Vitamin D
Vitamin D
Inhibits Kidney Cancer (RCC) cells proliferation, angiogenesis, clonogenicity, and metastasis across multiple RCC cell lines.
Mice studies showed RCC tumor growth was almost completely abolished in the group treated with Vit D3 injections. Some animals showed complete tumor regression.
Circulating vitamin D level was protectively associated with a lower risk of RCC 0.76 (95% CI: 0.64-0.89, P=0.001),
In 2019, three meta-analyses of RCTs of all cancer sites reported that vitamin D supplementation given pre-diagnostically reduced the risk of total cancer mortality by 13%.
Supplementing 2-4k IU/daily reduced epigenetic clock in healthy humans by ~2 yrs in 16 weeks. Circulating blood values were negatively correlated with epigenetic age.
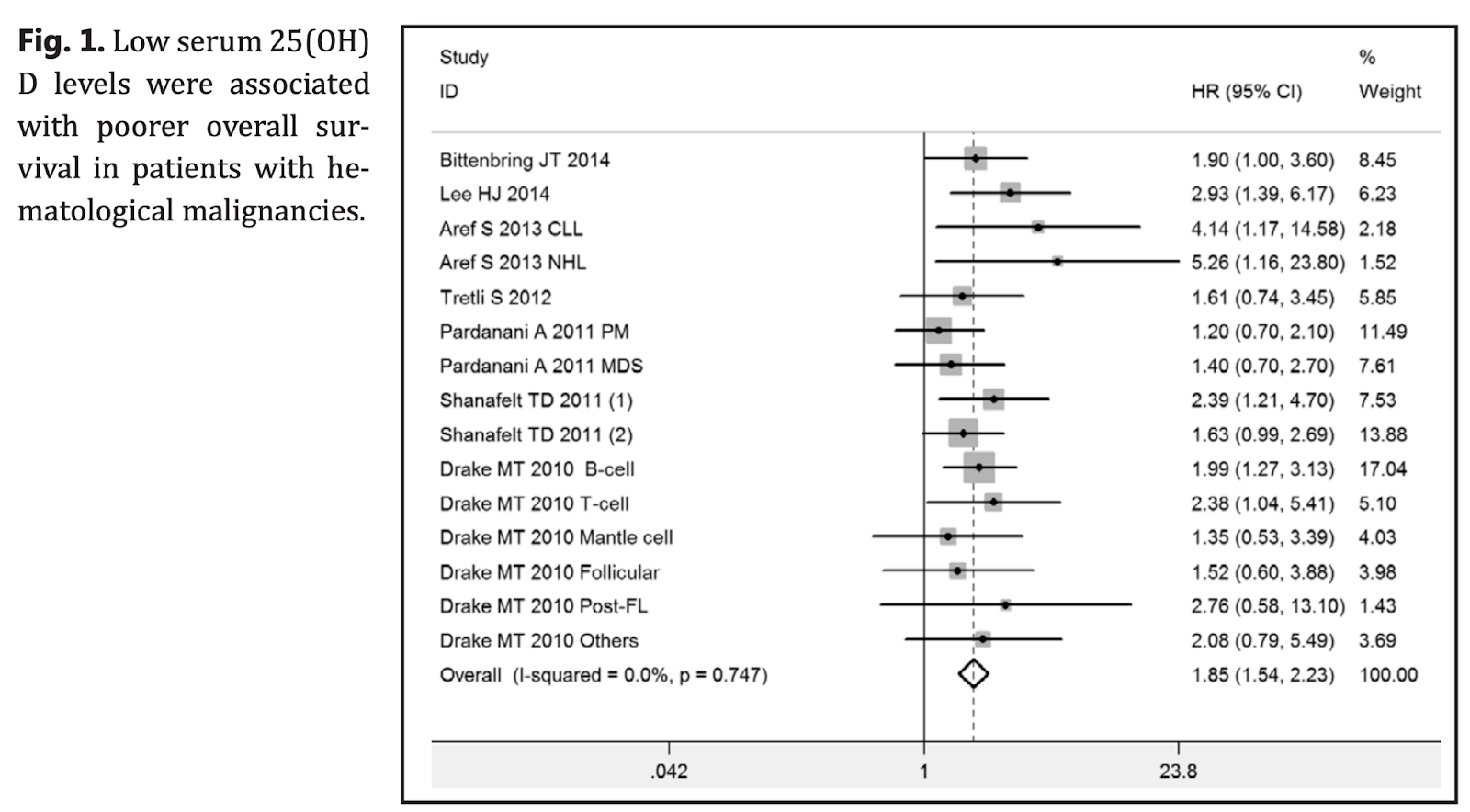
Low serum 25(OH)D levels are significantly associated with poorer prognosis in patients with hematological malignancies including lymphoma and leukemia.
Vitamin D and urological cancers, 2016
This paper presents a review of the current knowledge on the effects of vitamin D on the pathogenesis and treatment options in prostate, kidney, bladder, and testicular cancers.
