H1-Antihistamines / Loratadine (Claritin) / Desloratadine
Histamine and histamine receptor H1 (HRH1) are frequently increased in the tumor microenvironment and induce T cell dysfunction. Mechanistically, HRH1-activated macrophages polarize toward an M2-like immunosuppressive phenotype with increased expression of the immune checkpoint VISTA, rendering T cells dysfunctional. HRH1 knockout or antihistamine treatment reverted macrophage immunosuppression, revitalized T cell cytotoxic function, and restored immunotherapy response.
Allergy, via the histamine-HRH1 axis, facilitated tumor growth and induced immunotherapy resistance in mice and humans. Importantly, cancer patients with low plasma histamine levels had a more than tripled objective response rate to anti-PD-1 (immunotherapy) treatment compared with patients with high plasma histamine.
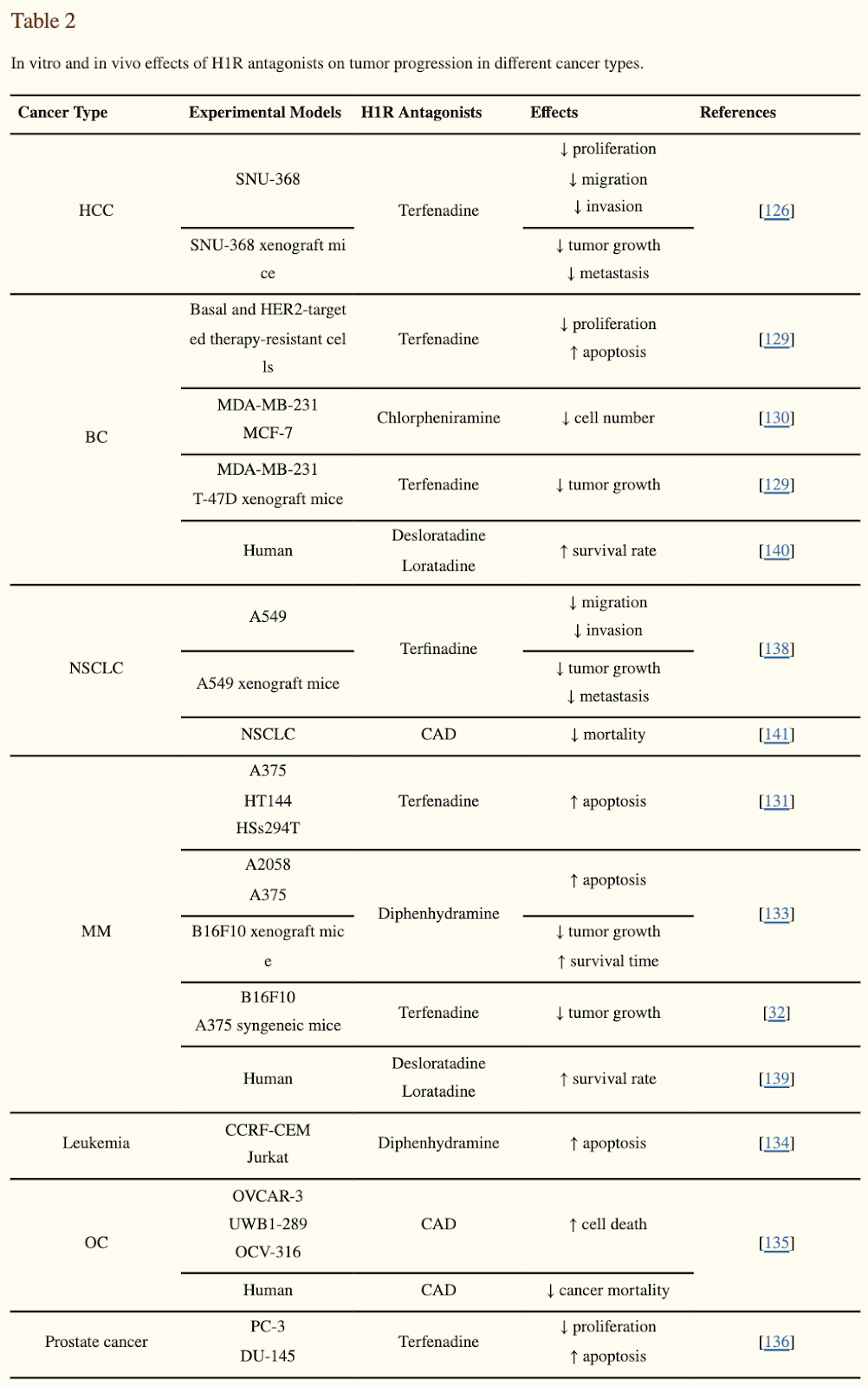
H1 antihistamines were found to induce anti-cancer effects across multiple cell lines (CLL, HCC, BC, NSCLC, MM, OC, PC…). Induce cancer-specific, lysosome-dependent cell death and sensitize cancer cells to chemotherapy.
Desloratadine use was associated with an improved survival for all immunogenic tumors including kidney cancer. Loratadine use didn’t show an equally strong association.
Whole blood histamine content was Increased in 60% of patients with uncontrolled polycythemia vera. The urine histamine findings paralleled the blood findings in 90 per cent of the cases. Myelosuppressive agents produced a reduction in histamine. Treatment with phlebotomy alone produced no change in histamine levels. The incidence of pruritus increased 7-fold in patients with elevated histamine.
Loratadine exhibits anti-inflammatory activity through suppression of the NF-kB pathway.
Loratadine administration to C Elegans extended lifespan by 18%.
[NEGATIVE] Prescription H1 antihistamine users had a significantly higher weight, waist circumference, and insulin concentration than matched controls. Prolonged intake of desloratadine induced development of an obesity-like phenotype and signs of metabolic syndrome in rats.
