ACE Inhibitor
Improves the survival odds of cancer patients with the largest effect seen in Renal Cell Carcinoma (RCC).
Reduces mortality amongst hypertensives in human RCTs (link).
Increases the lifespan in rodents, worms and fruit fly with normal blood pressure, acting as anti-aging drugs [132–134], (link), (link).
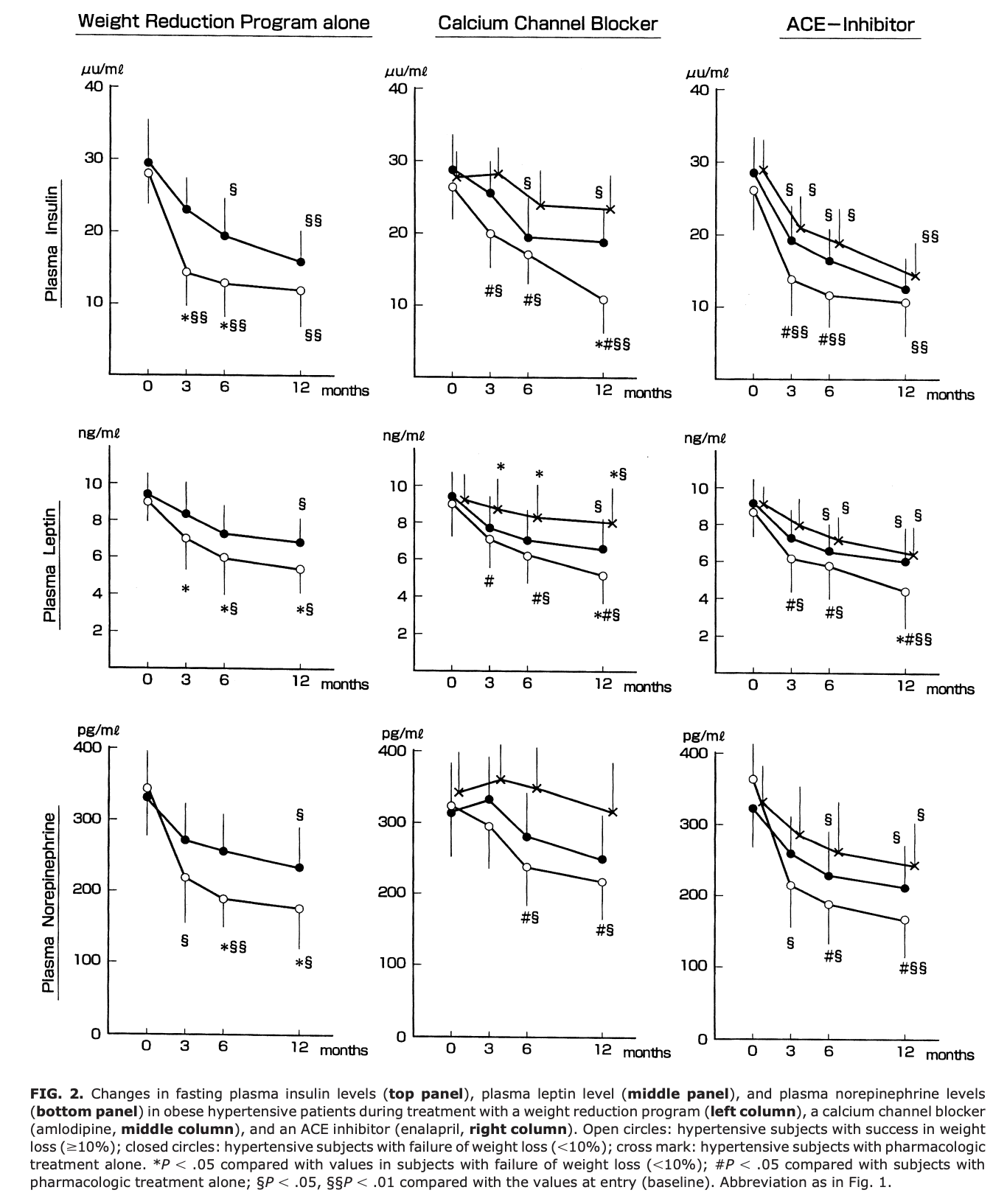
In obese hypertensives, it has a striking effect to lower plasma leptin. Suppresses sympathetic activity, insulinemia, and leptinemia. This appears to play a role in the BP reduction and weight loss.
Prognostic Impact of Renin-Angiotensin System Blockade on Renal Cell Carcinoma After Surgery
Background: Angiotensin 2 is a key biologic peptide in the renin-angiotensin system (RAS) that regulates blood pressure and renal hemodynamics. The potential role of the RAS in the promotion of tumor growth, angiogenesis, and metastasis also has been shown in the past few decades. This study investigated the prognostic impact of RAS blockade on patients with renal cell carcinoma (RCC) after surgery.