Renal cancer
Several biological links might support the VD influence on renal cell cancer (RCC) risk and RCC survival. It was shown in in-vitro and in-vivo studies that VD inhibits RCC cells proliferation, angiogenesis, clonogenicity, and metastasis, induces cell differentiation, and prolongs survival [18, 19, 20]. Moreover, VD modifies hypertension, diabetes, and obesity, all possible risk factors for RCC [21, 22]. Some ecologic studies have shown an inverse association between levels of solar ultraviolet irradiance and RCC incidence [23].
It was demonstrated 30 years ago that VD3 inhibits the growth of the RCC cell line [20]. Those finding were confirmed in more recent studies on both in-vitro cell lines and in-vivo in animal models [24, 25]. Dormoy et. al. have shown that VD3 inhibited cell proliferation and cell growth in cell lines, independently of VHL expression. In the same paper, it was demonstrated in the animal model that tumor growth was almost completely abolished in the group treated with VD3 injections. Some animals showed a complete tumor regression. It was also proven that cholecalciferol treatment of mice did not induce calcification or calcium reabsorption, and thus, was not toxic [26].
To date, a few big studies on circulating VD and the risk of RCC were conducted [27, 27, 29]. Gallicchio et al. combined data from 8 prospective cohort studies and did not support the hypothesis that higher circulating VD level measured in prediagnostic blood specimens was associated with a decreased risk of RCC overall or with RCC specifically [27]. In contrast, Afzal et. al. and Muller et. al. showed that low concentrations of VD were related with higher risk of RCC, as well as lower all-cause mortality among RCC cases [28]. Additionally, Muller proved that high concentrations of VD might also be associated with increased risk of all-cause mortality among RCC cases [29].
Other authors have focused on VD intake. Studies from Central and Eastern Europe, Italy, Finland, and the United States found no associations between VD intake and RCC risk [30, 31, 32, 33].
Vitamin D3 triggers antitumor activity through targeting hedgehog signaling in human renal cell carcinoma (link)
Human clear cell renal cell carcinoma (CCC) remains resistant to treatments despite the progress in targeted therapies. Several signaling pathways acting during renal development are reactivated during kidney tumorigenesis; this is the case of the sonic hedgehog (SHH)-Gli. Interestingly, the precursor of active vitamin D3 (VD3), cholecalciferol, has been demonstrated to be a strong inhibitor of SHH-Gli signaling. Here, we show the preclinical efficacy of cholecalciferol in CCC both in vitro and in vivo . A panel of CCC cell lines, tumors and normal corresponding tissues from CCC patients were used to evaluate the expression of the VD3 receptor and metabolizing enzymes and the effects of cholecalciferol treatment. Subsequently, xenografted mice were treated with cholecalciferol in a prophylactic or therapeutic manner; their response and the adverse effects were evaluated on the basis of weekly monitoring, followed by blood collection procedures and X-ray micro-computed tomography. VD3 receptor and metabolizing enzymes are dramatically decreased in human cell lines and tumors. Cholecalciferol decreases cell proliferation and increases cell death by inhibition of the SHH-Gli pathway. Xenografted mice treated with cholecalciferol exhibit absence of tumor development or substantial growth inhibition. The treatment was shown to be safe; it did not induce calcification or calcium reabsorption. These findings establish that, although VD3 receptors and metabolizing enzymes are absent in CCC, cholecalciferol supplementation is a strong tool to block the reactivation of SHH-Gli pathway in this pathology, leading ultimately to tumor regression. Cholecalciferol may have highly therapeutic potential in CCC.
Dietary and circulating vitamin D and risk of renal cell carcinoma: a meta-analysis of observational studies, 2021
A total of 9 publications were included in this meta-analysis. An overall analysis of the highest versus lowest intake levels revealed that circulating vitamin D level was protectively associated with a lower risk of RCC 0.76 (95% CI: 0.64-0.89, P=0.001), with no evidence of heterogeneity (I2=38.8%, P=0.162). In addition, dietary vitamin D intake was associated with a reduced risk of RCC (RR: 0.86; 95% CI: 75-0.99, P=0.030). Statistical heterogeneity was not identified (I2=28.8%, P=0.199). Subgroup analyses results showed the gender differences, and the associations were significant in results with women participants (RR: 0.70; 95% CI: 0.55-0.88) and case-control studies (RR: 0.80, 95% CI: 0.67-0.95).
Conclusion:
Higher circulating vitamin D level and higher dietary vitamin D intake both might be associated with a reduced risk of RCC. Further high-quality randomized controlled trials are required in the future to confirm our results.
Vitamin D and Cancer Survival: Does Vitamin D Supplementation Improve the Survival of Patients with Cancer? 2020
In 2019, three meta-analyses of RCTs of all cancer sites (Table 2) reported that vitamin D supplementation given pre-diagnostically reduced only the risk of total cancer mortality by 13% to 16%, but not risks of cancer incidence, all-cause mortality, cardiovascular mortality, or other mortality. Thus, there already exists the metaanalyses of RCTs with homogeneity, indicating that vitamin D supplementation may improve the prognosis of patients with cancer.

Vitamin D may prolong life in people with cancer (link)
Analyzed data from randomized controlled trials that had compared people who took vitamin D supplements with those who took a placebo for at least 3 years. 10 trials with a total of 79,055 participants. People who took vitamin D supplements had a 13% lower risk of dying from cancer than those who took a placebo over the same period.
