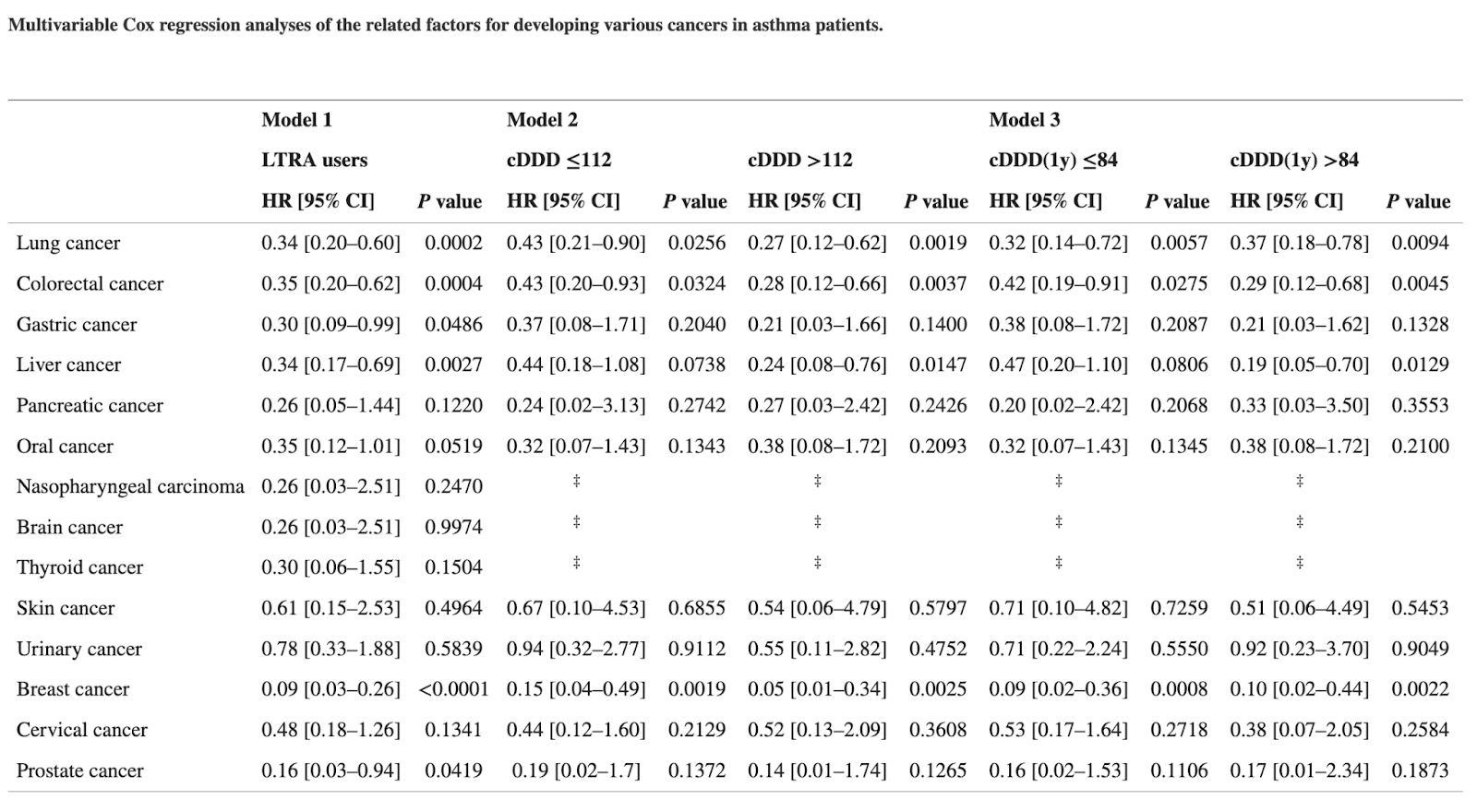
Cysteinyl Leukotriene Receptor Antagonists Associated With a Decreased Incidence of Cancer: A Retrospective Cohort Study, 2022 [From Korea]
Aim: Cysteinyl leukotrienes receptor antagonists (LTRAs) are promising chemoprevention options to target cysteinyl leukotriene signaling in cancer. However, only a number of randomized clinical trials (RCTs) or observational studies have been conducted to date; thus, the effect of LTRAs on patients is yet to be elucidated. Using insurance claim data, we aimed to evaluate whether LTRAs have cancer preventive effects by observing patients who took LTRAs.
Method: Patients diagnosed with asthma, allergic rhinitis, chronic cough, and have no history of cancer were followed-up from 2005 to 2017. Cox proportional hazard regression analysis was conducted to estimate the hazard ratios (HRs) for cancer risk of LTRA users.
Result: We followed-up (median: 5.6 years) 188,906 matched patients (94,453 LTRA users and 94,453 non-users). LTRA use was associated with a decreased risk of cancer (adjusted HR [aHR] = 0.85, 95% confidence interval [CI] = 0.83–0.87). The cancer risk showed a tendency to decrease rapidly when LTRAs were used in high dose (aHR = 0.56, 95% CI = 0.40–0.79) or for longer durations of more than 3 years (aHR = 0.68, 95% CI = 0.60–0.76) and 5 years (aHR = 0.33, 95% CI = 0.26–0.42). The greater preventive effects of LTRAs were also observed in patients with specific risk factors related to sex, age, smoking, and the presence of comorbidities.
Conclusion: In this study, we found that LTRA use was associated with a decreased risk of cancer. The high dose and long duration of the use of LTRAs correlated with a lower cancer risk. Since LTRAs are not yet used for the prevention or treatment of cancer, our findings could be used for developing a new chemo-regimen or designing feasible RCTs.
Leukotriene inhibition and the risk of lung cancer among U.S. veterans with asthma, 2021
Leukotriene inhibition, in vitro and in vivo, is found to suppress tumor growth across a variety of cancer cells. A mouse model of lung cancer revealed that the leukotriene inhibitor montelukast induced lung cancer cell death. Based on the preclinical data we hypothesize that exposure to a leukotriene inhibitor is associated with a lower risk of lung cancer. We conducted a national retrospective cohort study among U.S. Veterans with asthma to explore the relationship between leukotriene inhibition and incident lung cancer. We utilize a variety of statistical techniques, including cox proportional hazards models, propensity score matching and falsification testing to examine the association. A total of 558,466 patients met study criteria consisting of 23,730 patients with leukotriene exposure and 534,736 patients with no leukotriene medication use. Leukotriene inhibitor exposure reduced the risk of lung cancer by 17% (HR = 0.830; 95% CI = (0.757-0.911)) in the unmatched and 22.2% in the matched analysis (HR = 0.778 95% CI = (0.688-0.88)). Falsification testing with appendicitis and rotator cuff injury end points, suggest no evidence of selection bias. However, because treatment was not randomized, residual confounding cannot be ruled out. The pre-clinical data on leukotriene inhibition and lung cancer combined with our database analysis provide intriguing evidence warranting further research into the relationship between leukotrienes and lung cancer.
Leukotrienes: Inhibitors & Natural Ways to Block Them (selfhacked)
Lipoxygenase (LOX) Pathway: A Promising Target to Combat Cancer, 2021
Leukotrienes are one of the major eicosanoid lipid mediators produced due to an oxidative transformation of arachidonic acid. Subsequently, they get converted into various cellular signaling hormones by a series of enzymes of myeloid origin to mediate or debilitate inflammation. Interestingly, the available literature demonstrates the pivotal role of eicosanoids in neurodegenerative, obesity, diabetes, cardiovascular diseases, and cancers as well. The aberrant metabolism of arachidonic acid by the LOX pathway is a common feature of epithelial-derived malignancies and suggests the contributory role of dietary fats in carcinogenesis. The enzymes and receptors of the LOX pathway play a significant role in cell proliferation, differentiation and regulation of apoptosis through multiple signaling pathways and have been reported to be involved in various cancers, including prostate, colon, lung and pancreatic cancers. So far, leukotriene receptor antagonists and 5-LOX inhibitors have reached up to the clinical trials for treating various diseases. Keeping its various roles in cancer, the review highlights the components of the leukotriene synthesizing machinery, emerging opportunities for pharmacological intervention, and the probability of considering lipoxygenases and leukotriene receptors as good candidates for clinical chemoprevention studies.
Montelukast Induces Apoptosis-Inducing Factor-Mediated Cell Death of Lung Cancer Cells, 2017
CysLT1R Antagonists Inhibit Tumor Growth in a Xenograft Model of Colon Cancer, 2013
Leukotrienes in Tumor-Associated Inflammation, 2020
Leukotrienes are biologically active eicosanoid lipid mediators that originate from oxidative metabolism of arachidonic acid. Biosynthesis of leukotrienes involves a set of soluble and membrane-bound enzymes that constitute a machinery complex primarily expressed by cells of myeloid origin. Leukotrienes and their synthetic enzymes are critical immune modulators for leukocyte migration. Increased concentrations of leukotrienes are implicated in a number of inflammatory disorders. More recent work indicates that leukotrienes may also interact with a variety of tissue cells, contributing to the low-grade inflammation of cardiovascular, neurodegenerative, and metabolic conditions, as well as that of cancer. Leukotriene signaling contributes to the active tumor microenvironment, promoting tumor growth and resistance to immunotherapy. This review summarizes recent insights into the intricate roles of leukotrienes in promoting tumor growth and metastasis through shaping the tumor microenvironment. The emerging possibilities for pharmacological targeting of leukotriene signaling in tumor metastasis are considered.
Leukotriene Receptor Antagonist Therapy for the Chemoprevention of Human Rectal Aberrant Crypt Foci: Nonrandomized, Open-Label, Controlled Trial, 2022
From November 2017 to March 2020, 40 patients were enrolled. The first 30 were assigned to the LTRA group, and the remaining 10 were assigned to the observation group. In the LTRA group, the mean change in the number of ACFs per patient at 8 weeks from baseline was −2.4 ± 2.2, while the mean change in the observation group was 0.4 ± 2.3 (P = 0.002). There were no severe adverse events.
This is the first study to explore the effect of LTRAs against colorectal ACF formation in humans. LTRAs are potential candidates for chemoprevention in colorectal cancer.
Possibility of the Strategic Treatment for Various Tumors using the Leukotriene Receptor Antagonist, link
Although this is a closed trial, we have already administered the leukotriene receptor antagonist to several terminal patients, who were diagnosed as being unlikely to show any improvement, with pancreatic cancer and gastric cancer, even if conventional treatment was offered. These patients have all showed remarkable results in terms of treatment and we are currently preparing a clinical trial. As a future therapy for tumors, combination therapy with leukotriene receptor antagonists alone or other drugs is expected. We also hope that preventive medicine will be developed that prevents malignant transformation of benign tumors.
Overexpression of a cysteinyl leukotriene receptor, CysLT1R, has been shown in colorectal cancer, prostate cancer, renal cell carcinoma, transitional cell carcinoma and testicular cancer, and montelukast induces apoptosis of these cancer cells.
The leukotriene receptor antagonist montelukast in the treatment of non-alcoholic steatohepatitis: A proof-of-concept, randomized, double-blind, placebo-controlled trial, 2021
Non-alcoholic fatty liver disease (NAFLD) is associated with fat accumulation in the liver which can progress into non-alcoholic steatohepatitis (NASH). There is no specific treatment strategy for NASH. In this context, this study aimed at evaluating the efficacy and safety of montelukast in the treatment of patients with NASH. In this randomized double-blind placebo-controlled study, 52 overweight/obese patients with NASH were randomized into group 1 (n = 26) which received montelukast 10 mg tablets once daily and group 2 (n = 26) which received placebo tablets once daily for 12 weeks. The fibro-scan was used to assess liver stiffness as a primary outcome at baseline and 12 weeks post-treatment. Furthermore, patients were assessed for biochemical analysis of liver aminotransferases, metabolic parameters, TNF-α, 8-hydroxy-2'-deoxyguanosine (8-OHdG), liver fibrosis biomarkers including hyaluronic acid (HA) and transforming growth factor beta-1 (TGF-β1). Beck depression inventory questionnaire was used to report depressive symptoms. Data were statistically analyzed by paired and unpaired student's t-test, and Chi-square test. A total number of 44 patients completed the study. The two groups were statistically similar at baseline. After treatment and as compared to baseline data and placebo, montelukast showed a statistically significant improvement in liver stiffness, liver enzymes, metabolic parameters (except LDL-C), TNF-α, 8-OHdG, and liver fibrosis biomarkers (HA and TGF-β1). Furthermore, montelukast was well tolerated and didn't provoke depression. In this proof-of-concept study, treatment with montelukast may represent a promising therapeutic strategy for patients with non-alcoholic steatohepatitis secondary to its efficacy and safety.

The liver plays an important role in both synthesis and metabolism of leukotrienes (LTs). Leukotriene A4 (LTA4) is synthesized in kupffer cells which are the only liver cell type gifted with active 5-lipoxygenase (5-LO) pathway. LTA4 is taken up by hepatocytes which can’t synthesize denovo CysLTs but can conjugate LTA4 with glutathione to produce leukotriene C4 (LTC4) (Shimada et al., 1998). Moreover, inflammatory conditions are associated with increased CysLTs levels due to decreased leukotrienes excretion (Okunishi and Peters-Golden, 2011). Several studies showed that, CysLTs are involved in the pathogenesis of bile duct obstruction, hepato-renal syndrome, metabolic disorder, and other pathological conditions (Filgueiras et al., 2015; Martínez-Clemente et al., 2011). Furthermore, experimental data indicate that, CysLTs production is increased in fatty liver disease, abdominal obesity, obstructive jaundice, metabolic and hepatic disorders in fructose-induced metabolic syndrome (B¨ ack et al., 2014; Ibrahim et al., 2014; Kuru et al., 2015; Martínez-Clemente et al., 2011).
It has been demonstrated that, 5-lipoxygenase/leukotriene plays a role in obesity, insulin resistance and fatty liver disease (Martínez-Clemente et al., 2011). Leukotriene produced by 5-lipoxygenase pathway seems important in inflammation and chemotaxis. Therefore, enhanced expression of 5-lipoxygenase with subsequent increased leukotriene production could result in activation of nuclear factor-κB (NF-κB) which in turn can promote secretion of pro-inflammatory and insulin resistance mediators such as TNF-α. Oxidative stress stimulates liver X receptors, which release inflammatory mediators including TNF-α (Shoelson, 2006).
Montelukast is a CysLT1 receptor antagonist that blocks the proinflammatory action of leukotriene D4 (LTD4). Montelukast is approved for the maintenance treatment of asthma and to relieve symptoms of seasonal allergies. Montelukast inhibits neutrophil infiltration, balances oxidant-antioxidant status, fights oxidative stress and regulates the generation of inflammatory mediators (Dilek et al., 2015; Said and Bosland, 2017). Moreover, montelukast ameliorates insulin resistance which plays a critical role in the pathogenesis of NAFLD (Martínez-Clemente et al., 2011). Furthermore, it has been reported that montelukast protects against acetaminophen induced hepatotoxicity in a rat model (Weiskirchen, 2019).
Therefore, the above mentioned data encouraged us to run the current study which aimed at examining the efficacy and safety of montelukast as a possible potential therapy for patients with NASH through evaluating its effect on liver stiffness, serum levels of liver fibrosis biomarkers (hyaluronic acid (HA) and transforming growth factor beta1 (TGF-β1), insulin resistance, metabolic and inflammatory parameters.
The 5-lipoxygenase/leukotriene pathway in obesity, insulin resistance, and fatty liver disease, 2011
Purpose of review: Obesity is a major risk factor for metabolic syndrome-related comorbidities such as insulin resistance, type-II diabetes, and nonalcoholic fatty liver disease (NAFLD). A wealth of evidence indicates that the associated pathologies of the metabolic syndrome are aggravated by the presence of a chronic state of 'low-grade' inflammation in the adipose tissue. This article discusses recent data implicating lipoxygenases and especially 5-lipoxygenase and its derived products, the leukotrienes, in mounting adipose tissue inflammation and related pathologies in obesity.
Recent findings: Overexpression of selected members of the 5-lipoxygenase pathway and increased leukotriene production are common findings in excessive visceral fat depots. In these conditions, 5-lipoxygenase products exert potent proinflammatory actions including induction of nuclear factor-κB and secretion of proinflammatory and insulin resistant adipokines (i.e., monocyte chemotactic protein-1, tumor necrosis factor-α, macrophage inflammatory protein-1γ, and interleukin-6) by adipose tissue. The 5-lipoxygenase pathway also plays a major role in mounting inflammation in hepatic tissue and has emerged as a pathogenic factor in obesity-induced NAFLD. Similar role in NAFLD has been proposed for the 12/15-lipoxygenase pathway.
Summary: Modulation of lipoxygenases represents a novel target in the prevention of adipose tissue and hepatic dysfunction related to the metabolic syndrome.
Montelukast as a potential hepatoprotective drug: montelukast attenuates acetaminophen-induced liver injury in mice, 2019
Commentary: Montelukast Prevents Mice Against Acetaminophen-Induced Liver Injury, 2019
Evaluating the safety and efficacy of the leukotriene receptor antagonist montelukast as adjuvant therapy in obese patients with type 2 diabetes mellitus: A double-blind, randomized, placebo-controlled trial, 2023
Aim: This study aimed to evaluate the effectiveness, tolerability, and safety of combining montelukast therapy with metformin in obese diabetic patients.
Methods: One hundred obese diabetic adult patients were recruited and randomized into two equal groups. Group 1 received placebo plus metformin 2 g/d, and Group 2 received 2 g/d metformin plus 10 mg/d montelukast. Demographic, anthropometric measurements (e.g., body weight, body mass index [BMI], and visceral adiposity index), lipid profile, diabetes control measures (fasting blood glucose, glycated hemoglobin [HbA1c], and homeostatic model assessment for insulin resistance [HOMA-IR]), adiponectin, and inflammatory markers (e.g., TNF-α, IL-6, and leukotriene B4) were assessed and reported for each group at baseline and after 12 weeks of treatment.
Results: Both interventions significantly reduced all the measured parameters, except for adiponectin and HDL-C, levels of which increased compared to baseline data (p < 0.001). The montelukast group significantly improved in all parameters compared to the placebo group (ANCOVA test p < 0.001). The percentage changes in BMI, HbA1c, HOMA-IR, and inflammatory markers were 5%, 9%, 41%, and 5%–30%, respectively, in the placebo group compared to 8%, 16%, 58%, and 50%–70%, respectively, in the montelukast group.
Conclusion: Montelukast adjuvant therapy was superior to metformin-only therapy in diabetes control and weight loss, most likely due to its increased insulin sensitivity and anti-inflammatory properties. The combination was tolerable and safe throughout the study duration.
Potential role of leukotriene receptor antagonists in reducing cardiovascular and cerbrovascular risk: A systematic review of human clinical trials and in vivo animal studies, 2018
A total of 28 studies were included, of which 26 were conducted in animals, and 2 in humans.
Conclusions
All animal studies reported that using a leukotriene receptor antagonist brings to a reduction of either myocardial infarction, ischemic stroke, or atherosclerosis risk. Similar results were obtained from two clinical trials on humans, suggesting a potential role of montelukast in reducing some cardiovascular diseases.
Montelukast, cysteinyl leukotriene receptor 1 antagonist, inhibits cardiac fibrosis by activating APJ, 2022
Structural and functional rejuvenation of the aged brain by an approved anti-asthmatic drug, 2015
A 6-week treatment of young (4 months) and old (20 months) rats with montelukast, a marketed anti-asthmatic drug antagonizing leukotriene receptors, reduces neuroinflammation, elevates hippocampal neurogenesis and improves learning and memory in old animals. By using gene knockdown and knockout approaches, we demonstrate that the effect is mediated through inhibition of the GPR17 receptor. This work illustrates that inhibition of leukotriene receptor signalling might represent a safe and druggable target to restore cognitive functions in old individuals and paves the way for future clinical translation of leukotriene receptor inhibition for the treatment of dementias.
The 5-lipoxygenase pathway: oxidative and inflammatory contributions to the Alzheimer’s disease phenotype, 2015
5LO pathway suppression has the added benefit of being safe in other chronic conditions such as asthma (i.e., Zileuton, Monteleukast). Beyond AD, 5LO pathway targeting may also be useful in other dementias and related conditions including: non-AD amyloidoses (i.e., cerebral amyloid angiopathy), tauopathies (e.g., frontotemporal dementia, chronic traumatic encephalopathy, progressive supranuclear palsy), oxidation-linked nervous system disorders (i.e., amyotrophic lateral sclerosis) and inflammation-centered disease processes (i.e., multiple sclerosis).
A possible effect of montelukast on neurological aging examined by the use of register data, 2020
Background The leukotriene receptor antagonist montelukast has been shown to rejuvenate aged brains in rats; however, data on humans are still scarce. Objective To investigate if montelukast may alleviate degenerative neurological changes using a register data. Setting Norwegian registry data analyses. Method The present observational study was based on data from the Norwegian Prescription Database and the Tromsø Study. The former has information regarding the use of prescription medicine; the latter includes tests for brain function such as subjective memory and finger-tapping. Multivariate linear regression analyses were performed to see how the use of various medications correlated with the test results, correcting for likely confounders. Main outcome measure Results on seven different tests considered relevant for neurological health were used as outcome. Results Previous use of montelukast correlated with improved scores on cognitive or neurological functioning (F = 2.20, p = 0.03 in a multivariate test). A range of other medications were tested with the same algorithm, including drugs acting on the immune system, but none of them correlated with (overall) significantly improved test results. Conclusion The present data suggest that montelukast may alleviate degenerative neurological changes associated with human aging.
The data suggest that montelukast may postpone mental aging.
The dosage used for asthma may not be optimal for possible effects on the brain.
The data should help initiate a clinical trial to examine the effect of montelukast on aging.
Comparative study evaluating antihistamine versus leukotriene receptor antagonist as adjuvant therapy for rheumatoid arthritis, 2021
Purpose
Investigating the efficacy and safety of rupatadine (RUP) versus montelukast (MON) as adjuvant therapy for patients with rheumatoid arthritis (RA).
Methods
From December 2018 to December 2019, 75 patients with active RA were enrolled in this randomized double-blind placebo-controlled study. The patients were randomized into three groups (n = 25 in each group); methotrexate (MTX) group which received MTX 15–25 mg/week plus placebo tablet once daily; MTX/RUP group which received MTX plus RUP 10 mg once daily; and MTX/MON group which received MTX plus MON 10 mg once daily. The treatment duration was 3 months. At baseline and 3 months after treatment, blood samples were collected for the biochemical analysis of high-sensitivity C-reactive protein (hs-CRP), interleukins 8 and 17 (IL-8, IL-17), E-selectin, and clusterin (CLU) levels. Clinical and functional assessments using Disease Activity Score-CRP (DAS28-CRP) and Multidimensional Health Assessment Questionnaire (MDHAQ) were performed.
Results
Both RUP and MON produced clinical and functional improvements which were translated by significant improvements in DAS28-CRP score and MDHAQ. Rupatadine significantly reduced all measured parameters (P < 0.05) except for IL-17 and CLU. Montelukast significantly decreased all measured variables (P < 0.05) except for E-selectin. Interleukin-8 was positively correlated with IL-17 and CLU, while hs-CRP was positively correlated with E-selectin and body mass index (BMI). Both drugs were well tolerated; somnolence was the common side effect for RUP. No neuropsychiatric events were reported with MON.
Conclusion
Rupatadine or montelukast may serve as a potential adjuvant therapy for patients with rheumatoid arthritis secondary to the preliminary evidence of efficacy and safety.
The Effect of Montelukast and Low-Dose Theophylline on Cardiovascular Disease Risk Factors in Asthmatics, 2007
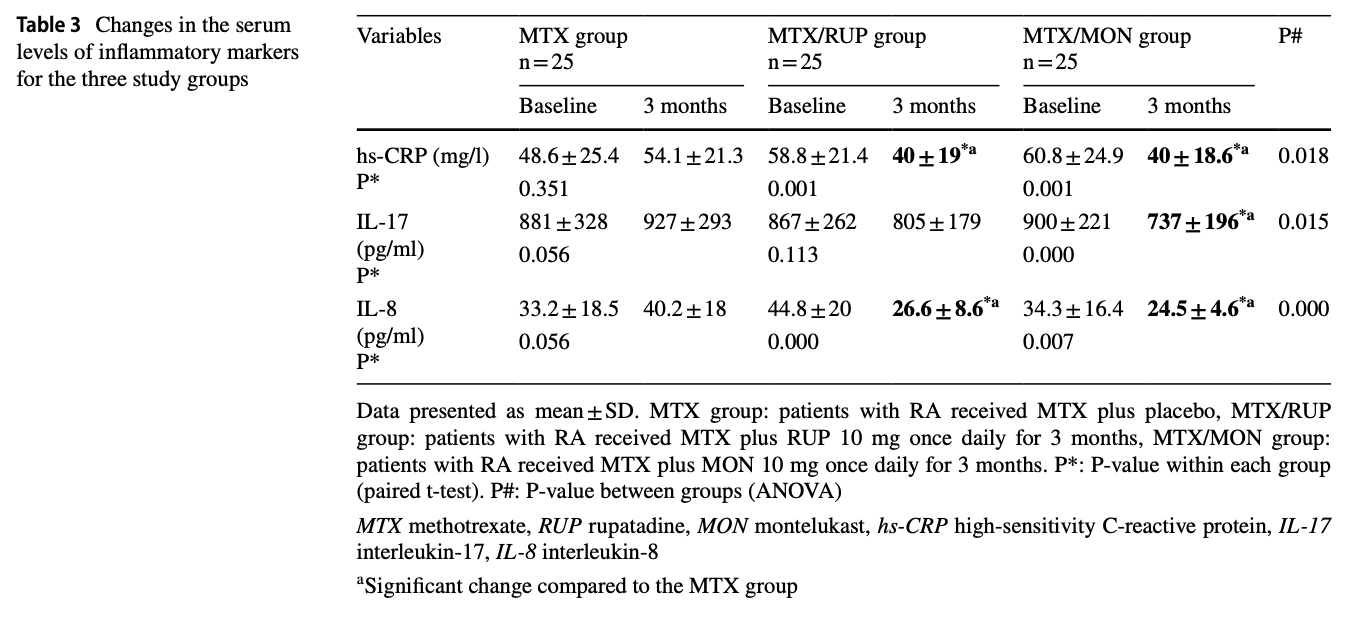
Background
Recent studies have implicated the 5-lipoxygenase/leukotriene (LT) pathway in cardiovascular disease (CVD), which may have important implications for asthmatics because several drugs that target this pathway are currently used to treat asthma. We sought to determine whether montelukast, a cysteinyl LT antagonist, and low-dose theophylline affected serum inflammatory and lipid CVD risk factors in a recently completed clinical trial in asthmatic patients.
Methods
Patients were randomized to receive either montelukast (10 mg/d), theophylline (300 mg/d), or placebo. A baseline run-in period of 7 to 14 days was followed by treatment for 6 months. Serum levels of C-reactive protein (CRP), interleukin-6, total cholesterol, triglycerides, low-density lipoprotein cholesterol, and high-density cholesterol (HDL-C) were measured 1 month and 6 months after treatment.
Results
Patients with moderate-to-severe asthma receiving montelukast (n = 60) had significantly lower serum CRP compared to placebo (n = 73) after 1 month (1.7 mg/L vs 3.2 mg/L, respectively; p < 0.006) and 6 months of treatment (2.3 mg/L vs 3.5 mg/L, respectively; p < 0.04). At both time points, serum levels of all lipids were also significantly lower in the montelukast and theophylline groups compared to placebo, but these effects were primarily observed in individuals who were also receiving inhaled corticosteroids as monotherapy for asthma.
Conclusions
Asthmatic patients receiving montelukast and, to some extent, low-dose theophylline have lower levels of CVD-associated inflammatory biomarkers and lipid levels. These observations suggest these asthma medications may have some beneficial value in asthmatics with respect to CVD risk, although the effects on HDL-C levels should also be taken into consideration.
NDGA is a cell-permeable antioxidant and a selective lipoxygenase (LOX) inhibitor (IC₅₀ = 200 nM, 30 µM, and 30 µM for 5-LOX, 12-LOX, and 15-LOX, respectively), link.
Dipyridamole + Simvastatin + Alendronate
A remarkable hematological and molecular response pattern in a patient with polycythemia vera during combination therapy with simvastatin and alendronate
https://www.sciencedirect.com/science/article/pii/S2213048916300127
Fascinating case report. The patient was on:
Aspirin 75 mg/day
Dipyramidole 200 mg 2 times/day
Simvastatin 40 mg/day
Alendronate 70 mg/week
JAK2 burden spontaneously dropped from 64% to 10-20% and the patient stayed in hematological remission for 56 months.
Dipyridamole as a new drug to prevent Epstein-Barr virus reactivation
Epstein-Barr virus (EBV) is a widely distributed gamma-herpesvirus that has been associated with various cancers mainly from lymphocytic and epithelial origin. Although EBV-mediated oncogenesis has been associated with viral oncogenes expressed during latency, a growing set of evidence suggested that antiviral treatments
directed against EBV lytic phase may contribute to prevent some forms of cancers, including EBV-positive PostTransplant Lymphoproliferative Diseases. It is shown here that dipyridamole (DIP), a safe drug with favorable and broad pharmacological properties, inhibits EBV reactivation from B-cell lines. DIP repressed immediate
early and early genes expression mostly through its ability to inhibit nucleoside uptake. Considering its wide clinical use, DIP repurposing could shortly be evaluated, alone or in combination with other antivirals, to treat EBV-related diseases where lytic replication plays a deleterious role.
Dipyridamole Anti-Platelet and Anti-Cancer Drug (link)
Inhibition of Metastases by Anticoagulants (link)
Metastasis involves several distinct steps, including one in which the tumor cell, after entry into the bloodstream, comes to rest in a capillary located at the distant site where a metastatic tumor will ultimately form. Components of the blood-clotting pathway may contribute to metastasis by trapping cells in capillaries or by facilitating adherence of cells to capillary walls. Conceivably, anticoagulants could interfere with this step in the metastatic process. In this review, we have summarized current knowledge on the interaction of malignant cells, clotting factors, and anticoagulants. We used computerized (MEDLINE®) and manual searches to identify studies done in humans, in animals, and in in vitro systems that were published in English between 1952 and 1998. We found many reports that the formation of metastatic tumors could be inhibited by heparin, a vitamin K antagonist (warfarin), and inhibitors of platelet aggregation (prostacyclin and dipyridamole). Despite these encouraging preliminary results and a compelling biochemical rationale, only limited information exists on the clinical use of anticoagulants for the prevention or treatment of metastatic cancer because there have been so few controlled and prospectively randomized studies on this topic. In view of the preliminary results, anticoagulants may hold promise for the prevention and treatment of metastases. We believe that larger controlled investigations are strongly warranted to evaluate the clinical potential of anticoagulants for the prevention and treatment of metastases in humans.
[See effects on EBV as well.]
One of the key drugs in my armamentarium was dipyridamole. Originally used as a metabolic drug to help prevent strokes before statins became widespread, it also had strong antiviral effects, so much so, that in the late 80’s it was used alongside AZT to treat HIV but then newer antiviral drug cocktails emerged. Dipyridamole became forgotten but it is once again being tested alongside the current cocktail of HIV drugs to improve outcomes in these patients. https://clinicaltrials.gov/ct2/show/NCT02121756
Dipyridamole has other effects besides being a cardiovascular and antiviral drug. I discovered reports of its powerful anticancer activity from an article in the Lancet that dated back to the mid 80's (Lancet: Mar 1985 EL Rhodes: Dipyridamole for the treatment of Melanoma). Seriously ill patients with stage 4 melanoma had no progression of their disease whilst on this drug. I explain why this is the case in my book, in brief- it is a growth inhibitor (MMP-9 inhibitor), a cholesterol modifying drug (SREBP-2 inhibitor) and nucleoside transport inhibitor (it stops nucleosides such as adenosine entering cancer cells to make new DNA).
I have long been aware of dipyridamole's potent antiviral effects and recent research from Dr Xi Liu, Wuhan Hospital University Feb 29th clearly shows potential against the Covid-19 virus. As well as being an antiviral, its has beneficial effects on the accompanying hypercoagulability that is a complication in severe cases of acute respiratory distress (ARDS). It also boosts the infection-killing white cells and it has known anti inflammatory effects. https://www.medrxiv.org/content/10.1101/2020.02.27.20027557v1
Dr Liu at the Wuhan University Hospital writes:
'The human coronavirus HCoV-19 infection can cause acute respiratory distress syndrome (ARDS), hypercoagulability, hypertension, extrapulmonary multiorgan dysfunction. Effective antiviral and anti-coagulation agents with safe clinical profiles are urgently needed to improve the overall prognosis. We screened an FDA approved drug library and found that an anticoagulant agent dipyridamole (DIP) suppressed HCoV-19 replication at an EC50 of 100 nM in vitro. It also elicited potent type I interferon responses and ameliorated lung pathology in a viral pneumonia model. In analysis of twelve HCoV-19 infected patients with prophylactic anti-coagulation therapy, we found that DIP supplementation was associated with significantly increased platelet and lymphocyte counts and decreased D-dimer levels in comparison to control patients. Two weeks after initiation of DIP treatment, 3 of the 6 severe cases and all 4 of the mild cases were discharged from the hospital. One critically ill patient with extremely high levels of D-dimer and lymphopenia at the time of receiving DIP passed away. All other patients were in clinical remission. In summary, HCoV-19 infected patients could potentially benefit from DIP adjunctive therapy by reducing viral replication, suppressing hypercoagulability and enhancing immune recovery. Larger scale clinical trials of DIP are needed to validate these therapeutic effects.'
Dipyridamole is off patent and cheap and is available TODAY. It could be trialled IMMEDIATELY as part of a cocktail to treat Covid 19, reducing the time patients spend in intense care units. With all the focus on the disease affecting the lungs, you would expect people with respiratory diseases to be top of the list for severe complications. In fact it is those with cardiovascular disease, diabetes and hypertension that are most at risk. These are all metabolic diseases. This is critically important information that is being overlooked. Blood becomes thicker, oxygenation levels reduce, heart failure and sepsis are common sequelae in these severe cases. All of these problems are not being given the attention they deserve. Doctors mistakenly believe dipyridamole, which is called an 'anti-platelet drug', reduces platelets, but as is shown above and in the medical literature, this is not the case. Dipyridamole stops platelets sticking together and as mentioned above ‘significantly increased platelets and lymphocytes’. Not only will improved blood flow help oxygenation and reduce sepsis, dipyridamole will reduce the viral load and may improve the white cell count which is critical to our ability to fight the disease.
Synergistic inhibitory effects of dipyridamole and vincristine on the growth of human leukaemia and lymphoma cell lines
The effects of combinations of dipyridamole, an effective blocker of the salvage pathway of DNA synthesis, and 8 types of anti-cancer drugs on the growth of human T, B and myeloid leukaemia/lymphoma cell lines in vitro were examined. In combinations, dipyridamole and vincristine (VCR), and dipyridamole and vindesine had synergistic inhibitory effects. Dipyridamole reduced the efflux of VCR from cells and enhanced their VCR accumulation in a dose-dependent manner at concentrations of up to 10 microM in the lymphoid cell lines, MOLT-3 and BL-TH, and of up to at least 20 microM in the myeloid cell line, ML-1. Dipyridamole also enhanced the accumulation of VCR in PHA-stimulated and un-stimulated lymphocytes of normal donors, but efflux of VCR was more rapid from normal lymphocytes than from cultured cell lines. It is proposed that combination therapy with dipyridamole plus VCR should be effective in the treatment of leukaemia and lymphoma.
Dipyridamole induces the phosphorylation of CREB to promote cancer cell proliferation
Dipyridamole, a traditional anti‑platelet drug, has been reported to inhibit the proliferation of cancer cells. The present study aimed to investigate the possibility of dipyridamole as an adjuvant of chemotherapy by enhancing the cytotoxicity of an anti‑cancer drug. The cytotoxicity of colorectal cancer cells (HCT‑8), CD133+/CD44+ stem‑like subpopulation of HCT‑8 cells and lymphoma cells (U937) to dipyridamole and/or doxorubicin was evaluated using MTT proliferation and colony forming assays. The expression levels of phosphorylated cAMP‑regulatory element‑binding protein (pCREB) and poly(ADP‑ribose) polymerase‑1 (PARP‑1) in cells were analyzed via western blotting and immunofluorescence. The present study reported controversial data regarding the anti‑cancer effect of dipyridamole. Dipyridamole increased, rather than inhibited, the proliferation of HCT‑8 and U937 cells in a dose‑dependent manner. Furthermore, it was found that dipyridamole significantly increased the expression levels of pCREB and PARP‑1. However, the combined usage of dipyridamole significantly enhanced the cytotoxicity of doxorubicin to HCT‑8 cells at particular doses. Based on the current findings, dipyridamole likely induces the phosphorylation of CREB to promote the proliferation of cancer cells, but may enhance the cytotoxicity of anti‑cancer drugs at particular doses.
Alendronate anticancer effects
Alendronate inhibits proliferation and invasion of human epidermoid carcinoma cells in vitro, 2005
Assessment of Anticancer Effect of Alendronate in Breast Cancer: An In vitro Study, 2019
Anti-Tumor Activity and Immunotherapeutic Potential of a Bisphosphonate Prodrug, 2017
Bisphosphonates have benefits in breast cancer and multiple myeloma patients and have been used with adoptive immunotherapy with γδ T cells expressing Vγ2 Vδ2 TCRs. Although treatment with γδ T cells is safe, it has shown limited efficacy. Present bisphosphonates stimulate γδ T cells but were designed to inhibit bone resorption rather than treating cancer and have limited oral absorption, tumor cell entry, and cause bone side effects. The development of phosphate and phosphonate nucleotide prodrugs has led to important drugs for hepatitis C and HIV. Using a similar approach, we synthesized bisphosphonate prodrugs and found that they efficiently limit tumor cell growth. Pivoxil bisphosphonate esters enter cells where esterases convert them to their active acids. The bisphosphonate esters stimulated γδ T cells to secrete TNF-α in response to a variety of tumor cells more efficiently than their corresponding acids. The most active compound, tetrakis-pivaloyloxymethyl 2-(thiazole-2-ylamino)ethylidene-1,1- bisphosphonate (7), specifically expanded γδ T cells and stimulated them to secrete interferon-γ and kill tumor cells. In preclinical studies, combination therapy with compound 7 and γδ T cells prolonged survival of mice inoculated with either human bladder cancer or fibrosarcoma cells. Therefore, bisphosphonate prodrugs could enhance the effectiveness of adoptive cancer immunotherapy with γδ T cells.
Technical Advance: Liposomal alendronate depletes monocytes and macrophages in the nonhuman primate model of human disease (link)
Alendronate inhalation ameliorates elastase-induced pulmonary emphysema in mice by induction of apoptosis of alveolar macrophages
We further show that alendronate inhibits macrophage migratory and phagocytotic activities and blunts the inflammatory response of alveolar macrophages by inhibiting nuclear factor-κB signalling.
In addition, there is current interest in therapeutically targeting the macrophages which provide critical support to the tumor cells, i.e. targeting them in chronic lymphocytic leukemia (CLL) has been shown to result in CLL cell death [79]. As mentioned previously, studies on animal models have shown that bisphosphonates (clodronate) induce macrophage depletion with the reversal of PV phenotype in mice. However, in a prospective, multi-center, phase II randomized trial, zoledronic acid in myelofibrosis patients showed a lack of response [80]. Finally, statins with their ‘pleiotropic effects’ have been shown to induce macrophage apoptosis and to reduce macrophage activation in atherosclerotic plaques, as well as the levels of proinflammatory cytokines, such as TNF-α and IL-6 [81–83]. These drugs have also been described to have strong antiproliferative and proapoptotic properties with the potential to decrease clonal myeloproliferation. In addition, MPN-associated JAK kinase localization to lipid rafts and its signaling was shown to be inhibited by statins [84–90]. One case report demonstrated a remarkable hematological and molecular response with the reduction of JAK2 allelic burden in a PV patient during simultaneous alendronate and simvastatin treatment [91]. However, further experimental and clinical research is needed on the potential role of these relatively non-toxic drugs in the treatment of MPNs. We can only speculate that potentially greater response could be seen in the ‘early’ disease, such as PV, than in the ‘fibrotic’ setting.
The JAK2V617 mutation induces constitutive activation and agonist hypersensitivity in basophils from patients with polycythemia vera (link)
Background: The JAK2V617F mutation has been associated with constitutive and enhanced activation of neutrophils, while no information is available concerning other leukocyte subtypes.
Design and methods: We evaluated correlations between JAK2V617F mutation and the count of circulating basophils, the number of activated CD63(+) basophils, their response in vitro to agonists as well as the effects of a JAK2 inhibitor.
Results: We found that basophil count was increased in patients with JAK2V617F -positive myeloproliferative neoplasms, particularly in those with polycythemia vera, and was correlated with the V617F burden. The burden of V617F allele was similar in neutrophils and basophils from patients with polycythemia vera, while total JAK2 mRNA content was remarkably greater in the basophils; however, the content of JAK2 protein in basophils was not increased. The number of CD63(+) basophils was higher in patients with polycythemia vera than in healthy subjects or patients with essential thrombocythemia or primary myelofibrosis and was correlated with the V617F burden. Ultrastructurally, basophils from patients with polycythemia vera contained an increased number of granules, most of which were empty suggesting cell degranulation in vivo. Ex vivo experiments revealed that basophils from patients with polycythemia vera were hypersensitive to the priming effect of interleukin-3 and to f-MLP-induced activation; pre-treatment with a JAK2 inhibitor reduced polycythemia vera basophil activation. Finally, we found that the number of circulating CD63(+) basophils was significantly greater in patients suffering from aquagenic pruritus, who also showed a higher V617F allele burden.