Methods: The study identified 557 patients with pathologically diagnosed RCC (pT1-4 N0M0) and evaluated the prognostic factors after surgery for patients administered or not administered angiotensin-converting enzyme inhibitors (ACEs) or angiotensin 2 receptor blockers (ARBs).
Results: The median follow-up period was 5.1 years. Radical nephrectomy was performed for 349 patients (62.7 %), whereas the remaining 208 patients (37.3 %) underwent partial nephrectomy. A total of 104 patients (18.7 %) were administered RAS inhibitors: ACEs (n = 22) or ARBs (n = 82). Multivariate analysis showed that administration of RAS inhibitors (P = 0.044; HR 2.69), longer tumor length (P < 0.001; HR 1.02), high-grade tumor (P < 0.001; HR 3.55), and positive microvascular invasion (P < 0.003; HR 3.13) were not independent risk factors for a decrease in subsequent disease-specific survival after surgery for RCC. The 5-year disease-specific survival rate was 96.8 % among the patients administered RAS inhibitors and 89.8 % among their counterparts (P = 0.019).
Conclusions: The authors propose renin-angiotensin blockade as a possible potent choice for effective treatment after surgical treatment of RCC.
Do renin–angiotensin system inhibitors influence the recurrence, metastasis, and survival in cancer patients? (link)
Evidence from a meta-analysis including 55 studies
Background:
Renin–angiotensin system inhibitors (RAS inhibitors) are antihypertensive agents with potential antitumor effects. However, various studies have yielded conflicting results on the influence of RAS inhibitors on survival of cancer patients. The aim of this study was to evaluate the effect of RAS inhibitors on recurrence, metastasis, and survival in cancer patients through a meta-analysis.
Methods:
PubMed, Web of Science, EMBASE, and Cochrane Library were systematically searched from inception to December 2016. The pooled hazard ratio (HR) with its 95% confidence interval (95% CI) was calculated to evaluate the association between RAS inhibitors and recurrence, metastasis, and survival in cancer patients.
Results:
Fifty-five eligible studies were included in the present meta-analysis. Results showed that there were significant improvements in overall survival (OS) (HR = 0.82; 95% CI: 0.77–0.88; P < 0.001), progression-free survival (HR = 0.74; 95% CI: 0.66–0.84; P < 0.001), and disease-free survival (HR = 0.80; 95% CI: 0.67–0.95; P = 0.01) in RAS inhibitor users compared with nonusers. Subgroup analyses revealed that the effect of RAS inhibitors on OS depended on the cancer type or different RAS inhibitors.
Conclusion:
This meta-analysis suggests that RAS inhibitors could improve the survival of cancer patients and depend on cancer type and types of RAS inhibitors.
Our results revealed a significantly better outcome in OS among RAS inhibitor users with renal cell carcinoma (HR = 0.64; 95% CI: 0.49–0.85; P = 0.002), gastric cancer (HR = 0.57; 95% CI: 0.38–0.84; P = 0.005), pancreatic cancer (HR = 0.91; 95% CI: 0.87–0.95; P < 0.001), hepatocellular carcinoma (HR = 0.59; 95% CI: 0.41–0.86; P = 0.007), upper-tract urothelial carcinoma (HR = 0.53; 95% CI: 0.29–0.97; P = 0.04), and bladder cancer (HR = 0.36; 95% CI: 0.18–0.72; P = 0.004). We also observed better outcome in OS among RAS inhibitor users with rectal/colorectal cancer (HR = 0.86; 95% CI: 0.68–1.08; P = 0.19), lung cancer (HR = 0.89; 95% CI: 0.76–1.05; P = 0.17), prostate cancer (HR = 0.85; 95% CI: 0.55–1.31; P = 0.45), glioblastoma (HR = 0.83; 95% CI: 0.47–1.47; P = 0.52), head and neck squamous cell carcinoma (HR = 0.38; 95% CI: 0.12–1.20; P = 0.10), oropharynx cancer (HR = 0.63; 95% CI: 0.38–1.04; P = 0.07), and melanoma (HR = 0.41; 95% CI: 0.10–1.68; P = 0.22).
