GLP-1 Agonists (Semaglutide)
GLP-1/GIP Receptor Agonists (Tirzepatide, Semaglutide)
Tirzepatide / Mounjaro
New diabetes/weight loss drug. FDA approved for T2D in May 2022, approval pending for weight loss.
Activates the body's receptors for GIP and GLP-1, whereas earlier similar drugs like Semaglutide, Liraglutide only activate GLP-1 (ref).
Obese participants lost 20.9% of body weight at the highest dose --- this is the biggest weight loss seen with any drug, approaching the results of bariatric surgery (ref).
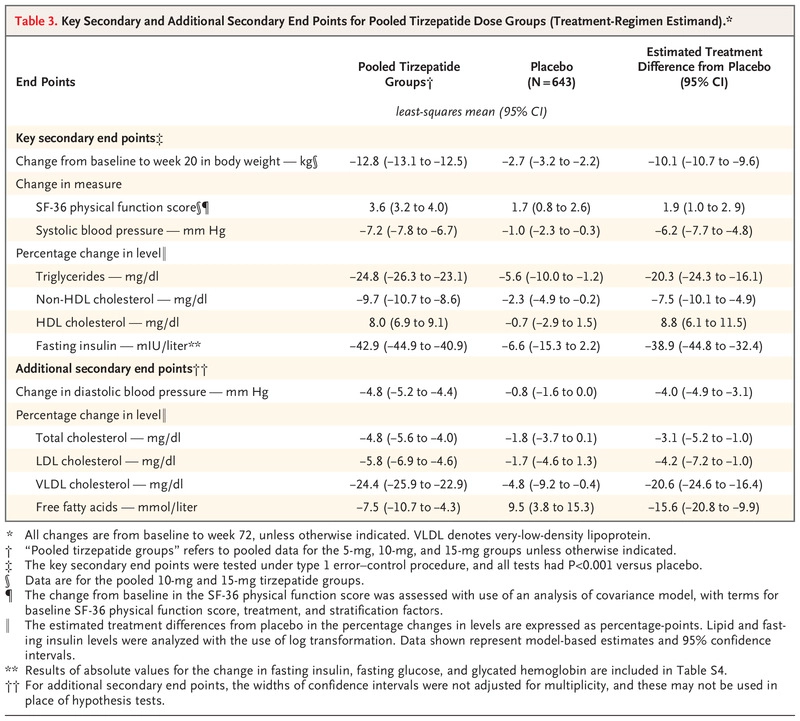
Increases insulin secretion in response to food, but paradoxically lowers basal insulin --- 42.9% drop in fasting insulin in obesity (ref).
Elevated insulin is probably the biggest activator of mTor in western societies. Huge drop in basal insulin suggests this is a life extension drug — the initial data is supportive.
Data from 4,887 tirzepatide users and 2,328 controls. The HRs for MACE-4 are 0.80 (95% CI, 0.57–1.11), cardiovascular mortality 0.90 (95% CI, 0.50–1.61) and all-cause mortality 0.80 (95% CI, 0.51–1.25) (ref).
Tirzepatide resulted in a significant 50% reduction in liver fat content (ref). Maybe the most effective of any drug — there’s no FDA approved drug for NAFLD.
Semaglutide
GLP-1 enhances satiety and reduces energy intake. Makes you practice CR by default.
Reduced all-cause mortality (HR=80%) and MACE (HR=76%) in Semaglutide RCTs.
Similarly, reduced all-cause mortality HR = 0.85 (95% CI 0.74 to 0.97, P = 0.02) in Liraglutide RCTs,
HOMA-IR decreased by 32% with semaglutide 0.5 mg and by 39% with semaglutide 1.0 mg (link).
Semaglutide reduced HS-CRP by 45% (link), SBP and DBP by -6 and -1.
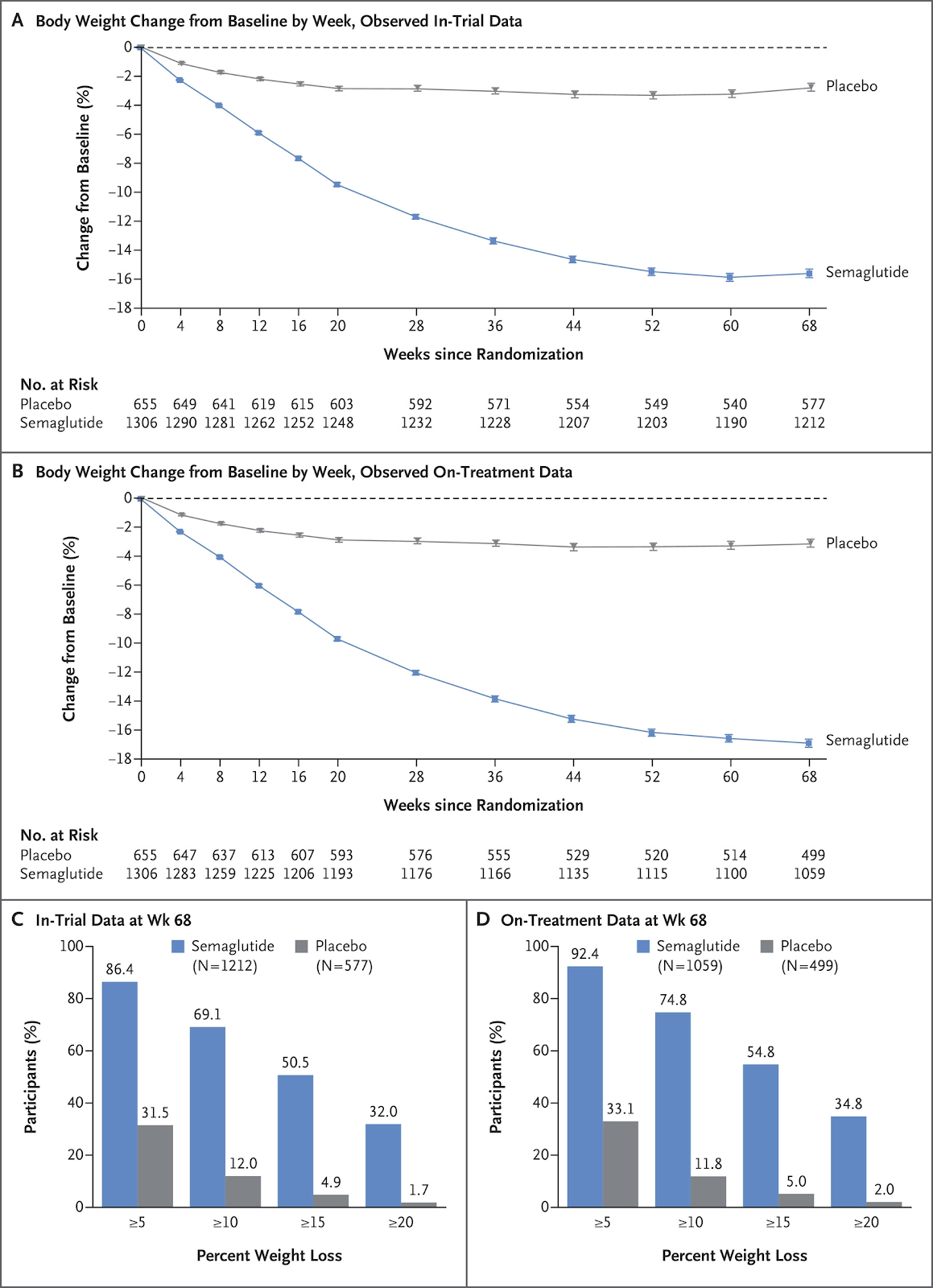
Semaglutide 2.4 mg/week resulted in body weight loss of 15% at week 68.
A promising treatment option for NAFLD or NASH.
Tirzepatide Once Weekly for the Treatment of Obesity, 2022

METHODS
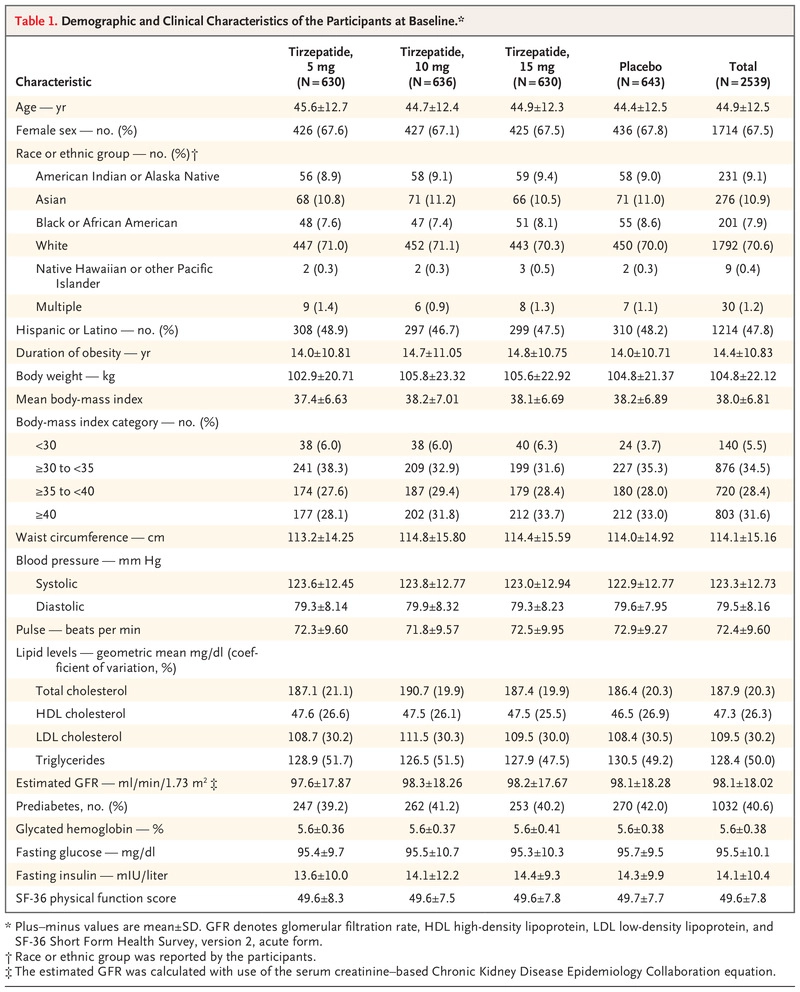
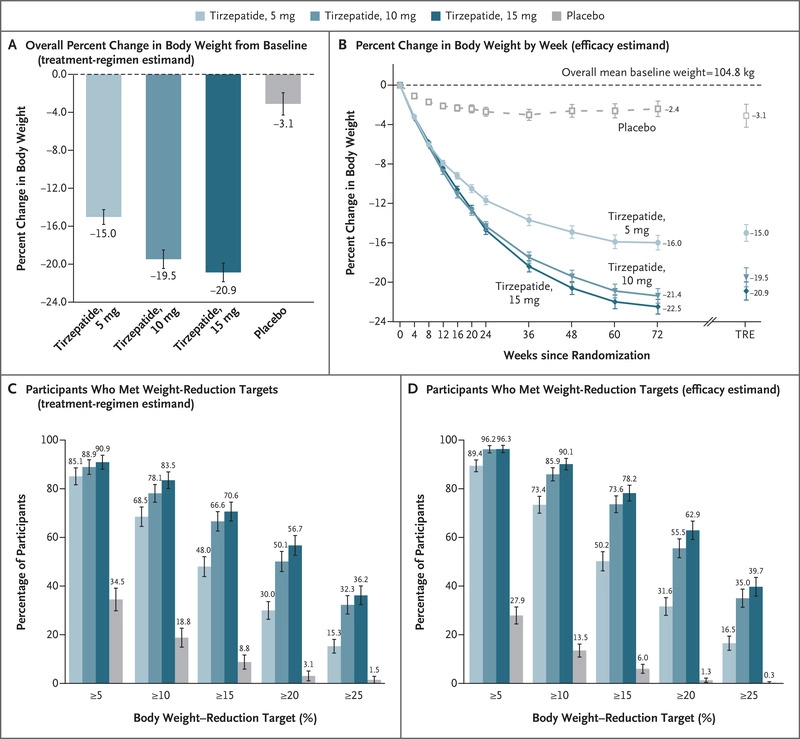
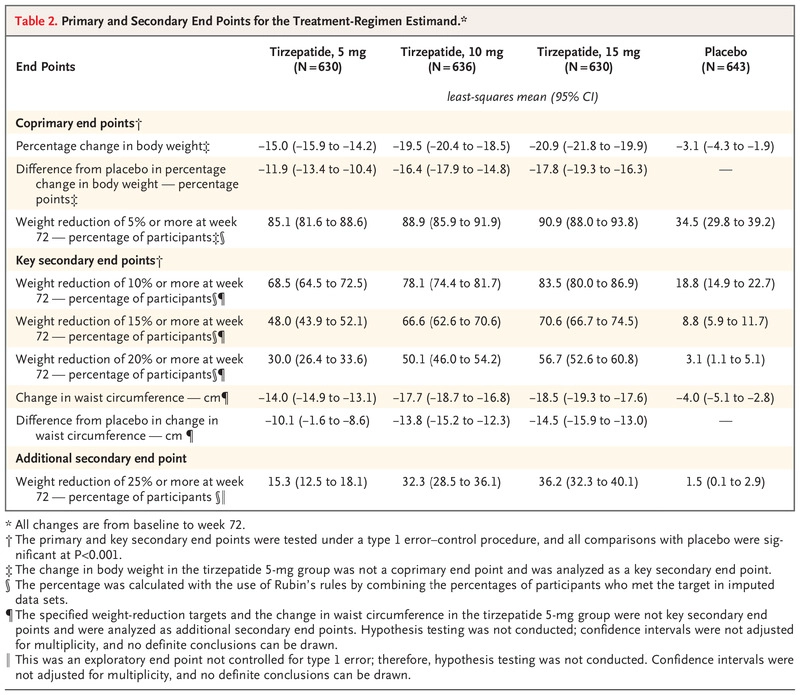
In this phase 3 double-blind, randomized, controlled trial, we assigned 2539 adults with a body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) of 30 or more, or 27 or more and at least one weight-related complication, excluding diabetes, in a 1:1:1:1 ratio to receive once-weekly, subcutaneous tirzepatide (5 mg, 10 mg, or 15 mg) or placebo for 72 weeks, including a 20-week dose-escalation period. Coprimary end points were the percentage change in weight from baseline and a weight reduction of 5% or more. The treatment-regimen estimand assessed effects regardless of treatment discontinuation in the intention-to-treat population.
Tirzepatide was initiated at a dose of 2.5 mg once weekly (or matching placebo) and was increased by 2.5 mg every 4 weeks during the dose-escalation period to reach a maintenance dose of up to 15 mg once weekly by week 20
RESULTS
At baseline, the mean body weight was 104.8 kg, the mean BMI was 38.0, and 94.5% of participants had a BMI of 30 or higher. The mean percentage change in weight at week 72 was −15.0% (95% confidence interval [CI], −15.9 to −14.2) with 5-mg weekly doses of tirzepatide, −19.5% (95% CI, −20.4 to −18.5) with 10-mg doses, and −20.9% (95% CI, −21.8 to −19.9) with 15-mg doses and −3.1% (95% CI, −4.3 to −1.9) with placebo (P<0.001 for all comparisons with placebo). The percentage of participants who had weight reduction of 5% or more was 85% (95% CI, 82 to 89), 89% (95% CI, 86 to 92), and 91% (95% CI, 88 to 94) with 5 mg, 10 mg, and 15 mg of tirzepatide, respectively, and 35% (95% CI, 30 to 39) with placebo; 50% (95% CI, 46 to 54) and 57% (95% CI, 53 to 61) of participants in the 10-mg and 15-mg groups had a reduction in body weight of 20% or more, as compared with 3% (95% CI, 1 to 5) in the placebo group (P<0.001 for all comparisons with placebo). Improvements in all prespecified cardiometabolic measures were observed with tirzepatide. The most common adverse events with tirzepatide were gastrointestinal, and most were mild to moderate in severity, occurring primarily during dose escalation. Adverse events caused treatment discontinuation in 4.3%, 7.1%, 6.2%, and 2.6% of participants receiving 5-mg, 10-mg, and 15-mg tirzepatide doses and placebo, respectively.
CONCLUSIONS
In this 72-week trial in participants with obesity, 5 mg, 10 mg, or 15 mg of tirzepatide once weekly provided substantial and sustained reductions in body weight.
Tirzepatide has a greater affinity to GIP receptors than to GLP-1 receptors, and this dual agonist behavior has been shown to produce greater reductions of hyperglycemia compared to a selective GLP-1 receptor agonist.[3] Signaling studies have shown that this is due to tirzepatide mimicking the actions of natural GIP at the GIP receptor.[12] However, at the GLP-1 receptor, tirzepatide shows bias towards cAMP (a messenger associated with regulation of glycogen, sugar and lipid metabolism) generation, rather than β-arrestin recruitment. This combination of preference towards GIP receptor and distinct signaling properties at GLP-1 suggest this biased agonism increases insulin secretion.[12] Tirzepatide has also been shown to increase levels of adiponectin, an adipokine involved in the regulation of both glucose and lipid metabolism, with a maximum increase of 26% from baseline after 26 weeks, at the 10 mg dosage.[3]
(Amazing % drop in fasting insulin, SBP, DBP!)

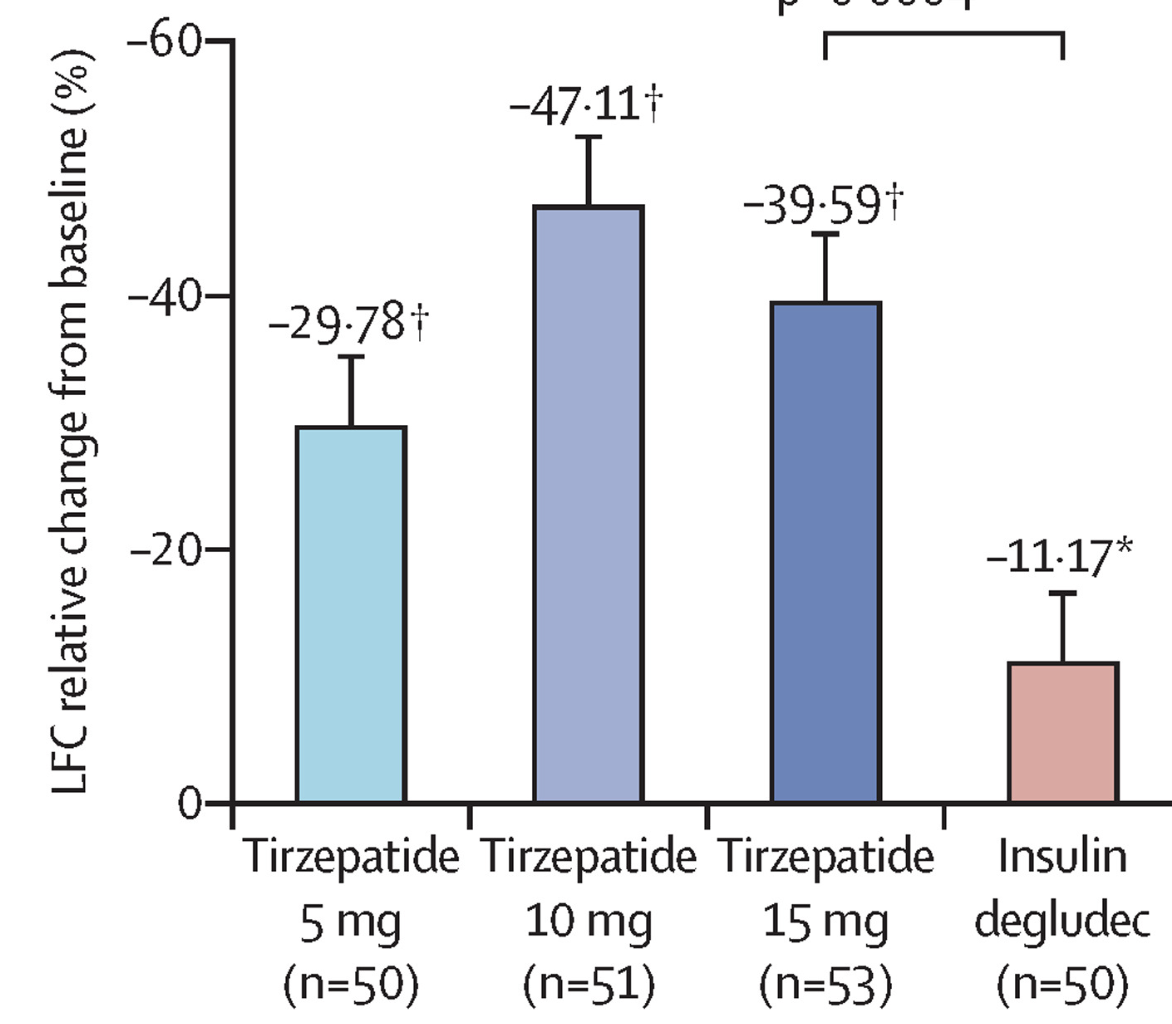
Effect of tirzepatide versus insulin degludec on liver fat content (LFC) and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial, 2022
This substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial was done at 45 medical research centres and hospitals across eight countries (Argentina, Austria, Greece, Hungary, Italy, Romania, Spain, and the USA). Eligible participants were adults with type 2 diabetes, a baseline HbA1c 7·0–10·5% (53–91 mmol/mol), a BMI of at least 25 kg/m2, stable weight, were insulin-naive, and on treatment with metformin alone or in combination with a SGLT2 inhibitor for at least 3 months before screening. In addition to the main study inclusion criteria, substudy participants had a fatty liver index of at least 60. Participants had an MRI scan and were randomised (1:1:1:1) in the main study to subcutaneous injection once per week of tirzepatide 5 mg, 10 mg, or 15 mg, or subcutaneous injection once per day of titrated insulin degludec, using an interactive web-response system, and were stratified by country, HbA1c, and concomitant oral anti-hyperglycaemic medication. The primary efficacy endpoint was the change from baseline in LFC (as measured by MRI-proton density fat fraction [MRI-PDFF]) at week 52 using pooled data from the tirzepatide 10 mg and 15 mg groups versus insulin degludec. Analyses were assessed in the enrolled MRI population, which consisted of participants in the modified intention-to-treat population of the main study who also had a valid MRI at either baseline or after baseline. This is a substudy of the trial registered with ClinicalTrials.gov, number NCT03882970, and is complete.
