Milk Thistle
GENERAL:
Milk thistle is an herbal supplement that has been used for centuries to treat liver conditions.
Contains silymarin and silybin, which exhibit hepatoprotective effects through antioxidant, anti-inflammatory, and antifibrotic mechanisms (2011).
Antioxidant: Silymarin inhibits free radicals and increases antioxidant enzymes like superoxide dismutase, glutathione, glutathione peroxidase (2001; 2013). Chelates iron for antioxidant effects (2001).
Anti-inflammatory: Downregulates COX-2, reducing inflammatory mediators (2013). Inhibits NF-kB, reducing proinflammatory cytokines like TNF-α and IL-1β (2003).
Antifibrotic: Silybin decreases platelet-derived growth factor, inhibiting activation of stellate cells. Reduces TGF-β, a key mediator of liver fibrosis (2016).
Silymarin may increase rapamycin levels in the blood by inhibiting its liver metabolism through CYP3A4 and P-gp inhibition.
TOXIN AND ALCOHOL EXPOSURE:
Milk thistle prevents toxin-induced damage when given before/during exposure, including alcohol and amatoxins (2002; 1982).
In alcoholic liver disease, 360 mg/day milk thistle reduced ALT and AST vs placebo (1993; 2007). Improved enzymes and pathology in another trial (1982).
In alcoholic/non-alcoholic cirrhosis, 420 mg/day milk thistle increased 4-year survival to 58% vs 39% vs placebo (1989). Greatest benefits in alcoholics.
NAFLD & METABOLIC DISORDERS:
In 25 NAFLD patients, silymarin 200 mg three times daily for 4 months significantly reduced fasting blood glucose (from 156 ± 46 to 133 ± 39 mg/dL), HbA1c (-1%), total cholesterol, triglycerides, and LDL compared to placebo (2014).
In 36 patients, silymarin 600 mg/day for 12 months decreased insulin resistance and fasting insulin versus baseline (1997).
A trial in 66 NAFLD patients found transaminase levels were significantly lower with silymarin comparable to metformin or pioglitazone over 4 months (2012).
A pilot study in 25 NAFLD patients found a silybin-vitamin E-phospholipid complex improved markers of liver damage and fibrosis, and insulin resistance over 4 months (2007).
For NAFLD, 48 weeks of milk thistle markedly reduced fibrosis scores compared to placebo in two trials (2006; 2012).
A meta-analysis of 8 trials concluded milk thistle significantly lowered ALT and AST in NAFLD patients versus controls (ALT: -5.08 U/L, AST: -5 U/L, p<0.05) (2017).
CANCER:
Inhibit growth of many cancer cell lines (prostate, breast, hepatic, epidermoid, colon, ovarian, lymphoma, leukemia) and tumor initiation in animal models (link).
In renal carcinoma cells, silibinin inhibited invasion, migration, and xenograft growth. Enhanced chemosensitivity to agents like 5-fluorouracil (2011)
In Acute Lymphoblastic Leukemia (ALL) silymarin reduced the harmful effects of chemotherapy on the liver without stopping the treatment from working (2016).
May reduce chemotherapy-induced hepatotoxicity, nephrotoxicity as well as improve radiodermatitis and radiation therapy-induced mucositis. (2019, 2015, 2020, 2016, 2011)
In men after prostatectomy, 570 mg/day silymarin plus selenium improved quality of life, decreased LDL and cholesterol compared to placebo (2010).