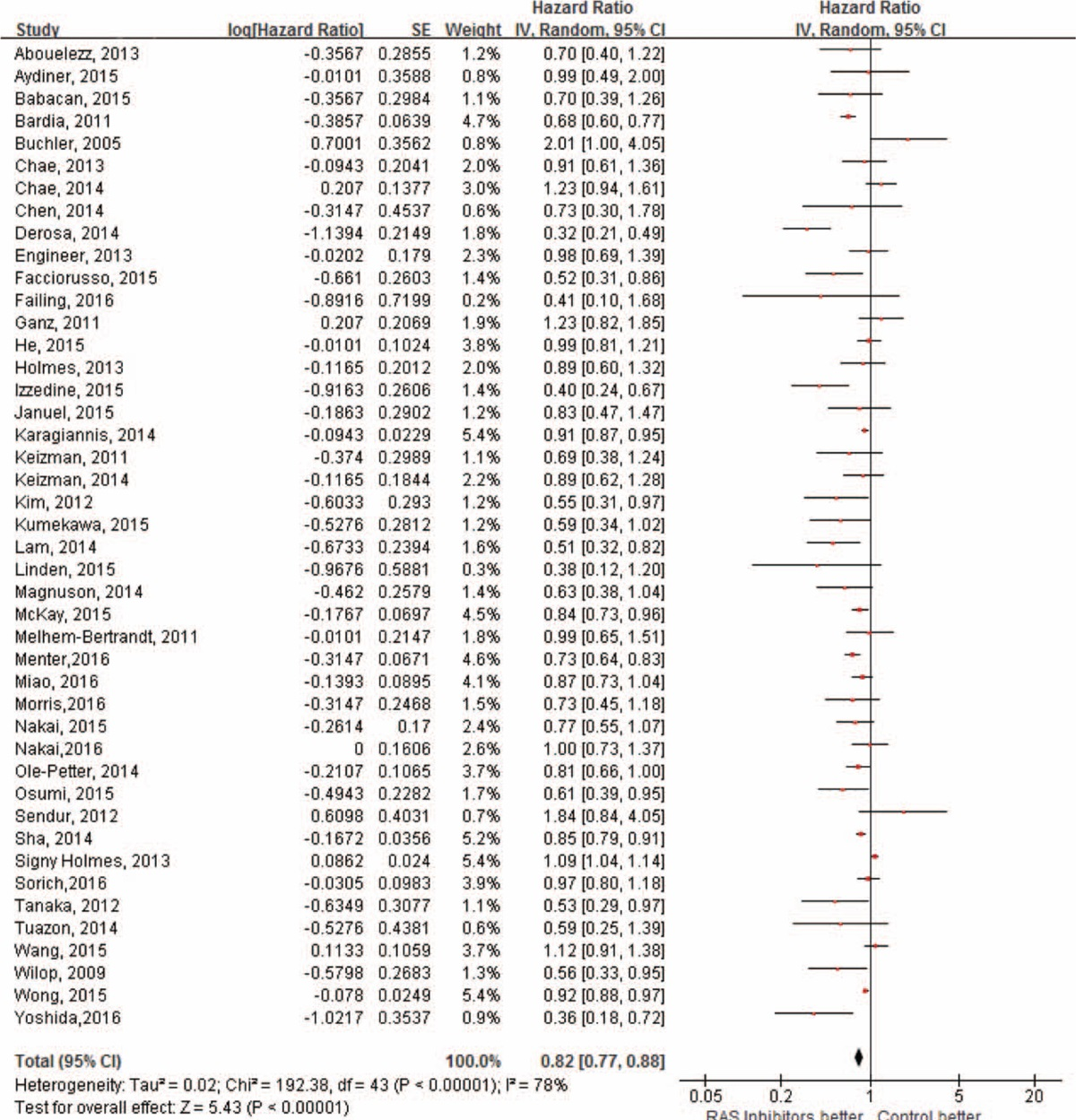
Forest plot for the association between renin–angiotensin system inhibitors and overall survival of cancer patients.
Targeting the renin-angiotensin system to improve cancer treatment: Implications for immunotherapy (link)
Renin-angiotensin system (RAS) inhibitors (RASi)—widely prescribed for the treatment of cardiovascular diseases—have considerable potential in oncology. Multiple clinical studies have revealed that RASi may have beneficial effects in a broad range of malignancies. The gain in survival is tumor type– and stage-dependent and ranged from 3 months (advanced NSCLC) to more than 25 months (metastatic RCC) in retrospective studies. However, response to RASi treatment may not only vary with tumor types but also depend on certain tumor characteristics, cancer treatment, and RASi type and dosing. More precisely, RCC, HCC, PDAC, glioblastoma, urinary tract cancer, and NSCLC seem to belong to the responsive tumor types, whereas breast cancer is rather unresponsive to RASi.
Blood pressure drugs lengthen survival in advanced kidney cancer (link)
Patients with advanced kidney cancer lived an average of seven months longer if they were taking a common type of high blood pressure medication during treatment, according to an analysis of clinical trials data presented by scientists from Dana-Farber Cancer Institute.
