Acarbose
13.5% average mice life extension (ref), more effective in male mice.
Mimics low carb diet (lowers glucose, trigs, insulin).
50% reduction in Cardio Vascular Disease (CVD) in insulin resistant (ref).
Reduces PP glucose peak by 66%+ while avoiding sugar crashes (ref).
Reduces fasting insulin by ~10%, and insulin resistance score by 15-25% (ref, ref).
Lowers trigs by ~20% in obese (ref); lowers trigs throughout the day by 32% in T2D (ref).
Makes you feel fuller; aids weight loss.
Lowers inflammatory markers such as HS-CRP, IL6 etc in T2D (ref, ref).
Slows cancer growth in Kidney Cancer animal models (ref). Associated with 14% reduced risk of developing any cancer in T2D humans (ref).
Effects appear additive with Metformin.
Benefits aren’t immediate but they’re cumulative. They increase over time (initially months, then years).
Raises serum butyrate in human subjects with impaired glucose tolerance (ref).
Typical dose: 25-100mg with meals (ref).
Mice lifespan extension
In studies conducted by three independent laboratories by the US National Institute on Aging's intervention testing programme, acarbose was shown to extend the lifespan of female mice by 5% and of male mice by 22%.[11][12]
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4620230/
Acarbose given orally blocks intestinal alpha glucosidase so that carbohydrates are not broken down and absorbed. This results in lower blood glucose levels and prevents postprandial insulin spikes. The lower blood glucose and decreased need for insulin activate adenosine monophosphate-activated protein kinase, which tends to block mtorc1, the drug target for rapamycin. The lowered blood glucose provides less available substrate for mitochondrial metabolism thereby sensitizing mitochondria to increased electron transport chain (ETC) efficiency induced by SS31-bound cardiolipin. The decreased need for insulin helps alleviate insulin resistance induced by rapamycin-suppressed mtorc2. (link)
With acarbose treatment, the mean fasting cholesterol level fell from 214±19 to 187±15 mg/dL, p<0.03, the mean high-density lipoprotein (HDL) cholesterol level rose from 41±4 to 44±7 mg/dL, p>0.05, and the HDL to total cholesterol (TC) ratio increased from 0.20±0.02 to 0.24±0.03, p<0.05. The triglyceride levels in patients on acarbose were lower throughout the day and the integrated area under the triglyceride concentration curve was 16 211 ±2875 mg/dL/h pretreatment compared to 11 127 ±1827 mg/dL/h post-treatment (p<0.05). (link)
Acarbose, 17-α-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males, 2014
Four agents — acarbose (ACA), 17-α-estradiol (EST), nordihydroguaiaretic acid (NDGA), and methylene blue (MB) — were evaluated for lifespan effects in genetically heterogeneous mice tested at three sites. Acarbose increased male median lifespan by 22% (P < 0.0001), but increased female median lifespan by only 5% (P = 0.01). This sexual dimorphism in ACA lifespan effect could not be explained by differences in effects on weight. Maximum lifespan (90th percentile) increased 11% (P < 0.001) in males and 9% (P = 0.001) in females. EST increased male median lifespan by 12% (P = 0.002), but did not lead to a significant effect on maximum lifespan. The benefits of EST were much stronger at one test site than at the other two and were not explained by effects on body weight. EST did not alter female lifespan. NDGA increased male median lifespan by 8–10% at three different doses, with P-values ranging from 0.04 to 0.005. Females did not show a lifespan benefit from NDGA, even at a dose that produced blood levels similar to those in males, which did show a strong lifespan benefit. MB did not alter median lifespan of males or females, but did produce a small, statistically significant (6%, P = 0.004) increase in female maximum lifespan. These results provide new pharmacological models for exploring processes that regulate the timing of aging and late-life diseases, and in particular for testing hypotheses about sexual dimorphism in aging and health.
Acarbose Treatment and the Risk of Cardiovascular Disease and Hypertension in Patients With Impaired Glucose Tolerance, 2003
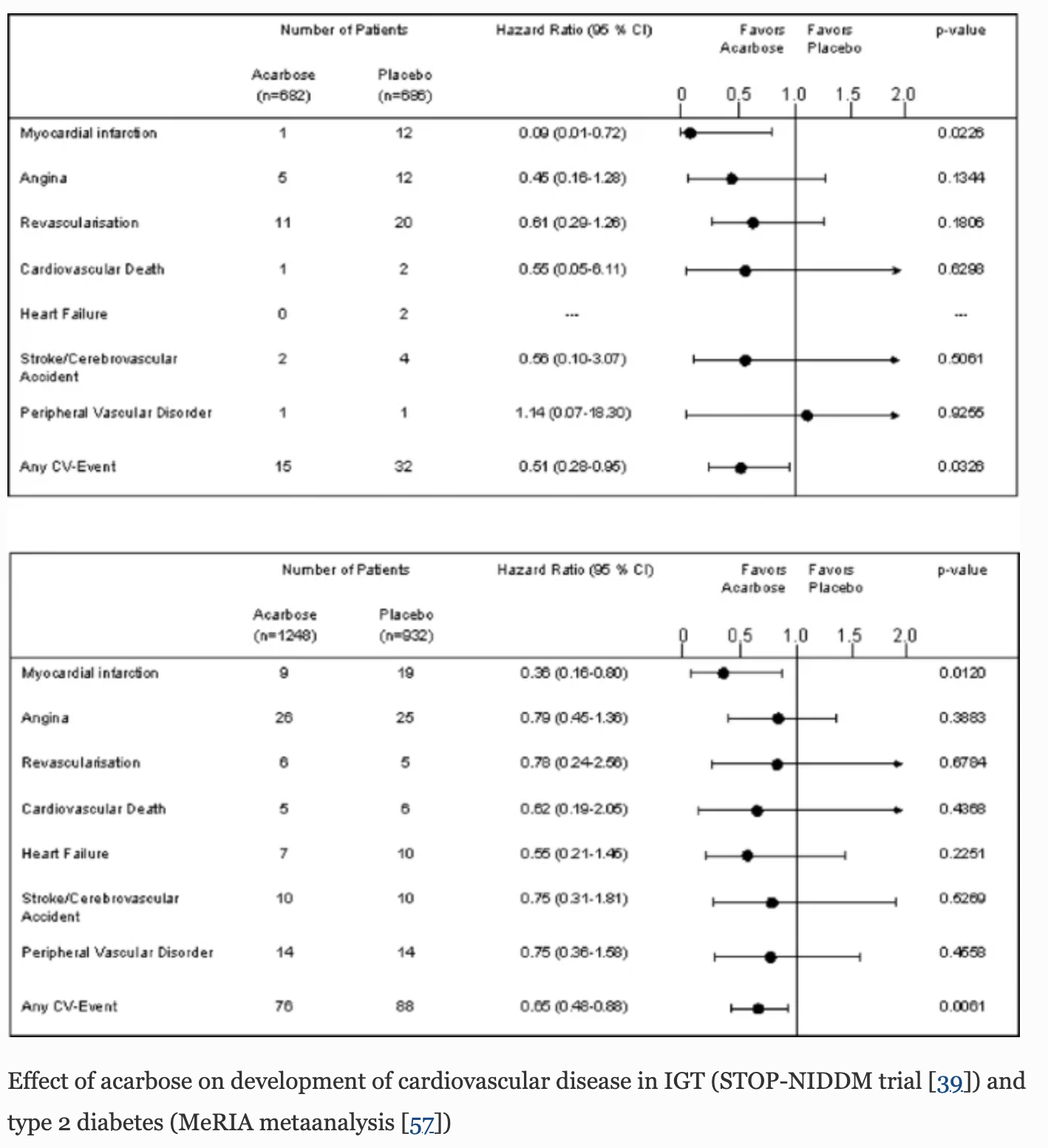
The STOP-NIDDM Trial
Objective To evaluate the effect of decreasing postprandial hyperglycemia with acarbose, an α-glucosidase inhibitor, on the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance (IGT).
Design, Setting, and Participants International, multicenter double-blind, placebo-controlled, randomized trial, undertaken in hospitals in Canada, Germany, Austria, Norway, Denmark, Sweden, Finland, Israel, and Spain from July 1998 through August 2001. A total of 1429 patients with IGT were randomized with 61 patients (4%) excluded because they did not have IGT or had no postrandomization data, leaving 1368 patients for a modified intent-to-treat analysis. Both men (49%) and women (51%) participated with a mean (SD) age of 54.5 (7.9) years and body mass index of 30.9 (4.2). These patients were followed up for a mean (SD) of 3.3 (1.2) years.
Intervention Patients with IGT were randomized to receive either placebo (n = 715) or 100 mg of acarbose 3 times a day (n = 714).
Main Outcome Measures The development of major cardiovascular events (coronary heart disease, cardiovascular death, congestive heart failure, cerebrovascular event, and peripheral vascular disease) and hypertension (≥140/90 mm Hg).
Conclusion Treating impaired glucose tolerance (IGT) patients with acarbose is associated with a significant reduction in the risk of cardiovascular disease and hypertension: 49% relative risk reduction in the development of cardiovascular events (hazard ratio [HR], 0.51; 95% confidence interval [CI]; 0.28-0.95; P = .03). Among cardiovascular events, the major reduction was in the risk of myocardial infarction (HR, 0.09; 95% CI, 0.01-0.72; P = .02). Acarbose was also associated with a 34% relative risk reduction in the incidence of new cases of hypertension (HR, 0.66; 95% CI, 0.49-0.89; P = .006) and a 5.3% absolute risk reduction. Even after adjusting for major risk factors, the reduction in the risk of cardiovascular events (HR, 0.47; 95% CI, 0.24-0.90; P = .02) and hypertension (HR, 0.62; 95% CI, 0.45-0.86; P = .004) associated with acarbose treatment was still statistically significant.
Acarbose treatment was associated with a significant reduction in body weight, BMI, and waist circumference, in blood pressure, in 2-hour plasma glucose concentration, and in triglyceride levels.