OTHER:
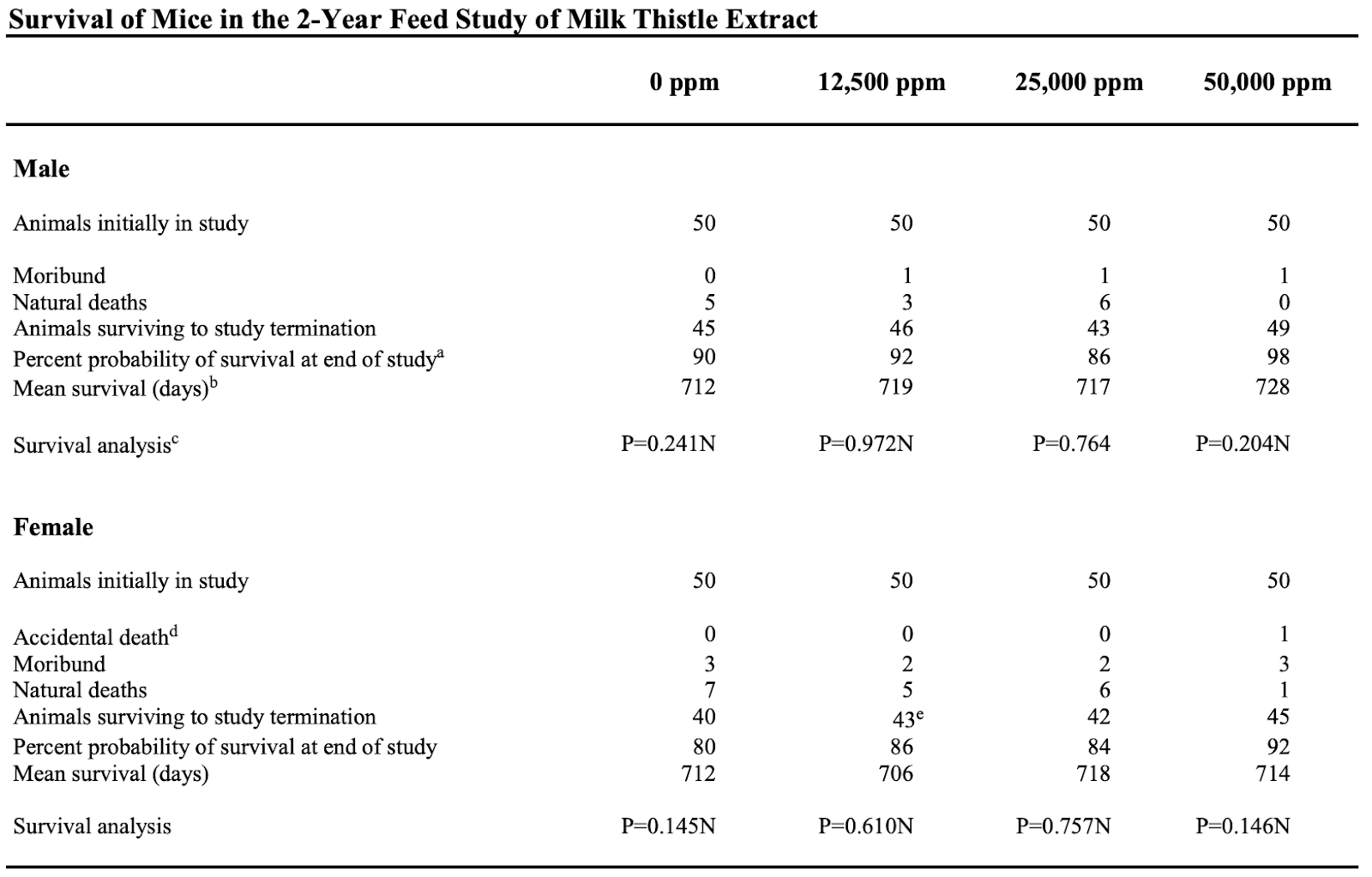
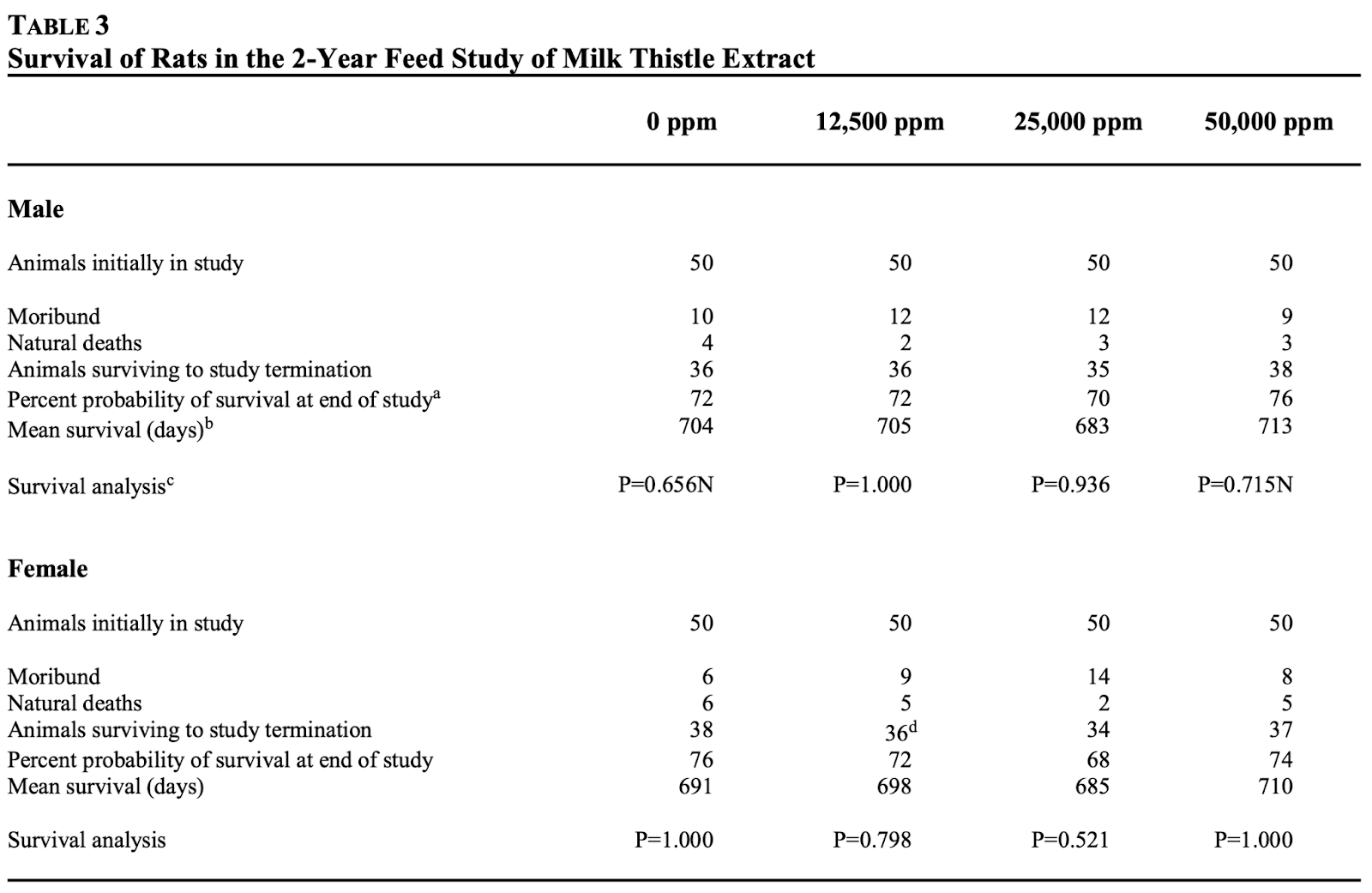
In 2-year rodent studies, milk thistle extract had no effect on survival vs control (mice control 85% vs milk thistle 89.7%; rats control 74% vs milk thistle 72%) (2011).
+4.31% increase in avg mice lifespan as part of cocktail that includes Bacopa, Milk Thistle, Ashwagandha, Curcumin (ITP).
Milk thistle and cancer (link)
Human Studies on Milk Thistle and Chemotherapy:
(2016) gave silymarin to children receiving methotrexate for acute lymphoblastic leukemia (ALL) to see if it could protect the liver and kidneys. 80 children received either silymarin or placebo. Silymarin improved some liver and kidney function results.
(2019) applied a silymarin gel to the chest of breast cancer patients undergoing radiotherapy after mastectomy, to prevent radiodermatitis. Those receiving the silymarin gel had reduced onset and severity of radiodermatitis compared to placebo gel.
(2015) gave silymarin to patients receiving cisplatin chemotherapy, to see if it offered protective effects on the liver and kidneys. Patients receiving 7 days of silymarin before cisplatin had lower blood urea nitrogen and creatinine levels compared to cisplatin alone. However, a higher 2-day dose showed no difference. Larger studies are needed.