[NEGATIVE] Loratadine should not be taken for more than 10 weeks in any year as there is a study showing that long-term use (but not short-term use) can increase breast cancer risk.
[Care oncology: Start taking claritin (antihistamine). 1 tablet daily. it helps so that cancer doesn't become resistant to treatment. you can start now]
Improved survival in several cancers with use of H 1-antihistamines desloratadine and loratadine (link)
Methods: We investigated survival and use of six common H1-antihistamines (cetirizine, clemastine, desloratadine, ebastine, fexofenadine and loratadine) in a nation-wide cohort of all 429,198 Swedish patients with ten types of immunogenic (gastric, colorectal/anal, pancreatic, lung, breast, prostate, kidney, and bladder cancer, melanoma and Hodgkin lymphoma) and six non-immunogenic (liver, uterine, ovarian, brain/CNS, and thyroid cancer and non-Hodgkin lymphoma) tumors diagnosed 2006–2017. Follow-up was until 2019–02–24.
Findings: Desloratadine use was associated with an improved survival for all immunogenic tumors, but not for the non-immunogenic ones. Loratadine use was associated with improved survival for some tumors. Use of the other antihistamines could not be shown to be consistently associated with improved survival to a statistically significant degree.
Fig. 1 Desloratadine use and tumor-specific mortality.
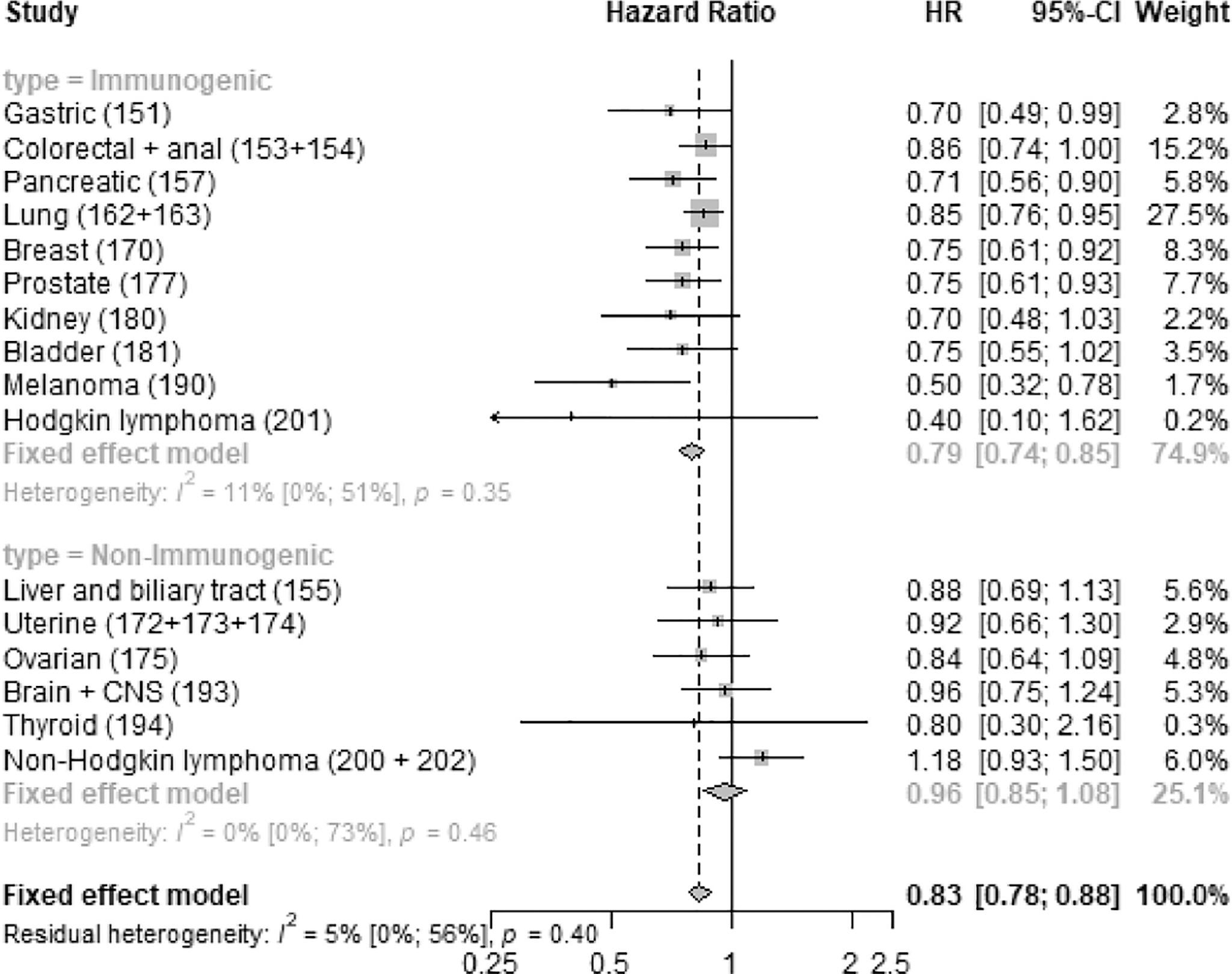
Fig. 5 Tumor-specific mortality of desloratadine users vs non-users with kidney cancer. Kidney cancer-specific survival probability plotted against time since diagnosis in years.
Antihistamines synergistically induce CLL cell death with TK inhibitors https://www.mdedge.com/hematology-oncology/article/227503/cll/antihistamines-synergistically-induce-cll-cell-death-tk

Three over-the-counter antihistamines, clemastine, desloratadine, and loratadine, preferentially induce cell death through lysosomal membrane permeabilization in chronic lymphocytic leukemia cells, compared with normal lymphocytes, according to the results of an in vitro study published in Leukemia Research.