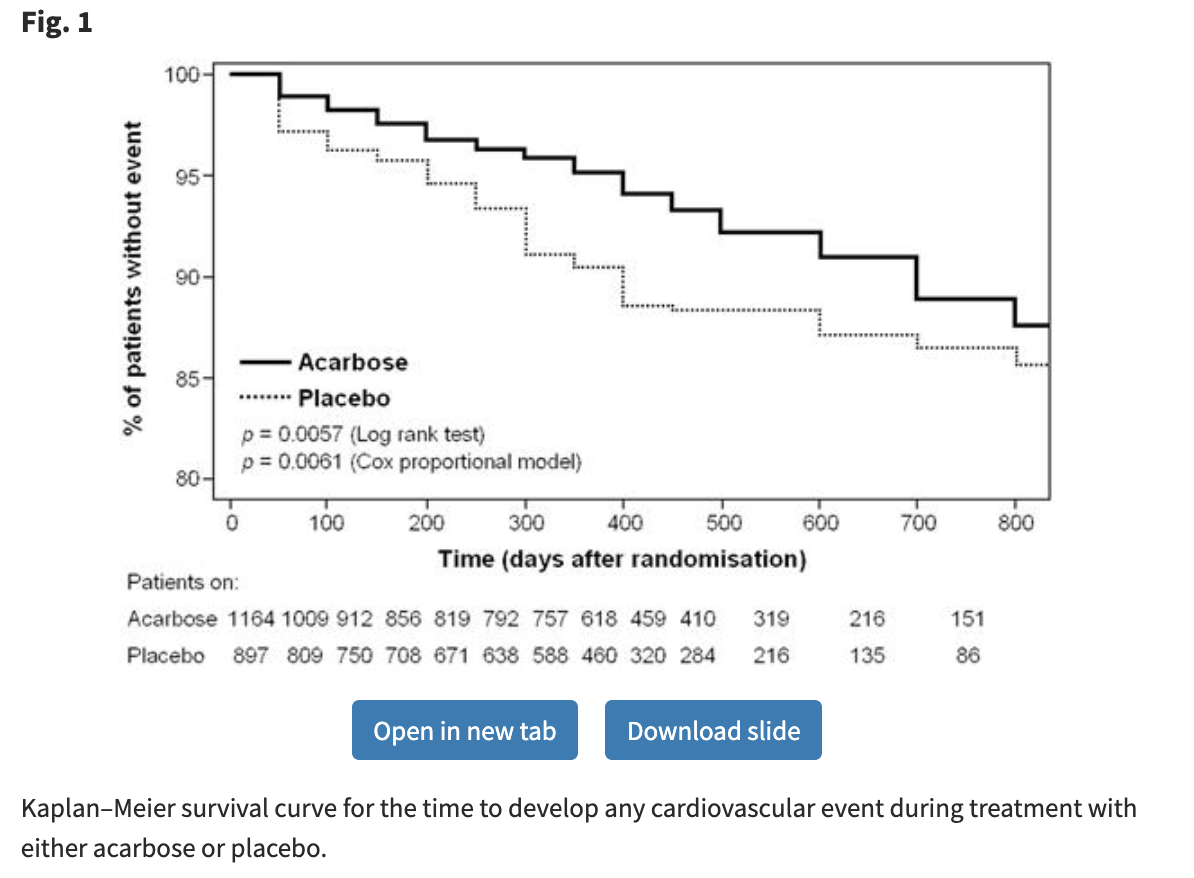
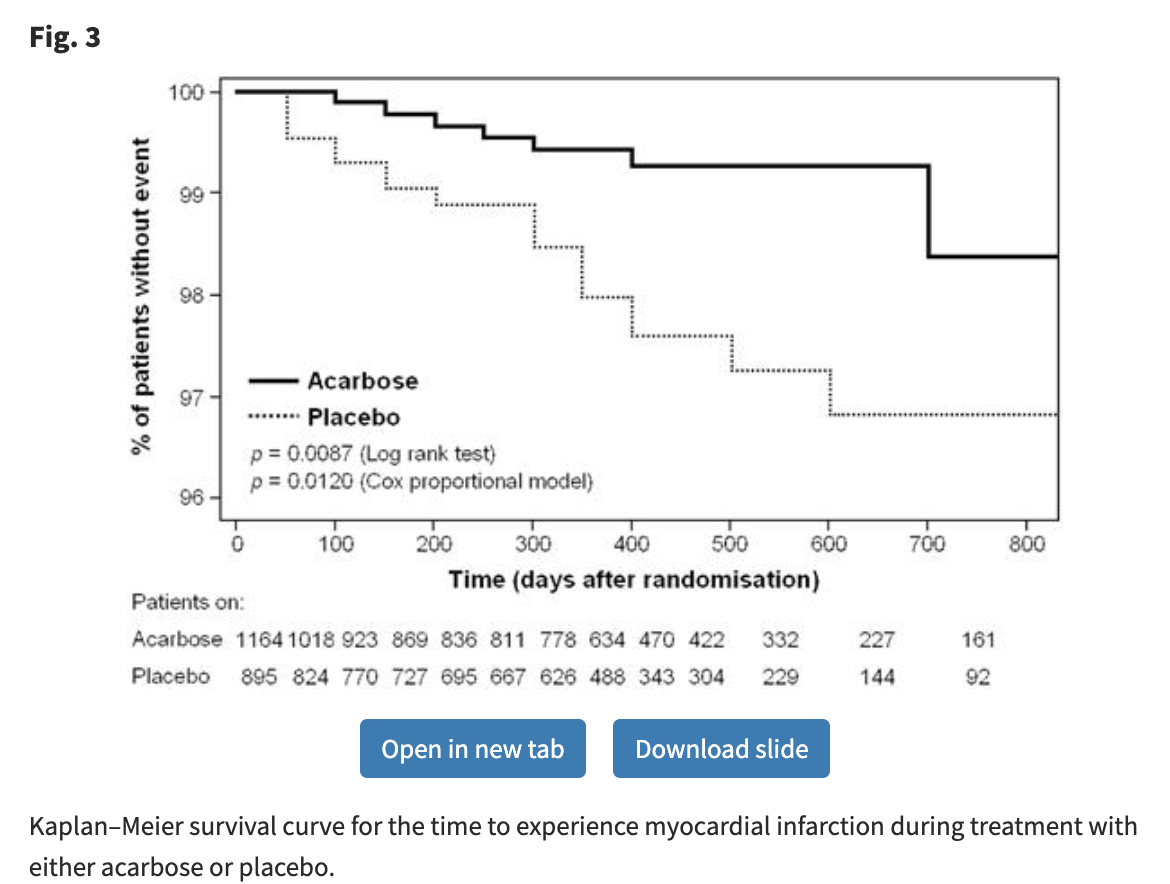
Acarbose reduces the risk for myocardial infarction in type 2 diabetic patients: meta-analysis of seven long-term studies, 2004
This meta-analysis included seven randomized, double-blind, placebo-controlled acarbose studies with a minimum treatment duration of 52 weeks. Type 2 diabetic patients valid for safety were randomized to either acarbose (n=1248) or placebo (n=932). The primary outcome measure was the time to develop a cardiovascular event. Primary analysis was conducted using Cox regression analysis. The effect of acarbose on metabolic parameters was also investigated. Acarbose therapy showed favourable trends towards risk reduction for all selected cardiovascular event categories. The treatment significantly reduced the risk for ‘myocardial infarction’ (hazards ratio=0.36 [95% Cl 0.16–0.80], P=0.0120) and ‘any cardiovascular event’ (0.65 [95% Cl 0.48–0.88], P=0.0061). Glycaemic control, triglyceride levels, body weight and systolic blood pressure also improved significantly during acarbose treatment.