Patients who were on medications called angiotensin system inhibitors (ASIs), including angiotensin-converting-enzyme (ACE) inhibitor and angiotensin system blockers, commonly used to treat high blood pressure and other medical conditions survived an average of 26.68 months, compared with 17.05 months in those who did not receive the drugs.
Angiotensin II receptor blockers and risk of cancer in patients with systemic hypertension (link)
A nationwide population-based study was conducted to investigate the possible influence of ARBs on the occurrence of new cancers in patients with hypertension by using the Taiwan National Health Insurance database. A total of 109,002 patients with newly diagnosed hypertension were identified from a cohort database of 1 million individuals from January 1, 1998, to December 31, 2006. Among them, 40,124 (36.8%) had received ARBs for hypertension. The end point was the development of any type of cancer before the end of 2007. During an average of 5.7 ± 2.6 years of follow-up, a total of 9,067 cases of new cancer occurrence were observed. The log-rank test showed that the occurrence rate of newly diagnosed cancers in the subjects receiving ARBs was significantly lower than those receiving treatment without ARBs (ARBs vs controls 3,082 vs 5,985, p <0.001). After adjusting for age, gender, co-morbidities, and medications for hypertension control, ARB use was found to be independently associated with a decreased risk for cancer occurrence (hazard ratio 0.66, 95% confidence interval 0.63 to 0.68, p <0.001). In conclusion, long-term use of ARBs is associated with a lower incidence of cancer occurrence, thereby suggesting that ARBs may prevent cancer development.
ACE Inhibitors and ARBs
[Inhibitors of the renin-angiotensin system (RAS), particularly angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), are commonly used in the treatment of hypertension. ]
