Metformin
T2D RCC patients receiving metformin had a 38% lower risk of cancer-specific death.
Metformin exerts multitarget antileukemia activity in JAK2V617F+ MPNs.
Metformin Suppresses Cellular and Molecular Processes Related to Maintenance and Proliferation of MPN Stem Cells.
Metformin reversed bone marrow fibrosis in a small study with MF patients.
Diabetics taking metformin had significantly lower all-cause mortality than non-diabetics (hazard ratio (HR)=0.93, 95%CI 0.88-0.99).
In case matched T2D controls, metformin usage was associated with additional lifespan. All cause mortality HR=0.72, 95%CI 0.65-0.80.
Helps with avoiding weight gain and aids in weight loss in the obese (-5.6%).
Metformin increased lifespan in mice (ref) and C. elegans (ref, ref).
Dose: 500mg x 2 is often the recommended for cancer, general wellness
Kidney Cancer Survival Better Among Metformin Users (link)
Pooled data from 8 original studies involving 254,329 patients with kidney cancer in Asia or North America. Patients receiving metformin had a significant 36% lower risk of death overall and 38% lower risk of cancer-specific death, according to results published online in International Urology and Nephrology. Metformin use is associated with a decreased risk of kidney cancer in patients with T2DM.
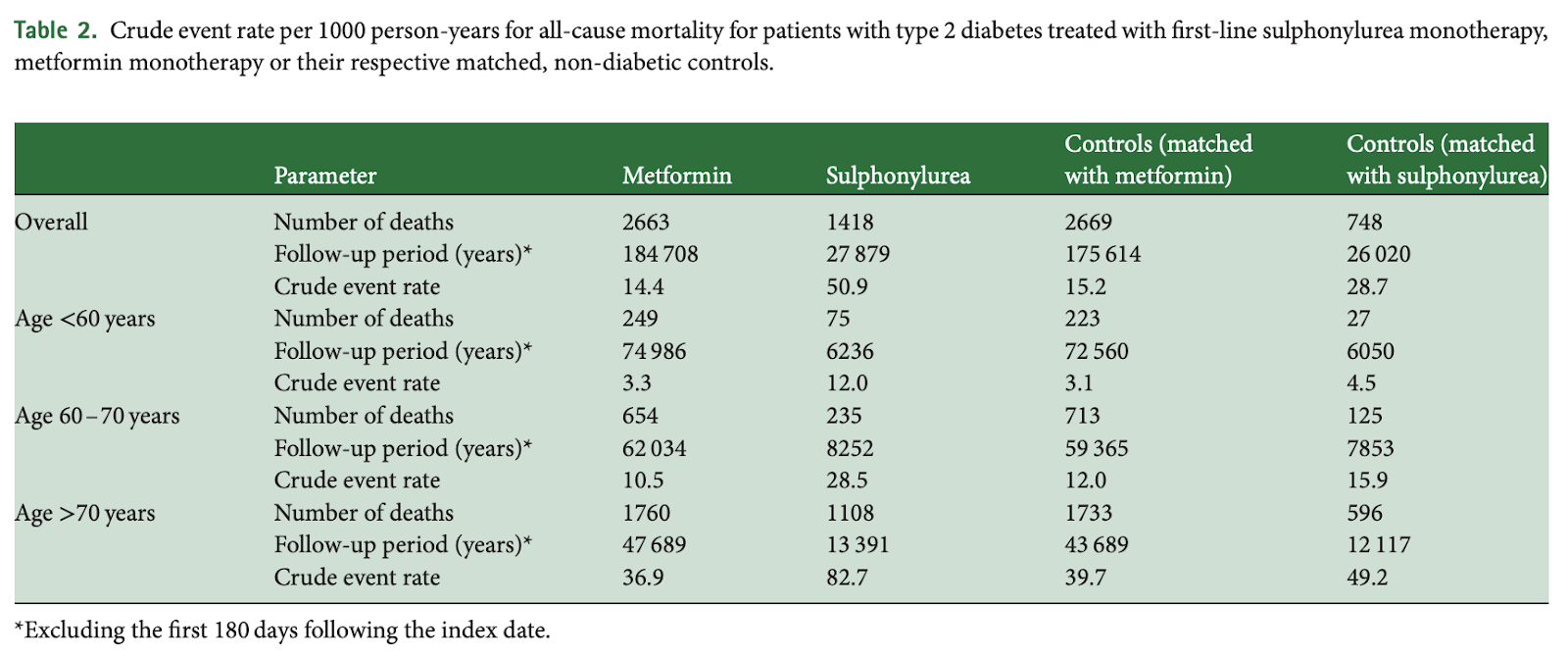
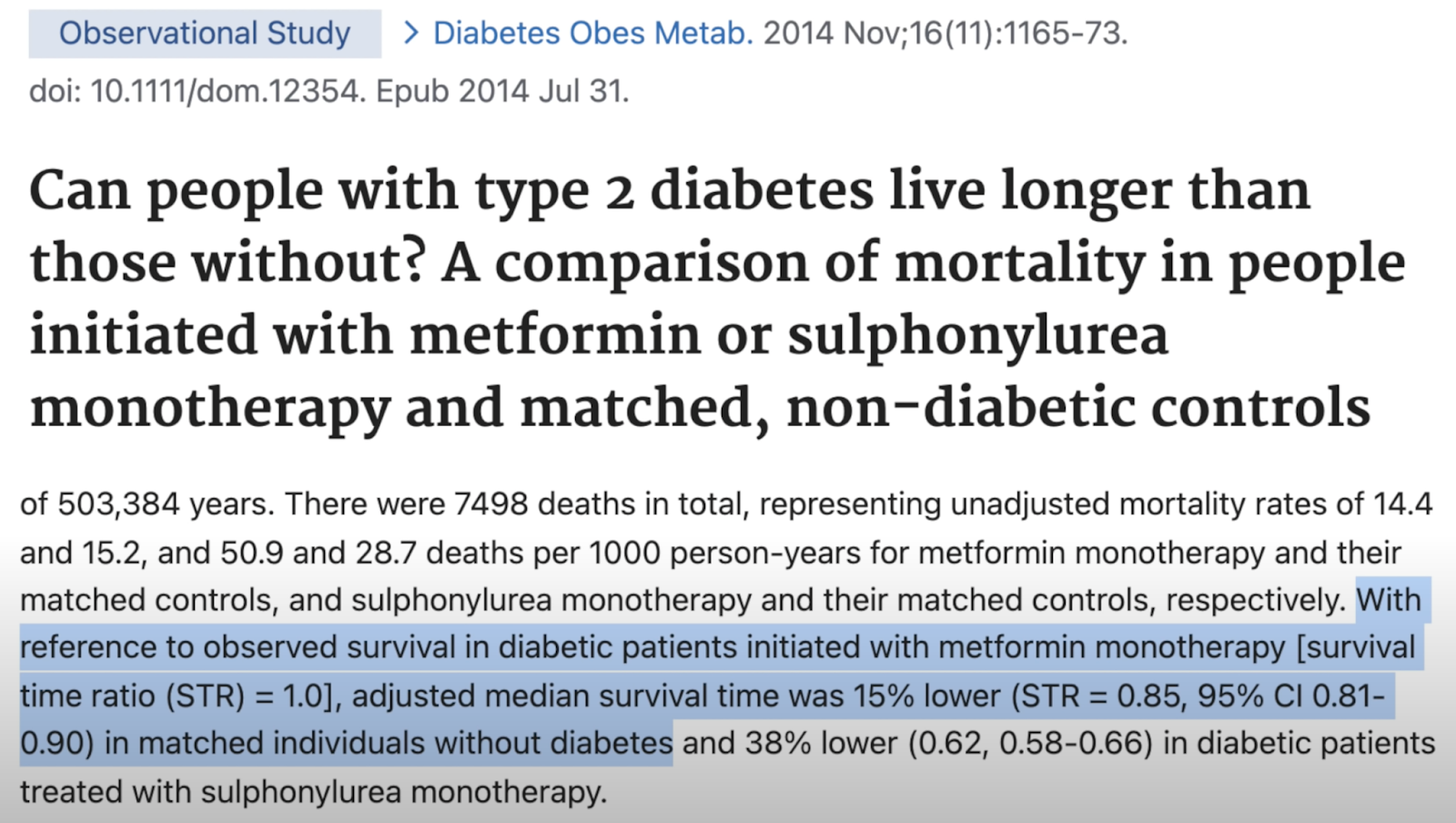
Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non-diabetic controls, 2014
Those on metformin had 5.2% lower all cause mortality vs non-diabetic controls.