Findings
From April 1, 2019, to Nov 15, 2019, 502 participants were assessed for eligibility to participate in this substudy, 296 (59%) of whom were included in the enrolled MRI population and randomly assigned to treatment (tirzepatide 5 mg, n=71; tirzepatide 10 mg, n=79; tirzepatide 15 mg, n=72; and insulin degludec, n=74). Baseline demographics and clinical characteristics were similar across all treatment groups. From an overall mean baseline LFC of 15·71% (SD 8·93), the absolute reduction in LFC at week 52 was significantly greater for the pooled tirzepatide 10 mg and 15 mg groups (–8·09%, SE 0·57) versus the insulin degludec group (–3·38%, 0·83). The estimated treatment difference versus insulin degludec was –4·71% (95% CI –6·72 to –2·70; p<0·0001). The reduction in LFC was significantly correlated (p≤0·0006) with baseline LFC (ρ=–0·71), reductions in VAT (ρ=0·29), reductions in ASAT (ρ=0·33), and reductions in body weight (ρ=0·34) in the tirzepatide groups.
Interpretation
Tirzepatide showed a significant reduction in LFC and VAT and ASAT volumes compared with insulin degludec in this subpopulation of patients with type 2 diabetes in the SURPASS-3 study. These data provide additional evidence on the metabolic effects of this novel dual GIP and GLP-1 receptor agonist.

Tirzepatide cardiovascular event risk assessment: a pre-specified meta-analysis, 2022
Tirzepatide is a novel, once weekly, dual GIP/GLP-1 receptor agonist and is under development for the treatment of type 2 diabetes (T2D) and obesity. Its association with cardiovascular outcomes requires evaluation. This pre-specified cardiovascular meta-analysis included all seven randomized controlled trials with a duration of at least 26 weeks from the tirzepatide T2D clinical development program, SURPASS. The pre-specified primary objective of this meta-analysis was the comparison of the time to first occurrence of confirmed four-component major adverse cardiovascular events (MACE-4; cardiovascular death, myocardial infarction, stroke and hospitalized unstable angina) between pooled tirzepatide groups and control groups. A stratified Cox proportional hazards model, with treatment as a fixed effect and trial-level cardiovascular risk as the stratification factor, was used for the estimation of hazard ratios (HRs) and confidence intervals (CIs) comparing tirzepatide to control. Data from 4,887 participants treated with tirzepatide and 2,328 control participants were analyzed. Overall, 142 participants, 109 from the trial with high cardiovascular risk and 33 from the six trials with lower cardiovascular risk, had at least one MACE-4 event. The HRs comparing tirzepatide versus controls were 0.80 (95% CI, 0.57–1.11) for MACE-4; 0.90 (95% CI, 0.50–1.61) for cardiovascular death; and 0.80 (95% CI, 0.51–1.25) for all-cause death. No evidence of effect modifications was observed for any subgroups, although the evidence was stronger for participants with high cardiovascular risk. Tirzepatide did not increase the risk of major cardiovascular events in participants with T2D versus controls.
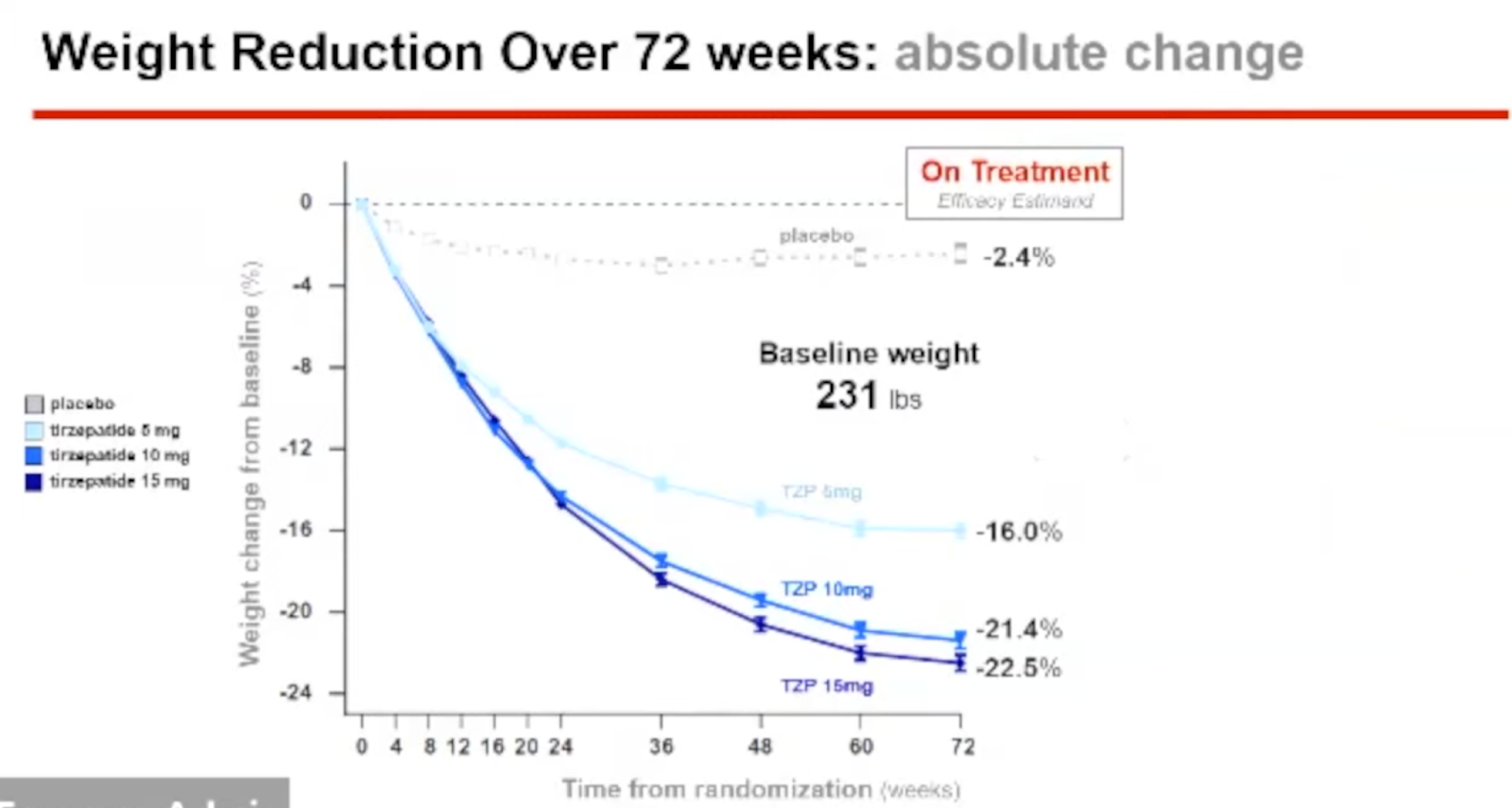
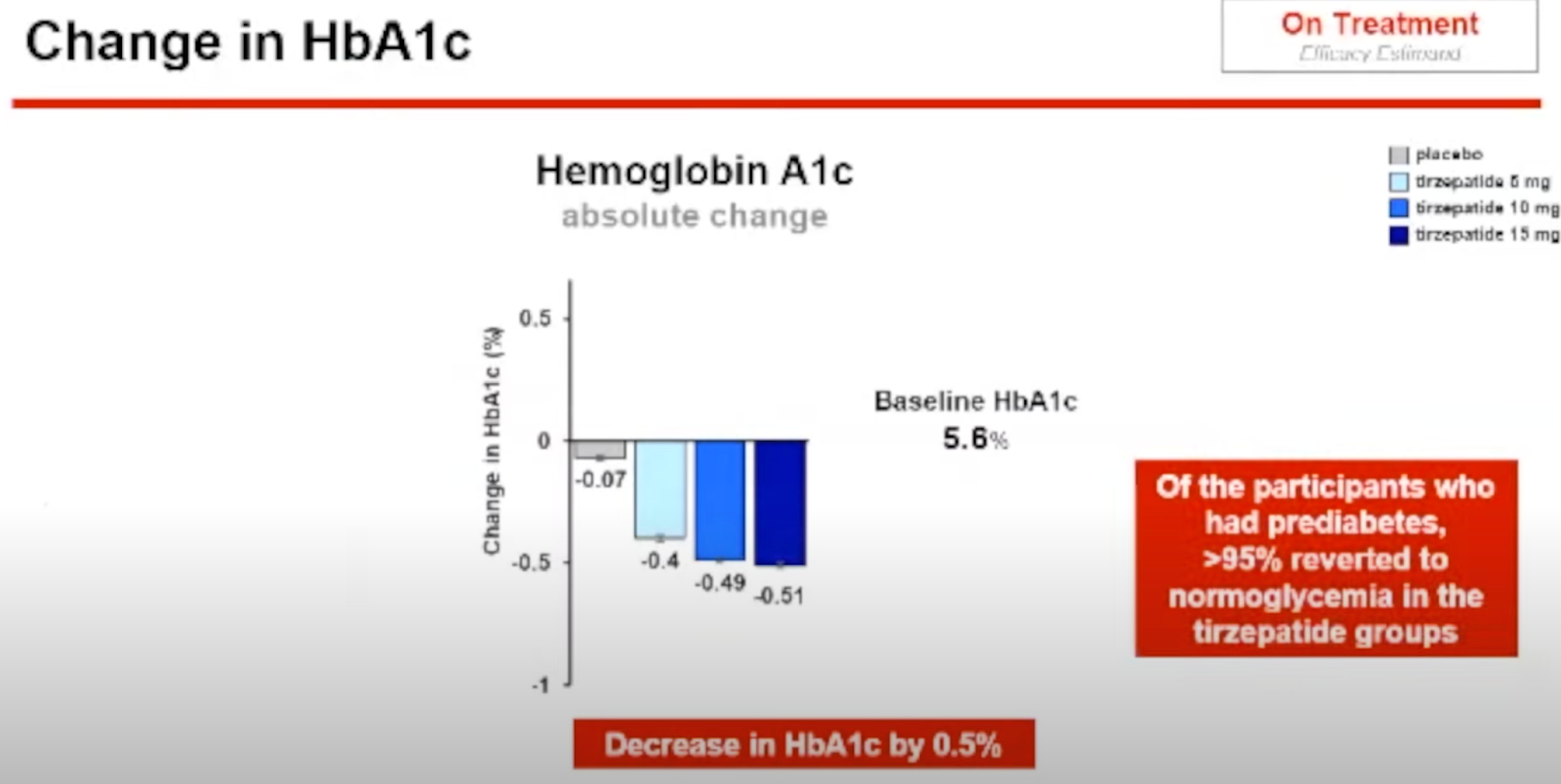
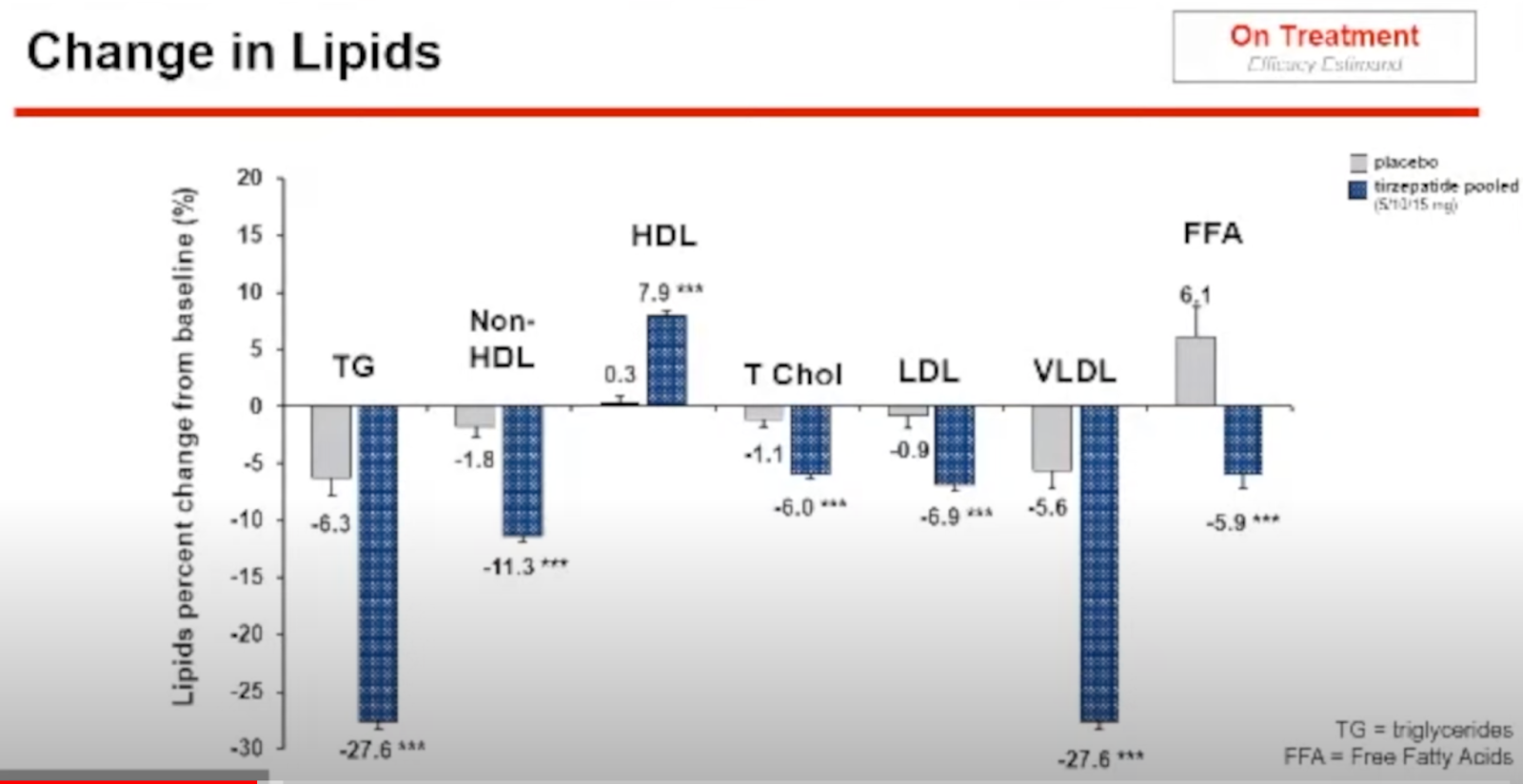
Surmount Press Briefing, 2022


Effects of Renal Impairment on the Pharmacokinetics of the Dual GIP and GLP-1 Receptor Agonist Tirzepatide
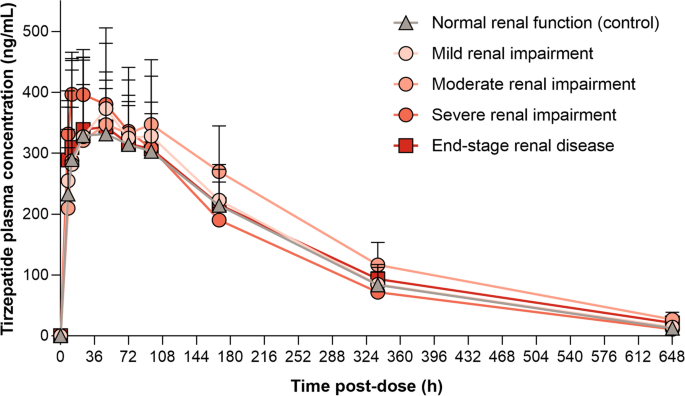
(12.5/9)/(10/7)=97%
GLP-1 analogue improves hepatic lipid accumulation by inducing autophagy via AMPK/mTOR pathway
The incidence of nonalcoholic fatty liver disease (NAFLD) keeps rising year by year, and NAFLD is rapidly becoming the most common liver disease worldwide. Clinical studies have found that glucagon-like peptide-1 (GLP-1) analogue, liraglutide (LRG), cannot only reduce glucose levels, but also improve hepatic lipase, especially in patients also with type 2 diabetes mellitus (T2DM). In addition, enhancing autophagy decreases lipid accumulation in hepatocytes. The aim of the present study is to explore the effect of LRG on hepatocyte steatosis and the possible role of autophagy. We set up an obesity mouse model with a high-fat diet (HFD) and induced hepatocyte steatosis with free fatty acids (FFA) in human L-O2 cells. LRG and two inhibitors of autophagy, Chloroquine (CQ) and bafilomycin A1 (Baf), were added into each group, respectively. The lipid profiles and morphological modifications of each group were tested. Immunohistochemistry, immunofluorescence staining and transmission electron microscopy (TEM) were used to measure autophagy in this study. The autophagy protein expression of SQSTM1 (P62), and LC3B, along with the signaling pathway proteins of mTOR, phosphorylated mTOR (p-mTOR), AMPK, phosphorylated AMPK (p-AMPK) and Beclin1, were evaluated by western blot. Our results showed that LRG improved hepatocyte steatosis by inducing autophagy, and the AMPK/mTOR pathway is involved. These findings suggest an important mechanism for the positive effects of LRG on hepatic steatosis, and provide new evidence for clinical use of LRG in NAFLD.