Conclusions: These data indicate that the number of constitutively activated and hypersensitive circulating basophils is increased in polycythemia vera, underscoring a role of JAK2V617F in these cells' abnormal function and, putatively, in the pathogenesis of pruritus.
Statin, osteoporosis drug combo may help treat parasitic infections, 2013
Athens, Ga. – Researchers at the University of Georgia have discovered that a combination of two commonly prescribed drugs used to treat high cholesterol and osteoporosis may serve as the foundation of a new treatment for toxoplasmosis, a parasitic infection caused by the protozoan Toxoplasma gondii. They published their findings recently in PLOS Pathogens.
Early experiments with an anti-malarial drug already suggest that combining atorvastatin with fosmidomycin, an antibiotic effective against malaria parasites, creates a more potent antimalarial cocktail and it may lessen the risk of drug resistance.
Epidemiologic Analysis Along the Mevalonate Pathway Reveals Improved Cancer Survival in Patients Who Receive Statins Alone and in Combination With Bisphosphonates
Purpose
Cohort studies report associations between statin use and improved survival in patients with cancer. We used pharmacoepidemiologic methods to evaluate the survival of patients with cancer who received statins alone or in ostensibly synergistic drug combinations.
Materials and Methods
Patients with cancer who were diagnosed from 2010 to 2013 were identified in a large health care claims database. The rate of all-cause death up to 1 year after diagnosis was compared by Cox proportional hazard regression. Sensitivity analyses included age stratification, statin type and intensity, and comparison with or without bisphosphonates and dipyridamole.
Results
Among 312,907 identified patients with cancer, treatment groups included statin users (n = 65,440), nonstatin users who received medications that block cholesterol absorption (n = 9,289), and nonusers (n = 226,007). Statin use before diagnosis was associated with improved overall survival compared with no treatment (hazard ratio [HR], 0.85; 95% CI, 0.80 to 0.91) and specifically in patients with leukemia, lung, or renal cancers. Nonstatin users had increased overall survival compared with no treatment (HR, 0.73; 95% CI, 0.62 to 0.85); when stratified, this difference held true only for pancreatic cancer and leukemia. No differences were observed between statin and nonstatin groups. Bisphosphonate use alone had no effect (n = 4,528), but patients who used both statins and bisphosphonates (n = 4,090) had increased survival compared with no treatment (HR, 0.60; 95% CI, 0.45 to 0.81). The effect of the combination of dipyridamole and statin use (n = 651) was not significant compared with no treatment.
Conclusion
This study suggests that the combination of statins with drugs that affect isoprenylation, such as bisphosphonates, improves survival in patients with cancer. Consideration of pathway-specific pharmacology allows for hypotheses testing with the pharmacoepidemiologic approach. Prospective evaluation of these findings warrants clinical investigation and preclinical mechanistic studies.
Bisphosphonates in renal cell carcioma
Renal cell carcinoma (RCC) is the eighth most common cancer in the USA. The approximate annual incidence is 58,240 cases and nearly a third of these present with metastases at diagnosis. Bone metastases from RCC is mostly osteolytic and leads to pathological fractures often times. At least in most of the large trials that were done in RCC, the incidence of bone metastases was in the range of 20–37%, constituting approximately a third of the metastatic RCC population. The goal of bisphosphonate therapy is purely palliative aimed at preventing skeletal-related events. There are a lack of randomized controlled trials regarding the use of bisphosphonates in RCC with bone metastases, but subgroup analysis from large bisphosphonate trials shows trends towards benefit in terms of delaying skeletal-related events and progression. However, there could be some antitumoral effect from bisphosphonate use that needs to be studied.
Bisphosphonates combined with sunitinib may improve the response rate, progression free survival and overall survival of patients with bone metastases from renal cell carcinoma (link)
Background
Bisphosphonates are used to prevent skeletal events of bone metastases, and may exhibit antitumour effects. We aimed to evaluate whether bisphosphonates can bring a response rate (RR), progression free survival (PFS) and overall survival (OS) benefit to patients with bone metastasis from renal cell carcinoma (RCC) that is treated with sunitinib.
Methods
We performed a multicentre retrospective study of patients with bone metastases from RCC that was treated with sunitinib. The effect of bisphosphonates on RR, PFS and OS was tested with adjustment for known prognostic factors using a chi-square test from contingency table and partial likelihood test from Cox regression model.
Results
Between 2004 and 2011, 209 patients with metastatic RCC were treated with sunitinib, 76 had bone metastases, 35 bisphosphonates users and 41 non-users. The groups of bisphosphonates users and non-users were balanced regarding known prognostic factors. Objective response was partial response/stable disease 86% (n = 30) versus 71% (n = 29), and progressive disease 14% (n = 5) versus 29% (n = 12) (p = 0.125, OR 2.48) in users versus non-users, respectively. Median PFS was 15 versus 5 months (HR = 0.55, p < 0.0001), and median OS was not reached (with a median follow-up time of 45 months) versus 14 months (HR = 0.4, p = 0.029), in favour of users. In multivariate analysis of the entire patient cohort (n = 76), factors associated with PFS were bisphosphonates use (HR = 0.58, p = 0.035), and pre-treatment neutrophil to lymphocyte ratio >3 (HR = 3.5, p = 0.009). Factors associated with OS were bisphosphonates use (HR = 0.5, p = 0.008), elevated pre-treatment alkaline phosphatase (HR = 2.9, p = 0.003) and sunitinib induced HTN (HR = 0.63, p < 0.0001).
Conclusions
Bisphosphonates may improve the RR, PFS and OS of sunitinib treatment in RCC with bone metastases.
Prognostic significance of bone metastases and bisphosphonate therapy in patients with renal cell carcinoma, 2014
Background: Bone metastases (BMs) are frequently present in patients with metastatic renal cell carcinoma (mRCC) and cause significant morbidity.
Objective: The purpose of this analysis was to assess the impact of BMs and bisphosphonate therapy (BT) on outcomes in mRCC.
Design, setting, and participants: We conducted a pooled analysis of patients with mRCC treated from 2003 to 2011 in phase 2 and 3 trials.
Outcome measurements and statistical analysis: Statistical analyses were performed using Cox regression and the Kaplan-Meier method.
Results and limitations: We identified 2749 patients treated with sunitinib (n=1059), sorafenib (n=355), axitinib (n=359), temsirolimus (n=208), temsirolimus plus interferon-α (IFN-α) (n=208), or IFN-α (n=560), with 28% (n=781) having BMs. A total of 285 patients (10.4%) received BT. The presence of BMs in patients was associated with shorter overall survival (OS) when compared with patients without BMs (13.2 vs 20.2 mo, respectively; p<0.0001) and shorter progression-free survival (PFS) (5.1 vs 6.7 mo, respectively; p<0.0008). When stratified by risk groups, the presence of BMs was associated with shorter OS in all risk groups. The use of BT in patients with BMs was not associated with improved OS compared with patients who did not receive BT (13.3 vs 13.1 mo, respectively; p=0.3801) or improved PFS (5.1 vs 4.9 mo, respectively; p=0.1785). Bisphosphonate users with BMs did not have a decreased rate of skeletal-related events (SREs) compared with nonusers (8.6% vs 5.8%, respectively; p=0.191). In addition, BT was associated with increased rates of hypocalcemia, renal insufficiency, and osteonecrosis of the jaw (p<0.0001). Data were analyzed retrospectively.
Conclusions: We confirm that the presence of BMs is associated with shorter survival in mRCC. BT did not affect survival or SRE prevention and was associated with increased toxicity.
Patient summary: In this analysis, we demonstrate that bone metastases are associated with shorter survival in patients with metastatic renal cell carcinoma. In addition, we call into question the utility of bisphosphonate therapy in this population.
Keywords: Bisphosphonates; Bone metastases; Renal cell carcinoma; VEGF-targeted therapy; mTOR inhibitors.
An interdisciplinary consensus on the management of bone metastases from renal cell carcinoma (link)
Bisphosphonates
Bisphosphonates are a heterogeneous group of bone-targeting agents, which are absorbed by active osteoclasts, thereby blocking their activity. Zoledronic acid is a potent inhibitor of osteoclast activity and is commonly used for treatment of bone metastases in patients with RCC26. Data in patients with RCC and bone metastases are limited to a subgroup analysis from a pivotal phase III study (n = 74) and a phase II trial (n = 50), which were performed when targeted therapies for RCC were not yet available. In these trials, zoledronic acid treatment decreased the rate of SREs to 22–37%, which compared favourably with a rate of 74% SREs in the placebo control arm of the phase III study. By contrast, a pooled analysis of data from 2,794 patients with RCC mainly treated with targeted therapies did not show a correlation between bisphosphonate, including zoledronic acid, use and outcomes (progression-free survival, overall survival, or SRE incidence)89. Interestingly, the rates of SREs in patients with or without bisphosphonate use were 8.6% and 5.8% (P = 0.1785), respectively, possibly underscoring the value of active antitumour therapy given to patients with RCC in recent years. Furthermore, an increase in hypocalcaemia, renal insufficiency, and osteonecrosis of the jaw (ONJ) was associated with the use of bisphosphonates (P < 0.0001)89. Adverse effects can be substantial. Atypical femur fractures have been reported for long-term use of bisphosphonates, including zoledronic acid. In addition, zoledronic acid requires renal function monitoring and corresponding dose adjustments44, which is of particular relevance in patients with RCC2 and are not required for denosumab treatment. As a class effect, bisphosphonates are associated with the risk of hypocalcaemia and, therefore, require calcium and vitamin D supplementation. Overall, bisphosphonates alone are of limited value in patients with bone metastases from RCC and are often used as an adjunct to targeted therapies. While the value of bisphosphonates in combination with TKIs remains unclear, such combinations have been associated with an increase of the incidence of ONJ.
Bisphosphonates May Improve Outcomes in Patients with RCC and Bone Metastases (2012)
Combining a bisphosphonate with sunitinib may improve progression-free survival (PFS) and overall survival (OS) in patients with bone metastases from renal cell carcinoma (RCC), that are treated with sunitinib, according to a multicenter, retrospective study presented at the 2012 Genitourinary Cancer Symposium.
Bisphosphonates can prevent skeletal events related to bone metastases, but the findings from this study suggest bisphosphonates also may have anti-tumor effects in this patient population, said lead investigator Daniel Keizman, MD, head of the Genitourinary Oncology Service at Meir Medical Center in Kfar-Saba, Israel, who presented the study findings.
For this investigation, he and his colleagues evaluated whether a bisphosphonate can improve the response rates, PFS, and OS in patients with RCC and bone metastases treated with sunitinib. Patients were divided into bisphosphonate users (Group 1) and non-users (Group 2).
From 2004-2011, 209 patients with metastatic RCC were treated with sunitinib. Of these, 76 patients had bone metastases (35 patients in Group 1 and 41 in Group 2). The groups were balanced in terms of known prognostic factors. The patients were also balanced with regard to past cytokines/targeted treatments, and mean sunitinib dose/cycle. Objective response was partial response/stable disease in 30 patients (86%) in Group 1 compared with 29 patients (71%) in Group 2. Moreover, disease refractory to sunitinib treatment occurred in five patients (14%) of Group 1 compared with 12 patients (29%) of Group 2. The median PFS was 15 months for Group 1 compared with five months for Group 2. Median OS was not reached (with a median follow-up of 45 months) for group 1 versus 14 months for group 2.
“We found that the use of bisphosphonates decreased the risk of disease progression by 45% and of dying by approximately 60%,” Dr. Keizman said.
Making Cholesterol-Lowering Statin Drugs More Effective Against Cancer
https://www.cancertreatmentsresearch.com/cholesterol-lowering-statin-drugs-to-fight-cancer/
New interferon/lovastatin treatment to battle cancer
https://www.news-medical.net/news/20090921/New-interferonlovastatin-treatment-to-battle-cancer.aspx
After the first round of surgical procedures, Cantrell enrolled in a clinical trial testing a cancer vaccine. The melanoma recurred anyway, and more surgery followed. Interferon was next but to no avail.
A year later the cancer changed into a much more aggressive form and began shooting new tumors around his neck and chest with alarming speed. Doctors then advised that his condition would deteriorate rapidly and he probably had about six weeks left to live. "They told me to find a nice beach somewhere and enjoy a few sunsets," Cantrell remembered. "I said no. I worked with some great surgeons, and they were willing to get me on the table the next day whenever a new metastasis popped up."
The surgeries to fight the new metastases were frequent. "Those were dark days," he continued. "I was getting my neck or chest sliced open sometimes every two or three weeks. At one point I had to stick a large needle in my own neck twice a day to drain the fluid buildup." It still wasn't enough.
In July 2000 he underwent yet another selective neck dissection, but two weeks later there were new tumors deeper in the neck. "I had access to some of the most prominent doctors in the field," Cantrell explained, "but there really wasn't anything else they could offer. At that point, nothing works." Realizing he was out of treatment options, he knew he would have to step into the unknown to fight any further.
He went back to the medical literature, searching for any reasonable thing that was too new to have been fully tested or perhaps had been overlooked. There was nothing. Finally, he took an educated guess that a combination of lovastatin and interferon might have a shot at working.
He was criticized sharply by most of his doctors; they urged him to quit making his own treatment decisions and go with the standard drugs, even though they held no real potential. Instead Cantrell decided that his only hope was to do something he would never ask of anyone else: experiment on himself with a completely untested treatment. "At that point there was nothing to lose," he explained. "As it stood I was going to be dead very soon, so any potential at all made it a risk worth taking." He continued keeping careful notes and became the guinea pig for the new technique.
Not even he was prepared for what happened next. After four weeks of the new combination, scans showed no remaining evidence of cancer. The radiologist assumed that the neck metastases had been surgically removed; their disappearance with a simple drug regimen was unthinkable. "I don't know what you did," he said, "but you're clean."
Novel aspects of mevalonate pathway inhibitors as antitumor agents
The mevalonate pathway for cholesterol biosynthesis and protein prenylation has been implicated in various aspects of tumor development and progression. Certain classes of drugs, such as statins and bisphosphonates, inhibit mevalonate metabolism and therefore have also been tested as antitumor agents. This concept is strongly supported by the recent finding that mutant p53, which is present in more than half of all human cancers, can significantly upregulate mevalonate metabolism and protein prenylation in carcinoma cells. The first evidence that mevalonate pathway inhibitors may have the potential to reverse the malignant phenotype has already been obtained. Moreover, recently discovered immunomodulatory properties of statins and bisphosphonates may also contribute to their known anticancer effects. Drug-induced inhibition of protein prenylation may induce sequential cellular stress responses, including the unfolded protein response and autophagy, that eventually translate into inflammasome-dependent and caspase-1-mediated activation of innate immunity. This review focuses on these novel capabilities of mevalonate pathway inhibitors to beneficially affect tumor biology and contribute to tumor immune surveillance.
Targeting tumor cell metabolism via the mevalonate pathway: Two hits are better than one
Statins are promising anticancer agents that target the mevalonate pathway. Tumor cells are sensitive to depletion of mevalonate-derived products but this activity triggers a homeostatic feedback loop that blunts statin efficacy. We showed that dipyridamole inhibits this feedback response and potentiates statin antitumor activity. This study identifies statins plus dypridamole as a preclinically effective combination of approved agents.
Keywords: Mevalonate, HMG-CoA Reductase, SREBP2, statins, dipyridamole
Some tumor cells have altered metabolism that culminates in an increased dependence on MVA-derived which products and sensitizes them to MVA pathway inhibition.1 For example, the MVA pathway contributes to oncogenic progression7 and is upregulated by mutant p53,8 supporting the concept that tumor cells can be dependent upon the MVA pathway. Tumor cell-specific apoptosis following statin-induced MVA pathway inhibition has been linked to depletion of the MVA end products farnesyl and geranylgeranyl pyrophosphate. These isoprenoid moieties are essential for the post-translational prenylation and activation of critical signaling proteins such as Ras. However, cholesterol depletion within both the tumor and the extracellular milieu may also contribute to tumor-specific apoptosis, which is triggered in response to statins.3 We anticipate that the mechanism of statin antitumor effects likely involves multiple aspects of statin activity on the MVA pathway. In our research7,9,10 we have focused our attention on the direct antiproliferative effects of statins on tumor cells and how best to use statins as anticancer agents.
[BIG] Loss of p53 induces leukemic transformation in a murine model of Jak2 V617F-driven polycythemia vera
Our results show that p53 loss is sufficient for inducing leukemic transformation in Jak2 V617F-positive MPN (mice).
Anti Cholesterol Strategy to Fight Cancer
https://www.cancertreatmentsresearch.com/reduce-cholesterol-in-cancer-cells-to-fight-cancer/
inhibit cholesterol production (mevalonate) pathway: use Statins (that inhibit HMG-CoA reductase (HMGCR)) and possibly bisphosphonates. Indeed recent research indicates that “Statin and Bisphosphonate Induce Starvation in Fast-Growing Cancer Cell Lines“.
Tumor cells are sensitive to depletion of mevalonate-derived products but this activity triggers a homeostatic feedback loop that blunts statin efficacy. Dipyridamole inhibits this feedback response and potentiates statin antitumor activity (inhibiting the cleavage of SREBP2). So Dipyridamole is an important addition in order to maintain statins effectiveness (Ref.1, Ref.2).
Dose: 200mg 2 x day
Source: any pharmacy
Risk of bleeding with aspirin and dipyridamole (link)
Results: adjusted odds ratios associating drug use with upper gastrointestinal bleeding were
1.8 (95% confidence interval 1.5 to 2.1) for low dose aspirin
1.1 (0.6 to 2.1) for clopidogrel
1.9 (1.3 to 2.8) for dipyridamole
1.8 (1.3 to 2.4) for vitamin K antagonists
corresponding figures for combined use were
7.4 (3.5 to 15) for clopidogrel and aspirin
5.3 (2.9 to 9.5) for vitamin K antagonists and aspirin,
2.3 (1.7 to 3.3) for dipyridamole and aspirin
number of treatment years needed to produce one excess case varied from 124 for the clopidogrel-aspirin combination to 8800 for clopidogrel alone
Risk of bleeding complications with antiplatelet agents: meta-analysis of 338,191 patients enrolled in 50 randomized controlled trials
Low-dose aspirin and dipyridamole therapy were associated with the lowest risk of bleeding (3.6% and 6.7%, respectively).
Apigenin (Celery / Parsley)
GENERAL SUMMARY:
Apigenin is a natural bioflavonoid found in a variety of plants such as parsley, celery, chamomile and artichokes. It is a yellow crystalline solid and is part of the flavone class of flavonoids, which are responsible for the color and flavor of many plants.
Research has shown that consuming foods high in apigenin is associated with protection against various diseases, including cardiovascular disease, neurodegenerative disorders, and certain types of cancer.
Apigenin sources: Dried parsley contains the highest apigenin concentration at 45,035 μg/g, followed by dried chamomile flowers (3,000-5,000 μg/g), celery seeds (786.5 μg/g), vine spinach (622 μg/g), and Chinese celery (240.2 μg/g).
I prefer Suja Uber Greens Juice daily (0.5 bottle/day). Gives me really good energy to get through the day or go out an do some exercise occasionally.
METABOLIC EFFECTS:
A 2022 study found that a specific CD38 inhibitor, 78c, increased mice lifespan (+10%) and healthspan in a model of chronological aging, raising the hopes that apigenin too might improve mice lifespan.
Apigenin may inhibit CD38, a major NAD+ consumer, thereby potentially boosting NAD+ levels, which could offer an alternative approach to taking NAD+ precursors for addressing age-related NAD+ depletion. (2013)
Apigenin inhibits platelet adhesion and thrombus formation, synergizing with aspirin in suppressing the arachidonic acid pathway (2008).
Anti-diabetic effects: Celery seeds contain an anti-microbial compound that effectively blocks gastric H. pylori growth, a bacterium linked to a nearly three-fold increased risk of type II diabetes (2012).
ANTI-CANCER EFFECTS:
Apigenin was reported to suppress various human cancers in vitro and in vivo by multiple biological effects, such as triggering cell apoptosis and autophagy, inducing cell cycle arrest, suppressing cell migration and invasion, and stimulating an immune response (2017).
In a 2008 study, long-term flavonoid treatment (daily 20 mg apigenin and 20 mg EGCG) treatment of 87 patients with resected colorectal cancer led to a 7% neoplasia recurrence rate compared to 47% in controls, suggesting that flavonoids could effectively reduce colon cancer recurrence (P = 0.027).
A 2010 study demonstrated that apigenin can inhibit leukemia cell proliferation and induce cell-cycle arrest, but may also reduce chemotherapy sensitivity in certain cell types, suggesting caution in its consumption during treatment.
Apigenin induced apoptosis in human leukemia cells by inactivating Akt, activating JNK, and downregulating Mcl-1 and Bcl-2, while in vivo apigenin administration led to attenuation of tumor growth in U937 xenografts, highlighting its potential for incorporation in leukemia treatment regimens (2012).
Apigenin acts as a cell-signaling pathway modulator in cancer prevention and treatment, reducing the expression of STAT3, STAT5, and JAK2 in breast cancer cell lines (SKBR3 and MDA-MB-453,HER2) and inhibiting tumor proliferation and growth. (2021)
Apigenin potentiates the inhibitory effect of interferon-α on cancer cell viability by inhibiting 26S proteasome-mediated interferon receptor degradation and activating JAK/STAT signaling pathway, providing a novel mechanism for increasing the efficacy of type I interferons (2016).
Apigenin enhances the IFN-α/β-induced activation of the JAK/STAT pathway by increasing ISRE luciferase reporter expression and the tyrosine phosphorylation of STAT1 and STAT2, ultimately leading to increased mRNA expression of IFN-α-responsive genes PKR and 2’,5’-OAS1. (2016)
Apigenin suppressed Renal Cell Carcinoma (RCC) cell proliferation, induced DNA damage, G2/M phase cell cycle arrest, and p53-dependent apoptosis, leading to reduced tumor growth in a xenograft mouse model, showing promise for RCC treatment (2017)
Prospective cohort comparison of flavonoid treatment in patients with resected colorectal cancer to prevent recurrence (link)
Aim: To investigate biological prevention with flavonoids the recurrence risk of neoplasia was studied in patients with resected colorectal cancer and after adenoma polypectomy.
Methods: Eighty-seven patients, 36 patients with resected colon cancer and 51 patients after polypectomy, were divided into 2 groups: one group was treated with a flavonoid mixture (daily standard dose 20 mg apigenin and 20 mg epigallocathechin-gallat, n = 31) and compared with a matched control group (n = 56). Both groups were observed for 3-4 years by surveillance colonoscopy and by questionnaire.
Results: Of 87 patients enrolled in this study, 36 had resected colon cancer and 29 of these patients had surveillance colonoscopy. Among the flavonoid-treated patients with resected colon cancer (n = 14), there was no cancer recurrence and one adenoma developed. In contrast the cancer recurrence rate of the 15 matched untreated controls was 20% (3 of 15) and adenomas evolved in 4 of those patients (27%). The combined recurrence rate for neoplasia was 7% (1 of 14) in the treated patients and 47% (7 of 15) in the controls (P = 0.027).
Conclusion: Sustained long-term treatment with a flavonoid mixture could reduce the recurrence rate of colon neoplasia in patients with resected colon cancer.
How much apigenin in parsley?
Dried parsley can contain about 45 mg/gram ... The apigenin content of fresh parsley is reportedly 215.5 mg …
Mike Lusgarten’s diet: (Parsley = 47g/day, only 13% is dry mass… around 6g)
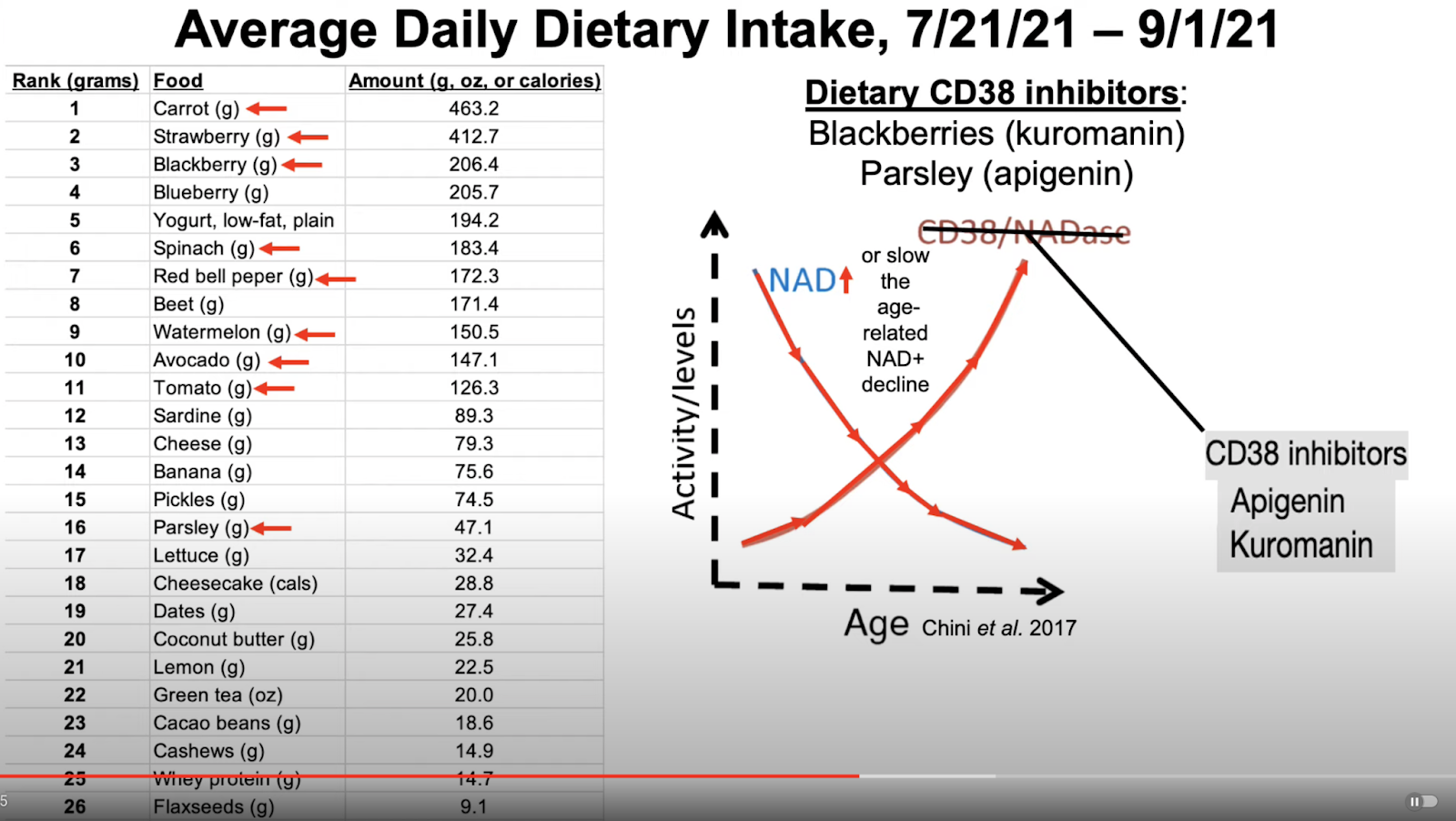
Cytotoxicity of apigenin on leukemia cell lines: implications for prevention and therapy, 2009
Natural-food-based compounds show substantial promise for prevention and biotherapy of cancers including leukemia. In general, their mechanism of action remains unclear, hampering rational use of these compounds. Herein we show that the common dietary flavonoid apigenin has anticancer activity, but also may decrease chemotherapy sensitivity, depending on the cell type. We analyzed the molecular consequences of apigenin treatment in two types of leukemia, the myeloid and erythroid subtypes. Apigenin blocked proliferation in both lineages through cell-cycle arrest in G2/M phase for myeloid HL60 and G0/G1 phase for erythroid TF1 cells. In both cell lines the JAK/STAT pathway was one of major targets of apigenin. Apigenin inhibited PI3K/PKB pathway in HL60 and induced caspase-dependent apoptosis. In contrast, no apoptosis was detected in TF1 cells, but initiation of autophagy was observed. The block in cell cycle and induction of autophagy observed in this erythroleukemia cell line resulted in a reduced susceptibility toward the commonly used therapeutic agent vincristine. Thus, this study shows that although apigenin is a potential chemopreventive agent due to the induction of leukemia cell-cycle arrest, caution in dietary intake of apigenin should be taken during disease as it potentially interferes with cancer treatment.
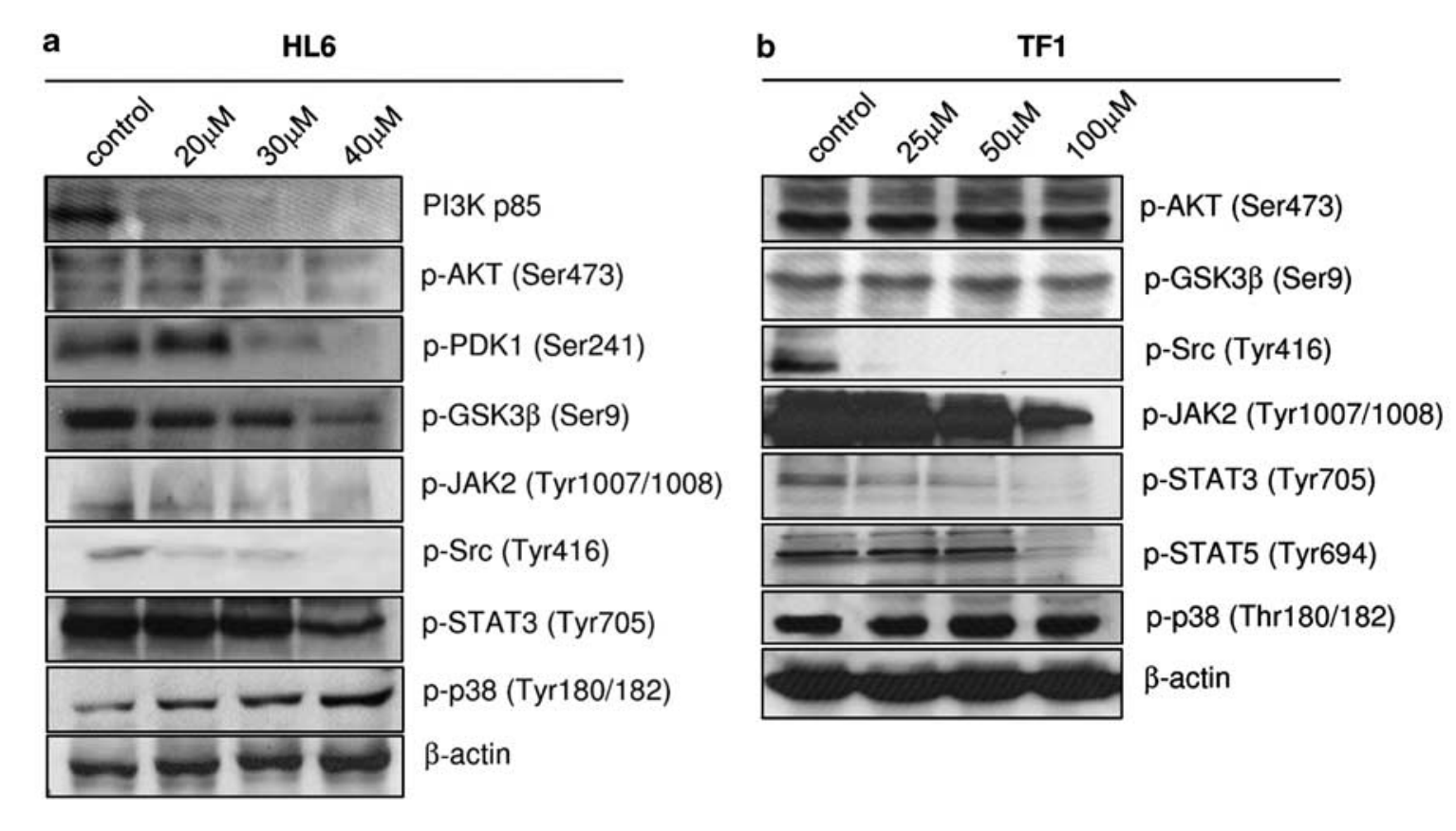
Apigenin induces apoptosis in human leukemia cells and exhibits anti-leukemic activity in vivo (link)
In this study, we investigated the functional role of Akt and c-jun-NH(2)-kinase (JNK) signaling cascades in apigenin-induced apoptosis in U937 human leukemia cells and anti-leukemic activity of apigenin in vivo. Apigenin induced apoptosis by inactivation of Akt with a concomitant activation of JNK, Mcl-1 and Bcl-2 downregulation, cytochrome c release from mitochondria, and activation of caspases. Constitutively active myristolated Akt prevented apigenin-induced JNK, caspase activation, and apoptosis. Conversely, LY294002 and a dominant-negative construct of Akt potentiated apigenin-induced apoptosis in leukemia cells. Interruption of the JNK pathway showed marked reduction in apigenin-induced caspase activation and apoptosis in leukemia cells. Furthermore, in vivo administration of apigenin resulted in attenuation of tumor growth in U937 xenografts accompanied by inactivation of Akt and activation of JNK. Attenuation of tumor growth in U937 xenografts by apigenin raises the possibility that apigenin may have clinical implications and can be further tested for incorporating in leukemia treatment regimens.
Apigenin Inhibits Platelet Adhesion and Thrombus Formation and Synergizes with Aspirin in the Suppression of the Arachidonic Acid Pathway (link)
Quercetin induces apoptosis by activating caspase-3 and regulating Bcl-2 and cyclooxygenase-2 pathways in human HL-60 cells (acute leukemia) (link)
Dietary apigenin potentiates the inhibitory effect of interferon-α on cancer cell viability through inhibition of 26S proteasome-mediated interferon receptor degradation, 2016 (link)
Background
Type I interferons (IFN-α/β) have broad and potent immunoregulatory and antiproliferative activities. However, it is still known whether the dietary flavonoids exhibit their antiviral and anticancer properties by modulating the function of type I IFNs.
Objective
This study aimed at determining the role of apigenin, a dietary plant flavonoid abundant in common fruits and vegetables, on the type I IFN-mediated inhibition of cancer cell viability.
Design
Inhibitory effect of apigenin on human 26S proteasome, a known negative regulator of type I IFN signaling, was evaluated in vitro. Molecular docking was conducted to know the interaction between apigenin and subunits of 26S proteasome. Effects of apigenin on JAK/STAT pathway, 26S proteasome-mediated interferon receptor stability, and cancer cells viability were also investigated.
Results
Apigenin was identified to be a potent inhibitor of human 26S proteasome in a cell-based assay. Apigenin inhibited the chymotrypsin-like, caspase-like, and trypsin-like activities of the human 26S proteasome and increased the ubiquitination of endogenous proteins in cells. Results from computational modeling of the potential interactions of apigenin with the chymotrypsin site (β5 subunit), caspase site (β1 subunit), and trypsin site (β2 subunit) of the proteasome were consistent with the observed proteasome inhibitory activity. Apigenin enhanced the phosphorylation of signal transducer and activator of transcription proteins (STAT1 and STAT2) and promoted the endogenous IFN-α-regulated gene expression. Apigenin inhibited the IFN-α-stimulated ubiquitination and degradation of type I interferon receptor 1 (IFNAR1). Apigenin also sensitized the inhibitory effect of IFN-α on viability of cervical carcinoma HeLa cells.
Conclusion
These results suggest that apigenin potentiates the inhibitory effect of IFN-α on cancer cell viability by activating JAK/STAT signaling pathway through inhibition of 26S proteasome-mediated IFNAR1 degradation. This may provide a novel mechanism for increasing the efficacy of IFN-α/β.
Apigenin enhances the IFN-α/β-induced activation of the JAK/STAT pathway (2016)
Considering the important role of 26S proteasome in the attenuation of JAK/STAT pathway signaling, we hypothesize that apigenin may enhance the activation of JAK/STAT pathway by inhibiting 26S proteasome. To test this, we first examined the effect of apigenin on IFNα/β-induced JAK/STAT signaling. As shown in Fig. 4a, apigenin potently increased ISRE luciferase reporter expression induced by IFN-α or IFN-β in a concentration-dependent manner. Apigenin at 10 µM alone significantly increased ISRE reporter expression, as previously reported (17). We then examined the effect of apigenin alone on tyrosine phosphorylation of STAT1, the key factor mediating ISRE gene transcription. However, no obvious tyrosine phosphorylation of STAT1 was observed, possibly owing to the limitation of detection using anti-phospho-STAT1 antibody (data not shown). To further determine the effect of apigenin on type I IFNs, we examined the phosphorylation state of STATs in response to IFN-α. Apigenin increased the tyrosine phosphorylation of STAT1 and STAT2 in a concentration-dependent manner over that observed with IFN-α alone (Fig. 4b). The tyrosine phosphorylation of STAT1 was also increased in combination with luteolin and various concentrations of IFN-α (Supplementary Fig. 3). PKR and 2’,5’-OAS1 are IFN-α-responsive genes that contain an ISRE consensus sequence in their promoter regions. We examined the effect of apigenin on the mRNA expression of these two genes in combination with IFN-α. As shown in Fig. 4c, the mRNA expression of both IFN-regulated genes significantly increased after treatment with a combination of apigenin and IFN-α over that accompanying IFN-α treatment alone. These results indicate that apigenin enhances the activation of type I IFNs-induced JAK/STAT signaling.
Apigenin role as cell-signaling pathways modulator: implications in cancer prevention and treatment, 2021
By preventing the STAT3 phosphorylation, apigenin prevents the activation of MMPs, TWIST1 and VEGF [23]. It has been evidenced from cell lines experiments conducted on Breat Cancer cell lines (SKBR3 and MDA-MB-453,HER2), that apigenin successfully reduces the expression of STAT3, STAT5 and JAK2 thus preventing tumor proliferation and growth.
Mike Lustgarten
Apigenin also inhibits CD38, thereby boosting NAD:
https://www.youtube.com/watch?v=5-2YoGctcCk&t=5s
May Inhibit CD38 in Vivo (2013)
Apigenin is actually gaining popularity because of the possibility that it may inhibit CD38, a major NAD+ consumer which increases with age, causing the noted depletion of NAD+. Rise in CD38 may be due to any number of factors further upstream, such as inflammation. Take care that your diet is not inflammatory first. Depending on your age, diet and other factors you may notice different results with this product. That said, rather than taking NAD+ precursors, this may be a better, and relatively cheaper alternative. Until studies show us more, or until recent drugs targeting CD38 pass phase III trials, this is all we have.
CD38 inhibitor 78c increases mice lifespan and healthspan in a model of chronological aging, 2022
Nicotinamide adenine dinucleotide (NAD) levels decline during aging, contributing to physical and metabolic dysfunction. The NADase CD38 plays a key role in age-related NAD decline. Whether the inhibition of CD38 increases lifespan is not known. Here, we show that the CD38 inhibitor 78c increases lifespan and healthspan of naturally aged mice. In addition to a 10% increase in median survival, 78c improved exercise performance, endurance, and metabolic function in mice. The effects of 78c were different between sexes. Our study is the first to investigate the effect of CD38 inhibition in naturally aged animals.
Apigenin has a great anxiolytic effect!
Within minutes after taking this product, I could experience a positive effect. I started to feel more relaxed and less nervous. I have started to take it because I read that it has this type of effect on the nervous system and the brain. Nevertheless the effect is rather on the mild side. But only one capsule a day is enough. Half life of this product in our bodies is more than 90 hours. Therefore it has a relatively long term effect. I also read that if we take a higher dosage of Apigenin it may have a sedative effect. I took two capsules a day but saw no difference, however, I still noticed a good relaxing and anxiolytic effect. Therefore, I continue with only one capsule a day. I also noticed that physically and mentally I feel less tired: I think that this is due to the fact that such flavonoids are good for strengthening for the blood vessels; thus the blood can circulate better and nurture the muscles and brain more easily. Furthermore, I read that Apigenin has a destructive effect on the proliferation of cancer cells. With so many benefits, I am surprised that Apigenin is not better known and that not more manufacturers are selling this anti-aging product.
* Sleeping better. Kind of relaxes the thoughts.
Apigenin Inhibits Renal Cell Carcinoma Cell Proliferation (2017)
We found that apigenin suppressed ACHN, 786-0, and Caki-1 RCC cell proliferation in a dose- and time-dependent manner. A comet assay suggested that apigenin caused DNA damage in ACHN cells, especially at higher doses, and induced G2/M phase cell cycle arrest through ATM signal modulation. Small interfering RNA (siRNA)-mediated p53 knockdown showed that apigenin-induced apoptosis was likely p53 dependent. Apigenin anti-proliferative effects were confirmed in an ACHN cell xenograft mouse model. Apigenin treatment reduced tumor growth and volume in vivo, and immunohistochemical staining revealed lower Ki-67 indices in tumors derived from apigenin-treated mice. These findings suggest that apigenin exposure induces DNA damage, G2/M phase cell cycle arrest, p53 accumulation and apoptosis, which collectively suppress ACHN RCC cell proliferation in vitro and in vivo. Given its antitumor effects and low in vivo toxicity, apigenin is a highly promising agent for treatment of RCC.
Dried parsley has been reported to have the maximum quantity of apigenin, at 45,035 μg/g. Additional sources of apigenin are dried flower of chamomile, containing 3,000 to 5,000 μg/g; celery seeds, containing 786.5 μg/g; and vine spinach and Chinese celery, containing 622 μg/g and 240.2 μg/g [16].
