Aspirin
Aspirin appears useful for a variety of cancers to avoid the metastatic spread especially for localized or regional tumors.
Anti-inflammatory effects, anti-thrombotic effects appear to improve cancer outcomes.
Safely prevents thrombotic complications in patients with polycythemia vera (PV).
Post diagnosis aspirin improves survival in all gastrointestinal cancers
Patients using aspirin after their diagnosis had a chance of survival twice as high than that of those who did not use it in the same circumstances. A significant association between aspirin use and survival was observed for patients with oesophageal, hepatobiliary and colorectal cancer. The beneficial effect of aspirin use on survival was seen in patients with GI tumours after adjusting for potential confounding factors.
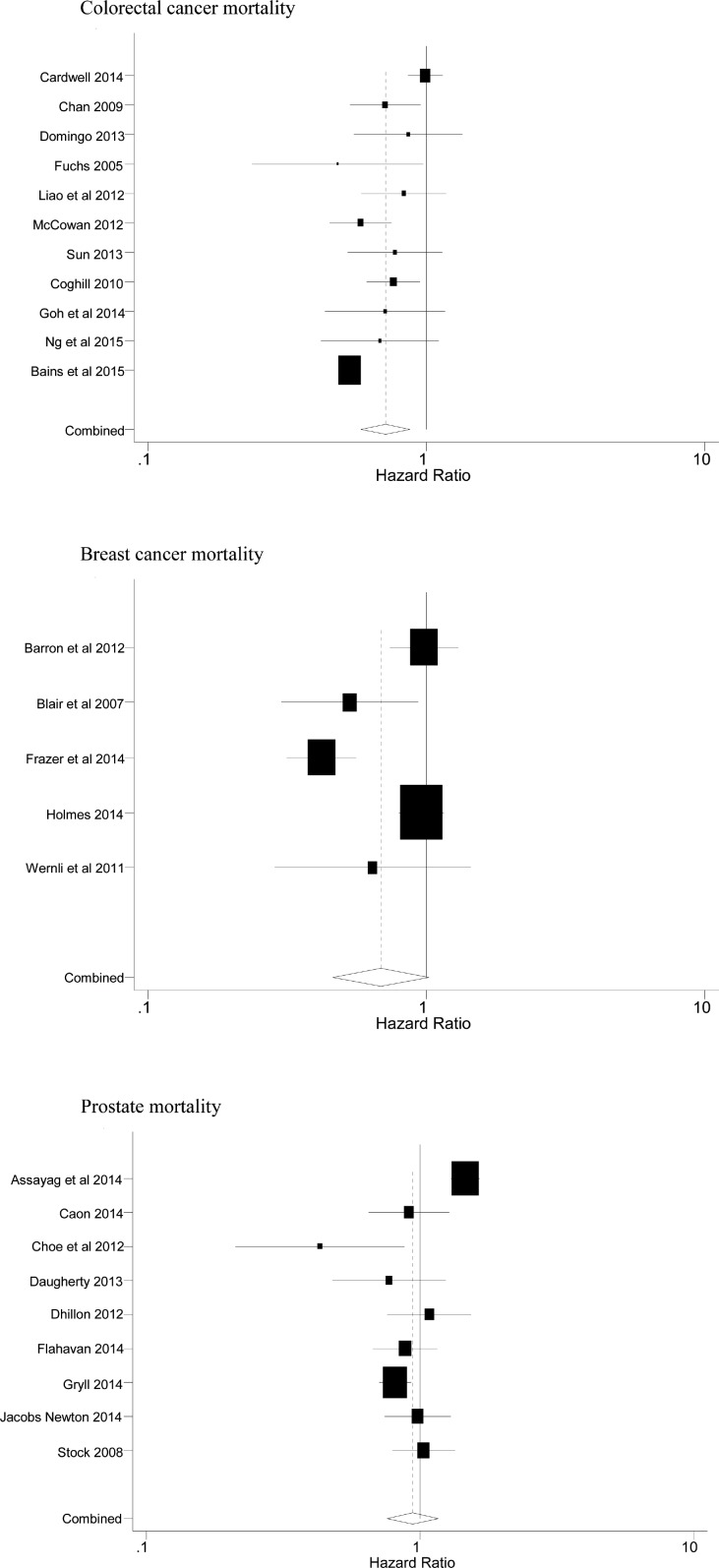
Aspirin use after diagnosis but not prediagnosis improves established colorectal cancer survival: a meta-analysis
Seven studies on postdiagnosis aspirin therapy and seven studies on prediagnosis aspirin use were finally included in this meta-analysis. The overall survival benefit associated with postdiagnosis aspirin use represented an HR of 0.84 (95% CI 0.75 to 0.94). This effect was observed both in colon cancer (HR=0.78, 95% CI 0.64 to 0.96) and in rectal cancer (HR=0.90, 95% CI 0.83 to 0.98). We observed no evidence of an association between prediagnosis aspirin use and CRC overall mortality (HR=1.01, 95% CI 0.96 to 1.06) or CRC-specific mortality (HR=0.93, 95% CI 0.82 to 1.05).
