Statin
In Renal Cell Carcinoma (RCC), statin use was associated with marked improvements in cancer-specific survival (pooled HR 0.67, 95% CI 0.47-0.94) and overall survival (pooled HR 0.74, 95% CI 0.63-0.88)
Statins inhibit the proliferation of human RCC cells via down-regulation of the survivin through IGF-1 Signaling.
Simvastatin Inhibits Renal Cancer Cell Growth and Metastasis via AKT/mTOR, ERK and JAK2/STAT3 Pathway.
In Polycythemia Vera (PV), use of statins was associated with improved survival and decreased risk of thrombosis.
Exposure to statins in PV had an 84% decrease in odds of needing a higher intensity of phelebotomies.
Statin use in cancer patients is associated with reduced cancer-related mortality across many cancer types.
Statins lower HS-CRP (inflammation).
Cholesterol Drugs May Boost Kidney Cancer Survival, 2013
Study finds statin medications tied to lower death risk after nearly 4 years of follow-up
Statins -- drugs such as Crestor, Lipitor, Pravachol and Zocor -- have anti-inflammatory and cell self-destruction properties, and previous research has shown that these drugs may lower the risk of developing some types of cancer. The new research, presented Tuesday at the annual meeting of the American Urological Association in San Diego, suggests that the drugs might fight kidney cancer.
Over three years, 10 percent of the patients who took statins died of their cancer, compared with 17 percent of those who did not take this type of drug.
Statin use and kidney cancer survival outcomes A systematic review and meta-analysis. (link)
We identified 12 studies meeting inclusion criteria and summarized data from 18,105 patients. No study was considered to be at high risk of bias. Statin use was not significantly associated with recurrence-free survival (pooled HR 0.97, 95% CI 0.89-1.06) or progression-free survival (pooled HR 0.92, 95% CI 0.51-1.65); however, statin use was associated with marked improvements in cancer-specific survival (pooled HR 0.67, 95% CI 0.47-0.94) and overall survival (pooled HR 0.74, 95% CI 0.63-0.88). There was no strong evidence of publication bias for any outcome.
Statin Use is Associated with Improved Survival in Patients Undergoing Surgery for Renal Cell Carcinoma, 2015
Data were analyzed from 916 RCC patients who underwent radical or partial nephrectomy at Vanderbilt University in Nashville, Tenn., from 2000 to 2010. The median follow-up was 42.5 months. The 3-year overall and disease-specific survival rates were 83% and 91%, respectively, for statin users versus 77% and 84% for non-users. Urologic Oncology (2015;33:e11-17).
Statin Inhibits the Proliferation of Human Renal Cancer Cells via Down-regulation of the Sruvivin through IGF-1 Signaling, 2010
In Caki1 cells, simvastatin significantly inhibited cell proliferation, and gene expression levels of IGF-1R were significantly decreased by simvastatin. These were not significant in KMRC1 cells.
Statins are able to induce variable degrees of antibacterial activity with atorvastatin, and simvastatin being the more potent than rosuvastatin. Methicillin-sensitive staphylococcus aureus (MSSA), methicillin-resistant staphylococcus aureus (MRSA), vancomycin-susceptible enterococci (VSE), vancomycin-resistant enterococcus (VRE), acinetobacter baumannii, staphylococcus epidermidis, and enterobacter aerogenes, were more sensitive to both atorvastatin, and simvastatin compared to rosuvastatin. On the other hand, escherichia coli, proteus mirabilis, and enterobacter cloacae were more sensitive to atorvastatin compared to both simvastatin and rosuvastatin.
Statin therapy in the treatment of active cancer: A systematic review and meta-analysis of randomized controlled trials, 2018
[not RCC] [Stations show promise in RCTs but the CIs are too wide]
Ten studies with 1,881 individuals were included with 1,572 deaths and a median follow-up of 23 months. All trials included patients with advanced (stage 3 or higher) disease. There was minimal between-study statistical heterogeneity (I2 = 1.8%, for OS; I2 = 0%, for PFS). The pooled HR for overall survival in patients randomized to statins plus standard anti-cancer therapy versus standard therapy alone was 0.94 (95% CI, 0.85 to 1.04). In the 9 studies that reported progression-free survival (1,798 participants), the pooled HR for statin plus standard therapy versus standard therapy alone was 0.97 (95% CI, 0.87 to 1.07).
The PI3K/AKT pathway is modestly mutated but highly activated in RCC, representing a promising drug target. Simvastatin and atorvastatin inhibited AKT phosphorylation and were cytotoxic starting at 10 μM in vivo.