Is There a Link Between Blood Pressure Medication and Cancer -- Particularly Kidney Cancer? (link)
Among the patients taking ACE inhibitors, the risk of death from cancer was a third less than the risk for patients never treated with an ACE inhibitor. Women taking ACE inhibitors had only half the risk of cancer-related death -- and only one-third the risk of dying from a sex-specific cancer such as breast or ovarian disease.
Reid says that there are several theories about why ACE inhibitors are protective against cancer, but "I think the most likely explanation is that angiotensin II [the body substance that ACE inhibitors block] is known to stimulate cells to divide -- so blocking that action is protective," he says. "Additionally, it blocks [blood vessel growth], thus reducing blood supply."
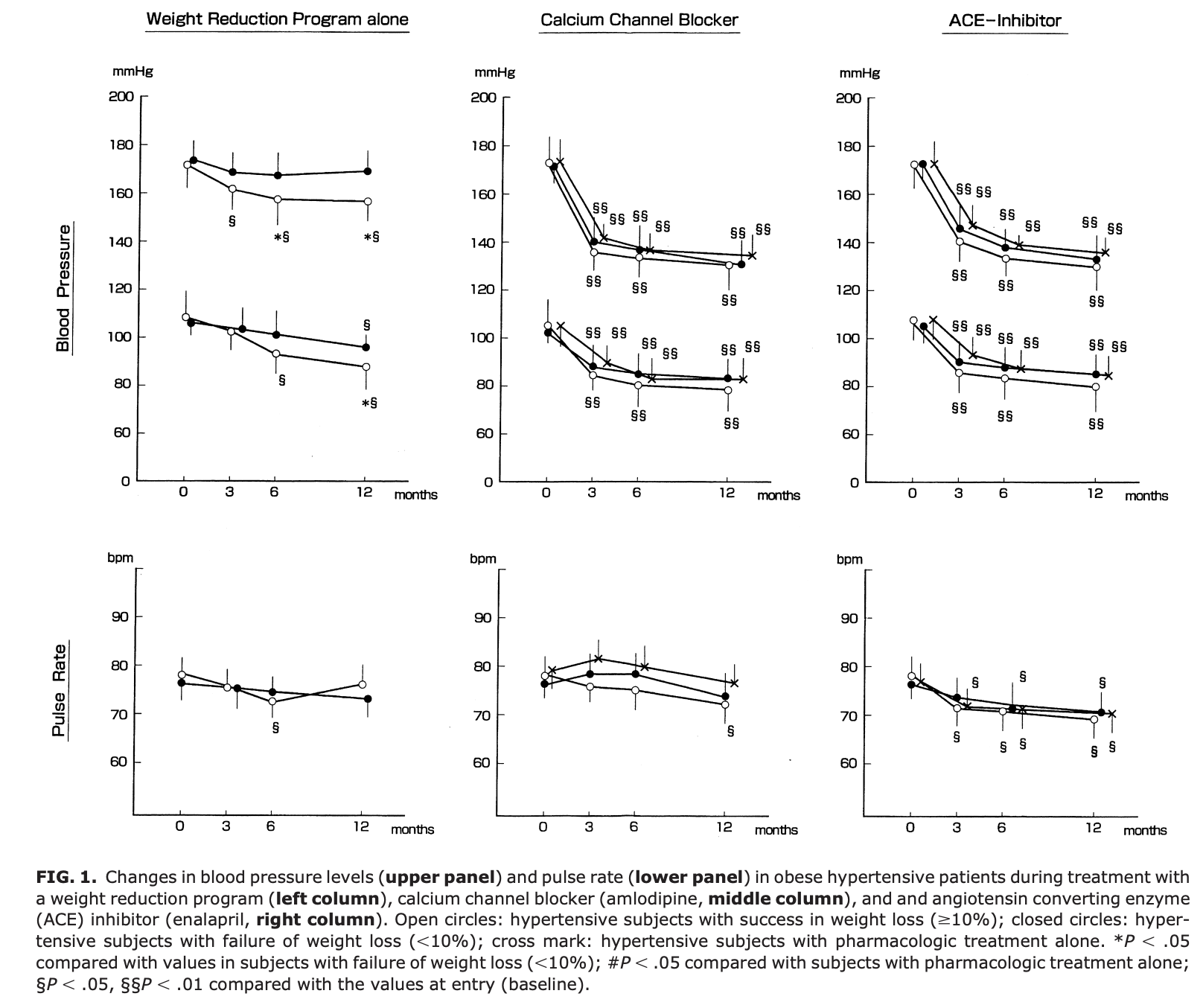
Weight Reduction and Pharmacologic Treatment in Obese Hypertensives (link)
[Human study.] A novel finding from this study is that ACE inhibition had a striking effect to lower plasma leptin. Suppression of sympathetic activity, insulinemia, and leptinemia appeared to play a role in the BP reduction accompanying weight loss. Angiotensin converting enzyme (ACE) inhibitor: enalapril.
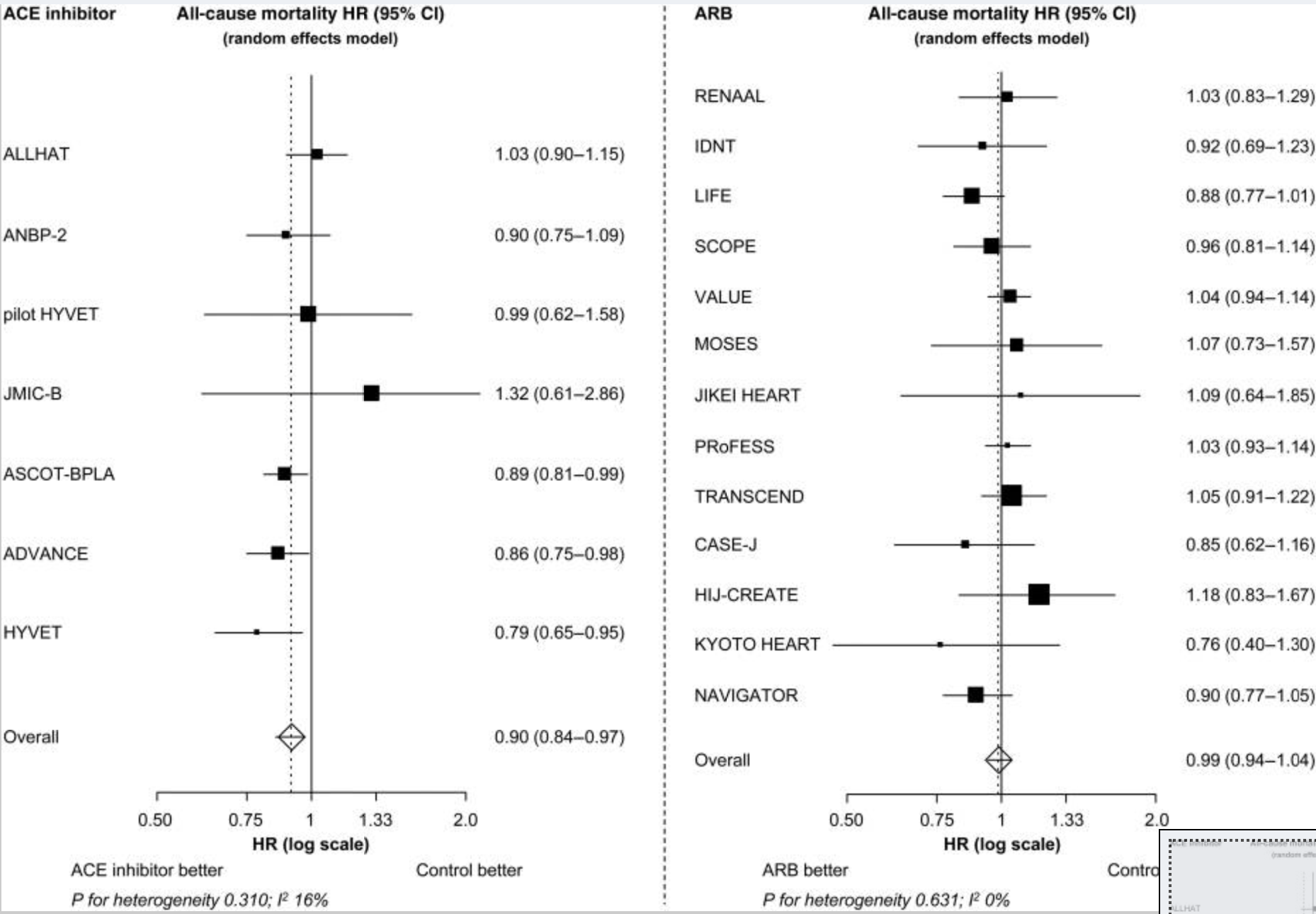
Angiotensin-converting enzyme inhibitors reduce mortality in hypertension: a meta-analysis of randomized clinical trials of renin–angiotensin–aldosterone system inhibitors involving 158 998 patients (link)
Renin–angiotensin–aldosterone system (RAAS) inhibitors are well established for the reduction in cardiovascular morbidity, but their impact on all-cause mortality in hypertensive patients is uncertain. Our objective was to analyse the effects of RAAS inhibitors as a class of drugs, as well as of angiotensin-converting enzyme (ACE) inhibitors and AT1 receptor blockers (ARBs) separately, on all-cause mortality.