In addition, the antihistamines showed a synergistic effect in killing off chronic lymphocytic leukemia (CLL) cells when combined with the tyrosine kinase inhibitor, ibrutinib, but not with chemotherapy, according to Aaron Chanas-Larue of CancerCare Manitoba, Winnipeg, Man., and colleagues.
Blood from CLL patients and age-matched healthy donors was collected, treated, and compared with two malignant B-cell lines. Cells were treated with the three different antihistamines at various concentrations alone and in the presence of ibrutinib. Cell death was determined by flow cytometry using fluorescent staining and EC50 (half-maximal effective concentration) values were calculated.
Of the three drugs, clemastine demonstrated the greatest degree of cytotoxicity, with a mean EC50 value of 12.3 mcmol in CLL cells. Desloratadine and loratadine also had a greater effect on leukemic cells, with mean EC50 values of 27.2 mcmol and 17.2 mcmol, respectively, according to the researchers.
Clemastine also showed the greatest tumor sensitivity, with an EC50 nearly three times lower for CLL cells (EC50, 12.3 mcmol) than for normal peripheral blood mononuclear cells (EC50, 32 mcmol). In addition, clemastine induced cell death over a 72-hour time course in CLL cells, and was equally effective against CLL cells with del17p, unmutated immunoglobulin heavy chain gene, or high Zeta-chain–associated protein kinase 70 expression.
Effective synergy
The researchers found that clemastine enhanced cell death when combined with targeted CLL therapies ibrutinib, idelalisib, or venetoclax, but did not enhance the activities of the chemotherapeutics fludarabine, chlorambucil, or bendamustine.
Ibrutinib increased cell death to the greatest degree when combined with antihistamines. The effect was demonstrated to be synergistic, showing “a unique interaction between the activities of the antihistamines and this inhibitor of the B-cell pathway, suggesting a clinical potential for this combination,” the authors stated.
“Repurposing well-characterized drugs such as antihistamines with defined mechanisms and toxicities allows for repositioning of these drugs to use in CLL treatment in the near future in the context of targeted therapies,” they concluded.
Antihistamine drugs might improve health of cancer patients receiving immunotherapy, 2021 (very good!)
The allergy mediator histamine confers resistance to immunotherapy in cancer patients via activation of the macrophage histamine receptor H1, 2021
Reinvigoration of antitumor immunity remains an unmet challenge. Our retrospective analyses revealed that cancer patients who took antihistamines during immunotherapy treatment had significantly improved survival. We uncovered that histamine and histamine receptor H1 (HRH1) are frequently increased in the tumor microenvironment and induce T cell dysfunction. Mechanistically, HRH1-activated macrophages polarize toward an M2-like immunosuppressive phenotype with increased expression of the immune checkpoint VISTA, rendering T cells dysfunctional. HRH1 knockout or antihistamine treatment reverted macrophage immunosuppression, revitalized T cell cytotoxic function, and restored immunotherapy response. Allergy, via the histamine-HRH1 axis, facilitated tumor growth and induced immunotherapy resistance in mice and humans. Importantly, cancer patients with low plasma histamine levels had a more than tripled objective response rate to anti-PD-1 treatment compared with patients with high plasma histamine. Altogether, pre-existing allergy or high histamine levels in cancer patients can dampen immunotherapy responses and warrant prospectively exploring antihistamines as adjuvant agents for combinatorial immunotherapy.
A pharmacological network for lifespan extension in Caenorhabditis elegans (link)
When Loratadine is given to worms, it extended lifespan by 18%.
Antihistaminic, Anti-Inflammatory, and Antiallergic Properties of the Nonsedating Second-Generation Antihistamine Desloratadine: A Review of the Evidence
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3500039/
Loratadine, an antihistamine drug, exhibits anti-inflammatory activity through suppression of the NF-kB pathway
Loratadine is an antihistamine drug that shows promise as an anti-inflammatory drug, but supportive studies are lacking. We elucidated the effects and mechanisms by which loratadine inhibits inflammatory responses. Molecular components were evaluated in macrophages by nitric oxide assay, polymerase chain reaction, luciferase assay, immunoblotting, overexpression strategies and cellular thermal shift assay. At the molecular level, loratadine reduced the levels of nitric oxide, iNOS, IL-1β, TNF-α, IL-6, and COX-2 in RAW264.7 cells treated with lipopolysaccharide. Loratadine also specifically inhibited the NF-kB pathway, targeting the Syk and Src proteins. Furthermore, loratadine bound Src in the bridge between SH2 and SH3, and bound Syk in the protein tyrosine kinase domain. The NF-kB signaling pathway was assessed along with putative binding sites through a docking approach. The anti-inflammatory effect of loratadine was tested using mouse models of gastritis, hepatitis, colitis, and peritonitis. Stomach tissue histopathology, liver morphology, and colon length in the loratadine group were improved over the group without loratadine treatment. Taken together, loratadine inhibited the inflammatory response through the NF-kB pathway by binding with the Syk and Src proteins.