(2020) found dietary milk thistle use during chemotherapy in breast cancer patients had no effect on survival outcomes. The authors say antioxidant supplements are not recommended during chemo/radiation as they may block cancer killing effects.
(2007) reviewed milk thistle for alcoholic and viral liver diseases, and found milk thistle was better than placebo for improving liver function, but more studies are needed.
Milk Thistle Inhibits the Growth of Cancer Cell Lines and Inhibits Tumor Initiation (link)
Epidermoid (A431).[11]
Colon (Caco-2).[12]
Ovarian (OVCA 433, A2780).[13]
Histiocytic lymphoma (U-937).[14]
In animal tumor models, tongue cancer,[17] skin cancer,[18-23] bladder cancer,[24] and adenocarcinoma of the colon [25,26] and small intestine [26] have been investigated. These studies have tested the ability of silymarin or silibinin to:
Mitigate the toxicity associated with chemotherapy agents.
Enhance the efficacy of chemotherapy agents.
Inhibit the growth of cancer cell lines and inhibit tumor initiation or tumor promotion.
Clinical Summary (link)
Milk thistle may reduce chemotherapy-induced hepatotoxicity in children with acute lymphoblastic leukemia (20), and cisplatin-induced nephrotoxicity (28) as well as improve capecitabine-induced hand-foot syndrome (6) and radiation therapy-induced mucositis (3). Topical administration of a silymarin gel was reported to reduce the severity of radiodermatitis and delay its occurrence (47).