Methods and results
We performed a pooled analysis of 20 cardiovascular morbidity–mortality trials. In each trial at least two-thirds of the patients had to be diagnosed with hypertension, according to the trial-specific definition, and randomized to treatment with an RAAS inhibitor or control treatment. The cohort included 158 998 patients (71 401 RAAS inhibitor; 87 597 control). The incidence of all-cause death was 20.9 and 23.3 per 1000 patient-years in patients randomized to RAAS inhibition and controls, respectively. Overall, RAAS inhibition was associated with a 5% reduction in all-cause mortality (HR: 0.95, 95% CI: 0.91–1.00, P= 0.032), and a 7% reduction in cardiovascular mortality (HR: 0.93, 95% CI: 0.88–0.99, P= 0.018). The observed treatment effect resulted entirely from the class of ACE inhibitors, which were associated with a significant 10% reduction in all-cause mortality (HR: 0.90, 95% CI: 0.84–0.97, P= 0.004), whereas no mortality reduction could be demonstrated with ARB treatment (HR: 0.99, 95% CI: 0.94–1.04, P= 0.683). This difference in treatment effect between ACE inhibitors and ARBs on all-cause mortality was statistically significant (P-value for heterogeneity 0.036).
Conclusion
In patients with hypertension, treatment with an ACE inhibitor results in a significant further reduction in all-cause mortality. Because of the high prevalence of hypertension, the widespread use of ACE inhibitors may result in an important gain in lives saved.
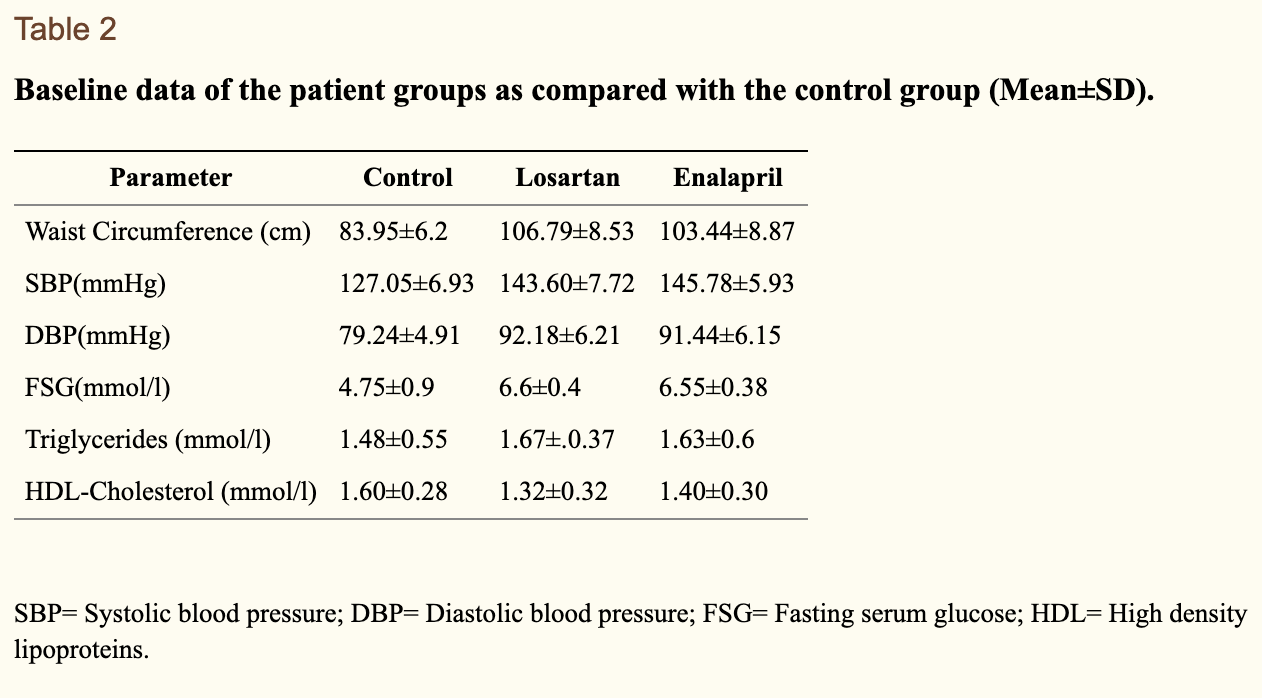
Effects of Losartan vs. Enalapril on the Markers of Metabolic Syndrome (link)
Both losartan and enalapril produced a significant reduction of markers of metabolic syndrome and may be regarded as effective drugs for treatment of hypertension in patients with markers of metabolic syndrome.