Involvement of mast cells by the malignant process in patients with Philadelphia chromosome negative myeloproliferative neoplasms
The Philadelphia chromosome negative myeloproliferative neoplasms (MPNs) are clonal hematologic malignancies frequently characterized by a mutation in JAK2 (JAK2V617F). Peripheral blood (PB) CD34+ cells from patients with polycythemia vera (PV) and primary myelofibrosis (PMF) generated in vitro significantly fewer mast cells (MCs) than normal PB CD34+ cells. The numbers of MC progenitors assayed from MPN CD34+ cells were, however, similar to that assayed from normal CD34+ cells. A higher percentage of the cultured MPN MCs expressed FcɛRIα, CD63 and CD69 than normal MCs, suggesting that cultured MPN MCs are associated with an increased state of MC activation. Further analysis showed that a higher proportion of cultured PV and PMF MCs underwent apoptosis in vitro. By using JAK2V617F, MplW515L and chromosomal abnormalities as clonality markers, we showed that the malignant process involved MPN MCs. JAK2V617F-positive MC colonies were assayable from the PB CD34+ cells of each of the 17 JAK2V617F positive MPN patients studied. Furthermore, erlotinib, a JAK2 inhibitor, was able to inhibit JAK2V617F-positive PV MC progenitor cells, indicating that malignant MC progenitor cells are a potential cellular target for such JAK2 inhibitor-directed therapy.
A Study of Histamine in Myeloproliferative Disease (link)
SUMMARY
1. Whole blood histamine content was measured in 80 patients with myeloproliferative disease. Increased levels were found in 60 per cent of patients with uncontrolled polycythemia vera, in 7 per cent of patients with polycythemia vera being controlled by myelosuppressive therapy, and in 71 per cent of a group with "spent" polycythemia, myeloid metaplasia and myelofibrosis.
2. The excretion of histamine in the urine was measured in 60 patients, 30 with elevated blood histamine and 30 with normal blood histamine. The urine histamine findings paralleled the blood findings in 90 per cent of the cases.
3. Measurements of cell-poor and cell-rich fractions of blood showed that the histamine is contained in the white cell fraction. Elevated basophil counts were present in 50 per cent of the patients and occurred with the greatest frequency in the groups with elevated blood and urine histamine. A rough correlation between the basophil count and the histamine content of blood and white cell fractions was observed in normal subjects and most cases with myeloproliferative disease. Data obtained in some cases of myeloproliferative disease suggest that the histamine content of the basophil may be abnormal and that other granulocytes may contribute to the total leukocyte histamine.
4. Myelosuppressive agents produced a reduction in histamine (expressed per 109 myeloid cells) and a decrease in urine histamine as control of the myeloproliferative process was achieved. Treatment with phlebotomy alone produced no change in histamine levels.
5. The incidence of pruritus, upper gastrointestinal distress and urticarial manifestations was increased 7-fold, 4-fold and 12-fold, respectively, in patients with elevated histamine levels as compared with those who had normal histamine levels.
Pathophysiological Roles of Histamine Receptors in Cancer Progression: Implications and Perspectives as Potential Molecular Targets, 2021
Abstract
High levels of histamine and histamine receptors (HRs), including H1R~H4R, are found in many different types of tumor cells and cells in the tumor microenvironment, suggesting their involvement in tumor progression. This review summarizes the latest evidence demonstrating the pathophysiological roles of histamine and its cognate receptors in cancer biology. We also discuss the novel therapeutic approaches of selective HR ligands and their potential prognostic values in cancer treatment. Briefly, histamine is highly implicated in cancer development, growth, and metastasis through interactions with distinct HRs. It also regulates the infiltration of immune cells into the tumor sites, exerting an immunomodulatory function. Moreover, the effects of various HR ligands, including H1R antagonists, H2R antagonists, and H4R agonists, on tumor progression in many different cancer types are described. Interestingly, the expression levels of HR subtypes may serve as prognostic biomarkers in several cancers. Taken together, HRs are promising targets for cancer treatment, and HR ligands may offer novel therapeutic potential, alone or in combination with conventional therapy. However, due to the complexity of the pathophysiological roles of histamine and HRs in cancer biology, further studies are warranted before HR ligands can be introduced into clinical settings.
Desloratadine, a Novel Antigrowth Reagent for Bladder Cancer
Desloratadine, a potent antagonist for human histamine H1 receptor, has been revealed to exhibit antihistaminic activity and anti-inflammatory activity. However, it is not yet known whether desloratadine has any effect on the biological behaviors of tumor cells. In this study, we aimed to investigate the effects of desloratadine on cell growth and invasion in bladder cancer EJ and SW780 cells in vitro. We observed that desloratadine inhibited cell viability of EJ and SW780 cells in a dose- and time-dependent manner. Desloratadine treatment was also revealed to suppress colony-formation ability and induce cell cycle arrest at G1 phase in EJ cells. Desloratadine promoted cell apoptosis via modulating the expression of Bcl-2, Bax, cleaved caspase 3, and cleaved caspase 9 in EJ and SW780 cells. Western blot resulted showed that desloratadine also impaired the expression of autophagy-related proteins, such as Beclin 1, P62, and LC3I/II in EJ and SW780 cells; while autophagy inhibitor LY294002 reversed the effects of desloratadine on these proteins. Moreover, desloratadine remarkably attenuated cell migration and invasion. Furthermore, we illustrated that desloratadine downregulated the expression of N-cadherin, Vimentin, Snail1, and Snail2, while upregulated the expression of E-cadherin in EJ and SW780 cells in vitro. The level of interleukin 6 was reduced in desloratadine-treated cells, while upregulation of interleukin 6 significantly abolished the anticancer activity of desloratadine in cell invasion and Bcl-2, Bax, Beclin1, LC3-I/II, N-cadherin, and E-cadherin expression in EJ cells. Taken together, our data suggest a potential anticancer activity of desloratadine on cell growth and invasion for bladder cancer, which may be mediated by diminishing the epithelial-to-mesenchymal transition and interleukin 6.