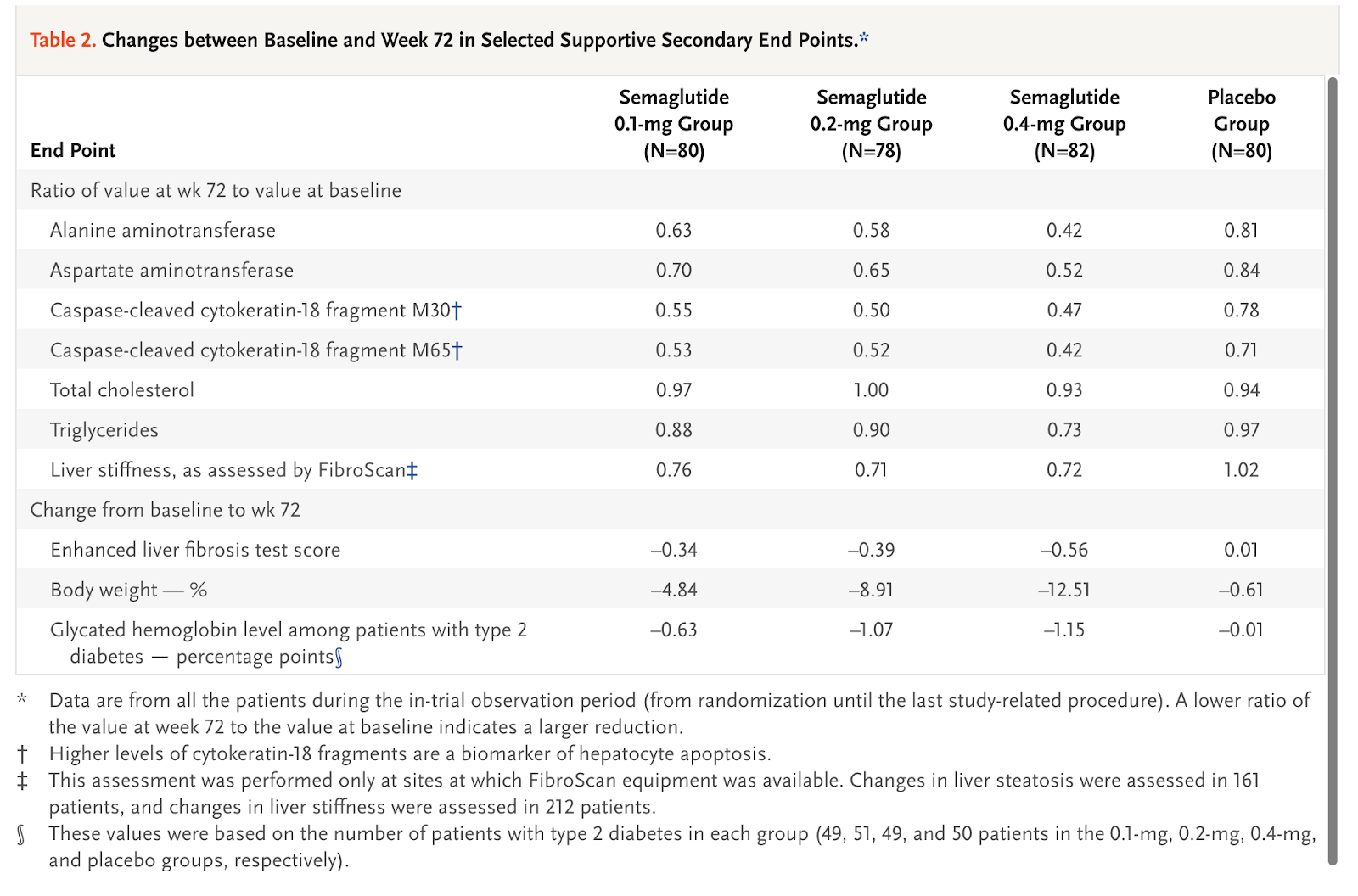
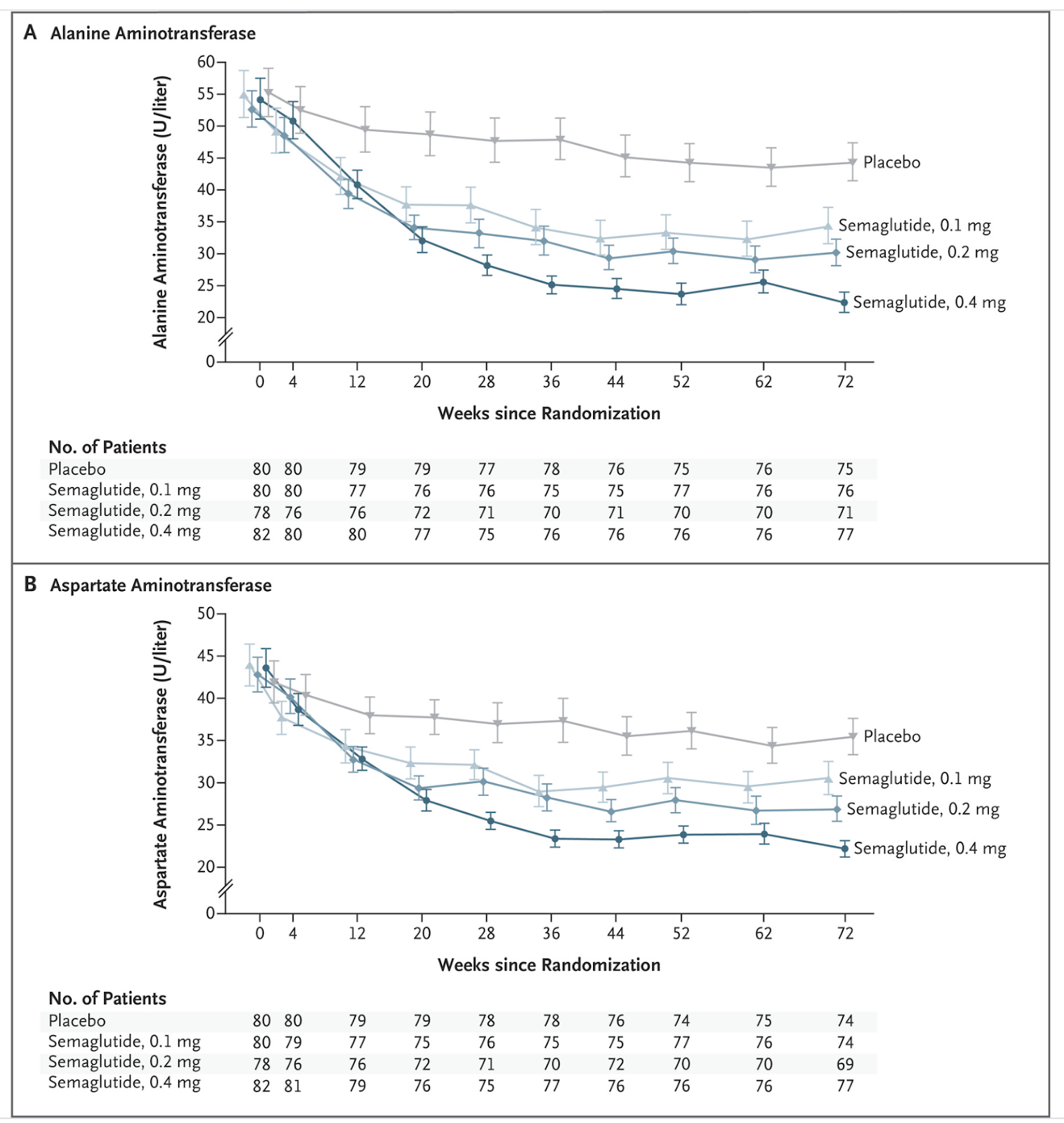
A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis, 2021
Nonalcoholic steatohepatitis (NASH) is a common disease that is associated with increased morbidity and mortality, but treatment options are limited. The efficacy and safety of the glucagon-like peptide-1 receptor agonist semaglutide in patients with NASH is not known.
METHODS
We conducted a 72-week, double-blind phase 2 trial involving patients with biopsy-confirmed NASH and liver fibrosis of stage F1, F2, or F3. Patients were randomly assigned, in a 3:3:3:1:1:1 ratio, to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg or corresponding placebo. The primary end point was resolution of NASH with no worsening of fibrosis. The confirmatory secondary end point was an improvement of at least one fibrosis stage with no worsening of NASH. The analyses of these end points were performed only in patients with stage F2 or F3 fibrosis; other analyses were performed in all the patients.
RESULTS
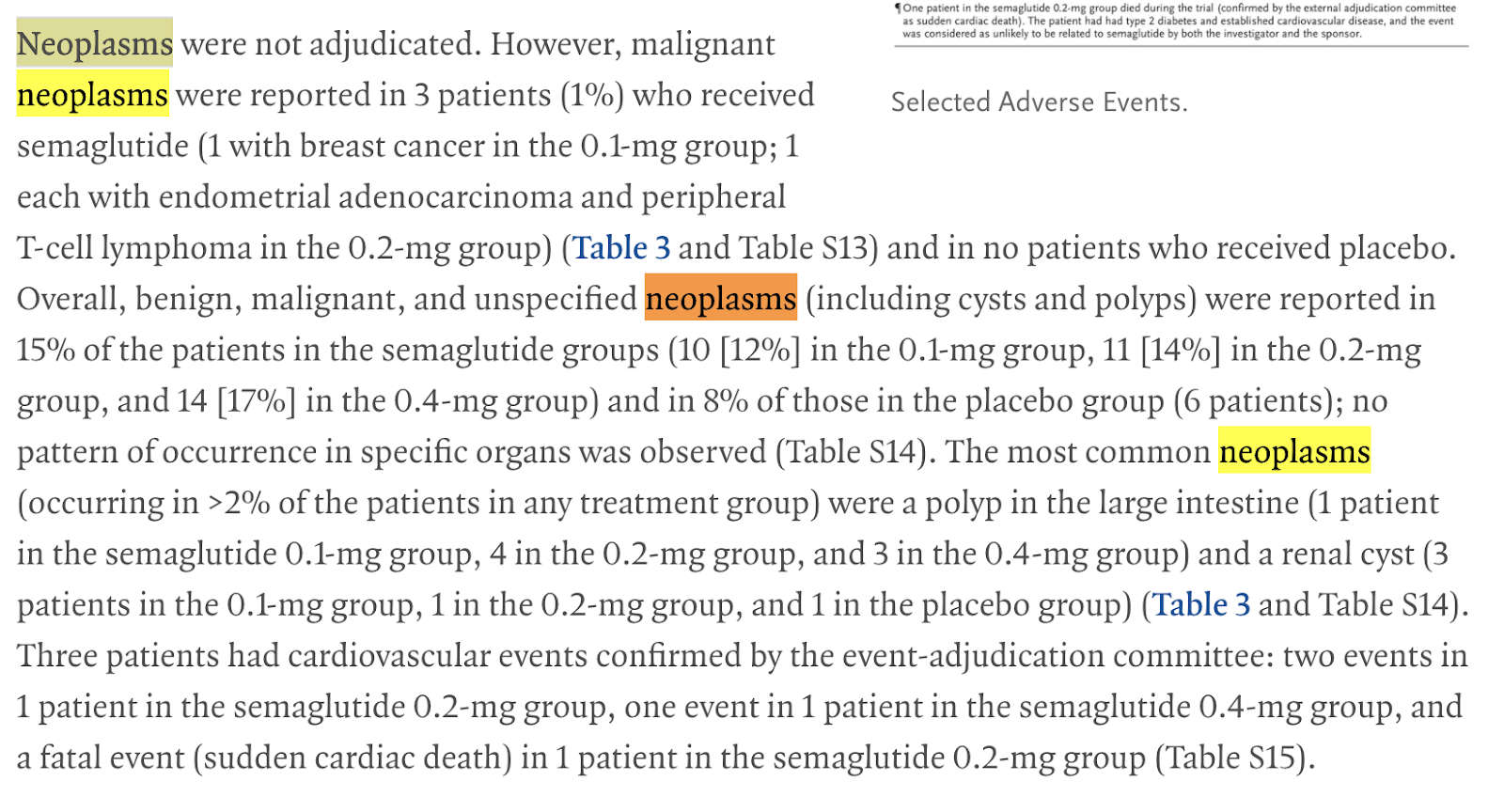
In total, 320 patients (of whom 230 had stage F2 or F3 fibrosis) were randomly assigned to receive semaglutide at a dose of 0.1 mg (80 patients), 0.2 mg (78 patients), or 0.4 mg (82 patients) or to receive placebo (80 patients). The percentage of patients in whom NASH resolution was achieved with no worsening of fibrosis was 40% in the 0.1-mg group, 36% in the 0.2-mg group, 59% in the 0.4-mg group, and 17% in the placebo group (P<0.001 for semaglutide 0.4 mg vs. placebo). An improvement in fibrosis stage occurred in 43% of the patients in the 0.4-mg group and in 33% of the patients in the placebo group (P=0.48). The mean percent weight loss was 13% in the 0.4-mg group and 1% in the placebo group. The incidence of nausea, constipation, and vomiting was higher in the 0.4-mg group than in the placebo group (nausea, 42% vs. 11%; constipation, 22% vs. 12%; and vomiting, 15% vs. 2%). Malignant neoplasms were reported in 3 patients who received semaglutide (1%) and in no patients who received placebo. Overall, neoplasms (benign, malignant, or unspecified) were reported in 15% of the patients in the semaglutide groups and in 8% in the placebo group; no pattern of occurrence in specific organs was observed.
CONCLUSIONS
This phase 2 trial involving patients with NASH showed that treatment with semaglutide resulted in a significantly higher percentage of patients with NASH resolution than placebo. However, the trial did not show a significant between-group difference in the percentage of patients with an improvement in fibrosis stage. (Funded by Novo Nordisk; ClinicalTrials.gov number, NCT02970942. opens in new tab.)


Mechanism of action
Semaglutide is a glucagon-like peptide-1 receptor agonist. It increases the production of insulin, a hormone that lowers the blood sugar level.[14] It also appears to enhance growth of β cells in the pancreas, which are the sites of insulin production.[15] On the other hand it inhibits glucagon, which is a hormone that increases blood sugar. It additionally reduces food intake by lowering appetite and slows down digestion in the stomach.[13] In this way it works in body fat reduction.[11]
Structure
In humans semaglutide is chemically similar to human glucagon-like peptide-1 (GLP-1), with 94% similarity. The only differences are two amino acid substitutions at positions 8 and 34, where alanine and lysine are replaced by 2-aminoisobutyric acid and arginine respectively.[16] Amino acid substitution at position 8 prevents chemical breakdown by an enzyme dipeptidyl peptidase-4. In addition, lysine at position 26 is in its derivative form (acylated with stearic diacid). Acylation with a spacer and C-18 fatty diacid chain increases the drug binding to blood protein (albumin), which enables longer presence in the blood circulation.[17] Its half-life in the blood is about 7 days (165–184 hours), therefore, once-weekly injection is enough.[5][15]
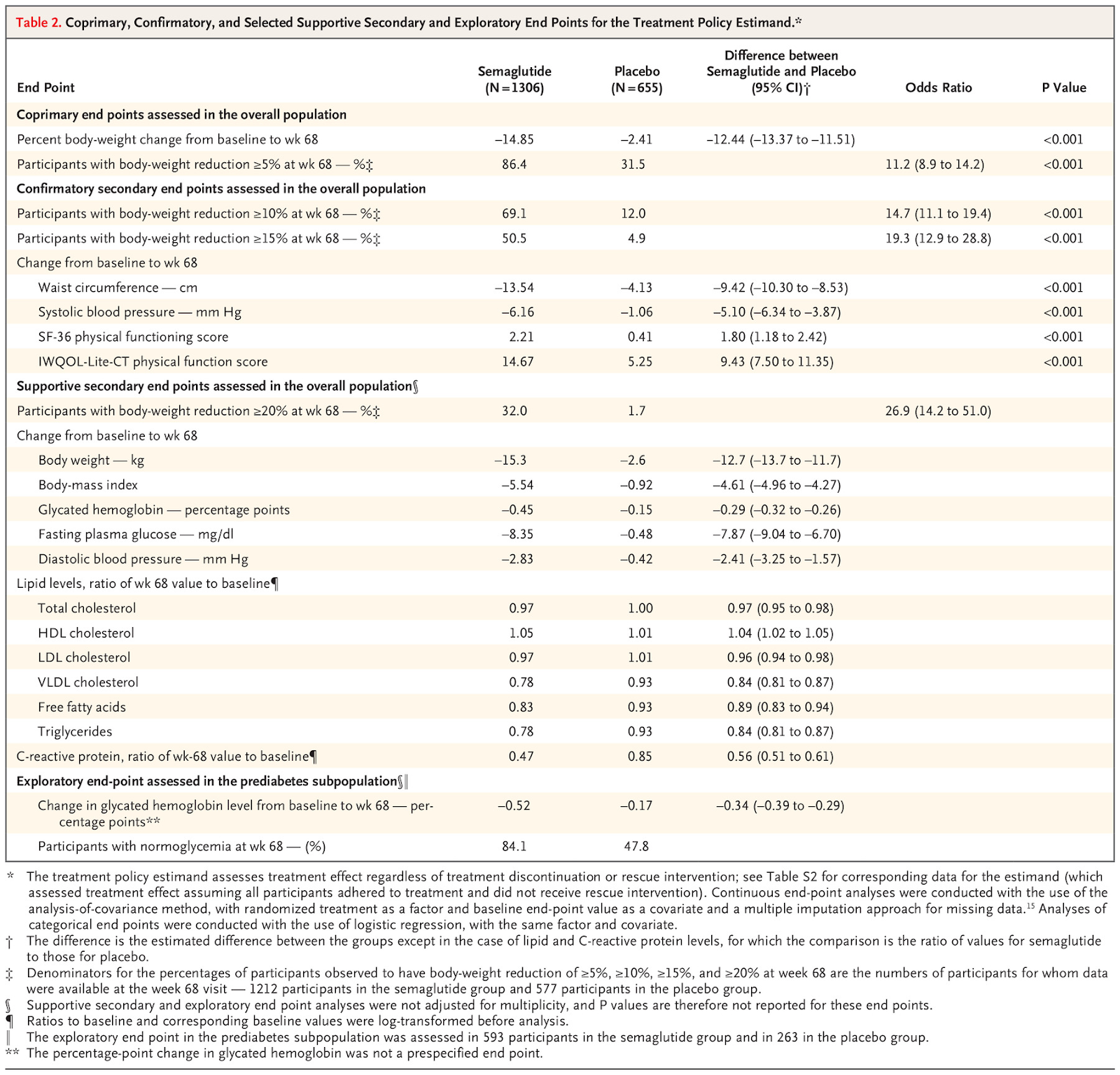
Once-Weekly Semaglutide in Adults with Overweight or Obesity (link)
BACKGROUND
Obesity is a global health challenge with few pharmacologic options. Whether adults with obesity can achieve weight loss with once-weekly semaglutide at a dose of 2.4 mg as an adjunct to lifestyle intervention has not been confirmed.
METHODS
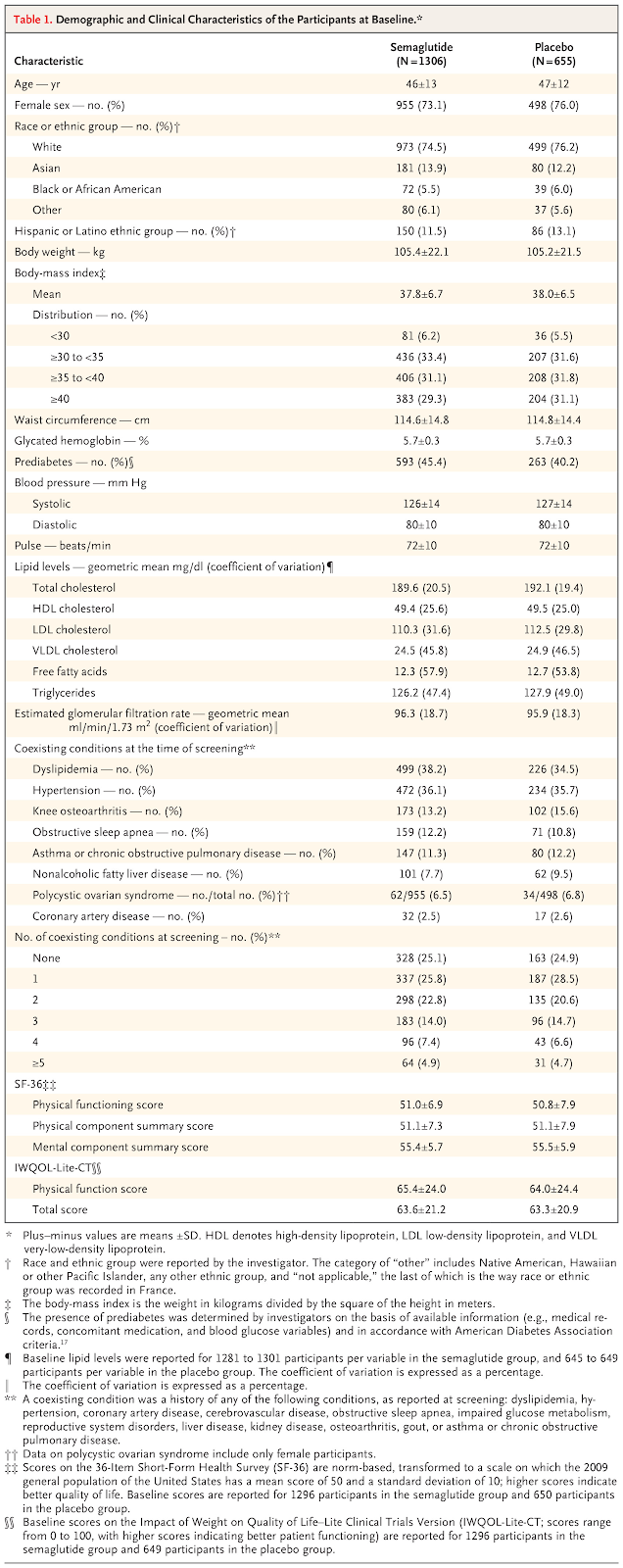
In this double-blind trial, we enrolled 1961 adults with a body-mass index (the weight in kilograms divided by the square of the height in meters) of 30 or greater (≥27 in persons with ≥1 weight-related coexisting condition), who did not have diabetes, and randomly assigned them, in a 2:1 ratio, to 68 weeks of treatment with once-weekly subcutaneous semaglutide (at a dose of 2.4 mg) or placebo, plus lifestyle intervention. The coprimary end points were the percentage change in body weight and weight reduction of at least 5%. The primary estimand (a precise description of the treatment effect reflecting the objective of the clinical trial) assessed effects regardless of treatment discontinuation or rescue interventions.
RESULTS
The mean change in body weight from baseline to week 68 was −14.9% in the semaglutide group as compared with −2.4% with placebo, for an estimated treatment difference of −12.4 percentage points (95% confidence interval [CI], −13.4 to −11.5; P<0.001). More participants in the semaglutide group than in the placebo group achieved weight reductions of 5% or more (1047 participants [86.4%] vs. 182 [31.5%]), 10% or more (838 [69.1%] vs. 69 [12.0%]), and 15% or more (612 [50.5%] vs. 28 [4.9%]) at week 68 (P<0.001 for all three comparisons of odds). The change in body weight from baseline to week 68 was −15.3 kg in the semaglutide group as compared with −2.6 kg in the placebo group (estimated treatment difference, −12.7 kg; 95% CI, −13.7 to −11.7). Participants who received semaglutide had a greater improvement with respect to cardiometabolic risk factors and a greater increase in participant-reported physical functioning from baseline than those who received placebo. Nausea and diarrhea were the most common adverse events with semaglutide; they were typically transient and mild-to-moderate in severity and subsided with time. More participants in the semaglutide group than in the placebo group discontinued treatment owing to gastrointestinal events (59 [4.5%] vs. 5 [0.8%]).