From rapalogs to anti-aging formula - Mikhail V. Blagosklonny (link)
Inhibitors of angiotensin II
Angiotensin II receptor blockers (ARB) such as Valsartan, Telmisartan, Losartan and angiotensin-converting enzyme (ACE) inhibitors such as Captopril, Lisinopril, Enalapril, Ramipril are widely used to treat hypertension. Hypertension is a clear-cut disease of hyperfunction. Angiotensin II, a hormone, is involved in age-related diseases in mammals [167, 168]. Disruption of the angiotensin II receptor increases longevity in mice [169]. Variations of the angiotensin II receptor gene are associated with longevity in humans [170]. Inhibitors of angiotensin II double lifespan of hypertensive rats [171, 172]. This dramatic (100%) increase is in part due to the anti-hypertensive effect. Yet, in healthy (those with normal blood pressure) rats, long-term treatment with enalapril decreases weight and prolongs life span dramatically [173]. In humans, inhibitors of angiotensin II prevent cardiac hypertrophy and organ fibrosis [168], [174], a hallmark of aging. In some studies, long-term use of ARBs was associated with a lower incidence of cancer [175]. Enalapril and perindopril did not decrease blood pressure in patients with normal blood pressure [176]. Importantly, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers are beneficial in normotensive atherosclerotic patients [177].
ACE inhibitors increase the lifespan in rodents with normal blood pressure [132–134], thereby acting as anti-aging drugs.
Angiotensin Converting Enzyme (ACE) Inhibitor Extends Caenorhabditis elegans Life Span (link)
Lisinopril Preserves Physical Resilience and Extends Life Span in a Genotype-Specific Manner in Drosophila melanogaster (link)
Long term treatment with ACE inhibitor enalapril decreases body weight gain and increases life span in rats (link)
Renin-angiotensin system is involved in homeostasis processes linked to renal and cardiovascular system and recently has been linked to metabolic syndrome. We analyzed the influence of long term angiotensin I converting enzyme (ACE) inhibitor enalapril treatment in normotensive adult Wistar rats fed with standard or palatable hyperlipidic diets. Our results show that long term enalapril treatment decreases absolute food intake, serum leptin concentration and body weight gain. Moreover, in adipose tissue, enalapril treatment led to decreased ACE activity, enhanced the expression of peroxisome proliferator activated receptor gamma, adiponectin, hormone-sensitive lipase, fatty acid synthase, catalase and superoxide dismutase resulting in prolonged life span. On the other hand, the ACE inhibitor was not able to improve the transport of leptin through the blood brain barrier or to alter the sensitivity of this hormone in the central nervous system. The effect of enalapril in decreasing body weight gain was also observed in older rats. In summary, these results extend our previous findings and corroborate data from the literature regarding the beneficial metabolic effects of enalapril and show for the first time that this ACE inhibitor prolongs life span in rats also fed with palatable hyperlipidic diet, an action probably correlated with adipose tissue metabolic modulation and body weight reduction.