Association between low-dose aspirin use and breast cancer outcomes overall: a Swedish population-based study
An inverse association between low-dose aspirin use after diagnosis and breast cancer death was found for women with stage I tumors (HR 0.53, 95% CI 0.29–0.96). Among women with stage IV disease at diagnosis, aspirin use was not associated with time to breast cancer death (HR 0.91, 95% CI 0.67–1.23).
Use of Low-Dose Aspirin and Mortality After Prostate Cancer Diagnosis: A Nationwide Cohort Study.
The secondary analyses showed that prostate cancer mortality was slightly reduced with low-dose aspirin use after the 5-year (HR, 0.91 [CI, 0.83 to 1.01]) and 7.5-year (HR, 0.84 [CI, 0.72 to 0.97]) postdiagnosis exposure periods, notably among patients filling prescriptions for a large quantity of low-dose aspirin tablets during the 7.5-year period.
Postdiagnosis Use of Aspirin in Patients With Biliary Tract Cancer
Among the 2,934 patients, 667 (23%) had gallbladder cancer, 1,159 (53%) had cholangiocarcinoma, 224 (8%) had ampulla of Vater cancer, and 484 (16%) had overlapping biliary tract cancer lesions. Death occurred in a total of 2,415 patients (82%), with a reported median overall survival of 5.8 months. In total, 256 patients (9%) were aspirin users at baseline, and an additional 349 (12%) initiated aspirin use after diagnosis; 96% of aspirin users were prescribed a dose of 75 mg. Aspirin use was associated with decreased risk of death in patients with gallbladder cancer (hazard ratio [HR] = 0.63, 95% confidence interval [CI] = 0.48–0.83), cholangiocarcinoma (HR = 0.71, 95% CI = 0.60–0.85), ampulla of Vater cancer (HR = 0.44, 95% CI = 0.26–0.76), and overlapping biliary tract cancer lesions (HR = 0.68, 95% CI = 0.50–0.92).
Aspirin in the Treatment of Cancer: Reductions in Metastatic Spread and in Mortality: A Systematic Review and Meta-Analyses of Published Studies (link)
Aspirin May Prevent Cancer from Spreading, New Research Shows - Scientific American
An aspirin a day keeps metastasis at bay | Science Translational Medicine
Can aspirin stop my cancer spreading? | Cancer Research UK
Efficacy and Safety of Low-Dose Aspirin in Polycythemia Vera (Link)
BACKGROUND
The use of aspirin for the prevention of thrombotic complications in polycythemia vera is controversial.
METHODS
We enrolled 518 patients with polycythemia vera, no clear indication for aspirin treatment, and no contraindication to such treatment in a double-blind, placebo-controlled, randomized trial to assess the safety and efficacy of prophylaxis with low-dose aspirin (100 mg daily). The two primary end points were the cumulative rate of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes and the cumulative rate of nonfatal myocardial infarction, nonfatal stroke, pulmonary embolism, major venous thrombosis, or death from cardiovascular causes. The mean duration of follow-up was about three years.