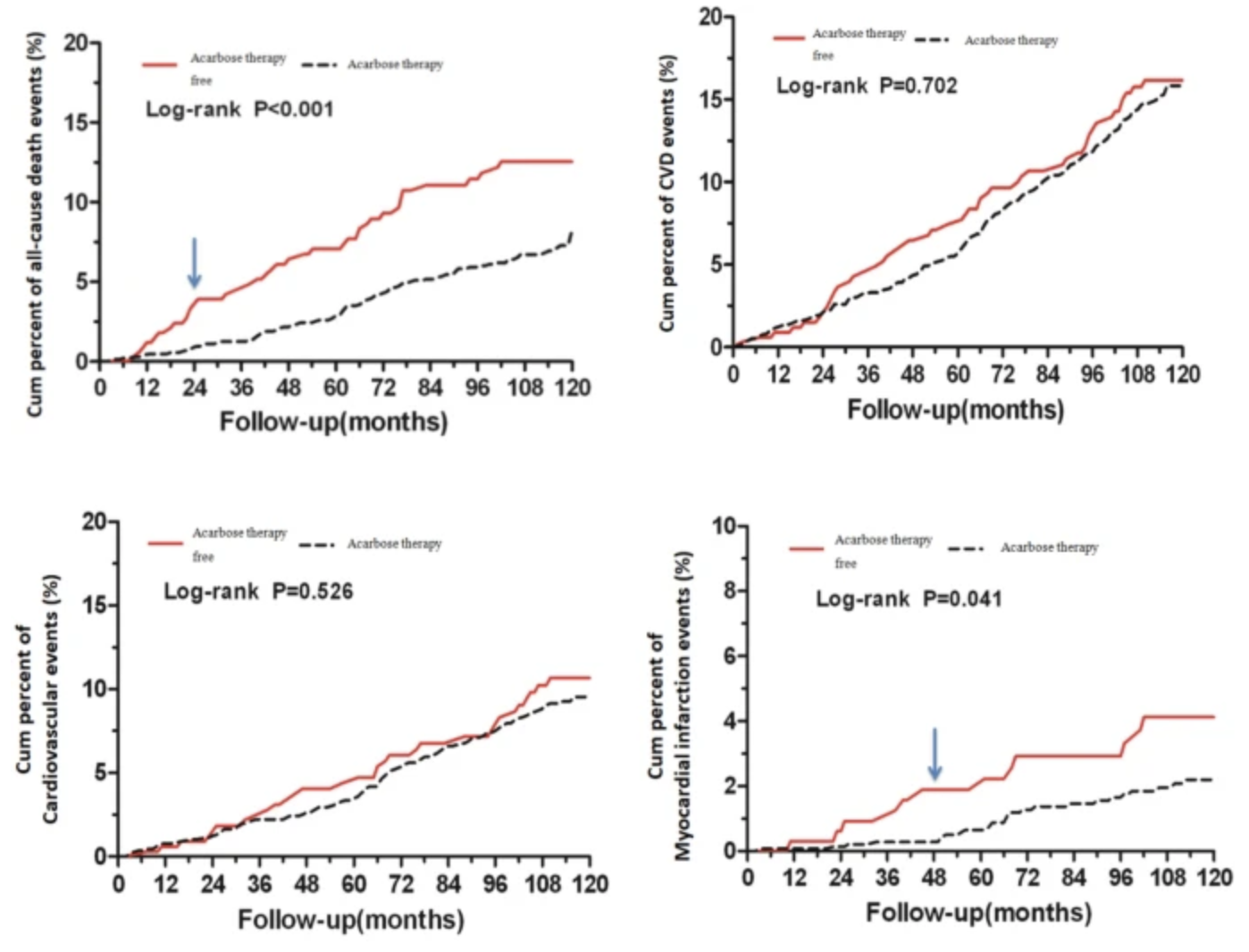
The effects of acarbose therapy on reductions of myocardial infarction and all-cause death in T2DM during 10-year multifactorial interventions (The Beijing Community Diabetes Study 24), 2021
To investigate the potential benefits of acarbose therapy on cardiovascular events (CVD) in Type 2 diabetes (T2DM) in an urban community over 10-year follow-up. The study population of Beijing Community Diabetes Study (BCDS) were type 2 diabetes (T2DM) living in 21 communities in Beijing. All patients received comprehensive intervention in accordance with the Chinese guidelines for the prevention and treatment of diabetes. Professors in endocrinology from top tier hospitals regularly visited the communities for consultations, which was a feature of this study. A total of 1797 T2DM in BCDS study had complete screening data, including blood glucose, blood pressure, lipid profiles and acarbose continuous therapy. After 10-year follow-up, the risks of CVD outcomes were assessed according to whether patients had received acarbose therapy or not. All patients were followed-up to assess the long-term effects of the multifactorial interventions. At baseline, compared with the acarbose therapy free in T2DM, there was no significant difference in achieving the joint target control in patients with acarbose therapy. From the beginning of 8th year follow-up, the joint target control rate in patients with acarbose therapy was significantly higher than that of acarbose therapy free. During the 10-year follow-up, a total of 446 endpoint events occurred, including all-cause death, cardiovascular events, cerebrovascular events. The incidences of myocardial infarction (from the 4th year of follow-up) and all-cause death (from the 2nd year of follow-up) in patients who received acarbose therapy were significantly lower than that of acarbose therapy free respectively. In Cox multivariate analyses, there were significant differences in incidences of myocardial infarction and all-cause death between afore two groups during the 10-year follow-up, and the adjusted HRs were 0.50 and 0.52, respectively. After multifactorial interventions, T2DM with acarbose therapy revealed significant reductions of myocardial infarction and all-cause death. The long-term effects of with acarbose therapy on improving joint target control might be one of the main reasons of myocardial infarction and all-cause death reduction.
The quest to slow ageing through drug discovery, 2020
Although death is inevitable, individuals have long sought to alter the course of the