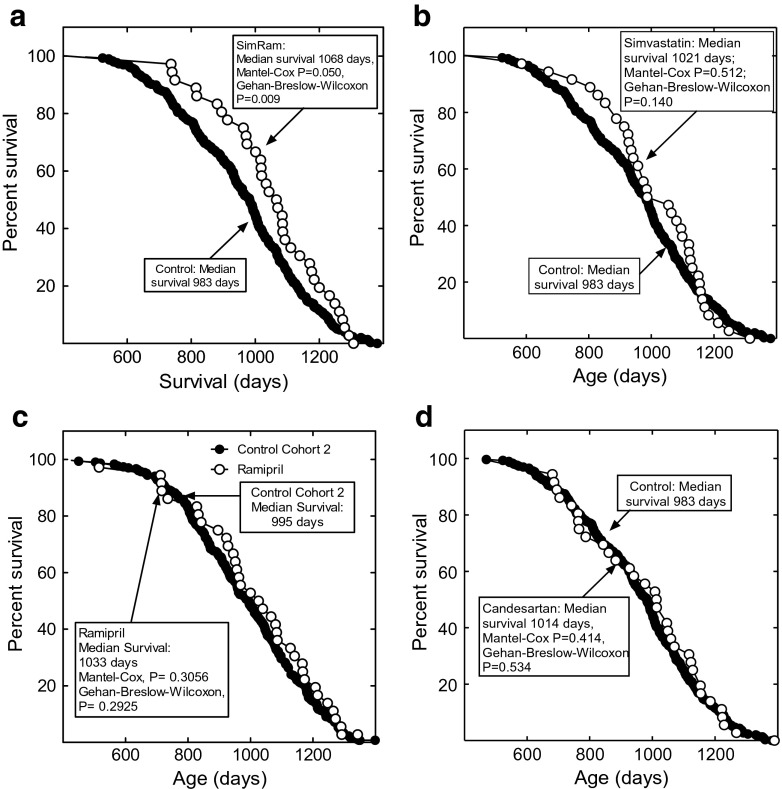
Combined statin and angiotensin-converting enzyme (ACE) inhibitor treatment increases the lifespan of long-lived F1 male mice
Statins, such as simvastatin, and ACE inhibitors (ACEis), such as ramipril, are standard therapies for the prevention and treatment of cardiovascular diseases. These types of drugs are commonly administered together. More recently, angiotensin II type 1 receptor (AT1R) antagonists, such as candesartan cilexetil (candesartan), have been used in the place of, or in combination with, ACEis. Here, we investigated the effects of simvastatin and ramipril single and combination therapy, and candesartan treatment on the lifespan of isocalorically fed, long-lived, B6C3F1 mice. Males were used for their relative endocrine simplicity and to minimize animal usage. The drugs were administered daily in food. The simvastatin and ramipril combination therapy significantly increased the mean and median lifespan by 9 %. In contrast, simvastatin, ramipril, or candesartan monotherapy was ineffective. All groups consumed the same number of calories. Simvastatin, alone or administered with ramipril, decreased body weight without changing caloric consumption, suggesting it may alter energy utilization in mice. Combination therapy elevated serum triglyceride and glucose levels, consistent with altered energy homeostasis. Few significant or consistent differences were found in mortality-associated pathologies among the groups. Simvastatin treatment did not reduce normal serum cholesterol or lipid levels in these mice, suggesting that the longevity effects may stem from the pleiotropic, non-cholesterol-related, effects of statins. Together, the results suggest that statins and ACEis together may enhance mouse longevity. Statins and ACE inhibitors are generally well-tolerated, and in combination, they have been shown to increase the lifespan of normotensive, normocholesterolemic humans.
Protective effect of long-term angiotensin II inhibition, 2007
Experimental studies indicate that angiotensin II (ANG II) through its type 1 receptor (AT1)
promotes cardiovascular hypertrophy and fibrosis. Therefore, the aim of this study was to analyze whether chronic long-term inhibition of the renin-angiotensin system (RAS) can prevent most of the deleterious effects due to aging in the cardiovascular system of the normal
rat. The main objective was to compare two strategies of ANG II blockade: a converting enzyme inhibitor (CEI) and an AT1 receptor blocker (AT1RB). A control group remained untreated; treatment was initiated 2 wk after weaning. A CEI, enalapril (10 mgkg1 day1), or an AT1RB, losartan (30 mgkg1 day1 ), was used to inhibit the RAS. Systolic blood pressure, body weight, and water and food intake were recorded over the whole experimental period. Heart, aorta, and
mesenteric artery weight as well as histological analysis of cardiovascular structure were performed at 6 and 18 mo. Twenty animals in each of the three experimental groups were allowed to die spontaneously. The results demonstrated a significant protective effect on the
function and structure of the cardiovascular system in all treated animals. Changes observed at 18 mo of age in the hearts and aortas were quite significant, but each treatment completely abolished this deterioration. The similarity between the results detected with either enalapril or losartan treatment clearly indicates that most of the effects are exerted through AT1 receptors. An outstanding finding was the significant and similar prolongation of life span in both groups of treated animals compared with untreated control animals.


Comments