CONCLUSIONS
In participants with overweight or obesity, 2.4 mg of semaglutide once weekly plus lifestyle intervention was associated with sustained, clinically relevant reduction in body weight.
‘A Game Changer’: Drug Brings Weight Loss in Patients With Obesity (NYT)
https://www.nytimes.com/2021/02/10/health/obesity-weight-loss-drug-semaglutide.html
Trial Finds Semaglutide With Lifestyle Intervention Reduces Body Weight by Nearly 15% (link)
Those who received semaglutide also exhibited greater reductions in waist circumference, BMI, and systolic and diastolic blood pressure compared with placebo, and had improved levels of glycated hemoglobin, fasting plasma glucose, C-reactive protein, and fasting lipid levels after 68 weeks. These participants reported greater increases in physical functioning from baseline compared with placebo.
Gastrointestinal disorders, including nausea, diarrhea, vomiting and constipation, were the most frequently reported events and occurred in 74.2% of those who took semaglutide compared with 47.9% of the placebo group. Approximately 10% of those who took semaglutide reported serious adverse events, compared with 6.4% in the placebo group, “with the difference due primarily to a difference between the groups in the incidence of serious gastrointestinal disorders and hepatobiliary disorders,” researchers wrote. In the semaglutide group, 2.6% of participants reported gallbladder-related disorders compared with 1.2% of the placebo group, and those who took semaglutide reported higher rates of cholelithiasis.
Weight reductions achieved with semaglutide were substantially greater at 14.9% compared with weight loss from baseline achieved using approved antiobesity medications, which ranges from 4% to 10.9%, researchers noted.
Previous research has found that 3 mg of daily liraglutide (the only GLP-1 receptor agonist approved for weight management) resulted in a 4.5% reduction in mean placebo-corrected weight after 56 weeks, compared with 12.4% seen with semaglutide after 68 weeks. However, authors cautioned that the 2 studies differed in participant population, limiting between-study comparisons.
Participants who maintained their regimen of liraglutide for 4 months lost an average of 7 kg and 6.3% of body weight compared with baseline (P < .001), and those who maintained the regimen for 6 months lost an average of 8 kg and 7.1% of body weight compared with baseline (P < .001). A majority of those who continued liraglutide for 4 months (63.1%) and 6 months (64.1%) achieved at least a 5% reduction in body weight.(link) (19.17lbs lost for a 270lbs person).
“It is important to note that oral semaglutide has been associated with pancreatitis and, in rodents, with thyroid C-cell tumors, which include medullary thyroid carcinoma,” the authors of an accompanying editorial2 pointed out.
Oral semaglutide for type 2 diabetes: A systematic review and meta-analysis, 2019
We included 11 RCTs with 9890 patients in the systematic review. Compared with placebo, oral semaglutide reduced HbA1c and body weight (WMD –0.89%, 95% CI −1.07 to −0.71 and − 2.99 kg, 95% CI −3.69 to −2.30, respectively). Oral semaglutide was also superior to other active comparators (including liraglutide, empagliflozin and sitaglipitin) in terms of lowering HbA1c (WMD –0.35%, 95% CI −0.43 to −0.26) and reduction of body weight (WMD −1.48 kg, 95% CI −2.28 to −0.67), and had a favourable effect on systolic blood pressure. Compared with placebo, oral semaglutide reduced all-cause mortality (OR 0.58, 95% CI 0.37 to 0.92) and cardiovascular mortality (OR 0.55, 95% CI 0.31 to 0.98), and had a neutral effect on myocardial infarction, stroke, severe hypoglycaemia and diabetic retinopathy. However, treatment with oral semaglutide increased the incidence of nausea, vomiting and diarrhea, while events of acute pancreatitis were rare.
Conclusions
Oral semaglutide can effectively and safely reduce blood glucose, body weight and systolic blood pressure. Nevertheless, it is associated with increased incidence of gastrointestinal adverse events. Further research is needed to clarify its long-term safety and comparative effectiveness against other antidiabetic agents.
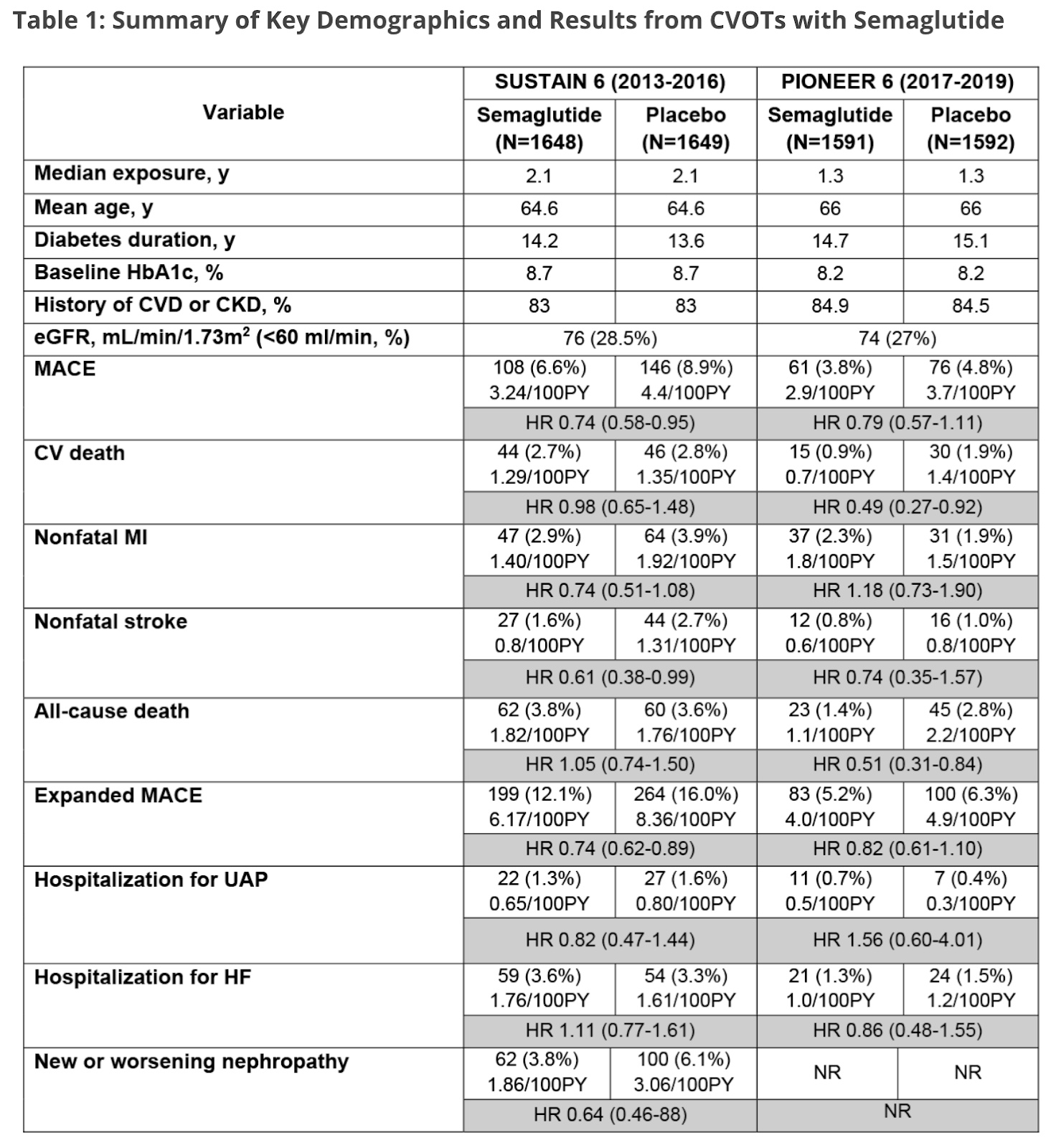
Key CVOTs with Semaglutide: SUSTAIN 6 and PIONEER 6, 2020
Two large phase 3a pre-approval Cardiovascular Outcomes Trials (CVOTs), SUSTAIN 63 and PIONEER 6,4 investigated the effects of subcutaneous and oral semaglutide versus placebo on Major Adverse Cardiovascular Events (MACE) in patients with type 2 diabetes (T2D) and high cardiovascular (CV) risk.
GLP-1 Receptor Agonists and Cardiovascular Prevention: Insights from the LEADER Trial, 2017
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial began in 2010 and involved 9,340 adults with increased cardiovascular risk and type 2 diabetes who were treated with liraglutide or placebo for a median treatment exposure of 3.5 years and median follow-up duration of 3.8 years.
The hazard ratio for the primary cardiovascular outcome was significantly reduced in the liraglutide group compared to placebo, with hazard ratio 0.87 (95% CI 0.78 to 0.97, P = 0.01). The expanded composite cardiovascular outcome (consisting of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke, coronary revascularization, or hospitalization for unstable angina pectoris or heart failure) was also significantly reduced, with a hazard ratio of 0.88 (95% CI 0.81 to 0.96, P = 0.005). The rate of cardiovascular mortality was significantly lower in the liraglutide group, with hazard ratio 0.78 (95% CI 0.66 to 0.93, P=0.007), and total mortality (death from any cause) was also significantly lower in the liraglutide group, with hazard ratio 0.85 (95% CI 0.74 to 0.97, P = 0.02). The individual rates of nonfatal myocardial infarction, nonfatal stroke, and hospitalization for heart failure were nonsignificantly lower in the liraglutide group. The rate of incident nephropathy was significantly reduced by liraglutide compared to placebo (HR 0.78, 95% CI 0.67 to 0.92, P = 0.003), but the incidence of retinopathy was unaffected (HR 1.15, 95% CI 0.87 to 1.53, P = 0.33).
Severe hypoglycemia was less frequent in the liraglutide group (2.4 vs 3.3%, P = 0.02). Side-effects that lead to discontinuation of treatment were significantly more common in the liraglutide group (9.5 vs 7.3%, P < 0.001) and included nausea (1.6 vs. 0.4%), vomiting (0.7 vs. < 0.1%), diarrhea (0.6 vs. 0.1%), abdominal pain (0.2 vs. 0.1%), decreased appetite (0.2 vs. < 0.1%), and abdominal discomfort (0.2 vs. 0%), as anticipated. The incidence of acute gallstone disease was 3.1 versus 1.9% (P < 0.001). Despite the prior suggestion that GLP-1 receptor agonists may increase the risk of pancreatitis, the rates of acute and chronic pancreatitis were not significantly different in the liraglutide treatment group compared to placebo (0.4 vs. 0.5%, P = 0.44 and 0 vs. 0.04%, P = 0.16, respectively). A subsequent analysis of these data confirmed these findings, as well as demonstrating that the incidence of pancreatitis among a subgroup of 267 individuals with a previous history of pancreatitis was not increased during treatment with liraglutide compared to placebo.7 Although the difference did not reach statistical significance, the rate of pancreatic cancer was 0.3% in the liraglutide group compared to 0.1% in the placebo group (P = 0.06). In general, liraglutide was well tolerated with a placebo-controlled excess discontinuation rate of only 2.2%.
Systemic GLP-1R agonist treatment reverses mouse glial and neurovascular cell transcriptomic aging signatures in a genome-wide manner, 2021
Pharmacological reversal of brain aging is a long-sought yet challenging strategy for the prevention and treatment of age-related neurodegeneration, due to the diverse cell types and complex cellular pathways impacted by the aging process. Here, we report the genome-wide reversal of transcriptomic aging signatures in multiple major brain cell types, including glial and mural cells, by systemic glucagon-like peptide-1 receptor (GLP-1R) agonist (GLP-1RA) treatment. The age-related expression changes reversed by GLP-1RA encompass both shared and cell type-specific functional pathways that are implicated in aging and neurodegeneration. Concomitantly, Alzheimer’s disease (AD)-associated transcriptomic signature in microglia that arises from aging is reduced. These results show the feasibility of reversing brain aging by pharmacological means, provide mechanistic insights into the neurological benefits of GLP-1RAs, and imply that GLP-1R agonism may be a generally applicable pharmacological intervention for patients at risk of age-related neurodegeneration.
Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (link)
BACKGROUND
Regulatory guidance specifies the need to establish cardiovascular safety of new diabetes therapies in patients with type 2 diabetes in order to rule out excess cardiovascular risk. The cardiovascular effects of semaglutide, a glucagon-like peptide 1 analogue with an extended half-life of approximately 1 week, in type 2 diabetes are unknown.
METHODS
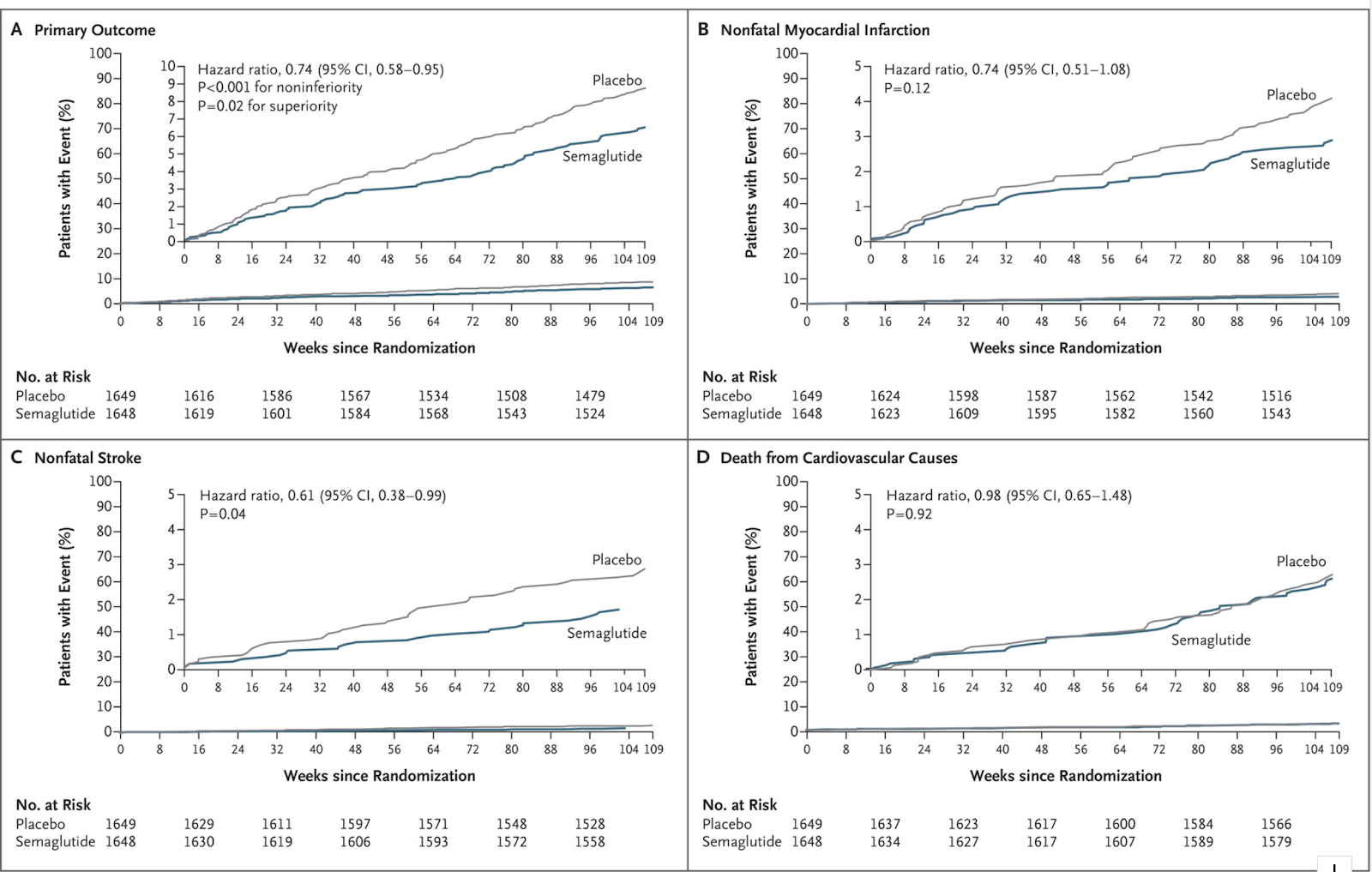
We randomly assigned 3297 patients with type 2 diabetes who were on a standard-care regimen to receive once-weekly semaglutide (0.5 mg or 1.0 mg) or placebo for 104 weeks. The primary composite outcome was the first occurrence of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. We hypothesized that semaglutide would be noninferior to placebo for the primary outcome. The noninferiority margin was 1.8 for the upper boundary of the 95% confidence interval of the hazard ratio.
RESULTS
At baseline, 2735 of the patients (83.0%) had established cardiovascular disease, chronic kidney disease, or both. The primary outcome occurred in 108 of 1648 patients (6.6%) in the semaglutide group and in 146 of 1649 patients (8.9%) in the placebo group (hazard ratio, 0.74; 95% confidence interval [CI], 0.58 to 0.95; P<0.001 for noninferiority). Nonfatal myocardial infarction occurred in 2.9% of the patients receiving semaglutide and in 3.9% of those receiving placebo (hazard ratio, 0.74; 95% CI, 0.51 to 1.08; P=0.12); nonfatal stroke occurred in 1.6% and 2.7%, respectively (hazard ratio, 0.61; 95% CI, 0.38 to 0.99; P=0.04). Rates of death from cardiovascular causes were similar in the two groups. Rates of new or worsening nephropathy were lower in the semaglutide group, but rates of retinopathy complications (vitreous hemorrhage, blindness, or conditions requiring treatment with an intravitreal agent or photocoagulation) were significantly higher (hazard ratio, 1.76; 95% CI, 1.11 to 2.78; P=0.02). Fewer serious adverse events occurred in the semaglutide group, although more patients discontinued treatment because of adverse events, mainly gastrointestinal.
CONCLUSIONS
In patients with type 2 diabetes who were at high cardiovascular risk, the rate of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke was significantly lower among patients receiving semaglutide than among those receiving placebo, an outcome that confirmed the noninferiority of semaglutide. (Funded by Novo Nordisk; SUSTAIN-6 ClinicalTrials.gov number, NCT01720446. opens in new tab.)

Do GLP-1–Based Therapies Increase Cancer Risk? (link)
Cases of pancreatitis have been described in connection with the use of exenatide (1), liraglutide (2) and other glucagon-like peptide (GLP)-1 receptor agonists. From these findings, the following hypothesis has been generated: stimulating the GLP-1 receptor with respective agonists has a potential to cause pancreatitis, perhaps chronic pancreatitis, and in the long term, potentially even pancreatic cancer (3–5). Furthermore, in rodents like mice and rats, stimulating the GLP-1 receptor raises cAMP in thyroid C cells, initiates the release of calcitonin, and upon longer-term exposure, is accompanied by C-cell proliferation and the formation of C-cell adenomas and (medullary thyroid) carcinomas (6). Based on these findings, it was hypothesized that GLP-1–derived medications have a potential to cause medullary thyroid carcinoma in humans as well (3,7). It is the purpose of the current review to discuss the evidence in favor and against the hypothesis that GLP-1–based therapies increase cancer risk, specifically the risk for pancreatic and thyroid carcinomas in patients with type 2 diabetes treated with exenatide and sitagliptin.
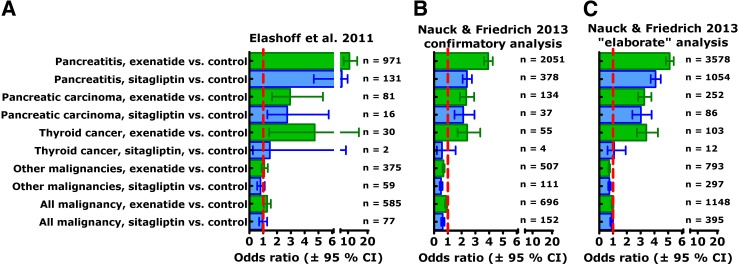
Conclusions
Regarding the controversy of whether GLP-1–based therapy can increase the risk for specific malignant disease like pancreatic carcinoma and thyroid cancer, our conclusion is that apparently there is neither firm evidence in favor of this hypothesis nor evidence strong enough to rule out any such increased risk based on results available at present.