Telomerase Inhibitors and Activators: Pharmaceutical Importance, 2017
Silibinin Inhibits the Invasion and Migration of Renal Carcinoma 786-O Cells In Vitro, Inhibits the Growth of Xenografts In Vivo and Enhances Chemosensitivity to 5-Fluorouracil and Paclitaxel (2011)
Silibinin, a flavonoid antioxidant known for anti-hepatotoxic qualities, inhibits the invasion and migration of 786-O renal cell carcinoma cells. Studies showed that silibinin reduces MMP-2, MMP-9, u-PA, p-p38, and p-Erk1/2 expressions in concentration-dependent ways. Pre-treatments with Erk1/2 and p38 inhibitors led to decreased MMP-2 and u-PA expressions and reduced cell invasion. In a mice xenograft model, silibinin reduced tumor volume by 70.1% and weight by 69.7%. Furthermore, combining silibinin with drugs like 5-fluorouracil and paclitaxel increased their chemosensitivity. This highlights silibinin's potential in both inhibiting 786-O cell activity and boosting certain cancer treatments
The effect of silymarin on telomerase activity in the human leukemia cell line K562, 2012
Telomerase is seen as a potential cancer therapy target. Silymarin, derived from the plant Silybum marianum, shows anti-cancer effects, but its impact on telomerase activity in the K562 human leukemia cell line was unclear. This study examined silymarin's role in inducing apoptosis in K562 cells, focusing on its telomerase activity effect. Silymarin's treatment significantly inhibited K562 cell growth and telomerase activity. There was a direct link between telomerase inhibition and increased apoptosis in treated cells, suggesting a new anti-cancer mechanism for silymarin. This offers insights for future anti-telomerase therapies.
Effects of silymarin and silymarin-doxorubicin applications on telomerase activity of human hepatocellular carcinoma cell line HepG2, 2015
In studying Hepatocellular carcinoma (HCC) resistance to doxorubicin, this research explored the effects of silymarin (from milk thistle extract) and doxorubicin both individually and in combination on telomerase activity. The HepG2 cell line's reaction to these agents was tested using MTT and Checkerboard micro plate methods, with untreated cells as a control. While the combined doxorubicin-silymarin treatment showed indifferent antiproliferative effects, both agents at IC50 levels independently and combined led to a marked decrease in telomerase activity. Notably, except for a specific silymarin dosage, all treatments significantly increased lipid peroxidation levels. The findings indicate that both doxorubicin and silymarin hinder telomerase activity, warranting deeper molecular analysis.
Milk Thistle (link)
Milk thistle (Silybum marianum) is an herbal supplement that has been used for centuries to treat a wide range of liver conditions. The active ingredients are flavonolignans called silymarin and silybin.
Mechanisms of Action
Milk thistle exhibits hepatoprotective effects through antioxidant, anti-inflammatory, and antifibrotic mechanisms (Loguercio and Festi, 2011).
Antioxidant: Silymarin inhibits free radical formation and acts as a free radical scavenger. It increases levels of the antioxidant enzymes superoxide dismutase, glutathione, and glutathione peroxidase (Wellington and Jarvis, 2001; Cacciapuoti et al., 2013). Silybin chelates iron, further strengthening antioxidant effects (Borsari et al., 2001).
Anti-inflammatory: Silymarin downregulates and inhibits COX-2, reducing inflammatory mediators (Abenavoli and Bellentani, 2013). It also inhibits NF-kB, reducing proinflammatory cytokines like TNF-α and IL-1β (Schümann et al., 2003).
Antifibrotic: Silybin decreases platelet-derived growth factor, inhibiting activation of stellate cells into fibrogenic myofibroblasts. It also reduces TGF-β, a key mediator of liver fibrosis (Fabregat et al., 2016).
Efficacy for NAFLD
Several human studies suggest milk thistle may improve biomarkers in NAFLD:
In 25 NAFLD patients, silymarin 200 mg three times daily for 4 months significantly reduced fasting blood glucose (from 156 ± 46 to 133 ± 39 mg/dL), HbA1c (-1%), total cholesterol, triglycerides, and LDL compared to placebo (Kazazis et al., 2014).
In 36 patients, silymarin 600 mg/day for 12 months decreased insulin resistance and fasting insulin versus baseline (Velussi et al., 1997).
A trial in 66 NAFLD patients found transaminase levels were significantly lower with silymarin compared to metformin or pioglitazone over 4 months (Hajiaghamohammadi et al., 2012).
A pilot study in 25 NAFLD patients found a silybin-vitamin E-phospholipid complex improved markers of liver damage and fibrosis, and insulin resistance over 4 months (Loguercio et al., 2007).
While results are promising, larger and longer clinical trials are still needed to confirm efficacy. The current data suggests silymarin may improve glucose and lipid metabolism, liver enzymes, and markers of hepatic fibrosis in NAFLD.