Metformin reduces all-cause mortality and diseases of ageing independent of its effect on diabetes control: A systematic review and meta-analysis (2017)
This systematic review investigated whether the insulin sensitiser metformin has a geroprotective effect in humans. Pubmed and Embase were searched along with databases of unpublished studies. Eligible research investigated the effect of metformin on all-cause mortality or diseases of ageing relative to non-diabetic populations or diabetics receiving other therapies with adjustment for disease control achieved. Overall, 260 full-texts were reviewed and 53 met the inclusion criteria. Diabetics taking metformin had significantly lower all-cause mortality than non-diabetics (hazard ratio (HR)=0.93, 95%CI 0.88-0.99), as did diabetics taking metformin compared to diabetics receiving non-metformin therapies (HR=0.72, 95%CI 0.65-0.80), insulin (HR=0.68, 95%CI 0.63-0.75) or sulphonylurea (HR=0.80, 95%CI 0.66-0.97). Metformin users also had reduced cancer compared to non-diabetics (rate ratio=0.94, 95%CI 0.92-0.97) and cardiovascular disease (CVD) compared to diabetics receiving non-metformin therapies (HR=0.76, 95%CI 0.66-0.87) or insulin (HR=0.78, 95%CI 0.73-0.83). Differences in baseline characteristics were observed which had the potential to bias findings, although statistical adjustments were made. The apparent reductions in all-cause mortality and diseases of ageing associated with metformin use suggest that metformin could be extending life and healthspans by acting as a geroprotective agent.
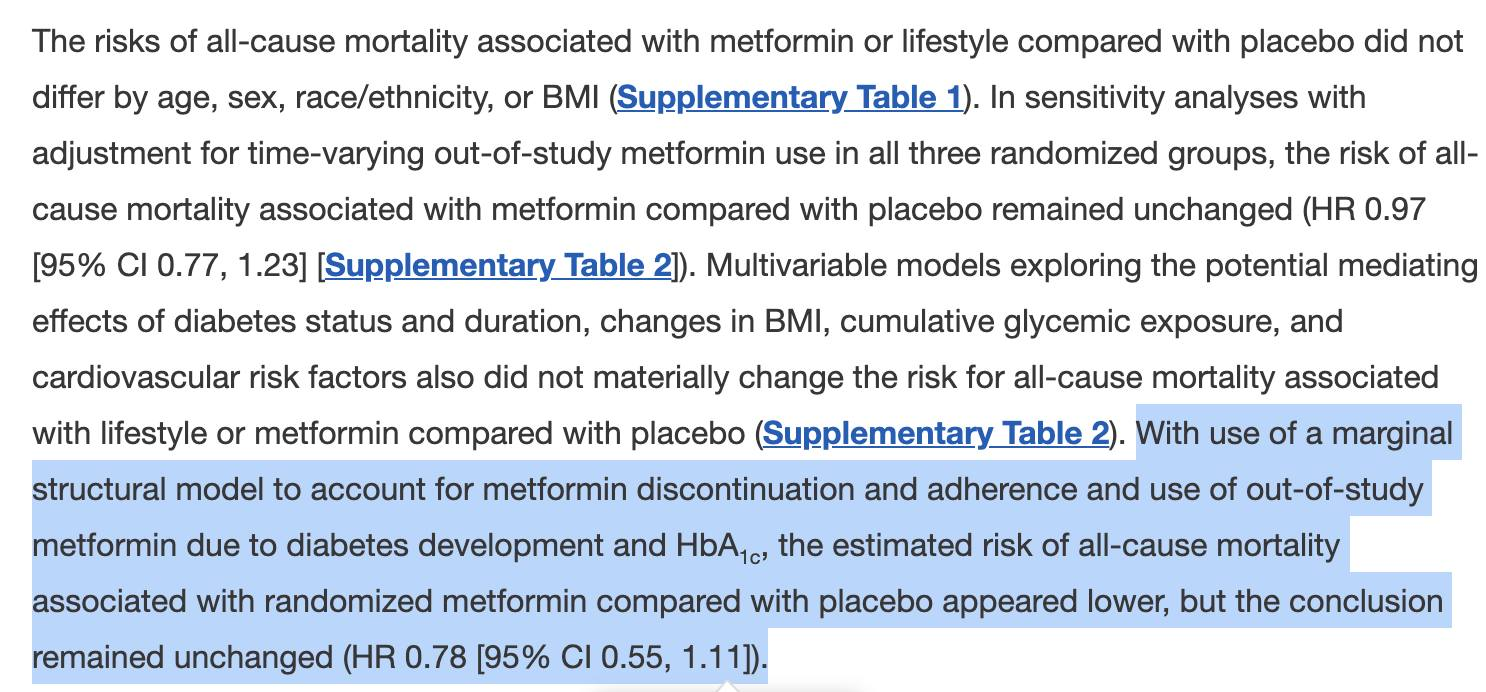
Effect of Metformin and Lifestyle Interventions on Mortality in the Diabetes Prevention Program and Diabetes Prevention Program Outcomes Study, 2021