Cardiovascular Benefits of GLP-1-BasedTherapies in Patients with Diabetes Mellitus Type 2: Effects on Endothelial and Vascular Dysfunction beyond Glycemic Control (link)
Type 2 diabetes mellitus (T2DM) is a progressive multisystemic disease accompanied by vascular dysfunction and a tremendous increase in cardiovascular mortality. Numerous adipose-tissue-derived factors and beta cell dysfunction contribute to the increased cardiovascular risk in patients with T2DM. Nowadays, numerous pharmacological interventions are available to lower blood glucose levels in patients with type 2 diabetes. Beside more or less comparable glucose lowering efficacy, some of them have shown limited or probably even unfavorable effects on the cardiovascular system and overall mortality. Recently, incretin-based therapies (GLP-1 receptor agonists and DPP-IV inhibitors) have been introduced in the treatment of T2DM. Beside the effects of GLP-1 on insulin secretion, glucagon secretion, and gastrointestinal motility, recent studies suggested a couple of direct cardiovascular effects of GLP-1-based therapies. The goal of this paper is to provide an overview about the current knowledge of direct GLP-1 effects on endothelial and vascular function and potential consequences on the cardiovascular outcome in patients with T2DM treated with GLP-1 receptor agonists or DPP-IV inhibitors.
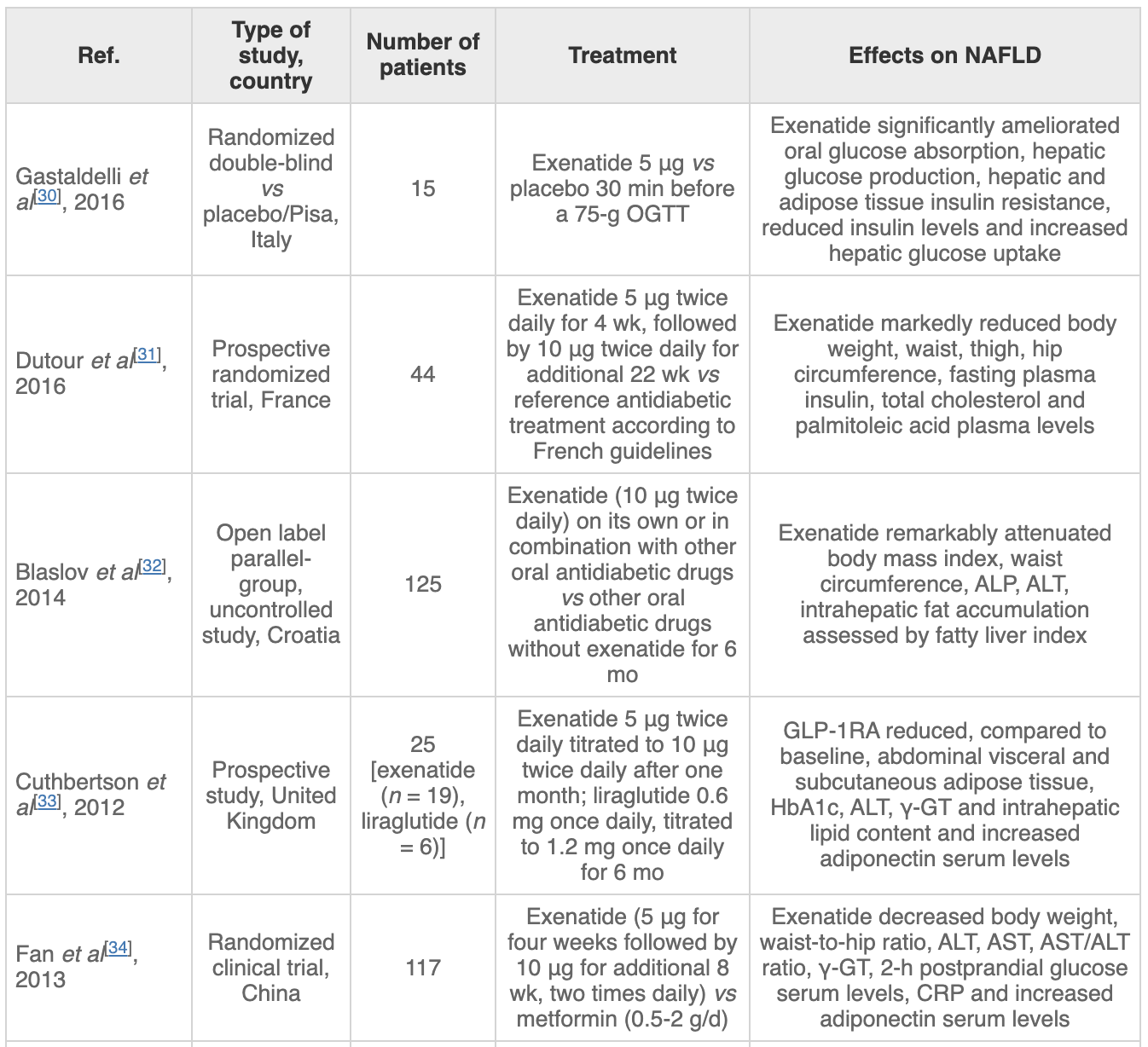
GLP-1 receptor agonists for NAFLD treatment in patients with and without type 2 diabetes: an updated meta-analysis (2020)
Aim: Recent randomized controlled trials (RCTs) have tested the efficacy of glucagon-like peptide-1 receptor agonists (GLP-1 RA) to specifically treat non-alcoholic fatty liver disease (NAFLD). We performed a meta-analysis of RCTs to investigate the efficacy of GLP-1 RAs for treatment of NAFLD or non-alcoholic steatohepatitis (NASH).
Methods: We systematically searched PubMed and ClinicalTrials.Gov databases utilizing specific terms to identify placebo-controlled or head-to-head RCTs (last research on March 1, 2020) involving NAFLD patients with the aim of evaluating the efficacy of GLP-1 RAs to treat NAFLD/NASH. Primary outcomes were changes in serum liver enzymes, liver fat content, or histologic resolution of NASH. Weighted mean differences (WMD) were used to test the differences between the treatment arms.
Results: Overall, we found 7 placebo-controlled or head-to-head RCTs involving 472 middle-aged individuals (66% men; 77% with established diabetes) followed for a median of 16 weeks that have used liraglutide or exenatide to treat NAFLD on imaging (n = 6) or biopsy (n = 1). Compared to placebo or reference therapy, treatment with GLP-1 RAs decreased serum alanine aminotransferase [n = 7 studies; WMD: –8.77 IU/L, 95% confidence intervals (CI) –17.69 to 0.14 IU/L; I2 = 87.3%], gamma-glutamyltransferase levels (n = 4 studies; WMD: –10.17 IU/L, 95% CI –14.27 IU/L to –6.07 IU/L; I2 = 0%) and imaging-defined liver fat content (n = 4 studies; WMD: –6.23%, 95% CI –8.95% to –3.51%; I2 = 85.9%). In one RCT involving 55 patients with biopsy-proven NASH, a 48-week treatment with liraglutide also led to a greater histological resolution of NASH than placebo.
Conclusions: GLP-1 RAs (mostly liraglutide) seem to be a promising treatment option for NAFLD or NASH.
Liraglutide Produces Clinically Significant Weight Loss in Nondiabetic Patients (link)
Objective. To evaluate the efficacy of liraglutide for weight loss in a group of nondiabetic patients with obesity.
Design. Randomized double-blind placebo-controlled trial.
Setting and participants . This trial took place across 27 countries in Europe, North America, South America, Asia, Africa and Australia. It was funded by NovoNordisk, the pharmaceutical company that manufactures liraglutide. Participants were 18 years or older, with a BMI of 30 kg/m 2 (or 27 kg/m 2 with hypertension or dyslipidemia). Patients with diabetes, those on medications known to induce weight gain (or loss), those with history of bariatric surgery, and those with psychiatric illness were excluded from participating. Patients with prediabetes were not excluded.
Intervention. Participants were randomized (2:1 in favor of study drug) to liraglutide or placebo, stratified according to BMI category and pre-diabetes status. They were started at a 0.6–mg dose of medication and up-titrated as tolerated to a dose of 3.0 mg over several weeks. All received counseling on behavioral changes to promote weight loss. Participants were then followed for 56 weeks. A small subgroup in the liraglutide arm was randomly assigned to switch to placebo after 12 weeks on medication to examine for durability of effect of medication, and to evaluate for safety issues that might occur on drug discontinuation.
Main outcome measures . This study focused on 3 primary outcomes: individual-level weight change from baseline, group-level percentage of participants achieving at least 5% weight loss, and percentage of participants with at least 10% weight loss, all assessed at 56 weeks.
Secondary outcomes included change in BMI, waist circumference, markers of glycemia (hemoglobin A1c, insulin level), markers of cardiometabolic health (blood pressure, lipids, CRP), and health-related quality of life (using several validated survey measures). Adverse events were also assessed.
The investigators used an intention-to-treat analysis, comparing outcomes among all patients who were randomized and received at least 1 dose of liraglutide or placebo. For patients with missing values (eg, due to dropout), outcome values were imputed using the last-observation-carried-forward method. A multivariable analysis of covariance model was used to analyze changes in the primary outcomes and included a covariate for the baseline measure of the outcome in question. Sensitivity analyses were conducted in which the investigators used different imputation techniques (multiple imputation, repeated measures) to account for missing data.
Results. The trial enrolled 3731 participants, 2487 of whom were randomized to receive liraglutide and 1244 of whom received placebo. The groups were similar on measured baseline characteristics, with a mean age of 45 years, mostly female participants (78.7% in liraglutide arm, 78.1% in placebo), and the vast majority of participants identified as “white” race/ethnicity (84.7% in liraglutide, 85.3% in placebo). Mean baseline BMI was 38.3 kg/m 2 in both groups. Although overweight patients with BMI 27 kg/m 2 or greater were included, they represented a small fraction of all participants (2.7% in liraglutide group and 3.5% in placebo group). Furthermore, although patients with overt diabetes were excluded from participating, over half of the participants qualified as having prediabetes (61.4% in liraglutide group, 60.9% in placebo group). Just over one-third (34.2% of liraglutide group, 35.9% placebo) had hypertension diagnosed at baseline. Study withdrawal was relatively substantial in both groups – 71.9% remained enrolled at 56 weeks in the liraglutide group, and 64.4% remained in the placebo arm. The investigators note that withdrawal due to adverse events was more common in the liraglutide group (9.9% of withdrawals vs. 3.8% in placebo), while other reasons for withdrawing (ineffective therapy, withdrawal of consent) were more common among placebo participants.
Liraglutide participants lost significantly more weight than placebo participants at 56 weeks (mean [SD] 8.0 [6.7] kg vs. 2.6 [5.7] kg). Similarly, more patients in the liraglutide group achieved at least 5% weight loss (63% vs. 27%), and 10% weight loss (33.1% vs. 10.6%) than those taking placebo [GM: Average weight loss ~ .1/3+0.05*⅔ = 6.6%?] When subgroups of patients were examined according to baseline BMI, the investigators suggested that liraglutide appeared to be more effective at promoting weight loss among patients starting below 40 kg/m 2.
Hemoglobin A1c dropped significantly more (–0.23 points, P < 0.001) among liraglutide participants than among placebo participants. Similarly, fasting insulin levels dropped by 8% more ( P < 0.001) in the liraglutide group at 56 weeks. In keeping with the greater weight loss, markers of cardiometabolic health also improved to a greater extent among liraglutide participants, with larger decreases in blood pressure (SBP –2.8 mm Hg lower in liraglutide, P < 0.001), and LDL (–2.4% difference, P = 0.002), and a larger increase in HDL (1.9% difference, P = 0.001). By week 56, 14% of prediabetic patients in the placebo arm had received a new diagnosis of diabetes, compared to just 4% in the liraglutide group ( P < 0.001).
Quality of life scores were higher for liraglutide participants on all included measures except those related to side effects of treatment, where placebo participants reported lower levels of side effects. The most common side effects reported by liraglutide participants related to GI upset, including nausea (40%), diarrhea (21%), and vomiting (16%). More serious events, including cholelithiasis (0.8%), cholecystitis (0.5%), and pancreatitis (0.2%), were also reported. Somewhat surprisingly, although liraglutide is also used to improve glycemic control in diabetics, rates of reported spontaneous hypoglycemia were fairly low in the liraglutide group (1.3% vs. 1.0% in placebo).
Conclusion. Liraglutide given at a dose of 3.0 mg daily, along with lifestyle advice, produces clinically significant weight loss and improvement in glycemic and cardiometabolic parameters that is sustained after 1 full year of treatment.
Weight Loss with Saxenda, Victoza, Liraglutide (same drug)
Ford Brewer MD MPH
https://www.youtube.com/watch?v=IQPW5xmi5is
Liver-derived fibroblast growth factor 21 mediates effects of glucagon-like peptide-1 in attenuating hepatic glucose output
Findings
Utilizing the cytokine array, we identified that FGF21 secretion was upregulated by exenatide (exendin-4). Similarly, FGF21 production in hepatocytes was stimulated by exenatide or liraglutide. FGF21 blockage attenuated the inhibitory effects of the GLP-1 analogs on hepatic glucose output. Similar results were also observed in primary hepatocytes from Fgf21 knockout mice. Furthermore, exenatide treatment increased serum FGF21 level in patients with T2D, particularly in those with better glucose control.
Interpretation
We identify that function of GLP-1 in inhibiting hepatic glucose output is mediated via the liver hormone FGF21. Thus, we provide a new extra-pancreatic mechanism by which GLP-1 regulates glucose homeostasis.
Effects of Glucagon Like Peptide-1 Receptor Agonists on Tumor Diseases (link)
GLP-1RAs could limit the growth of prostate cancer by inhibiting the PI3K/AKT/mTOR and ERK/MAPK pathways, while could also limit the growth of pancreatic and prostate cancer cells by inhibiting the NF-kB pathway (210–212). Similarly, GLP-1RAs were also demonstrated to exert an inhibitory effect on the growth of breast and cervical cancer, implying the potential application of GLP-1RAs for the treatment of these cancer (10). Zhang et al. reported for the first time that liraglutide exhibited significant anti-proliferation and pro-apoptotic effects on gemcitabine-resistant human pancreatic cancer cells resistant to a variety of drugs, by regulating the NF-κB signaling pathway and downstream ATP-binding cassette subfamily G member 2 (ABCG2) (213, 214).
Likewise, Wenjing et al. found that exendin-4 could reduce the resistance of prostate cancer cells to enzalutamide by targeting the PI3K/AKT/mTOR pathway, while combined use of exendin-4 and enzalutamide could significantly inhibit the growth of prostate cancer cells (210). Therefore, a combination of GLP-1RAs with anticancer drugs could indirectly inhibit the migration, invasion, and growth of tumors by increasing the chemosensitivity of cancer cells. Interestingly, this approach seems to be more effective for the treatment of patients with advanced cancer (210, 215).
Liraglutide and exenatide were reported to induce apoptosis and autophagy through the AMPK signaling pathway, inhibiting the progression of endometrial cancer (216, 217). In addition, exenatide was shown to activate GLP-1R and inhibit the PI3K/AKT pathway to inhibit the growth, migration, and invasion of ovarian cancer cells, and promote cell apoptosis, thereby producing anticancer effects on diabetic patients with ovarian cancer (218). Besides, exenatide-4 has been found to inhibit the survival, migration, proliferation, and invasion of glioma cells in a GLP-1R/SIRT3 pathway dependent manner (219). The continuous in-depth research on the effects of GLP-1RAs on the occurrence and development of cancer in recent years have highlighted the increased potential for their use in the clinical treatment of cancer.
To date, no clear clinical evidence has been found to suggest the tumorigenic effect of GLP-1RAs (226), whereas plenty of studies have indicated that GLP-1RAs can inhibit the growth of ovarian, breast, prostate, and pancreatic cancer (227, 228). However, our understanding of the function of GLP-1RAs is not complete, and further research, including long-term and large clinical trials are warranted to properly evaluate the causal relationship between GLP-1RAs and the development and progression of various cancers.
Risk of Malignant Neoplasia with Glucagon-Like Peptide-1 Receptor Agonist Treatment in Patients with Type 2 Diabetes: A Meta-Analysis, 2019
Thirty-four relevant articles, providing data for 50452 patients, were included in the meta-analysis. Compared with the incidence of malignant neoplasia with placebo or other interventions, no increase in malignant neoplasm formation was observed with the use of GLP-1 receptor agonists (OR 1.04, 95% confidence interval (CI) 0.94–1.15; p = 0.46), liraglutide (OR 1.08, 95% CI 0.91–1.27; p = 0.38), exenatide (OR 1.00, 95% CI 0.86–1.16; p = 1.00), semaglutide (OR 0.89, 95% CI 0.35–2.22; p = 0.80), or albiglutide (OR 1.07, 95% CI 0.23–4.88; p = 0.93). A subanalysis of trials lasting longer than 3 years also showed no increase in the neoplasia risk with GLP-1 receptor agonist use (OR 1.03, 95% CI 0.92–1.15; p = 0.60). Between-trial statistical heterogeneity was low for all comparisons.
GLP-1 receptor agonist as treatment for cancer as well as diabetes: beyond blood glucose control, 2016
Activation of glucagon-like peptide-1 receptor inhibits tumourigenicity and metastasis of human pancreatic cancer cells via PI3K/Akt pathway, 2014
Exendin-4, a Glucagonlike Peptide-1 Receptor Agonist, Attenuates Breast Cancer Growth by Inhibiting NF-κB Activation, 2017
Exendin-4, a GLP-1 Receptor Agonist, Attenuates Prostate Cancer Growth, 2014
Exendin-4 inhibits growth and augments apoptosis of ovarian cancer cells, 2016
Synergistic anti-tumor effects of liraglutide with metformin on pancreatic cancer cells, 2018
A Novel Use of Liraglutide: Induction of Partial Remission in Ulcerative Colitis and Ankylosing Spondylitis, 2019
Nonalcoholic Steatohepatitis (NASH) (link)
Nonalcoholic steatohepatitis is associated with an inflammation of the liver by an aberrant accumulation of fat in the liver. GLP-1 receptor agonists reduced alanine aminotransferase and aspartate aminotransferase levels in patients with nonalcoholic fatty liver disease (or type 2 diabetes) and improved lipid metabolism and reduced fat mass [21]. Liraglutide (50, 100, and 200 μg/kg/12 h) treatment protected against nonalcoholic fatty liver disease by inhibition of ER stress-associated apoptosis in HFD-fed rats [28]. Liraglutide or exendin-4 (1 nmol/kg/day) treatment dose-dependently reduced steatosis and lobular inflammation in HFD-fed rats or mice compared with the saline-injected group [28, 95], probably due to an increase of SIRT1 [96]. As a matter of fact, exendin-4 (50 μg/kg/day) treatment increased the expression of SIRT1 and its downstream factor, AMPK, in exendin-4 treated mouse livers and hepatocytes. Exendin-4 treatment reduced hepatic expression of the inflammatory markers TNF-α, IL-1β, and IL-6 and macrophage markers, cluster of differentiation 68 (CD68), and F4/80 in the liver of mice fed a western-type diet [63].
In nonalcoholic steatohepatitis patients with glucose intolerance, liraglutide (0.9 mg/person/day) therapy for 96 weeks resulted in improvement of histological indicators of inflammation in seven subjects out of ten subjects [97]. CRP is produced by the liver and is a marker of inflammation. In a retrospective analysis of 110 obese patients with type 2 diabetes treated with liraglutide, the mean concentration of CRP declined after treatment with liraglutide for a mean duration of 7.5 months [9]. In addition, exenatide plus metformin resulted in a significant reduction in CRP and TNF-α compared with baseline [98]. These reports suggest that GLP-1-based therapies improve fatty liver disease by ameliorating inflammation in rodents and humans.
Efficacy and safety of semaglutide in glycemic control, body weight management, lipid profiles and other biomarkers among obese type 2 diabetes patients initiated or switched to semaglutide from other GLP-1 receptor agonists, 2021
A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis, 2021
Risk of Malignant Neoplasia with Glucagon-Like Peptide-1 Receptor Agonist Treatment in Patients with Type 2 Diabetes: A Meta-Analysis, 2019
Background. Glucagon-like peptide-1 (GLP-1) receptor agonists are effective glucose-lowering drugs, but there is concern that they may increase the risk of malignant neoplasia. The present meta-analysis examined the safety of GLP-1 receptor agonists with regard to malignant neoplasia. Methods. We analyzed data from randomized controlled trials with a minimum duration of 24 weeks that assessed the incidence of neoplasms in type 2 diabetes patients receiving GLP-1 receptor agonists compared with placebo or other hypoglycemic drugs. We searched the MEDLINE, Embase, and Cochrane databases with a language restriction of English through October 1, 2018, and carried out a meta-analysis of the available trial data using a fixed effects model to calculate odds ratios (ORs) for neoplasia. Results. Thirty-four relevant articles, providing data for 50452 patients, were included in the meta-analysis. Compared with the incidence of malignant neoplasia with placebo or other interventions, no increase in malignant neoplasm formation was observed with the use of GLP-1 receptor agonists (OR 1.04, 95% confidence interval (CI) 0.94–1.15; ), liraglutide (OR 1.08, 95% CI 0.91–1.27; ), exenatide (OR 1.00, 95% CI 0.86–1.16; ), semaglutide (OR 0.89, 95% CI 0.35–2.22; ), or albiglutide (OR 1.07, 95% CI 0.23–4.88; ). A subanalysis of trials lasting longer than 3 years also showed no increase in the neoplasia risk with GLP-1 receptor agonist use (OR 1.03, 95% CI 0.92–1.15; ). Between-trial statistical heterogeneity was low for all comparisons. Conclusion. GLP-1 receptor agonists can be used without safety concerns related to malignant neoplasia in patients with type 2 diabetes.