Administration
Milk thistle is available as capsules, tablets, or liquid extracts. The typical daily dose is 140-800 mg silymarin, taken orally in 2-3 divided doses (Tamayo and Diamond, 2007). Silymarin has also been used intravenously as an antidote for Amanita mushroom poisoning (Hruby et al., 1983).
Adverse Effects
Milk thistle is generally considered safe at typical doses. Adverse effects are rare but may include diarrhea, abdominal pain, nausea, headache, joint pain, or rash (Tamayo and Diamond, 2007). High doses above 1500 mg/day may cause gastrointestinal upset or liver toxicity (Abenavoli and Bellentani, 2013).
Interactions
Milk thistle can inhibit cytochrome P450 and other liver enzymes, so may interact with certain medications metabolized by these pathways. Drug interactions should be monitored, but are likely not clinically significant at typical doses (Kawaguchi-Suzuki et al., 2014).
Conclusion
In summary, milk thistle has demonstrated antioxidant, anti-inflammatory, and antifibrotic effects that may benefit NAFLD and other liver diseases. Early research shows promise for improving markers of liver damage, glucose control, and dyslipidemia. However, larger clinical trials are still needed to establish efficacy and safety.
Non-Alcoholic Fatty Liver Disease (Life Extension / 2019)
Milk thistle contains compounds like silymarin that protect the liver through antioxidant and anti-inflammatory effects (2010; 2001).
For toxin-induced injury, milk thistle prevents damage when given before or during toxin exposure, including alcohol and amatoxins (2002; 1982).
In patients with alcoholic liver disease, 360 mg/day of a standardized milk thistle extract reduced ALT and AST compared to placebo (1993; 2007). Another trial found improvements in enzymes and pathology with milk thistle treatment (1982).
For NAFLD, 48 weeks of milk thistle markedly reduced fibrosis scores compared to placebo in two trials (2006; 2012). A meta-analysis of 8 trials concluded milk thistle significantly lowered ALT and AST in NAFLD patients versus controls (2017).
In patients with alcoholic or non-alcoholic cirrhosis, 420 mg/day of milk thistle increased 4-year survival to 58% compared to 39% for placebo (1989). Greatest benefits were seen in alcoholics.
Absorption of active compounds in milk thistle is enhanced when bound to phospholipids like phosphatidylcholine (2016).
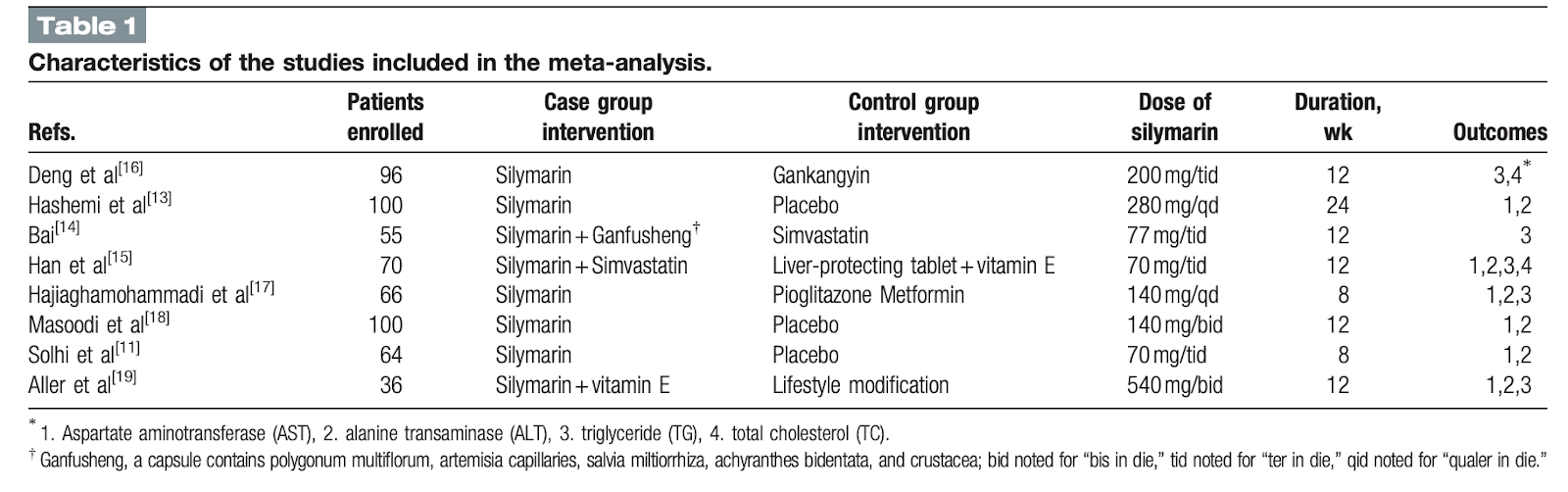
The therapeutic effect of silymarin in the treatment of nonalcoholic fatty disease: A meta-analysis (PRISMA) of randomized control trials (2017)
Background: Silymarin (SIL) is an active extraction of the silybum marianum, milk thistle, which is an ancient medicinal plant for treatment of various liver diseases for centuries. This study is to assess the therapeutic effect of SIL in the treatment of nonalcoholic fatty liver disease through meta-analysis.