Time to Celebrate Celery (link)
It is believed apigenin works by decreasing the expression of vascular endothelial growth factor (VEGF), a protein that stimulates the formation of new blood vessels that are vital for tumor growth. In a study published in the journal Pharmacology Magazine, scientists found that rats supplemented with celery seed extract daily for 60 days significantly reduced triglycerides levels by 22% and LDL cholesterol by 27%, along with a 28% increase in beneficial HDL cholesterol.14 The lipid lowering effects of celery are due to the increased conversion of cholesterol into bile acids, which are eliminated in feces.15
In addition to its beneficial effects on lipid levels, celery also shows promise in lowering blood pressure. In the laboratory, celery seeds exhibited potent inhibition of angiotensin converting enzyme (ACE), a protein responsible for constricting blood vessels and elevating blood pressure. This may partially explain the results reported in a study published in the Tehran University Medical Journal in which 37 hypertensive patients between the ages of 45 and 65 administered 6 grams of celery seed powder significantly lowered mean systolic and diastolic readings by 17.1 and 4.4 mmHg, respectively.17
The anti-diabetic benefits of celery can also be attributed to its unique ability to fight Helicobacter pylori (H. pylori), a bacterium that leads to a near three-fold increase in the risk of type II diabetes. In a study reported in the Journal of Pharmacy and Pharmacology, researchers identified an anti-microbial compound in celery seeds that is highly effective in blocking the growth of gastric H. pylori.21
Beta Alanine / Carnosine
GENERAL EFFECTS (REF):
Beta-alanine is the rate-limiting precursor for carnosine synthesis. Carnosine is a dipeptide found in high levels in muscles and brain.
Carnosine is concentrated in high-energy tissues and declines significantly with human age (2015). Supplementation restores youthful tissue concentrations. (2-5)
Extends lifespan and improves healthspan in multiple animal species including mice, fruit flies, and rotifers. It maintains youthful physiology and appearance. (12-16)
Rejuvenates aged senescent human cells in culture, restoring youthful morphology. It preserves cell viability at late passages. (10-11)
Has broad antioxidant effects, defending cells and tissues from oxidative damage. This may prevent cancers and atherosclerosis. (1, 62, 66-68)
Protects the brain from multiple age-related insults. It is concentrated in brain regions vulnerable in Alzheimer's and further reduced in patients. (43-47)
Guards the heart and vessels from ischemic damage and atherosclerosis through antioxidant, anti-glycation, and acid-buffering mechanisms. (19-27)
Mitigates accelerated aging processes like glycation, protein cross-linking, and mitochondrial dysfunction. It improves proteostasis. (5, 65, 67-68, 73-74)
Enhances exercise capacity and performance in the elderly by buffering lactic acid accumulation. It reduces fatigue and improves endurance. (54-63)
Proposed mechanisms include multifaceted antioxidant effects, AGE/ALE reduction, improved proteostasis, reduced methylglyoxal, membrane stabilization, heavy metal chelation, and telomere preservation. (1, 47, 62-74)
Animal studies demonstrate carnosine can bind to and neutralize formaldehyde, a toxic compound. A rat study showed carnosine supplements reduced oxidative damage and improved learning impairments caused by inhaled formaldehyde.
Optimal dosing is not established. Doses of 800-3000 mg beta-alanine per day are commonly used, split into multiple servings.
EFFECTS ON CANCER (REF):
Animal and cell studies show carnosine and beta-alanine inhibit growth and proliferation in many cancer cell types through various proposed mechanisms. These include reducing ATP energy production, inhibiting cell signaling pathways like mTOR, decreasing inflammation, and buffering lactic acid.
Reduced cancer growth significantly in cell and mice studies across cancers: Breast, renal, cervical, pancreatic etc.
Some users report life-changing relief from severe itching from polycythemia vera.
Small human studies provide preliminary evidence of anticancer effects, but larger clinical trials are required to verify optimal dosing, safety and efficacy in humans.
EFFECTS ON EXERCISE (REF):
A popular ingredient in pre-workout stacks.
Carnosine acts as a buffer against acid buildup during high-intensity exercise, reducing fatigue. Secondary to that, it improves time to exhaustion.
Supplementation enhances muscular endurance. Many people report being able to perform one or two additional reps in the gym. Also improves moderate- to high-intensity cardiovascular exercise performance.
Acts as an acid buffer in the body. Carnosine is stored in cells and released in response to drops in pH. Increased stores of carnosine can protect against diet-induced drops in pH (which might occur from ketone production in ketosis, for example), as well as offer protection from exercise-induced lactic acid production.
Typical dosage is 2-5 grams per day, split into smaller doses throughout the day.
Side effects can include flushing, tingling, and numbness but are usually mild. It appears safe overall but long-term studies are limited.
Examine.com
https://examine.com/supplements/beta-alanine/
Can beta-alanine treat cancer?
[Breast Cancer] β-alanine treatment reduces extracellular acidity, a constituent of the invasive microenvironment that promotes progression, we investigated the effect of β-alanine on breast cell viability and migration. β-alanine was shown to reduce both cell migration and proliferation without acting in a cytotoxic fashion. Moreover, β-alanine significantly increased malignant cell sensitivity to doxorubicin, suggesting a potential role as a co-therapeutic agent.
[RCC & Cervical Cancer] Our experimental data suggest that β-alanine may be a potential anti-tumor agent exhibiting several anti-cancer effects in renal and cervical tumor cells.
[Pancreatic Cancer] βA supplementation reprograms cell metabolism by normalizing energy production and reducing microenvironment acidification, thus enhancing chemo-sensitivity in Gem resistant PDAC cells and xenografts. βA can be potentially used as a co-therapeutic in Pancreatic ductal adenocarcinoma (PDAC).
Does beta-alanine make you gain weight?
Beta alanine does nothing to boost muscle gain or burn fat, rather, it buffers against acid build up which then allows the individual to work out harder and longer. The net result of this is of course greater muscle gain and fat loss.
Does beta-alanine give you energy?
Beta-alanine can fuel the athlete in all of us. As the go-to ingredient for sports nutrition formulations, beta-alanine helps build better muscle, faster. It helps us gain focus, energy, and strength. When it comes to enhancing muscle strength, power, growth, and endurance, beta-alanine is the athlete's secret weapon.
β-Alanine intercede metabolic recovery for amelioration of human cervical and renal tumors, 2017 (link)
β-Alanine is a non-essential amino acid and presents as a major component of various sports supplements. It is a non-proteogenic amino acid, formed in vivo by degradation of carnosine, anserine, balenine, and dihydrouracil. The present study was aimed at investigating the anti-tumor effects of β-alanine in renal and cervical tumor cells. Sulforhodamine-B assay and flow cytometric analysis were used to measure cell viability. Lactate dehydrogenase (LDH) expression was analyzed using FITC-conjugated fluorescent antibody. The cellular adenosine triphosphate (ATP) content was measured using bioluminescence method. Cell migration was determined by the simple standard-scratch method. β-Alanine reduced renal and cervical cell growth significantly. Percentage of inhibition of renal and cervical tumor cells was increased at higher concentration of β-alanine. LDH expression and ATP content were significantly reduced in renal and cervical tumor cells in a dose-dependent manner. Renal and cervical tumor cell migration were significantly reduced following 10 and 100 mM of β-alanine treatment. In our study, β-alanine exerts no significant effect on normal MDCK cells except a marginal effect at the highest concentration (100 mM). In summary, our experimental data suggest that β-alanine may be a potential anti-tumor agent exhibiting several anti-cancer effects in renal and cervical tumor cells.
β-alanine suppresses malignant breast epithelial cell aggressiveness through alterations in metabolism and cellular acidity in vitro, 2014
Background: Deregulated energetics is a property of most cancer cells. This phenomenon, known as the Warburg Effect or aerobic glycolysis, is characterized by increased glucose uptake, lactate export and extracellular acidification, even in the presence of oxygen. β-alanine is a non-essential amino acid that has previously been shown to be metabolized into carnosine, which functions as an intracellular buffer. Because of this buffering capacity, we investigated the effects of β-alanine on the metabolic cancerous phenotype.
Methods: Non-malignant MCF-10a and malignant MCF-7 breast epithelial cells were treated with β-alanine at 100 mM for 24 hours. Aerobic glycolysis was quantified by measuring extracellular acidification rate (ECAR) and oxidative metabolism was quantified by measuring oxygen consumption rate (OCR). mRNA of metabolism-related genes was quantified by qRT-PCR with corresponding protein expression quantified by immunoblotting, or by flow cytometry which was verified by confocal microscopy. Mitochondrial content was quantified using a mitochondria-specific dye and measured by flow cytometry.
Results: Cells treated with β-alanine displayed significantly suppressed basal and peak ECAR (aerobic glycolysis), with simultaneous increase in glucose transporter 1 (GLUT1). Additionally, cells treated with β-alanine exhibited significantly reduced basal and peak OCR (oxidative metabolism), which was accompanied by reduction in mitochondrial content with subsequent suppression of genes which promote mitochondrial biosynthesis. Suppression of glycolytic and oxidative metabolism by β-alanine resulted in the reduction of total metabolic rate, although cell viability was not affected. Because β-alanine treatment reduces extracellular acidity, a constituent of the invasive microenvironment that promotes progression, we investigated the effect of β-alanine on breast cell viability and migration. β-alanine was shown to reduce both cell migration and proliferation without acting in a cytotoxic fashion. Moreover, β-alanine significantly increased malignant cell sensitivity to doxorubicin, suggesting a potential role as a co-therapeutic agent.
Conclusion: Taken together, our results suggest that β-alanine may elicit several anti-tumor effects. Our observations support the need for further investigation into the mechanism(s) of action and specificity of β-alanine as a co-therapeutic agent in the treatment of breast tumors.
Metabolic reprogramming with β-alanine to overcome chemotherapy resistance in pancreatic cancer, 2019
Background: Increased aerobic glycolysis (Warburg effect) leading to acidic microenvironment confers chemoresistance to weakly basic Gemcitabine, the standard treatment in Pancreatic ductal adenocarcinoma (PDAC). Metabolomic perturbations in two PDAC cell lines having differential sensitivity to Gemcitabine was investigated by profiling over 40 metabolites using 1H-NMR spectroscopy. Notably, a significant decrease in the concentration of β-alanine (βA) was observed in Gem resistant compared to Gem sensitive cell line, suggesting βA may have a role in chemotherapy response. We aimed to evaluate the role of βA supplementation in improving Gem efficacy in Gem resistant cell lines
Methods: PDAC Panc-1 cell line extracts treated with Gem with and without βA supplementation were analysed via 1H-NMR spectroscopy. Aerobic glycolysis was quantified by measuring extracellular acidification rate (ECAR) and oxygen consumption rate (OCR) using the Seahorse XF analyser platform. Global mRNA profiling was done by Next Generation Sequencing. Proliferation, migration and cell cycle analysis was measured by Xcelligence real time cell analysis system and flow cytometry, respectively. PANC-1 and BxPC-3 tumor xenografts treated with Gemcitabine with and without βA for 4 weeks and the tumor volumes and weights were measured.
Results: βA supplementation in Gem resistant cells results in: (1) decreased basal glycolytic rate, proton leak and ATP production; (2) increased pyruvate, decreased lactic acid and NAD+ concentrations with decreased LDH-A transcription; also increased carnosine levels with a more basic pH in the conditioned media; (3) enhanced sensitivity to Gem treatment, with a significant reduction in proliferation, cell migration, and increased apoptosis and relative hENt-1 mRNA levels and (5) xenograft tumor volumes and weights were significantly reduced upon βA supplementation.
Conclusion: βA supplementation reprograms cell metabolism by normalizing energy production and reducing microenvironment acidification, thus enhancing chemo-sensitivity in Gem resistant PDAC cells and xenografts. βA can be potentially used as a co-therapeutic in PDAC.
Can anyone suggest anything to do about severe itching from polycythemia vera. Thank you.
Changed my life: Nutricost Beta Alanine Powder 300 Grams (10.6oz) - 3 Grams Per Serving
Carnosine and beta-alanine from a supplement that increase physical performance to potent anticancer agent, Jose de Felippe Junior
L-carnosine is a dipeptide formed by the amino acids Beta-alanine and L-histidine. It is believed that L-carnosine (beta-alanyl-L histidine) inhibits the senescence of somatic cells and thus exhibits their anticancer activities. It is a naturally occurring substance with a high potential to inhibit the growth of neoplastic cells, socalled “malignant” cells, in vivo. Carnosine mimics rapamycin, a powerful mTOR inhibitor.
Carnosine has an anti-inflammatory effect, neurotransmitter, aldehyde scavenger, works as organic pH buffer and metal chelator. It has therapeutic potential
in Alzheimer’s disease, stroke, diabetes and vision disorders.
Beta-alanine administration increases carnosine tissue concentration through carnosine synthetase. In this way, carnosine-synthetase-rich neoplastic tissues
generate carnosine from Beta-alanine causing a decrease in proliferation, increased apoptosis and increased cell differentiation. It is important to know that
glioblastoma multiform is very rich in the enzyme carnosine synthetase.
The usual dose of L-carnosine is 400mg twice daily. The usual dose of beta-alanine is 800-1000mg 3 times daily in fasting. The smell of carnosine is unbearable
for many people.
The carnosine formula is C9H14N4O3, molecular weight 226.3 g/mol, known as: L-Carnosine, Carnosine, Beta-Alanyl-L-histidine, Ignotine, Karnozin and Karnozzin. It donates 4 electrons and is acceptor of 5: oxidant molecule.
We prefer to use beta-alanine.
Carnosine or Beta-alanine molecular targets on malignant gliomas
1. Decrease cell proliferation in vitro and in vivo.
2. Increases apoptosis or necrosis.
3. Mimetizes caloric restriction.
4. Mimetizes rapamycin and inhibits mTOR.
5. Decreases anaerobic glycolysis.
6. Drastically decreases the ATP production of the glycolytic pathway of T98G malignant glioma and does not interfere in the mitochondrial pathway.
7. Scavenger of reactive oxygen and aldehyde species.
8. Inhibits carbonic anhydrase – CAIX and acidifies the cytoplasm.
9. Decreases ERK pathway activation and decreases mitotic proliferation.
10. Inhibits ERK1/2.
11. Stops the cell cycle in G1/S.
12. Inhibits p38 MAP Kinase.
13. Inhibits Akt phosphorylation.
14. Inhibits the PI3K/Akt proliferative pathway.
15. Inhibits proliferative pathway ras/MAP Kinase.
16. Inhibits initiation of RNA translation via eIF4E.
17. Decreases HIF-1alpha expression.
18. Inhibits EGFR-2 – erbB-2 tyrosine kinase family involved in cell cycle and differentiation.
19. Inhibits erbB-2.
20. Decrease DHL activity and decrease the generation of glycolytic ATP.
21. Carnosine induces inhibition of the proliferation of glioblastoma U-118-MG cells associated with decreased oxidative stress, increased SOD-Mn and
increased expression of cyclin D1 resulting in blocking the cycle in G2.
22. Carnosine decreases the proliferation of glioblastoma associated with “BCL2-associated athanogene 2” and “von Hippel-Lindau binding protein 1”
which links the action of carnosine to decrease HIF-1alpha signaling.
23. Carnosine inhibits the growth of cells isolated from human glioblastoma multiform. It reduces the activity of dehydrogenases and thus significantly decreases the generation of ATP. It reduces DNA synthesis by 10% to 50% depending on the culture. Inhibits cell proliferation.
24. Carnosine inhibits glycolytic ATP production in malignant glioma, T98G.
25. Decreased circulating carnosine dipeptidase-1 is associated with poor prognosis and cachexia.
26. Aldehyde dehydrogenase increases stem cells proliferation. Carnosine inhibits aldehyde dehydrogenase.
27. Carnosine increases expression of SOD-Mn and cyclin B1 and inhibits proliferation of glioblastoma U-118-MG cells.
28. In normal astrocytes, mitochondrial respiration accounts for 80% of total cellular respiration and 85% of ATP synthesis. Carnosine in normal astrocytes
reduces the cellular ATP concentration by 42%.
29. Carnosine selectively inhibits migration of IDHwild type glioblastoma cells in a co-culture model with fibroblasts (Oppermann-2018).
Carnosine or Beta-alanine. Molecular targets in other neoplasias
1. Carnosine and rapamycin (sirolimus) inhibit glycolytic activity, stimulate proteolysis, and modulate protein synthesis at the translational level, both of
which inhibit the onset of translation via effects on eukaryotic translation initiation factor 4E (eIF4E).
2. Carnosine decreases the proliferation of NIH3T3 fibroblasts expressing HER2/neu (human epidermal growth factor receptor 2) in vivo. Fibroblasts implanted in the mouse.
3. Carnosine reacts strongly with aldehyde groups and keto groups of sugars in the Amadori reaction and thus depletes certain intermediates of glycolysis: one of the anticancer mechanisms.
4. Immune System
a) Suppresses sympathetic activity of the spleen, increases the activity of Natural-Killer cells and decreases the proliferation of colorectal cancer.
b) Non-specific increase in immune system function.
5. Breast cancer
a) Beta-alanine suppresses the aggressiveness of breast cancer epithelial cells through changes in metabolism and cellular acidity in vitro.
b) Beta-alanine suppresses glycolytic and oxidative metabolism and decreases metabolic rate, without altering cell viability, in the MCF-7 line of breast cancer. It reduces extracellular acidity and decreases invasion and metastasis. Increases glucose uptake into cells via increased GLUT-1.
6. Gastric cancer
a) Decrease of circulating carnosine dipeptidase-1 is associated with poor prognosis and cachexia.
b) Carnosine does not induce apoptosis or necrosis in gastric cancer cells, SGC-7901, however, reduces its proliferation through the inhibition of
mitochondrial and glycolytic respiration.
c) Carnosine inhibits the proliferation of gastric carcinoma cells by delaying the Akt/mTOR/ p70S6K signaling pathway. It mimics the rapamycin and thus inhibits mTOR.
7. Hepatoma
a) Inhibits metastasis of hepatocarcinoma by inhibiting the expression of MMP-9 and inducing the anti-metastatic gene nm23-H1 in SK-Hep-1 strain.
b) Anti-carcinogenic effects of L-carnosine on human liver carcinoma cells SNU-423. There is a significant decrease in proliferation in a dose-dependent manner (Ding, 2018).
8. Colorectal cancer
a) Inhibits the proliferation of colorectal cancer: decreases glycolytic ATP, decreases mitochondrial ROS, decreases via ERK1/2 and increases protein p21waf1.
b) Decreases HIF1-alpha and induces apoptosis in HT29 colon cancer cells.
c) Decreases HIF1-alpha and induces apoptosis in HT29 cells of 5-fluoracil resistant colon cancer.
d) Decrease HIF-1 expression in human colon cancer HCT-116 cells.
e) Anti-proliferative effect of L-carnosine correlates with decreased HIF1-alpha expression in colon cancer cells, HCT-116.
f) In the HCT116 line, the activation of the KRAS mutation induces the production of free radicals of oxygen (ERTOS) mitochondrial, which increases neoplastic proliferation. Carnosine inhibits KRAS, decreases the proliferation of HCT116 cells from colon cancer by decreasing ATP and ERTOS, and induces cell cycle arrest in G1. These feats are related to ERK1/2 pathway decrease and p21waf1 protein increase.
g) Carnosine has protective effect against oxidative stress in intestinal epithelial cells.
h) Carnosine activates the CREB pathway and CREB-related pathways by activating Ca++ related pathways in Caco-2 colon cancer cells which regulate genes of the intestinal mucosa.
i) L-carnosine induces apoptosis and cell cycle arrest via suppression of NF-kappaB/STAT1 in HCT116 colorectal cancer cells (Lee, 2018).
9. Cervical cancer
a) Carnosine inhibits cell growth by 23%, ERTOS increase by 30% in HeLa and MDCK cells (Madin-Darby Kidney Cells) and apoptosis occurs in 42 and 14% in normal and neoplastic cells, respectively.
b) Carnosine inhibits carbonic anhydrase IX that causes extracellular acidosis and suppresses growth of the HeLa tumor implanted in the mouse. I believe the following happened: extracellular acidosis caused intracellular acidosis that inhibited glycolysis and provoked tumor growth suppression.
c) Carnosine inhibits the proliferation of cervical carcinoma glandular cells, HeLa and SiHa (squamous cell carcinoma) by inhibiting mitochondrial and glycolytic bioenergetics, which slows the progression of the cell cycle. It reduces the activity of isocitrate dehydrogenase and malate dehydrogenase from the Krebs cycle and reduces the activity of the mitochondrial electron transport chain l, II, III and IV in HeLa cells, but not in SiHa. It induces cell cycle arrest in G1 by inhibiting the G1-S transition in both strains.
d) Carnosine inhibits the proliferation of HeLa human cervical carcinoma cells by inhibiting mitochondrial bioenergetics and glycolysis that delays the progression of the proliferative cell cycle. There is a decrease in mitochondrial and glycolytic ATP generation; reduction of isocitrate dehydrogenase and malate dehydrogenase activity; decrease in mitochondrial electron chain activity I, II, II, and IV and cell cycle arrest in G1 (Bao2018).
10. Ovarian cancer
a) Carnosine is an anticancer drug of real value in the prevention and treatment of intraperitoneal metastases of ovarian cancer.
11. Renal cancer
a) Carnosine activates caspase-3 in human renal carcinoma and inhibits proliferation in 40%.
12. Leukemia and Lymphomas
a) Antigenotoxic and antioxidant in culture of human lymphocytes.
13. Sarcoma
a) In murine sarcoma 180: decreases proliferation, prolongs survival and decreases mortality.
b) Antineoplastic effects of carnosine and beta-alanine on solid sarcoma 180: inhibits tumor growth and increases survival by 132%.
c) Carnosine and gallic acid inhibit MMP-2 and MMP-9 in HT1080 fibrosarcoma cells (Kim2014).
d) Beta-alanine inhibits PTHR1 (parathyroid hormone 1 receptor) and suppresses proliferation, adhesion, invasion, migration and carcinogenesis in human osteosarcoma metastatic U2OS. There is a decrease in mMP-2/9 mRNA expression, reduction of PTHR1 protein and mRNA and increase of tissue inhibitors of MMPs (Li2018).
e) Carnosine and beta-alanine in mice implanted with the solid tumor Sarcoma-180. Occurs tumor growth inhibition, prolongation of survival,
and decreased mortality (Nagai-1986).
f) Beta-2-thienyl-DL-alanine decreases the growth of sarcoma T241 in C57 black mice (Jacquez1953).
14. Renal carcinoma
a) Carnosine inhibited renal cancer cell growth up to 40%, whereas it was 25% in normal cells. Caspase-3 enzyme activity gradually increased in
renal carcinoma cells in a concentration-dependent manner that indicated apoptosis. It is suggested that the carnosine may be a potential antiproliferative agent in renal carcinoma tumor.
15. Metabolism
a) Reacts with AGE’s.
b) Slows aging.
c) Delays lactate accumulation during exercise by turning lactate into pyruvate.
d) Carnosine and Beta-alanine stimulate granulation and accelerate the healing of wounds, besides increasing immunocompetence, which accelerates the healing of the traumatized region.
Carnosine: A Longevity Factor, 2012
Carnosine is concentrated in the brain, heart, and muscles. Studies have shown that carnosine slows the aging of human cells and protects against age-inducing processes such as glycation and mitochondrial dysfunction. Carnosine levels in the body plummet as humans age, making supplementation a key component of an age-delaying program.
12. Snell TW, Fields AM, Johnston RK. Antioxidants can extend lifespan of Brachionus manjavacas (Rotifera), but only in a few combinations. Biogerontology. 2012 Jan 24.
Carnosine extends the life span of rotifers, a microscopic aquatic organism now being used as a model of aging in many laboratories.12 In this experiment, scientists tested many different antioxidant compounds, identifying carnosine as one of just four that had significant effects on the organisms’ longevity.
13. Yuneva AO, Kramarenko GG, Vetreshchak TV, Gallant S, Boldyrev AA. Effect of carnosine on Drosophila melanogaster life span. Bull Exp Biol Med. 2002 Jun;133(6):559-61.
14. Stvolinsky S, Antipin M, Meguro K, Sato T, Abe H, Boldyrev A. Effect of carnosine and its Trolox-modified derivatives on life span of Drosophila melanogaster. Rejuvenation Res. 2010 Aug;13(4):453-7.
Carnosine extends the life span of fruit flies, another organism commonly used to study aging, up to 20% in males.13,14 Normally, male fruit flies die much sooner than do females, but when fed a steady diet including a carnosine supplement, the males attained the same age as the females.
15. Boldyrev AA, Gallant SC, Sukhich GT. Carnosine, the protective, anti-aging peptide. Biosci Rep. 1999 Dec;19(6):581-7.
16. Gallant S, Semyonova M, Yuneva M. Carnosine as a potential anti-senescence drug. Biochemistry (Mosc). 2000 Jul;65(7):866-8.
Carnosine extends the life span of laboratory mice, complex, warm-blooded mammals with many of the aging features common to humans.15,16
Effect of Carnosine on Age-Induced Changes in Senescence-Accelerated Mice, 1999
The effect of carnosine on the life span and several brain biochemical characteristics in senescence-accelerated mice—prone 1 (SAMP1) was investigated. A 50% survival rate of animals treated with carnosine increased by 20% as compared to controls. Moreover, the number of animals that lived to an old age significantly increased. The effect of carnosine on life span was accompanied by a decrease in the level of ′-tiobarbituric acid reactive substances (TBARS), monoamine oxidase b (MAO b), and Na/K-ATPase activity. There was also an increase in glutamate binding to N-methyl-D-aspartate receptors. These observations are consistent with the conclusion that carnosine increases life span and quality of life by diminishing production of lipid peroxides and reducing the influence of reactive oxygen species (ROS) on membrane proteins.
Long-term supplementation with EGCG and beta-alanine decreases mortality but does not affect cognitive or muscle function in aged mice, 2017
We have previously shown that 6weeks of a diet containing epigallocatechin gallate (EGCG) and beta-alanine (B-ALA) was not effective in improving either cognitive or muscle function in aged (18month) mice (Gibbons et al. Behav Brain Res 2014). However, diet reduced oxidative stress in the brain, and previous studies using longer-term interventions have documented beneficial effects in cognitive, but not muscle, function. Therefore, we investigated the effect of 6months of feeding on measures of cognitive and muscle function in mice. Mice (12months, N=15/group) were fed AIN-93M containing 0.15% EGCG and 0.34% B-ALA or standard AIN-93M for 6months, then underwent a battery of tests for cognitive and muscle function at 18months. Interestingly, a higher percentage of mice receiving EGCG and B-ALA (E+B, 80%) survived to study end compared to control (Ctrl, 40%) mice (p=0.02). E+B did not affect arm preference in the Y-maze test (p=0.74, novel arm) and did not alter performance in an active avoidance test (p=0.16, avoidances per 50 trials). E+B increased rotarod performance (p=0.03), did not affect grip strength (p=0.91), and decreased time to exhaustion in a treadmill fatigue test (p=0.02) compared to Ctrl. In conclusion, E+B reduced mortality, had no effect on cognitive function and variable effects on muscle function.
On the enigma of carnosine's anti-ageing actions, 2009
Carnosine (beta-alanyl-L-histidine) has described as a forgotten and enigmatic dipeptide. Carnosine's enigma is particularly exemplified by its apparent anti-ageing actions; it suppresses cultured human fibroblast senescence and delays ageing in senescence-accelerated mice and Drosophila, but the mechanisms responsible remain uncertain. In addition to carnosine's well-documented anti-oxidant, anti-glycating, aldehyde-scavenging and toxic metal-ion chelating properties, its ability to influence the metabolism of altered polypeptides, whose accumulation characterises the senescent phenotype, should also be considered. When added to cultured cells, carnosine was found in a recent study to suppress phosphorylation of the translational initiation factor eIF4E resulting in decreased translation frequency of certain mRNA species. Mutations in the gene coding for eIF4E in nematodes extend organism lifespan, hence carnosine's anti-ageing effects may be a consequence of decreased error-protein synthesis which in turn lowers formation of protein carbonyls and increases protease availability for degradation of polypeptides altered postsynthetically. Other studies have revealed carnosine-induced upregulation of stress protein expression and nitric oxide synthesis, both of which may stimulate proteasomal elimination of altered proteins. Some anti-convulsants can enhance nematode longevity and suppress the effects of a protein repair defect in mice, and as carnosine exerts anti-convulsant effects in rodents, it is speculated that the dipeptide may participate in the repair of protein isoaspartyl groups. These new observations only add to the enigma of carnosine's real in vivo functions. More experimentation is clearly required.
I suffer from Itchy skin, Aquagenic Pruritus and change in temperature itch. Beta Alanine has been a game changer. I take 1,500 mg 30 mins before showering and have little – to no itch. I also take 750 mg when I get up in the morning and anytime during the day when I feel an itch coming on…and it stops the itch.
β-Alanine intercede metabolic recovery for amelioration of human cervical and renal tumors, 2017
Abstract and Figures
β-Alanine is a non-essential amino acid and presents as a major component of various sports supplements. It is a non-proteogenic amino acid, formed in vivo by degradation of carnosine, anserine, balenine, and dihydrouracil. The present study was aimed at investigating the anti-tumor effects of β-alanine in renal and cervical tumor cells. Sulforhodamine-B assay and flow cytometric analysis were used to measure cell viability. Lactate dehydrogenase (LDH) expression was analyzed using FITC-conjugated fluorescent antibody. The cellular adenosine triphosphate (ATP) content was measured using bioluminescence method. Cell migration was determined by the simple standard-scratch method. β-Alanine reduced renal and cervical cell growth significantly. Percentage of inhibition of renal and cervical tumor cells was increased at higher concentration of β-alanine. LDH expression and ATP content were significantly reduced in renal and cervical tumor cells in a dose-dependent manner. Renal and cervical tumor cell migration were significantly reduced following 10 and 100 mM of β-alanine treatment. In our study, β-alanine exerts no significant effect on normal MDCK cells except a marginal effect at the highest concentration (100 mM). In summary, our experimental data suggest that β-alanine may be a potential anti-tumor agent exhibiting several anti-cancer effects in renal and cervical tumor cells.
Integrated transcriptomic and metabolomic analysis shows that disturbances in metabolism of tumor cells contribute to poor survival of RCC patients
Purpose: Cellular metabolism of renal cell carcinoma (RCC) tumors is disturbed. The clinical significance of these alterations is weakly understood. We aimed to find if changes in metabolic pathways contribute to survival of RCC patients.
Material and methods: 35 RCC tumors and matched controls were used for metabolite profiling using gas chromatography-mass spectrometry and transcriptomic analysis with qPCR-arrays targeting the expression of 93 metabolic genes. The clinical significance of obtained data was validated on independent cohort of 468 RCC patients with median follow-up of 43.22months.
Results: The levels of 31 metabolites were statistically significantly changed in RCC tumors compared with controls. The top altered metabolites included beta-alanine (+4.2-fold), glucose (+3.4-fold), succinate (-11.0-fold), myo-inositol (-4.6-fold), adenine (-4.2-fold), uracil (-3.7-fold), and hypoxanthine (-3.0-fold). These disturbances were associated with altered expression of 53 metabolic genes. ROC curve analysis revealed that the top metabolites discriminating between tumor and control samples included succinate (AUC=0.91), adenine (AUC=0.89), myo-inositol (AUC=0.87), hypoxanthine (AUC=0.85), urea (AUC=0.85), and beta-alanine (AUC=0.85). Poor survival of RCC patients correlated (p<0.0001) with altered expression of genes involved in metabolism of succinate (HR=2.7), purines (HR=2.4), glucose (HR=2.4), beta-alanine (HR=2.5), and myo-inositol (HR=1.9).
Conclusions: We found that changes in metabolism of succinate, beta-alanine, purines, glucose and myo-inositol correlate with poor survival of RCC patients.
Effect of Carnosine or β-Alanine Supplementation on Markers of Glycemic Control and Insulin Resistance in Humans and Animals: A Systematic Review and Meta-analysis, 2021
There is growing evidence that supplementation with carnosine, or its rate-limiting precursor β-alanine, can ameliorate aspects of metabolic dysregulation that occur in diabetes and its related conditions. The purpose of this systematic review and meta-analysis was to evaluate the effect of carnosine or β-alanine supplementation on markers of glycemic control and insulin resistance in humans and animals.
Twenty studies (n = 4 human, n = 16 rodent) were included, providing data for 2 primary outcomes (fasting glucose and HbA1c) and 3 additional outcomes (fasting insulin, HOMA-β, and HOMA-IR).
The model provides evidence that supplementation decreases
fasting glucose [humans: mean difference (MD)0.5 = –0.95 mmol/L (90% CrI: –2.1, 0.08);
HbA1c [humans: MD0.5 = –0.91% (90% CrI: –1.46, –0.39);
HOMA-IR [humans: standardized mean difference (SMD)0.5 = –0.41 (90% CrI: –0.82, –0.07)
fasting insulin [humans: SMD0.5 = –0.41 (90% CrI: –0.77, –0.07)].
Genotoxic aldehyde stress prematurely ages hematopoietic stem cells in a p53-driven manner (link, link)
New research identifies formaldehyde, a molecule produced by the body's own metabolism, as a source of DNA damage that can accelerate aging and increase cancer risk in blood stem cells. The research found that formaldehyde causes DNA damage that triggers increased levels of the p53 protein, which speeds up aging in mice blood stem cells. This provides evidence that DNA damage drives aging in blood stem cells in a programmed way through p53 activation, rather than just through gradual accumulation of damage. The researchers suggest that if we can find ways to lower formaldehyde levels in cells, we may be able to slow this accelerated aging process and reduce cancer risk. The findings may be relevant not just for blood cancers but possibly other cancer types as well.
TET2 / GDF11
Mutual regulation between GDF11 and TET2 prevents senescence of mesenchymal stem cells
Growth differentiation factor 11 (GDF11) is a putative systemic rejuvenation factor. In this study, we characterized the mechanism by which GDF11 reversed aging of mesenchymal stem cells (MSCs). In culture, aged MSCs proliferate slower, and are positive for senescence markers SA-β-gal and P16ink4a. They have shortened telomeres, decreased GDF11 expression, and reduced osteogenic potential. GDF11 can block MSC aging in vitro, and reverse age-dependent bone loss in vivo. The anti-aging effect of GDF11 is via activation of the Smad2/3-PI3K-AKT-mTOR pathway. Unexpectedly, GDF11 also upregulated a DNA demethylase Tet2, which served as a key mediator for GDF11 to autoregulate itself via demethylation of specific CpG sites within the GDF11 promoter. Mutation of Tet2 facilitates MSC aging by blocking GDF11 expression. Mutagenesis of Tet2-regulated CpG sites also blocks GDF11 expression, leading to MSC aging. Together, a novel mutual regulatory relationship between GDF11 and an epigenetic factor Tet2 unveiled their anti-aging roles.
One Sentence Summary An epigenetic mechanism by which GDF11 rejuvenates mesenchymal stem cells
GDF11 has been found to reverse the methylation age in stem cells. I wonder if this age reduction would show up in a regular methylation age test? Not sure if they check stem cell methylation age in tests.
GDF11 belongs to the transforming growth factor beta superfamily that controls anterior-posterior patterning by regulating the expression of Hox genes.[36] GDF11 activates the TGF-β pathway in cardiomyocytes derived from pluripotent hematopoietic stem cells and suppresses the phosphorylation of Forkhead (FOX proteins) transcription factors.
Pre-clinical rationale for TGF-β inhibition as a therapeutic target for the treatment of myelofibrosis (link)
Transforming growth factor-β promotes aggressiveness and invasion of clear cell renal cell carcinoma (link)
GDF11 Implications in Cancer Biology and Metabolism. Facts and Controversies (link)
GDF11 contributes to hepatic hepcidin (HAMP) inhibition through SMURF1-mediated BMP-SMAD signalling suppression, 2020
Boswellia
Studies have also found that boswellia may fight advanced breast cancer cells, and it may limit the spread of malignant leukemia and brain tumor cells. Another study showed boswellic acids to be effective in suppressing the invasion of pancreatic cancer cells. Studies continue and the anti-cancer activity of boswellia is becoming better understood.
Boswellia serrata
Novel inhibitory of a pro-inflammatory enzyme called 5-Lipoxygenase (5-LOX) and may possess other anti-inflammatory effects (such as nF-kB inhibition, which are not as novel). These anti-inflammatory effects have been investigated for their benefits in osteoarthritis (OA), and it appears that oral Boswellia supplements can suppress pain and immobility associated with OA quite significantly with the effects taking as little as a week to occur. The studies are well conducted, but funded by the producers of the tested supplements. There are limited non-funded interventions with Boswellic for this claim, but they seem to agree with the battery of funded study in effect size.
Remarkably, Boswellia appears to be quite anti-cancer that appears to be more anti-proliferative rather than apoptotic (the latter meaning to induce regulated cell death) since it is a potent inhibitor of angiogenesis and cell invasiveness. There are not a large battery of studies on these claims, but preliminary mouse and rat evidence where the rodents are injected with tumors suggest that Boswellia can potently suppress tumor growth (Pancreatic, Colorectal) and in some cases actually outright prevent tumor growth (Prostatic, Glioma). Boswellia appears to be a very promising anti-cancer herb due to the potency it exhibits in animals, with one study noting this after oral administration (100mg/kg of the main boswellic acid in animals). The potency has been replicated in other cancer cell lines in vitro (including breast, cervical, myeloma and leukemia) but these cancers do not yet have animal interventions yet.
Inhibitory activity of boswellic acids from Boswellia serrata against human leukemia HL-60 cells in culture
Four major triterpene acids including beta-boswellic acid (1), 3-O-acetyl-beta-boswellic acid (2), 11-keto-beta-boswellic acid (3), and 3-O-acetyl-11-keto-beta-boswellic acid (4) were isolated from the gum resin of Boswellia serrata and examined for their in vitro antitumor activity. They inhibited the synthesis of DNA, RNA and protein in human leukemia HL-60 cells in a dose dependent manner with IC50 values ranging from 0.6 to 7.1 microM. Among them, compound 4 induced the most pronounced inhibitory effects on DNA, RNA and protein synthesis with IC50 values of 0.6, 0.5, and 4.1 microM, respectively. The effect of 4 on DNA synthesis was found to be irreversible. Compound 4 significantly inhibited the cellular growth of HL-60 cells, but did not affect cell viability.
Frankincense oil derived from Boswellia carteri induces tumor cell specific cytotoxicity
Background
Originating from Africa, India, and the Middle East, frankincense oil has been important both socially and economically as an ingredient in incense and perfumes for thousands of years. Frankincense oil is prepared from aromatic hardened gum resins obtained by tapping Boswellia trees. One of the main components of frankincense oil is boswellic acid, a component known to have anti-neoplastic properties. The goal of this study was to evaluate frankincense oil for its anti-tumor activity and signaling pathways in bladder cancer cells.
Methods
Frankincense oil-induced cell viability was investigated in human bladder cancer J82 cells and immortalized normal bladder urothelial UROtsa cells. Temporal regulation of frankincense oil-activated gene expression in bladder cancer cells was identified by microarray and bioinformatics analysis.
Results
Within a range of concentration, frankincense oil suppressed cell viability in bladder transitional carcinoma J82 cells but not in UROtsa cells. Comprehensive gene expression analysis confirmed that frankincense oil activates genes that are responsible for cell cycle arrest, cell growth suppression, and apoptosis in J82 cells. However, frankincense oil-induced cell death in J82 cells did not result in DNA fragmentation, a hallmark of apoptosis.
Conclusion
Frankincense oil appears to distinguish cancerous from normal bladder cells and suppress cancer cell viability. Microarray and bioinformatics analysis proposed multiple pathways that can be activated by frankincense oil to induce bladder cancer cell death. Frankincense oil might represent an alternative intravesical agent for bladder cancer treatment.
H1-Antihistamines / Loratadine (Claritin) / Desloratadine
Histamine and histamine receptor H1 (HRH1) knockout or antihistamine treatment reverted macrophage immunosuppression, revitalized T cell cytotoxic function, and restored immunotherapy response (2021, 2021, 2023).
Allergy, via the histamine-HRH1 axis, facilitated tumor growth and induced immunotherapy resistance in mice and humans. Importantly, cancer patients with low plasma histamine levels had a more than tripled objective response rate to anti-PD-1 (immunotherapy) treatment compared with patients with high plasma histamine (2021).
H1 antihistamines were found to induce anti-cancer effects across multiple cell lines (CLL, HCC, BC, NSCLC, MM, OC, PC…). Induce cancer-specific, lysosome-dependent cell death and sensitize cancer cells to chemotherapy (2021)
Desloratadine use was associated with an improved survival for all immunogenic tumors including kidney cancer. Loratadine use didn’t show an equally strong association. (2020)
Whole blood histamine content was Increased in 60% of patients with uncontrolled polycythemia vera. The urine histamine findings paralleled the blood findings in 90 per cent of the cases. Myelosuppressive agents produced a reduction in histamine. Treatment with phlebotomy alone produced no change in histamine levels. The incidence of pruritus increased 7-fold in patients with elevated histamine. (1966)
Loratadine exhibits anti-inflammatory activity through suppression of the NF-kB pathway. (2020)
Loratadine administration to C Elegans extended lifespan by 18% (2014).
[NEGATIVE] Prescription H1 antihistamine users had a significantly higher weight, waist circumference, and insulin concentration than matched controls (2010). Prolonged intake of desloratadine induced development of an obesity-like phenotype and signs of metabolic syndrome in rats.
[Care oncology: Start taking claritin (antihistamine). 1 tablet daily. it helps so that cancer doesn't become resistant to treatment. you can start now]
ANTI-CANCER EFFECTS:
Cationic amphiphilic antihistamines significantly improved overall survival (24.8 vs. 10.4 months) and progression-free survival (10.6 vs. 4.93 months) in patients receiving immune checkpoint inhibitors, with a 50% lower risk of all-cause mortality (2022)
Desloratadine use was associated with improved survival for all immunogenic tumors (but not non-immunogenic ones) and loratadine use was associated with improved survival for some tumors, while the other antihistamines did not show a consistent, statistically significant association with improved survival (2020).