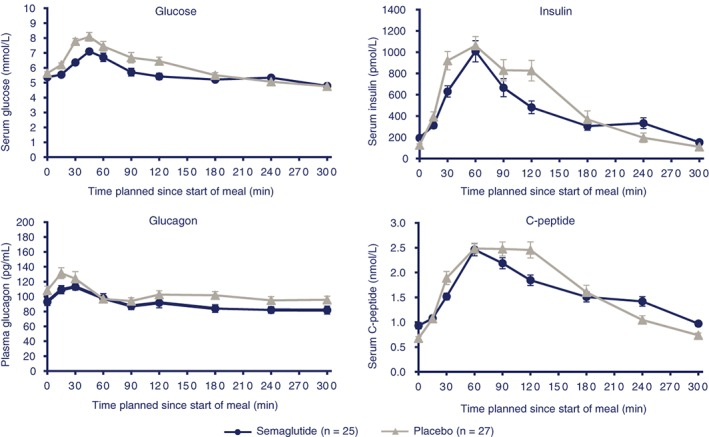
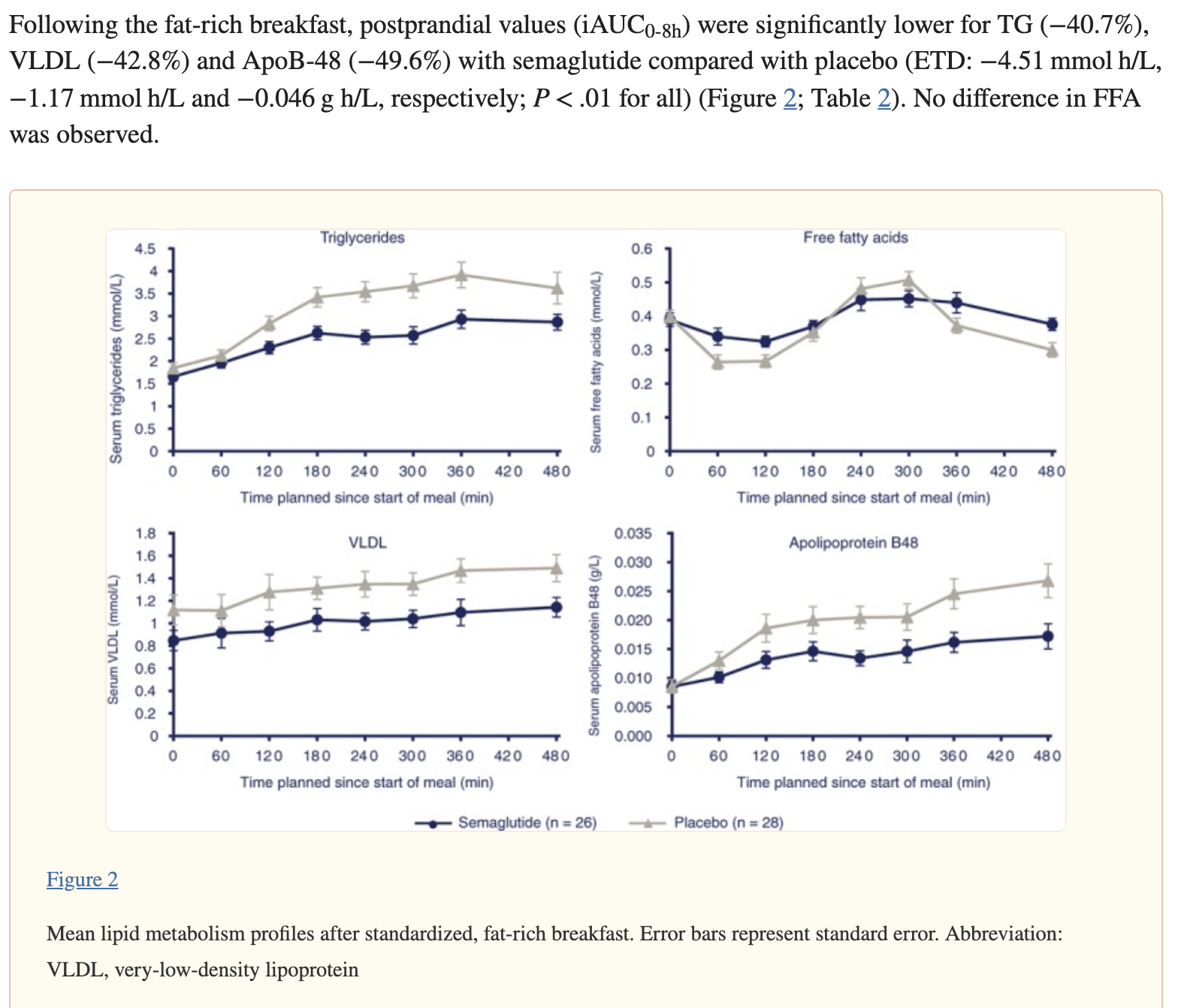
Semaglutide improves postprandial glucose and lipid metabolism, and delays first-hour gastric emptying in subjects with obesity, 2017
Aim: To investigate the effects of semaglutide on fasting and postprandial glucose and lipid responses, and on gastric emptying.
Materials and methods: This was a randomized, double-blind, placebo-controlled, 2-period, crossover trial. Subjects with obesity (N = 30) received once-weekly subcutaneous semaglutide, dose-escalated to 1.0 mg, or placebo. After each 12-week treatment period, glucose and lipid metabolism were assessed before and after standardized meals. Gastric emptying (paracetamol absorption test) and peptide YY (PYY) response were also assessed.
Results: Semaglutide treatment significantly lowered fasting concentrations of glucose and glucagon, and increased insulin vs placebo (estimated treatment ratio: 0.95 [95% confidence interval: 0.91, 0.98]; 0.86 [0.75, 0.98]; 1.45 [1.20, 1.75], respectively). Postprandial glucose metabolism significantly improved with semaglutide vs placebo (incremental area under the curve 0 to 5 hours [iAUC0-5h ]; estimated treatment difference: glucose -1.34 mmol h/L [-2.42, -0.27]; insulin -921 pmol h/L [-1461, -381]; C-peptide -1.42 nmol h/L [-2.33, -0.51]). Fasting and postprandial lipid metabolism improved with semaglutide vs placebo. First-hour gastric emptying after the meal was delayed with semaglutide vs placebo (AUC0-1h ; estimated treatment ratio: 0.73 [0.61, 0.87]); this may have contributed to the lower postprandial glucose increase in semaglutide-treated subjects. Overall gastric emptying (AUC0-5h ) was not statistically different between treatments. Fasting and postprandial PYY responses were significantly lower with semaglutide vs placebo (P = .0397 and P = .0097, respectively).
Conclusion: Semaglutide improved fasting and postprandial glucose and lipid metabolism. Overall gastric emptying was similar to that with placebo; however, the observed first-hour delay with semaglutide may contribute to a slower entry of glucose into the circulation.
—-----------------------
Incretin based treatments and mortality in patients with type 2 diabetes: systematic review and meta-analysis (link)
Objective To assess the impact of incretin based treatment on all cause mortality in patients with type 2 diabetes.
Design Systematic review and meta-analysis of randomised trials.
Data sources Medline, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov.
Eligibility criteria Randomised controlled trials that compared glucagon-like peptide-1 (GLP-1) receptor agonists or dipeptidyl peptidase-4 (DPP-4) inhibitors with placebo or active anti-diabetic drugs in patients with type 2 diabetes.
Data collection and analysis Paired reviewers independently screened citations, assessed risk of bias of included studies, and extracted data. Peto’s method was used as the primary approach to pool effect estimates from trials, sensitivity analyses were carried out with other statistical approaches, and meta-regression was applied for six prespecified hypotheses to explore heterogeneity. The GRADE approach was used to rate the quality of evidence.
Results 189 randomised controlled trials (n=155 145) were included, all of which were at low to moderate risk of bias; 77 reported no events of death and 112 reported 3888 deaths among 151 614 patients. Meta-analysis of 189 trials showed no difference in all cause mortality between incretin drugs versus control (1925/84 136 v 1963/67 478; odds ratio 0.96, 95% confidence interval 0.90 to 1.02, I2=0%; risk difference 3 fewer events (95% confidence interval 7 fewer to 1 more) per 1000 patients over five years; moderate quality evidence). Results suggested the possibility of a mortality benefit with GLP-1 agonists but not DPP-4 inhibitors, but the subgroup hypothesis had low credibility. Sensitivity analyses showed no important differences in the estimates of effects.
Conclusions Current evidence does not support the suggestion that incretin based treatment increases all cause mortality in patients with type 2 diabetes. Further studies are warranted to examine if the effect differs between GLP-1 agonists versus DPP-4 inhibitors.
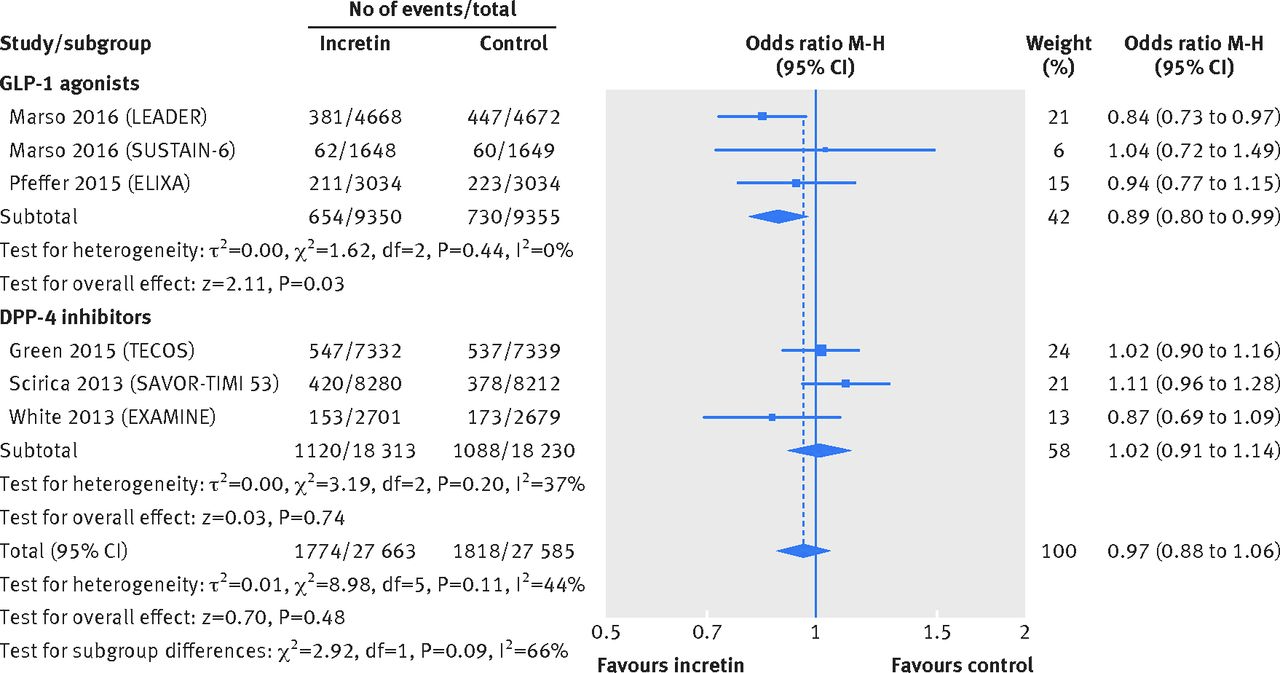
All cause mortality in patients with type 2 diabetes receiving incretin based treatment versus placebo in large cardiovascular outcomes trials:
Composite cardiovascular events (death from cardiovascular causes, non-fatal myocardial infarction, or non-fatal stroke) in patients with type 2 diabetes receiving incretin based treatment versus placebo in large cardiovascular outcomes trials:
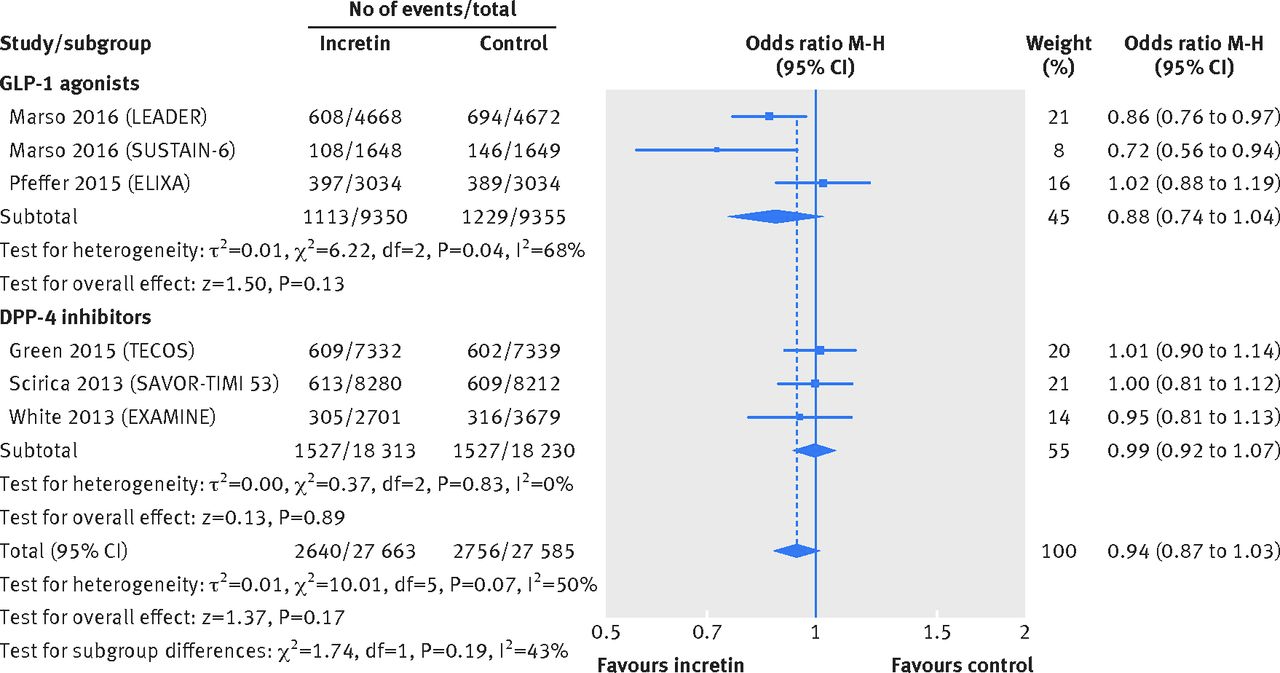
Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials (Lancet, 2019)
Background
Glucagon-like peptide-1 (GLP-1) receptor agonists differ in their structure and duration of action and have been studied in trials of varying sizes and with different patient populations, with inconsistent effects on cardiovascular outcomes reported. We aimed to synthesise the available evidence by doing a systematic review and meta-analysis of cardiovascular outcome trials of these drugs.
Methods
We searched MEDLINE (via PubMed) and the Cochrane Central Register of Controlled Trials for eligible placebo-controlled trials reporting major adverse cardiovascular events (MACE; ie, cardiovascular death, stroke, or myocardial infarction) up to June 15, 2019. We did a meta-analysis using a random-effects model to estimate overall hazard ratios (HRs) for MACE, its components, death from any cause, hospital admission for heart failure, kidney outcomes, and key safety outcomes (severe hypoglycaemia, pancreatitis, and pancreatic cancer). We also examined MACE in several subgroups based on patient characteristics (history of cardiovascular disease, BMI, age, baseline HbA1c, and baseline estimated glomerular filtration rate), trial duration, treatment dosing interval, and structural homology.
Findings
Of 27 publications screened, seven trials, with a combined total of 56 004 participants, were included: ELIXA (lixisenatide), LEADER (liraglutide), SUSTAIN-6 (semaglutide), EXSCEL (exenatide), Harmony Outcomes (albiglutide), REWIND (dulaglutide), and PIONEER 6 (oral semaglutide). Overall, GLP-1 receptor agonist treatment reduced MACE by 12% (HR 0·88, 95% CI 0·82–0·94; p<0·001). There was no statistically significant heterogeneity across the subgroups examined. HRs were 0·88 (95% CI 0·81–0·96; p=0·003) for death from cardiovascular causes, 0·84 (0·76–0·93; p<0·001) for fatal or non-fatal stroke, and 0·91 (0·84–1·00; p=0·043) for fatal or non-fatal myocardial infarction. GLP-1 receptor agonist treatment reduced all-cause mortality by 12% (0·88, 0·83–0·95; p=0·001), hospital admission for heart failure by 9% (0·91, 0·83–0·99; p=0·028), and a broad composite kidney outcome (development of new-onset macroalbuminuria, decline in estimated glomerular filtration rate [or increase in creatinine], progression to end-stage kidney disease, or death attributable to kidney causes) by 17% (0·83, 0·78–0·89; p<0·001), mainly due to a reduction in urinary albumin excretion. There was no increase in risk of severe hypoglycaemia, pancreatitis, or pancreatic cancer.
Interpretation
Treatment with GLP-1 receptor agonists has beneficial effects on cardiovascular, mortality, and kidney outcomes in patients with type 2 diabetes.

Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity (2017)
Aim: The aim of this trial was to investigate the mechanism of action for body weight loss with semaglutide.
Materials and methods: This randomised, double-blind, placebo-controlled, two-period crossover trial investigated the effects of 12 weeks of treatment with once-weekly subcutaneous semaglutide, dose-escalated to 1.0 mg, in 30 subjects with obesity. Ad libitum energy intake, ratings of appetite, thirst, nausea and well-being, control of eating, food preference, resting metabolic rate, body weight and body composition were assessed.
Results: After a standardised breakfast, semaglutide, compared with placebo, led to a lower ad libitum energy intake during lunch (-1255 kJ; P < .0001) and during the subsequent evening meal ( P = .0401) and snacks ( P = .0034), resulting in a 24% reduction in total energy intake across all ad libitum meals throughout the day (-3036 kJ; P < .0001). Fasting overall appetite suppression scores were improved with semaglutide vs placebo, while nausea ratings were similar. Semaglutide was associated with less hunger and food cravings, better control of eating and a lower preference for high-fat foods. Resting metabolic rate, adjusted for lean body mass, did not differ between treatments. Semaglutide led to a reduction from baseline in mean body weight of 5.0 kg, predominantly from body fat mass.
Conclusion: After 12 weeks of treatment, ad libitum energy intake was substantially lower with semaglutide vs placebo with a corresponding loss of body weight observed with semaglutide. In addition to reduced energy intake, likely mechanisms for semaglutide-induced weight loss included less appetite and food cravings, better control of eating and lower relative preference for fatty, energy-dense foods.

2.1 | Trial design
This was a single-centre, randomised, double-blind, placebo-controlled, two-period crossover trial (NCT02079870, EudraCT number: 2013-000012-24)
2.2 | Trial population
Eligible subjects were ≥18 years of age, with a body mass index (BMI) of 30 to 45 kg/m2
, HbA1c < 6.5% and stable body weight (< 3 kg change during the 3 months prior to screening). Key exclusion criteria were: diagnosis of type 1 or 2 diabetes; history of chronic/idiopathic acute pancreatitis; personal/family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2; previous surgical treatment for obesity; smoking or use of any nicotine products; use of any medication that could interfere with trial results.
Mean age, body weight and BMI were 42 years, 101.3 kg and 33.8 kg/m2, respectively. Two-thirds of subjects were male.
2.3 | Interventions
The trial consisted of two 12-week crossover treatment periods, separated by a wash-out period of 5 to 7 weeks. Eligible subjects were randomised 1:1 to one of two treatment sequences: semaglutide–placebo or placebo–semaglutide. Subjects received either semaglutide (1.34 mg/mL) or matching placebo administered subcutaneously (s.c.) once-weekly. The starting dose was 0.25 mg (4 weeks), escalating to 0.5 mg (4 weeks) and then 1.0 mg (4 weeks). Subjects received a fifth dose (administered at the clinic) of 1.0 mg at the last visit of each treatment period and assessments were conducted. Subjects attended the clinic for each dose escalation and were reminded, by text message or telephone, to administer the remaining doses at home.