Histamine H1 receptor antagonists selectively kill cisplatin-resistant human cervical cancer cells, 2021
Cancer therapy is often hampered by the disease’s development of resistance to anticancer drugs. We previously showed that the autonomously upregulated product of fibroblast growth factor 13 gene (FGF13; also known as FGF homologous factor 2 (FHF2)) is responsible for the cisplatin resistance of HeLa cisR cells and that it is likely responsible for the poor prognosis of cervical cancer patients treated with cisplatin. Here we show that cloperastine and two other histamine H1 receptor antagonists selectively kill HeLa cisR cells at concentrations that little affect parental HeLa S cells. The sensitivity of HeLa cisR cells to cloperastine was abolished by knocking down FGF13 expression. Cisplatin-resistant A549 cisR cells were similarly susceptible to cloperastine. H2, H3, and H4 receptor antagonists showed less or no cytotoxicity toward HeLa cisR or A549 cisR cells. These results indicate that histamine H1 receptor antagonists selectively kill cisplatin-resistant human cervical cancer cells and suggest that this effect is exerted through a molecular mechanism involving autocrine histamine activity and high-level expression of FGF13. We think this represents a potential opportunity to utilize H1 receptor antagonists in combination with anticancer agents to treat cancers in which emergent drug-resistance is preventing effective treatment.
Astemizole: an old anti-histamine as a new promising anti-cancer drug, 2011
Mortality-to-incidence ratio in cancer patients is extremely high, positioning cancer as a major cause of death worldwide. Despite hundreds of clinical trials for anti-cancer drugs that are currently in progress, most clinical trials for novel drug treatments fail to pass Phase I. However, previously developed drugs with novel anti-tumor properties offer a viable and cost-effective alternative to fight cancer. Histamine favors the proliferation of normal and malignant cells. Several anti-histamine drugs, including astemizole, can inhibit tumor cell proliferation. Astemizole has gained enormous interest since it also targets important proteins involved in cancer progression, namely, ether à-go-go 1 (Eag1) and Eag-related gene (Erg) potassium channels. Furthermore, Eag1 is thought to be an important marker and a therapeutic target for several different cancers. Astemizole inhibits Eag1 and Erg channel activity, and in cells expressing the Eag1 channel it decreases tumor cell proliferation in vitro and in vivo. It should be noted that some cardiovascular side effects have been reported for astemizole in a few rare cases. Nevertheless, astemizole stands as a very promising anti-cancer tool because it displays several anti-proliferative mechanisms, may serve as the basis to synthesize new anti-cancer agents, and has been previously administered clinically. In this review we will summarize the main findings relating to histamine and anti-histamines in cancer cell proliferation focusing on astemizole targets (Eag1 and Erg channels), and its anti-cancer effects in vitro and in vivo. We will also describe the side effects of astemizole and discuss proposals to overcome such effects in cancer patients. Finally, we will remark on the relevance of developing novel astemizole-related compounds.
Antihistamines as promising drugs in cancer therapy
Histamine is a biogenic amine, synthetized and released by mast cells, which acts as a vasodilator in several pathologic processes, namely in allergies and conjunctivitis. Its role on cancer is not fully understood. High levels of histamine have been associated with a bivalent behavior in regulation of several tumors (i.e. cervical, ovarian, vaginal, uterine, vulvar, colorectal cancer, and melanoma), promoting or inhibiting their growth. Histamine receptors (H1, H2, H3 and H4) are present in a vast group of cells, including tumor cells, making them sensitive to histamine variations. In this work, we review the role of mast cells and histamine on cancer development and the possibility of use antihistamines in the clinical management of this disease.
[NEGATIVE] Association of Prescription H1 Antihistamine Use With Obesity: Results From the National Health and Nutrition Examination Survey, 2010
Abstract
The incidence of obesity in the United States has reached epidemic proportions. Previous research has shown several medications exert noticeable effects on body-weight regulation. Histamine-1 (H1) receptor blockers commonly used to alleviate allergy symptoms are known to report weight gain as a possible side effect. Therefore, we investigated the association between prescription H1 antihistamine use and obesity in adults using data from the 2005-2006 National Health and Nutrition Examination Survey (NHANES). Adults taking prescription H1 antihistamines were matched by age and gender with controls and compared on the basis of body measurements, plasma glucose, insulin concentrations, and lipid levels. Prescription H1 antihistamine users had a significantly higher weight, waist circumference, and insulin concentration than matched controls. The odds ratio (OR) for being overweight was increased in prescription H1 antihistamine users. H1 antihistamine use may contribute to the increased prevalence of obesity and the metabolic syndrome in adults given these medications are also commonly used as over-the-counter remedies.
Antihistamines and Weight Gain | Obesity Medicine Association (link)
[NEGATIVE] Prolonged intake of desloratadine: mesenteric lymphatic vessel dysfunction and development of obesity/metabolic syndrome, 2019
This study aimed to establish mechanistic links between the prolonged intake of desloratadine, a common H1 receptor blocker (i.e., antihistamine), and development of obesity and metabolic syndrome. Male Sprague-Dawley rats were treated for 16 wk with desloratadine. We analyzed the dynamics of body weight gain, tissue fat accumulation/density, contractility of isolated mesenteric lymphatic vessels, and levels of blood lipids, glucose, and insulin, together with parameters of liver function. Prolonged intake of desloratadine induced development of an obesity-like phenotype and signs of metabolic syndrome. These alterations in the body included excessive weight gain, increased density of abdominal subcutaneous fat and intracapsular brown fat, high blood triglycerides with an indication of their rerouting toward portal blood, high HDL, high fasting blood glucose with normal fasting and nonfasting insulin levels (insulin resistance), high liver/body weight ratio, and liver steatosis (fatty liver). These changes were associated with dysfunction of mesenteric lymphatic vessels, specifically high lymphatic tone and resistance to flow together with diminished tonic and abolished phasic responses to increases in flow, (i.e., greatly diminished adaptive reserves to respond to postprandial increases in lymph flow). The role of nitric oxide in this flow-dependent adaptation was abolished, with remnants of these responses controlled by lymphatic vessel-derived histamine. Our current data, considered together with reports in the literature, support the notion that millions of the United States population are highly likely affected by underevaluated, lymphatic-related side effects of antihistamines and may develop obesity and metabolic syndrome due to the prolonged intake of this medication.