Daily antihistamine use for over a year may be associated with a decreased cancer risk: a 1.93% cancer risk in the first group compared to 4.76% in the as-needed medication group (P=0.008). (2009)
OTC antihistamines (clemastine, desloratadine, and loratadine) preferentially induced cell death in chronic lymphocytic leukemia (CLL) cells through lysosomal membrane permeabilization and showed a synergistic effect with the tyrosine kinase inhibitor ibrutinib, but not with chemotherapy, with clemastine having the greatest cytotoxicity and tumor sensitivity (2020)
OTC, second-generation antihistamine drugs may improve outcomes for cancer patients treated with anti-PD-1/PD-L1 checkpoint inhibitors, with H1-antihistamines significantly associated with improved overall survival in some tumor types (2021)
Concurrent use of antihistamines targeting HRH1 was correlated with significantly improved survival outcomes for immunotherapy-treated patients with melanoma or lung cancer, while breast and colon cancer patients showed similar trends but lacked statistical significance due to small sample sizes.
Antihistamine treatment combined with checkpoint blockade enhanced therapeutic efficacy and prolonged survival in preclinical breast cancer and melanoma models.
Histamine and its receptors (HRs) are implicated in cancer development, growth, and metastasis, with HR ligands offering potential therapeutic value and prognostic biomarkers in various cancers (2021)
Loratadine, an antihistamine drug, demonstrates anti-inflammatory activity by inhibiting the NF-kB pathway and binding with Syk and Src proteins, leading to improved stomach tissue histopathology, liver morphology, and colon length in mouse models of gastritis, hepatitis, colitis, and peritonitis (2020)
The malignant process in MPNs involves mast cells with increased activation markers, despite fewer mast cells generated from patient CD34+ cells, and JAK2V617F-positive MC colonies were found in all 17 JAK2V617F-positive MPN patients studied. Erlotinib, a JAK2 inhibitor, can inhibit JAK2V617F-positive PV MC progenitor cells, suggesting their potential as cellular targets for JAK2 inhibitor-directed therapy. (2009)
Elevated histamine levels were found in 60% of uncontrolled polycythemia vera patients, 7% of controlled polycythemia vera patients, and 71% of patients with "spent" polycythemia, myeloid metaplasia, and myelofibrosis; with higher histamine levels correlating to increased incidence of pruritus, gastrointestinal distress, and urticarial manifestations (1966)
Desloratadine exhibited potential anticancer activity on bladder cancer cell growth and invasion by inhibiting cell viability, colony-formation ability, cell migration, and invasion, as well as modulating apoptosis and autophagy-related proteins, and affecting epithelial-to-mesenchymal transition and interleukin 6 (2020).
Histamine H1 receptor antagonists, including cloperastine, selectively killed cisplatin-resistant human cervical cancer cells, potentially offering a combination therapy for cancers with emergent drug-resistance, through a mechanism involving autocrine histamine activity and high-level expression of FGF13 (2021).
Antihistamines in cancer therapy study: Histamine displayed a bivalent role in tumor growth regulation, and antihistamines showed promise for cancer therapy by targeting histamine receptors present in various cells, including tumor cells, but further research is needed to understand their role in cancer development and clinical management (2017)
METABOLIC EFFECTS:
Loratadine extended worm lifespan by 18% (2014).
Prescription H1 antihistamine use is associated with a higher weight, waist circumference, and insulin concentration, increasing the odds ratio for being overweight and possibly contributing to the prevalence of obesity and metabolic syndrome (2010)
Prolonged intake of desloratadine, an antihistamine, can lead to an obesity-like phenotype, signs of metabolic syndrome, and mesenteric lymphatic vessel dysfunction in rats, suggesting that millions of people may be at risk for obesity and metabolic syndrome due to long-term antihistamine use (2018)
Improved survival in several cancers with use of H1-antihistamines desloratadine and loratadine (2020)
Methods: We investigated survival and use of six common H1-antihistamines (cetirizine, clemastine, desloratadine, ebastine, fexofenadine and loratadine) in a nation-wide cohort of all 429,198 Swedish patients with ten types of immunogenic (gastric, colorectal/anal, pancreatic, lung, breast, prostate, kidney, and bladder cancer, melanoma and Hodgkin lymphoma) and six non-immunogenic (liver, uterine, ovarian, brain/CNS, and thyroid cancer and non-Hodgkin lymphoma) tumors diagnosed 2006–2017. Follow-up was until 2019–02–24.
Findings: Desloratadine use was associated with an improved survival for all immunogenic tumors, but not for the non-immunogenic ones. Loratadine use was associated with improved survival for some tumors. Use of the other antihistamines could not be shown to be consistently associated with improved survival to a statistically significant degree.
Fig. 1 Desloratadine use and tumor-specific mortality.
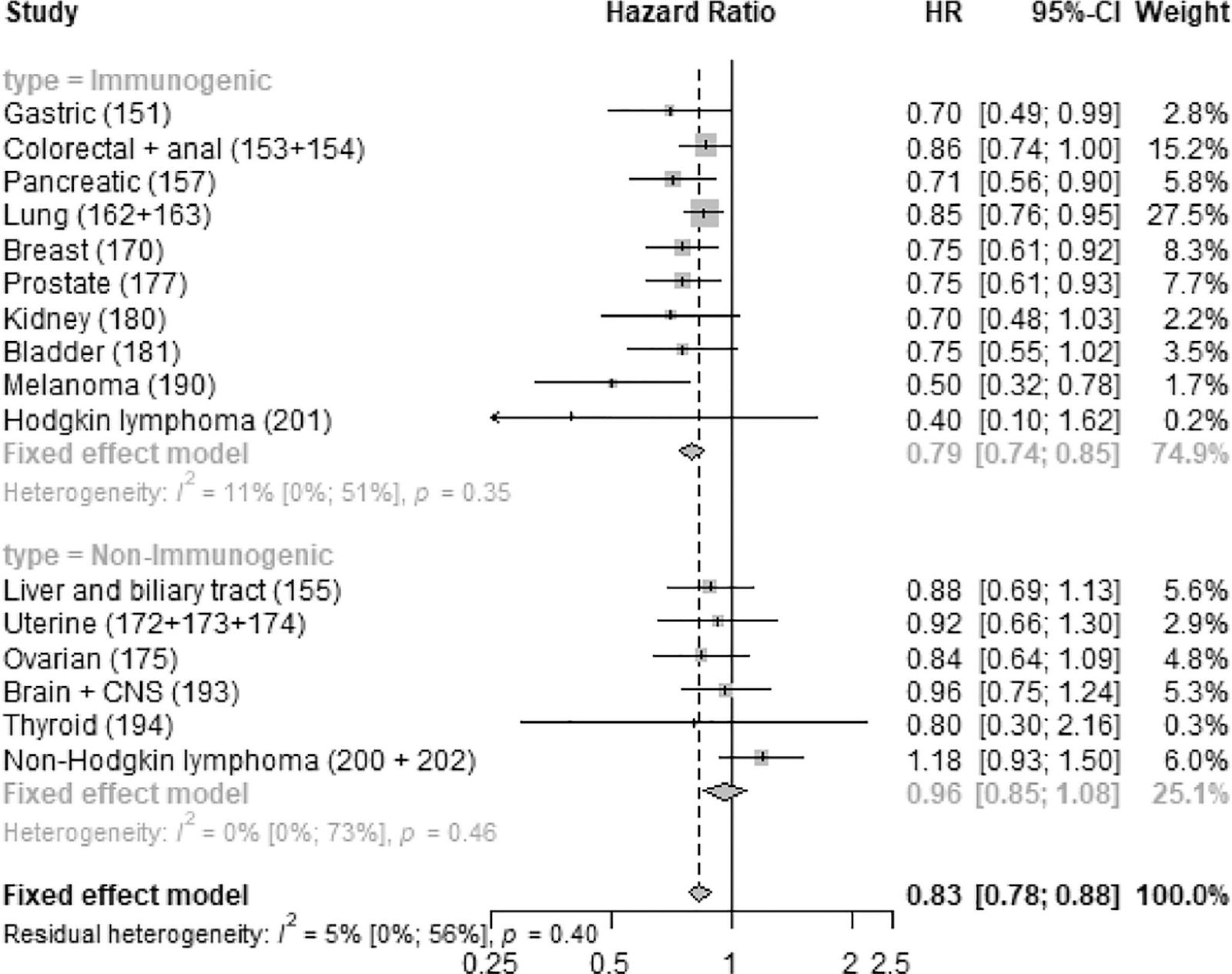
Fig. 5 Tumor-specific mortality of desloratadine users vs non-users with kidney cancer. Kidney cancer-specific survival probability plotted against time since diagnosis in years.
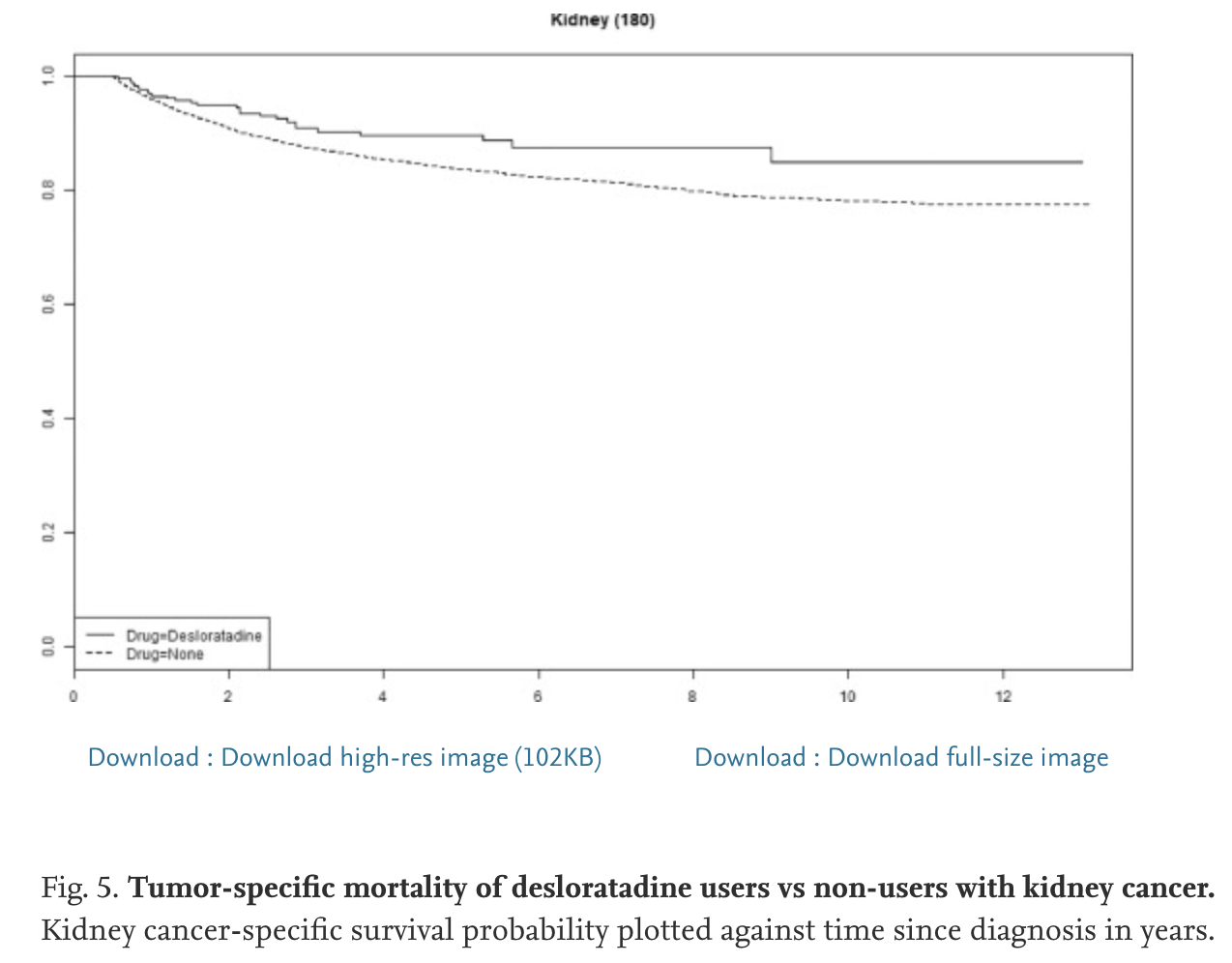
Antihistamines are synergistic with Bruton’s tyrosine kinase inhibiter
ibrutinib mediated by lysosome disruption in chronic lymphocytic leukemia
(CLL) cells (2020)
Introduction
Chronic lymphocytic leukemia (CLL) is the most common leukemia in the western world. Novel targeted therapies like ibrutinib have improved outcomes but resistance can develop.
Lysosomes are a potential therapeutic target in CLL. Recent studies show antihistamines can induce lysosomal membrane permeabilization (LMP) in cancer cells.
Results
The antihistamines clemastine, desloratadine and loratadine preferentially induced cytotoxicity and LMP in CLL cells compared to normal lymphocytes.
Clemastine was the most potent, with an EC50 of 12.3 μM in CLL cells vs 32 μM in normal PBMCs. It rapidly induced LMP, similar to the lysosomotropic agent siramesine.
LMP induction by clemastine was reduced by antioxidants but not cathepsin inhibitors, suggesting a ROS-mediated process.
Clemastine synergistically enhanced cytotoxicity of the BTK inhibitor ibrutinib in CLL cells and cell lines, but not chemotherapies. The combination induced ROS accumulation, loss of mitochondrial membrane potential, and apoptosis.
The combination decreased expression of the anti-apoptotic protein Mcl-1 in CLL cells. It also reduced phosphorylation of survival kinases like Akt and ERK more than ibrutinib alone.
Conclusions
Antihistamines like clemastine are promising lysosomotropic agents against CLL due to their ability to preferentially disrupt lysosomes and induce oxidative cell death.
They synergize with ibrutinib by enhancing ROS, targeting mitochondria, and downregulating Mcl-1. This represents a potential new treatment approach for CLL.
Further studies are needed to verify if this synergy can be achieved at clinically relevant doses and improve outcomes long-term. Overall, repurposing antihistamines represents a novel therapeutic strategy for CLL worth pursuing.
Antihistamines synergistically induce CLL cell death with TK inhibitors (2020)
Three over-the-counter antihistamines, clemastine, desloratadine, and loratadine, preferentially induce cell death through lysosomal membrane permeabilization in chronic lymphocytic leukemia cells, compared with normal lymphocytes, according to the results of an in vitro study published in Leukemia Research.
In addition, the antihistamines showed a synergistic effect in killing off chronic lymphocytic leukemia (CLL) cells when combined with the tyrosine kinase inhibitor, ibrutinib, but not with chemotherapy, according to Aaron Chanas-Larue of CancerCare Manitoba, Winnipeg, Man., and colleagues.
Blood from CLL patients and age-matched healthy donors was collected, treated, and compared with two malignant B-cell lines. Cells were treated with the three different antihistamines at various concentrations alone and in the presence of ibrutinib. Cell death was determined by flow cytometry using fluorescent staining and EC50 (half-maximal effective concentration) values were calculated.
Of the three drugs, clemastine demonstrated the greatest degree of cytotoxicity, with a mean EC50 value of 12.3 mcmol in CLL cells. Desloratadine and loratadine also had a greater effect on leukemic cells, with mean EC50 values of 27.2 mcmol and 17.2 mcmol, respectively, according to the researchers.
Clemastine also showed the greatest tumor sensitivity, with an EC50 nearly three times lower for CLL cells (EC50, 12.3 mcmol) than for normal peripheral blood mononuclear cells (EC50, 32 mcmol). In addition, clemastine induced cell death over a 72-hour time course in CLL cells, and was equally effective against CLL cells with del17p, unmutated immunoglobulin heavy chain gene, or high Zeta-chain–associated protein kinase 70 expression.
Effective synergy
The researchers found that clemastine enhanced cell death when combined with targeted CLL therapies ibrutinib, idelalisib, or venetoclax, but did not enhance the activities of the chemotherapeutics fludarabine, chlorambucil, or bendamustine.
Ibrutinib increased cell death to the greatest degree when combined with antihistamines. The effect was demonstrated to be synergistic, showing “a unique interaction between the activities of the antihistamines and this inhibitor of the B-cell pathway, suggesting a clinical potential for this combination,” the authors stated.
“Repurposing well-characterized drugs such as antihistamines with defined mechanisms and toxicities allows for repositioning of these drugs to use in CLL treatment in the near future in the context of targeted therapies,” they concluded.
Antihistamine drugs might improve health of cancer patients receiving immunotherapy, 2021 (very good!)
Second-Generation Antihistamine Drugs May Improve Outcomes for Cancer Patients Receiving Immunotherapy, 2021 (detailed! nice)
The allergy mediator histamine confers resistance to immunotherapy in cancer patients via activation of the macrophage histamine receptor H1, 2021
Histamine binding of HRH1 on macrophages induces an immunosuppressive phenotype
H1-antihistamine treatment enhances immunotherapy response
Allergic reaction promotes immune evasion and resistance to immunotherapy
High histamine and HRH1 levels correlate with poor immunotherapy response in patients
Reinvigoration of antitumor immunity remains an unmet challenge. Our retrospective analyses revealed that cancer patients who took antihistamines during immunotherapy treatment had significantly improved survival. We uncovered that histamine and histamine receptor H1 (HRH1) are frequently increased in the tumor microenvironment and induce T cell dysfunction. Mechanistically, HRH1-activated macrophages polarize toward an M2-like immunosuppressive phenotype with increased expression of the immune checkpoint VISTA, rendering T cells dysfunctional. HRH1 knockout or antihistamine treatment reverted macrophage immunosuppression, revitalized T cell cytotoxic function, and restored immunotherapy response. Allergy, via the histamine-HRH1 axis, facilitated tumor growth and induced immunotherapy resistance in mice and humans. Importantly, cancer patients with low plasma histamine levels had a more than tripled objective response rate to anti-PD-1 treatment compared with patients with high plasma histamine. Altogether, pre-existing allergy or high histamine levels in cancer patients can dampen immunotherapy responses and warrant prospectively exploring antihistamines as adjuvant agents for combinatorial immunotherapy.
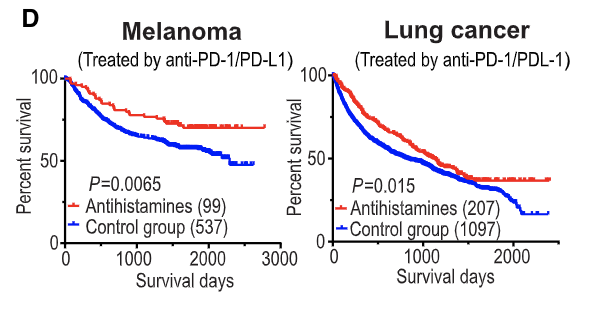
Table S1. List of drugs taken by ICB-treated melanoma patients, related to Figure 1
Efficacy of cationic amphiphilic antihistamines on outcomes of patients treated with immune checkpoint inhibitors, 2022
Background
Cationic amphiphilic antihistamines have been shown to improve patient outcomes in immunogenic tumours, but whether they can augment and improve response to immunotherapy is unknown. We aim to evaluate the effect of cationic amphiphilic antihistamines in patients receiving immune checkpoint inhibitors (ICIs).
Methods
We conducted a retrospective propensity score-matched cohort study at two tertiary referral centres in Taiwan between January 2015 and December 2021. Patients who received desloratadine, cyproheptadine, and ebastine were classified as cationic amphiphilic antihistamine users. The primary outcome was overall survival, and the secondary outcomes were progression-free survival and clinical benefit rate. Patients treated with cationic amphiphilic antihistamines were matched to patients who received non-cationic amphiphilic antihistamines based on variables including age, cancer type, stage, and history of allergic diseases.
Results
A total of 734 ICI-treated patients were included. After matching, 68 cationic amphiphilic antihistamine and non-cationic amphiphilic antihistamine users remained for analysis. Compared with non-cationic amphiphilic antihistamine users, patients who received cationic amphiphilic antihistamines had a significantly longer median overall survival (24.8 versus 10.4 months; Log-rank, p = 0.018) and progression-free survival (10.6 versus 4.93 months; Log-rank, p = 0.004). The use of cationic amphiphilic antihistamines was associated with an approximately 50% lower risk of all-cause mortality (HR, 0.55 [95% CI: 0.34–0.91]). Survival benefits were not seen in patients who received cationic amphiphilic antihistamines before immune checkpoint blockade. These survival benefits were observed regardless of the generation of cationic amphiphilic antihistamines.
Conclusion
The use of cationic amphiphilic antihistamines was associated with improved survival among patients treated with immunotherapy.
The emergence of antihistamines as unexpected allies in our fight against acute myeloid leukaemia, 2019
The article discusses how antihistamines, a class of drugs commonly used to treat allergic reactions, were unexpectedly found to have cytotoxic effects against acute myeloid leukemia (AML) cells. An in silico screening identified a subset of antihistamines that induced apoptosis and autophagy in AML cell lines and primary samples by simultaneously disrupting lysosomes and mitochondria. This effect was independent of AML genetic landscape and did not rely on disrupting receptor signaling. The authors suggest repurposing these FDA-approved antihistamines as chemosensitizing agents that could target AML cells diffusely, including in sanctuary sites like the CNS. While targeted AML therapies have risks of late adverse events, antihistamines are well-studied supportive care drugs unlikely to have serious side effects. More study is needed to determine if antihistamines can improve outcomes for AML as part of combination therapy regimens.
Dual lysosomal-mitochondrial targeting by antihistamines to eradicate leukaemic cells, 2019
An in silico screening was performed using Connectivity Maps to identify FDA-approved drugs that may revert an early leukaemic transformation gene signature. Hit compounds were validated in AML cell lines. Cytotoxic effects were assessed both in primary AML patient samples and healthy donor blood cells. Xenotransplantation assays were undertaken to determine the effect on engraftment of hit compounds. The mechanism of action responsible for the antileukaemic effect was studied focussing on lysosomes and mitochondria.
Findings
We identified a group of antihistamines (termed ANHAs) with distinct physicochemical properties associated with their cationic-amphiphilic nature, that selectively killed leukaemic cells. ANHAs behaved as antileukaemic agents against primary AML samples ex vivo, sparing healthy cells. Moreover, ANHAs severely impaired the in vivo leukaemia regeneration capacity. ANHAs' cytotoxicity relied on simultaneous mitochondrial and lysosomal disruption and induction of autophagy and apoptosis. The pharmacological effect was exerted based on their physicochemical properties that permitted the passive targeting of both organelles, without the involvement of active molecular recognition.
Interpretation
Dual targeting of lysosomes and mitochondria constitutes a new promising therapeutic approach for leukaemia treatment, supporting the further clinical development.
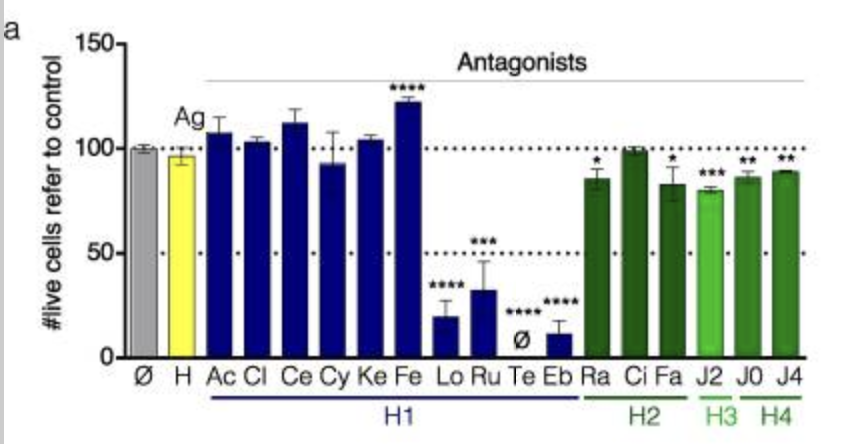
Histamine antagonists promote cancer immunosurveillance, 2023
(H1 Antihistamines making immunotherapy more effective across cancers.)
1. Histamine receptor H1 antagonists and T cells: A cellular mini-immune system demonstrated that histamine receptor H1 antagonists can stimulate T cell proliferation and polarization, increasing their anticancer activity when used in combination with chemotherapy.
2. Role of Immune Checkpoint Inhibitors (ICIs) in cancer therapy: For a decade, ICIs targeting the PD-1–PD-L1 axis and CTLA-4 have shown durable therapeutic effects against various cancers, highlighting the importance of T cell-mediated anticancer immunity.
3. Immunogenic cell death (ICD): ICD caused by some anti-cancer treatments can stimulate tumor infiltration and antigen presentation by dendritic cells (DCs). The resulting expansion of tumor-antigen-specific cytotoxic T lymphocytes facilitates tumor regression and enhances therapeutic efficacy.
4. Screening system for ICD enhancers: A screening system utilizing antigen-presenting DCs and B3Z T cell hybridomas led to the discovery that the histamine receptor H1 antagonist astemizole can elicit T cell activation without requiring DC-mediated co-stimulation.
5. Mechanism of astemizole's T cell activation: Astemizole induced phosphorylation of specific proteins involved in TCR signaling, directly leading to T cell activation. This effect is attributed to astemizole's role as an HRH1 antagonist.
6. Astemizole's role in tumor therapy: In immunocompetent mice, astemizole alone showed no anticancer effects. However, in combination with an ICD inducer like oxaliplatin, it slowed tumor growth, an effect lost in immunodeficient animals, implicating an immune-mediated mechanism.
7. HRH1 expression in human cancers: Bioinformatic analysis revealed HRH1 expression in human cancers correlates with T cell exhaustion markers and inversely correlates with CD4+ TH1 cells.
8. Implications of HRH1 antagonists: HRH1 antagonists have been shown to enhance the efficacy of certain ICIs in cancer models. Retrospective clinical data also suggest HRH1 antagonist usage correlates with improved survival in some cancer patients. A recent trial showed circulating histamine levels inversely correlate with clinical response to PD-1 inhibitor immunotherapy.
A pharmacological network for lifespan extension in Caenorhabditis elegans (2014)
When Loratadine is given to worms, it extended lifespan by 18%.
Antihistaminic, Anti-Inflammatory, and Antiallergic Properties of the Nonsedating Second-Generation Antihistamine Desloratadine: A Review of the Evidence (2011)
Loratadine, an antihistamine drug, exhibits anti-inflammatory activity through suppression of the NF-kB pathway (2020)
Loratadine is an antihistamine drug that shows promise as an anti-inflammatory drug, but supportive studies are lacking. We elucidated the effects and mechanisms by which loratadine inhibits inflammatory responses. Molecular components were evaluated in macrophages by nitric oxide assay, polymerase chain reaction, luciferase assay, immunoblotting, overexpression strategies and cellular thermal shift assay. At the molecular level, loratadine reduced the levels of nitric oxide, iNOS, IL-1β, TNF-α, IL-6, and COX-2 in RAW264.7 cells treated with lipopolysaccharide. Loratadine also specifically inhibited the NF-kB pathway, targeting the Syk and Src proteins. Furthermore, loratadine bound Src in the bridge between SH2 and SH3, and bound Syk in the protein tyrosine kinase domain. The NF-kB signaling pathway was assessed along with putative binding sites through a docking approach. The anti-inflammatory effect of loratadine was tested using mouse models of gastritis, hepatitis, colitis, and peritonitis. Stomach tissue histopathology, liver morphology, and colon length in the loratadine group were improved over the group without loratadine treatment. Taken together, loratadine inhibited the inflammatory response through the NF-kB pathway by binding with the Syk and Src proteins.
Involvement of mast cells by the malignant process in patients with Philadelphia chromosome negative myeloproliferative neoplasms (2009)
The Philadelphia chromosome negative myeloproliferative neoplasms (MPNs) are clonal hematologic malignancies frequently characterized by a mutation in JAK2 (JAK2V617F). Peripheral blood (PB) CD34+ cells from patients with polycythemia vera (PV) and primary myelofibrosis (PMF) generated in vitro significantly fewer mast cells (MCs) than normal PB CD34+ cells. The numbers of MC progenitors assayed from MPN CD34+ cells were, however, similar to that assayed from normal CD34+ cells. A higher percentage of the cultured MPN MCs expressed FcɛRIα, CD63 and CD69 than normal MCs, suggesting that cultured MPN MCs are associated with an increased state of MC activation. Further analysis showed that a higher proportion of cultured PV and PMF MCs underwent apoptosis in vitro. By using JAK2V617F, MplW515L and chromosomal abnormalities as clonality markers, we showed that the malignant process involved MPN MCs. JAK2V617F-positive MC colonies were assayable from the PB CD34+ cells of each of the 17 JAK2V617F positive MPN patients studied. Furthermore, erlotinib, a JAK2 inhibitor, was able to inhibit JAK2V617F-positive PV MC progenitor cells, indicating that malignant MC progenitor cells are a potential cellular target for such JAK2 inhibitor-directed therapy.
A Study of Histamine in Myeloproliferative Disease (link)
SUMMARY
1. Whole blood histamine content was measured in 80 patients with myeloproliferative disease. Increased levels were found in 60 per cent of patients with uncontrolled polycythemia vera, in 7 per cent of patients with polycythemia vera being controlled by myelosuppressive therapy, and in 71 per cent of a group with "spent" polycythemia, myeloid metaplasia and myelofibrosis.
2. The excretion of histamine in the urine was measured in 60 patients, 30 with elevated blood histamine and 30 with normal blood histamine. The urine histamine findings paralleled the blood findings in 90 per cent of the cases.
3. Measurements of cell-poor and cell-rich fractions of blood showed that the histamine is contained in the white cell fraction. Elevated basophil counts were present in 50 per cent of the patients and occurred with the greatest frequency in the groups with elevated blood and urine histamine. A rough correlation between the basophil count and the histamine content of blood and white cell fractions was observed in normal subjects and most cases with myeloproliferative disease. Data obtained in some cases of myeloproliferative disease suggest that the histamine content of the basophil may be abnormal and that other granulocytes may contribute to the total leukocyte histamine.
4. Myelosuppressive agents produced a reduction in histamine (expressed per 109 myeloid cells) and a decrease in urine histamine as control of the myeloproliferative process was achieved. Treatment with phlebotomy alone produced no change in histamine levels.
5. The incidence of pruritus, upper gastrointestinal distress and urticarial manifestations was increased 7-fold, 4-fold and 12-fold, respectively, in patients with elevated histamine levels as compared with those who had normal histamine levels.
Pathophysiological Roles of Histamine Receptors in Cancer Progression: Implications and Perspectives as Potential Molecular Targets, 2021
Abstract
High levels of histamine and histamine receptors (HRs), including H1R~H4R, are found in many different types of tumor cells and cells in the tumor microenvironment, suggesting their involvement in tumor progression. This review summarizes the latest evidence demonstrating the pathophysiological roles of histamine and its cognate receptors in cancer biology. We also discuss the novel therapeutic approaches of selective HR ligands and their potential prognostic values in cancer treatment. Briefly, histamine is highly implicated in cancer development, growth, and metastasis through interactions with distinct HRs. It also regulates the infiltration of immune cells into the tumor sites, exerting an immunomodulatory function. Moreover, the effects of various HR ligands, including H1R antagonists, H2R antagonists, and H4R agonists, on tumor progression in many different cancer types are described. Interestingly, the expression levels of HR subtypes may serve as prognostic biomarkers in several cancers. Taken together, HRs are promising targets for cancer treatment, and HR ligands may offer novel therapeutic potential, alone or in combination with conventional therapy. However, due to the complexity of the pathophysiological roles of histamine and HRs in cancer biology, further studies are warranted before HR ligands can be introduced into clinical settings.

Desloratadine, a Novel Antigrowth Reagent for Bladder Cancer (2020)
Desloratadine, a potent antagonist for human histamine H1 receptor, has been revealed to exhibit antihistaminic activity and anti-inflammatory activity. However, it is not yet known whether desloratadine has any effect on the biological behaviors of tumor cells. In this study, we aimed to investigate the effects of desloratadine on cell growth and invasion in bladder cancer EJ and SW780 cells in vitro. We observed that desloratadine inhibited cell viability of EJ and SW780 cells in a dose- and time-dependent manner. Desloratadine treatment was also revealed to suppress colony-formation ability and induce cell cycle arrest at G1 phase in EJ cells. Desloratadine promoted cell apoptosis via modulating the expression of Bcl-2, Bax, cleaved caspase 3, and cleaved caspase 9 in EJ and SW780 cells. Western blot resulted showed that desloratadine also impaired the expression of autophagy-related proteins, such as Beclin 1, P62, and LC3I/II in EJ and SW780 cells; while autophagy inhibitor LY294002 reversed the effects of desloratadine on these proteins. Moreover, desloratadine remarkably attenuated cell migration and invasion. Furthermore, we illustrated that desloratadine downregulated the expression of N-cadherin, Vimentin, Snail1, and Snail2, while upregulated the expression of E-cadherin in EJ and SW780 cells in vitro. The level of interleukin 6 was reduced in desloratadine-treated cells, while upregulation of interleukin 6 significantly abolished the anticancer activity of desloratadine in cell invasion and Bcl-2, Bax, Beclin1, LC3-I/II, N-cadherin, and E-cadherin expression in EJ cells. Taken together, our data suggest a potential anticancer activity of desloratadine on cell growth and invasion for bladder cancer, which may be mediated by diminishing the epithelial-to-mesenchymal transition and interleukin 6.
Histamine H1 receptor antagonists selectively kill cisplatin-resistant human cervical cancer cells, 2021
Cancer therapy is often hampered by the disease’s development of resistance to anticancer drugs. We previously showed that the autonomously upregulated product of fibroblast growth factor 13 gene (FGF13; also known as FGF homologous factor 2 (FHF2)) is responsible for the cisplatin resistance of HeLa cisR cells and that it is likely responsible for the poor prognosis of cervical cancer patients treated with cisplatin. Here we show that cloperastine and two other histamine H1 receptor antagonists selectively kill HeLa cisR cells at concentrations that little affect parental HeLa S cells. The sensitivity of HeLa cisR cells to cloperastine was abolished by knocking down FGF13 expression. Cisplatin-resistant A549 cisR cells were similarly susceptible to cloperastine. H2, H3, and H4 receptor antagonists showed less or no cytotoxicity toward HeLa cisR or A549 cisR cells. These results indicate that histamine H1 receptor antagonists selectively kill cisplatin-resistant human cervical cancer cells and suggest that this effect is exerted through a molecular mechanism involving autocrine histamine activity and high-level expression of FGF13. We think this represents a potential opportunity to utilize H1 receptor antagonists in combination with anticancer agents to treat cancers in which emergent drug-resistance is preventing effective treatment.
Astemizole: an old anti-histamine as a new promising anti-cancer drug (2011)
Mortality-to-incidence ratio in cancer patients is extremely high, positioning cancer as a major cause of death worldwide. Despite hundreds of clinical trials for anti-cancer drugs that are currently in progress, most clinical trials for novel drug treatments fail to pass Phase I. However, previously developed drugs with novel anti-tumor properties offer a viable and cost-effective alternative to fight cancer. Histamine favors the proliferation of normal and malignant cells. Several anti-histamine drugs, including astemizole, can inhibit tumor cell proliferation. Astemizole has gained enormous interest since it also targets important proteins involved in cancer progression, namely, ether à-go-go 1 (Eag1) and Eag-related gene (Erg) potassium channels. Furthermore, Eag1 is thought to be an important marker and a therapeutic target for several different cancers. Astemizole inhibits Eag1 and Erg channel activity, and in cells expressing the Eag1 channel it decreases tumor cell proliferation in vitro and in vivo. It should be noted that some cardiovascular side effects have been reported for astemizole in a few rare cases. Nevertheless, astemizole stands as a very promising anti-cancer tool because it displays several anti-proliferative mechanisms, may serve as the basis to synthesize new anti-cancer agents, and has been previously administered clinically. In this review we will summarize the main findings relating to histamine and anti-histamines in cancer cell proliferation focusing on astemizole targets (Eag1 and Erg channels), and its anti-cancer effects in vitro and in vivo. We will also describe the side effects of astemizole and discuss proposals to overcome such effects in cancer patients. Finally, we will remark on the relevance of developing novel astemizole-related compounds.
Antihistamines as promising drugs in cancer therapy (2017)
Histamine is a biogenic amine, synthetized and released by mast cells, which acts as a vasodilator in several pathologic processes, namely in allergies and conjunctivitis. Its role on cancer is not fully understood. High levels of histamine have been associated with a bivalent behavior in regulation of several tumors (i.e. cervical, ovarian, vaginal, uterine, vulvar, colorectal cancer, and melanoma), promoting or inhibiting their growth. Histamine receptors (H1, H2, H3 and H4) are present in a vast group of cells, including tumor cells, making them sensitive to histamine variations. In this work, we review the role of mast cells and histamine on cancer development and the possibility of use antihistamines in the clinical management of this disease.
Can Antihistamines Decrease Cancer Risk If Used Daily For Over One Year? (2009)
RATIONALE: Epidemiologic studies have suggested individuals with any type of allergy have a decreased risk for cancer (compared with the general population). Allergy treatment has not been looked at as a factor of this association.
METHODS: A survey was conducted on patients of 7 allergists' offices. Patients were divided into 2 groups. In one group, the survey questionnaires were answered from the medical records by the nurses and patients' responses if available (1539 patients). The second group voluntarily answered the survey (521 patients). The survey lasted for 2 months, ending in May 2007. Patients were excluded if their allergy symptoms were < 1 year or < 18 years old, or if had cancer before their allergy symptoms began. Medications used, their duration, if used daily (80 to 100% of the year) for over a year were requested. The study was approved by Essex Institutional Review Board.
RESULTS: The risk of developing cancer in the first group was 1.93% for daily antihistamines and 4.76% for as needed medications and with P value 0.0081. In second group the risk of cancer was 5.31% for daily medications and 6.84% for as needed group. The difference was not statistical significant.
CONCLUSIONS: Daily intake of antihistamines, when well documented, for > 1year may be associated with decrease cancer risk. Repeating the same work on a larger scale by others might be needed before confirming this association.
[NEGATIVE] Association of Prescription H1 Antihistamine Use With Obesity: Results From the National Health and Nutrition Examination Survey, 2010
Abstract
The incidence of obesity in the United States has reached epidemic proportions. Previous research has shown several medications exert noticeable effects on body-weight regulation. Histamine-1 (H1) receptor blockers commonly used to alleviate allergy symptoms are known to report weight gain as a possible side effect. Therefore, we investigated the association between prescription H1 antihistamine use and obesity in adults using data from the 2005-2006 National Health and Nutrition Examination Survey (NHANES). Adults taking prescription H1 antihistamines were matched by age and gender with controls and compared on the basis of body measurements, plasma glucose, insulin concentrations, and lipid levels. Prescription H1 antihistamine users had a significantly higher weight, waist circumference, and insulin concentration than matched controls. The odds ratio (OR) for being overweight was increased in prescription H1 antihistamine users. H1 antihistamine use may contribute to the increased prevalence of obesity and the metabolic syndrome in adults given these medications are also commonly used as over-the-counter remedies.
Antihistamines and Weight Gain | Obesity Medicine Association (link)
[NEGATIVE] Prolonged intake of desloratadine: mesenteric lymphatic vessel dysfunction and development of obesity/metabolic syndrome, 2018
This study aimed to establish mechanistic links between the prolonged intake of desloratadine, a common H1 receptor blocker (i.e., antihistamine), and development of obesity and metabolic syndrome. Male Sprague-Dawley rats were treated for 16 wk with desloratadine. We analyzed the dynamics of body weight gain, tissue fat accumulation/density, contractility of isolated mesenteric lymphatic vessels, and levels of blood lipids, glucose, and insulin, together with parameters of liver function. Prolonged intake of desloratadine induced development of an obesity-like phenotype and signs of metabolic syndrome. These alterations in the body included excessive weight gain, increased density of abdominal subcutaneous fat and intracapsular brown fat, high blood triglycerides with an indication of their rerouting toward portal blood, high HDL, high fasting blood glucose with normal fasting and nonfasting insulin levels (insulin resistance), high liver/body weight ratio, and liver steatosis (fatty liver). These changes were associated with dysfunction of mesenteric lymphatic vessels, specifically high lymphatic tone and resistance to flow together with diminished tonic and abolished phasic responses to increases in flow, (i.e., greatly diminished adaptive reserves to respond to postprandial increases in lymph flow). The role of nitric oxide in this flow-dependent adaptation was abolished, with remnants of these responses controlled by lymphatic vessel-derived histamine. Our current data, considered together with reports in the literature, support the notion that millions of the United States population are highly likely affected by underevaluated, lymphatic-related side effects of antihistamines and may develop obesity and metabolic syndrome due to the prolonged intake of this medication.
Is the next 'new' cancer drug already in your medicine cabinet? Antihistamines may have anti-cancer properties -- ScienceDaily (link)
Antihistamines may have significant anti-cancer properties as they interfere with the function of a type of cell that is known to reduce the body's ability to fight tumors (called "myeloid derived suppressor cells"). Mast cell histamine promotes the immunoregulatory activity of myeloid-derived suppressor cells, 2014.
Can antihistamines like Cimetidine, Desloratadine and Loratadine play an integrative role in cancer cure?
17 May 2020
Antihistamines can reduce metastases and increase cancer survival
Cimetidine, or Tagamet, has been shown in research to increase cancer survival following colorectal cancer surgery; Desloratadine and Loratadine have been shown to increase survival of both ER+ve and ER-ve breast cancer patients by more than 30 per cent. Here we look at just how antihistamines might help fight cancer. (Chris Woollams; CANCERactive).