From 1996 to 1999, 3,234 adults at high risk for type 2 diabetes were randomized to an intensive lifestyle intervention, masked metformin, or placebo. Placebo and lifestyle interventions stopped in 2001, and a modified lifestyle program was offered to everyone, but unmasked study metformin continued in those originally randomized. Causes of deaths through 31 December 2018 were adjudicated by blinded reviews. All-cause and cause-specific mortality hazard ratios (HRs) were estimated from Cox proportional hazards regression models and Fine-Gray models, respectively.
Over a median of 21 years (interquartile range 20–21), 453 participants died. Cancer was the leading cause of death (n = 170), followed by cardiovascular disease (n = 131). Compared with placebo, metformin did not influence mortality from all causes (HR 0.99 [95% CI 0.79, 1.25]), cancer (HR 1.04 [95% CI 0.72, 1.52]), or cardiovascular disease (HR 1.08 [95% CI 0.70, 1.66]). Similarly, lifestyle modification did not impact all-cause (HR 1.02 [95% CI 0.81, 1.28]), cancer (HR 1.07 [95% CI 0.74, 1.55]), or cardiovascular disease (HR 1.18 [95% CI 0.77, 1.81]) mortality. Analyses adjusted for diabetes status and duration, BMI, cumulative glycemic exposure, and cardiovascular risks yielded results similar to those for all-cause mortality.
Cancer was the leading cause of mortality among adults at high risk for type 2 diabetes. Although metformin and lifestyle modification prevented diabetes, neither strategy reduced all-cause, cancer, or cardiovascular mortality rates.

Is Metformin an Anti-aging Drug? (link)
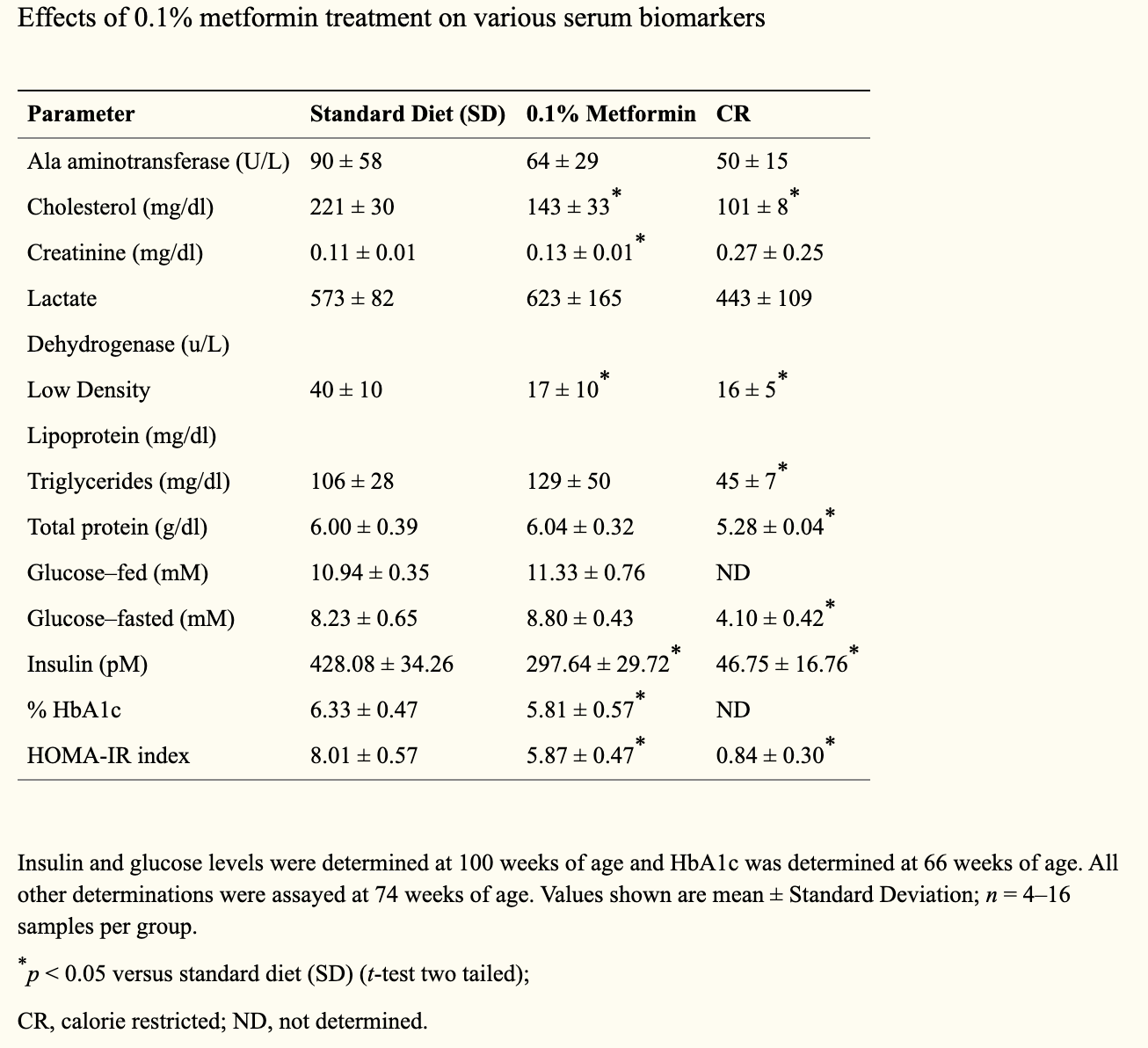
Metformin improves healthspan and lifespan in mice (link
Diet supplementation with 0.1% metformin led to a 5.83% extension of mean lifespan.