RESULTS
Treatment with aspirin, as compared with placebo, reduced the risk of the combined end point of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes (relative risk 0.41; 95 percent confidence interval, 0.15 to 1.15; P=0.09) and the risk of the combined end point of nonfatal myocardial infarction, nonfatal stroke, pulmonary embolism, major venous thrombosis, or death from cardiovascular causes (relative risk 0.40; 95 percent confidence interval, 0.18 to 0.91; P=0.03). Overall mortality and cardiovascular mortality were not reduced significantly. The incidence of major bleeding episodes was not significantly increased in the aspirin group (relative risk, 1.62; 95 percent confidence interval, 0.27 to 9.71).
CONCLUSIONS
Low-dose aspirin can safely prevent thrombotic complications in patients with polycythemia vera who have no contraindications to such treatment.
Twice-Daily Low-Dose Aspirin Improves Antiplatelet Response in Essential Thrombocythemia
The authors reported that, after 2 weeks of treatment, patients who received aspirin 100 mg twice- or thrice-daily experienced substantial reductions in serum TXB₂ values. Between randomization and follow-up, the median values of serum TXB₂ reductions were as follows:
twice-daily aspirin 100 mg: from 20 ng/mL (IQR=11.6-6.4) to 4 ng/mL (IQR=2.1-6.7)
thrice-daily aspirin 100 mg: from 23.3 ng/mL (IQR=9.6-46.4) to 2.5 ng/mL (IQR=1.4-5.7)
In comparison, patients who were assigned to receive once-daily aspirin experienced “no appreciable short-term change in platelet COX-1 inhibition,” the authors reported.
Aspirin in ET: will twice a day keep thrombosis away? 2020
A Simple, One-Time, Inexpensive and Non-Toxic Intervention to Improve Cancer Survival (link)
Aspirin/antiplatelet agent use improves disease-free survival and reduces the risk of distant metastases in Stage II and III triple-negative breast cancer patients
Associations between aspirin use and the risk of cancers: a meta-analysis of observational studies
Aspirin use was associated with a significant decrease in the risk of overall cancer (RR = 0.89, 95% CI: 0.87–0.91), and gastric (RR = 0.75, 95% CI: 0.65–0.86), esophageal (RR = 0.75, 95% CI: 0.62–0.89), colorectal (RR = 0.79, 95% CI: 0.74–0.85), pancreatic (RR = 0.80, 95% CI: 0.68–0.93), ovarian (RR = 0.89, 95% CI: 0.83–0.95), endometrial (RR = 0.92, 95% CI: 0.85–0.99), breast (RR = 0.92, 95% CI: 0.88–0.96), and prostate (RR = 0.94, 95% CI: 0.90–0.99) cancers, as well as small intestine neuroendocrine tumors (RR = 0.17, 95% CI: 0.05–0.58).
Impact of Aspirin and Non-Aspirin Nonsteroidal Anti-Inflammatory Drugs on Outcomes in Patients with Metastatic Renal Cell Carcinoma
[Aspirin doesn’t seem to help after metastasis occurs. It’s important to take it before it happens.]
We investigated the impact of NSAIDs on survival outcomes in patients with metastatic RCC (mRCC). We conducted a pooled retrospective analysis of 4,736 mRCC patients treated on phase II and III clinical trials. Patients were categorized as: aspirin (ASA) only users, non-ASA NSAIDs only users, ASA and non-ASA NSAIDs users, and NSAIDs non-users. OS and PFS were significantly worse in non-ASA NSAIDs users compared to the NSAIDs non-users (OS hazard ratio (HR): 1.47, p < 0.0001, median 11.6 versus 21.1 months; PFS HR: 1.29, p < 0.0001, median 4.6 versus 7.4 months). There was no difference in survival in ASA users or ASA and non-ASA NSAIDs users compared to NSAIDs non-users.