Histamines are essential to cancer proliferation
It is of no surprise then that high histamine levels have been found in people with breast cancer, colorectal cancer, ovarian cancer, melanoma, cervical cancer and pancreatic cancer. Indeed, cancer cells have more histamine receptors on their surface than healthy cells, and these help inflame the cancer cell, help it spread and help cancer cells stick together to form tumours, and stick to organs like your lungs, bones and liver. Histamine levels also seem to increase simultaneously in peripheral tissues, almost as if they were drawing cancer cells towards them.
Antihistamines stop cancer cells sticking and spreading
2. Antihistamines like Desloratadine and Loratadine (Claritin) increase survival times
Unfortunately, all anti-histamines were not created equal. Cimetidine is an H2 antagonist like ranitidine and primarily used for acid reflux. Antihistamines like Desloratadine are H1 antagonists and used for allergies.
Swedish researchers(1) reviewed more than 50,000 women who had ER+ Breast cancer and those who simultaneously took a second generation antihistamine. When comparing users with non-users a significant survival improvement was seen for the users of 30 per cent or more. Various antihistamines were compared and Desloratadine provided the best results; Loratadine was not far behind.
Repurposed drugs for Oncology (ReDo) like Antihistamines seem able to reduce metastases, improve immune response and increase survival times
Although the exact method of action is not clear, there is more than enough research now to suggest using any of these inexpensive drugs is of significant benefit to people with cancer. There are a good number of scientific reviews on the Internet, for example (5) explaining how histamines enhance cancer growth and spread and how anti-histamines can block this action.
Anti-histamines reduce cancer membrane velco patches by blocking histamine receptor sites; and have immuno-modulating action increase immune response, They thus reduce cancer growth, cancer metastases and increase survival. We believe all our readers should consider the use of antihistamines as part of their Integrative Cancer Treatment Programme.
We do not believe Loratadine should be taken for more than 10 weeks in any year as there is a study showing that long-term use (but not short-term use) can increase breast cancer risk.
Repurposing Cationic Amphiphilic Antihistamines for Cancer Treatment
Loratadine, was associated with significantly reduced all-cause mortality among patients with non-localized NSCLC or any non-localized cancer when compared with use of non-CAD antihistamines and adjusted for potential confounders. Of the less frequently described CAD antihistamines, astemizole showed a similar significant association with reduced mortality as loratadine, and ebastine use showed a similar tendency. In line with this, sub-micromolar concentrations of loratadine, astemizole and ebastine sensitized cancer cells to chemotherapy and reverted multidrug resistance in NSCLC, breast and prostate cancer cells. Thus, CAD antihistamines may improve the efficacy of cancer chemotherapy.
Effects of antihistamine use on survival in breast cancer.
We investigated the effects of six antihistamines on breast cancer-specific and overall mortality in a nation-wide register-based study of all 61,627 Swedish women with newly diagnosed breast cancer. We found a consistently beneficial effect of desloratadine and loratadine use on breast cancer survival (with HRs ranging from 0.47-0.84 for desloratadine users relative to non-use), regardless of age, stage and estrogen receptor status, and a consistently negative effect on breast cancer survival of clemastine use.
Conclusions: We suggest trials of high-dose and long-duration desloratadine and loratadine as adjuvant treatment of breast cancer.
Brain Cancer (GBM) Halted in Mice Using Antihistamine Drug
Studies demonstrated an association between the fatty acid binding protein mammary-derived growth inhibitor (MDGI) and poorer prognosis in patients. MDGI shuttles fatty acids into cells, and the team’s studies found that blocking the MDGI gene in glioblastoma cell lines disrupted fatty acid transport into cells and incorporation into lysosomal membranes. Antihistamines and other drugs that increase the permeability of the lysosomal membrane can be considered as an enhancing therapy for patients with glioblastoma alongside established treatments.
Potential of Antihistamine Allergy Meds in Combatting Cancer
A specific group of antihistamine medications can eradicate leukaemic stem cells. These antihistamines cannot currently be used to combat leukaemia due to how quickly they degrade in the body and the lack of a direct administration method on cancer cells.
The second generation antihistamine, loratadine (LOR), was found to have tumor inhibiting effects on human colon carcinoma cell line.
Antihistamines and Ovarian Cancer Survival: Nationwide Cohort Study and in Vitro Cell Viability Assay
Evaluated the association between filled antihistamine prescriptions and cancer mortality. In our cohort study, CAD antihistamine use (≥1 prescription; n = 133) was associated with a hazard ratio of 0.63 (95% CI = 0.40 to 0.99) compared to use of non-CAD antihistamines (n = 304), and we found a tendency toward a dose-response association. In our cell viability assay, we found consistent and dose-dependent cytotoxicity for all CAD but not non-CAD antihistamines.
MPNs and Bone Pain (link)
As the panel from MD Anderson explained, over-the-counter treatments may provide relief to people experiencing pruritus. Antihistamines such as Benadryl and Zyrtec can be used to help control itching. As always, please speak to your cancer team before starting any new medications or complementary therapies.
Another MPN side effect is bone pain. This is often caused by an overload of histamines in the blood but can also be a side effect of MPN treatments.
The team at MD Anderson treats bone pain with antihistamines, similar to how they treat itching. Having access to an over-the-counter drug — under the care of a doctor — allows patients easier and more affordable ways of control the disease and its side effects.
Is loratadine metabolized in liver or kidney?
Loratadine is primarily metabolized in the liver. Cytochrome P450 enzymes, specifically CYP3A4 and, to a lesser extent, CYP2D6, are responsible for converting loratadine to its active metabolite, desloratadine. Once metabolized, both loratadine and its metabolites are excreted in the urine and feces. The kidneys play a role in excreting these substances, but the metabolism (chemical modification) primarily occurs in the liver. If someone has liver impairment, it might affect the metabolism of loratadine, so it's essential to consult with a healthcare professional regarding its use in such cases.
—---------
Antihistamines and azithromycin as a treatment for COVID-19 on primary health care – A retrospective observational study in elderly patients
Between March and April 2020, 84 elderly patients with suspected COVID-19 living in two nursing homes of Yepes, Toledo (Spain) were treated early with antihistamines (dexchlorpheniramine, cetirizine or loratadine), adding azithromycin in the 25 symptomatic cases. The outcomes are retrospectively reported. The primary endpoint is the fatality rate of COVID-19. The secondary endpoints are the hospital and ICU admission rates. Endpoints were compared with the official Spanish rates for the elderly. The mean age of our population was 85 and 48% were over 80 years old. No hospital admissions, deaths, nor adverse drug effects were reported in our patient population. By the end of June, 100% of the residents had positive serology for COVID-19. Although clinical trials are needed to determine the efficacy of both drugs in the treatment of COVID-19, this analysis suggests that primary care diagnosis and treatment with antihistamines, plus azithromycin in selected cases, may treat COVID-19 and prevent progression to severe disease in elderly patients.
Desloratadine inhibits constitutive and histamine-stimulated nuclear factor-kappaB activity consistent with inverse agonism at the histamine H1 Receptor
Background: The human histamine H1 receptor is constitutively active and exhibits basal activation of nuclear factor-kappaB (NF-kappaB), an important modulator of allergic inflammation. Certain H1 antihistamines have recently been shown to inhibit basal NF-kappaB activity by stabilizing the H1 receptor in an inactive state, a phenomenon called 'inverse agonism'.
Methods: We evaluated the effect of the new H1 antihistamine, desloratadine, on basal and histamine-stimulated NF-kappaB activity and compared it with the activities of other H1 antihistamines.
Results: Transiently transfected COS-7 cells co-expressing NF-kappaB-luciferase and the H1 receptor exhibited constitutive NF-kappaB activity. H1 antihistamines reduced basal NF-kappaB activity (rank order of potency: desloratadine > pyrilamine > cetirizine > loratadine > fexofenadine). Histamine stimulated basal NF-kappaB activity 8-fold, which was blocked by H1 antihistamines (rank order of potency: desloratadine > cetirizine > pyrilamine > loratadine > fexofenadine). Neither histamine nor antihistamines had any effect on NF-kappaB activity in the absence of the H1 receptor.
Conclusions: Desloratadine, acting through the histamine H1 receptor, inhibited basal NF-kappaB activity and can thus be classified as an inverse agonist. Inhibition of basal and histamine-stimulated NF-kappaB activity may help to explain previously reported inhibitory effects of desloratadine on allergic inflammatory mediators.
Chronic ingestion of H1-antihistamines increase progression of atherosclerosis in apolipoprotein E-/- mice, 2014
Although increased serum histamine levels and H1R expression in the plaque are seen in atherosclerosis, it is not known whether H1R activation is a causative factor in the development of the disease, or is a host defense response to atherogenic signals. In order to elucidate how pharmacological inhibition of histamine receptor 1 (H1R) signaling affects atherogenesis, we administered either cetirizine (1 and 4 mg/kg. b.w) or fexofenadine (10 and 40 mg/kg. b.w) to ApoE-/- mice maintained on a high fat diet for three months. Mice ingesting a low dose of cetirizine or fexofenadine had significantly higher plaque coverage in the aorta and cross-sectional lesion area at the aortic root. Surprisingly, the higher doses of cetirizine or fexofenadine did not enhance atherosclerotic lesion coverage over the controls. The low dose of fexofenadine, but not cetirizine, increased serum LDL cholesterol. Interestingly, the expression of iNOS and eNOS mRNA was increased in aortas of mice on high doses of cetirizine or fexofenadine. This may be a compensatory nitric oxide (NO)-mediated vasodilatory mechanism that accounts for the lack of increase in the progression of atherosclerosis. Although the administration of cetirizine did not alter blood pressure between the groups, there was a positive correlation between blood pressure and lesion/media ratio at the aortic root in mice receiving the low dose of cetirizine. However, this association was not observed in mice treated with the high dose of cetirizine or either doses of fexofenadine. The macrophages or T lymphocytes densities were not altered by low doses of H1-antihistamines, whereas, high doses decreased the number of macrophages but not T lymphocytes. The number of mast cells was decreased only in mice treated with low dose of fexofenadine. These results demonstrate that chronic ingestion of low therapeutic doses of cetirizine or fexofenadine enhance progression of atherosclerosis.
Histamine H1 Receptor Promotes Atherosclerotic Lesion Formation by Increasing Vascular Permeability for Low-Density Lipoproteins, 2010
Objective— Enhanced endothelial permeability leading to intimal accumulation of low-density lipoproteins (LDL) stimulates the formation of atherosclerotic lesions. Histamine is known to increase vascular permeability. Whether this affects the formation of atherosclerotic lesions, however, remains elusive.
Methods and Results— Apolipoprotein E–null (ApoE−/−) mice treated with a histamine H1 receptor but not an H2 receptor antagonist developed 40% fewer atherosclerotic lesions in the aorta than placebo-treated controls. Similarly, genetic deletion of the H1 but not the H2 receptor resulted in a 60% reduction of lesions compared with ApoE−/− controls. The H1 receptor enhanced LDL permeability and lipid accumulation in the aorta, whereas plasma lipoprotein levels remained unaltered. In contrast, the H1 receptor did not affect proliferation and migration of vascular smooth muscle cells. Bone marrow transplantation confirmed that the formation of atherosclerotic lesions depended on the H1 receptor in vascular cells, whereas its presence in bone marrow-derived cells was irrelevant for plaque development. Mice expressing the H1 receptor exhibited higher levels of the chemokine (C-C motif) ligand 5 and higher numbers of macrophages and T-helper lymphocytes in plaques, higher numbers of circulating lymphocytes, and larger spleens.
Conclusion— These data indicate that H1 but not H2 receptor activation drives the formation of atherosclerotic lesions through an increased vascular permeability for LDL, which is associated with an enhanced secondary aortic and systemic inflammation. These data open novel perspectives for the prevention and treatment of atherosclerotic vascular disease.
Effect of chronic ingestion of a histamine H1 receptor antagonist on the progression of atherosclerosis in the apolipoprotein-E null mouse (54.1), 2011
Histamine (HIS) is a known modulator of vascular functions and its levels are elevated in coronary arteries in ischemic heart disease and variant angina. We have shown that HIS, acting via H1 receptors (H1R), stimulates the expression of IL-6, COX2, TLR2 and TLR4 in human endothelial cells. The study tested the effect of chronic ingestion of cetirizine (CET), an H1R antagonist, on atherosclerosis progression in ApoE-/- mice. CET containing water (5 mg/L) or plain water was supplied ad libitum to male ApoE-/- mice for 3 and 5 months, after which 24h urine, blood, and aorta were collected. The lesion coverage in the descending aorta and intima/media thickness at aortic root were quantified. The aortic tissue was also analyzed for COX1, COX2, H1R, IL10, Egr1 and MCP2 mRNA expression and for macrophages (MAC3+), T lymphocytes (CD3+) and mast cells (CD117+). A significant increase in plaque thickness was noted in CET-treated mice at 3 months but not at 5 months. Aortic lesion coverage between control and CET groups remained unchanged at 3 and 5 months. PGI2 and TXA2 indices in urine at 3 months showed reduction in PGI2/TXA2 ratio. RT- PCR data showed significantly decreased expression of COX1 and H1R but no changes in other genes. The lesion coverage, urinary prostanoid levels, gene expression, serum lipids, and MAC3+, CD3+ and CD117+ cell numbers were unchanged at 5 months. The results suggest that long-term use of CET does not alter atherosclerosis progression in ApoE-/- mice.
Histamine H1 type receptor antagonist loratadine ameliorates oxidized LDL induced endothelial dysfunction, 2019
Abstract
Oxidized LDL (ox-LDL) is one of the major risk factors of atherosclerosis. Endothelial dysfunction caused by ox-LDL is an early event in the pathogenesis of cardiovascular diseases. Preclinical studies have been performed to explore efficient means of preventing endothelial abnormalities. In this study, we revealed that loratadine, a histamine H1 type receptor specific antagonist, possesses a protective effect by relieving ox-LDL-induced endothelial inflammation. Treatment of endothelial cells with ox-LDL induces expression of the H1 receptor. The presence of loratadine in endothelial culture efficiently suppressed ox-LDL-induced attachment of monocytes to endothelial cells, production of ROS and vascular adhesion molecules, and induction cytokines including VCAM-1, E-selectin, TNF-α, IL-6 and IL-8. Mechanistically, we show that loratadine potently blocks ox-LDL-induced JNK activation as well as the AP-1 and NF-κB signaling pathways. Collectively, our data disclose a new role for loratadine in endothelial protection.
Influence of prior comorbidities and chronic medications use on the risk of COVID-19 in adults: a population-based cohort study in Tarragona, Spain
Objective: To investigate possible relationships between pre-existing medical conditions (including common comorbidities and chronic medications) and risk for suffering COVID-19 disease in middle-aged and older adults.
Design: Population-based retrospective cohort study.
Setting: Twelve primary care centres (PCCs) in Tarragona (Spain).
Participants: 79 083 people (77 676 community-dwelling and 1407 nursing-home residents), who were all individuals aged >50 years affiliated to the 12 participating PCCs.
Outcomes: Baseline cohort characteristics (age, sex, vaccinations, comorbidities and chronic medications) were established at study start (1st. March 2020) and primary outcome was time to COVID-19 confirmed by PCR among cohort members throughout the epidemic period (from 1st. March 2020 to 23rd. May 2020). Risk for suffering COVID-19 was evaluated by Cox regression, estimating multivariable HRs adjusted for age, sex, comorbidities and medications use.
Results: During the study period, 2324 cohort members were PCR-tested, with 1944 negative and 380 positive results, which means an incidence of 480.5 PCR-confirmed COVID-19 cases per 100 000 persons-period. Assessing the total study cohort, only age (HR 1.02; 95% CI 1.01 to 1.03; p=0.002), nursing-home residence (HR 21.83; 95% CI 16.66 to 28.61; p<0.001) and receiving diuretics (HR 1.35; 95% CI 1.04 to 1.76; p=0.026) appeared independently associated with increased risk. Smoking (HR 0.62; 95% CI 0.41 to 0.93; p=0.022), ACE inhibitors (HR 0.68; 95% CI 0.47 to 0.99; p=0.046) and antihistamine (HR 0.47; 95% CI 0.22 to 1.01; p=0.052) were associated with a lower risk. Among community-dwelling individuals, cancer (HR 1.52; 95% CI 1.03 to 2.24; p=0.035), chronic respiratory disease (HR 1.82; 95% CI 1.08 to 3.07; p=0.025) and cardiac disease (HR 1.53; 95% CI 1.06 to 2.19; p=0.021) emerged to be also associated with an increased risk. Receiving ACE inhibitors (HR 0.66; 95% CI 0.44 to 0.99; p=0.046) and influenza vaccination (HR 0.63; 95% CI 0.44 to 0.91; p=0.012) was associated with decreased risk.
Conclusion: Age, nursing-home residence and multiple comorbidities appear predisposing for COVID-19. Conversely, receiving ACE inhibitors, antihistamine and influenza vaccination could be protective, which should be closely investigated in further studies specifically focused on these concerns.
Ellagitannins
JAK2 and AMP-kinase inhibition in vitro by food extracts, fractions and purified phytochemicals
We have identified a range of food phytochemicals that inhibit Janus Kinase 2 (JAK2) and Adenosine Monophosphate Kinase (AMPK). A mutated and dysregulated form of JAK2, a tyrosine kinase, is associated with several diseases including Crohn's disease. Using an in vitro, time-resolved fluorescence (TR-FRET) assay, we tested 49 different types of food extracts, plus 10 concentrated fractions of increasing hydrophobicity from each extract, to find foods containing JAK2 inhibitors. The food extracts tested included grains, meat, fish, shellfish, dairy products, herbs, mushrooms, hops, fruits and vegetables. Several fruits were potent inhibitors of JAK2: blackberry, boysenberry, feijoa, pomegranate, rosehip and strawberry, which all contain ellagitannins, known inhibitors of kinases. These fruits are in the Rosales and Myrtales plant orders. No other foods gave >1% of the maximal JAK2 inhibitory activities of these fruits. AMPK, a sensor and regulator of energy metabolism in cells, is a serine-threonine kinase which is reported to be activated by various flavonoid phytochemicals. Using a TR-FRET assay, we tested various fruit extracts for AMPK activation and inhibition. Ellagitannin containing foods scored highly as AMPK inhibitors. Despite several reports of AMPK activation in whole cells by phytochemicals, no extracts or pure compounds activated AMPK in our assay.
(I think higher the compound, the better.)
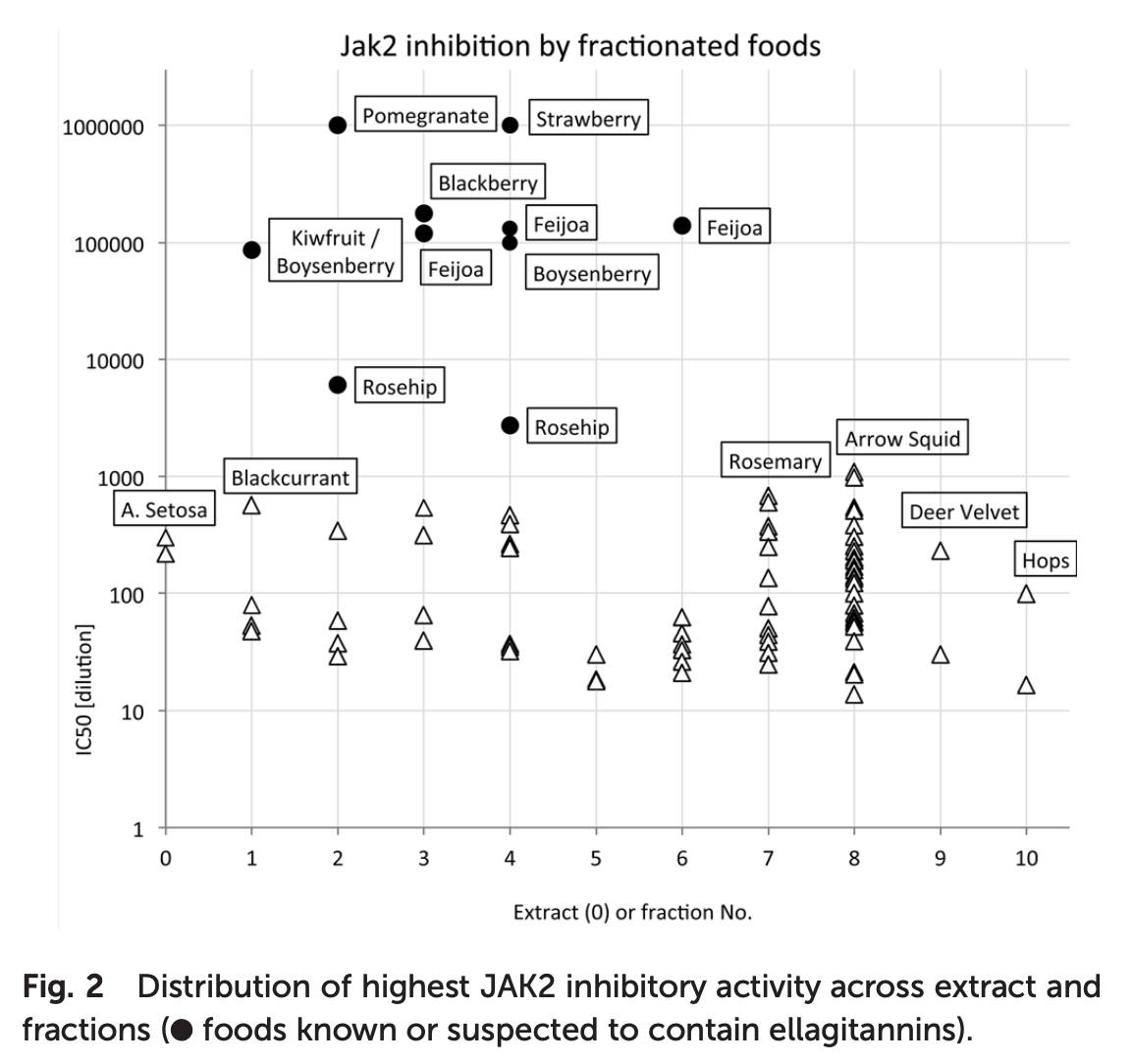
What are Ellagitannins?
Ellagitannins are a type of polymer that is formed when ellagic acid and a hydroxyl group, like glucose, bind together. Considered a type of antioxidant, it can be found in various fruits, such as raspberries and blackberries, and in red wine. Although research is still preliminary, some people believe ellagic acid may help to prevent certain cancers and heart disease. Ellagitannins may be taken as part of a meal, or in capsule form as a nutritional supplement.
Antioxidants like ellagitannins may help to protect the body's cells against the damage caused by free radicals. Many antioxidants are combined in nutritional supplements that are also rich in vitamin C and iron to provide complete antioxidant supplementation. It should be noted that many of the purported benefits of ellagitannins have not been proven in scientific studies; in the US, the Food and Drug Administration has warned supplement makers against promoting ellagic acid as a cure for disease.
It's been suggested that ellagitannins can help prevent prostate cancer in men.
It's been suggested that ellagitannins can help prevent prostate cancer in men.
There has been some suggestion that ellagitannins may help to prevent cancer, specifically cervical cancer in women and prostate cancer in elderly men. Some users believe it helps by preventing the cancerous cells from dividing and effectively slows down the rate at which the cancer may grow. Although research into this benefit is ongoing, there is no proof to support this claim.
Pomegranate juice and extract extended lifespan and reduced intestinal fat deposition in Caenorhabditis elegans, 2017
Pomegranate juice with a high content of polyphenols, pomegranate extract, ellagic acid, and urolithin A, have anti-oxidant and anti-obesity effects in humans. Pomegranate juice extends lifespan of Drosophila melanogaster. Caenorhabditis elegans (C. elegans) (n = 6) compared to the control group in each treatment, lifespan was increased by pomegranate juice in wild type (N2, 56 %, P < 0.001) and daf-16 mutant (daf-16(mgDf50)I) (18 %, P = 0.00012), by pomegranate extract in N2 (28 %, P = 0.00004) and in daf-16(mgDf50)I (10 %, P < 0.05), or by ellagic acid (11 %, P < 0.05). Pomegranate juice reduced intestinal fat deposition (IFD) in C. elegans (n = 10) N2 (−68 %, P = 0.0003) or in the daf-16(mgDf50)I (−33 %, P = 0.0034). The intestinal fat deposition was increased by pomegranate extract in N2 (137 %, P < 0.0138) and in daf-16(mgDf50)I (26 %, P = 0.0225), by ellagic acid in N2 (66 %, P < 0.0001) and in daf-16(mgDf50)I (74 %, P < 0.0001), or by urolithin A in N2 (57 %, P = 0.0039) and in daf-16(mgDf50)I (43 %, P = 0.0001). These effects were partially mediated by the daf-16 pathway. The data may offer insights to human aging and obesity due to homology with C. elegans.
Pomegranate for Your Cardiovascular Health (2013)
Blood samples were collected before treatment and after 3, 6, 9, and 12 months of PJ consumption. Patients’ carotid intima-media thickness (CIMT) was compared between the PJ group and the control group. While in the control patients group (no PJ) CIMT increased by 10% after 1 year (Figure 1A), PJ consumption resulted in a significant CIMT reduction, by up to 35% (Figure 1B). Analysis of the mean CIMT (of the left and right common carotid arteries) before and during PJ consumption revealed a gradual reduction of 13%, 22%, 26%, and 35%, as observed after 3, 6, 9, and 12 months of PJ consumption, respectively, in comparison to baseline values.
(This paper suggests PJ attenuates cardiovascular diseases. Blood velocity increases due to reduction of inner carotid wall thickening. I've been drinking diet PJ daily for over a year. No idea if it's the PJ, but when I run now I have to run extra hard to feel fatigue. The numbers in the study seem significant compared to controls.)
Pomegranate for Your Cardiovascular Health, 2013
"Blood samples were collected before treatment and after 3, 6, 9, and 12 months of PJ consumption. Patients’ carotid intima-media thickness (CIMT) was compared between the PJ group and the control group. While in the control patients group (no PJ) CIMT increased by 10% after 1 year (Figure 1A), PJ consumption resulted in a significant CIMT reduction, by up to 35% (Figure 1B). Analysis of the mean CIMT (of the left and right common carotid arteries) before and during PJ consumption revealed a gradual reduction of 13%, 22%, 26%, and 35%, as observed after 3, 6, 9, and 12 months of PJ consumption, respectively, in comparison to baseline values."
Effect of pomegranate juice consumption on biochemical parameters and complete blood count
Pomegranate has been used therapeutically for centuries. The aim of the present study was to examine the effects of pomegranate juice (PJ) supplementation on complete blood count (CBC), glucose, blood lipids and C-reactive protein (CRP) in healthy subjects. A total of 5 males and 5 females (aged 31.8±6.6 years, weighing 66.2±12.9 kg) were randomly assigned into one of two groups and either consumed 500 ml PJ/day or no PJ for 14 days. Blood samples were obtained from participants prior to and following the experimental period. PJ consumption resulted in a significant increase in red blood cell count (P<0.05), hemoglobin levels (P<0.001) and hematocrit levels (P<0.05). Other CBC parameters, glucose, cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein and CRP levels did not significantly change following PJ consumption. These results indicate that PJ intake for a short period of time may result in increased erythropoiesis or decreased degradation without any significant alterations in factors associated with metabolic health and inflammation in healthy individuals.
Researchers Rejuvenate Aging Immune Systems (link)
As we age, our immune system declines due to changes in hematopoietic stem cells, the progenitor cells that produce all blood and immune cells. These stem cells accumulate dysfunctional mitochondria, lose the ability to differentiate properly, and can't replenish immune cells.
The natural compound urolithin A can rejuvenate aged hematopoietic stem cells by improving mitochondrial health and function. Treating old stem cells with urolithin A in lab dishes restores their ability to produce immune cells.
When urolithin A-treated aged stem cells were transplanted into irradiated mice, the mice recovered just as well as those receiving young stem cells. This effect lasted 24 weeks.
Simply feeding old mice a diet enriched with urolithin A also rejuvenated their hematopoietic stem cells and immune function. The treated mice fought viruses better than untreated old mice.
Urolithin A shows promise as a potential anti-aging compound. It may improve immune function and resilience in old age. Dietary sources like pomegranates can provide urolithin A. More research is needed to develop consumer therapies.
Induction of mitophagy reverts age-associated decline of the hematopoietic and immune systems (2023)
The study by Girotra et al. (2023) demonstrates that inducing mitophagy through administration of the natural compound Urolithin A (UroA) reverts age-associated functional decline in hematopoietic stem cells (HSCs) and improves immune responses in aged mice. The key findings are:
- Aging leads to accumulation of dysfunctional mitochondria and reduced autophagy in HSCs, compromising their function. In vitro treatment with 20μM UroA for 3 days induced mitophagy, restored mitochondrial fitness and completely rejuvenated the long-term blood reconstitution capability of HSCs from old (>18 months) mice. UroA-treated old HSCs showed similar multi-lineage engraftment and self-renewal capability as HSCs from young mice upon transplantation into irradiated recipients and in secondary transplants.
- UroA treatment also improved colony forming potential of CD34+ hematopoietic progenitors from elderly human donors, suggesting conserved mechanisms.
- Oral supplementation of UroA for 4 months in old mice expanded the HSC pool, restored common lymphoid progenitors and improved T cell compartments in the spleen. Bone marrow from UroA-treated old mice showed improved engraftment upon transplantation compared to controls.
- UroA supplementation for 8 weeks improved virus-specific CD8+ T cell responses in old mice infected with lymphocytic choriomeningitis virus, with increased effector differentiation and cytotoxicity. This resulted in improved viral control. UroA treatment reversed age-associated decline in IL-7 signaling and exhaustion markers like PD-1 in virus-specific CD8+ T cells.
- The rejuvenating effects of UroA were mediated through induction of mitophagy, restored mitochondrial fitness and reduced mitochondrial content in HSCs. CD150high HSCs showed greater accumulation of dysfunctional mitochondria with age compared to CD150low HSCs, which was reversed by UroA.
In conclusion, the study demonstrates that UroA-mediated induction of mitophagy in aged HSCs restores their mitochondrial and metabolic fitness, reverses age-associated functional decline and improves immune responses against viral infection in old mice. The results establish mitophagy induction as a conserved mechanism for rejuvenation of hematopoietic and immune systems compromised by aging. The natural compound UroA represents a promising therapeutic approach to improve health and function of the hematopoietic system in elderly individuals.
Urolithin A is a metabolite compound resulting from the transformation of ellagitannins by the gut bacteria.
Gut Health and Aging: A Summary of Urolithin A
https://www.lifespan.io/topic/gut-health-and-aging-a-summary-of-urolithin-a/
A 2016 study showed that urolithin A improved muscle function in aged mice and extended lifespan in worms [6].
Could Pomegranate Polyphenols Hold The Key To Longevity? (link)
The importance of mitochondrial health for healthy aging. Mitochondria provide energy to cells and become less efficient as we age. Boosting mitochondrial health can promote longevity.
Mitophagy is the process cells use to clear out old, dysfunctional mitochondria and regenerate new healthy ones. It declines with age. Activities like exercise, fasting, and certain nutrients can stimulate mitophagy.
Dr. Singh has researched compounds from pomegranates called polyphenols. These get converted by gut bacteria into a molecule called urolithin A, which stimulates mitophagy based on his trials.
However, only 10-40% of people can make urolithin A from eating pomegranates due to variation in gut microbiome. So most can't get enough just through diet.
His company developed a direct urolithin A supplement to provide a consistent dose, since levels made naturally are variable. It's intended as an additional support on top of diet and exercise.
In trials, urolithin A improved measures of mitochondrial function, muscle strength and endurance within 1-4 months. It reduced inflammation and may help the immune system. No adverse effects were seen.
Urolithin A works by stimulating mitophagy - clearing out faulty mitochondria. Over a month or two, healthier mitochondria regenerate. This enhances cellular energy.
Muscle and brain cells have the highest numbers of mitochondria, so they are most impacted by mitochondrial dysfunction with aging. Urolithin A aims to maintain their vitality.
Three hallmarks of aging are: reduced mitophagy leading to mitochondrial dysfunction; chronic inflammation; and gut microbiome issues. Urolithin A may help address the first two.
Maintaining mitochondrial health appears key for healthy longevity, based on comparing muscle biopsies from fit vs frail seniors. Enhancing it may extend healthspan.
Dr. Wahls sees potential for urolithin A to support domains affected in neurological diseases like MS, such as fatigue, cognition and remyelination. Myelin repair requires cellular energy.
She is interested in exploring clinical trials using urolithin A as an add-on therapy in MS to reduce fatigue, boost cognition and improve myelin repair.
Urolithin A protects against acetaminophen-induced liver injury in mice via sustained activation of Nrf2 (2022)
This study investigated the effects of urolithin A (UA), a metabolite of ellagitannins produced by gut microbiota, on protecting against acetaminophen (APAP)-induced liver injury in mice. The key findings are:
UA treatment reduced liver damage and mortality in APAP-overdosed mice, as evidenced by decreased serum ALT/AST levels, reduced hepatic necrosis, and improved survival rate.
Mechanistically, UA induced mitophagy and activated Nrf2/ARE signaling pathway, which alleviated APAP-induced oxidative stress and mitochondrial dysfunction in the liver. However, mitophagy activation was not essential for UA's hepatoprotective effects.
Molecular modeling suggested UA could directly bind to Nrf2 and trigger its nuclear translocation and activation of downstream antioxidant genes like HO-1 and NQO1. Nrf2 knockdown abolished UA's protection against APAP toxicity.
Compared to N-acetylcysteine, UA conferred better therapeutic effects on APAP-induced liver injury, with lower dosage and longer treatment time window.
Overall, this study demonstrates UA protects against APAP overdose-induced liver damage mainly through activating Nrf2-mediated antioxidant response, and suggests UA's translational potential for treating acetaminophen hepatotoxicity.
Current and hypothetical therapies targeting liver mitochondria to treat NAFLD and hyperglycemia (2021)
Modulating mitophagy could decrease lipogenesis in the liver by targeting lipogenic mitochondria for degradation. Indeed, preclinical studies suggested that mitochondrial quality control and mitophagy are reduced in NAFLD, with the restoration of mitophagy preventing or reversing some features of simple steatosis and NASH [[90], [91], [92]]. One could hypothesize that lipogenic mitochondria accumulate in simple steatosis and NASH because hyperinsulinemia and hyperlipidemia suppress their elimination by mitophagy. Agreeing with this hypothesis, treatment with a natural molecule that restores mitophagy, urolithin A [93], improves glucose homeostasis and protects mice from hepatic steatosis [94]. Moreover, current drugs improving steatosis and NASH in humans, such as metformin and liraglutide, increase mitophagy in rodent models of simple steatosis and NASH [95,96]. Cotadutide, which targets GLP1R and GCGR and improves NASH, also enhances mitophagy [8]. Of note, cotadutide mimics glucagon action, implying that mitophagy of lipogenic mitochondria might be a new mechanism by which glucagon decreases lipogenesis. Understanding whether hepatic GCGR activation can selectively target lipogenic mitochondria for mitophagy would resolve the conundrum on how eliminating mitochondria, which oxidize fatty acids, can counteract steatosis.
Urolithin A induces mitophagy and prolongs lifespan in C. elegans and increases muscle function in rodents, 2016
The biological effects of urolithins remain poorly characterized, despite wide-spread human exposure via the dietary consumption of their metabolic precursors, the ellagitannins, which are found in the pomegranate fruit, as well as in nuts and berries. We identified urolithin A (UA) as a first-in-class natural compound that induces mitophagy both in vitro and in vivo following oral consumption. In C. elegans, UA prevented the accumulation of dysfunctional mitochondria with age and extended lifespan. Likewise, UA prolonged normal activity during aging in C. elegans, including mobility and pharyngeal pumping, while maintaining mitochondrial respiratory capacity. These effects translated to rodents, where UA improved exercise capacity in two different mouse models of age-related decline of muscle function, as well as in young rats. Our findings highlight the health benefits of urolithin A and its potential application in strategies to improve mitochondrial and muscle function.
Other JAK2/STAT3 Inhibitors
A 2015 paper scanned 2000 drugs and natural molecules to discover new JAK/STAT inhibitors. They came up with an interesting list (attached as txt and pdf). I quickly skimmed through. Found the following as the most interesting. Looks like Vit A in various forms suppress JAK/STAT. So does EPA. So does Hydrea :) (effect not as significant as top molecules). They have 4 "z scores" from 4 experiments, then the right-most number is their average.
Some human data regarding the top molecule they identified (METHOTREXATE): link.
01300027 IVERMECTIN 100122-04 B02 sample 70288-86-7 C48H74O14 875.11658 antiparasitic semisynthetic USP, INN, BAN Science 221:823 (1983); J Vet Pharmacol Ther 7:1 (1984) -9.09 -4.82 -3.73 -2.40 -5.01
01505444 METHYLENE BLUE 100122-12 B05 sample 7220-79-3 C16H20ClN3OS 337.8743 antimethemoglobinemic, cyanide antidote synthetic USP, INN, BAN -3.22 -3.83 -4.25 -2.67 -3.49
01503604 RETINYL PALMITATE 100122-10 E04 sample 79-81-2 C36H60O2 524.8784 provitamin, antixerophthalamic semisynthetic; Vitamin A palmitate USP, JAN -9.56 -0.62 -0.83 -0.54 -2.88
01503968 TACROLIMUS 100122-10 H02 sample 109581-93-3, 104987-11-3
[anhydrous]
C44H69NO12 804.04003 immune suppressant, antifungal Streptomyces tsukubaensis USAN, INN, BAN, JAN -9.14 -3.31 -3.47 -2.82 -4.68
01500398 METHOTREX
ATE(+/-) 100122-01 B06 sample 60388-53-6 C20H22N8O5 454.44894 antineoplastic, antirheumatic, folic acid antagonist synthetic; AMETHOPTERIN US
P, INN, BAN, JAN -8.26 -9.36 -8.49 -8.77 -8.72
01500679 AMINOPTERIN 100122-14 A10 sample 54-62-6, 58602-66-7
[aminopterin sodium]
C19H20N8O5 440.42185 antineoplastic, antirheumatic, folic acid antagonist synthetic; NSC-739 INN, BAN -6.65 -7.74 -7.80 -10.61 -8.20
00100009 CEDRELONE 100122-17 B09 sample 1254-85-9 C26H30O5 422.526 Cedrela species undetermined activity J Chem Soc 1963: 2506, 2515 -21.11 -9.87 -6.22 -3.16 -10.09
01504094 TENIPOSIDE 100122-03 C03 sample 29767-20-2 C32H32O13S 656.66804 antineoplastic semisynthetic USAN, INN, BAN -9.31 -11.19 -13.15 -12.42 -11.51
01505708 EPIRUBICIN HYDROCHLORIDE 100122-12 H02 sample 56390-09-1 C27H30ClNO11 579.99325 antineoplastic synthetic; IMI-28 USAN, INN, BAN, JAN -11.12 -16.09 -12.37 -5.86 -11.36
01503904 PATULIN 100122-18 C03 sample 149-29-1 C7H6O4 154.12347 antibacterial Aspergillus clavatus, Penicillium patulum experimental J Chem Soc 1944: 415 -13.10 -12.18 -8.02 -5.32 -9.65
01500835 URSOCHOLANIC ACID (BILE ACID) 100122-21 A04 sample 546-18-9 C24H40O2 360.5852 Abrus pecatorius undetermined activity Steroids 23:357 (1974) -12.11 -4.31 -2.60 -3.50 -5.63
00100005 ANTHOTHECOL 100122-17 B08 sample 10410-83-0 C28H32O7 480.56304 also as 11-ACETOXYCEDRELONE undetermined activity J Chem Soc 1963:983; 1970: 205; Nature 207:1101(1965) -16.35 -24.62 -23.30 -13.70 -19.49
01505483 DOXORUBICIN 100122-12 D03 sample 23214-92-8 C27H29NO11 543.53228 antineoplastic semisynthetic USAN, INN, BAN -7.58 -9.64 -6.87 -3.89 -6.99
01504412 PODOPHYLLIN ACETATE 100122-17 B06 sample 1180-34-3 C24H24O9 456.45348 derivative undetermined activity -8.29 -7.27 -9.07 -8.36 -8.25
01503076 QUINAPRIL HYDROCHLORIDE 100122-09 E10 sample 82586-55-8, 85441-61-8
[quinapril]
C25H31ClN2O5 474.98922 antihypertensive, ACE inhibitor synthetic USP, INN, BAN -8.06 -1.88 -0.42 -0.39 -2.69
01500143 beta-CAROTENE 100122-04 F02 sample 7235-40-7 C40H56 536.89232 provitamin A provitamin A; widespread in plants and animals USP, INN -7.36 -1.96 -1.78 -0.40 -2.87
01300030 OMEGA-3-ACID ESTERS (EPA shown) 100122-15 D02 sample 86227-47-6 C22H34O2 330.51508 hypolipidemic semisynthetic; K-85 USAN -5.26 -1.61 -1.50 -1.19 -2.39
01500344 HYDROXYUREA 100122-06 E06 sample 127-07-1 CH4N2O2 76.05523 antineoplastic, inhibits ribonucleoside diphosphate reductase synthetic USP, INN, BAN -4.05 -1.04 -2.79 -1.43 -2.32
01504300 ORLISTAT 100122-11 C02 sample 96829-58-2 C29H53NO5 495.74946 reversible lipase inhibitor, antiobesity synthetic USAN, INN, BAN -4.16 -3.71 -2.26 -1.68 -2.95
Methylene Blue as an Agent for Reducing Red Blood Cell Count
William B. Wendel, Martha Lou HefleyFirst Published May 1, 1934 Research Article
methylene blue may find practical application in the treatment of polycythemia Vera.