ageing process. Indeed, ageing has proved to be modifiable; by intervening in biological systems, such as nutrient sensing, cellular senescence, the systemic environment and the gut microbiome, phenotypes of ageing can be slowed sufficiently to mitigate age-related functional decline. These interventions can also delay the onset of many disabling, chronic diseases, including cancer, cardiovascular disease and neurodegeneration, in animal models. Here, we examine the most promising interventions to slow ageing and group them into two tiers based on the robustness of the preclinical, and some clinical, results, in which the top tier includes rapamycin, senolytics, metformin, acarbose, spermidine, NAD+ enhancers and lithium. We then focus on the potential of the interventions and the feasibility of conducting clinical trials with these agents, with the overall aim of maintaining health for longer before the end of life.
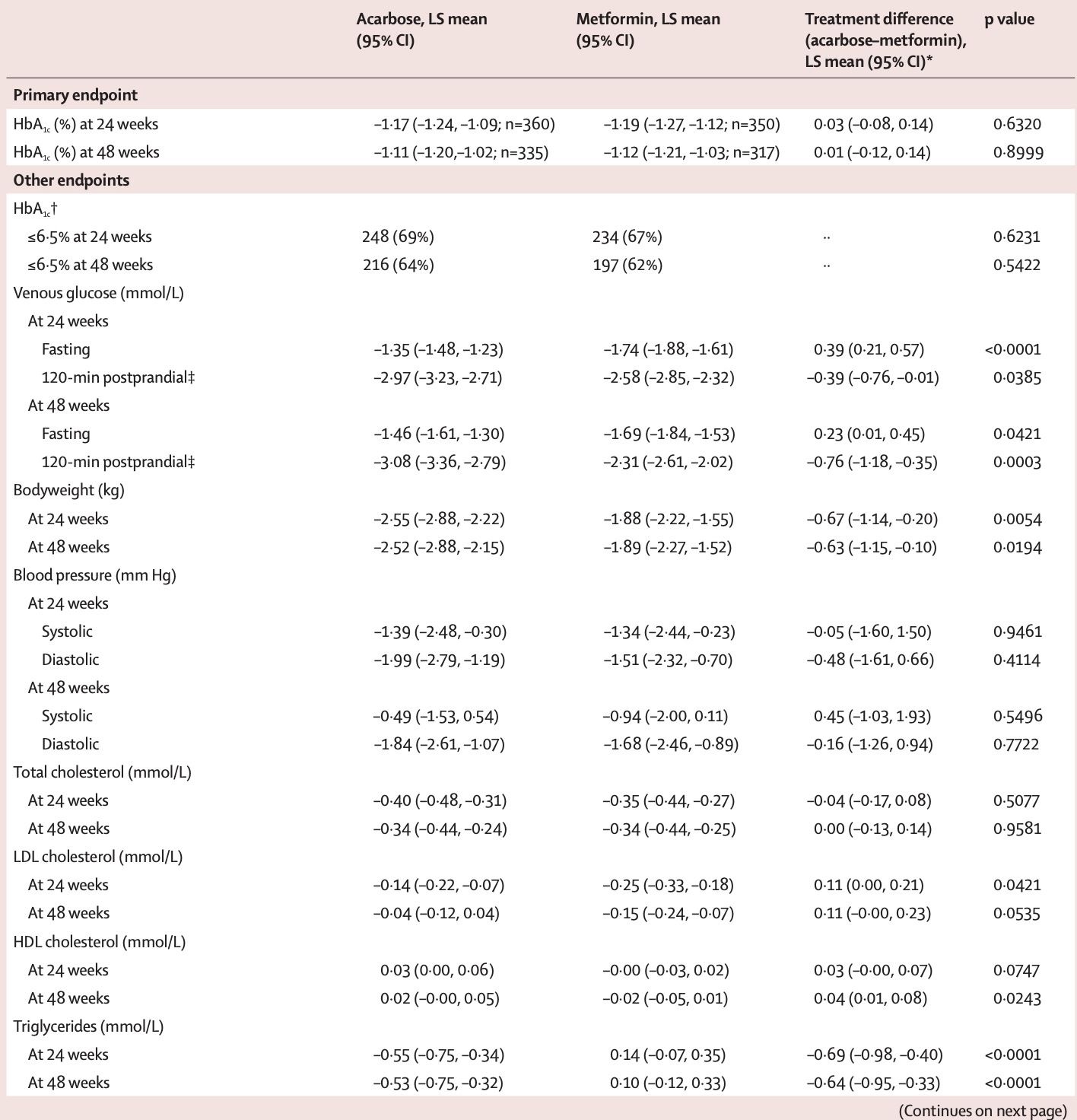
Acarbose compared with metformin as initial therapy in patients with newly diagnosed type 2 diabetes: an open-label, non-inferiority randomised trial

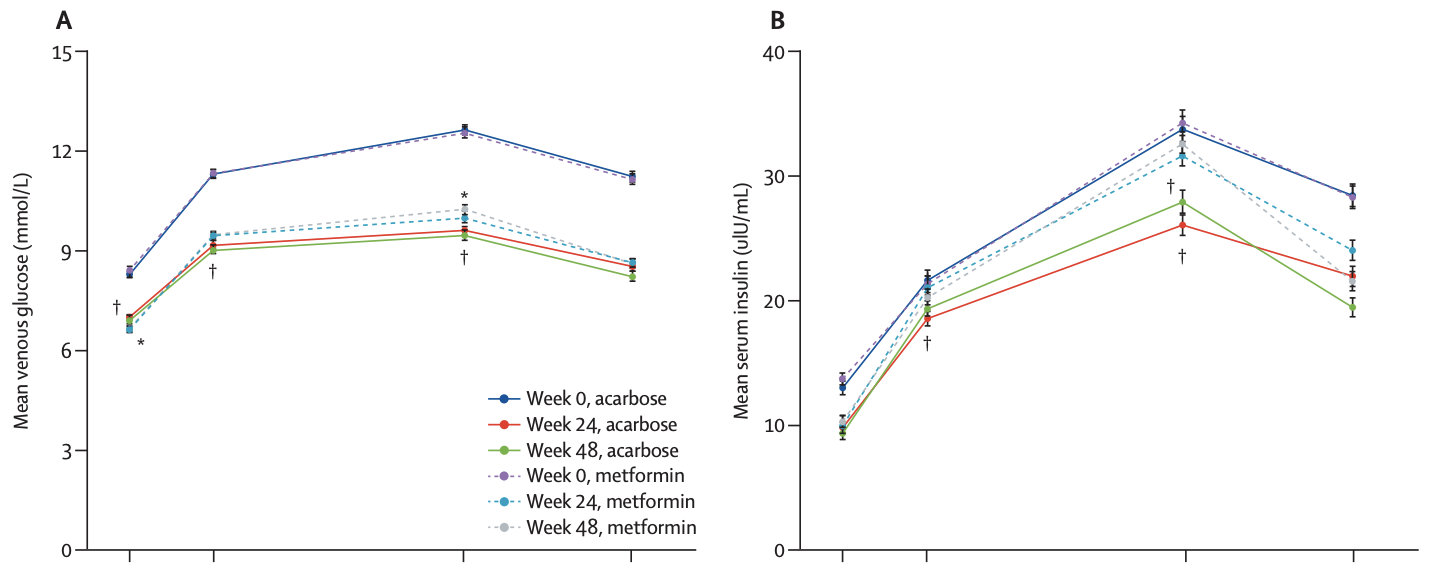
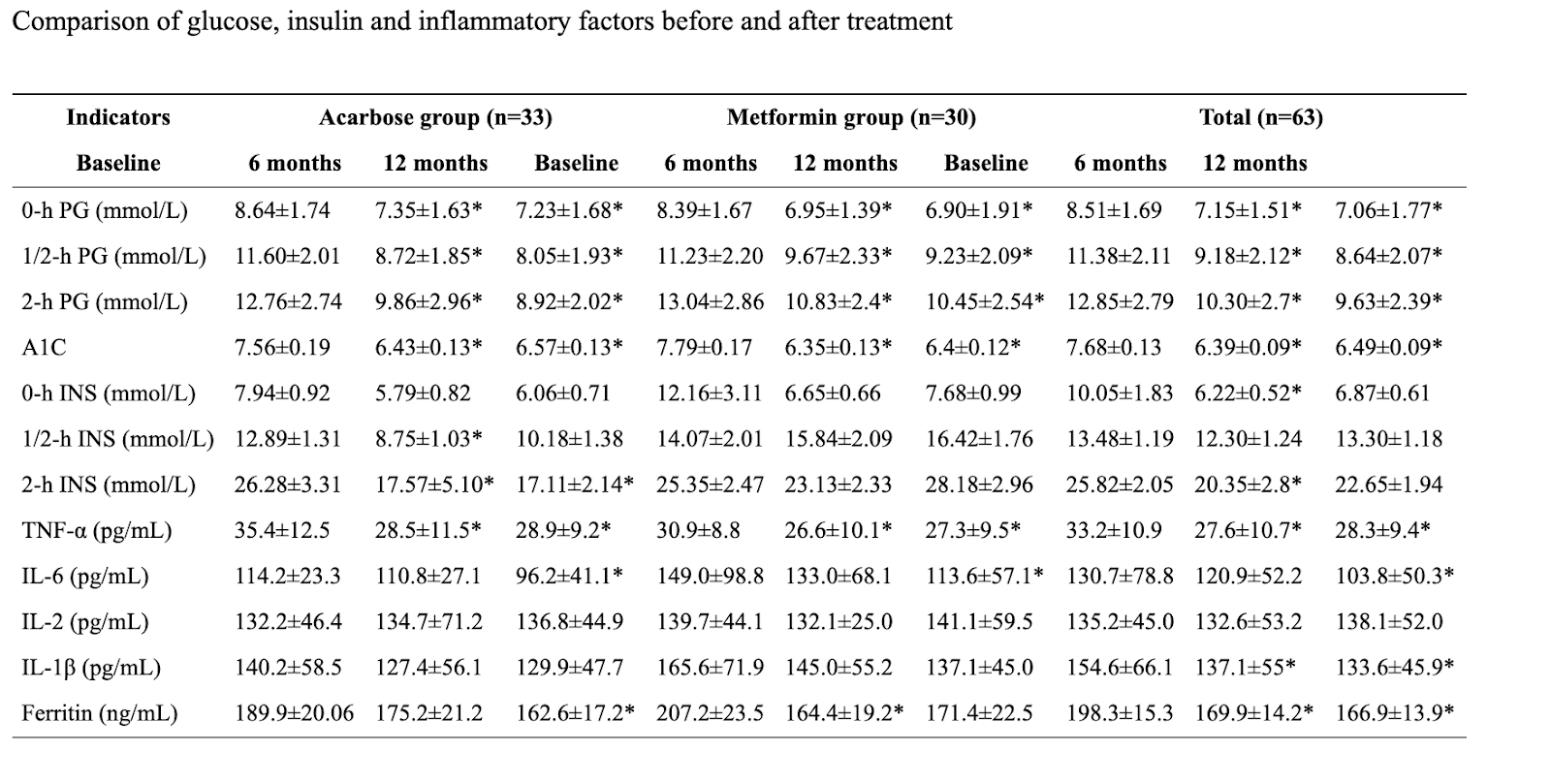
Effects of acarbose and metformin on the inflammatory state in newly diagnosed type 2 diabetes patients: a one-year randomized clinical study, 2019
Conclusion
Patients with newly diagnosed T2DM exhibited a marked chronic inflammatory state characterized by increased IL-6, TNF-α, IL-1β, IL-2 and ferritin levels. After 1 year of treatment with acarbose or metformin, IL-6, TNF-α, IL-1β and ferritin levels were significantly decreased compared with the baseline. The anti-inflammatory effects of acarbose and metformin were comparable and required a long-term treatment (1 year), but the characteristics were different. Further investigations are needed to determine whether this effect was independent of the hypoglycemic effects.
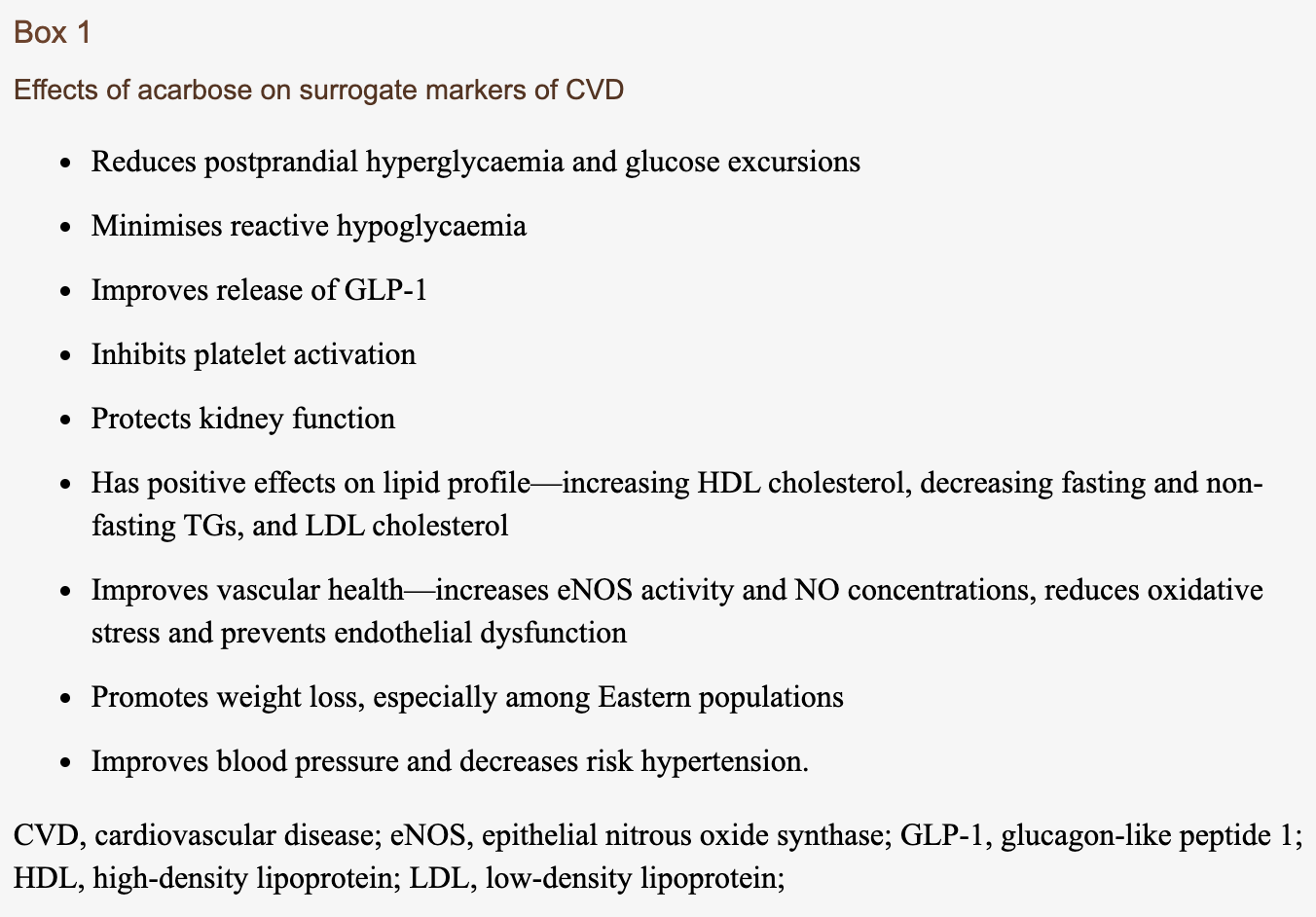
Acarbose: safe and effective for lowering postprandial hyperglycaemia and improving cardiovascular outcomes (link)
Wachters-Hagedoorn et al24 demonstrated that the peak glucose concentration and area under curve (AUC) from 0 to 120 min was significantly lower for corn pasta with acarbose (CPac) (6.0±0.2 mmol/L) versus CP (corn pasta alone) (6.7±0.3; p=0.007) and CPac (25.7±7.1 mmol/L/ 2 h) than for CP (65.3±17.3; p=0.034), respectively. Acarbose was also shown to significantly reduce the percentage of administered dose excreted as 13CO2 in breath (CP 37.5±2.8 cum %dose/6 h vs CPac 27.2±2.2; p=0.004) over the 360 min post-test meal.