Effect of Vitamin D Supplements on Cancer Incidence, Trial
Almost 26,000 participants with no history of invasive cancer or cardiovascular disease enrolled in the trial. Participants taking vitamin D saw their blood levels of the vitamin rise by 40%. The incidence of invasive cancer was about the same between the groups: 793 participants in the vitamin D group (6.1%) received a cancer diagnosis during the trial, compared with 824 in the placebo group (6.3%). The incidence of cardiovascular events (such as heart attacks) was also similar between the vitamin D and placebo groups. Over the follow-up period, there were 341 deaths from cancer: 154 among participants who took vitamin D (1.1%) and 187 among those who took the placebo (1.4%). Although this difference was not statistically significant, the difference in cancer deaths between the groups started to widen over time, the researchers reported.
Vitamin D engaged with known longevity genes – it extended median c elegans lifespan by 33% and slowed the aging-related misfolding of hundreds of proteins in the worm. 2016, (link)
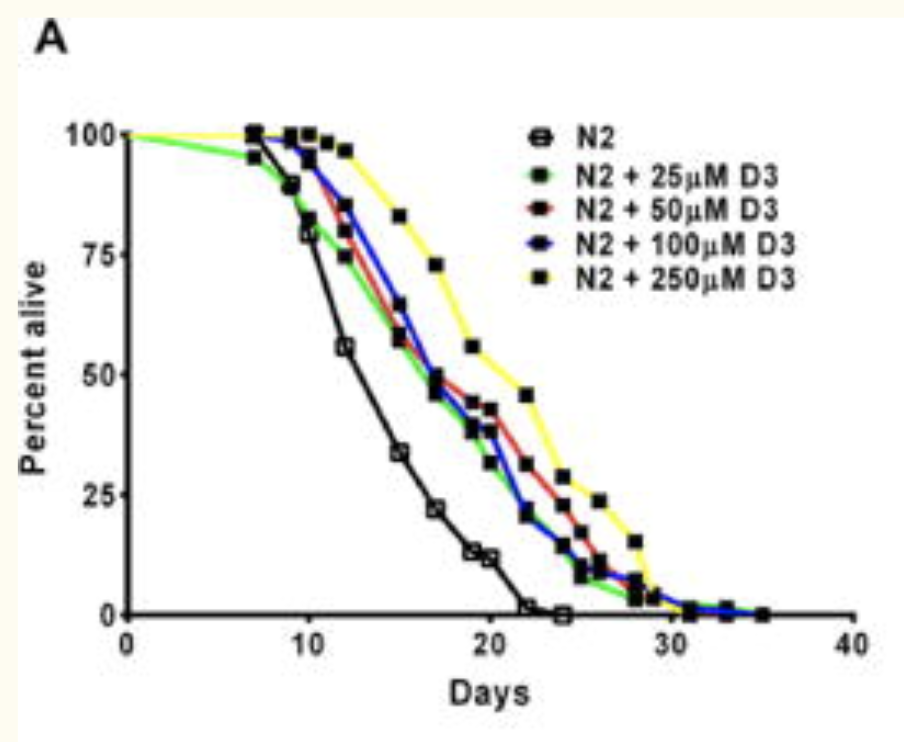
(A) Kaplan-Meier survival curves of N2 hermaphrodite worms exposed to increasing concentrations of D3 from day 1 of adulthood (P< 0.0001; log-rank test). (paper)
Effects of Vitamin D3 Supplementation on Epigenetic Aging in Overweight and Obese African Americans With Suboptimal Vitamin D Status: A Randomized Clinical Trial, 2019
Methods
A randomized clinical trial was previously conducted among 70 overweight/obese African Americans with serum 25-hydroxyvitamin D [25(OH)D] < 50 nmol/L, who were randomly assigned into four groups of 600 IU/d, 2,000 IU/d, 4,000 IU/d of vitamin D3 supplements or placebo followed by 16-week interventions. Whole genome-wide DNA methylation analysis was conducted in 51 participants. DNA methylation ages were calculated according to the Horvath and the Hannum methods. Methylation-based age acceleration index (∆Age) is defined as the difference between DNA methylation age and chronological age in years. Mixed-effects models were used to evaluate the treatment effects.
Results
Fifty-one participants (aged 26.1 ± 9.3 years, 16% are male) were included in the study. After the adjustment of multi-covariates, vitamin D3 supplementation of 4,000 IU/d was associated with 1.85 years decrease in Horvath epigenetic aging compared with placebo (p value = .046), and 2,000 IU/d was associated with 1.90 years decrease in Hannum epigenetic aging (p value = .044). Serum 25(OH)D concentrations were significantly associated with decreased Horvath ∆Age only (p values = .002), regardless of treatments.
[NEGATIVE] Vitamin D and immune cells stimulate bone marrow disease (link)
The bone marrow disease myelofibrosis is stimulated by excessive signaling from vitamin D and immune cells known as macrophages, reveals a research team. These findings could help to develop alternative treatments that do not target problem genes. By giving mice a low vitamin D diet and suppressing the macrophages, the team was able to largely prevent the onset of myelofibrosis.
Vitamin D receptor-mediated skewed differentiation of macrophages initiates myelofibrosis and subsequent osteosclerosis.