Is the next 'new' cancer drug already in your medicine cabinet? Antihistamines may have anti-cancer properties -- ScienceDaily (link)
Can antihistamines like Cimetidine, Desloratadine and Loratadine play an integrative role in cancer cure?
17 May 2020
Antihistamines can reduce metastases and increase cancer survival
Cimetidine, or Tagamet, has been shown in research to increase cancer survial following colorectal cancer surgery; Desloratadine and Loratadine have been shown to increase survival of both ER+ve and ER-ve breast cancer patients by more than 30 per cent. Here we look at just how antihistamines might help fight cancer. (Chris Woollams; CANCERactive).
Histamines are essential to cancer proliferation
It is of no surprise then that high histamine levels have been found in people with breast cancer, colorectal cancer, ovarian cancer, melanoma, cervical cancer and pancreatic cancer. Indeed, cancer cells have more histamine receptors on their surface than healthy cells, and these help inflame the cancer cell, help it spread and help cancer cells stick together to form tumours, and stick to organs like your lungs, bones and liver. Histamine levels also seem to increase simultaneously in peripheral tissues, almost as if they were drawing cancer cells towards them.
Antihistamines stop cancer cells sticking and spreading
2. Antihistamines like Desloratadine and Loratadine (Claritin) increase survival times
Unfortunately, all anti-histamines were not created equal. Cimetidine is an H2 antagonist like ranitidine and primarily used for acid reflux. Antihistamines like Desloratadine are H1 antagonists and used for allergies.
Swedish researchers(1) reviewed more than 50,000 women who had ER+ Breast cancer and those who simultaneously took a second generation antihistamine. When comparing users with non-users a significant survival improvement was seen for the users of 30 per cent or more. Various antihistamines were compared and Desloratadine provided the best results; Loratadine was not far behind.
Repurposed drugs for Oncology (ReDo) like Antihistamines seem able to reduce metastases, improve immune response and increase survival times
Although the exact method of action is not clear, there is more than enough research now to suggest using any of these inexpensive drugs is of significant benefit to people with cancer. There are a good number of scientific reviews on the Internet, for example (5) explaining how histamines enhance cancer growth and spread and how anti-histamines can block this action.
Anti-histamines reduce cancer membrane velco patches by blocking histamine receptor sites; and have immuno-modulating action increase immune response, They thus reduce cancer growth, cancer metastases and increase survival. We believe all our readers should consider the use of antihistamines as part of their Integrative Cancer Treatment Programme.
We do not believe Loratadine should be taken for more than 10 weeks in any year as there is a study showing that long-term use (but not short-term use) can increase breast cancer risk.
Repurposing Cationic Amphiphilic Antihistamines for Cancer Treatment
Loratadine, was associated with significantly reduced all-cause mortality among patients with non-localized NSCLC or any non-localized cancer when compared with use of non-CAD antihistamines and adjusted for potential confounders. Of the less frequently described CAD antihistamines, astemizole showed a similar significant association with reduced mortality as loratadine, and ebastine use showed a similar tendency. In line with this, sub-micromolar concentrations of loratadine, astemizole and ebastine sensitized cancer cells to chemotherapy and reverted multidrug resistance in NSCLC, breast and prostate cancer cells. Thus, CAD antihistamines may improve the efficacy of cancer chemotherapy.
Effects of antihistamine use on survival in breast cancer.
We investigated the effects of six antihistamines on breast cancer-specific and overall mortality in a nation-wide register-based study of all 61,627 Swedish women with newly diagnosed breast cancer. We found a consistently beneficial effect of desloratadine and loratadine use on breast cancer survival (with HRs ranging from 0.47-0.84 for desloratadine users relative to non-use), regardless of age, stage and estrogen receptor status, and a consistently negative effect on breast cancer survival of clemastine use.
Conclusions: We suggest trials of high-dose and long-duration desloratadine and loratadine as adjuvant treatment of breast cancer.
Brain Cancer (GBM) Halted in Mice Using Antihistamine Drug
Studies demonstrated an association between the fatty acid binding protein mammary-derived growth inhibitor (MDGI) and poorer prognosis in patients. MDGI shuttles fatty acids into cells, and the team’s studies found that blocking the MDGI gene in glioblastoma cell lines disrupted fatty acid transport into cells and incorporation into lysosomal membranes. Antihistamines and other drugs that increase the permeability of the lysosomal membrane can be considered as an enhancing therapy for patients with glioblastoma alongside established treatments.
Potential of Antihistamine Allergy Meds in Combatting Cancer
A specific group of antihistamine medications can eradicate leukaemic stem cells. These antihistamines cannot currently be used to combat leukaemia due to how quickly they degrade in the body and the lack of a direct administration method on cancer cells.
The second generation antihistamine, loratadine (LOR), was found to have tumor inhibiting effects on human colon carcinoma cell line.
Antihistamines and Ovarian Cancer Survival: Nationwide Cohort Study and in Vitro Cell Viability Assay
Evaluated the association between filled antihistamine prescriptions and cancer mortality. In our cohort study, CAD antihistamine use (≥1 prescription; n = 133) was associated with a hazard ratio of 0.63 (95% CI = 0.40 to 0.99) compared to use of non-CAD antihistamines (n = 304), and we found a tendency toward a dose-response association. In our cell viability assay, we found consistent and dose-dependent cytotoxicity for all CAD but not non-CAD antihistamines.