A Cochrane meta-analysis found that acarbose therapy reduced glycated haemoglobin (HbA1c) levels by a mean of 0.8%. This decrease was accentuated in individuals with higher baseline HbA1C levels (baseline HbA1c of <7%, 7–9%, and >9% had decreases of 0.56% (95% CI 0.36 to 0.76), 0.78% (95% CI 0.63 to 0.93) and 0.93% (95% CI 0.53 to 1.33), respectively). A meta-regression analysis revealed regression coefficient of −0.12 (95% CI −0.26 to 0.03), showing an additional 0.12% decrease in HbA1c for every 1% increase in baseline HbA1c. Moreover, acarbose was shown to reduce fasting blood glucose by 1.09 mmol/L (28 comparisons; 95% CI 0.83 to 1.36) and 1 h postprandial glucose by 2.32 mmol/L (acarbose; 22 comparisons; 95% CI 1.92 to 2.73).11
The glycaemic effect of acarbose on HbA1c did not vary with dose, however, acarbose did decrease postprandial glucose in a dose-dependent manner. Acarbose 50, 100, 200 and 300 mg three times a day reduced HbA1c by 0.90, 0.76, 0.77 and 0.78%, respectively, and postprandial glucose by 1.63, 2.26, 2.78 and 3.62 mmol/L, respectively.11 This glycaemic benefit of acarbose has been more significant in Asian trials than those in the West, due to predominant consumption of a carbohydrate-rich diet among Asian populations.25
Acarbose, lente carbohydrate, and prebiotics promote metabolic health and longevity by stimulating intestinal production of GLP-1, 2015
In mice, lifetime acarbose feeding can increase median and maximal lifespan-an effect associated with increased plasma levels of fibroblast growth factor 21 (FGF21) and decreased levels of insulin-like growth factor-I (IGF-I). There is growing reason to suspect that an upregulation of fasting and postprandial production of glucagon-like peptide-1 (GLP-1)-stemming from increased delivery of carbohydrate to L cells in the distal intestinal tract-is largely responsible for the versatile health protection conferred by acarbose. Indeed, GLP-1 exerts protective effects on vascular endothelium, the liver, the heart, pancreatic β cells, and the brain which can rationalise many of the benefits reported with acarbose. And GLP-1 may act on the liver to modulate its production of FGF21 and IGF-I, thereby promoting longevity.
Acarbose raises serum butyrate in human subjects with impaired glucose tolerance, 2000
[NEGATIVE] Effects of acarbose on cardiovascular and diabetes outcomes in patients with coronary heart disease and impaired glucose tolerance (ACE): a randomised, double-blind, placebo-controlled trial (2017) (link)
Methods: The Acarbose Cardiovascular Evaluation (ACE) trial was a randomised, double-blind, placebo-controlled, phase 4 trial, with patients recruited from 176 hospital outpatient clinics in China. Chinese patients with coronary heart disease and impaired glucose tolerance were randomly assigned (1:1), in blocks by site, by a centralised computer system to receive oral acarbose (50 mg three times a day) or matched placebo, which was added to standardised cardiovascular secondary prevention therapy. All study staff and patients were masked to treatment group allocation. The primary outcome was a five-point composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, hospital admission for unstable angina, and hospital admission for heart failure, analysed in the intention-to-treat population (all participants randomly assigned to treatment who provided written informed consent). The secondary outcomes were a three-point composite outcome (cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke), death from any cause, cardiovascular death, fatal or non-fatal myocardial infarction, fatal or non-fatal stroke, hospital admission for unstable angina, hospital admission for heart failure, development of diabetes, and development of impaired renal function. The safety population comprised all patients who received at least one dose of study medication. This trial is registered with ClinicalTrials.gov, number NCT00829660, and the International Standard Randomised Controlled Trial Number registry, number ISRCTN91899513.
Findings: Between March 20, 2009, and Oct 23, 2015, 6522 patients were randomly assigned and included in the intention-to-treat population, 3272 assigned to acarbose and 3250 to placebo. Patients were followed up for a median of 5·0 years (IQR 3·4-6·0) in both groups. The primary five-point composite outcome occurred in 470 (14%; 3·33 per 100 person-years) of 3272 acarbose group participants and in 479 (15%; 3·41 per 100 person-years) of 3250 placebo group participants (hazard ratio 0·98; 95% CI 0·86-1·11, p=0·73). No significant differences were seen between treatment groups for the secondary three-point composite outcome, death from any cause, cardiovascular death, fatal or non-fatal myocardial infarction, fatal or non-fatal stroke, hospital admission for unstable angina, hospital admission for heart failure, or impaired renal function. Diabetes developed less frequently in the acarbose group (436 [13%] of 3272; 3·17 per 100 person-years) compared with the placebo group (513 [16%] of 3250; 3·84 per 100 person-years; rate ratio 0·82, 95% CI 0·71-0·94, p=0·005). Gastrointestinal disorders were the most common adverse event associated with drug discontinuation or dose changes (215 [7%] of 3263 patients in the acarbose group vs 150 [5%] of 3241 in the placebo group [p=0·0007]; safety population). Numbers of non-cardiovascular deaths (71 [2%] of 3272 vs 56 [2%] of 3250, p=0·19) and cancer deaths (ten [<1%] of 3272 vs 12 [<1%] of 3250, p=0·08) did not differ between groups.
Interpretation: In Chinese patients with coronary heart disease and impaired glucose tolerance, acarbose did not reduce the risk of major adverse cardiovascular events, but did reduce the incidence of diabetes.
[Interpretation: Acarbose isn’t a cure for after getting CVD (secondary prevention). Results for other populations might be different.]
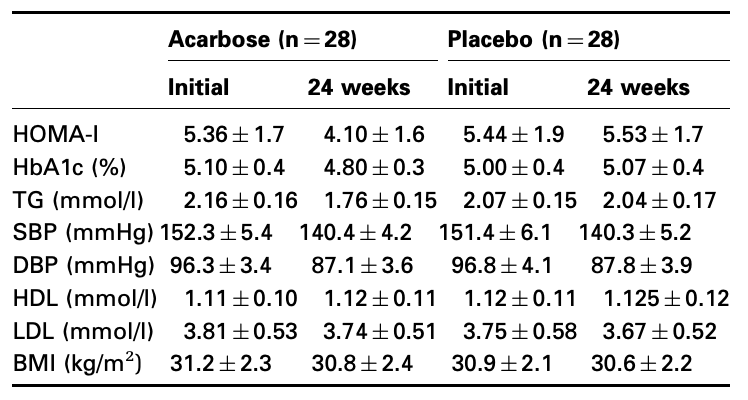
The effect of acarbose on insulin resistance in obese hypertensive subjects with normal glucose tolerance: a randomized controlled study
Aim: Acarbose, a glucose oxidase inhibitor, delays the absorption of glucose thus reducing post-prandial blood glucose level, haemoglobin A1c (HbA1c) and insulin resistance in patients with diabetes mellitus and in subjects with impaired glucose tolerance. The effect of acarbose in subjects with normal glucose tolerance (NGT) has hitherto not been examined. The aim of the present study was to examine the effect of acarbose in obese hypertensive subjects with NGT.
Methods: A double-blinded, parallel group study was performed on 56 male subjects with hypertension, body mass index (BMI) 27-35 kg/m2, fasting blood glucose < or =6 mmol/l and a normal oral glucose tolerance test. Blood pressure, HbA1c, lipid profile and insulin resistance [homeostasis model assessment (HOMA) index] were determined initially and following 24 weeks of acarbose, 150 mg/day or placebo. The primary end point was the change in insulin resistance. Anti-hypertensive treatment and diet were kept constant during the study.
Results: Insulin resistance decreased in acarbose users but not on placebo. HOMA index declined from 5.36 +/- 1.7 to 4.10 +/- 1.6 (p=0.001) on acarbose, the corresponding values on placebo were 5.44 +/- 1.9 and 5.53 +/- 1.7. A decrease in serum triglyceride values (2.16 +/- 0.16 mmol/l to 1.76 +/- 0.15 mmol/l, p=0.02) (191mg/dl → 156mg/dl) took place on acarbose with no change on placebo. There was no change in BMI, low-density lipoprotein or high-density lipoprotein values in either group. Blood pressure declined equally in both the groups, probably due to better patient compliance.
Conclusions: Acarbose may reduce insulin resistance and triglycerides also in obese hypertensive subjects with normal glucose tolerance.
Acarbose improves indirectly both insulin resistance and secretion in obese type 2 diabetic patients
Abstract
Background: Acarbose is an oral antidiabetic mainly acting on postprandial blood glucose, inhibiting alphaglucosidase. Through this mechanism, it could improve the peripheral insulin sensitivity and/or increase the insulin secretion. The aim of the present study is to assess the therapeutic efficacy of Acarbose in obese type 2 diabetic patients on both insulin resistance and insulin secretion.
Methods: 17 obese non insulin-dependent diabetic patients, well controlled with diet alone were randomized into 2 groups: acarbose (2 x 50 mg) or placebo during 16 weeks. A glucagon test allowed to evaluate insulin secretion before and after treatment as well as a triple test (glucose-insulin-somatostatin) with indirect calorimetry allowed to evaluate insulin sensitivity.
Results: A significant improvement in post-prandial plasma glucose was detected only in the Acarbose group (8.0 +/- 0.5 mmol/l before vs 6.5 0.5 mmol/l after, p<0.05). Basal C-peptide secretion was similar between groups and remained unchanged after treatment. However, stimulated insulin secretion was significantly increased by 30%, p<0.05, in the Acarbose group while no change was detected in the placebo group. Interestingly, the group receiving Acarbose disclosed a 15% reduction in insulin resistance (15.0 +/- 1.8 mmol/l before vs 12.8 +/- 1.4 mmol/l after).
Conclusions: Our results show that a treatment with Acarbose is efficient even in diabetic patients presenting a good glucose control without any other associated treatment. By decreasing post-prandial blood glucose, acarbose improves both insulin sensitivity and secretion.
Alpha-glucosidase inhibitors and risk of cancer in patients with diabetes mellitus: a systematic review and meta-analysis
Abstract
Several studies have shown that anti-diabetic medications may modify the risk of cancer. We performed a systematic review and meta-analysis to evaluate the effect of alpha-glucosidase inhibitors (AGIs) on the risk of cancer in patients with diabetes mellitus. AGIs such as acarbose, voglibose, and miglitol are commonly used oral hypoglycemic agents in China and other eastern Asian countries. The association between AGI and risk of cancer has been inconsistently reported. We conducted a systematic search of Medline, EMBASE, and Web of Science databases, up to September 30, 2016. Random-effects model was used to estimate the summary odds ratios (ORs) with 95% CI. Twenty-five studies (14 cohort, 7 case-control, and 4 randomized controlled trials) involving 1,285,433 patients with diabetes were included. Meta-analysis of observational studies showed that the use of AGIs was associated with a lower risk of developing cancer (OR = 0.86, 95% CI 0.78-0.96), especially gastrointestinal cancer (OR = 0.83, 95% CI 0.71-0.97). There was considerable heterogeneity across the studies introduced partly by the quality of included studies and adjustment for potential confounders. Meta-analysis of randomized controlled trials did not reveal any significant association between AGIs and cancer risk. Meta-analysis of observational studies indicated that AGIs may decrease the risk of cancer in individuals with diabetes.