A Phase II Study of Curcumin and Vitamin D in Previously Untreated Patients with Early Stage Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL), 2018
[Seems safe!]
Vitamin D supplementation and total cancer incidence and mortality: a meta-analysis of randomized controlled trials, 2019
Background
Previous meta-analyses of randomized controlled trials (RCTs) of vitamin D supplementation and total cancer incidence and mortality found inconsistent results, and most included trials administered generally low doses of vitamin D (≤1100 IU/day). We updated the meta-analysis by incorporating recent RCTs that have tested higher doses of vitamin D supplements.
Materials and methods
PubMed and Embase were searched from the inception to November 2018. Summary relative risks (RRs) and 95% confidence intervals (CIs) were estimated using a random-effects model.
Results
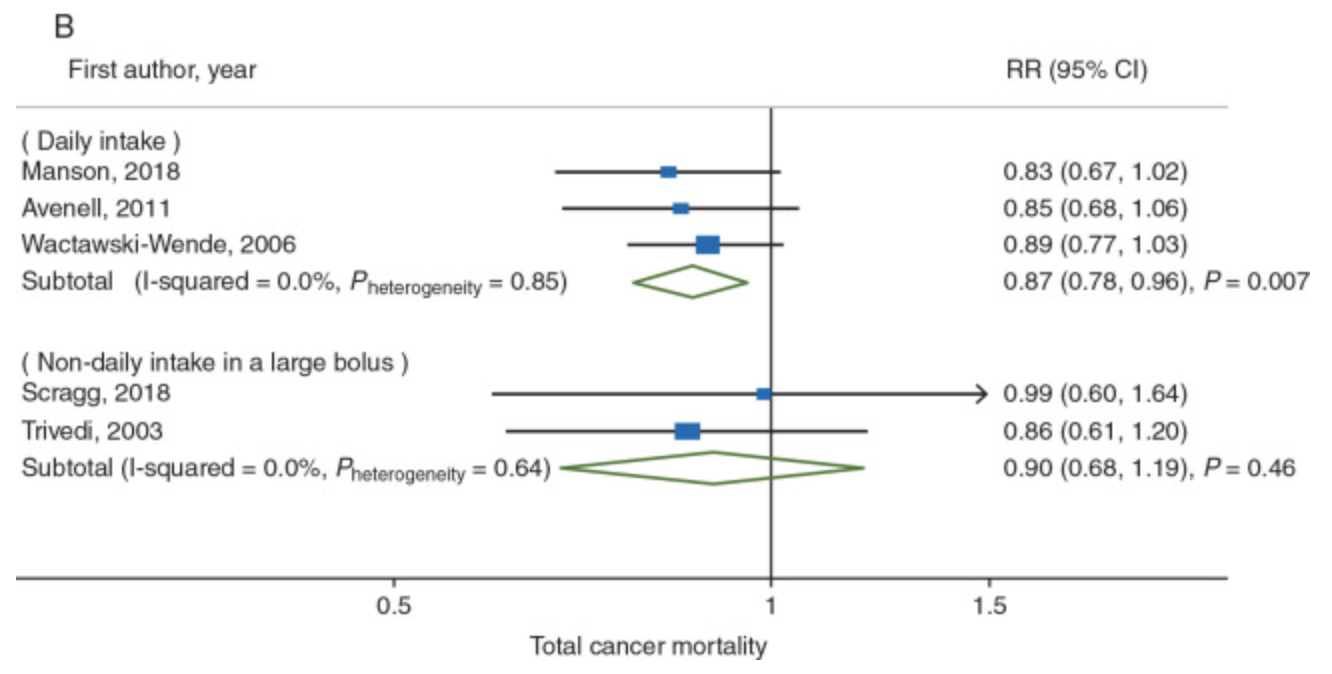
For total cancer incidence, 10 trials were included [6537 cases; 3–10 years of follow-up; 54–135 nmol/l of attained levels of circulating 25(OH) vitamin D [25(OH)D] in the intervention group]. The summary RR was 0.98 (95% CI, 0.93–1.03; P = 0.42; I2 = 0%). The results remained null across subgroups tested, including even when attained 25(OH)D levels exceeded 100 nmol/l (RR, 0.95; 95% CI, 0.83–1.09; P = 0.48; I2 = 26%). For total cancer mortality, five trials were included [1591 deaths; 3–10 years of follow-up; 54–135 nmol/l of attained levels of circulating 25(OH)D in the intervention group]. The summary RR was 0.87 (95% CI, 0.79–0.96; P = 0.005; I2 = 0%), which was largely attributable to interventions with daily dosing (as opposed to infrequent bolus dosing). No statistically significant heterogeneity was observed by attained levels of circulating 25(OH)D (Pheterogeneity = 0.83), with RR being 0.88 (95% CI, 0.78–0.98; P = 0.02; I2 = 0%) for ≤100 nmol/l and 0.85 (95% CI, 0.70–1.03; P = 0.11; I2 = 0%) for >100 nmol/l.
Conclusions
In an updated meta-analysis of RCTs, vitamin D supplementation significantly reduced total cancer mortality but did not reduce total cancer incidence.
The effect of vitamin D supplementation on survival in patients with colorectal cancer: systematic review and meta-analysis of randomised controlled trials, 2020
Background
Low circulating vitamin D levels are associated with poor colorectal cancer (CRC) survival. We assess whether vitamin D supplementation improves CRC survival outcomes.