—---------
Antihistamines and azithromycin as a treatment for COVID-19 on primary health care – A retrospective observational study in elderly patients
Between March and April 2020, 84 elderly patients with suspected COVID-19 living in two nursing homes of Yepes, Toledo (Spain) were treated early with antihistamines (dexchlorpheniramine, cetirizine or loratadine), adding azithromycin in the 25 symptomatic cases. The outcomes are retrospectively reported. The primary endpoint is the fatality rate of COVID-19. The secondary endpoints are the hospital and ICU admission rates. Endpoints were compared with the official Spanish rates for the elderly. The mean age of our population was 85 and 48% were over 80 years old. No hospital admissions, deaths, nor adverse drug effects were reported in our patient population. By the end of June, 100% of the residents had positive serology for COVID-19. Although clinical trials are needed to determine the efficacy of both drugs in the treatment of COVID-19, this analysis suggests that primary care diagnosis and treatment with antihistamines, plus azithromycin in selected cases, may treat COVID-19 and prevent progression to severe disease in elderly patients.
Desloratadine inhibits constitutive and histamine-stimulated nuclear factor-kappaB activity consistent with inverse agonism at the histamine H1 Receptor
Background: The human histamine H1 receptor is constitutively active and exhibits basal activation of nuclear factor-kappaB (NF-kappaB), an important modulator of allergic inflammation. Certain H1 antihistamines have recently been shown to inhibit basal NF-kappaB activity by stabilizing the H1 receptor in an inactive state, a phenomenon called 'inverse agonism'.
Methods: We evaluated the effect of the new H1 antihistamine, desloratadine, on basal and histamine-stimulated NF-kappaB activity and compared it with the activities of other H1 antihistamines.
Results: Transiently transfected COS-7 cells co-expressing NF-kappaB-luciferase and the H1 receptor exhibited constitutive NF-kappaB activity. H1 antihistamines reduced basal NF-kappaB activity (rank order of potency: desloratadine > pyrilamine > cetirizine > loratadine > fexofenadine). Histamine stimulated basal NF-kappaB activity 8-fold, which was blocked by H1 antihistamines (rank order of potency: desloratadine > cetirizine > pyrilamine > loratadine > fexofenadine). Neither histamine nor antihistamines had any effect on NF-kappaB activity in the absence of the H1 receptor.
Conclusions: Desloratadine, acting through the histamine H1 receptor, inhibited basal NF-kappaB activity and can thus be classified as an inverse agonist. Inhibition of basal and histamine-stimulated NF-kappaB activity may help to explain previously reported inhibitory effects of desloratadine on allergic inflammatory mediators.
Chronic ingestion of H1-antihistamines increase progression of atherosclerosis in apolipoprotein E-/- mice, 2014
Although increased serum histamine levels and H1R expression in the plaque are seen in atherosclerosis, it is not known whether H1R activation is a causative factor in the development of the disease, or is a host defense response to atherogenic signals. In order to elucidate how pharmacological inhibition of histamine receptor 1 (H1R) signaling affects atherogenesis, we administered either cetirizine (1 and 4 mg/kg. b.w) or fexofenadine (10 and 40 mg/kg. b.w) to ApoE-/- mice maintained on a high fat diet for three months. Mice ingesting a low dose of cetirizine or fexofenadine had significantly higher plaque coverage in the aorta and cross-sectional lesion area at the aortic root. Surprisingly, the higher doses of cetirizine or fexofenadine did not enhance atherosclerotic lesion coverage over the controls. The low dose of fexofenadine, but not cetirizine, increased serum LDL cholesterol. Interestingly, the expression of iNOS and eNOS mRNA was increased in aortas of mice on high doses of cetirizine or fexofenadine. This may be a compensatory nitric oxide (NO)-mediated vasodilatory mechanism that accounts for the lack of increase in the progression of atherosclerosis. Although the administration of cetirizine did not alter blood pressure between the groups, there was a positive correlation between blood pressure and lesion/media ratio at the aortic root in mice receiving the low dose of cetirizine. However, this association was not observed in mice treated with the high dose of cetirizine or either doses of fexofenadine. The macrophages or T lymphocytes densities were not altered by low doses of H1-antihistamines, whereas, high doses decreased the number of macrophages but not T lymphocytes. The number of mast cells was decreased only in mice treated with low dose of fexofenadine. These results demonstrate that chronic ingestion of low therapeutic doses of cetirizine or fexofenadine enhance progression of atherosclerosis.
istamine H1 Receptor Promotes Atherosclerotic Lesion Formation by Increasing Vascular Permeability for Low-Density Lipoproteins, 2010
Objective— Enhanced endothelial permeability leading to intimal accumulation of low-density lipoproteins (LDL) stimulates the formation of atherosclerotic lesions. Histamine is known to increase vascular permeability. Whether this affects the formation of atherosclerotic lesions, however, remains elusive.
Methods and Results— Apolipoprotein E–null (ApoE−/−) mice treated with a histamine H1 receptor but not an H2 receptor antagonist developed 40% fewer atherosclerotic lesions in the aorta than placebo-treated controls. Similarly, genetic deletion of the H1 but not the H2 receptor resulted in a 60% reduction of lesions compared with ApoE−/− controls. The H1 receptor enhanced LDL permeability and lipid accumulation in the aorta, whereas plasma lipoprotein levels remained unaltered. In contrast, the H1 receptor did not affect proliferation and migration of vascular smooth muscle cells. Bone marrow transplantation confirmed that the formation of atherosclerotic lesions depended on the H1 receptor in vascular cells, whereas its presence in bone marrow-derived cells was irrelevant for plaque development. Mice expressing the H1 receptor exhibited higher levels of the chemokine (C-C motif) ligand 5 and higher numbers of macrophages and T-helper lymphocytes in plaques, higher numbers of circulating lymphocytes, and larger spleens.