Effects of Omega-3 Fatty Acids on Lipid Profile and Anemia (link)
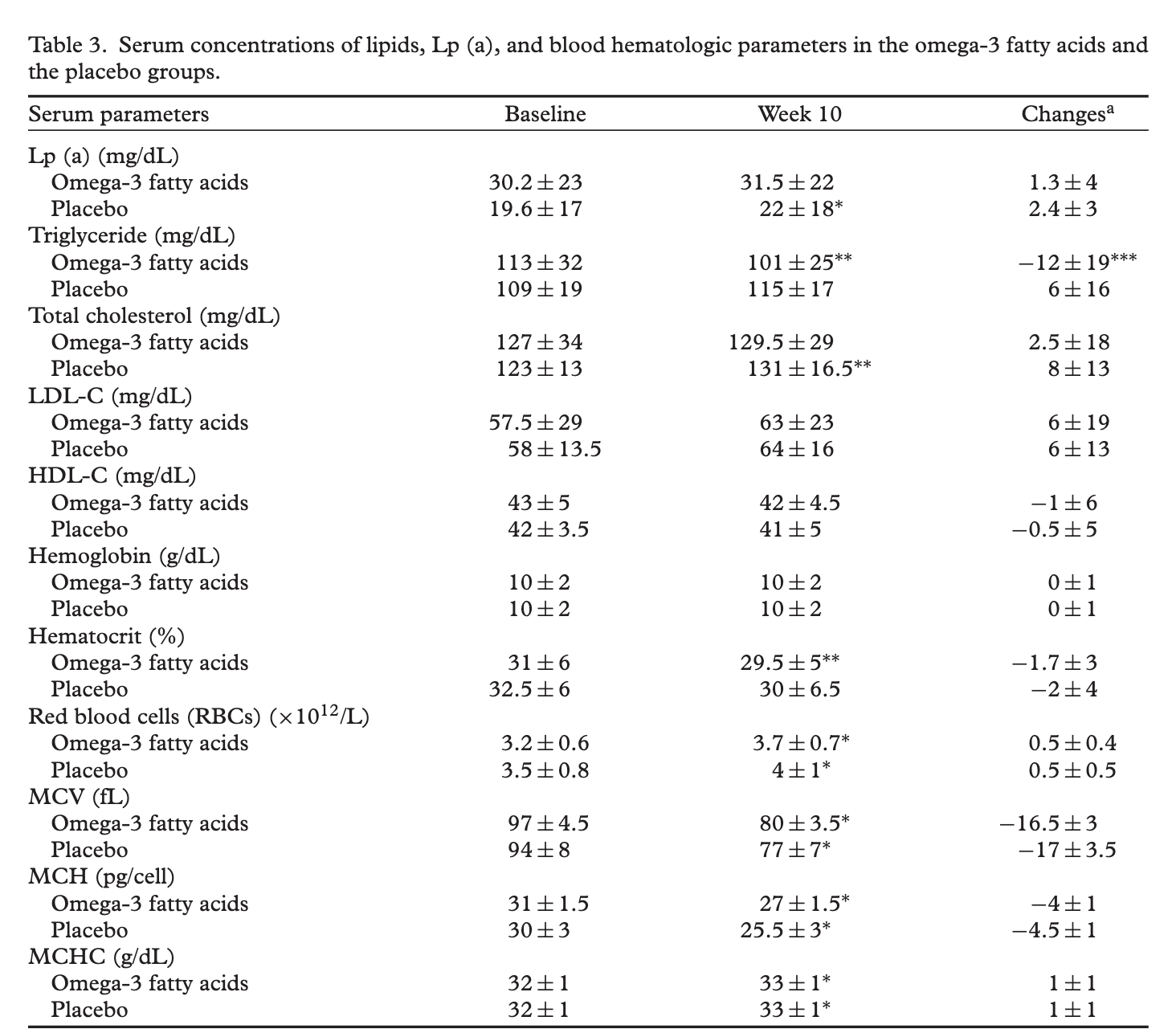
Liposome Delivery of Natural STAT3 Inhibitors for the Treatment of Cancer












All-trans Retinoic Acid
All-trans retinoic acid (ATRA) is a drug that can help treat acute promyelocytic leukemia (APL). ATRA is a retinoid, which is similar to vitamin A. It is not a chemotherapy drug, but it can be used with chemotherapy drugs to treat APL. ATRA can cause a short-term remission in at least 80% of patients. However, it cannot eliminate the leukemic clone and must be used in combination with anthracycline-based chemotherapy.
ATRA works by helping white blood cells mature into healthy white blood cells. It causes a marked decrease in the concentration of leukemic blast cells in the marrow. ATRA can induce complete remission in most patients with APL. However, the rates of overall survival at one, two, and three years after entry into a study were 75, 57, and 50. ATRA is taken as a capsule that you swallow.
Long-term molecular remission in promyelocytic transformation of myeloproliferative disease (1999)
12 weeks of all-trans retinoic acid (45 mg/m2 day) followed by two cycles of cytarabine 1 g/m2 days 1, 3, 5, 7, daunorubicin 50 mg/m2 days 1–3, and etoposide 75 mg/m2 days 1–7 achieved complete remission.
Decitabine combined with all-trans retinoic acid as treatment in a case of primary myelofibrosis transforming into acute myeloid leukaemia
Primary myelofibrosis (PMF) is a type of cloned myeloproliferative neoplasm stemming from haematopoietic stem cells, and tends to transform to acute myeloid leukaemia (AML) in approximately 10–20% of cases over a 10-year period. The transformation into AML has a poor prognosis, with a median overall survival of only 2.6 months in patients receiving supportive treatment. To date, treatment of AML transformation remains poor. The case of a 58-year-old female patient with AML transformed from PMF, who was treated with decitabine combined with all-trans retinoic acid, is reported. The patient had complete remission and a 17-month overall survival from initial diagnosis of transformed AML, with tolerated haematologic toxicity during the treatment period.
Rescue of a primary myelofibrosis model by retinoid-antagonist therapy
PNAS November 19, 2013 110 (47) 18820-18825;
Significance
Our work identifies a therapeutically tractable yet previously unrecognized repressive epigenetic feature of primary myelofibrosis that controls a key cytokine circuit in the bone marrow microenvironment. Though lacking previous clinical utility, we show that an orally active retinoic acid receptor antagonist can normalize thrombopoietin production, restore bone integrity, and dramatically reduce fibrosis. This identification of a pathway-specific drug for primary myelofibrosis opens up an avenue of treatment options and provides insight into the complex mechanisms underlying myelofibrosis.
Abstract
Molecular targeting of the two receptor interaction domains of the epigenetic repressor silencing mediator of retinoid and thyroid hormone receptors (SMRTmRID) produced a transplantable skeletal syndrome that reduced radial bone growth, increased numbers of bone-resorbing periosteal osteoclasts, and increased bone fracture risk. Furthermore, SMRTmRID mice develop spontaneous primary myelofibrosis, a chronic, usually idiopathic disorder characterized by progressive bone marrow fibrosis. Frequently linked to polycythemia vera and chronic myeloid leukemia, myelofibrosis displays high patient morbidity and mortality, and current treatment is mostly palliative. To decipher the etiology of this disease, we identified the thrombopoietin (Tpo) gene as a target of the SMRT–retinoic acid receptor signaling pathway in bone marrow stromal cells. Chronic induction of Tpo in SMRTmRID mice results in up-regulation of TGF-β and PDGF in megakaryocytes, uncontrolled proliferation of bone marrow reticular cells, and fibrosis of the marrow compartment. Of therapeutic relevance, we show that this syndrome can be rescued by retinoid antagonists, demonstrating that the physical interface between SMRT and retinoic acid receptor can be a potential therapeutic target to block primary myelofibrosis disease progression.
The combination of valproic acid, all-trans retinoic acid and low-dose cytarabine as disease-stabilizing treatment in acute myeloid leukemia (2013)
Background
A large proportion of patients with acute myeloid leukemia (AML) are not fit for intensive and potentially curative therapy due to advanced age or comorbidity. Previous studies have demonstrated that a subset of these patients can benefit from disease-stabilizing therapy based on all-trans retinoic acid (ATRA) and valproic acid. Even though complete hematological remission is only achieved for exceptional patients, a relatively large subset of patients respond to this treatment with stabilization of normal peripheral blood cell counts.
Methods
In this clinical study we investigated the efficiency and safety of combining (i) continuous administration of valproic acid with (ii) intermittent oral ATRA treatment (21.5 mg/m2 twice daily) for 14 days and low-dose cytarabine (10 mg/m2 daily) for 10 days administered subcutaneously. If cytarabine could not control hyperleukocytosis it was replaced by hydroxyurea or 6-mercaptopurin to keep the peripheral blood blast count below 50 × 109/L.
Results
The study included 36 AML patients (median age 77 years, range 48 to 90 years) unfit for conventional intensive chemotherapy; 11 patients responded to the treatment according to the myelodysplastic syndrome (MDS) response criteria and two of these responders achieved complete hematological remission. The most common response to treatment was increased and stabilized platelet counts. The responder patients had a median survival of 171 days (range 102 to > 574 days) and they could spend most of this time outside hospital, whereas the nonresponders had a median survival of 33 days (range 8 to 149 days). The valproic acid serum levels did not differ between responder and nonresponder patients and the treatment was associated with a decrease in the level of circulating regulatory T cells.
Conclusion
Treatment with continuous valproic acid and intermittent ATRA plus low-dose cytarabine has a low frequency of side effects and complete hematological remission is seen for a small minority of patients. However, disease stabilization is seen for a subset of AML patients unfit for conventional intensive chemotherapy.
FDA Approves Combo of Arsenic Trioxide and Tretinoin for acute promyelocytic leukemia (APL)
Jan 16, 2018 — The FDA approved a new first-line treatment combination for patients with newly diagnosed low-risk acute promyelocytic leukemia (APL).
Acute promyelocytic leukemia
Acute promyelocytic leukemia (APML, APL ) is a subtype of acute myeloid leukemia (AML), a cancer of the white blood cells.[1] In APL, there is an abnormal accumulation of immature granulocytes called promyelocytes. The disease is characterized by a chromosomal translocation involving the retinoic acid receptor alpha (RARα or RARA) gene and is distinguished from other forms of AML by its responsiveness to all-trans retinoic acid (ATRA; also known as tretinoin) therapy. Acute promyelocytic leukemia was first characterized in 1957[2][3] by French and Norwegian physicians as a hyperacute fatal illness,[1] with a median survival time of less than a week.[4] Today, prognoses have drastically improved; 10-year survival rates are estimated to be approximately 80-90% according to one study.[5][4][6]
Methotrexate
Methotrexate Is a JAK/STAT Pathway Inhibitor, 2015
The JAK/STAT pathway transduces signals from multiple cytokines and controls haematopoiesis, immunity and inflammation. In addition, pathological activation is seen in multiple malignancies including the myeloproliferative neoplasms (MPNs). Given this, drug development efforts have targeted the pathway with JAK inhibitors such as ruxolitinib. Although effective, high costs and side effects have limited its adoption. Thus, a need for effective low cost treatments remains.
Methods & Findings
We used the low-complexity Drosophila melanogaster pathway to screen for small molecules that modulate JAK/STAT signalling. This screen identified methotrexate and the closely related aminopterin as potent suppressors of STAT activation. We show that methotrexate suppresses human JAK/STAT signalling without affecting other phosphorylation-dependent pathways. Furthermore, methotrexate significantly reduces STAT5 phosphorylation in cells expressing JAK2 V617F, a mutation associated with most human MPNs. Methotrexate acts independently of dihydrofolate reductase (DHFR) and is comparable to the JAK1/2 inhibitor ruxolitinib. However, cells treated with methotrexate still retain their ability to respond to physiological levels of the ligand erythropoietin.
Conclusions
Aminopterin and methotrexate represent the first chemotherapy agents developed and act as competitive inhibitors of DHFR. Methotrexate is also widely used at low doses to treat inflammatory and immune-mediated conditions including rheumatoid arthritis. In this low-dose regime, folate supplements are given to mitigate side effects by bypassing the biochemical requirement for DHFR. Although independent of DHFR, the mechanism-of-action underlying the low-dose effects of methotrexate is unknown. Given that multiple pro-inflammatory cytokines signal through the pathway, we suggest that suppression of the JAK/STAT pathway is likely to be the principal anti-inflammatory and immunosuppressive mechanism-of-action of low-dose methotrexate. In addition, we suggest that patients with JAK/STAT-associated haematological malignancies may benefit from low-dose methotrexate treatments. While the JAK1/2 inhibitor ruxolitinib is effective, a £43,200 annual cost precludes widespread adoption. With an annual methotrexate cost of around £32, our findings represent an important development with significant future potential.
Low-dose methotrexate: potential clinical impact on haematological and constitutional symptoms in myeloproliferative neoplasms
https://onlinelibrary.wiley.com/doi/10.1111/bjh.16193
We recently identified low-dose methotrexate (MTX) as a JAK/STAT pathway inhibitor and have demonstrated its activity in humanised animal models of myeloproliferative neoplasms (MPNs) (Thomas et al, 2015; Chinnaiya et al, 2017). Here, we describe a retrospective service evaluation of 11 MPN patients treated with low-dose MTX for unrelated co-morbidities. Three showed haematological changes following initiation/interruption of MTX while standardised symptom assessments suggested that MTX-treated MPN patients suffer significantly decreased constitutional symptoms. Given the inflammatory nature of MPN symptoms we suggest that low-dose MTX may represent a low cost, safe and effective treatment for the wider MPN population and propose further studies to test this hypothesis.
Mutations that constitutively activate JAK/STAT signalling represent key drivers of MPNs and, consequently, pathway inhibitors, such as ruxolitinib, have been developed and licenced (Quintás-Cardama & Verstovsek, 2013). Previously identified as a JAK/STAT pathway inhibitor with efficacy in mouse MPN models (Thomas et al, 2015; Chinnaiya et al, 2017), the low cost, generic drug MTX is generally well tolerated with a favourable risk profile (Shinde et al, 2014).
CBD Oil for MPN
JESSICA HARSHBARGER - Essential Thrombocythemia (ET) (link)
In 2018 while working at the dispensary Jessica met a medical cannabis patient who was having phenomenal results shrinking her brain tumor using a high concentration of CBD oil. Jessica thought that this might, in fact, help with her high platelets. At the time she had been taking high doses of THC for two years but didn’t feel well, and her platelet counts weren’t dropping as much as she had originally hoped, so she changed her combination to 8 parts CBC and 1 part THC. “I believe the more CBD I take the better my CBC tests are coming out,” she says. Since she began taking high doses of CBD in early 2018 her platelets have dropped from the 800-900 range to the 500-600 range. Dr. Mauricio Consaulter, Jessica’s internal medicine doctor, who originally helped Jessica gain access to medical cannabis discussed the possibility of publishing her favorable results.
Mebendazole/Ivermectin
Mebendazole exhibits potent anti-leukemia activity on acute myeloid leukemia
2018
Acute myeloid leukemia (AML) is one of the most common types of acute leukemia in adults with the lowest survival rate of all leukemia. Resistance to cytarabine and anthracycline-based chemotherapy is a major cause of treatment failure. Thus, finding new drugs with anti-leukemia activities and minimal side effect is urgently needed. Here through screening more than 1000 drugs approved by the Food and Drug Administration (FDA) of United States, the anthelmintic drug mebendazole (MBZ) was found to inhibit the growth of AML cell lines (THP-1, U937, NB4 and K562) and bone marrow mononuclear cells (BM-MNCs) from AML patients at pharmacologically achievable concentrations. In contrast, similar concentration of MBZ had little inhibitory effect on the growth of normal peripheral blood mononuclear cells (PBMC) or human umbilical vein endothelial cells (HUVEC). In addition, MBZ induced mitotic arrest and mitotic catastrophe in AML cells based on nuclear morphology, cell cycle distribution, mitotic marker analyses and the number of multinucleated cells and apoptotic cells. Furthermore, MBZ treatment inhibited activation of Akt and Erk in AML leukemic cells. Finally, MBZ repressed the progression of leukemic cells in vivo and prolonged survival in AML xenograft mouse model. Taken together, our results suggest that MBZ could be a potential new therapeutic agent for the treatment of AML patients.
Mebendazole Mediates Its Anti-Leukemic Effects By Proteasomal Degradation of GLI Transcription Factors Via Inhibition of HSP70/90-Chaperone Activity in Acute Myeloid Leukemia in a Preclinical and Clinical Setting, 2019
Aberrant activation of hedgehog signaling (HH) is associated with a wide variety of neoplasms, including acute myeloid leukemia (AML). The GLI transcription factors are the main downstream effectors of the HH signaling cascade and play a fundamental role in cancer development, progression and maintenance of leukemic stem cells, which are responsible for therapy failure and tumor relapse due to their resistance to chemotherapy. Moreover, the GLI transcription factors represent central hubs in oncogenic signaling and thus are an attractive therapeutic target for anti-cancer therapy. However non-canonical GLI activation by multiple oncogenic signaling pathways limit the use of SMO inhibitors, while treatment strategies directly targeting the GLI transcription factors are limited. Mebendazole (MBZ) is a commonly used anthelmintic drug with a favorable toxicity profile. MBZ has been shown to exhibit strong anti-tumor effects in different cancer entities, including AML.
We treated AML cell lines and primary AML samples with different MBZ concentrations and could show a dose-dependent effect on the proliferation, colony formation and apoptosis in AML cells. In addition, therapeutic synergy between cytarabine and MBZ was demonstrated in OCI-AML3 cells with a combination index <1 and a dose reduction index (DRI) of 2.5- to 23.0-fold. GLI1 and -2 protein levels were clearly reduced in AML cell lines 24h after MBZ exposure, whereas mRNA levels did not decrease. To study the functional activity of GLI transcription factors, we transduced various AML cell lines with a construct where luciferase expression is under the control of the GLI promoter. MBZ strongly inhibited GLI signaling activity in a dose-dependent manner. Furthermore, inhibiting the 26s proteasome with bortezomib partly abolished the effect of MBZ on GLI1 and -2 protein levels and GLI activity, indicating that MBZ promotes their proteasomal degradation. The HSP70/HSP90-based chaperone machinery stabilizes a spectrum of client substrates for protein folding, including transcription factors. Inhibition of either HSP90 or HSP70 with small-molecule inhibitors VER-155008 and PU-H71 resulted in markedly reduction of GLI1 and -2 protein levels in Western Blots. Next, we investigated the impact of MBZ on HSP70/HSP90-mediated refolding of the heat-denatured firefly luciferase. In cell-lines constitutively expressing a firefly luciferase, the luciferase signal was recovered without inhibitor following a heat-shock, but incubation of AML cells with MBZ or specific HSP inhibitors impaired recovery of the signal, suggesting strong inhibition of HSP70/90-mediated luciferase refolding. This indicates that the anti-leukemic activity of MBZ is at least partly mediated through GLI protein destabilization by inhibition of cooperative HSP70/HSP90-chaperone activity. This is further supported by our observation that MBZ activates HSF-1, a major regulator of the heat shock pathway. MBZ may address additional pathways by HSP70/HSP90 inhibition such as FLT3-ITD, MYB or MYC degradation and inactivation of ERK and AKT as shown by us and others.
To further evaluate if MBZ is a suitable GLI inhibitor in clinical practice, we transferred these findings into the clinical setting by treating two patients with refractory AML with MBZ monotherapy in an off-label setting. We demonstrated an effective MBZ concentration in the plasma using a modified plasma inhibitory assay (PIA) by incubating an indicator cell lines carrying the GLI luciferase promoter transgene with the patient's plasma. In one patient, a clear continuous decrease in leukemic blasts in peripheral blood was noted. In this patient a reduction in the luciferase activity in the PIA assay and a fast reduction in GLI2 levels in peripheral leukemic blood were detected. Moreover, a healthy volunteer ingested MBZ at a dose of 50 mg/kg divided in two doses at time 0h and 12h. Blood was drawn at 4h and at 24h. PIA results indicated a biological active plasma concentration.
Taken together, our results demonstrate that MBZ functions as an effective GLI inhibitor with strong anti-leukemic activity in a clinical setting and encourage for further studies to translate the scientific findings into clinical practice. A clinical study of mebendazole plus low dose cytarabine in patients with refractory AML is planned.
Repurposing anthelmintic agents to eradicate resistant leukemia, 2020
Despite rapid progress in genomic profiling in acute lymphoblastic leukemia (ALL), identification of actionable targets and prediction of response to drugs remains challenging. To identify specific vulnerabilities in ALL, we performed a drug screen using primary human ALL samples cultured in a model of the bone marrow microenvironment combined with high content image analysis. Among the 2487 FDA-approved compounds tested, anthelmintic agents of the class of macrocyclic lactones exhibited potent anti-leukemia activity, similar to the already known anti-leukemia agents currently used in induction chemotherapy. Ex vivo validation in 55 primary ALL samples of both precursor B cell and T-ALL including refractory relapse cases confirmed strong anti-leukemia activity with IC50 values in the low micromolar range. Anthelmintic agents increased intracellular chloride levels in primary leukemia cells, inducing mitochondrial outer membrane depolarization and cell death. Supporting the notion that simultaneously targeting cell death machineries at different angles may enhance the cell death response, combination of anthelmintic agents with the BCL-2 antagonist navitoclax or with the chemotherapeutic agent dexamethasone showed synergistic activity in primary ALL. These data reveal anti-leukemia activity of anthelmintic agents and support exploiting drug repurposing strategies to identify so far unrecognized anti-cancer agents with potential to eradicate even refractory leukemia.
Repurposing Drugs for Acute Myeloid Leukemia: A Worthy Cause or a Futile Pursuit?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7072462/
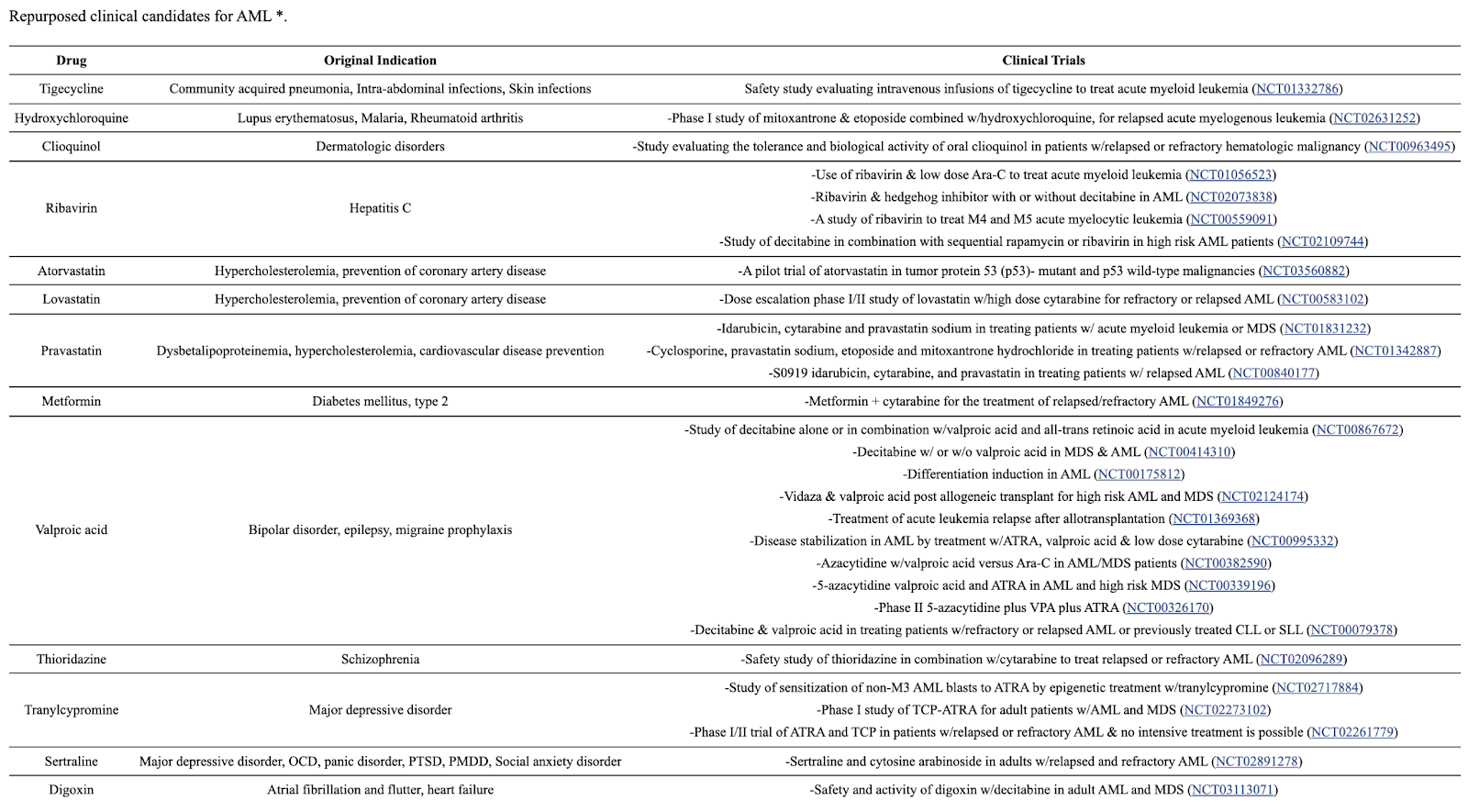
Other Topics
How to eliminate senescent blood cancer cells?
Senolytic drugs - Experimental compounds like navitoclax, dasatinib, quercetin, and fisetin have shown ability to selectively induce apoptosis in senescent and cancer cells while sparing healthy cells. Their efficacy against blood cancers needs more research.
Targeting cell survival pathways - Inhibiting pro-survival signaling pathways like Bcl-2, mTOR, NF-kB that maintain senescent cells may help eliminate them.
CAR-T cell therapy - T cells genetically engineered to target CD19, BCMA and other antigens on cancer cells can potentially also target senescent markers to eliminate exhausted, dysfunctional T cells.
Epigenetic modulators - Drugs targeting epigenetic alterations and cell reprogramming may be able to shift senescent cancer cells into a proliferative state to regain chemosensitivity.
Immunotherapy - Checkpoint inhibitor drugs help revive anti-tumor immune responses. Combining these with senolytics may boost cancer and senescent cell clearance.
Exercise and fasting - These stressors may selectively induce apoptosis of senescent cells through metabolic modulation. Effects against blood cancer need study.
Photodynamic therapy - Photosensitizers concentrate in cancer cells then react to light to create oxidants that induce cell death. Could target senescent forms.
Further research into senescent cell biology may uncover more specific vulnerabilities to exploit. Combination therapies will likely be needed to effectively clear senescent blood cancer cells.
Rhodiola inhibits JAK2/STAT3
Anticancer effect of salidroside on colon cancer through inhibiting JAK2/STAT3 signaling pathway, 2015
Salidroside is considered to have anti-tumor properties. We investigate its effects on colon carcinoma SW1116 cells. Cell viability was assessed by CCK-8. Propidium iodide (PI) staining was used to determine the cell cycle by flow cytometry. The migration and invasion were detected by Transwell. Western blot was used to detect the expression of STAT3 signal related proteins. As the result, high concentrations of salidroside (10, 20. 50 μg/ml) significantly inhibited proliferation of SW1116 cells in a parallelly, cell cycle arrest was increased at the G0/G1 phase after salidroside treatment. Furthermore, salidroside inhibited migration and invasion of SW1116 cells. Salidroside treatment decreased proteins expression of phosphorylation levels in JAK2/STAT3 signaling, while MMP-2 and MMP-9 proteins levels were decreased and protein expression of VEGF and VEGFR-2 were down-regulated. In Conclusion, salidroside inhibited proliferation, decreased the migration and invasion of SW1116 cells in JAK2/STAT3-dependent pathway, the specific mechanisms need further study.
Pulmonary Hypertension (common in MPNs)
Pulmonary hypertension diagnosis
Here are some key points about the diagnosis of pulmonary hypertension:
Pulmonary hypertension is defined as a mean pulmonary arterial pressure (mPAP) ≥25 mmHg at rest measured by right heart catheterization. This invasive procedure is required for definitive diagnosis.
Symptoms of pulmonary hypertension are nonspecific and can include shortness of breath, fatigue, chest pain, dizziness, and fainting episodes. However, symptoms may not appear until the disease has progressed.
During the initial workup, a transthoracic echocardiogram is often used as a screening test. Findings suggestive of pulmonary hypertension include an elevated tricuspid regurgitant jet velocity and enlarged right ventricle.
Other tests that may be used to help diagnose pulmonary hypertension include pulmonary function tests, chest x-ray, CT scan of the chest, ventilation/perfusion scan, 6-minute walk test, and blood tests.
The cause of pulmonary hypertension guides treatment. Common causes include left heart disease, lung disease, chronic thromboembolic pulmonary hypertension, and idiopathic pulmonary arterial hypertension. Additional testing can help determine the underlying cause.
Right heart catheterization allows direct measurement of pulmonary artery pressures and is required to confirm the diagnosis of pulmonary hypertension. It can also assess the severity of disease and response to treatment.
Pulmonary hypertension is diagnosed when the mPAP is ≥25 mmHg at rest or ≥30 mmHg with exercise. Precapillary pulmonary hypertension is present when pulmonary artery wedge pressure is ≤15 mmHg.
In summary, diagnosis requires a comprehensive workup including screening tests like echocardiogram and definitive confirmation via right heart catheterization, along with tests to identify the underlying cause. Early diagnosis is important to guide appropriate treatment and management.
Pulmonary hypertension in patients with chronic myeloproliferative disorders (2015)
Pulmonary hypertension (PH) is a known complication of chronic myeloproliferative disorders (CMPDs). CMPDs associated with PH are classified as Group 5 PH, meaning the mechanism is multifactorial or unclear. This review discusses the epidemiology, pathogenesis, and treatment of the main types of PH in CMPDs: chronic thromboembolic PH (CTEPH), precapillary PH, and drug-induced PH.
Epidemiology:
The prevalence of PH in CMPDs is not well established but seems to range from 13-48% based on echocardiographic studies. Right heart catheterization is required for definitive diagnosis.
CTEPH may manifest concurrently with a new CMPD diagnosis. Precapillary PH arises later, on average 8-13 years after CMPD diagnosis.
Polycythemia vera and essential thrombocythemia have the strongest association with PH. Factors like platelet count, hematocrit, and splenectomy may increase risk.
CTEPH Pathogenesis:
Thrombophilic state in CMPDs leads to increased risk of arterial and venous clots. Mechanisms include blood hyperviscosity, abnormal RBCs, spontaneous platelet activation, presence of JAK2 mutation.
Splenectomy is a risk factor, likely due to loss of filtering function and worsening extramedullary hematopoiesis.
Elevated hematocrit correlates with CTEPH compared to precapillary PH.
CTEPH Treatment:
Pulmonary endarterectomy is first-line. Medical therapy (diuretics, anticoagulants, PAH-specific drugs) may help inoperable cases. Small studies show benefit from endothelin receptor antagonists like bosentan.
Cytoreductive drugs like hydroxyurea may reduce risk of clots by lowering cell counts. Antiplatelet role is controversial.
Precapillary PH Pathogenesis:
Due to multiple factors: portal hypertension, pulmonary veno-occlusive disease from chemotherapy, tumor microembolism of megakaryocytes, extramedullary hematopoiesis, enhanced angiogenesis.
Megakaryocyte occlusion of pulmonary vasculature may occur, especially in myelofibrosis. Platelets implicated through growth factor release.
Relationship to JAK2 mutation unclear.
Precapillary PH Treatment:
No proven effective therapies. Case reports of benefit with cytoreductive drugs, radiotherapy, JAK inhibitors like ruxolitinib. However, worsening PH also reported with ruxolitinib.
Role of anticoagulants, PAH-specific vasodilators remains unclear.
Drug-Induced PH:
Tyrosine kinase inhibitors for CML like dasatinib can cause PH, with onset typically after months/years. Imatinib may improve PH.
Prognosis:
Precapillary PH has poor prognosis with median survival of months after diagnosis. CTEPH prognosis better if pulmonary endarterectomy is an option.
In summary, PH is an important complication of CMPDs that manifests through various mechanisms. More research is needed to clarify epidemiology, improve early diagnosis, and establish effective treatments. Collaboration between hematologists and PH experts is key to optimizing outcomes in this population.
Pulmonary hypertension symptoms
Symptoms are often nonspecific, especially early in the disease, and may mimic other common conditions. Many patients are diagnosed late.
The most common symptom is shortness of breath, especially with exertion. Fatigue and weakness are also very common.
As pulmonary hypertension advances, shortness of breath may occur at rest along with fatigue. Chest pain and dizziness may also develop.
Other symptoms may include swelling in the ankles and legs, bluish lips and skin, racing heartbeat or palpitations, and fainting episodes.
Symptoms tend to worsen over time as the right side of the heart strains to pump against the high pressure and eventually fails.
Severity of symptoms does not always correlate with the degree of pulmonary hypertension. Some patients have severe PH but mild symptoms, while others have moderate PH and more severe symptoms.
Symptoms are caused by the high pulmonary pressures making the right ventricle work harder, and the eventual right heart failure this leads to.
Exertional dyspnea and fatigue are hallmark early symptoms. As disease advances, shortness of breath occurs at rest along with other symptoms of right heart failure.
Because symptoms mimic many other conditions, a high index of suspicion, risk factor assessment, and echocardiogram are needed for prompt diagnosis.
Pulmonary hypertension in polycythemia vera
Polycythemia vera is a chronic myeloproliferative neoplasm that can be associated with pulmonary hypertension.
The hyperviscosity and increased red cell mass in polycythemia vera leads to abnormal blood flow and increases risk of thrombosis. This predisposes to development of chronic thromboembolic pulmonary hypertension (CTEPH).
CTEPH is one of the most frequent types of pulmonary hypertension seen in polycythemia vera. It results from chronic organized thromboemboli that obstruct the pulmonary arteries.
Polycythemia vera also creates a pro-thrombotic state through increased platelet activation, leukocyte activation, and presence of JAK2 mutations. This further increases risk of CTEPH.
Precapillary pulmonary hypertension can also develop, thought to be related to high hematocrit/hyperviscosity or through extramedullary hematopoiesis and pulmonary myeloid metaplasia.
Pulmonary hypertension in polycythemia vera tends to develop later in the disease course, on average about 8-13 years after diagnosis.
Treatment focuses on pulmonary endarterectomy for CTEPH when possible. PAH-specific medications may be tried for inoperable CTEPH or precapillary PH.
Cytoreductive therapies like hydroxyurea and phlebotomy may help lower risk of pulmonary hypertension development.
In summary, the hyperviscosity and thrombotic state of polycythemia vera significantly increase the risk of developing both chronic thromboembolic and precapillary pulmonary hypertension through several mechanisms. Close monitoring for signs of pulmonary hypertension is important in management.
Pulmonary Arterial Hypertension in Hospitalized Patients With Polycythemia Vera (from the National Inpatient Database (2021)
The prevalence and pathophysiology of pulmonary arterial hypertension (PAH) in myeloproliferative neoplasms are poorly understood and have not been evaluated on larger scale studies. These reports generally focus on all myeloproliferative neoplasms rather than each disease individually. We aim to establish the prevalence and association of PAH in patients with polycythemia vera (P. vera) using the Nationwide Inpatient Sample database. We identified 38,395 patients with a discharge diagnosis of P. vera and 39,395,521 patients without P. vera. Both groups were queried for a concomitant discharge diagnosis of PAH. Unadjusted and multivariate adjusted logistic regression analyses were performed to determine if presence of P. vera predicted PAH after adjusting for clinically relevant risk factors. The prevalence of P. vera was 0.1% of all hospital discharge records. Pulmonary arterial hypertension was more prevalent in patients with P. vera compared with the control population (7.9% vs 1.9%, p <0.0001). Presence of P. vera was a determinant of PAH in unadjusted analysis (odds ratio 4.4 [4.1 to 4.8]; p <0.001). After adjusting for age, gender, race, diabetes, tobacco use, previous history of tumor, previous history of pulmonary embolism, chronic lung disease, and chronic kidney disease, P. vera was associated with nearly a 3-fold higher risk for PAH after adjusting for several risk factors (2.98 [2.7 to 3.2], p <0.001).
Randomized Clinical Trial of Aspirin and Simvastatin for Pulmonary Arterial Hypertension
ASA-STAT (2011)
Background
Pulmonary arterial hypertension (PAH) is a progressive disease that causes exercise limitation, heart failure, and death. We aimed to determine the safety and efficacy of aspirin and simvastatin in PAH.
Methods and Results
We performed a randomized, double-blind, placebo-controlled 2×2 factorial clinical trial of aspirin and simvastatin in patients with PAH receiving background therapy at 4 centers. A total of 92 patients with PAH were to be randomized to aspirin 81 mg or matching placebo and simvastatin 40 mg or matching placebo. The primary outcome was 6-minute walk distance at 6 months. Sixty-five subjects had been randomized when the trial was terminated by the Data Safety and Monitoring Board after an interim analysis showed futility in reaching the primary end point for simvastatin. After adjustment for baseline 6-minute walk distance, there was no significant difference in the 6-minute walk distance at 6 months between aspirin (n=32) and placebo (n=33; placebo-corrected difference −0.5 m, 95% confidence interval −28.4 to 27.4 m; P=0.97) or between simvastatin (n=32) and placebo (n=33; placebo-corrected difference −27.6 m, 95% confidence interval −59.6 to 4.3 m; P=0.09). There tended to be more major bleeding episodes with aspirin than with placebo (4 events versus 1 event, respectively; P=0.17).
Conclusions
Neither aspirin nor simvastatin had a significant effect on the 6-minute walk distance, although patients randomized to simvastatin tended to have a lower 6-minute walk distance at 6 months. These results do not support the routine treatment of patients with PAH with these medications.
Pulmonary Arterial Hypertension drugs
Here is an overview of the major drugs used to treat pulmonary arterial hypertension (PAH):
Prostacyclin analogs (e.g. epoprostenol, treprostinil, iloprost) - Vasodilators that inhibit platelet aggregation. Can be given intravenously, subcutaneously, or inhaled.
Endothelin receptor antagonists (e.g. bosentan, ambrisentan, macitentan) - Block endothelin-1 mediated vasoconstriction. Given orally.
Phosphodiesterase type 5 inhibitors (e.g. sildenafil, tadalafil) - Increase cGMP leading to vasodilation. Given orally.
Guanylate cyclase stimulators (e.g. riociguat) - Increase cGMP production. Given orally.
Calcium channel blockers (e.g. amlodipine, diltiazem) - Vasodilators sometimes used for PAH but limited efficacy.
Soluble guanylate cyclase stimulators (e.g. vericiguat) - Increase cGMP production. Given orally.
Prostacyclin receptor agonists (e.g. selexipag) - Activate prostacyclin pathway. Given orally.
Rho kinase inhibitors (e.g. fasudil) - Vasodilator. Given intravenously.
Goals of treatment include improving exercise tolerance, functional status, and hemodynamics. Combination therapy is frequently used. Supportive care like diuretics and oxygen are also important. Lung transplant may be considered for severe disease. The prognosis of PAH has improved significantly with newer medical therapies.
Epstein-Barr (EBV) present in Bone Marrow
Presence of Epstein-Barr virus genome in the bone marrow of patients with hematopoietic malignancies (link)
https://sci-hub.se/10.1159/000203558
<EBV is known to cause many cancers (e.g. Lymphoma).>
"Viral repeated sequences were detected in 42 of 82 (51%) hematopoietic malignancies, including polycythemia vera, but not in nonneoplastic cases. These results suggest that a novel form of EBV latent infection is present in the bone marrow of patients with hematopoietic malignancies."