Methods
PubMed and Web of Science were searched. Randomised controlled trial (RCTs) of vitamin D supplementation reporting CRC mortality were included. RCTs with high risk of bias were excluded from analysis. Random-effects meta-analysis models calculated estimates of survival benefit with supplementation. The review is registered on PROSPERO, registration number: CRD42020173397.
Results
Seven RCTs (n = 957 CRC cases) were identified: three trials included patients with CRC at outset, and four population trials reported survival in incident cases. Two RCTs were excluded from meta-analysis (high risk of bias; no hazard ratio (HR)). While trials varied in inclusion criteria, intervention dose and outcomes, meta-analysis found a 30% reduction in adverse CRC outcomes with supplementation (n = 815, HR = 0.70; 95% confidence interval (CI): 0.48–0.93). A beneficial effect was seen in trials of CRC patients (progression-free survival, HR = 0.65; 95% CI: 0.36–0.94), with suggestive effect in incident CRC cases from population trials (CRC-specific survival, HR = 0.76; 95% CI: 0.39–1.13). No heterogeneity or publication bias was noted.
Conclusions
Meta-analysis demonstrates a clinically meaningful benefit of vitamin D supplementation on CRC survival outcomes. Further well-designed, adequately powered RCTs are needed to fully evaluate benefit of supplementation in augmenting ‘real-life’ follow-up and adjuvant chemotherapy regimens, as well as determining optimal dosing.
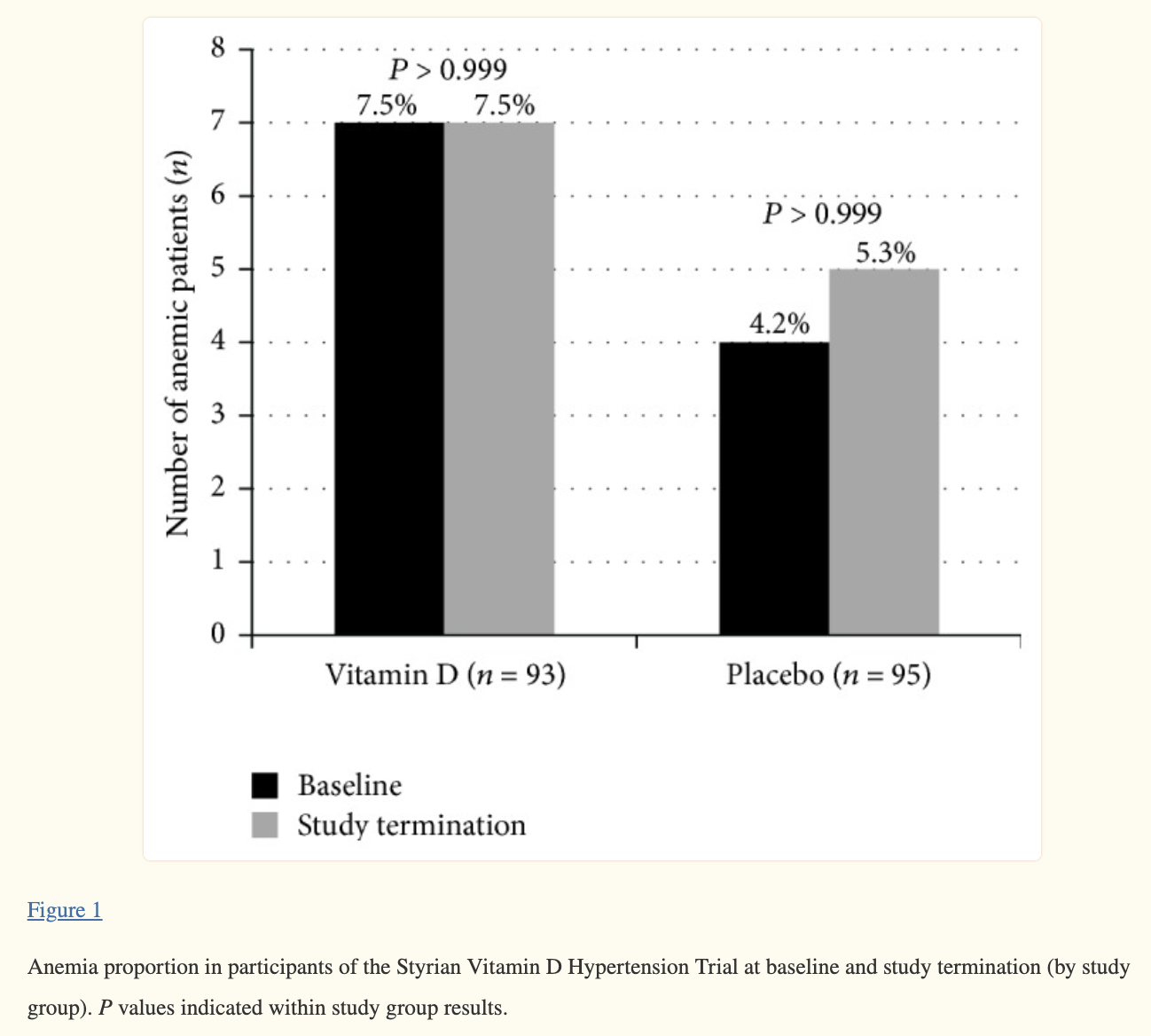
Vitamin D Supplementation and Hemoglobin Levels in Hypertensive Patients: A Randomized Controlled Trial (link)
Two hundred patients with 25OHD levels <75 nmol/L who attended the Styrian Vitamin D Hypertension Trial were included, of whom 188 completed the trial. Patients randomly received 2800 IU vitamin D3 daily or a matching placebo for eight weeks. Initially, the prevalence of anemic status (Hb levels <12.5 g/dL) and deficient 25OHD levels (<30 nmol/L) was 6.5% and 7.5%, respectively. All anemic patients had 25OHD levels >50 nmol/L. The mean (95% confidence interval) vitamin D effect on Hb levels was 0.04 (−0.14 to 0.22) g/dL (). Moreover, vitamin D treatment did not influence anemic status significantly (). Likewise, vitamin D had no significant effect on Hb levels in the subgroups of anemic patients or in patients with initial 25OHD levels <30 nmol/L. In conclusion, a daily vitamin D supplement of 2800 IU for eight weeks did not improve Hb levels or anemic status in hypertensive patients. Future trials should focus on anemic patients with deficient 25OHD levels (e.g., <30 nmol/L).