The Antidiabetic Agent Acarbose Improves Anti-PD-1 and Rapamycin Efficacy in Preclinical Renal Cancer, 2020 (link)
We found that acarbose blunted postprandial blood glucose elevations in lean, nondiabetic mice and impeded the growth of orthotopic renal tumors, an outcome that was reversed by exogenous glucose administration. Delayed renal tumor outgrowth in mice on acarbose occurred in a CD8 T cell-dependent manner. Tumors from these mice exhibited increased frequencies of CD8 T cells that retained production of IFNγ, TNFα, perforin, and granzyme B. Combining acarbose with either anti-PD-1 or the mammalian target of rapamycin inhibitor, rapamycin, significantly reduced lung metastases relative to control mice on the same therapies. Our findings in mice suggest that combining acarbose with current RCC therapeutics may improve outcomes, warranting further study to determine whether acarbose can achieve similar responses in advanced RCC patients in a safe and likely cost-effective manner.
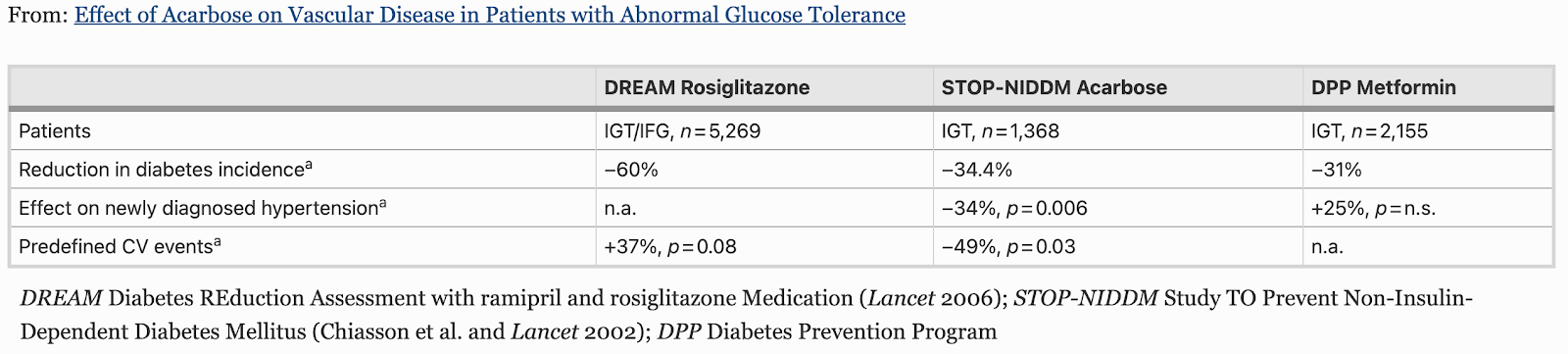
Effect of Acarbose on Vascular Disease in Patients with Abnormal Glucose Tolerance (link)
Introduction
Excessive postprandial (pp) glucose excursion in people with IGT and type 2 diabetes is associated with a cascade of proatherogenic events. Acarbose, a potent competitive inhibitor of α-glucosidases of the small intestine specifically reduces pp hyperglycemia with an average reduction of HbA1c by 0.8% in Cochrane metaanalysis. This is associated with pleiotropic effects on a broad spectrum of cardiovascular (CV) risk factors: reduction of overweight, lowering of blood pressure, triglycerides, hsCRP, fibrinogen and other biomarkers of low grade inflammation.
Results and discussion
Flow mediated vasodilation was improved and progression of intima media thickness was reduced by acarbose. In the STOP-NIDDM trial in people with IGT acarbose decreased the incidence of diabetes by 36%. The STOP-NIDDM trial with CV events as secondary objective is the only intervention trial in people with IGT so far with a significant benefit for CV disease inclusive hypertension. In a metaanalysis of controlled studies (MeRIA) in patients with type 2 diabetes, treatment with acarbose was associated with a 64% lower rate of myocardial infarction and 35% less CV events.
Conclusion
Thus results so far available prove that acarbose is an effective and safe drug to treat abnormal glucose tolerance. They suggest that acarbose can help to control a broad spectrum of CV risk factors and may prevent CV disease.
Acarbose is poorly absorbed into the bloodstream, and has a low systemic availability of less than 2% [9, 10]. As a result, the risk of any toxic reaction is very low and, to date, no interactions have been reported between acarbose and β-blockers, sulphonylureas, angiotensin-converting enzyme (ACE) inhibitors or warfarin therapy [56].
Gastrointestinal side effects—flatulence, meteorism, diarrhoea are frequently reported in the first few weeks after starting acarbose treatment. They are the consequence of mode of action of the drug on digestion of complex carbohydrates. In STOP-NIDDM, which recruited 1,429 individuals with IGT, 48% of those who discontinued early did so in the first year, and the most common single cause of discontinuation was GI side-effects [22]. Trial results indicate that initial intolerance owing to GI side-effects is transient, and that once tolerance is achieved, compliance is easier to maintain. In addition, owing to its mechanism of action, the effectiveness of acarbose does not decrease over time.
The side-effect profiles of two different acarbose dosing regimens, compared with placebo, were determined in a multicentre trial of 164 outpatients with type 2 diabetes [53]. A stepwise-increasing regimen, in which acarbose therapy was initiated at 50 mg twice daily and progressed to 100 mg three-times daily, was found to be as effective at reducing postprandial glucose levels as a flat-dosing regimen, in which patients received 100 mg three-times daily from the onset. Both regimens significantly reduced 2 hPG and mean HbA1c levels (both p < 0.0001 vs placebo). However, the stepwise-dosing regimen was associated with ~50% fewer GI side-effects that were significantly less persistent than the flat-dosing regimen over the course of treatment. A ‘start low, go slow’ stepwise-dosing regimen is, therefore, recommended to minimize side-effects.
The Effect of Acarbose on Glycemic Variability in Patients with Type 2 Diabetes Mellitus Using Premixed Insulin Compared to Metformin (AIM): An Open-Label Randomized Trial, 2020
Background: Acarbose (ACA) can effectively reduce the postprandial blood glucose and has similar antidiabetic effects as metformin (MET). To our knowledge, few studies have compared the effect of ACA or MET on glucose fluctuations. In the present study, we explored the effect of ACA or MET combined with premixed insulin (INS) on glycemic control and glycemic variability (GV).
Methods: This was an open-label randomized trial that was conducted in type 2 diabetic patients taking premixed insulin. The patients were assigned to 12 weeks of MET (n = 62) or ACA (n = 62) treatment combined with INS. The main outcomes were changes in GV and glycosylated hemoglobin A1c (HbA1c) compared with baseline.
Results: Compared with baseline, several GV indices (standard deviation [SD], mean amplitude of glycemic excursions [MAGE]) and blood glucose control indices (mean glucose [MG], time in range [TIR] and HbA1c) were both significantly improved in INS+ACA and INS+MET after 12-week therapy. However, coefficient of variation (CV) was significantly reduced in INS+ACA but not in INS+MET. Moreover, compared with INS+MET, INS+ACA led to a more pronounced percentage change from baseline in CV (26.3% [1.7%–44.6%] vs. 11.9% [−7.0% to 29.9%], P = 0.022), MAGE (40.5% [20.1%–60.5%] vs. 25.2% [−2.1% to 43.4%], P = 0.007) and SD (38.6% [25.2%–57.9%] vs. 30.1% [10.8%–46.5%], P = 0.041).
Conclusion: Both MET and ACE combined with INS effectively reduced blood glucose. Compared with MET, ACA combined with INS reduced GV.
Acarbose actions on insulin resistance and inflammatory parameters during an oral
fat load
The aim of this study was to evaluate the effects of acarbose on inflammatory biomarkers and insulin resistance in diabetic patients before and after a standardized oral fat load (OFL). Ninety six patients were assigned to take acarbose 50mg three times a day and 92 to take placebo; after the first month acarbose was titrated to 100mg three times a day. We evaluated the following parameters at the baseline, and after 1, 2 and 7months: body mass index (BMI), glycemic control, fasting plasma insulin, post-prandial plasma insulin, homeostasis model assessment insulin resistance index (HOMA-IR), blood pressure, lipid profile, soluble intercellular adhesion molecule-1 (sICAM-1), interleukin-6 (IL-6), high-sensitivity C reactive protein (Hs-CRP), soluble vascular cell adhesion molecule-1 (sVCAM-1), and soluble E-selectin (sE-selectin). Furthermore, at the baseline and at the end of the study all patients underwent OFL, and an euglycemic hyperinsulinemic clamp to evaluate M value and total glucose requirement. Acarbose was better than placebo in improving glycemic and lipid profile, and HOMA-IR. Furthermore, acarbose gave a decrease of fasting plasma insulin, post-prandial insulin, s-ICAM-1, sVCAM-1, IL-6, and Hs-CRP, not observed with placebo, even if no significant differences between the two groups were observed. During the second OFL performed after the therapy with acarbose, we observed a significant decrease of all inflammatory parameters' peaks compared to the OFL administered at baseline. Acarbose was more effective than acarbose in reducing the post-OFL peaks of the various parameters included the inflammatory markers, after 7months of therapy.