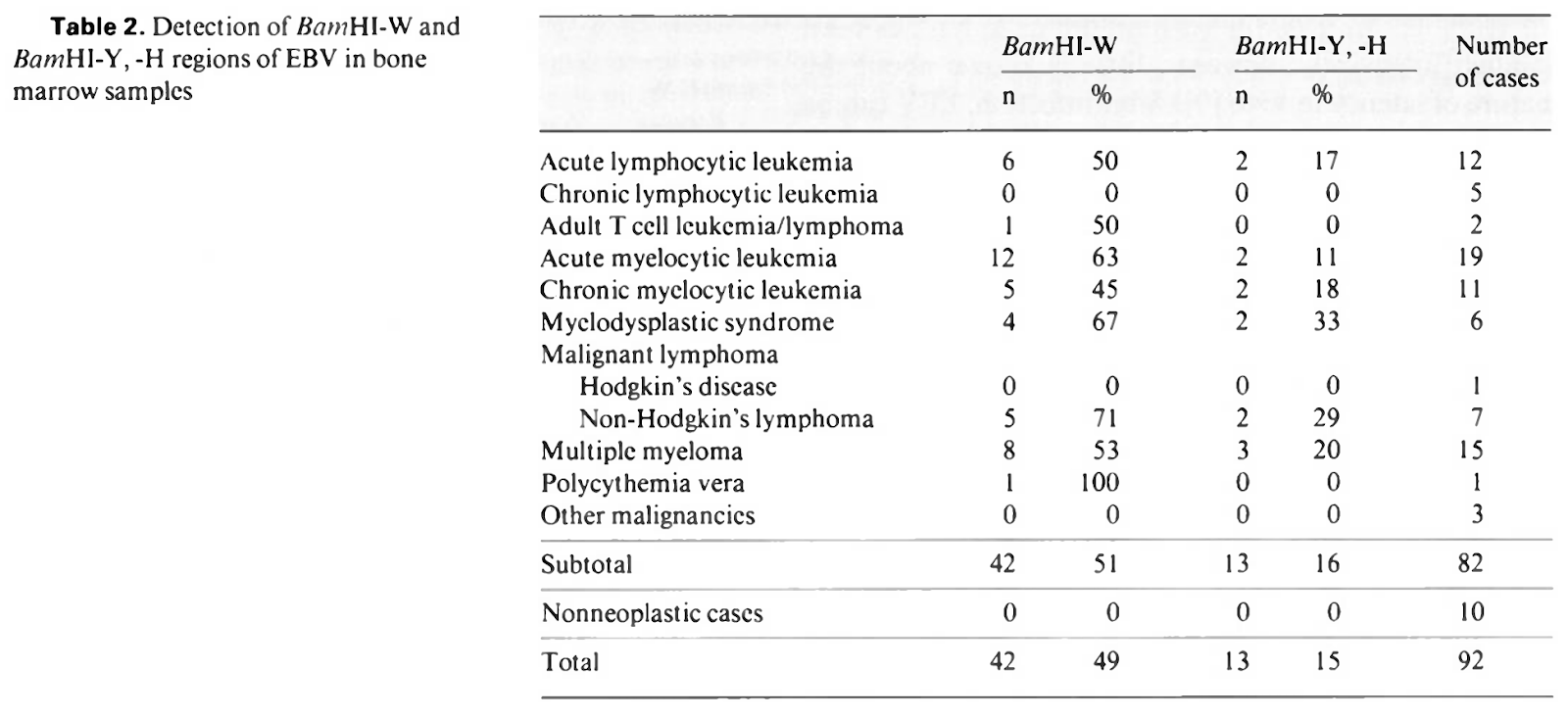
Epstein-Barr virus subverts mevalonate and fatty acid pathways to promote infected B-cell proliferation and survival
Epstein-Barr virus (EBV) causes infectious mononucleosis and is associated with multiple human malignancies. EBV drives B-cell proliferation, which contributes to the pathogenesis of multiple lymphomas. Yet, knowledge of how EBV subverts host biosynthetic pathways to transform resting lymphocytes into activated lymphoblasts remains incomplete. Using a temporal proteomic dataset of EBV primary human B-cell infection, we identified that cholesterol and fatty acid biosynthetic pathways were amongst the most highly EBV induced. Epstein-Barr nuclear antigen 2 (EBNA2), sterol response element binding protein (SREBP) and MYC each had important roles in cholesterol and fatty acid pathway induction. Unexpectedly, HMG-CoA reductase inhibitor chemical epistasis experiments revealed that mevalonate pathway production of geranylgeranyl pyrophosphate (GGPP), rather than cholesterol, was necessary for EBV-driven B-cell outgrowth, perhaps because EBV upregulated the low-density lipoprotein receptor in newly infected cells for cholesterol uptake. Chemical and CRISPR genetic analyses highlighted downstream GGPP roles in EBV-infected cell small G protein Rab activation. Rab13 was highly EBV-induced in an EBNA3-dependent manner and served as a chaperone critical for latent membrane protein (LMP) 1 and 2A trafficking and target gene activation in newly infected and in lymphoblastoid B-cells. Collectively, these studies identify highlight multiple potential therapeutic targets for prevention of EBV-transformed B-cell growth and survival.
Numerous drugs inhibit Epstein-Barr virus replication in vitro. These include acyclovir, desciclovir, ganciclovir, interferon-alfa, interferon-gamma, adenine arabinoside, and phosphonoacetic acid. (link)
Curbing Lipids: Impacts ON Cancer and Viral Infection (link)
Simvastatin induces apoptosis of Epstein-Barr virus (EBV)-transformed lymphoblastoid cell lines and delays development of EBV lymphomas (2004)
HMG CoA reductase inhibitors (statins) to treat Epstein–Barr virus-driven lymphoma (link)
STATIN USE AND PROGNOSIS IN 12,865 NON-HODGKIN LYMPHOMA PATIENTS TREATED IN THE RITUXIMAB-ERA
Results: Among 12,865 NHL patients (4,166 diffuse large B-cell, DLBCL, 1,765 FL, 772 mantle cell, MCL, 772 marginal zone, MZL, 131 Burkitt, 922 T- and NK-cell and 4,337 discordant or other lymphomas), 19% used statins at diagnosis. At end of follow-up (Sept 2013), 2,731 (21%) had died from lymphoma. We found no association between statin use and lymphoma-specific mortality for NHL overall, adjusted HR 0.94 (0.85, 1.04) or its subtypes (DLBCL 1.00 (0.86, 1,16), treated FL1.30 (0.81, 2.10), FL “watch and wait” 1.53 (0.74, 3.13), MCL 0.91 (0.62, 1.32), MZL 0.49 (0.22, 1.09), T- and NK-cell 0.92 (0.65, 1.30), discordant or other lymphomas 0.99 (0.80, 1.23)). However, for Burkitt lymphoma, we found a statistically significant decreased lymphoma-specific mortality, adjusted HR 0.09 (0.01, 0.64). Further dose-response analyses are planned.
Conclusions: In this very large population-based unselected lymphoma population, statins were not associated with worse outcomes and thus appear safe to use during lymphoma treatment. Interestingly, Burkitt patients using statins had a statistically significant decreased lymphoma-specific mortality.
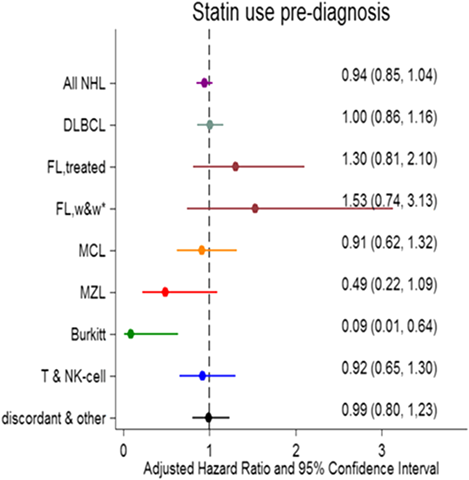
Aspirin induces lytic cytotoxicity in Epstein-Barr virus-positive cells (2008)
Epstein–Barr virus RNA confers resistance to interferon-α-induced apoptosis in Burkitt's lymphoma (2002)
Risk Factors for Ganciclovir-Induced Thrombocytopenia and Leukopenia (2015)
A yeast-based assay identifies drugs that interfere with immune evasion of the Epstein-Barr virus (2014)
Niacin May Lower Blood Counts
Correction of refractory thrombocytopenia and anemia following withdrawal of extended release niacin
Niacin (Niaspan, Nicotinic acid, Vitamin B3) is an FDA-approved water-soluble vitamin known to reduce serum LDL and triglycerides while boosting HDL. Cutaneous flushing is the most common dose-limiting adverse reaction but other effects, including thrombocytopenia, are documented. FDA prescribing literature states that extended-release (ER) niacin (Niaspan, Abbott Laboratories) is associated with a “statistically significant dose-dependent reduction in platelet counts, with an average drop of −11% on a dose of 2,000 mg/day” 1. In a study reported by Kei and Elisaf, 50 patients with hyperlipidemia undergoing statin therapy experienced a 20% reduction in platelet counts when niacin-ER was added at a starting dose of 1,000 mg/day and titrated to 2,000 mg/day for a period of 3 months 2. Here, we report four patients, evaluated in our clinical practice from 2012 to 2015, in whom long-term treatment with niacin-ER was associated with a progressive and reversible thrombocytopenia.
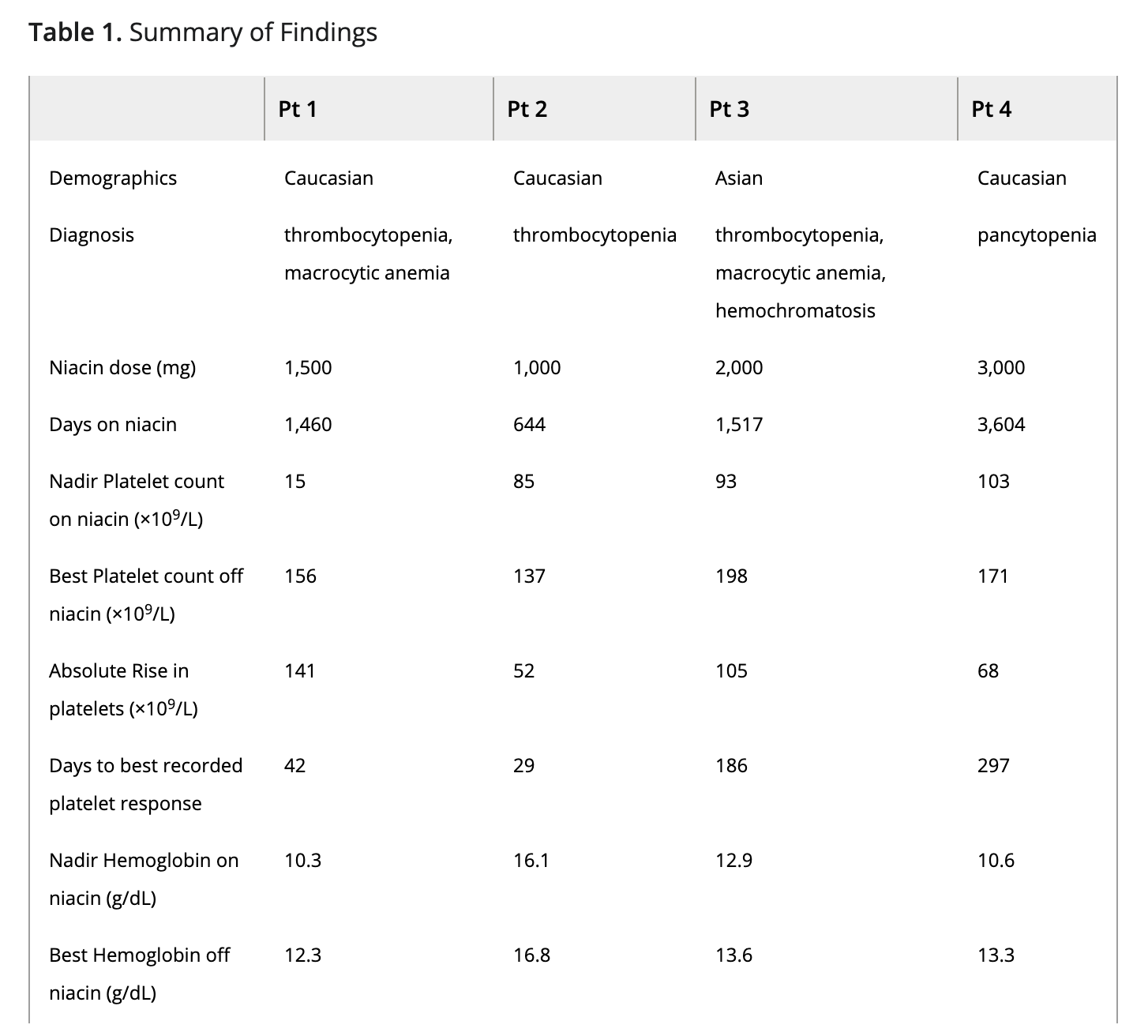
(Niacin suppressed Hemoglobin as well)
Antiatherothrombotic effects of nicotinic acid, 2003
Cardiovascular event reduction in hypercholesterolemic subjects appropriately emphasizes the prominent role of statin therapy; however, niacin (nicotinic acid) is also an effective lipid-altering agent that prevents atherosclerosis and reduces cardiovascular events. Niacin has multifarious lipoprotein and anti-atherothrombosis effects that improve endothelial function, reduce inflammation, increase plaque stability, and diminish thrombosis. Niacin reduces the atherogenicity of low-density lipoprotein (LDL) by changing the distribution of small LDL to large LDL subclass, and the susceptibility of LDL to oxidative modification. It is the most effective agent for increasing high-density lipoprotein cholesterol. Moreover, it favorably alters high-density lipoprotein composition, increasing apolipoprotein AI relative to apolipoprotein AII. Niacin reduces blood viscosity through a variety of mechanisms, thus improving blood flow and perfusion through stenotic segments of the vasculature. Finally, niacin has cardioprotective effects that may limit ischemia-reperfusion injury. By preserving glycolysis during periods of ischemia and improving subendocardial blood flow during reperfusion, niacin can improve the functional recovery of the myocardium.
Does Aspartame cause blood cancer?
Aspartame and cancer – new evidence for causation
There is a statistically significant increase in incidence of all hematolymphatic malignancies (p = 0.006), including significant increases in both lymphomas (p = 0.032) and leukemias (p = 0.031). in rodents exposed to aspartame;
The finding of increased HLTs in animals exposed to aspartame at a dose of 100 mg/Kg body weight is of great concern. This is a relatively low-dose exposure - dangerously close to the current Acceptable Daily Intake (ADI) levels for aspartame established by regulatory agencies in the European Union [8, 9] and the United States [10]. In large populations, significant numbers of persons frequently consume food ingredients, aspartame included, at levels exceeding ADIs. Such exceedances are especially common among infants and young children because of their greater food intake per Kg body weight compared to adults and their unusual dietary patterns [11]. The implication of this finding is that current ADI levels for aspartame may be set too high and may not offer sufficient protection against cancer. ADI levels for aspartame need urgently to be reevaluated, especially as they apply to pregnant women and young children.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8042911/
Comprehensive Blood Testing for MPNs
Inflammation & insulin resistance
Omega 3
Nutrient levels test
Bacteria and viruses test
Toxin test
Growth: Insulin, IGF1
Inflammation: HS-CRP, IL6, TNF-Alpha, ESR
Nutrients: B12, Folate, Vit D, Ferritin
Cholesterol: ApoB
Oxidation: GGT, Urinary Malondialdehyde (link), erythrocyte superoxide dismutase (SOD), catalase (CAT), glutathione (GSH), glutathione peroxidase (GPx), and glutathione S-transferase (GST)
Omega 3 finger stick test
Insulin - $29.90
https://www.lifeextension.com/search#q=Insulin&t=coveo4A2453FD
HS-CRP - $42.00
https://www.lifeextension.com/search#q=HS-CRP&t=coveo4A2453FD
IL6 - $75.00
https://www.lifeextension.com/search#q=il6&t=coveo4A2453FD
ESR - Inflammation test
TNF-alpha - $75.00
https://www.lifeextension.com/search#q=tnf%20alpha&t=coveo4A2453FD
Insulin-like growth factor 1 (IGF-1) - $56.25
https://www.lifeextension.com/lab-testing/itemlc010363/somatomedin-c-frozen-growth-hormone-marker-blood-test
Glutathione Blood Test - $149.00
https://www.lifeextension.com/lab-testing/itemlc007700/glutathione-blood-test
Gamma Glutamyl Transferase (GGT) Blood Test - $19.55
Used in conjunction with ALT and AST to evaluate liver function
https://www.lifeextension.com/lab-testing/itemlc001958/gamma-glutamyl-transferase-ggt-blood-test
Omega-3 Index Complete Finger Stick Test - $99.00
https://www.lifeextension.com/lab-testing/itemlc100066/omega-3-index-complete
Omega-3 Index Plus Finger Stick Test - $79.00
https://www.lifeextension.com/lab-testing/itemlc100065/omega-3-index-plus
Vitamin B12 and Folate Blood Test - $39.68
https://www.lifeextension.com/lab-testing/itemlc000810/vitamin-b12-and-folate-blood-test
Nutrient Panel Blood Test - $349.00
https://www.lifeextension.com/lab-testing/itemlc100024/nutrient-panel-blood-test
Vitamin B12
Folate
Vitamin D 25-hydroxy
Vitamin A
Vitamin C
Selenium
Zinc
CoQ10
RBC magnesium
Antioxidant and Nutrient Testing
https://shop.spectracell.com/micronutrient-test/

Epstein-Barr Virus (EBV) Antibody Profile - $95.00
https://www.lifeextension.com/lab-testing/itemlc240610/epstein-barr-virus-ebv-antibody-profile
Epstein-Barr Virus Antibodies (IgG and IgM)
Cytomegalovirus (CMV) Antibodies, IgG Blood Test - $59.00
https://www.lifeextension.com/lab-testing/itemlc006494/cytomegalovirus-cmv-antibodies-igg-blood-test
Cytomegalovirus (CMV) Antibodies, IgM Blood Test - $99.00
https://www.lifeextension.com/lab-testing/itemlc096727/cytomegalovirus-cmv-antibodies-igm-blood-test
Human Herpes Virus 6 IgG Antibodies (HHV-6) Blood Test - $49.00
https://www.lifeextension.com/lab-testing/itemlc161075/human-herpes-virus-6-igg-antibodies-blood-test
Human Herpes Virus 6 IgM Antibodies (HHV-6) Blood Test - $175.00
https://www.lifeextension.com/lab-testing/itemlc138529/human-herpes-virus-6-igm-antibodies-blood-test
Heavy Metals Panel (Mercury, Arsenic, Aluminum) Blood Test - $179.00
https://www.lifeextension.com/lab-testing/itemlc100003/heavy-metals-panel-mercury-arsenic-aluminum-blood-test
Heavy Metals Test (Urine) - $199
https://www.everlywell.com/products/elements-panel/
Arsenic, Mercury, Cadmium, Bromine, Selenium, Iodine, Urinary Creatinine
Standard Heavy Metals Profile, Blood Test - $219
https://www.healthlabs.com/heavy-metal-toxin-testing
This blood test measure levels of three types of heavy metals in the blood: Lead, Arsenic, and Mercury.
Standard Plus Heavy Metals Profile, Urine Test
This urine test measures levels of four types of heavy metals: Arsenic, Cadmium, Lead and Mercury. A creatinine test is also performed.
$398
Chitotriosidase / Fungus
Summarize some actionable steps a polycythemia vera patient can take to cure or monitor or improve their disease based on this information:
Get tested for chitotriosidase levels. Since research suggests chitotriosidase could be a biomarker for disease progression in polycythemia vera, monitoring levels over time may help gauge if the disease is worsening.
Get tested for fungal infections like candida. Some research suggests there could be a link between polycythemia vera and fungal infections. Getting tested for candida antibodies (IgA, IgG, IgM) or doing a comprehensive fungus culture test may uncover an infection that could potentially be treated.
Consider antifungal supplements. Supplements like caprylic acid, olive leaf extract, garlic extract and oregano oil have antifungal properties and some research shows they may inhibit candida overgrowth. Taking these as part of a candida cleanse diet may help.
Ask about antifungal medication. For confirmed fungal infections, prescription antifungal medications like fluconazole or itraconazole may be warranted. Discuss options with your hematologist.
Improve diet and lifestyle. A diet low in sugars, high in probiotics, and limiting alcohol intake may help prevent candida overgrowth. Manage stress levels since chronic stress weakens immunity.
Chitotriosidase is an enzyme produced by activated macrophages which plays a role in the defense against fungi, insects, and nematodes.
Research Discover Key Biomarker for Polycythemia Vera Progression
PV <-> fungus connection?
The authors noted that targeting the CHIT1 activation cascade diminished inflammation and fibrosis in studies on animals and could provide a targeted therapy option for PV, though the risk of fungal and protozoal infections would need to be considered.
The authors concluded that “CHIT1 could be considered as a circulating biomarker in PV,” an observation that “highlights the role of the tumor microenvironment in pathogenesis and the clinical presentation of MPNs, which might help in recognizing new therapeutic targets in these neoplasms.”
https://www.mdalert.com/ms/hematology/article/key-biomarker-for-polycythemia-vera-progression?fbclid=IwAR06d9xwW8D-F4JIMchgi4bk8g_sHULfbYW77LxkrQ1vBS5NlFsNaVawTII
Serum chitotriosidase: a circulating biomarker in polycythemia vera, 2018
Objectives: Serum chitotriosidase activity (CHIT1) is a biomarker of macrophage activation with an important role in inflammation-induced tissue remodeling and fibrosis. Macrophages have been described to play a crucial role in regulating pathological erythropoiesis in polycythemia vera (PV). The aim of this study was to evaluate CHIT1 in patients diagnosed with Philadelphia-negative myeloproliferative neoplasms (MPNs).
Methods: Using fluorometric assay, we measured CHIT1 in 28 PV, 27 essential thrombocythemia (ET), 17 primary myelofibrosis (PMF), 19 patients with secondary myelofibrosis and in 25 healthy controls.
Results: CHIT1 was significantly higher in PV (p < .001) and post-PV myelofibrosis (MF) transformation (post-PV MF) (p = .020), but not in ET (p = .080), post-ET MF transformation (p = .086), and PMF patients (p = .287), when compared to healthy controls. CHIT1 in PV was positively correlated with hemoglobin (p = .026), hematocrit (p = .012), absolute basophil count (p = .030) and the presence of reticulin fibrosis in the bone marrow (p = .023).
Discussion: A positive correlation between CHIT1 and these distinct laboratory PV features might imply macrophages closely related to clonal erythropoiesis as cells of CHIT1 origin. In addition, a positive association between CHIT1 and reticulin fibrosis might indicate its potential role in PV progression.
Conclusion: CHIT1 might be considered as a circulating biomarker in PV. Additional studies are needed to clarify the role of CHIT1 in promoting disease progression and bone marrow fibrosis in PV.
Characterization of human phagocyte-derived chitotriosidase, a component of innate immunity, 2005
Man has been found to produce highly conserved chitinases. The most prominent is the phagocyte-derived chitotriosidase, the plasma levels of which are markedly elevated in some pathological conditions. Here, we report that both polymorphonuclear neutrophils (PMNs) and macrophages (mϕ) are a source of chitotriosidase. The enzyme is located in specific granules of human PMNs and secreted following stimulation with granulocyte macrophage colony-stimulating factor (GM-CSF). In addition, GM-CSF induces expression of chitotriosidase in mϕ that constitutively secrete the enzyme and partly accumulate it in their lysosomes. Studies with recombinant human chitotriosidase revealed that the enzyme targets chitin-containing fungi. These findings are consistent with earlier observations concerning anti-fungal activity of homologous plant chitinases and beneficial effects of GM-CSF administration in individuals suffering from invasive fungal infections. In conclusion, chitotriosidase should be viewed as a component of the innate immunity that may play a role in defence against chitin-containing pathogens and the expression and release of which by human phagocytes is highly regulated.
Recombinant human chitotriosidase improves survival in neutropenic mouse models of Candidiasis and Aspergillosis
The in vivo efficacy of recombinant human chitotriosidase was studied in neutropenic mouse models of systemic Candidiasis and systemic Aspergillosis, the major causes of mortality in immunosuppressed individuals (14, 15). Recombinant human chitotriosidase, when administrated daily by i.p. injection for 10 consecutive days, promoted survival in a dose-dependent manner when compared with control Candidiasis mice (Fig. 4A). In the control group, all mice died by day 14 of the study. In the groups treated with chitotriosidase, a clear increase in survival was observed. When treated with 10 and 30 mg kg−1, ∼30–40% of the mice survived at this time point, whereas in the group treated with 100 mg kg−1 a striking increase to 80% survival was achieved. The latter group also demonstrates highest survival (55%) at the end-point of the study and this is ∼20% in the lower dose groups. Of note, recombinant chitotriosidase activity rapidly disappeared from the circulation, 90% is lost 1 h post-dose and the tissue half-life is 3 h. Efficacy could be improved by repetitive dosing (data not shown).
IgA antibodies: this type is normally found in the mucous secretions. It plays a major role in local immunity; and, constitutes 15 to 20% of all human immunoglobulins. It is the major class of antibodies found in our seromucous secretions. When the IgA levels against the candida are high, they reflect high levels of mucosal epithelial, trachea-bronchial, genital and urinary candida infections.
IgM antibodies: this type is the first antibody released, following any first-time exposure to a certain antigen. Once formed, it activates the compliment and initiate the phagocytic system to help the body getting rid of invading antigens. IgM are specific to our intravascularly tissues. They are the most predominant immunoglobulins released upon any early infection. If the body gets re-infected with the same pathogen, the IgM levels will no longer be as elevated as in early infections. The body will then release IgG’s antibodies instead.
Why take the Candida IgA, IgM and IgG test?
This test is the most accurate way to check for a candida infection. Measuring all three antibodies can explain more about where the infection is. The IgM antibodies can help identify if you have an active infection. The IgG antibodies will show the presence of a past or ongoing infection. Finally, the IgA antibody levels will indicate if the candida infection is a serious one (reached the outside surfaces of the mucosal milieu in the body) or just a superficial one.
Detecting a problem early will help address the candida infection and prevent its progress into a more serious health condition. Untreated candida infections will have negative effects on the quality of your life. You will be uncomfortable, with burning and increased discharges. If the overgrowth became invasive, it could lead to possible organ malfunctions. The Candida antibodies blood test can also help follow up the effectiveness of a given treatment. It will help monitor your infection.
4 Things Clinicians Need to Know About Candida Immunoglobulin (Ig) Screening
https://www.usbiotek.com/blog/4-things-clinicians-need-know-about-candida-immunoglobulin-ig-screening
Candida Antibody Panel $210
https://www.accesalabs.com/Candida-Antibody-Panel
Blood test cuts time to diagnosis for common, deadly yeast infection, national trial shows
https://www.sciencedaily.com/releases/2018/02/180209174532.htm
The T2Candida Panel is the first diagnostic test for candidemia -- a type of bloodstream infection caused by Candida yeast -- that has been cleared by the U.S. Food and Drug Administration and doesn't require culturing a blood sample from the patient to see what grows. The results of the trial, named DIRECT2, are reported today in the journal Clinical Infectious Diseases. The trial was funded by T2 Biosystems, the company that makes the panel, which is used by UPMC.
T2Candida Panel
Faster targeted therapy and reduction in empiric antifungal costs
https://www.t2biosystems.com/products-technology/t2candida-panel/
Unprecedented speed and accuracy: The T2Candida Panel pivotal clinical trial demonstrated results in 3 to 5 hours.4 All other FDA-cleared Candida diagnostic methods require a positive blood culture. Blood culture misses up to half of infections and often will take 2 to 8 days to become positive.5 Only then can identification be performed. In most cases, a negative result is not confirmed for 5 days after collection and processing of the blood culture.
Fungus (Mycology) Culture - Candida Test 79.95$
With the Candida Test, your stool sample is examined to determine:
1.) Candida albicans
2.) Candida spec.
3.) Geotrichum spec.
4.) Mold
Candida & intestinal fungi can lead to a variety of complaints – e.g. during digestion, but also to a weak immune system, sleeping disorders, food intolerances and concentration difficulties.
Our Candida Test gives you information about the candida concentration in your gut. In case of a detected candida overgrowth, you can work to restore the balance of your gut as a healthy gut flora is the best protection against future candida infestation.
How does it work?
You collect the samples at home, send them back to us and we will provide you with your level of each analyte and whether your level falls within the reference ranges for your age. In addition to that, the results include graphs showing whether your are in the “green” (=normal/healthy) or “red” (=too high/low) area, making it easy to understand the results.
What will my results tell me?
Your results will provide detailed information about whether your candida, geotrichum and yeast levels are normal, low, or high compared to reference ranges in your age group. You can then discuss the results with your doctor or health practitioner, who can give you further guidance and treatment recommendations.
What guidance will I get along with my results?
We always recommend the discussion of the mailed results with your doctor or practitioner. Although we do not offer therapy service ourselves, we will gladly assist you in finding a suitable therapist in your area. Besides, further information is available on our website, especially in the different test categories, under “health conditions” and the FAQs. Still have questions? Send us an email at contact@verisana.com.
Candida IgA, IgM, IgG Blood - $349
IgG Antibodies: this is the most commonly formed antibody. It is usually released upon a secondary exposure to the antigen. This type of antibody can reflect either an ongoing or a previous infection. It usually comes in a secondary stage. When the body first gets exposed to a certain antigen (primary exposure), it releases another kind of antibodies. When these decrease in number, following a secondary exposure, the body will start releasing IgG. This kind of antibody plays a major role in the phagocytic process that aims at eliminating antigens from our system.
IgG antibodies are predominant immunoglobulins; and, are found everywhere in our fluids: in both intra- and extravascular fluids. When a person becomes infected, these type of antibodies may remain in your system for many years, even after the infection is eradicated.
Candida Test (link)
An Overview of the Management of the Most Important Invasive Fungal Infections in Patients with Blood Malignancies, 2020
Abstract
In patients with hematologic malignancies due to immune system disorders, especially persistent febrile neutropenia, invasive fungal infections (IFI) occur with high mortality. Aspergillosis, candidiasis, fusariosis, mucormycosis, cryptococcosis and trichosporonosis are the most important infections reported in patients with hematologic malignancies that undergo hematopoietic stem cell transplantation. These infections are caused by opportunistic fungal pathogens that do not cause severe issues in healthy individuals, but in patients with hematologic malignancies lead to disseminated infection with different clinical manifestations. Prophylaxis and creating a safe environment with proper filters and air pressure for patients to avoid contact with the pathogens in the surrounding environment can prevent IFI. Furthermore, due to the absence of specific symptoms in IFI, rapid and accurate diagnosis reduces the mortality rate of these infections and using molecular techniques along with standard mycological methods will improve the diagnosis of disseminated fungal infection in patients with hematologic disorders. Amphotericin B products, extended-spectrum azoles, and echinocandins are the essential drugs to control invasive fungal infections in patients with hematologic malignancies, and according to various conditions of patients, different results of treatment with these drugs have been reported in different studies. On the other hand, drug resistance in recent years has led to therapeutic failures and deaths in patients with blood malignancies, which indicates the need for antifungal susceptibility tests to use appropriate therapies. Life-threatening fungal infections have become more prevalent in patients with hematologic malignancies in recent years due to the emergence of new risk factors, new species, and increased drug resistance. Therefore, in this review, we discuss the different dimensions of the most critical invasive fungal infections in patients with hematologic malignancies and present a list of these infections with different clinical manifestations, treatment, and outcomes.
Keywords: invasive fungal infection, blood malignancies, aspergillosis, candidiasis, fusariosis, mucormycosis, cryptococcosis, trichosporonosis
Role of chitotriosidase (chitinase 1) under normal and disease conditions, link
Mammalian chitinases belong to the glycosyl hydrolase 18 family based on structural homology and the family includes a large number of bacterial and eukaryotic chitinases. Among the mammalian chitinases, chitotriosidase (CHIT1) and acidic mammalian chitinase (AMCase) are capable of hydrolyzing the β-(1, 4)-linkage between the adjacent N-acetyl glucosamine residues of chitin. CHIT1 is one of the most abundantly secreted proteins, being mainly produced by activated macrophages and epithelial cells. CHIT1 plays a pivotal role in the context of infectious disease including malaria and fungi infections as a host defense towards chitin in pathogen's cell structure and as a diagnostic marker of disease. In contrast, CHI1 released by activated Kupffer cells in liver could induce hepatic fibrosis and cirrhosis. Increased serum levels of CHIT1 were observed in patients with many disorders, including Gaucher's disease, bronchial asthma, and atherosclerosis. Therefore, CHIT1 seems to have dual (regulatory and pathogenic) roles depending on the disease and producing cell types during the inflammatory conditions.
Chitotriosidase: A New Inflammatory Marker in Diabetic Complications, link
Chitotriosidase (CHIT1) belongs to chitinase family. So far this enzyme has been the best investigated human chitinase regarding its biological activity and association with various disorders. In a healthy population, CHIT1 activity is very low and originates in the circulating polymorphonuclear cells. Conversely, during the development of acute/chronic inflammatory disorders, the enzymatic activity of CHIT1 increases significantly. Recently, CHIT1 has also been involved in the pathogenesis of diabetes mellitus (DM). Mounting evidence from experimental studies revealing the increase of CHIT1 levels in pathological conditions, such as atherosclerosis, coronary artery disease, acute ischemic stroke, cerebrovascular dementia, nonalcoholic fatty liver disease, and osteolytic processes suggest its critical role in the evolutions and complications of DM. This review is addressed to provide mechanistic insights by highlighting the relationship between CHIT1 and diabetes, and their contribution in the exacerbation of this disease.
Serum Chitotriosidase Activity Is Increased in Subjects With Atherosclerosis Disease
Objective— This study was undertaken to analyze the relation between serum activity of chitotriosidase enzyme, a protein synthesized exclusively by activated macrophages, and atherosclerotic lesion extent in subjects with atherothrombotic stroke (ATS) and in subjects with ischemic heart disease (IHD).
Methods and Results— We assayed the serum chitotriosidase activity and a common chitotriosidase gene polymorphism that causes deficiency in chitotriosidase activity in 3 Spanish populations, ATS (n=153), IHD (n=124), and control (n=148) subjects. Statistical differences were found in serum chitotriosidase activity between ATS (88.1±4.6 nmol/mL · h, P<0.0001) and IHD subjects (79.0±6.3, P=0.002) versus control group (70.9±5.2). These observed differences were not attributable to a distinct allelic or genotype distribution. The extension of the atherosclerotic lesion in carotids of ATS subjects was measured by duplex sonography. Chitotriosidase activities were 66.9±9.6, 88.7±8.3, and 107.7±11.8 for subjects with carotid stenosis ≤30%, 31% to 60%, and >60%, respectively. Statistical differences were observed between subjects with major and intermediate stenosis grade compared with subjects with minor stenosis, P=0.005 and P=0.016, respectively.
Conclusions— Serum chitotriosidase activity is significantly increased in individuals suffering from atherosclerosis disease and is related to the severity of the atherosclerotic lesion, suggesting a possible role as atherosclerotic extent marker.
TOP 7 ANTIFUNGAL SUPPLEMENTS TO FIGHT CANDIDA (link)
1. CAPRYLIC ACID
Coconut oil is made up of three fatty acids: caprylic acid capric acid and lauric. Of these, caprylic acid is its most important active ingredient. Caprylic acid is renowned as one of the strongest Candida killers, and also for restoring normal acidity levels in the gut. Taking caprylic acid during your treatment can get your intestinal tract back in shape and help to prevent Candida colonies from growing again.
Studies have shown caprylic acid’s potency to be similar to prescription antifungals.
It works by interfering with the cell walls of the Candida yeast. Its short chain length means it can penetrate the cell wall of the yeast relatively easily. It then inhibits the growth of the yeast by incorporating itself into the cell membrane and causing it to rupture. This effectively destroys the yeast cell and can even prevent it from returning.
A study conducted by Japan’s Niigata University found that the fungicidal effect of caprylic acid on Candida albicans was “exceedingly powerful” (1). More recent studies have found that oral supplementation with caprylic acid reduces the symptoms of Candida more quickly and efficiently than some pharmaceutical antifungal drugs such as Diflucan.
6. GARLIC EXTRACT
Garlic is one of the world’s most-researched herbs – and one of the most powerful! There’s a massive amount of scientific evidence supporting its use as an antifungal, particularly against Candida albicans.
One of garlic’s most important antifungal agents is Ajoene, an organosulfur compound that has been shown to kill off a variety of fungal infections. Ajoene is formed from a compound named allicin and an enzyme named alliinase. When garlic is chopped or crushed, allicin and alliinase come together to form the powerful antimicrobial agent ajoene.
Much research has found ajoene to have the strongest activity of all garlic compounds in inhibiting the growth of Candida albicans. One study showed garlic markedly inhibited the growth of Candida when the samples of the disease were treated with aqueous garlic extract. This was later supported by further research showing that garlic has the power to halt the growth and spread of Candida albicans. (7)
Although ajoene’s antifungal properties are well-documented, its exact mechanism of action is not so clear. As with other antifungals, scientists hypothesize that ajoene works by disrupting the cell walls of the Candida yeast cells and thus preventing them from functioning properly.
A typical recommendation is to take two or three antifungals at any one time as this helps to prevent Candida from adapting to a single ingredient. Garlic works well when used in combination with other natural antifungals.
7. OLIVE LEAF EXTRACT
Olive leaf extract is derived from the dark green olive leaves and contains an active ingredient named oleuropein.
Research has shown that oleuropein has an incredible array of health properties as an antimicrobial, antifungal, antioxidant, anti-inflammatory, anti-atherogenic and antiviral.
As well as being a natural and effective antifungal, olive leaf extract is shown to have anti-parasitic properties. It also appears to contain almost double the antioxidant capacity of green tea, Vitamins C and E, and grape seed extract. A 2015 study on fresh olive leaf extract showed that it exhibited antifungal activity against Candida yeast. (8)
A similar study in 2016 showed oleuropein to have powerful antifungal activity against Candida albicans, with researchers noting that the oleuropein appeared to target various factors that the fungal infection needed to survive. It was also found that the oleuropein was able to inhibit Candida from growing. (9)
Antifungal Prophylaxis in Cancer Patients After Chemotherapy or Hematopoietic Stem-Cell Transplantation: Systematic Review and Meta-Analysis
Purpose
To evaluate the effect of antifungal prophylaxis on all-cause mortality as primary outcome, invasive fungal infections (IFIs), and adverse events. Many studies have evaluated the role of antifungal prophylaxis in cancer patients, with inconsistent conclusions.
Methods
We performed a systematic review and meta-analysis of randomized, controlled trials comparing systemic antifungals with placebo, no intervention, or other antifungal agents for prophylaxis in cancer patients after chemotherapy. The Cochrane Library, MEDLINE, conference proceedings, and references were searched. Two reviewers independently appraised the quality of trials and extracted data.
Results
Sixty-four trials met inclusion criteria. Antifungal prophylaxis decreased all-cause mortality significantly at end of follow-up compared with placebo, no treatment, or nonsystemic antifungals (relative risk [RR], 0.84; 95% CI, 0.74 to 0.95). In allogeneic hematopoietic stem-cell transplantation (HSCT) recipients, prophylaxis reduced all-cause mortality (RR, 0.62; 95% CI, 0.45 to 0.85), fungal-related mortality, and documented IFI. In acute leukemia patients, there was a significant reduction in fungal-related mortality and documented IFI, whereas the difference in mortality was only borderline significant (RR, 0.88; 95% CI, 0.74 to 1.06). Prophylaxis with itraconazole suspension reduced documented IFI when compared with fluconazole, with no difference in survival, and at the cost of more adverse events. On the basis of two studies, posaconazole prophylaxis reduced all-cause mortality (RR, 0.74; 95% CI, 0.56 to 0.98), fungal-related mortality, and IFI when compared with fluconazole.
Conclusion
Antifungal prophylaxis decreases all-cause mortality significantly in patients after chemotherapy. Antifungal prophylaxis should be administered to patients undergoing allogeneic HSCT, and should probably be administered to high-risk acute leukemia patients.
Treatment of invasive fungal infections in cancer patients—updated recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3889633/
Preventative use of antifungal drugs in patients treated for cancer
https://academic.oup.com/jac/article/53/2/130/850679
Herpes Virus / HSV / CMV Cancer
Antiviral prophylaxis in haematological patients: systematic review and meta-analysis, 2009
Purpose: Antiviral prophylaxis is commonly prescribed to haematological cancer patients. We conducted a systematic review and meta-analysis to quantify its overall benefit in specific clinical scenarios.
Methods: Randomised controlled trials assessing antiviral prophylaxis versus placebo, no treatment, pre-emptive treatment or another antiviral drug were included. Patients undergoing haematopoietic stem cell transplantation (HSCT) or intensive chemotherapy for acute leukaemia or high-grade lymphoma were included. No restrictions on language, year or publication status were applied. Overall mortality, herpes simplex virus (HSV) and cytomegalovirus (CMV) diseases were assessed as primary outcomes. Pooled relative risks (RRs) and numbers needed to treat (NNT) with 95% confidence intervals (CI) are reported.
Results: HSCT was the condition assessed in 22 trials and intensive chemotherapy in 5 trials. In the pre-engraftment setting of autologous or allogeneic HSCT, antiviral prophylaxis (mainly acyclovir for HSV seropositive recipients) significantly reduced HSV (NNT 2, 2-2, control event rate (CER) 61.9%) and CMV disease, with no effect on overall mortality. In the allogeneic post-engraftment setting (mainly CMV-seropositive recipients/donors), antiviral prophylaxis resulted in a significant reduction in overall mortality, RR 0.79 (0.65-0.95), NNT 12 (7-50, CER 39.4%) and all viral-related outcomes. In this setting, acyclovir significantly reduced overall mortality (RR 0.71, 0.53-0.96, 4 trials) and ganciclovir/maribavir significantly reduced CMV disease (RR 0.26, 0.14-0.48, 5 trials). During chemotherapy, acyclovir significantly decreased HSV disease (NNT 3, 2-4, CER 37.4%) and infection rates, with no effect on mortality.
Conclusions: Antiviral prophylaxis reduced mortality with a small NNT in the post-engraftment setting of allogeneic HSCT. In the pre-engraftment phase and during chemotherapy only viral-related morbidity was reduced.
Detection of herpes simplex virus DNA sequences in human blood and bone marrow cells
Herpes simplex virus type 1 (HSV1) establishes latent infections in neural tissues of humans and experimental animals. Utilizing a sensitive polymerase chain reaction (PCR) assay we detected HSV DNA sequences in blood cells of healthy prospective bone marrow transplant (BMT) donors and patients. In three healthy individuals studied, HSV DNA sequences were found in all blood cell types and also in bone marrow cells as well as in stem cell progenitor colonies isolated from in vitro cultures. Studies of BMT donor-recipient pairs suggested that HSV reactivation may occur in hematopoietic cells after transplantation, as the PCR signal intensity increased over time simultaneous with an increased antibody titer to HSV. In a mouse model for HSV infection, HSV DNA sequences were found in blood and bone marrow cells at the latent stage of infection, after intravenous (IV) inoculation, but not after ocular inoculation. These studies suggest that bone marrow cells may be an additional site of HSV latency capable of reactivation after BMT. These studies have broad implications for understanding pathogenesis of HSV disease and are of particular significance in situations where allogeneic bone marrow cells are given therapeutically.