Serum 25-hydroxyvitamin D levels and prognosis in hematological malignancies: a systematic review and meta-analysis, 2015
Results: Seven studies with a total of 2,643 patients with hematological cancer were included into the meta-analysis. Overall, compared with normal serum 25(OH)D levels, low serum 25(OH)D levels were significantly associated with both poorer OS (HR = 1.85, 95% CI 1.54-2.23, P <0.001) and poorer RFS (HR = 1.45, 95% CI 1.25 to 1.70, P <0.001) in hematological malignancies. Subgroup analysis further showed that low serum 25(OH)D levels were significantly associated with poorer OS and RFS in both lymphoma and leukemia.
Conclusion: Low serum 25(OH)D levels are significantly associated with poorer prognosis in patients with hematological malignancies including lymphoma and leukemia.
Vitamin D Decreases Serum VEGF Correlating with Clinical Improvement in Vitamin D-Deficient Women with PCOS: A Randomized Placebo-Controlled Trial (link)
This is a randomized placebo-controlled trial conducted between October 2013 and March 2015. Sixty-eight VitD-deficient women with PCOS were recruited. Women received either 50,000 IU of oral VitD3 or placebo once weekly for 8 weeks. There was a significant decrease in serum VEGF levels (1106.4 ± 36.5 to 965.3 ± 42.7 pg·mL–1; p < 0.001) in the VitD group.
Vitamin D in haematological disorders and malignancies, 2017
ABSTRACT
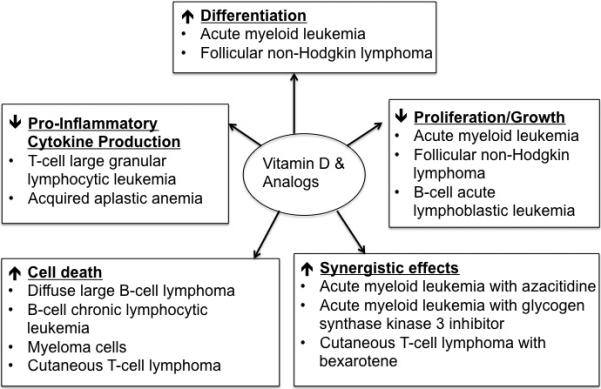
Commonly known for its critical role in calcium homeostasis and bone mineralization, more recently vitamin D has been implicated in haematological cancer pathogenesis and shows promise as an anti-cancer therapy. Serum levels of 25(OH)D3, the precursor to the active form of vitamin D, calcitriol, are typically lower in patients with haematological disease compared to healthy individuals. This often correlates with worse disease outcome. Furthermore, diseased cells typically highly express the vitamin D receptor (VDR), which is required for many of the anti-cancer effects observed in multiple in vivo and in vitro cancer models. In abnormal haematological cells, vitamin D supplementation promotes apoptosis, induces differentiation, inhibits proliferation, sensitizes tumor cells to other anti-cancer therapies, and reduces the production of pro-inflammatory cytokines. Although the dosage of vitamin D required to achieve these effects may induce hypercalcemia in humans, analogs and combinatorial treatments have been developed to circumvent this side effect. Vitamin D and its analogs are well tolerated in clinical trials and thus further investigation into the use of these agents in the clinic is warranted. Here we review the current literature in this field.
CALCITRIOL AND THE JAK-STAT PATHWAY
Dysregulation of the Janus kinase (JAK)-signal transducers and activators of transcription (STAT) pathway is common in leukemias and lymphomas including large granular lymphocytic leukemia (LGLL) (63, 64), T-cell lymphomas (65), AML (61, 66), B-CLL (67), and T-cell acute lymphoblastic leukemia (T-ALL) (68). This aberrant activation can be due to an increase in JAK-STAT promoting cytokines, repression of JAK-STAT inhibitors, activating mutations in the JAKs or STATs themselves (69), or fusion proteins as observed in KG1 (61).