Methods: Published randomized controlled trials (RCTs) were included from electronic databases (PubMed, Embase, Cochrane library, Web of Science, and so forth). Cochrane handbook was applied to evaluate the methodological quality. All statistical analyses were directed by Revman 5.3 software, and statistical significance was defined as P < .05.
Results: Eight RCTs involved 587 patients were included in this study. The results showed that SIL reduced the AST and ALT levels more significantly than the control group (AST UI/L: MD = -6.57; 95% CI, -10.03 to -3.12; P = .0002; ALT UI/L: MD = -9.16; 95% CI, -16.24 to -2.08; P = .01). Compared with other interventions, there were significant differences decreasing AST and ALT levels when SIL was used alone (AST UI/L: MD = -5.44; 95% CI, -8.80 to -2.08; P = .002; ALT UI/L: MD = -5.08; 95% CI, -7.85 to -2.32; P = .0003).
Conclusion: SIL has positive efficacy to reduce transaminases levels in NAFLD patients. SIL can be an encouraging and considerable phytotherapy for NAFLD patients.


A Randomized Trial of Silymarin for the Treatment of Nonalcoholic Steatohepatitis (2017)
[NASH - reduced fibrosis progression]
Methods: We performed a randomized, double-blind, placebo-controlled trial of consecutive adults with biopsy-proven NASH and a NAFLD activity score (NAS) of 4 or more at a tertiary care hospital in Kuala Lumpur, Malaysia, from November 2012 through August 2014. Patients were randomly assigned to groups given silymarin (700 mg; n = 49 patients) or placebo (n = 50 patients) 3 times daily for 48 weeks. After this 48-week period, liver biopsies were repeated. The primary efficacy outcome was a decrease of 30% or more in NAS; findings from 48-week liver biopsies were compared with those from the baseline biopsy. Secondary outcomes included changes in steatosis, lobular inflammation, hepatocyte ballooning, NAS and fibrosis score, and anthropometric measurements, as well as glycemic, lipid, and liver profiles and liver stiffness measurements.
Results: The percentage of patients achieving the primary efficacy outcome did not differ significantly between the groups (32.7% in the silymarin group vs 26.0% in the placebo group; P = .467). A significantly higher proportion of patients in the silymarin group had reductions in fibrosis based on histology (reductions of 1 point or more; 22.4%) than did the placebo group (6.0%; P = .023), and based on liver stiffness measurements (decrease of 30% or more; 24.2%) than did the placebo group (2.3%; P = .002). The silymarin group also had significant reductions in mean aspartate aminotransferase to platelet ratio index (reduction of 0.14, P = .011 compared with baseline), fibrosis-4 score (reduction of 0.20, P = .041 compared with baseline), and NAFLD fibrosis score (reduction of 0.30, P < .001 compared with baseline); these changes were not observed in the placebo group (reduction of 0.07, P = .154; increase of 0.18, P = .389; and reduction of 0.05, P = .845, respectively). There was no significant difference between groups in number of adverse events; adverse events that occurred were not attributed to silymarin.
Conclusions: In a randomized trial of 99 patients, we found that silymarin (700 mg, given 3 times daily for 48 weeks) did not reduce NAS scores by 30% or more in a significantly larger proportion of patients with NASH than placebo. Silymarin may reduce liver fibrosis but this remains to be confirmed in a larger trial. It appears to be safe and well tolerated.
Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unsuccessfully treated with interferon therapy: a randomized controlled trial (2012)
[No significant improvement in HCV outcomes, including ALT levels and fibrosis scores]
Context: The botanical product silymarin, an extract of milk thistle, is commonly used by patients to treat chronic liver disease, despite scant and conflicting evidence of its efficacy.
Objective: To determine the effect of silymarin on liver disease activity in patients with chronic hepatitis C virus (HCV) infection unsuccessfully treated with interferon-based therapy.
Design, setting, and participants: Multicenter, double-blind, placebo-controlled trial conducted at 4 medical centers in the United States. Participants included 154 persons with chronic HCV infection and serum alanine aminotransferase (ALT) levels of 65 U/L or greater who were previously unsuccessfully treated with interferon-based therapy. Enrollment began in May 2008 and was completed in May 2010, with the last follow-up visit completed in March 2011.