Ruxolitinib Treatment Is Associated with Increased Incidence of Infections and Higher Risk of HSV/Vzv Recurrence in Patients with Myeloproliferative Neoplasm (MPN) Related Myelofibrosis (MF)
Introduction: Ruxolitinib (RUX) is a JAK 1/2 inhibitor approved for the treatment of intermediate and high-risk primary or secondary MF. In addition to the intrinsic immune system modulation in MF patients, JAK inhibition exerts an immunosuppressive effect that may increase the risk of infections (Heine A et al., Blood, 2013). We aimed to investigate the association between treatment with RUX and infectious complications in a large monocentric cohort of MF patients.
Methods: We performed a retrospective study including all patients diagnosed with primary, post-polycythemia vera or post-essential thrombocythemia MF in our MPN clinic between January 2011 and April 2020. Patients were considered RUX treated when exposed to treatment for at least two consecutive months. Clinical and biological characteristics at time of MF diagnosis and follow-up were collected from medical charts and electronic medical records. We used logistic regression models to identify specific infection subtypes associated with RUX treatment. Univariate and multivariate analysis assessing the impact of categorical and continuous variables on infectious events cumulative incidence were performed using Cox models.
Results: 213 MF patients were included in the study. 114 (51.1%) patients were treated with RUX while 99 didn't receive RUX. Overall 102 patients exhibited a total of 231 infectious episodes.
To search for factors associated with occurrence of infectious events, we evaluated the characteristics of MF, potential clinical and biological immune suppression factors (immunosuppressive treatment, prior non-MPN cancer, diabetes, hepatic/renal failure, neutropenia, lymphopenia, hypo-gammaglobulinemia, complement deficiency, prior history of infection), use of infection prophylaxis and RUX treatment using Cox models. In this cohort of MF patients, we found that RUX treatment (HR 5.91, 95%CI[3.48; 10.04], p<0.001) and a performance status > 2 (HR 4.91, 95%CI[2.62; 9.21], p<0.001) were independently associated with infectious complications (Figure A). Infections rates were 74.0% in RUX treated patients versus 28.3% in non-RUX patients.
41 (22.2%) and 16 (34.0%) infections were of grade 3-4, 61 (33.1%) and 19 (40.4%) required hospitalization, while 8 (4.3%) and 2 (4.2%) resulted in patients' death, in RUX treated and RUX naïve patients, respectively (all non-significantly different). Bacterial infections represented 48.0%, viral infections 16.0% and fungal infections 4.8% of the total infectious events. The most frequently infected sites were lungs/respiratory tract (28.1%) and skin/soft tissue (24.2%). RUX treatment was significantly associated with recurrence of HSV-1/2 or VZV (OR 7.57, 95%CI[1.01-57.30], p=0.050), and skin/soft tissue infections including the above herpetic recurrences (OR 3.33, 95%CI[1.13-9.78], p=0.029). 17 (14.9%) patients presented with HSV/VZV recurrence in the RUX treated group compared to 1 (1.0%) in non-treated patients (Figure B).
We then thought to evaluate the impact of potential infections risk factors in RUX treated patients at time of treatment initiation in order to inform clinicians' therapeutic decision and follow-up guidance. For this analysis, we evaluated the characteristics of MF, potential clinical and biological immune suppression factors, treatment lines prior to RUX, dose and cumulative exposition to RUX. No clinical or biological factor was significantly associated with the overall risk of infectious events. However, hypo-gammaglobulinemia at time of RUX initiation was independently associated with HSV and/or VZV recurrence (HR 4.57, 95%CI[1.29-16.16], p=0.018).
The higher rate of infections in RUX treated patients was associated with a not statistically significant trend towards shorter OS (HR 1.97, 95%CI[0.98; 3.94], p=0.055).
Conclusion: This retrospective study shows an association between the occurrence of infectious complications and Ruxolitinib treatment in MF patients, and in particular, a higher incidence of HSV/VZV recurrence and skin/soft tissue infection. Patients with hypo-gammaglobulinemia at time of RUX initiation were at higher risk of HSV/VZV recurrence, suggesting that protein electrophoresis should be performed prior to treatment initiation and primary antiviral prophylaxis proposed to patients with hypo-gammaglobulinemia.
Virscan
The new test, known as VirScan, works by screening the blood for antibodies against any of the 206 species of viruses known to infect humans, according to a study published Thursday in the journal Science. The immune system, which churns out specific antibodies when it encounters a virus, can continue to produce those antibodies decades after an infection subsides. VirScan detects those antibodies and uses them as a window in time to create a blueprint of nearly every virus an individual has encountered. It's a dramatic alternative to existing diagnostic tools, which test only for a single suspected virus.
Comprehensive serological profiling of human populations using a synthetic human virome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4844011/
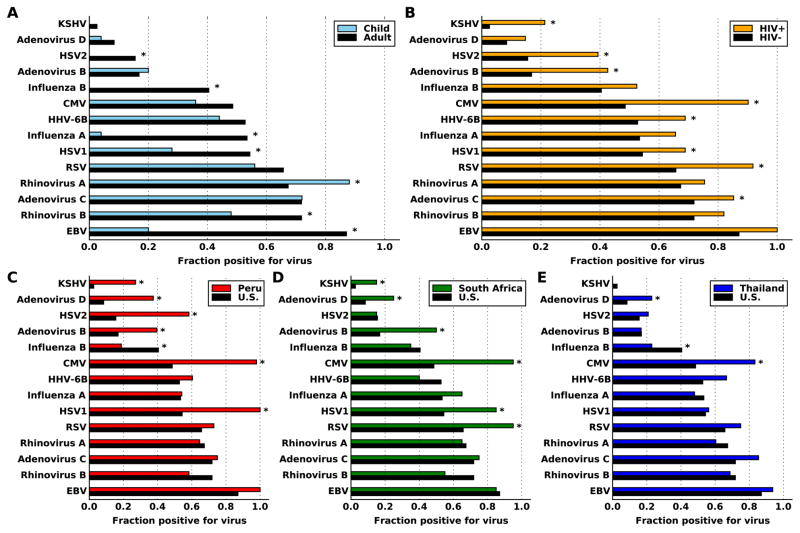
The effects of antiviral treatment on breast cancer cell line, link
Results
We demonstrate the suppressive effect of acyclovir on breast cancer cells. Acyclovir treatment decreases the growth and the proliferation rate of cells and correlates with the upregulated levels of apoptosis associated cytokine Caspase-3. Moreover, acyclovir inhibits colony formation ability and cell invasion capacity of the cancer cells while enhancing the expression of E-cadherin protein in MCF7 cells. Breast cancer cells are characterized by high ALDH activity and associated with upregulated proliferation and invasion. According to this study, acyclovir downregulates ALDH activity in MCF7 cells.
Conclusions
These results are encouraging and demonstrate the possibility of partial suppression of cancer cell proliferation using an antiviral agent. Acyclovir antiviral agents have a great potential as an adjuvant therapy in the cancer treatment. However, more research is necessary to identify relevant biochemical mechanisms by which acyclovir induces a potent anti-cancer effect.
Antiviral agents such as acyclovir and ribavirin have been reported to have a suppressive effect on the proliferation and ability to increase an apoptosis in various cancers [7, 8]. Acyclovir was discovered 40 years ago and remains one of the main existing therapies for herpes simplex virus (HSV) infections. This drug is a highly potent inhibitor of this virus and commonly used for the treatment of the infections caused by the herpes viruses, CMV and EBV. It also has a low toxicity for the normal cells [10].
In the present study, we propose to investigate how cancer cells respond to the antiviral agent as acyclovir in vitro and whether this treatment can affect the metastatic phenotype of cancer cells. We report results on the potential effect of acyclovir treatment on the cell proliferation, invasion capacity, cytotoxicity, and the expression of tumor suppressing genes.
[NEGATIVE] Cytomegalovirus prophylaxis using low-dose valganciclovir in patients with acute leukemia undergoing allogeneic hematopoietic stem-cell transplantation
Background: Letermovir prophylaxis is currently the standard of care for the prevention of cytomegalovirus (CMV) infections in allogeneic hematopoietic stem-cell transplantation (allo-HSCT). However, drug-drug interactions between letermovir and azoles or calcineurin inhibitors and the high financial burden of letermovir remain problematic, especially in resource-limited countries. It has not been clarified whether a lower dose of valganciclovir would constitute an effective strategy for CMV prevention in patients with acute leukemia undergoing allo-HSCT.
Methods: We retrospectively assessed 84 consecutive adult patients with acute leukemia who underwent allo-HSCT. These 84 patients were stratified into a valganciclovir prophylaxis group (n = 20) and a non-valganciclovir prophylaxis group (n = 64).
Results: Patients in the valganciclovir prophylaxis group had a lower possibility of CMV DNAemia at week 14 after allo-HSCT than those in the non-valganciclovir prophylaxis group (15.0% versus 50.0%; p = 0.012). The cumulative incidence of CMV DNAemia at week 14 was also lower in patients with valganciclovir CMV prophylaxis than in those without (15.0% versus 50.4%; p = 0.006). Multivariate analysis validated these data, showing that a low dose of valganciclovir significantly reduced the risk of CMV DNAemia at week 14 by 88% (hazard ratio: 0.12; 95% confidence interval: 0.04-0.42; p = 0.001). However, these two groups had similar overall survival rates at week 48 (75.0% versus 76.6%; p = 0.805). Four of 20 (20%) patients discontinued valganciclovir prophylaxis because of adverse events.
Conclusion: Low-dose valganciclovir prophylaxis could be an alternative to letermovir to prevent CMV infection in allo-HSCT, especially in resource-limited countries.
Antiviral Drug May Extend Survival in Glioblastoma (2018)
The common antiviral drug Valcyte (valganciclovir) may extend survival in glioblastoma, according to the results of a study published in the New England Journal of Medicine.
The results indicate that the rate of survival was remarkably high among patients receiving Valcyte. After two years, 62 percent of these patients were still alive compared with only 18 percent of patients from the control group. Median overall survival in the Valcyte group was 25.0 months, compared with 13.5 months in the control group.
It appears that longer treatment with Valcyte produced better results. Among 40 patients who took the drug for at least six months, the two-year survival rate was 70 percent and median survival was 30.1 months. The highest survival rate occurred in a group of 25 patients who received continuous Valcyte treatment after the first six months. This group had a two-year survival rate of 90 percent and a median overall survival of 56.4 months.
These results are stunning in the face of a disease with an average survival of one year. The researchers note that selection bias was highly unlikely to play a role in the face of such high survival rates. They state that the results warrant a randomized trial targeting CMV in patients with glioblastoma.
Valganciclovir as Add-on to Standard Therapy in Glioblastoma Patients, 2020
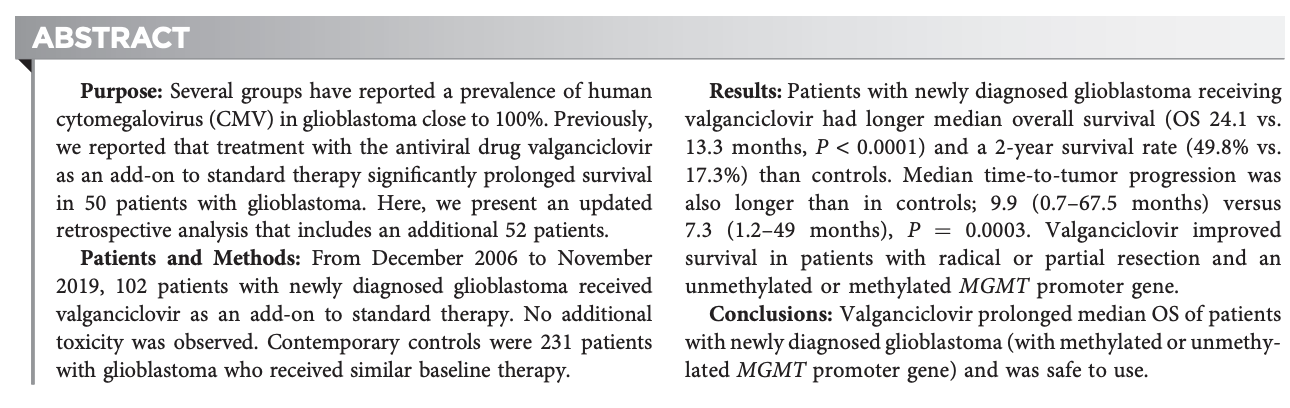
How I treat resistant cytomegalovirus infection in hematopoietic cell transplantation recipients, 2016
Cytomegalovirus (CMV) infection is a significant complication in hematopoietic cell transplantation (HCT) recipients. Four antiviral drugs are used for preventing or treating CMV: ganciclovir, valganciclovir, foscarnet, and cidofovir. With prolonged and repeated use of these drugs, CMV can become resistant to standard therapy, resulting in increased morbidity and mortality, especially in HCT recipients. Antiviral drug resistance should be suspected when CMV viremia (DNAemia or antigenemia) fails to improve or continue to increase after 2 weeks of appropriately dosed and delivered antiviral therapy. CMV resistance is diagnosed by detecting specific genetic mutations. UL97 mutations confer resistance to ganciclovir and valganciclovir, and a UL54 mutation confers multidrug resistance. Risk factors for resistance include prolonged or previous anti-CMV drug exposure or inadequate dosing, absorption, or bioavailability. Host risk factors include type of HCT and degree of immunosuppression. Depending on the genotyping results, multiple strategies can be adopted to treat resistant CMV infections, albeit no randomized clinical trials exist so far, after reducing immunosuppression (if possible): ganciclovir dose escalation, ganciclovir and foscarnet combination, and adjunct therapy such as CMV-specific cytotoxic T-lymphocyte infusions. Novel therapies such as maribavir, brincidofovir, and letermovir should be further studied for treatment of resistant CMV.
Randomized clinical trial to evaluate the efficacy and safety of valganciclovir in a subset of patients with chronic fatigue syndrome, 2013
There is no known treatment for chronic fatigue syndrome (CFS). Little is known about its pathogenesis. Human herpesvirus 6 (HHV-6) and Epstein-Barr virus (EBV) have been proposed as infectious triggers. Thirty CFS patients with elevated IgG antibody titers against HHV-6 and EBV were randomized 2:1 to receive valganciclovir (VGCV) or placebo for 6 months in a double-blind, placebo-controlled trial. Clinical endpoints aimed at measuring physical and mental fatigue included the Multidimensional Fatigue Inventory (MFI-20) and Fatigue Severity Scale (FSS) scores, self-reported cognitive function, and physician-determined responder status. Biological endpoints included monocyte and neutrophil counts and cytokine levels. VGCV patients experienced a greater improvement by MFI-20 at 9 months from baseline compared to placebo patients but this difference was not statistically significant. However, statistically significant differences in trajectories between groups were observed in MFI-20 mental fatigue subscore (P = 0.039), FSS score (P = 0.006), and cognitive function (P = 0.025). VGCV patients experienced these improvements within the first 3 months and maintained that benefit over the remaining 9 months. Patients in the VGCV arm were 7.4 times more likely to be classified as responders (P = 0.029). In the VGCV arm, monocyte counts decreased (P < 0.001), neutrophil counts increased (P = 0.037) and cytokines were more likely to evolve towards a Th1-profile (P < 0.001). Viral IgG antibody titers did not differ between arms. VGCV may have clinical benefit in a subset of CFS patients independent of placebo effect, possibly mediated by immunomodulation and/or antiviral effect. Further investigation with longer treatment duration and a larger sample size is warranted.
Valganciclovir has been reported to improve physical and cognitive symptoms in patients with chronic fatigue syndrome (CFS) with elevated human herpesvirus 6 (HHV-6) and Epstein-Barr virus (EBV) IgG antibody titers.
Chronic Fatigue Syndrome (ME/CFS) Physicians Report…
https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/valcyte-valganciclovir-for-chronic-fatigue-syndrome-mecfs/
A range of ME/CFS physicians have provided their assessments of Valcyte’s effectiveness in this disorder. Calling Valcyte a ‘significant step forward’ Dr. Guyer reports ‘encouraging results’ from a relatively small number of patients.
Dr. Holtof finds Valcyte effective in a subset of patients with evidence of herpesvirus reactivation (high IgG/Ea levels for EBV, HHV-6, CMV) and immune activation/suppression (high RNase L activity, low NK cell activity).
Dr. Peterson’s decades long focus on treating immune dysfunctional ME/CFS patients has lead him to assert that 6 months of treatment is necessary to get significant benefits. Kristin Loomis, Director of the HHV-6 Foundation, agrees, stating that long term treatment is necessary to overcome the long term immune suppression (6 months) caused by the herpesviruses found in ME/CFS. Dr. Enlander reports its effects range from highly dramatic to minimal.
Given valcytes potentially serious side effects, Dr. Podell feels ME/CFS patients with a ‘decent quality of life’ not try Valcyte.
Chronic Fatigue Syndrome (ME/CFS) Patients Report
I know of two patients who failed miserably on Valtrex only to respond very favorably to Valcyte. One patients shocking decline on Valtrex was quickly reversed on Valcyte and he returned to full health.
Dose
Dr. Lerner’s Valcyte Protocol for ME/CFS – Dr. Lerner recommends “valganciclovir (Valcyte) one 450-mg capsule daily for three days, followed by two 450-mg capsules in the morning daily. Liver function tests are studied very carefully. If there is any abnormality, one alters the dosage. Given the patient’s ability to safely tolerate two 450-mg capsules, dosing can be increased to two, 450-mg capsules in the morning and a one additional 450-mg capsule twelve hours later. Liver function tests, again, must be studied carefully and frequently.
Patients are monitored up to twice weekly in the beginning of treatment for liver toxicity. Despite the hoary warnings, side effects were not an issue in the Montoya ME/CFS studies.
Cost
Valcyte costs about $2,000/month in the U.S.
Hypertension in MPNs
Primary Arterial Hypertension and Drug-Induced Hypertension in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review, 2023
The impact of primary arterial hypertension (HTN) in myeloproliferative neoplasms (MPNs) remains unclear, with scant literature available, mostly focusing on cardiovascular risk factors as a singular entity or on organ-specific HTN. Furthermore, available studies reporting findings on drug-induced HTN in MPNs report varying and contradictory findings. In consideration of the above, this study set out to systematically review the available literature and shed light on the occurrence of HTN in MPNs, its association with thrombosis, as well as the drugs used in MPN management that could increase blood pressure. The literature search yielded 598 potentially relevant records of which 315 remained after the duplicates (n = 283) were removed. After we screened the titles and the abstracts of these publications, we removed irrelevant papers (n = 228) and evaluated the full texts of 87 papers. Furthermore, 13 records did not meet the inclusion criteria and were excluded from the systematic review. Finally, a total of 74 manuscripts were entered into the qualitative synthesis and included in the present systematic review. Our systematic review highlights that HTN is the most common comorbidity encountered in MPNs, with an impact on both the occurrence of thrombosis and survival. Moreover, drug-induced HTN remains a challenge in the management of MPNs. Further research should investigate the characteristics of patients with MPNs and HTN, as well as clarify the contribution of HTN to the development of thrombotic complications, survival and management in MPNs. In addition, the relationship between clonal hematopoiesis of indeterminate potential, HTN, cardiovascular disease and MPNs requires examination in upcoming assessments.
The study aims to systematically review the impact of primary arterial HTN in MPNs, its association with thrombosis, and the effects of MPN management drugs on blood pressure due to limited and unclear literature on the subject.
Philadelphia-negative MPNs are hematological clonal disorders with growing global burden and significant negative effects on prognosis and overall survival rates due to comorbidities, particularly cardiovascular comorbidities like HTN which account for 45% of MPN patient deaths.
Multiple factors contribute to the association between MPNs and HTN, such as the JAK2V617F mutation, altered cardiac physiology, impaired neural control of blood pressure, high platelet count and dysfunction, and drugs used in MPN management that inhibit JAK2/STAT3 pathways, leading to end-organ damage and dysfunction.
Understanding the epidemiology and impact of each CVRF on thrombosis and survival in MPNs is crucial, with HTN being the most common CVRF in the general adult population, and the significance of drug-induced HTN in MPN management is also important to consider.
The study followed PRISMA guidelines and registered the protocol in PROSPERO, using three assessors to search PubMed/MEDLINE, Web of Science, and SCOPUS databases for relevant articles.
The authors included publications in the qualitative synthesis based on specific criteria, such as original research on HTN in MPNs, diagnosis, adult subjects, language, and availability of full text, while excluding others based on reasons like reviews, non-clinical investigations, and insufficient data.
The eligibility of identified publications was assessed through title and abstract screening, followed by a full-text examination, with disagreements resolved by consensus with a fourth investigator.
The methodological quality and risk of bias were assessed using MINORS and MMAT, respectively.
A meta-analysis was not possible due to heterogeneity in the manuscripts, but a systematic review was conducted and results were presented in different categories.
The literature search identified 598 potentially relevant records, with 74 manuscripts ultimately included in the qualitative synthesis after various stages of screening and evaluation.
Hypertension (HTN) is the most common comorbidity in myeloproliferative neoplasms (MPNs) with prevalence ranging from 50-90% in various studies.
HTN is associated with JAK2V617F mutation and is more common in polycythemia vera (PV) and essential thrombocythemia (ET) patients.
HTN is a common comorbidity in MPN patients with COVID-19, but does not impact survival.
PV patients with HTN exhibit distinct sympathetic nervous system activity, retinal microperfusion, and kidney artery resistive index compared to non-PV HTN patients.
HTN contributes to kidney dysfunction in MPN patients and is a risk factor for thrombotic events, particularly in ET and PMF/SMF.
MPN patients with HTN and high uric acid levels at diagnosis have a higher likelihood of kidney dysfunction.
MPN patients may exhibit a distinct diurnal blood pressure rhythm compared to the general hypertensive population.
52% of PMF/SMF patients with splenomegaly had increased BP, while HTN was the most common comorbidity in PMF/SMF.
HTN was the most prevalent comorbidity in PV patients enrolled in the United States Veterans Health Administration database, with around 72% prevalence.
HTN was more prevalent in high-risk PV patients compared to low-risk PV patients.
HTN was the #1 cardiovascular risk factor in MPNs and was prevalent in 63% of PV, 64% of ET, 15% of pre-fibrotic PMF, and 63% of PMF/SMF patients.
HTN was the most common comorbidity in ET and PV patients, with its prevalence varying across different MPN subtypes.
HTN was found to be the top comorbidity in myeloid cancers with no impact on survival in the COVID-19 setting.
Increased BP was found in 75% of PV subjects, with decreased heart rate values per 24 hours, decreased microneurography-evaluated muscle sympathetic nervous activity, and decreased serum free epinephrine and aldosterone concentrations in HTN+PV versus HTN non-PV patients.
HTN may aggravate MPN-related glomerulopathy via nephrosclerosis with the development of polar vasculosis and exudative lesions.
HTN was found to be a risk factor for kidney dysfunction and thrombotic events in ET and PMF/SMF patients.
ET patients with concomitant HTN had increased creatinine concentrations before treatment and experienced further increases after cytoreduction with hydroxyurea or anagrelide.
HTN was found to be more likely in PMF/SMF patients with high versus low uric acid levels at diagnosis.
PV patients were more likely to be non-dippers and have elevated nighttime SBP and DBP compared to hypertensive non-PV counterparts.
No significant differences were found in office or 24-hour SBP, DBP, heart rate, or use of antihypertensive agents in PV versus healthy counterparts, but signs of systolic and diastolic dysfunction of the heart were detected in PV patients.
Hypertension, T2DM, or smoking were predictors of major arterial thrombotic events in ET patients (HR = 1.91, 95% CI = 1.19-3.07, p = 0.007), but not of major venous thrombosis.
Hypertension was a risk factor for thrombosis development in ET (univariate model: HR = 3.43, p = 0.03; multivariate model: HR = 3.33, p = 0.07), and specifically arterial thrombosis (univariate model: HR = 3.76, p = 0.04).
Coexistence of two or more CVRFs was linked to thrombotic event development in ET patients (p = 0.02).
Hypertension and the presence of ≥1 CVRF were risk factors for thrombotic events in MPN patients (OR = 2.8, p < 0.001; OR = 3.2, p = 0.001, respectively).
The presence of CVRFs (HR = 2.33) and CVRFs + tobacco use (HR = 2.08) was linked with shorter overall survival in ET patients.
In MPN subjects, hypertension was the most common cardiovascular comorbidity, and its presence was associated with decreased survival in both PV (p = 0.014) and ET (p = 0.036).
Hypertension impacted thrombosis incidence in low-risk PV patients (IR = 0.85, 95% CI 0.57–1.25 vs. IR = 2.05, 95% CI 1.34–3.14, p = 0.025).
Hypertension emerged as a predictor of both major hemorrhages (HR = 1.33, p = 0.02) and thrombohemorrhagic complications (HR = 1.69, p = 0.04) in high-risk ET patients.
Patients with any CVRF were at an elevated risk for thrombosis (OR = 14.9, p = 0.003) and had lower thrombosis-free survival (~83% vs. 97%, p = 0.02) in a Spanish cohort of PMF/SMF subjects.
Thrombosis, but not hemorrhage, was more common in ET subjects with hypertension (p = 0.002 and p = 0.287, respectively).
Several studies reported no impact of hypertension on thrombosis development in MPNs, with some highlighting cigarette use as a more common risk factor.
Carobbio et al. (2011): HTN, T2DM, or smoking were predictors of major thrombotic events in ET patients (HR = 1.56, p = 0.038) and major arterial thrombotic events (HR = 1.91, p = 0.007), but not of major venous thrombosis.
Buxhofer-Ausch et al. (2014): HTN was a risk factor for thrombosis in ET patients (univariate model HR = 3.43, p = 0.03; multivariate model HR = 3.33, p = 0.07) and arterial thrombosis (univariate model HR = 3.76, p = 0.04), but not venous thrombosis.
Pósfai et al. (2015): Coexistence of two or more CVRFs was linked to thrombotic events development (p = 0.02), with thrombosis-free survival being lower in ET patients with ≥ 1 CVRF (p = 0.01) and in those with one CVRF vs. ≥ 2 CVRFs (p = 0.002).
Pósfai et al. (2014): HTN was a predisposing factor for thrombotic complications in females with ET (p = 0.001), with ≥ 2 CVRFs linked to a higher probability of thrombotic events (RR = 4.728, p = 0.01).
Horvat et al. (2018): HTN and presence of ≥ 1 CVRF were risk factors for thrombotic events, especially arterial thrombosis, in PV and PMF patients, with both factors also being risk factors for overall thrombosis, arterial and venous thrombosis separately in ET.
Lekovic et al. (2014): HTN and CVRFs were associated with the development of arterial and global thrombosis in ET patients (p = 0.01 and p = 0.001, respectively).
Lekovic et al. (2015): Presence of CVRFs and CVRFs + tobacco use were linked with shorter overall survival in ET patients (HR = 2.33 and HR = 2.08, respectively).
Schwarz et al. (2015): HTN was a predictor of overall thrombosis, major thrombosis, and arterial thrombosis in MPNs treated with anagrelide, and was the best predictor of arterial thrombotic events in the multivariate analysis (OR = 1.813, p = 0.001).
Accurso et al. (2020): CVRFs were associated with decreased survival in PV (p = 0.014) and ET (p = 0.036) patients.
Benevolo et al. (2021): HTN (HR = 1.77, p = 0.04) and previous history of thrombosis (HR = 2.10, p = 0.01) increased the risk of thrombosis in PV patients.
Birgegård et al. (2018): HTN was a predictor of major hemorrhages (HR = 1.33, p = 0.02) and thrombohemorrhagic complications (HR = 1.69, p = 0.04) in ET patients.
Cervantes et al. (2006): Patients with any CVRF were at an elevated risk for thrombosis (OR = 14.9, p = 0.003) and had lower
ACEIs as the first choice for managing HTN in PV can reduce chemotherapy use and improve kidney function, with no significant difference in thrombosis-free survival.
Lisinopril monotherapy led to decreased blood pressure, improved BP variability, and reached target BP in 65% of PV patients with HTN without side effects.
HTN is a common comorbidity in blood cancer patients and is a predictor of treatment modifications.
Ruxolitinib does not significantly affect DBP but increases SBP, and drug-induced HTN is a frequently underdiagnosed entity.
Ruxolitinib-related HTN is generally mild and manageable, occurring at different grades and frequencies across various studies.
AT9283, a small molecule inhibitor, caused HTN as a dose-limiting toxicity in a study on refractory AML and advanced PMF/SMF.
Givinostat in PV led to HTN as a grade 3 adverse event in only one patient out of 50.
Gotic et al.'s study found HTN as the most frequent vascular disorder in ET subjects treated with anagrelide or hydroxyurea, and Tortorella et al. discovered that cardiovascular assessment before anagrelide treatment doesn't predict adverse events in ET patients.
Hypertension (HTN) is the most common comorbidity in myeloproliferative neoplasms (MPNs), with the JAK2V617F mutation possibly implicated in systemic and pulmonary arterial hypertension.
HTN is prevalent in MPN patients with COVID-19, but not associated with significant morbidity or mortality increases; it correlates with other cardiovascular risk factors in MPN patients.
HTN in MPNs increases the risk for organ dysfunction and is linked to altered cardiac physiology and neural control of blood pressure.
Hypertension and other cardiovascular risk factors contribute to thrombotic events in MPNs, with HTN more closely related to arterial rather than venous thrombotic events.
Some studies report no correlation between HTN and arterial/venous thrombotic events in MPNs, while others find HTN associated with CNS thrombotic phenomena.
ACEIs are the first choice for managing HTN in PV, showing reduction in chemotherapy use, improved kidney function, and increased eGFR, but without altering thrombosis-free survival.
Ruxolitinib, a JAK2/STAT3 inhibitor, is associated with HTN, hyperlipidemia, and increased BMI in MPN treatment, necessitating dietary counseling and lifestyle modifications.
AT9283 and anagrelide cause HTN in some patients, but anagrelide-induced HTN can be managed without discontinuing the drug.
HTN is a common comorbidity in MPNs, influencing thrombosis risk, management strategies, and patient survival, and this systematic review is the first to examine the interplay between primary arterial HTN and drug-induced HTN in MPNs.
Future research should focus on molecular assessments and genomic-directed stratification to understand the interplay between MPNs and HTN, with the aim of improving prognostication and treatment selection.
Clonal hematopoiesis of indeterminate potential (CHIP) may contribute to MPN development and cardiometabolic disorders, with future treatments potentially focusing on antioxidant and anti-inflammatory properties.
MPN pathogenesis involves genetic mutations and a series of maladaptive events leading to increased blood viscosity, vascular resistance, and arterial hypertension.
This systematic review is the first to examine the relationship between MPNs and primary arterial HTN, and drug-induced HTN, though limitations include the inability to compute a meta-analysis and HTN not being a primary outcome in some studies.
HTN is the most common comorbidity in MPNs, affecting thrombosis occurrence and survival, with drug-induced HTN posing a management challenge and necessitating further research on patient characteristics and HTN's contributions to complications.
Primary Arterial Hypertension and Drug-Induced Hypertension in MPNs: A Systematic Review
(Message: High BP is extremely common in MPNs. Get your blood pressure checked, and have it treated if at all possible. ACE inhibitors like lisinopril are most promising regarding outcomes)
A total of 74 manuscripts were entered into the qualitative synthesis and included in the present systematic review. Our systematic review highlights that Hypertension is the most common comorbidity encountered in MPNs, with an impact on both the occurrence of thrombosis and survival.
Cardiovascular Disease in Myeloproliferative Neoplasms: JACC: CardioOncology State-of-the-Art Review
(Anti-inflammatories might be helpful for MPNs just like they've proved helpful for CVD)
The authors review the pathophysiologic mechanisms of cardiovascular complications of myeloproliferative neoplasms, which involve inflammation, prothrombotic and profibrotic factors (including transforming growth factor–beta and lysyl oxidase), and abnormal function of circulating clones of mutated leukocytes and platelets from affected individuals. Anti-inflammatory therapies may provide cardiovascular benefit in patients with myeloproliferative neoplasms, a hypothesis that requires rigorous evaluation in clinical trials.
RENIN-ANGIOTENSIN SYSTEM (RAS) ALTERATIONS IN MPNS AND ATHEROSCLEROSIS
A dysregulated renin-angiotensin system causes deleterious effects on the cardiovascular system.80 Increased renin-angiotensin system activation in the bone marrow of patients may result from overactivity of the JAK/STAT signaling pathway in MPNs.158 Additionally, the use of angiotensin-converting enzyme inhibitors in patients with polycythemia vera improved hematocrit levels and reduced the need for cytoreductive drugs.159 Similarly, mice with experimental myelofibrosis treated with captopril (an angiotensin-converting enzyme inhibitor) have reduced splenomegaly and bone marrow fibrosis.160
Impact of Inflammation on Myeloproliferative Neoplasm Symptom Development, 2015
Myeloproliferative neoplasms (essential thrombocythemia, ET; polycythemia vera, PV; myelofibrosis, MF) are monoclonal malignancies associated with genomic instability, dysregulated signaling pathways, and subsequent overproduction of inflammatory markers. Acknowledged for their debilitating symptom profiles, recent investigations have aimed to determine the identity of these markers, the upstream sources stimulating their development, their prevalence within the MPN population, and the role they play in symptom development. Creation of dedicated Patient Reported Outcome (PRO) tools, in combination with expanded access to cytokine analysis technology, has resulted in a surge of investigations evaluating the potential associations between symptoms and inflammation. Emerging data demonstrates clear relationships between individual MPN symptoms (fatigue, abdominal complaints, microvascular symptoms, and constitutional symptoms) and cytokines, particularly IL-1, IL-6, IL-8, and TNF-α. Information is also compiling on the role symptoms paradoxically play in the development of cytokines, as in the case of fatigue-driven sedentary lifestyles. In this paper, we explore the symptoms inherent to the MPN disorders and the potential role inflammation plays in their development.
The past half-century has shed light on the development of myeloproliferative neoplasms (MPNs) and their impact on quality of life, with inflammation playing a critical role in their pathobiology, disease progression, and symptom development.
MPN symptoms, including fatigue, early satiety, and abdominal pain, significantly impact patients' daily living and overall quality of life, with many feeling anxious and worried about their conditions, and symptoms often promoting the development of other symptoms.
Symptom prevalence and severity vary among MPN subtypes, and recent studies have shown significant heterogeneity even within these subtypes, with symptomatology presenting independently of disease stage and risk scores.
The first investigation to systematically analyze MPN symptoms revealed the limitations of available treatments and contributed to the development of three MPN-specific patient-reported outcome (PRO) tools: MF-SAF, MPN-SAF, and MPN-SAF TSS/MPN-10.
The MF-SAF, MPN-SAF, and MPN-SAF TSS (MPN-10) are PRO tools designed to capture and assess the most common symptoms within myelofibrosis, PV and ET, and have been used to evaluate various novel targeted compounds.
Dysregulation of the inflammatory cascade is a hallmark feature of MPNs, which arise from genetic defects in pluripotent stem cell populations, with JAK2V617F being the first recognized mutation; cytokine dysregulation is also associated with other MPN mutations.
Chronic inflammation is hypothesized to support oncogenesis through various mechanisms; MPN disorders involve a perpetual cycle of DNA damage, cellular remodeling, and fibrosis, which is of great interest in relation to the heterozygous clinical presentation of MPN patients.
In myelofibrosis (MF), specific cytokines are independently predictive of inferior survival and associated with transfusion needs and splenomegaly; a study found that changing levels of five cytokines was significantly associated with changes in MPN-SAF TSS.
IL-8 plays a unique role in MPNs, and various cytokines are associated with specific MPN types, such as polycythemia vera (PV) and essential thrombocythemia (ET); some cytokines may serve as markers to distinguish between PV and ET.
The combination of inflammatory markers is as important as the type of factor present, and specific inflammatory markers are associated with disease severity and complications; the presence of specific gene mutations impacts the type and degree of cytokine expression.
Fatigue is a common symptom in MPN patients, and cytokines have been documented to induce fatigue in both malignant and nonmalignant states; anemia and cytokine-induced hypocortisolism contribute to fatigue, and cancer-related depression and fatigue contribute to a sedentary lifestyle that encourages a proinflammatory state.
Abdominal complaints in MPN patients are largely attributable to splenomegaly and other factors, but cytokines may also play a role in symptom development; cytokines are associated with splenomegaly and abdominal pain, and cytokine-induced nerve hyperstimulation may exacerbate abdominal pain.
Microvascular symptoms in MPNs result from capillary-level disease activity and may include cognitive symptoms; proinflammatory cytokines disrupt neurotransmitters like serotonin, dopamine, and norepinephrine, which are crucial for sleep, mood, and memory.
Inflammation's role in cognitive impairment has been studied in animals and humans; IL-6 plays a key role in interrupting memory and learning processes, while IL-1, TNF-α, IL-6, and CRP are linked to impaired memory and neurodegenerative disorders in the elderly.
Pruritus is linked to the inflammatory cascade, with mast cells and basophils potentially playing a role; PV patients show the highest prevalence of pruritus (65%).
Constitutional symptoms in MPNs, such as fevers, night sweats, and weight loss, are partially cytokine-driven and linked to cancer-cachexia, which is associated with a dismal survival rate.
Targeting cytokines to improve MPN symptoms includes increasing physical activity and reducing fat intake, which may reduce inflammatory cytokines and improve survival; patient activity programs may impact cytokine-induced symptomatology.
JAK2 inhibition has become a rational target for preventing cytokine dysregulation, with ruxolitinib therapy inducing profound reductions in TNF-α and MIP-1α expression, and improving symptoms such as itching, night sweats, and weight loss.
Emerging JAK2 inhibitors like momelotinib and pacritinib, and other cellular signaling networks like the PI3K-Akt-mTOR pathway, are potential targets for intervention in MPN symptom management.
Clear relationships exist between MPN symptoms and markers of inflammation, but more research is needed to understand how these markers differ between MPN subtypes, change with disease progression, and relate to transformation; targeted agents provide a platform for inhibiting cytokine signals early and limiting potential toxicity.
MOLECULAR PROFILING REVEALS HIGHLY DEREGULATED INSULIN GROWTH FACTOR BINDING PROTEINS IN PATIENTS WITH MYELOFIBROSIS AND RELATED NEOPLASMS
Background:
The Insulin Growth Factor (IGF) system has been extensively studied in polycythemia vera (PV) showing erythroid progenitors to be hypersensitive to IGF1, levels of the IGF1-binding protein – IGFBP-1 to be fourfold increased but normal levels of IGF1 and IGFBP3. Furthermore, the stimulatory effect of IGFBP1 on erythroid progenitors in vitro provided a connection to overproduction of red blood cells in PV through IGF1. Most lately, increased IGF-1R expression of mononuclear cells was found in patients with Philadelphia-negative myeloproliferative neoplasms (MPN). In addition, the JAK2V617F mutation has been shown to result in IGF1 hypersensitivity in Ba/F3 cells providing a molecular basis for significance of IGF1 signaling in MPNs.
Dysregulation of the IGF system is important in cancer development. We herein for the first time demonstrate several genes of IGF system to be markedly deregulated in MPNs
Aims:
To study whole blood gene expression profiling in patients with MPNs.
Methods:
Gene expression microarrays were applied to whole blood from control subjects (n = 21) and patients with ET (n = 19), PV (n = 41), and PMF (n = 9). Affymetrix HG-U133 2.0 Plus microarrays were used to generate gene expression profiles of 54.675 probe sets (38.500 genes). Total RNA was purified from whole-blood, amplified to biotin-labeled aRNA and hybridized to microarray chips. The statistical software R was applied to perform initial data processing and statistical analysis of microarray data.
Results:
20,439, 25,307, and 17,417 probe sets were significantly differentially expressed between control subjects and patients with ET, PV and PMF, respectively (FDR<0.05). Several of the insulin-like growth factor (IGF) and insulin-like growth factor binding protein (IGFBP) genes were significantly deregulated (Table 1). IGF1, IGF2, IGFALS, IGFBP2, and IGF2BP1 were significantly upregulated in all three disease entities of which IGFBP2 was progressively and significantly upregulated from ET over PV to PMF (FDR<0.05).
Summary/Conclusion:
In the present study we found several IGF-related genes to be significantly deregulated in MPNs. Of note, IGF-1 was significantly upregulated in all three subgroups of patients (ET, PV and PMF) and IGFBP1 was significantly downregulated in ET and PV patients. These observations are not in line with previous findings of normal IGF-1 and highly elevated IGFBP1 levels in patients with PV. IGF-1 has been shown to stimulate cell growth and up-and down-regulate the expression of anti- and pro-apoptotic molecules, respectively, thereby protecting cancer cells from apoptosis. Enhanced IGF-I gene expression might contribute to the chronic inflammatory state in MPN through enhancement of IL-6 activity. It is intriguing to consider if IGF-1 might also promote angiogenesis in MPN by stimulating VEGF secretion by e.g. megakaryocytes and monocytes similar to stimulation of VEGF-secretion by e.g. myeloma cells. In conclusion, we have shown a number of genes in the IGF-1 system to be deregulated in MPN, which altogether might contribute in driving clonal myeloproliferation, decreased apoptosis, bone marrow angiogenesis, immune evasion and inflammation as well. Future studies on the interplay between the transcriptome, IGF-related proteins and IGF-R expression levels might deliver new insight into the role of IGF-system in the pathogenesis of MPNs and ultimately give the impetus to studies on the efficacy of inhibitors of IGF1 or IGF1R, which prohibit development of MPN-phenotype in JAK2V617F mice.
AXL
Escape from Type II JAK2 Inhibition in MPN Depends on AXL/MAPK Activation and Is Targetable, 2022
AXL Inhibition Represents a Novel Therapeutic Approach in BCR-ABL Negative Myeloproliferative Neoplasms, 2021
AXL Inhibition Extinguishes Primitive JAK2 Mutated Myeloproliferative Neoplasm Progenitor Cells, 2019


Comments