Inhibition of the JAK-STAT signaling pathway leads to apoptosis of several cancer cells, including LGLL (64). Thus, investigations into potential JAK-STAT pharmacological inhibitors are underway. Unfortunately, limited potency of STAT inhibitors and negative side effects currently prevent the clinical use of STAT inhibitors (70). Vitamin D may serve as a novel JAK-STAT inhibitor as vitamin D has been found to reduce STAT3 activation in the mouse model of experimental diabetes (71) and experimental allergic encephalomyelitis (EAE) (72) as well as human esophageal squamous cell carcinoma (SCC) cell lines (73). Furthermore, vitamin D decreases STAT1 activation and pro-inflammatory cytokine output in the mouse model of EAE, correlating with a lesser disease state and improved symptomology (72). In hepatocellular carcinoma this reduction in pro-inflammatory cytokines is hypothesized to occur in a p27(kip1) gene dependent manner (74).
Recently the effects of vitamin D on the JAK-STAT pathway in LGLL have been investigated. Although 30-40% of LGLL patients exhibit somatic activating mutations in STAT3 (63, 75), constitutive activation of STAT3 and STAT1 is also observed in patients without STAT3 mutation (64) and to date no activating mutations in STAT1 have been found (27). The reason for the increased activation in non-mutated individuals may be due to aberrant cytokine signaling, particularly IL-6, and repression of JAK-STAT inhibitors, specifically suppressor of cytokine signaling 3 (SOCS3) (76). This suppression of SOCS and increase in IL-6 production is found in other cancers (77-79). We recently found that calcitriol increases VDR protein levels, reduces STAT1 and STAT3 activation, and decreases pro-inflammatory cytokine production, specifically IFN-γ production (27). Viability remained unaltered in both the T-LGLL cell line and primary patient cells, supporting a potential shift away from pro-inflammatory cells to a more anti-inflammatory phenotype (27).
Similarly, calcitriol alters pro-inflammatory cytokine production in PBMCs from AA patients. One study found that IFN-γ, TNF-α, IL-10, IL-17A, and TGF-β1 levels were elevated in acquired aplastic anemia (AA) PBMCs, but calcitriol treatment significantly decreased the production of IFN-γ, TNF-α, and IL-17A while increasing TGF-β1 (31). Calcitriol also inhibited the differentiation of Th17 and Th1 cells while increasing Th2 cells (31). Calcitriol decreased T-bet mRNA levels in AA patient cells (31), supporting a shift from Th1 phenotype. Several autoimmune and haematological disorders share a similar cytokine profile of higher IFN-γ, IL-10, IL-6, and IL-17, as observed across ITP, AIHA, Evan's syndrome, and CIN (23). Although this study did not measure changes in cytokine profile after vitamin D treatment, anti-erythrocyte autoantibody production was decreased following vitamin D treatment in patients with AIHA (23), suggesting that vitamin D may decrease the autoimmune nature of autoimmune cytopenias.
Given that vitamin D can decreases the JAK-STAT pathway activation and inflammatory cytokine output, further studies are warranted in cancers with this pathway dysregulation. Future work could determine whether vitamin D treatment of JAK-STAT activated cancers works via the same mechanism to cause inhibition, or whether unique mechanisms are at play.
CONCLUSION
With the discovery of vitamin D deficiency in many haematological disorders, understanding the role of vitamin D in the progression and treatment of such disorders is critical. Treatment with vitamin D or its analogs has shown promise in primary patient cells and cell lines in numerous haematological disorders and malignancies. Interestingly, the exact effects of calcitriol vary for different cell types. In general, calcitriol suppresses pro-inflammatory cytokine production, curtails proliferation, and inhibits antibody production in normal lymphocytes. In malignant cells, calcitriol inhibits proliferation, induces apoptosis, promotes differentiation, sensitizes malignant cells to anti-cancer therapies, and enhances cell cycle arrest. Interestingly, the exact mechanism(s) responsible for these anti-cancer effects is not yet known and should be determined in an effort to better understand how calcitriol exerts its effects.
Furthermore, vitamin D and its analogs have been well tolerated in the clinic (7, 8) and show promise in clinical trials for MDS (8). These studies have shown the potential of vitamin D as a combinatorial treatment. However, the adequate serum vitamin D level in humans and which form of vitamin D is the most appropriate to use for everyday supplementation versus cancer treatment needs to be determined. Regardless, further investigations are warranted to better elucidate the effects of calcitriol on abnormal cells and to determine its potential utility in the clinical management and treatment of haematological diseases.
Vitamin D and immune cells stimulate bone marrow disease, 2019
The research team focused on the relationship between blood and bone. Vitamin D is a hormone that regulates calcium, and the team had already shown that vitamin D receptors control the location of hematopoietic cells in the bone marrow. In this study, the team performed a bone marrow (with vitamin D receptors) transplant for a mouse model without vitamin D receptors (this means it has a high concentration of vitamin D in the body) to create a myelofibrosis model. By analyzing this model, they found that hematopoietic stem cells were strongly stimulated by vitamin D signaling and grew into immune system cells called macrophages. These pathological macrophages stimulated young osteoblasts (cells that create bone) to induce myelofibrosis and bone hardening. The cells known as fibroblasts are thought to be these young osteoblasts. By giving these mice a low vitamin D diet and suppressing the macrophages, the team was able to largely prevent the onset of myelofibrosis.