Clinical study: Preventive Effects of Low-dose Aspirin as Adjuvant Therapy After Radical Nephrectomy on Disease Recurrence/Metastasis and Survival in Patients With Locally Advanced Renal Cell Carcinoma: an Observational Prospective Cohort Study (link)
Effects of Aspirin, Nonsteroidal Anti-inflammatory Drugs, Statin, and COX2 Inhibitor on the Developments of Urological Malignancies: A Population-Based Study with 10-Year Follow-up Data in Korea
Purpose
The purpose of this study was to determine the impact of aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), statin, and cyclooxygenase 2 (COX-2) inhibitor on the development of kidney, prostate, and urothelial cancers by analyzing the Korean National Health Insurance Service–National Sample Cohort (NHIS-NSC) database.
Materials and Methods
Among a representative sample cohort of 1,025,340 participants in NHIS-NSC database in 2002, we extracted data of 799,850 individuals who visited the hospital more than once, and finally included 321,122 individuals aged 40 and older. Following a 1-year washout period between 2002 and 2003, we analyzed 143,870 (male), 320,861 and 320,613 individuals for evaluating the risk of prostate cancer, kidney cancer and urothelial cancer developments, respectively, during 10-year follow-up periods between 2004 and 2013. The medication group consisted of patients prescribed these drugs more than 60% of the time in 2003. To adjustfor various parameters of the patients, a multivariate Cox regression model was adopted.
Results
During 10-year follow-up periods between 2004 and 2013, 9,627 (6.7%), 1,107 (0.4%), and 2,121 (0.7%) patients were diagnosed with prostate cancer, kidney cancer, and urothelial cancer, respectively. Notably, multivariate analyses revealed that NSAIDs significantly increased the risk of prostate cancer (hazard ratio [HR], 1.35). Also, it was found that aspirin (HR, 1.28) and statin (HR, 1.55) elevated the risk of kidney cancer. No drugs were associated with the risk of urothelial cancer.
Conclusion
In sum, our study provides the valuable information for the impact of aspirin, NSAID, statin, and COX-2 inhibitor on the risk of prostate, kidney, and urothelial cancer development and its survival outcomes.
A comparison of every-third-day versus daily low-dose aspirin therapy on serum thromboxane concentrations in healthy men and women
Aspirin's antithrombotic effect is mediated predominately by inhibition of platelet cyclooxygenase-1, leading to a decline in serum thromboxane A2 concentrations. We performed a placebo-controlled, randomized, double-blind trial to determine whether aspirin could be given at 3-day intervals and still achieve potent serum thromboxane inhibition. One hundred nine healthy men and women with no recent exposure to aspirin and no contraindications to its use participated. Subjects received 325 mg, 81 mg, or 40 mg of plain aspirin every third day, with placebo on other days; 81 mg of aspirin every day; or placebo every day. Serum concentrations of thromboxane B2 (the metabolite of thromboxane A2) were measured at 3-day intervals during a 31-day treatment period, as well as 4, 7, and 14 days after treatment ended. Serum thromboxane B2 concentrations were nearly identical during treatment with 325 mg of aspirin every third day or 81 mg of aspirin per day (86% inhibition [84%, 89%] and 85% inhibition [73%, 96%], respectively). An aspirin dose of 81 mg every third day was nearly as potent (74% inhibition [70%, 79%]), whereas 40 mg of aspirin every third day achieved only 50% inhibition (40%, 60%). Every-third-day low-dose aspirin regimens (325 and 81 mg) deserve comparison with daily low-dose aspirin regimens in controlled clinical trials because the former regimens could prove to have equal efficacy with reduced toxicity.
Influence of aspirin on platelet count and volume in humans.
20 healthy young male volunteers in vivo. Repeated blood sampling during a 7-day treatment with 250 mg aspirin daily showed an increased platelet count (7.3% on day 1, 3.0% on day 2, 6.8% on day 4 and 9.3% on day 7; p < 0.01) and total platelet mass (7.2, 5.0, 8.6 and 11.5% on days 1, 2, 4 and 7, respectively, p < 0.01).


Comments