Glucagon-Like Peptide-1 (GLP-1) Reduces Mortality and Improves Lung Function in a Model of Experimental Obstructive Lung Disease in Female Mice
The incretin hormone glucagon-like peptide-1 (GLP-1) is an important insulin secretagogue and GLP-1 analogs are used for the treatment of type 2 diabetes. GLP-1 displays antiinflammatory and surfactant-releasing effects. Thus, we hypothesize that treatment with GLP-1 analogs will improve pulmonary function in a mouse model of obstructive lung disease. Female mice were sensitized with injected ovalbumin and treated with GLP-1 receptor (GLP-1R) agonists. Exacerbation was induced with inhalations of ovalbumin and lipopolysaccharide. Lung function was evaluated with a measurement of enhanced pause in a whole-body plethysmograph. mRNA levels of GLP-1R, surfactants (SFTPs), and a number of inflammatory markers were measured. GLP-1R was highly expressed in lung tissue. Mice treated with GLP-1R agonists had a noticeably better clinical appearance than the control group. Enhanced pause increased dramatically at day 17 in all control mice, but the increase was significantly less in the groups of GLP-1R agonist-treated mice (P < .001). Survival proportions were significantly increased in GLP-1R agonist-treated mice (P < .01). SFTPB and SFTPA were down-regulated and the expression of inflammatory cytokines were increased in mice with obstructive lung disease, but levels were largely unaffected by GLP-1R agonist treatment. These results show that GLP-1R agonists have potential therapeutic potential in the treatment of obstructive pulmonary diseases, such as chronic obstructive pulmonary disease, by decreasing the severity of acute exacerbations. The mechanism of action does not seem to be the modulation of inflammation and SFTP expression.
Acarbose, lente carbohydrate, and prebiotics promote metabolic health and longevity by stimulating intestinal production of GLP-1
The α-glucosidase inhibitor acarbose, which slows carbohydrate digestion and blunts postprandial rises in plasma glucose, has long been used to treat patients with type 2 diabetes or glucose intolerance. Like metformin, acarbose tends to aid weight control, postpone onset of diabetes and decrease risk for cardiovascular events. Acarbose treatment can favourably affect blood pressure, serum lipids, platelet aggregation, progression of carotid intima-media thickness and postprandial endothelial dysfunction. In mice, lifetime acarbose feeding can increase median and maximal lifespan—an effect associated with increased plasma levels of fibroblast growth factor 21 (FGF21) and decreased levels of insulin-like growth factor-I (IGF-I). There is growing reason to suspect that an upregulation of fasting and postprandial production of glucagon-like peptide-1 (GLP-1)—stemming from increased delivery of carbohydrate to L cells in the distal intestinal tract—is largely responsible for the versatile health protection conferred by acarbose. Indeed, GLP-1 exerts protective effects on vascular endothelium, the liver, the heart, pancreatic β cells, and the brain which can rationalise many of the benefits reported with acarbose. And GLP-1 may act on the liver to modulate its production of FGF21 and IGF-I, thereby promoting longevity. The benefits of acarbose are likely mimicked by diets featuring slowly-digested ‘lente’ carbohydrate, and by certain nutraceuticals which can slow carbohydrate absorption. Prebiotics that promote colonic generation of short-chain fatty acids represent an alternative strategy for boosting intestinal GLP-1 production. The health benefits of all these measures presumably would be potentiated by concurrent use of dipeptidyl peptidase 4 inhibitors, which slow the proteolysis of GLP-1 in the blood.
Glucagon-like peptide 1 (GLP-1) (link)
The glucagon-like peptide-1 (GLP-1) is a multifaceted hormone with broad pharmacological potential. Among the numerous metabolic effects of GLP-1 are the glucose-dependent stimulation of insulin secretion, decrease of gastric emptying, inhibition of food intake, increase of natriuresis and diuresis, and modulation of rodent β-cell proliferation. GLP-1 also has cardio- and neuroprotective effects, decreases inflammation and apoptosis, and has implications for learning and memory, reward behavior, and palatability. Biochemically modified for enhanced potency and sustained action, GLP-1 receptor agonists are successfully in clinical use for the treatment of type-2 diabetes, and several GLP-1-based pharmacotherapies are in clinical evaluation for the treatment of obesity.
GLP-1 release and vagal afferent activation mediate the beneficial metabolic and chronotherapeutic effects of d-allulose
Overeating and arrhythmic feeding promote obesity and diabetes. Glucagon-like peptide-1 receptor (GLP-1R) agonists are effective anti-obesity drugs but their use is limited by side effects. Here we show that oral administration of the non-calorie sweetener, rare sugar d-allulose (d-psicose), induces GLP-1 release, activates vagal afferent signaling, reduces food intake and promotes glucose tolerance in healthy and obese-diabetic animal models. Subchronic d-allulose administered at the light period (LP) onset ameliorates LP-specific hyperphagia, visceral obesity, and glucose intolerance. These effects are blunted by vagotomy or pharmacological GLP-1R blockade, and by genetic inactivation of GLP-1R signaling in whole body or selectively in vagal afferents. Our results identify d-allulose as prominent GLP-1 releaser that acts via vagal afferents to restrict feeding and hyperglycemia. Furthermore, when administered in a time-specific manner, chronic d-allulose corrects arrhythmic overeating, obesity and diabetes, suggesting that chronotherapeutic modulation of vagal afferent GLP-1R signaling may aid in treating metabolic disorders.
A Preliminary Study for Evaluating the Dose-Dependent Effect of d-Allulose for Fat Mass Reduction in Adult Humans: A Randomized, Double-Blind, Placebo-Controlled Trial (2018, pdf)
d-allulose is a rare sugar with zero energy that can be consumed by obese/overweight individuals. Many studies have suggested that zero-calorie d-allulose has beneficial effects on obesity-related metabolism in mouse models, but only a few studies have been performed on human subjects. Therefore, we performed a preliminary study with 121 Korean subjects (aged 20–40 years, body mass index ≥ 23 kg/m2). A randomized controlled trial involving placebo control (sucralose, 0.012 g × 2 times/day), low d-allulose (d-allulose, 4 g × 2 times/day), and high d-allulose (d-allulose, 7 g × 2 times/day) groups was designed. Parameters for body composition, nutrient intake, computed tomography (CT) scan, and plasma lipid profiles were assessed. Body fat percentage and body fat mass were significantly decreased following d-allulose supplementation. The high d-allulose group revealed a significant decrease in not only body mass index (BMI), but also total abdominal and subcutaneous fat areas measured by CT scans compared to the placebo group. There were no significant differences in nutrient intake, plasma lipid profiles, markers of liver and kidney function, and major inflammation markers among groups. These results provide useful information on the dose-dependent effect of d-allulose for overweight/obese adult humans. Based on these results, the efficacy of d-allulose for body fat reduction needs to be validated using dual energy X-ray absorption.
Interesting: D-Allulose Promotes Fat Loss - Not Compared to Sugar, but Compared to Non-Caloric Sweeteners (link)

Figure 1: Changes in body composition (kg) in response to 2x4g and 2x7g of d-allulose per day for 12 weeks (Han 2018).
Activation of GLP-1 receptor enhances the chemosensitivity of pancreatic cancer cells (2020)
This study aimed to determine whether and how the glucagon-like peptide 1 receptor (GLP-1R) agonist liraglutide affects the chemoresistance and chemosensitivity of pancreatic cancer cells to gemcitabine in vitro and in vivo. The GLP-1R and protein kinase A (PKA) levels were compared between the human pancreatic cancer cell line PANC-1 and the gemcitabine-resistant cell line PANC-GR. The in vitro effects of liraglutide on the cell proliferation and apoptosis as well as the nuclear factor-kappa B NF-κB expression levels of PANC-GR cells were evaluated. In addition, a mouse xenograft model of human pancreatic cancer was established by s.c. injection of PANC-1 cells, and the effects of liraglutide on the chemosensitivity were evaluated in vitro and in vivo. In contrast to PANC-1 cells, PANC-GR cells exhibited lower expression levels of GLP-1R and PKA. Incubation with liraglutide dose dependently inhibited the growth, promoted the apoptosis, and increased the expression of GLP-1R and PKA of PANC-GR cells. Similar effects of liraglutide were observed in another human pancreatic cancer cell line MiaPaCa-2/MiaPaCa-2-GR. Either the GLP-1R antagonist Ex-9, the PKA inhibitor H89, or the NF-κB activator lipopolysaccharide (LPS) could abolish the antiproliferative and proapoptotic activities of liraglutide. Additionally, each of these agents could reverse the expression of NF-κB and ABCG2, which was decreased by liraglutide treatment. Furthermore, liraglutide treatment increased the chemosensitivity of pancreatic cancer cells to gemcitabine, as evidenced by in vitro and in vivo experiments. Thus, GLP-1R agonists are safe and beneficial for patients complicated with pancreatic cancer and diabetes, especially for gemcitabine-resistant pancreatic cancer.
Glucagon-like peptide-1 analogues and risk of breast cancer in women with type 2 diabetes: population based cohort study using the UK Clinical Practice Research Datalink
Objective To determine whether the use of glucagon-like peptide-1 (GLP-1) analogues, compared with the use of dipeptidylpeptidase-4 (DPP-4) inhibitors, is associated with an increased risk of incident breast cancer in patients with type 2 diabetes.
Design Population based cohort study.
Setting Clinical Practice Research Datalink, UK.
Participants 44 984 women aged at least 40 years, who were newly treated with glucose lowering drugs between 1 January 2007 and 31 March 2015, with follow-up until 31 March 2016.
Main outcomes and measures Time varying use of GLP-1 analogues compared with use of DPP-4 inhibitors, with exposures lagged by one year for latency purposes. Time dependent Cox proportional hazards models were used to estimate adjusted hazard ratios with 95% confidence intervals of incident breast cancer associated with use of GLP-1 analogues overall, by cumulative duration of use, and time since initiation.
Results The cohort was followed for a mean of 3.5 years (standard deviation 2.2), with 549 incident events of breast cancer recorded (crude incidence 3.5 (95% confidence interval 3.3 to 3.8) per 1000 person years). Overall, compared with use of DPP-4 inhibitors, use of GLP-1 analogues was not associated with an increased risk of breast cancer (incidence 4.4 v 3.4 per 1000 person years; hazard ratio 1.40 (95% confidence interval 0.91 to 2.16)). Hazard ratios gradually increased with longer durations of use, with a peak between two to three years of GLP-1 use (2.66 (95% confidence interval 1.32 to 5.38)), and returned closer to the null after more than three years of use (0.98 (0.24 to 4.03)). A similar pattern was observed with time since initiation of GLP-1 analogues.
Conclusions In this population based cohort study, use of GLP-1 analogues was not associated with an overall increased risk of breast cancer. Although it is not possible to rule out a tumour promoter effect, the observed duration-response associations are likely the result of a transient increase in detection of breast cancers in GLP-1 analogue users.
Montanya E, Nacher V, Biarnes M, Soler J: Linear correlation between β-cell mass and body weight throughout the lifespan in Lewis rats: role of β-cell hyperplasia and hypertrophy. Diabetes49 :1341 –1346,2000
Glucagon-like peptide-1 receptor agonists in non-alcoholic fatty liver disease: An update (2020)
In patients with NAFLD, the GLP-1 receptor production is down-regulated. Recently, several animal and human studies have emphasized the role of GLP-1RAs in ameliorating liver fat accumulation, alleviating the inflammatory environment and preventing NAFLD progression to NASH. In this review, we summarize the updated literature data on the beneficial effects of GLP-1RAs in NAFLD/NASH. Finally, as GLP-1RAs seem to be an attractive therapeutic option for T2DM patients with concomitant NAFLD.
Weight Loss
Optimal BMI to minimize all cause mortality (2016)
The summary relative risk for a 5 unit increment in BMI was 1.18 among never smokers, 1.21 among healthy never smokers, 1.27 among healthy never smokers with exclusion of early follow-up, and 1.05 (1.04 to 1.07; I2=97%, n=198) among all participants. There was a J shaped dose-response relation in never smokers (Pnon-linearity <0.001), and the lowest risk was observed at BMI 23-24 in never smokers, 22-23 in healthy never smokers, and 20-22 in studies of never smokers with ≥20 years’ follow-up.
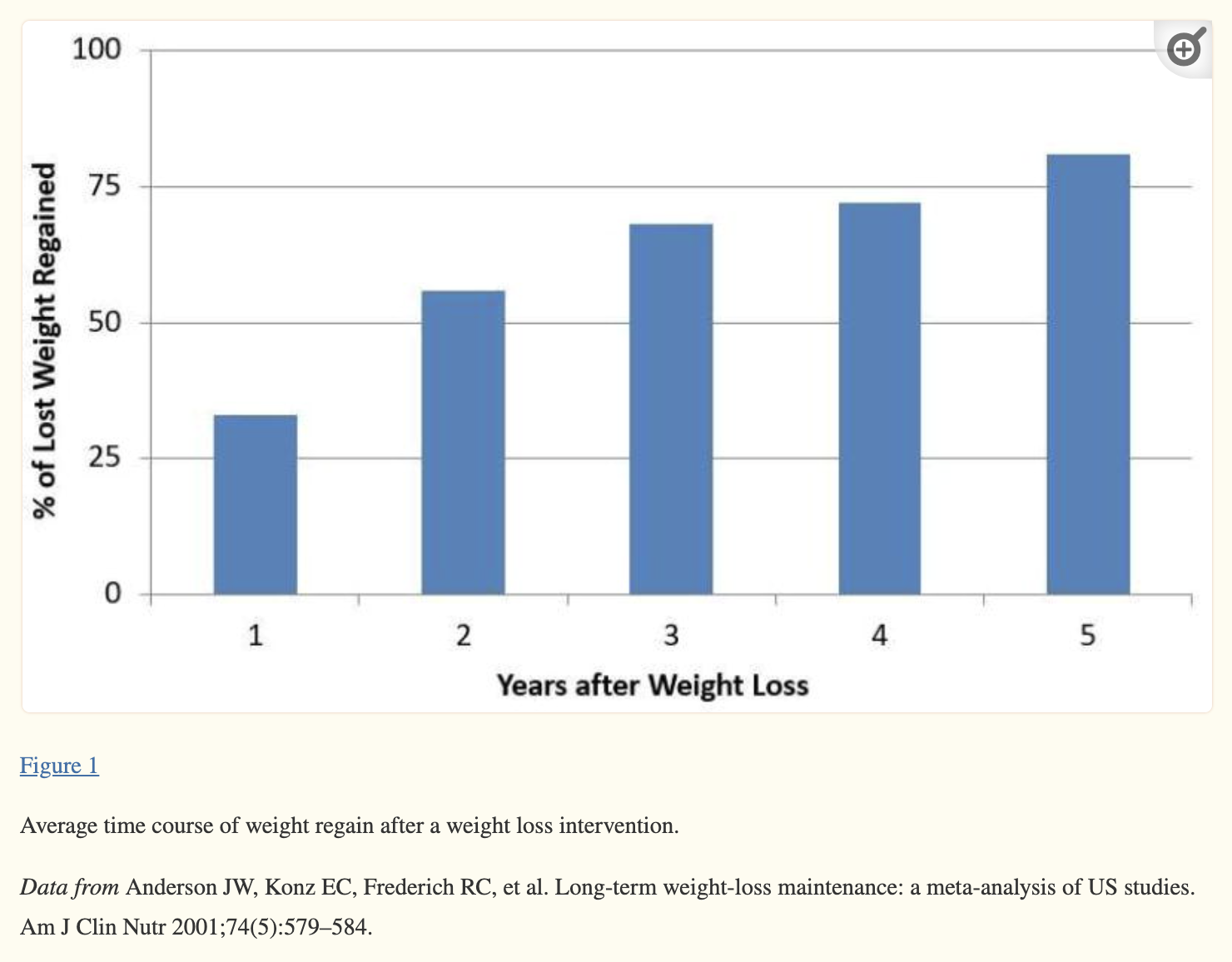
Once you become obese, permanent weight loss is very unlikely (2019)
In a meta-analysis of 29 long-term weight loss studies, more than half of the lost weight was regained within two years, and by five years more than 80% of lost weight was regained (Figure 1).
How to lower your body weight set point permanently?
[RCT] Lifestyle interventions: 15% reduction in all cause mortality after 5.5 kg avg. weight loss (ref) ← less likely to be permanent, works better if you aren't insulin resistant.
[RCT] Anti-diabetic drugs: Tirzepatide 22.5% (ref), Semaglutide 17% (ref), Acarbose 3%-7.5% (ref, ref, ref), Metformin 5.6% (ref) weight loss.
I.e. Metformin, Acarbose, SLT2-i, Rapamycin (anectodal) are extremely helpful for small weight loss. For big permanent weight loss, GLP1-RA class of drugs are the way to go.
[Association] Bariatric surgery: 38%-41% reduction in all cause mortality (ref, ref) after 10%-27% avg. weight loss (ref, ref, ref) ← last resort but extremely effective.
Bariatric Surgery
Impact on Mortality (link)
Studies show bariatric surgery reduces a patient’s risk of premature death by 20-30%.
Bariatric surgery is associated with significant improvement in long-term survival of over eight years in nearly 8,000 patients; mortality rate was 1.5% versus 2.1% for the general population (Surgical Endoscopy, 2015).
Extended from eight to 14 years, surgery patients’ mortality was 2.5% compared with a mortality rate for the general population of 3.1%
Bariatric surgery helps to improve or resolve more than 40 obesity-related diseases and conditions including type 2 diabetes, heart disease, certain cancers, sleep apnea, high blood pressure, high cholesterol, sleep apnea and joint problems.
60% reduction in mortality from cancer, with the largest reductions in breast and colon cancers
56% reduction in mortality from coronary artery disease
92% reduction in mortality from type 2 diabetes
Among nearly 16,000 patients with severe obesity, all-cause mortality decreased by 40% for up to seven years after gastric bypass compared to those who did not have surgery (NEJM, 2007).
Deaths from any obesity-related disease decreased by 52%, and were significantly lower for diabetes (92%), coronary artery disease (59%), and cancer (60%).
Findings from 2,010 patients in the Swedish Obese Subjects (SOS) study show bariatric surgery was associated with a nearly 30% long-term reduction in overall mortality over a 20-year period compared with usual care (Journal of Internal Medicine, 2012).
Bariatric Surgery and Long-term Durability of Weight Loss
OBJECTIVES
To examine 10-year weight change in a large, multisite, clinical cohort of veterans who underwent Roux-en-Y gastric bypass (RYGB) compared with nonsurgical matches and the 4-year weight change in veterans who underwent RYGB, adjustable gastric banding (AGB), or sleeve gastrectomy (SG).
DESIGN, SETTING, AND PARTICIPANTS
In this cohort study, differences in weight change up to 10 years after surgery were estimated in retrospective cohorts of 1787 veterans who underwent RYGB from January 1, 2000, through September 30, 2011 (573 of 700 eligible [81.9%] with 10-year follow-up), and 5305 nonsurgical matches (1274 of 1889 eligible [67.4%] with 10-year follow-up) in mixed-effects models. Differences in weight change up to 4 years were compared among veterans undergoing RYGB (n = 1785), SG (n = 379), and AGB (n = 246). Data analysis was performed from September 9, 2014, to February 12, 2016.
EXPOSURES
Bariatric surgical procedures and usual care.
MAIN OUTCOMES AND MEASURES
Weight change up to 10 years after surgery through December 31, 2014.
RESULTS
The 1787 patients undergoing RYGB had a mean (SD) age of 52.1 (8.5) years and 5305 nonsurgical matches had a mean (SD) age of 52.2 (8.4) years. Patients undergoing RYGB and nonsurgical matches had a mean body mass index of 47.7 and 47.1, respectively, and were predominantly male (1306 [73.1%] and 3911 [73.7%], respectively). Patients undergoing RYGB lost 21% (95% CI, 11%-31%) more of their baseline weight at 10 years than nonsurgical matches. A total of 405 of 564 patients undergoing RYGB (71.8%) had more than 20% estimated weight loss, and 224 of 564 (39.7%) had more than 30% estimated weight loss at 10 years compared with 134 of 1247 (10.8%) and 48 of 1247 (3.9%), respectively, of nonsurgical matches. Only 19 of 564 patients undergoing RYGB (3.4%) regained weight back to within an estimated 5% of their baseline weight by 10 years. At 4 years, patients undergoing RYGB lost 27.5% (95% CI, 23.8%-31.2%) of their baseline weight, patients undergoing AGB lost 10.6% (95% CI, 0.6%-20.6%), and patients undergoing SG lost 17.8% (95% CI, 9.7%-25.9%). Patients undergoing RYGB lost 16.9% (95% CI, 6.2%-27.6%) more of their baseline weight than patients undergoing AGB and 9.7% (95% CI, 0.8%-18.6%) more than patients undergoing SG.
CONCLUSIONS AND RELEVANCE
Patients in the Veterans Administration health care system lost substantially more weight than nonsurgical matches and sustained most of this weight loss in the long term. Roux-en-Y gastric bypass induced significantly greater weight loss among veterans than SG or AGB at 4 years. These results provide further evidence of the beneficial association between surgery and long-term weight loss that has been demonstrated in shorter-term studies of younger, predominantly female populatio
Short- and long-term mortality after bariatric surgery: A systematic review and meta-analysis
Aims: The objective of this study was to investigate short- (≤ 30 days) and long-term (≥ 2 years) all-cause mortality after bariatric surgery among adult patients with obesity.