Metformin exerts multitarget antileukemia activity in JAK2V617F-positive myeloproliferative neoplasms, 2018
The recurrent gain-of-function JAK2V617F mutation confers growth factor-independent proliferation for hematopoietic cells and is a major contributor to the pathogenesis of myeloproliferative neoplasms (MPN). The lack of complete response in most patients treated with the JAK1/2 inhibitor ruxolitinib indicates the need for identifying novel therapeutic strategies. Metformin is a biguanide that exerts selective antineoplastic activity in hematological malignancies. In the present study, we investigate and compare effects of metformin and ruxolitinib alone and in combination on cell signaling and cellular functions in JAK2V617F-positive cells. In JAK2V617F-expressing cell lines, metformin treatment significantly reduced cell viability, cell proliferation, clonogenicity, and cellular oxygen consumption and delayed cell cycle progression. Metformin reduced cyclin D1 expression and RB, STAT3, STAT5, ERK1/2 and p70S6K phosphorylation. Metformin plus ruxolitinib demonstrated more intense reduction of cell viability and induction of apoptosis compared to monotherapy. Notably, metformin reduced Ba/F3 JAK2V617F tumor burden and splenomegaly in Jak2V617F knock-in-induced MPN mice and spontaneous erythroid colony formation in primary cells from polycythemia vera patients. In conclusion, metformin exerts multitarget antileukemia activity in MPN: downregulation of JAK2/STAT signaling and mitochondrial activity. Our exploratory study establishes novel molecular mechanisms of metformin and ruxolitinib action and provides insights for development of alternative/complementary therapeutic strategies for MPN.