[Note the weight loss]


To Compare the Anti-Inflammatory Effect of Oral Hypoglycemic Drugs in Type 2 Diabetes Mellitus
Insulin resistance and endothelial dysfunction which shares multiple signaling pathways likehyperinsulinemia, glucotoxicity and inflammation in type 2 Diabetes Mellitus (DM) leads to several micro and macrovascular complications. Studies have shown the antiinflammatory effects of certain oral hypoglycemic agents which will be helpful in preventing the impact of diabetes related complications. The study aimed to compare the anti-inflammatory effects of Sitagliptin and Acarbose in combination with Metformin and Sulfonylurea in Type2DM patients by using Anti-inflammatory markers Interleukin-6 (IL6), high sensitive C-reactive protein (hsCRP) and also to compare the clinical outcome between these two groups by using the parameters Fasting blood sugar (FBS), Post prandial blood sugar (PPBS), hemoglobin A1c (HbA1C), Plasma Insulin. In this open labeled prospective parallel group clinical study 30 type 2 diabetes patients on Metformin and Sulfonylurea combination, with HbA1c value >/=7.5 were recruited in tertiary care hospital and divided into two groups based on their HbA1C levels and were added on either Acarbose or Sitagliptin along with Metformin Sulfonylurea combinations and were followed for 3 months. Parameters like FBS, PPBS, HbA1c, Plasma Insulin hs CRP, IL-6 were measured before and after the study. In the study the mean value of FBS, PPBS, HbA1c, Plasma Insulin, Insulin Resistance, hsCRP were reduced in both Sitagliptin and Acarbose group, which were similar to the results of previous studies except IL6 which got reduced in Sitagliptin group but increased in Acarbose group. The study had showed the synergism of Sitagliptin with Metformin Sulfonylurea combinationin reducing inflammation however; still long term studies are required to confirm their anti-inflammatory effects.

Acarbose comes as a tablet to take by mouth. It is usually taken three times a day. It is very important to take each dose with the first bite of each main meal.
Starting with a low dosage of 50 mg/day and gradual dosage increments may help
to reduce these symptoms. The tablets should be swallowed whole or chewed with the first mouthful of each main meal. It is estimated that approximately 5% of patients are unable to tolerate the drug.
Elevated Hepatic Transaminases
Increases in serum hepatic transaminase levels were observed in early studies in the USJlO41 These abnormalities were reversible on discontinuation of the drug, which was administered in dosages of up to 900 mg/day. Elevated transaminase levels in rats during long term studies were not accompanied by histological changes in the liver, and were attributed to intestinal malabsorption causing mainutritionJlO61 The manufacturer recommends that hepatic transaminases are monitored monthly in patients taking more than 300 mg/day of acarbose, and that a reduction in dosage or withdrawal of therapy should be considered if elevations persist.
Cognitive Vitality / Alzheimer’s (link)
Lifespan: BENEFIT. No evidence in humans yet. The National Institute on Aging Interventions Testing Program (NIA ITP) was designed to test compounds such as acarbose that are purported to extend lifespan and/or delay onset of age-related diseases. This collaborative program uses 1) parallel studies in males and females at 3 different sites, 2) genetically heterogeneous mice to guard against conclusions based on a single inbred genotype, and 3) enough samples to provide statistical power. In the 2014 report, mice were fed acarbose mixed in the diet (1000 mg of acarbose in 1 kg of diet; 1000 ppm) from 4 months of age and onward (Harrison et al., 2014). Acarbose increased male median lifespan by 22% but increased female medial lifespan by only 5%, based on data pooled across 3 sites (statistically significant for both sexes). This sex effect of acarbose could not be accounted for by differences in weight changes--acarbose reduced body weights considerably more in females (15, 22, 23, 22% lighter) than in males (15, 14, 11, 9% lighter). One possible reason for this sex effect is the unusually short lifespan of the male controls at 2 out of 3 test sites, magnifying the apparent effect of acarbose in males. Maximum lifespan (90th percentile) increased 11% in males and 9% in females. Acarbose did not affect HbA1c levels, but fasting blood glucose levels were higher in acarbose-fed males and females. This counterintuitive effect may be due to acarbose delaying the digestion of complex carbohydrates and absorption of sugars from the GI tract. Acarbose also reduced fasting insulin in males, but not females, suggesting that males may have achieved greater insulin sensitivity. In both males and females, acarbose significantly reduced plasma levels of insulin-like growth factor 1 (IGF1), a hormone that has been associated with shorter lifespan (Teumer et al., 2016; Suh et al., 2008). FGF21, a hormone produced by the liver in response to fasting (extends lifespan in mice), was elevated by acarbose, but was greatly reduced with dietary restriction in the same study. Thus the mechanisms of action for life extension are not entirely the same for acarbose and dietary restriction.
Acarbose, lente carbohydrate, and prebiotics promote metabolic health and longevity by stimulating intestinal production of GLP-1