Conclusion— These data indicate that H1 but not H2 receptor activation drives the formation of atherosclerotic lesions through an increased vascular permeability for LDL, which is associated with an enhanced secondary aortic and systemic inflammation. These data open novel perspectives for the prevention and treatment of atherosclerotic vascular disease.
Effect of chronic ingestion of a histamine H1 receptor antagonist on the progression of atherosclerosis in the apolipoprotein-E null mouse (54.1), 2011
Histamine (HIS) is a known modulator of vascular functions and its levels are elevated in coronary arteries in ischemic heart disease and variant angina. We have shown that HIS, acting via H1 receptors (H1R), stimulates the expression of IL-6, COX2, TLR2 and TLR4 in human endothelial cells. The study tested the effect of chronic ingestion of cetirizine (CET), an H1R antagonist, on atherosclerosis progression in ApoE-/- mice. CET containing water (5 mg/L) or plain water was supplied ad libitum to male ApoE-/- mice for 3 and 5 months, after which 24h urine, blood, and aorta were collected. The lesion coverage in the descending aorta and intima/media thickness at aortic root were quantified. The aortic tissue was also analyzed for COX1, COX2, H1R, IL10, Egr1 and MCP2 mRNA expression and for macrophages (MAC3+), T lymphocytes (CD3+) and mast cells (CD117+). A significant increase in plaque thickness was noted in CET-treated mice at 3 months but not at 5 months. Aortic lesion coverage between control and CET groups remained unchanged at 3 and 5 months. PGI2 and TXA2 indices in urine at 3 months showed reduction in PGI2/TXA2 ratio. RT- PCR data showed significantly decreased expression of COX1 and H1R but no changes in other genes. The lesion coverage, urinary prostanoid levels, gene expression, serum lipids, and MAC3+, CD3+ and CD117+ cell numbers were unchanged at 5 months. The results suggest that long-term use of CET does not alter atherosclerosis progression in ApoE-/- mice.
Histamine H1 type receptor antagonist loratadine ameliorates oxidized LDL induced endothelial dysfunction, 2019
Abstract
Oxidized LDL (ox-LDL) is one of the major risk factors of atherosclerosis. Endothelial dysfunction caused by ox-LDL is an early event in the pathogenesis of cardiovascular diseases. Preclinical studies have been performed to explore efficient means of preventing endothelial abnormalities. In this study, we revealed that loratadine, a histamine H1 type receptor specific antagonist, possesses a protective effect by relieving ox-LDL-induced endothelial inflammation. Treatment of endothelial cells with ox-LDL induces expression of the H1 receptor. The presence of loratadine in endothelial culture efficiently suppressed ox-LDL-induced attachment of monocytes to endothelial cells, production of ROS and vascular adhesion molecules, and induction cytokines including VCAM-1, E-selectin, TNF-α, IL-6 and IL-8. Mechanistically, we show that loratadine potently blocks ox-LDL-induced JNK activation as well as the AP-1 and NF-κB signaling pathways. Collectively, our data disclose a new role for loratadine in endothelial protection.
Influence of prior comorbidities and chronic medications use on the risk of COVID-19 in adults: a population-based cohort study in Tarragona, Spain
Objective: To investigate possible relationships between pre-existing medical conditions (including common comorbidities and chronic medications) and risk for suffering COVID-19 disease in middle-aged and older adults.
Design: Population-based retrospective cohort study.
Setting: Twelve primary care centres (PCCs) in Tarragona (Spain).
Participants: 79 083 people (77 676 community-dwelling and 1407 nursing-home residents), who were all individuals aged >50 years affiliated to the 12 participating PCCs.
Outcomes: Baseline cohort characteristics (age, sex, vaccinations, comorbidities and chronic medications) were established at study start (1st. March 2020) and primary outcome was time to COVID-19 confirmed by PCR among cohort members throughout the epidemic period (from 1st. March 2020 to 23rd. May 2020). Risk for suffering COVID-19 was evaluated by Cox regression, estimating multivariable HRs adjusted for age, sex, comorbidities and medications use.
Results: During the study period, 2324 cohort members were PCR-tested, with 1944 negative and 380 positive results, which means an incidence of 480.5 PCR-confirmed COVID-19 cases per 100 000 persons-period. Assessing the total study cohort, only age (HR 1.02; 95% CI 1.01 to 1.03; p=0.002), nursing-home residence (HR 21.83; 95% CI 16.66 to 28.61; p<0.001) and receiving diuretics (HR 1.35; 95% CI 1.04 to 1.76; p=0.026) appeared independently associated with increased risk. Smoking (HR 0.62; 95% CI 0.41 to 0.93; p=0.022), ACE inhibitors (HR 0.68; 95% CI 0.47 to 0.99; p=0.046) and antihistamine (HR 0.47; 95% CI 0.22 to 1.01; p=0.052) were associated with a lower risk. Among community-dwelling individuals, cancer (HR 1.52; 95% CI 1.03 to 2.24; p=0.035), chronic respiratory disease (HR 1.82; 95% CI 1.08 to 3.07; p=0.025) and cardiac disease (HR 1.53; 95% CI 1.06 to 2.19; p=0.021) emerged to be also associated with an increased risk. Receiving ACE inhibitors (HR 0.66; 95% CI 0.44 to 0.99; p=0.046) and influenza vaccination (HR 0.63; 95% CI 0.44 to 0.91; p=0.012) was associated with decreased risk.
Conclusion: Age, nursing-home residence and multiple comorbidities appear predisposing for COVID-19. Conversely, receiving ACE inhibitors, antihistamine and influenza vaccination could be protective, which should be closely investigated in further studies specifically focused on these concerns.


Comments