Metformin Suppress Cellular and Molecular Processes Related to Maintenance and Proliferation of Myeloproliferative Neoplasm Stem Cell, 2019
Results: At randomization, mice of both groups were similar according PB chimerism, body weight and blood counts (all P>0.05). After 6 weeks of metformin treatment mice had no evidence of hematological toxicity or weight loss. Metformin treated mice presented lower platelets counts in PB (mean for vehicle vs. metformin: 4370×103/uL vs. 3451×103/uL; P=0.04) and reduction of splenomegaly (P=0.02). Metformin reduced CD45.2 chimerism (92.7% vs. 88.9%; P=0.03), and showed a trend in reducing pro-erythroblasts (0.91% vs. 0.53%; P=0.06) and early erythroid progenitors (37.4% vs. 32.4%; P=0.11), while increased late erythroid progenitors (16.2% vs. 27.2%; P=0.008) in spleen. Metformin significantly increased ST-HSC frequency (0.06% vs. 0.29%; P=0.001) compared to vehicle. Conversely, bone marrow mononuclear cells from metformin treated mice showed decreased clonogenic capacity (2.5 colonies/1000 BMMC vs. 8.6 colonies/1000 BMMC; P=0.001). Competitive secondary transplant into lethally irradiated mice was performed and results will be show at meeting. Metformin treatment did not modulate the frequency of erythroid progenitors, LT-HSC, MPP, MEP, GMP and CMP in BM nor of the stromal cells evaluated. In c-Kit enriched cells, PCR-array identified 31 downregulated and 64 upregulated genes by metformin treatment. Metformin reduced expression of anti-apoptotic genes (Bcl2 [Fold-change: 0.33] and Xiap [0.48]), cell cycle regulators (Cdkn2a [0.21], Ccnd1 [0.27], Ccn1a [0.42]), while increased expression of TP53 family members (Trp63 [4.1] and Trp53 [2.1]), pro-apoptotic (Bid [2.5] and Bcl10 [1.9]) and cellular-stress response genes (Atm [66.9] and Cdkn2a [3.1]).
Conclusions: In a conditional Jak2V617F-induced MPN murine model, daily treatment with metformin reduced tumor burden, extramedullary hematopoiesis, and clonogenic capacity of HSPC by acting on molecular processes related to maintenance and proliferation of MPN stem cell.
Analysis of Metformin Effects on Bone Marrow Fibrosis and Disease Progression in Primary Myelofibrosis Patients: Preliminary Results of an Open Label Phase II Trial (FIBROMET), 2019
MF patients received Metformin 1500-2000mg for 6 months. Primary endpoint was BM fibrosis reversion.
A reduction in BM collagen area percentage was observed comparing pretreatment biopsies (26.9% (14.8-53.1%)) versus 3 months (3.8% (2.3-4.0%), p=0.062) and versus 6 months of MTF use (0.84% (0.12-17.1%), p=0.125), however, this result was not statistically significant probably due to the low number of patients analyzed (n=5).
Metformin Plus Ruxolitinib: A Potential Therapeutic Alternative for Myeloproliferative Neoplasms, 2018
Assay results showed that metformin alone reduced cell viability in a dose- and time-dependent manner, and further analysis of metformin and ruxolitinib alone confirmed significantly reduced cell viability.
In combination, ruxolitinib and metformin demonstrated a synergistic effect and significantly reduced cell viability compared to monotherapy. Additional investigations revealed metformin plus ruxolitinib increased apoptotic activity, reduced cell proliferation, clonogenicity, cellular oxygen, suspended the cell cycle, and completely inhibited colony formation.
Metformin therapy also reduced tumor burden in Ba/F3 JAK2V617F, splenomegaly in Jak2V617F knock-in-induced MPN mice, and inhibited spontaneous erythroid colony formation in primary cells from patients with polycythemia vera.
Multitarget Antileukemic Effects of Metformin in Myeloproliferative Neoplasm Cells: Inhibition of JAK2/STAT Signaling and Mitochondrial Activity
Background: The recurrent JAK2V617F gain-of-function mutation confers growth factor-independent proliferation for hematopoietic cells and is a major contributor to the pathogenesis of myeloproliferative neoplasms (MPN). The lack of complete response in most patients treated with the JAK1/2 inhibitor, ruxolitinib, indicates the need for identifying novel therapeutic strategies. Metformin is a biguanide that inhibits the mitochondrial complex I and metformin antineoplastic activity has been described in leukemia, lymphoma and multiple myeloma. More importantly, metformin antineoplastic effects appear to act selectively in cancer cells, since cytotoxicity was not observed for normal hematopoeitic cells. Considering that metformin has been widely used in clinical practice, preclinical studies in an attempt to determine its effects, alone or in combination with ruxolitinib, in MPN, may be of interest, since these findings have a translational potential.