The α-glucosidase inhibitor acarbose, which slows carbohydrate digestion and blunts postprandial rises in plasma glucose, has long been used to treat patients with type 2 diabetes or glucose intolerance. Like metformin, acarbose tends to aid weight control, postpone onset of diabetes and decrease risk for cardiovascular events. Acarbose treatment can favourably affect blood pressure, serum lipids, platelet aggregation, progression of carotid intima-media thickness and postprandial endothelial dysfunction. In mice, lifetime acarbose feeding can increase median and maximal lifespan-an effect associated with increased plasma levels of fibroblast growth factor 21 (FGF21) and decreased levels of insulin-like growth factor-I (IGF-I). There is growing reason to suspect that an upregulation of fasting and postprandial production of glucagon-like peptide-1 (GLP-1)-stemming from increased delivery of carbohydrate to L cells in the distal intestinal tract-is largely responsible for the versatile health protection conferred by acarbose. Indeed, GLP-1 exerts protective effects on vascular endothelium, the liver, the heart, pancreatic β cells, and the brain which can rationalise many of the benefits reported with acarbose. And GLP-1 may act on the liver to modulate its production of FGF21 and IGF-I, thereby promoting longevity. The benefits of acarbose are likely mimicked by diets featuring slowly-digested 'lente' carbohydrate, and by certain nutraceuticals which can slow carbohydrate absorption. Prebiotics that promote colonic generation of short-chain fatty acids represent an alternative strategy for boosting intestinal GLP-1 production. The health benefits of all these measures presumably would be potentiated by concurrent use of dipeptidyl peptidase 4 inhibitors, which slow the proteolysis of GLP-1 in the blood.
Effects of 24-week treatment with acarbose on glucagon-like peptide 1 in newly diagnosed type 2 diabetic patients: a preliminary report, 2013
Following 24 weeks of acarbose treatment, both fasting and postprandial plasma GLP-1 levels were increased. In patients with increased postprandial GLP-1 levels, serum NO levels and NOS activities were also significantly increased and were positively related to GLP-1 levels. Although the CIMT was not significantly altered following treatment with acarbose, a decreased CIMT was negatively correlated with increased GLP-1 levels.
Conclusions: Twenty-four weeks of acarbose monotherapy in newly diagnosed patients with T2D is associated with significantly increased levels of both fasting and postprandial GLP-1 as well as significantly increased NO levels and NOS activity for those patients in whom postprandial GLP-1 levels were increased. Therefore, the benefits of acarbose on cardiovascular risk may be related to its stimulation of GLP-1 secretion.

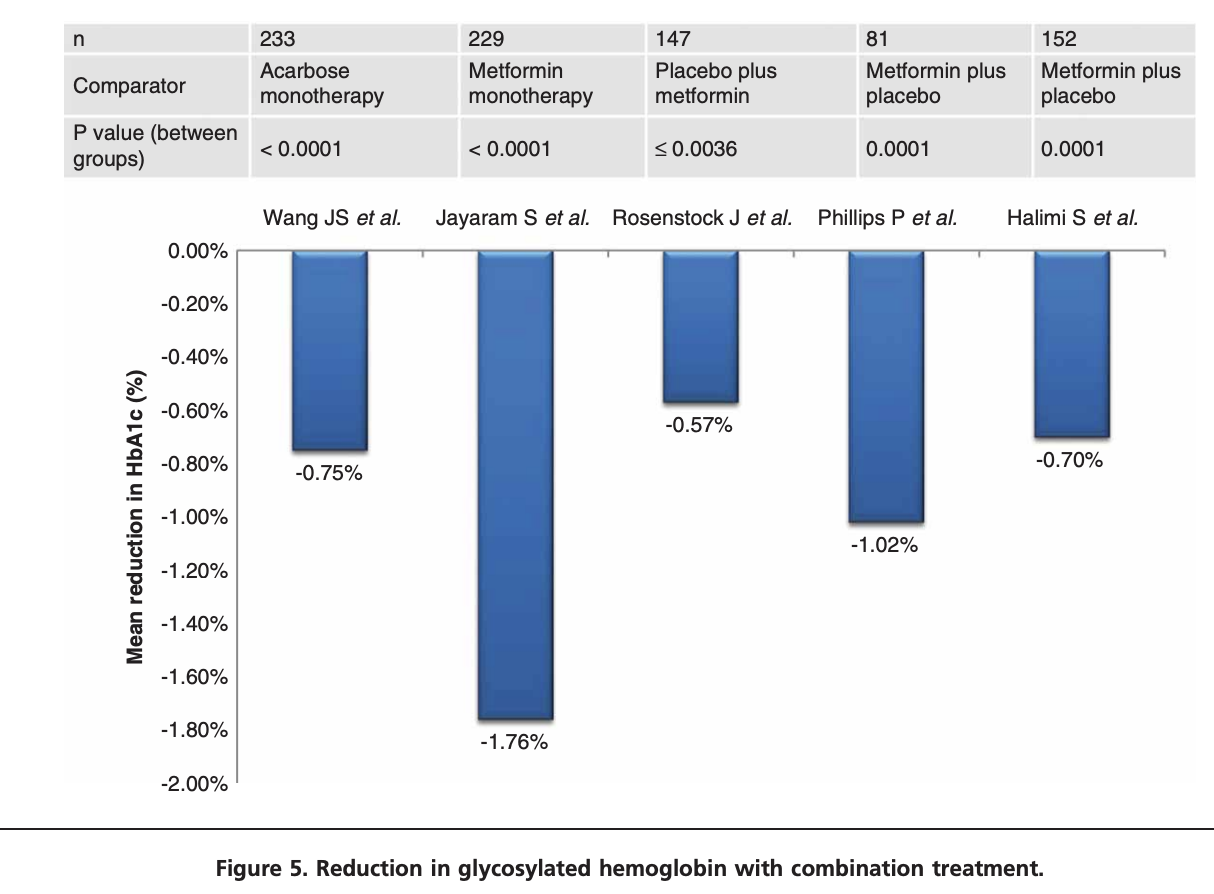
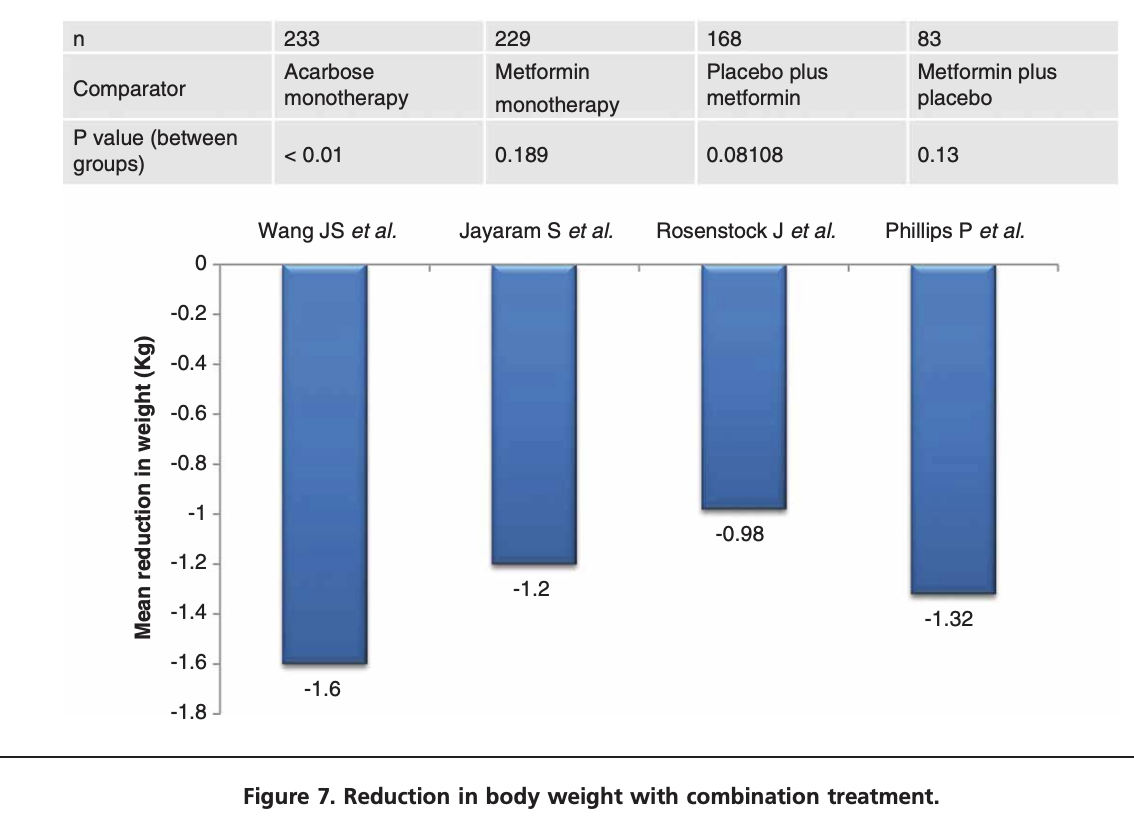
Acarbose plus metformin fixed-dose combination outperforms acarbose monotherapy for type 2 diabetes, 2013
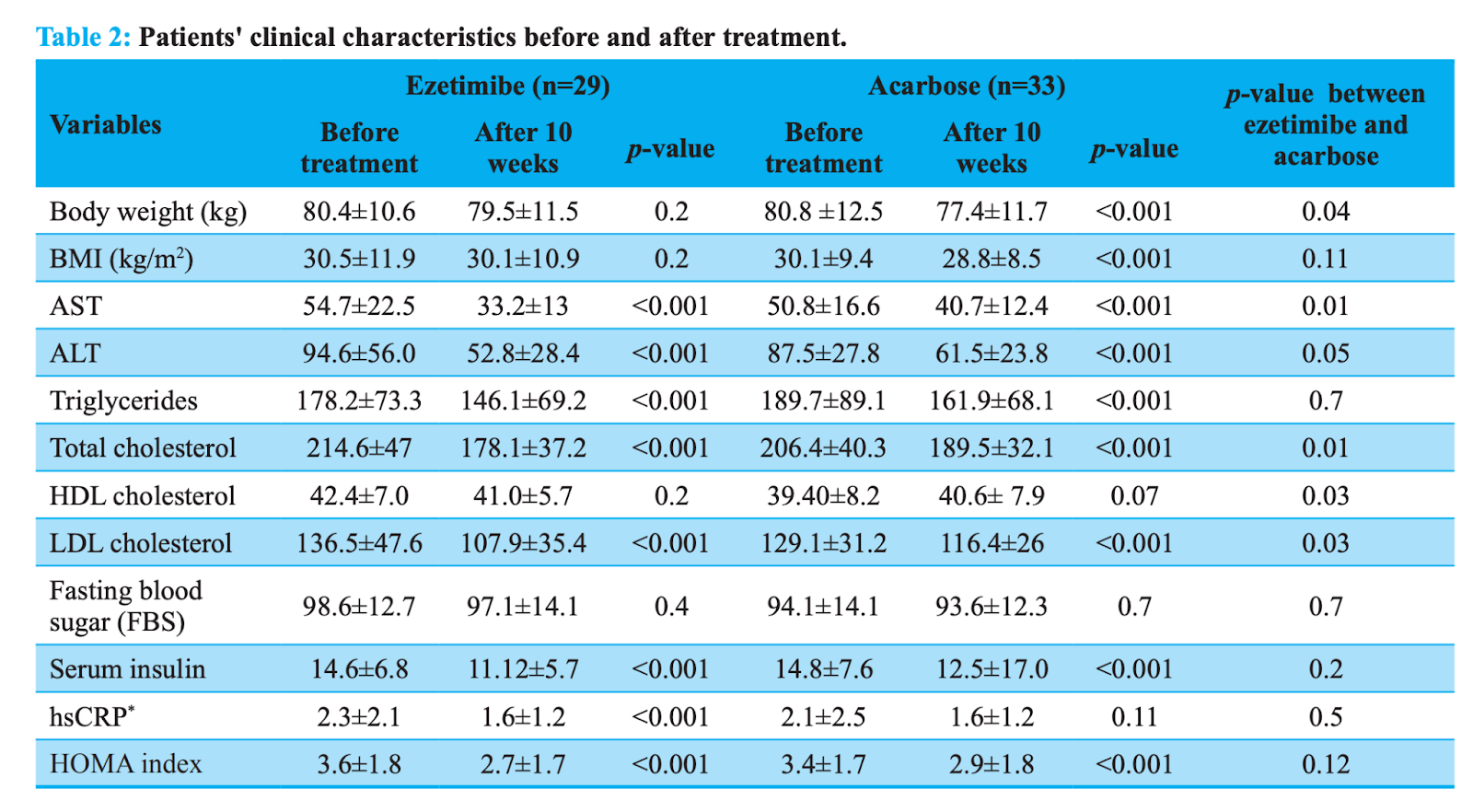
A Comparison of Ezetimibe and Acarbose in Decreasing Liver Transaminase in Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial, 2013
This was a single center, double-blind, parallel-group study conducted at Bu-Ali Sina Hospital, Qazvin, Iran. In this trial, we enrolled, by simple randomization, a total of 62 patients diagnosed with NASH. There were 29 patients treated with ezetimibe and 33 who were treated with acarbose over a ten-week period.
Ezetimibe treatment significantly reduced ALT, AST, triglycerides, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-sensitivity C-reactive protein (hsCRP), and serum insulin levels and the insulin resistance homeostasis model assessment (HOMA-IR) index compared to patients treated with acarbose (p‹0.001). Ezetimibe treatment decreased ALT (p=0.05), AST (p=0.01), total cholesterol (p=0.01), HDL cholesterol (p=0.03) and LDL cholesterol (p=0.03) levels to a significantly higher extent.
Both ezetimibe and acarbose improved metabolic and biochemical abnormalities in patients with NASH, however these effects were more prominent with ezetimibe.
Postprandial hyperglycemia as an etiological factor in vascular failure, 2009

Acarbose treatments improve arterial stiffness in patients with type 2 diabetes mellitus, 2011
A total of 22 patients with type 2 diabetes mellitus were treated with acarbose. Cardio-ankle vascular index (CAVI) as the arterial stiffness was measured by using a VaSera CAVI instrument before and 12 months after acarbose treatment. Serum high-sensitivity C-reactive protein (hs-CRP), pentraxin-3 (PTX3) and matrix metalloproteinase (MMP) -2, -9 were measured at the same time points. Furthermore, circulating peripheral blood mononuclear cells were examined for the frequencies of CD14 positive cells expressing membrane type-1 MMP (MT1-MMP) at the single cell level using flow cytometry.
Results: After acarbose treatment, postprandial glucose and glycosylated hemoglobin (HbA1c) were significantly decreased. Serum levels of hs-CRP, PTX3, MMP-2 and MMP-9 were significantly decreased. CAVI showed a significant reduction, although the changes were not significant in blood pressure and heart rate. MT1-MMP expression was significantly decreased by acarbose treatment. In multivariate analysis, improvement of blood glucose, decrease of PTX3 levels and MT1-MMP expression were independent predictors of beneficial change in CAVI.
Conclusions: The present study showed that the beneficial effects of acarbose on arterial stiffness are mediated by an improvement of postprandial hyperglycemia and vascular remodeling markers. In conclusion, acarbose treatment might reduce the risk of cardiovascular diseases by altering the arterial stiffness in postprandial hyperglycemic status.
A randomized double-blind trial of acarbose in type 2 diabetes shows improved glycemic control over 3 years (U.K. Prospective Diabetes Study 44) (link)
The HbA1c difference at 3 years (309 acarbose, 470 placebo) was 0.5% lower median HbA1c (8.1 vs. 8.6%, P < 0.0001).

Alpha-glucosidase inhibitors for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk of developing type 2 diabetes mellitus, 2018 (html link)
[Very little data for deciding on key metrics like all cause mortality]


Comments