Materials and methods: For short-term mortality, eligible studies comprised randomized controlled trials (RCTs) reporting perioperative mortality. For long-term mortality, eligible studies comprised RCTs and observational studies comparing mortality between obese patients after bariatric surgery and non-operated controls. Random-effects models using a Bayesian or frequentist approach were used to pool effect estimates of short- and long-term mortality, respectively.
Results: Short-term all-cause mortality based on 38 RCTs involving 4030 patients was 0.18% (95% CI, 0.04%-0.38%) and was higher for open surgeries (0.31%; 95% CI, 0.03%-0.97%) and similar in mixed surgeries (0.17%; 95% CI, 0.03%-0.43%) and restrictive surgeries (0.17%; 95% CI, 0.03%-0.45%). For long-term mortality, 12 observational studies involving 27 258 operated patients and 97 154 non-operated obese controls were included. Of these, 8 studies were eligible for the meta-analysis, which showed a reduction of 41% in all-cause mortality (hazard ratio, 0.59; 95% CI, 0.52-0.67; P < .001). Additionally, operated patients were 0.42 times as likely (95% CI, 0.25-0.72, P < .001) and 0.47 times as likely (95% CI, 0.36-0.63, P < .001) as non-operated obese controls to die from cardiovascular diseases and cancer, respectively.
Conclusions: Bariatric surgery is associated with low short-term mortality and may be associated with long-term reductions in all-cause, cardiovascular and cancer-related mortality.
A 23-year study of mortality and development of co-morbidities in patients with obesity undergoing bariatric surgery (laparoscopic gastric banding) in comparison with medical treatment of obesity
Background and aim
Several studies have shown that bariatric surgery reduces long term mortality compared to medical weight loss therapy. In a previous study we have demonstrated that gastric banding (LAGB) is associated with reduced mortality in patients with and without diabetes, and with reduced incidence of obesity co-morbidities (cardiovascular disease, diabetes, and cancer) at a 17 year follow-up. The aim of this study was to verify at a longer time interval (23 years) mortality and incidence of co-morbidities in patients undergoing LAGB or medical weight loss therapy.
Patients and methods
As reported in the previous shorter-time study, medical records of obese patients [body mass index (BMI) > 35 kg/m2 undergoing LAGB (n = 385; 52 with diabetes) or medical treatment (controls, n = 681; 127 with diabetes), during the period 1995–2001 (visit 1)] were collected. Patients were matched for age, sex, BMI, and blood pressure. Identification codes of patients were entered in the Italian National Health System Lumbardy database, that contains life status, causes of death, as well as exemptions, prescriptions, and hospital admissions (proxies of diseases) from visit 1 to June 2018. Survival was compared across LAGB patients and matched controls using Kaplan–Meier plots adjusted Cox regression analyses.
Results
Final observation period was 19.5 ± 1.87 years (13.4–23.5). Compared to controls, LAGB was associated with reduced mortality [HR = 0.52, 95% CI 0.33–0.80, p = 0.003], significant in patients with diabetes [HR = 0.46, 95% CI 0.22–0.94, p = 0.034], borderline significant in patients without diabetes [HR = 0.61, 95% CI = 0.35–1.05, p = 0.076]. LAGB was associated with lower incidence of diabetes (15 vs 75 cases, p = 0.001), of CV diseases (61 vs 226 cases, p = 0.009), of cancer (10 vs 35, p = 0.01), and of renal diseases (0 vs 35, p = 0.001), and of hospital admissions (92 vs 377, p = 0.001).
Conclusion
The preventive effect of LAGB on mortality is maintained up to 23 years, even with a decreased efficacy compared with the shorter-time study, while the preventive effect of LAGB on co-morbidities and on hospital admissions increases with time.
Association of Bariatric Surgery Using Laparoscopic Banding, Roux-en-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management With All-Cause Mortality
Exposures Bariatric surgery (laparoscopic banding, Roux-en-Y gastric bypass, or laparoscopic sleeve gastrectomy) or usual care obesity management only (provided by a primary care physician and which may include dietary counseling and behavior modification).
Main Outcomes and Measures The primary outcome, all-cause mortality, matched and adjusted for BMI prior to surgery, age, sex, socioeconomic status, diabetes, hyperlipidemia, hypertension, cardiovascular disease, and smoking.
Results The study population included 8385 patients who underwent bariatric surgery (median age, 46 [IQR, 37-54] years; 5490 [65.5%] women; baseline median BMI, 40.6 [IQR, 38.5-43.7]; laparoscopic banding [n = 3635], gastric bypass [n = 1388], laparoscopic sleeve gastrectomy [n = 3362], and 25 155 nonsurgical matched patients (median age, 46 [IQR, 37-54] years; 16 470 [65.5%] women; baseline median BMI, 40.5 [IQR, 37.0-43.5]). The availability of follow-up data was 100% for all-cause mortality. There were 105 deaths (1.3%) among surgical patients during a median follow-up of 4.3 (IQR, 2.8-6.6) years (including 61 [1.7%] who underwent laparoscopic banding, 18 [1.3%] gastric bypass, and 26 [0.8%] sleeve gastrectomy), and 583 deaths (2.3%) among nonsurgical patients during a median follow-up of 4.0 (IQR, 2.6-6.2) years. The absolute difference was 2.51 (95% CI, 1.86-3.15) fewer deaths/1000 person-years in the surgical vs nonsurgical group. Adjusted hazard ratios (HRs) for mortality among nonsurgical vs surgical patients were 2.02 (95% CI, 1.63-2.52) for the entire study population; by surgical type, HRs were 2.01 (95% CI, 1.50-2.69) for laparoscopic banding, 2.65 (95% CI, 1.55-4.52) for gastric bypass, and 1.60 (95% CI, 1.02-2.51) for laparoscopic sleeve gastrectomy.
Conclusions and Relevance Among obese patients in a large integrated health fund in Israel, bariatric surgery using laparoscopic banding, gastric bypass, or laparoscopic sleeve gastrectomy, compared with usual care nonsurgical obesity management, was associated with lower all-cause mortality over a median follow-up of approximately 4.5 years. The evidence of this association adds to the limited literature describing beneficial outcomes of these 3 types of bariatric surgery compared with usual care obesity management alone.
Adjustable Gastric Banding Surgery
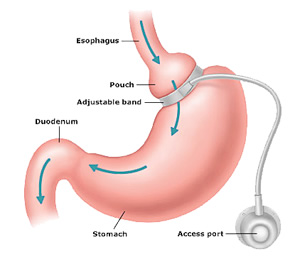
Adjustable Gastric Banding Surgery (laporascopic banding) features an inflatable band that is placed around the upper part of the stomach, dividing it into two unequal parts. The upper part acts as the new stomach, restricting food intake and promoting weight loss.
Adjustable Gastric Banding Surgery is performed through 4 or 5 tiny incisions. An inflatable silicone band is placed around the top portion of the stomach. The band is connected to a plastic reservoir or “port” which can be filled with fluid (saline solution). The port is placed beneath the skin on the abdominal wall for easy access.
Inflation of the band is accomplished by injecting small amounts of saline through the skin into the port. Inflation begins several weeks after its surgical placement. Subsequent band adjustments (inflation/deflation) are performed by the doctor throughout the weeks and months that follow until you attain a comfortable balance between eating restriction and weight loss.
Benefits of Adjustable Gastric Banding Surgery
The main benefit of laparoscopic banding is safety, with a 0.2% mortality rate and a 3-5% early complication rate.
Adjustable gastric banding surgery features the lowest mortality rate of all types of bariatric surgery
Least invasive bariatric surgical procedure
No cutting or rerouting of the intestines required
Low risk of nutritional deficiencies
Easy adjustability and reversibility
Generally good weight control in cooperative patients
Adjustable Gastric Banding Surgery vs. Gastric Bypass
While there are many benefits to Adjustable Gastric Banding surgery, there are also several disadvantages. Weight loss has been shown to occur more rapidly and over a longer period of time with gastric bypass. The reasons for superior weight loss stem from the small degree of malabsorption caused by bypassing nearly all of the stomach and the first two feet of the small intestine. To date, weight loss with gastric bypass has been much more consistent than with other gastric restrictive procedures.
Additionally, more than 20% of all Adjustable Gastric Banding surgeries in the U.S. require revisions during the first few years following surgery. Revisional surgery is performed for either device-related problems or unsatisfactory weight loss. The surgeons at the Center for Weight Loss & Metabolic Medicine regularly perform these revisions.
Our surgeons are ready to help you decide which bariatric procedure is right for you.
Is Adjustable Gastric Banding surgery reversible?
Yes, laparoscopic banding is reversible. Therefore, in the unlikely event that problems with the band develop, it can be removed through the same tiny incisions.
How well does Adjustable Gastric Banding surgery work?
Patients who have laparoscopic banding typically lose between 1-2 pounds per week. Studies reveal that patients can lose as much as 50% of their excess body weight and maintain their weight loss long term. A few patients will lose very little weight. However, patients who are compliant with their aftercare can have excellent results that compare well with other types of weight loss surgery at only a fraction of the risk.
Laparoscopic Adjustable Gastric Banding and Other Devices for the Management of Obesity, 2012
Association of metabolic-bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174 772 participants, 2021
Overall, about 7700 deaths occurred among 174,000 participants with 1.2 million patient-years of follow-up. Bariatric surgery, compared with nonsurgical management, was associated with significantly lower all-cause mortality (hazard ratio, 0.51) and an estimated 6.1-year longer median life expectancy. Both patients with and without diabetes had significantly lower rates of all-cause mortality with bariatric surgery than with nonsurgical management, but the treatment effect was greater for those with diabetes (HRs, 0.41 and 0.70, respectively). Median estimated life-expectancy gains after bariatric surgery for patients with and without diabetes were 9.3 and 5.1 years, respectively. Treatment effects were similar for gastric bypass, sleeve gastrectomy, and gastric banding, although differences could emerge with larger studies or longer follow-up.
Association of Bariatric Surgery With Cancer Risk and Mortality in Adults With Obesity, 2022
The study included 30,318 patients (median age, 46 years; median body mass index, 45; 77% female; and 73% White) with a median follow-up of 6.1 years (IQR, 3.8-8.9 years). The mean between-group difference in body weight at 10 years was 24.8 kg (95% CI, 24.6-25.1 kg) or a 19.2% (95% CI, 19.1%-19.4%) greater weight loss in the bariatric surgery group. During follow-up, 96 patients in the bariatric surgery group and 780 patients in the nonsurgical control group had an incident obesity-associated cancer (incidence rate of 3.0 events vs 4.6 events, respectively, per 1000 person-years). The cumulative incidence of the primary end point at 10 years was 2.9% (95% CI, 2.2%-3.6%) in the bariatric surgery group and 4.9% (95% CI, 4.5%-5.3%) in the nonsurgical control group (absolute risk difference, 2.0% [95% CI, 1.2%-2.7%]; adjusted hazard ratio, 0.68 [95% CI, 0.53-0.87], P = .002). Cancer-related mortality occurred in 21 patients in the bariatric surgery group and 205 patients in the nonsurgical control group (incidence rate of 0.6 events vs 1.2 events, respectively, per 1000 person-years). The cumulative incidence of cancer-related mortality at 10 years was 0.8% (95% CI, 0.4%-1.2%) in the bariatric surgery group and 1.4% (95% CI, 1.1%-1.6%) in the nonsurgical control group (absolute risk difference, 0.6% [95% CI, 0.1%-1.0%]; adjusted hazard ratio, 0.52 [95% CI, 0.31-0.88], P = .01).
Loss of Insulin Resistance after Roux-en-Y Gastric Bypass Surgery: a Time Course Study, 2005
Background: Gastric bypass has repeatedly been shown to improve and even cure type 2 diabetes by substantially improving insulin resistance. The mechanism by which it achieves this is not currently known, but some have hypothesized that there may be important humoral effects brought about by the bypass of the stomach, duodenum or proximal jejunum. A better understanding of the time course of the changes in insulin resistance after surgery might assist our understanding of potential mechanisms.
Methods: Intravenous glucose tolerance tests (IVGTT) were performed in 26 severely obese patients on the morning of gastric bypass surgery and again 6 days later. In addition insulin resistance was assessed in 71 patients undergoing gastric bypass surgery by the homeostasis model assessment (HOMA) method before surgery, and again at 6 days, 3, 6, 9, and 12 months. Patients were divided into 3 groups for analysis: diabetics, impaired glucose tolerance and normal glucose tolerance.
Results: All 3 groups of patients were noted to have insulin resistance prior to surgery. This was greatest in the diabetic patients, as indicated by HOMA. There was marked loss of/improvement in insulin resistance within 6 days of gastric bypass by both IVGTT and HOMA methods in all groups, which was maintained over the 12-month period. The study included 31 diabetic patients, of whom only 3 required medication following hospital discharge.
Conclusion: The changes in insulin resistance seen after gastric bypass, which are responsible for the resolution or improvement of type 2 diabetes occur within 6 days of the surgery, before any appreciable weight loss has occurred. This finding has implications for our understanding of the mechanism of insulin resistance in severely obese patients and is consistent with a humoral mechanism emanating from the GI tract.


Calorie Restriction
Slower Biological Aging In People On A Calorie Restricted Diet
https://www.youtube.com/watch?v=vQOTkkCVAJU
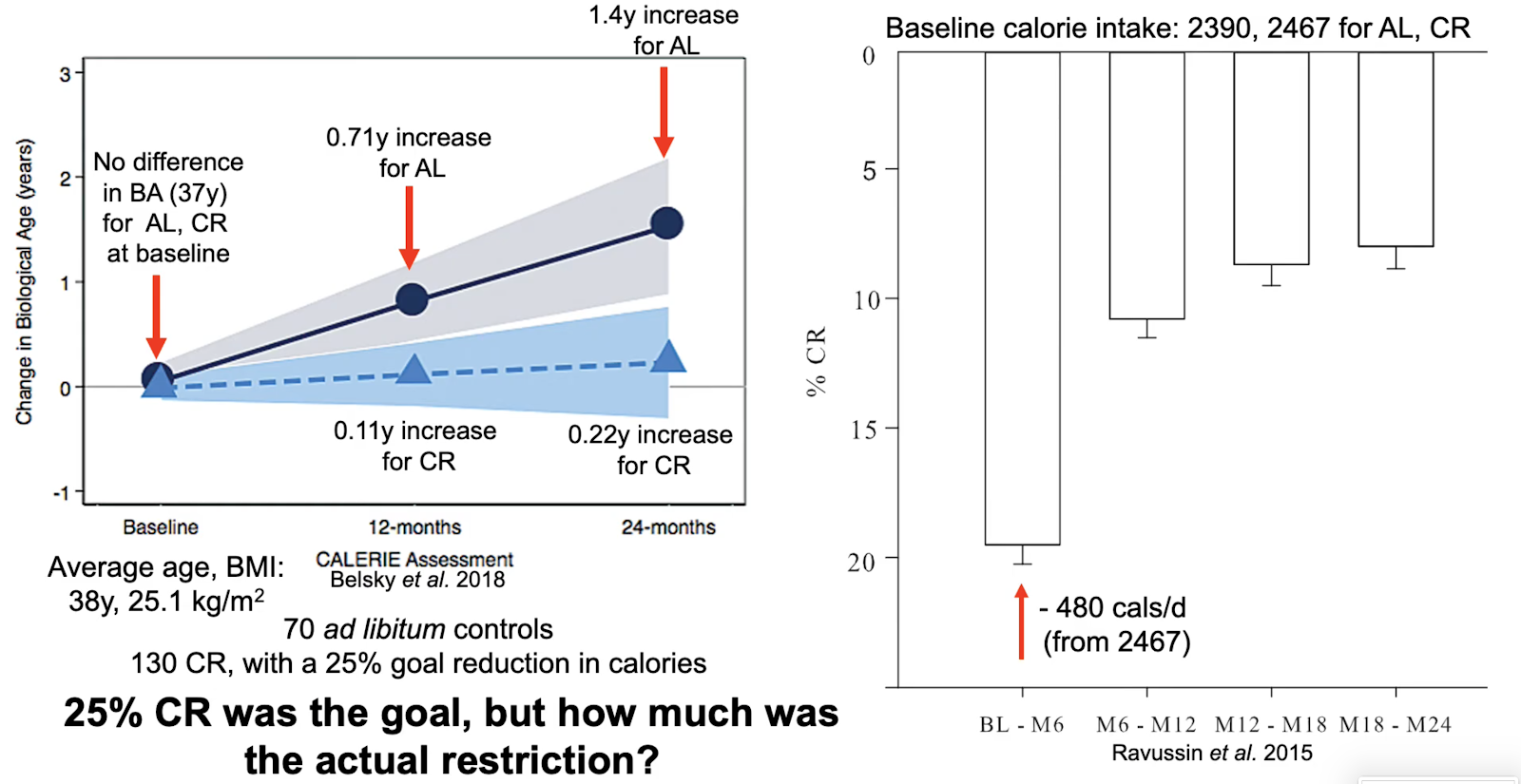
Life span extension by glucose restriction is abrogated by methionine supplementation: Cross-talk between glucose and methionine and implication of methionine as a key regulator of life span
https://advances.sciencemag.org/content/6/32/eaba1306.full

Using DNA methylation profiling to evaluate biological age and longevity interventions

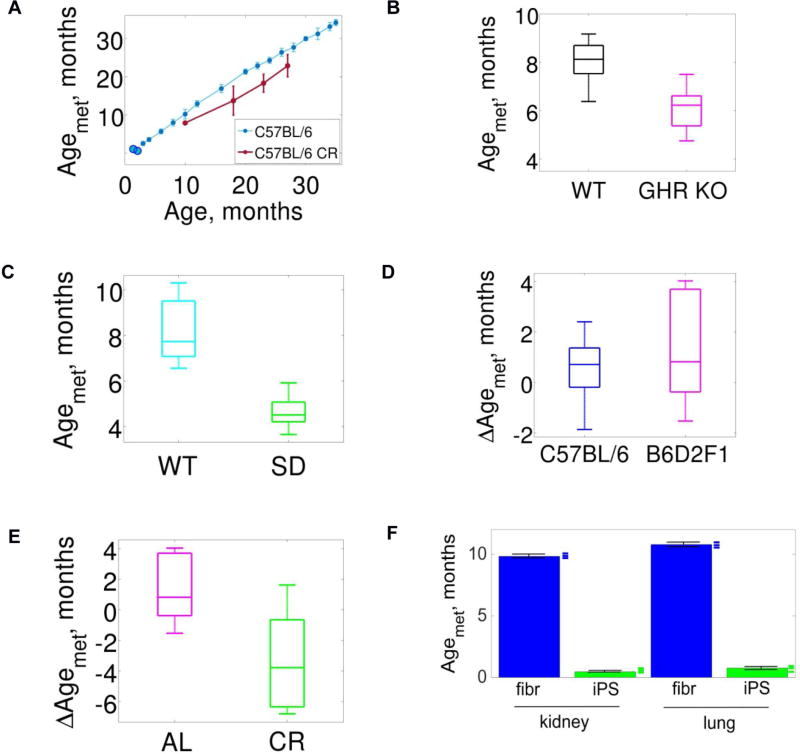

Longevity, body weight, and neoplasia in ad libitum-fed and diet-restricted C57BL6 mice fed NIH-31 open formula diet, 1995
Groups of C57BL6 mice of each sex were assigned to one of 2 dietary regimens, ad libitum (AL) or dietary restriction (DR), to study effects of food restriction on body weight, survival, and neoplasia. The AL and DR groups were subdivided into a scheduled sacrifice group for examination at 6-mo intervals, and a lifetime group to provide longevity data. Necropsies and microscopic examinations were conducted on 911 animals. In the lifetime group food consumption averaged 33.6 and 34.4 g per week by AL males and AL females, respectively; the DR counterparts were given 40% less. The diet contained 4.35 kcal/g. The average lifetime body weights were 34.8, 26.8, 22.6, and 21.6 g for AL males, AL females, DR males, and DR females, respectively, and their age at 50% survival was 27.5, 26.9, 31.7, and 33.5 mo. Maximal lifespan was increased 18% in DR males and females. Lifetime incidence of tumor-bearing mice was 89% and 86% for AL males and females, versus 64% for each sex of DR mice. Dramatic reduction occurred in female DR mice in lymphoma (9% vs 29%), pituitary neoplasms (1% vs 37%), and thyroid neoplasms (0.4% vs 8%). In males, hepatocellular tumors were reduced to 1% from 10% by DR. In contrast, the incidence of histiocytic sarcoma was increased in DR females and unaffected in DR males. Tumor onset was delayed in DR animals; 87% of all neoplasms in males and 95% in females had occurred in the AL mice by 24 mo, whereas the DR animals had only 52% and 39% of their lifetime incidence, respectively, by that age. This study provided comparative AL and DR data from C57BL6 mice examined randomly at 6-mo intervals (cross-sectional group) in parallel with data from animals in similar cohort that was unsampled and allowed to succumb naturally (longevity group). Dietary restriction reduced the lifetime percentage of tumor-bearing animals and the number of tumors per animal, and delayed the age at onset of most neoplasms.
[40% CR vs Ad Lib => 20% increase in median lifespan]


Comments