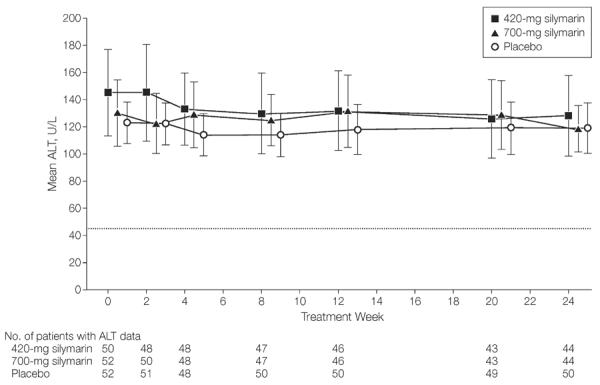
Intervention: Participants were randomly assigned to receive 420-mg silymarin, 700-mg silymarin, or matching placebo administered 3 times per day for 24 weeks.
Main outcome measures: The primary outcome measure was serum ALT level of 45 U/L or less (considered within the normal range) or less than 65 U/L, provided this was at least a 50% decline from baseline values. Secondary outcomes included changes in ALT levels, HCV RNA levels, and quality-of-life measures.
Results: After 24 weeks of treatment, only 2 participants in each treatment group (P ≥ .99) met the primary outcome measure (3.8% [95% CI, 0.5% to 13.2%] for placebo, 4.0% [95% CI, 0.5% to 13.7%] for 420-mg silymarin, and 3.8% [95% CI, 0.5% to 13.2%] for 700-mg silymarin). The mean decline in serum ALT activity at the end of treatment did not differ significantly (P = .75) across the 3 treatment groups (mean decline, -4.3 [95% CI, -17.3 to 8.7] U/L for placebo, -14.4 [95% CI, -41.6 to 12.7] U/L for 420-mg silymarin, -11.3 [95% CI, -27.9 to 5.4] U/L for 700-mg silymarin); there likewise were no significant differences in HCV RNA levels (mean change, 0.07 [95% CI, -0.05 to 0.18] log10 IU/mL for placebo, -0.03 [95% CI, -0.18 to 0.12] log10 IU/mL for 420-mg silymarin, 0.04 [95% CI, -0.08 to 0.16] log10 IU/mL for 700-mg silymarin; P = .54) or quality-of-life measures. The adverse event profile of silymarin was comparable with that of placebo.
Conclusion: Higher than customary doses of silymarin did not significantly reduce serum ALT levels more than placebo in participants with chronic HCV infection unsuccessfully treated with interferon-based therapy.
Milk Thistle (PDQ®)–Health Professional Version (link)
Hepatitis
In patients with hepatitis A and B, silymarin (140 mg daily for 3-4 weeks) reduced liver enzymes AST, ALT, and bilirubin compared to placebo (1978).
In patients with chronic hepatitis C, silymarin reduced fatigue, nausea, pain, appetite loss, and muscle/joint pain compared to no treatment (2008).
In HCV nonresponder patients, intravenous silibinin showed increased antiviral effects when combined with antiviral therapy compared to silibinin alone (2008).
In a study of 154 HCV patients, oral silymarin at 420-700 mg three times daily failed to significantly reduce ALT levels compared to placebo (2012).
In a large observational study of 2,637 patients with chronic liver disease, 560 mg/day silymarin for 8 weeks reduced liver enzymes AST, ALT, and GGT compared to baseline (1992).
Mushroom Poisoning
Silibinin given intravenously at 35-55 mg/kg was reported as an effective antidote for liver damage from Amanita mushroom poisoning, with no adverse events (1983).
A retrospective review also suggested silymarin is effective for treatment of Amanita mushroom poisoning based on improved liver histology (2002).
Other Conditions
In children with leukemia and chemotherapy-induced hepatotoxicity, silibinin 80-320 mg/day significantly decreased AST and trended toward decreased ALT compared to placebo (2010).
In men after prostatectomy, 570 mg/day silymarin improved quality of life, decreased LDL and cholesterol, and increased selenium compared to placebo (2010).
In patients getting radiation therapy, 420 mg/day silymarin resulted in lower mucositis scores compared to placebo (2016).
In breast cancer patients getting radiation, an external silymarin cream resulted in less radiation dermatitis compared to standard care (2011).
Milk Thistle (Memorial Sloan Kettering)
Potential Benefits
Used for cirrhosis, hepatitis, drug-induced liver damage. Protect liver during chemotherapy.
Preclinical studies show antioxidant, anticancer, anti-inflammatory, and neuroprotective effects (2002, 2002, 2008, 2008).
Small human studies show benefits for fatty liver disease and diabetes:
No significant improvement in HCV outcomes, including ALT levels and fibrosis scores, in 2 large studies (2012, 2011).
Mixed results for alcoholic liver disease. Improvements seen in some studies (1989, 2008), but not others.