Objectives: To investigate the effects of metformin and/or ruxolitinib on cell signaling and cellular functions of JAK2V617F cells. Metformin and/or ruxolitinib effects were also evaluated on spontaneous erythroid colony formation from polycythemia vera (PV) patients.
Materials and methods: HEL, SET2 (JAK2V617F) and Ba/F3 JAK2V617F cell lines treated or not with metformin (5 and 10 mM) and/or ruxolitinib (300 nM) were submitted for cell viability (MTT), clonogenicity (colony formation), cell cycle (flow cytometry), cell proliferation (Ki-67 staining), apoptosis (annexin-V/PI and caspase 3/PARP1 cleavage), PCR array for PI3K/AKT-related genes and oxygen consumption (high-resolution respirometry). For spontaneous erythroid colony formation assays, mononuclear cells from peripheral blood or bone marrow of PV patients (n=3) were cultured on methylcellulose supplied with hematopoietic growth factors except EPO, in the presence or not of metfomin (2.5 mM) and/or ruxolitnib (50 nM). Gene and protein expressions were evaluated by qPCR and Western blot. Statistical analyses were performed by ANOVA test or Student's t-test.
Results: In HEL, SET2 and Ba/F3 JAK2V617F cells, metformin or ruxoltinib treatment significantly reduced cell viability and clonogenicity (p<0.05). Ruxolitinib plus metformin significantly decreased cell viability and induced apoptosis when compared with monotherapy (p<0.05). Metformin and/or ruxolitinib delay cell cycle progression (p<0.05). In HEL cells, PCR-array identified 11, 14 and 17 genes modulated by metformin, ruxolitinib, and combined treatment, respectively. Reduced cyclin D1 (CCND1) and upregulated p27 (CDKN1B) were validated in HEL and SET2 cells (p<0.05). We also observed downregulation of retinoblastoma (RB) phosphorylation, a cyclin D1 target and a key cell cycle progression-related protein, in both JAK2V617F cell lines upon all treatment conditions. Ruxolitinib treatment reduced STAT3, STAT5, ERK1/2, 4EBP1 and P70S6K phosphorylation. Metformin also reduced activation of same proteins, but combined treatment presented more intense inhibition of ERK1/2 and P70S6K activation compared to metformin or ruxolitinib monotherapy. A strong reduction of cellular oxygen consumption supported by exogenous substrates in culture media (ROUTINE state), at the non-phosphorylating state (LEAK) and at the maximum respiratory capacity (ETS state) was observed in metformin- and metformin plus ruxolitinib-treated HEL, SET2 and Ba/F3 JAK2V617F cells (p<0.05). Ruxolitinib significantly reduced oxygen consumption at routine, leak and ETS states only in SET2 and Ba/F3 JAK2V617F cells and at LEAK state in HEL cells. In primary cells from PV patients, a reduction of 71±21%, 94±4%, 98±1% was observed on spontaneous erythroid colony formation upon metformin, ruxolitinib and metformin plus ruxolitinib treatment, respectively.
Conclusion: Metformin exerts an anticancer activity and downregulates JAK2/STAT and MAPK signaling in JAK2V617F cells. PCR-array identified cyclin D1 and p27 as target of metformin and ruxolitinib, corroborating cell cycle and proliferation findings. Our exploratory study establishes novel molecular mechanisms of metformin and ruxolitinib action on JAK2V617F aberrant signaling and provides insights for development of alternative/complementary therapeutic strategies for MPN.
Effectiveness of metformin on weight loss in non-diabetic individuals with obesity (link)
Metformin is an effective drug to reduce weight in a naturalistic outpatient setting in insulin sensitive and insulin resistant overweight and obese patients.