The team also examined mouse models with the same genetic disorder as myelofibrosis patients (JAK2V61F transgenic mice). These mice presented similar symptoms to myelofibrosis patients, displaying both fibrosis and bone hardening. They treated the mice by rearing them on a low vitamin D diet, blocking vitamin D receptor signals (removing the vitamin D receptor gene in blood cells) and suppressing macrophages. This proved to be extremely effective in preventing bone marrow fibrosis.
The results show that pathological macrophages produced by vitamin D receptor signaling play an important role in the development of myelofibrosis. Clinical treatment uses inhibitors to target the causative genes of myeloproliferative tumors, but this is not always effective in treating myelofibrosis. Professor Katayama comments: "The only permanent cure for this disease is hematopoietic stem cell transplant, but this method is unsuitable for many elderly patients. These new findings may help to develop a treatment method for the elderly targeting the vitamin D pathway and macrophages."
The bone marrow disease myelofibrosis is stimulated by excessive signaling from vitamin D and immune cells known as macrophages, reveals a research team. These findings could help to develop alternative treatments that do not target problem genes.
Vitamin D receptor–mediated skewed differentiation of macrophages initiates myelofibrosis and subsequent osteosclerosis, 2019
Reprogramming of Tumor-Associated Macrophages with Anticancer Therapies: Radiotherapy versus Chemo- and Immunotherapies, 2017
[Nice paper. Has a lot of depth]
Defining M1 and M2 Macrophages (link)
Tumor-associated macrophages: an accomplice in solid tumor progression, 2019
Macrophages are extremely plastic cells. They have two polarization states: classically activated M1 and alternatively activated M2 subtypes (Fig. 1a) [3]. Th1 cytokines such as interleukin-12 (IL-12) and IL-18 or activated Toll-like receptors (TLRs) promote macrophages to M1 polarization. M1 macrophages are involved in Th1 responses to pathogens [4]. M1 macrophages play critical roles in innate host defense and killing tumor cell by producing reactive oxygen/nitrogen species (ROS/RNS) and pro-inflammatory cytokines such as IL-1β, IL-6, tumor necrosis factor α (TNF-α). Therefore, they are considered as antitumor or “good” macrophages [4]. On the other hand, macrophages are induced polarization into the M2 by Th2 cytokines such as IL-4, IL-10 and IL-13. M2 macrophages are crucial for Th2 immune response including humoral immunity, wound healing and tissue remodeling. Moreover, M2 macrophages produce anti-inflammatory cytokines such as IL-10, IL-13 and TGF-β to promote tumor development. Therefore, they are considered as pro-tumor or “bad” macrophages
Tumour macrophages as potential targets of bisphosphonates, 2011
Tumour cells communicate with the cells of their microenvironment via a series of molecular and cellular interactions to aid their progression to a malignant state and ultimately their metastatic spread. Of the cells in the microenvironment with a key role in cancer development, tumour associated macrophages (TAMs) are among the most notable. Tumour cells release a range of chemokines, cytokines and growth factors to attract macrophages, and these in turn release numerous factors (e.g. VEGF, MMP-9 and EGF) that are implicated in invasion-promoting processes such as tumour cell growth, flicking of the angiogenic switch and immunosuppression. TAM density has been shown to correlate with poor prognosis in breast cancer, suggesting that these cells may represent a potential therapeutic target. However, there are currently no agents that specifically target TAM's available for clinical use.
Bisphosphonates (BPs), such as zoledronic acid, are anti-resorptive agents approved for treatment of skeletal complication associated with metastatic breast cancer and prostate cancer. These agents act on osteoclasts, key cells in the bone microenvironment, to inhibit bone resorption. Over the past 30 years this has led to a great reduction in skeletal-related events (SRE's) in patients with advanced cancer and improved the morbidity associated with cancer-induced bone disease. However, there is now a growing body of evidence, both from in vitro and in vivo models, showing that zoledronic acid can also target tumour cells to increase apoptotic cell death and decrease proliferation, migration and invasion, and that this effect is significantly enhanced in combination with chemotherapy agents. Whether macrophages in the peripheral tumour microenvironment are exposed to sufficient levels of bisphosphonate to be affected is currently unknown. Macrophages belong to the same cell lineage as osteoclasts, the major target of BPs, and are highly phagocytic cells shown to be sensitive to bisphosphonates in model studies; In vitro, zoledronic acid causes increased apoptotic cell death; in vivo the drug has been shown to inhibit the production of pro-angiogenic factor MMP-9, as well as most recent evidence showing it can trigger the reversal of the TAMs phenotype from pro-tumoral M2 to tumoricidal M1. There is thus accumulating evidence supporting the hypothesis that effects on TAMs may contribute to the anti-tumour effect of bisphosphonates. This review will focus in detail on the role of tumour associated macrophages in breast cancer progression, the actions of bisphosphonates on macrophages in vitro and in tumour models in vivo and summarise the evidence supporting the potential for the targeting of tumour macrophages with bisphosphonates.


Comments