Small studies show reduced liver toxicity during cancer treatment (2010, 2022). Topical silymarin improved skin reactions (Elyasi et al 2016, Karbasforooshan et al 2019).
Clinical Safety
Generally well tolerated. High doses may increase bilirubin and liver enzymes (2007).
Allergic reactions occur rarely (Wojas et al 2020, Adverse Reactions Advisory Committee 1999).
7 cases of pancreatitis reported with antipsychotics like haloperidol and risperidone (Woroń & Siwek, 2018).
Increased INR and bleeding seen with warfarin (Lash & Ward, 2019).
Drug Interactions
May inhibit CYP3A4 and increase drug levels in vitro (Venkataramanan et al 2000), but clinical significance is unclear (Mills et al 2005, Gurley et al 2006, Fuhr et al 2007).
Inhibits UGT in vitro (Mohamed & Frye 2011). Monitor with UGT substrates.
Decreased sirolimus clearance reported. Avoid with nivolumab in kidney transplants (Jiao et al 2009, Barnett et al 2017).
Dosage
Typical dose 140-800 mg/day standardized to 70-80% silymarin or silibinin.
Doses in studies range from 420 mg to 700 mg daily.
700 mg showed antioxidant effects (Bannwart et al 2010). 600 mg reduced skin reactions to cancer treatment (Elyasi et al 2016, Karbasforooshan et al 2019).
Higher doses increase risk of side effects like elevated liver enzymes.
In summary, milk thistle shows promise for metabolic and liver conditions, but efficacy is still inconclusive. Large, high-quality studies on clinically meaningful endpoints are needed. Caution is advised with high doses and drug interactions. More research on long-term safety is warranted.
A new silybin-vitamin E-phospholipid complex improves insulin resistance and liver damage in patients with non-alcoholic fatty liver disease: preliminary observations. Gut. (2006 )
Silybin combined with phosphatidylcholine and vitamin E in patients with nonalcoholic fatty liver disease: a randomized controlled trial. Free Radic Biol Med. (2012)
Silymarin in non alcoholic fatty liver disease. World J Hepatol. (2013)
Milk Thistle Lowers Blood Sugar, 2021
A randomized controlled trial tested milk thistle on people with type II diabetes.
The study involved 40 diabetic adults, aged 25-50, who were on anti-diabetic medications. They were given either a pill containing 140 mg of silymarin (an extract of milk thistle), or a placebo, three times daily for 45 days.
Compared with the placebo, milk thistle extract:
Reduced fasting blood sugar by 11%,
Reduced blood insulin levels by 14%,
Reduced insulin resistance, when cells ignore insulin’s signal to remove sugar from the blood, by 26%,
Reduced triglyceride levels by 24%,
Raised HDL (“good”) cholesterol by 7%,
Reduced the triglyceride-to-HDL ratio by 28%, and
Increased insulin sensitivity, how well cells respond to insulin, by over 5.5%.
Silymarin inhibits endothelial progenitor cells' senescence and protects against the antiproliferative activity of rapamycin: preliminary study, 2010
Rapamycin, an antiproliferative agent used on drug-eluting stents, induces endothelial progenitor cells (EPCs) senescence through telomerase inactivation and may impair the reendothelization of an injured arterial wall, leading to thrombosis. We examined whether silymarin, a complex of flavonolignans with hepatoprotective and antioxidative properties, can protect EPCs against rapamycin-induced senescence. Mononuclear cells were isolated from peripheral blood of healthy volunteers. EPCs were cultured in endothelial cell growth medium-2 in the presence or absence of rapamycin (0.1 ng/mL) and/or silymarin (12.5–50 μg/mL). EPCs senescence–associated b-galactosidase activity, telomerase activity, and prolifertive activity were measured. The influence on tubular-like structure formation in vitro was investigated, and colony-forming assay on methylcellulose plates was performed. Silymarin increased telomerase activity 3-fold, reduced the number of senescent cells, and increased EPC proliferative activity (up to 64%) in comparison with cells cultured with rapamycin alone. Moreover, silymarin partially prevented impairment of tubular-like structure formation in Matrigel by rapamycin. These findings suggest that silymarin counteracts the inhibitory effects of rapamycin in EPCs. Silymarin may protect EPCs against the antiproliferative effects of rapamycin and restore their reconstructive ability.
Toxicology and carcinogenesis studies of milk thistle extract (2011)
Control group (100 mice): 85% @ 2 years
Milk Thistle group (300 mice): 89.7% @ 2 years
z-score = 1.28
P-value = 10%
Control group (100 rats): 74% @ 2 years
Milk Thistle group (300 rats): 72% @ 2 years
Avg between rats and mice: 79.5% (control) -> 80.85% (experiment)


Comments