Repurposing metformin for cancer treatment: current clinical studies (link)
In recent years, several studies have presented evidence suggesting a potential role for metformin in anti-cancer therapy. Preclinical studies have demonstrated several anticancer molecular mechanisms of metformin including mTOR inhibition, cytotoxic effects, and immunomodulation. Epidemiologic data have demonstrated decreased cancer incidence and mortality in patients taking metformin. Several clinical trials, focused on evaluation of metformin as an anti-cancer agent are presently underway. Data published from a small number of completed trials has put forth intriguing results.
The beneficial effects of metformin on cancer prevention and therapy: a comprehensive review of recent advances, 2019
Metformin is a widely used drug in today’s prescriptions by physicians due to its specific effects in treating and curing type II diabetes. Diabetes is a common disease that may occur throughout human life, and can increase the likelihood of the occurrence of various types of cancer, such as colon, rectum, pancreas and liver cancers, compared to non-diabetic patients. Metformin inhibits mTOR activity by activating ATM (ataxia telangiectasia mutated) and LKB1 (liver kinase B1) and then adenosine monophosphate-activated kinase (AMPK), and thus prevents protein synthesis and cell growth. Metformin can activate p53 by activating AMPK and thereby ultimately stop the cell cycle. Given the potential of metformin in the treatment of cancer, it can be used in radiotherapy, chemotherapy and to improve the response to treatment in androgen derivatives (ADT), and also, according to available evidence, metformin can also be used to prevent various types of cancers. Generally, metformin can: 1) reduce the incidence of cancers, 2) reduce the mortality from cancers, 3) increase the response to treatment in cancer cells when using radiotherapy and chemotherapy, 4) optimize tumor movement and reduce the malignancy, 5) reduce the likelihood of relapse, and 6) reduce the damaging effects of ADT. Therefore, this drug can be used as a complementary therapeutic agent for cancer treatment and prevention. In this review, we have summarized the data from various experimental and clinical studies and highlight the possible potential effects of metformin on cancer therapeutic responses.
Effect of Metformin Use on Survival Outcomes in Patients With Metastatic Renal Cell Carcinoma, 2016
In light of the emerging evidence of the antineoplastic potential of metformin, we investigated its effect on survival outcomes in metastatic renal cell carcinoma using a large clinical trial database. Although metformin did not affect survival in the overall cohort, it conferred a survival advantage in diabetic metastatic renal cell carcinoma patients treated with sunitinib.
Is it still worth pursuing the repurposing of metformin as a cancer therapeutic? (2023)
Larger randomized trials across cancer types have not demonstrated a clear benefit for metformin treatment. Key negative trials:
Breast (Goodwin et al, 2022): No improvement in disease-free survival when added to standard adjuvant therapy.
Lung (Tsakiridis et al, 2021; Skinner et al, 2021): No benefit when combined with concurrent chemoradiotherapy.
Prostate (Martin-Castillo et al, 2021): No improvement in progression-free survival when added to docetaxel.
A few small positive trials have observed potential benefits but were underpowered (El-Haggar et al, 2016; Arrieta et al, 2019).
Overall, metformin has failed to show efficacy in late phase trials across cancer types.
Breast Cancer: Results: 40 patients were randomized (22 metformin, 18 placebo) with a mean age of 55 vs 57 years and ER/PR positive BC in 86.4% vs 83.3% off metformin vs placebo, respectively. ...
Conclusion: In this population metformin showed no significant effect on RR, PFS or OS. These results do not support the use of metformin with chemotherapy in non-diabetic MBC patients. (link)
Breast Cancer: MA.32. Among patients with high-risk operable breast cancer without diabetes, the addition of metformin vs placebo to standard breast cancer treatment did not significantly improve invasive disease-free survival (link)
Endometrial Cancer: PFS and OS were not significantly increased with the addition of metformin to paclitaxel and carboplatin for the treatment of advanced and recurrent endometrial cancer (link).
Prostate Cancer: MET addition failed to improve the standard DOCE regimen in mCRPC. But the trend is in the right direction (link).
Lung Cancer: In this randomized clinical trial, the addition of metformin to chemoradiotherapy was associated with worse treatment efficacy and increased toxic effects compared with combined modality therapy alone in LA-NSCLC.
Lung Cancer: In this randomized clinical trial, the addition of metformin to concurrent chemoradiation was well tolerated but did not improve survival among patients with unresectable stage III NSCLC.


Comments