Simvastatin Inhibits Renal Cancer Cell Growth and Metastasis via AKT/mTOR, ERK and JAK2/STAT3 Pathway, 2013
Statins and survival outcomes in patients with metastatic renal cell carcinoma (link)
We identified 4736 patients treated with sunitinib (n = 1059), sorafenib (n = 772), axitinib (n = 896), temsirolimus (n = 457), temsirolimus + interferon (IFN)-α (n = 208), bevacizumab + temsirolimus (n = 393), bevacizumab + IFN-α (n = 391) or IFN-α (n = 560), of whom 511 were statin users. Overall, statin users demonstrated an improved overall survival (OS) compared to non-users (25.6 versus 18.9 months, adjusted hazard ratio [aHR] 0.801, 95% confidence interval [CI] 0.659–0.972, p = 0.025). When stratified by therapy type, a benefit in OS was demonstrated in statin users compared to non-users in individuals receiving therapy targeting vascular endothelial growth factor (28.4 versus 22.2 months, aHR 0.749, 95% CI 0.584–0.961, p = 0.023) or mammalian target of rapamycin (18.6 versus 14.0 months, aHR 0.657, 95% CI 0.445–0.972, p = 0.035) but not in those receiving IFN-α (15.6 versus 14.8 months, aHR 1.292, 95% CI 0.703–2.275, p = 0.410). Adverse events were similar between users and non-users.
Statin Use and Reduced Cancer-Related Mortality, 2012
Cholesterol is a fundamental structural component of mammalian cell membranes and is essential for cellular proliferation.1,2 Statins inhibit the production of endogenous cholesterol3 and block protein prenylation, and statin use may therefore influence cell proliferation and migration.4,5
Cancer-cell proliferation is seen clinically as cancer growth and metastasis, and it ultimately results in the death of the patient. A reduction in the availability of cholesterol could lead to decreased proliferation and migration of cancer cells.6,7 Also, a reduction in the downstream products in the mevalonate pathway due to statin use has been associated with several potential anticancer properties8-12 and a reduced risk of cancer recurrence.13,14 At the cellular level, statins have been linked to the halting of cell-cycle progression and to increased radiosensitization in cancer cells.10,15,16 Thus, regular statin use before and after a diagnosis of cancer could theoretically reduce cancer-related mortality. In large-scale trials of statins to reduce the risk of cardiovascular disease among persons without cancer, statin use did not influence the incidence of cancer or related mortality.17,18

Use of Statins, Survival and Incidence of Thrombosis Among Older Adults with Polycythemia Vera: A Population-Based Study, 2018
Introduction: Patients with myeloproliferative neoplasms (MPN) are at increased risk for cardiovascular morbidity and mortality with the highest risk among polycythemia vera (PV) patients. MPN guidelines recommend aggressive management of cardiovascular risk factors which may include statin administration. Statins can induce apoptosis and inhibit JAK2-V617F-dependent cell growth in vitro, as well as inhibit erythropoietin-independent erythroid colony formation of primary cells from patients with MPN. JAK2-V617F mutation is a common somatic event occurring in over 95% of PV patients. There is no published data regarding the impact of statins on the outcomes of PV patients.
Methods: Using the Surveillance, Epidemiology, and End Results-Medicare linked database, we assembled a population-based cohort of older adults who were diagnosed with PV during 2007-2013 and fulfilled the following eligibility criteria: 1) aged 66-99 years at diagnosis; 2) had continuous Medicare Parts A and B coverage and not enrolled in health maintenance organizations from 12 months before diagnosis to death or the end of study (12/31/2014), whichever was earlier (i.e., the end of follow up); and 3) continuously enrolled in Medicare Part D from 6 months before diagnosis to end of follow up. Patients were identified as statin users if they had any prescription for statins in Part D claims from their PV diagnosis to the end of follow up. For both statins and hydroxyurea (HU, a common treatment of PV), percentage of days covered (PDC) was defined as the percentage of days from diagnosis to the end of follow-up covered by respective prescriptions. We further classifed statins as lipophilic or hydrophilic. Therapeutic phlebotomy intensity was defined based on the number of phlebotomies per year (>0 but < 3: low intensity, ≥3: high intensity).
Log-rank tests were used to compare Kaplan-Meier (K-M) curves between statin users and non-users with regard to overall survival and risk of thrombosis after PV diagnosis. Multivariate Cox proportional hazards models were used to assess the impact of statins use on overall survival. Multivariate competing risk models with death as a competing risk were utilized to evaluate the relationship between statin PDC and thrombosis risk. All multivariate models adjusted for HU PDC, phlebotomy intensity, age, sex, race, state buy-in, influenza vaccination 12 months prior to PV diagnosis (a marker for healthcare access), disability status, modified Elixhauser score for comorbidities, and previous thrombosis. All statistical tests were two-sided and conducted with SAS (Version 9.4).
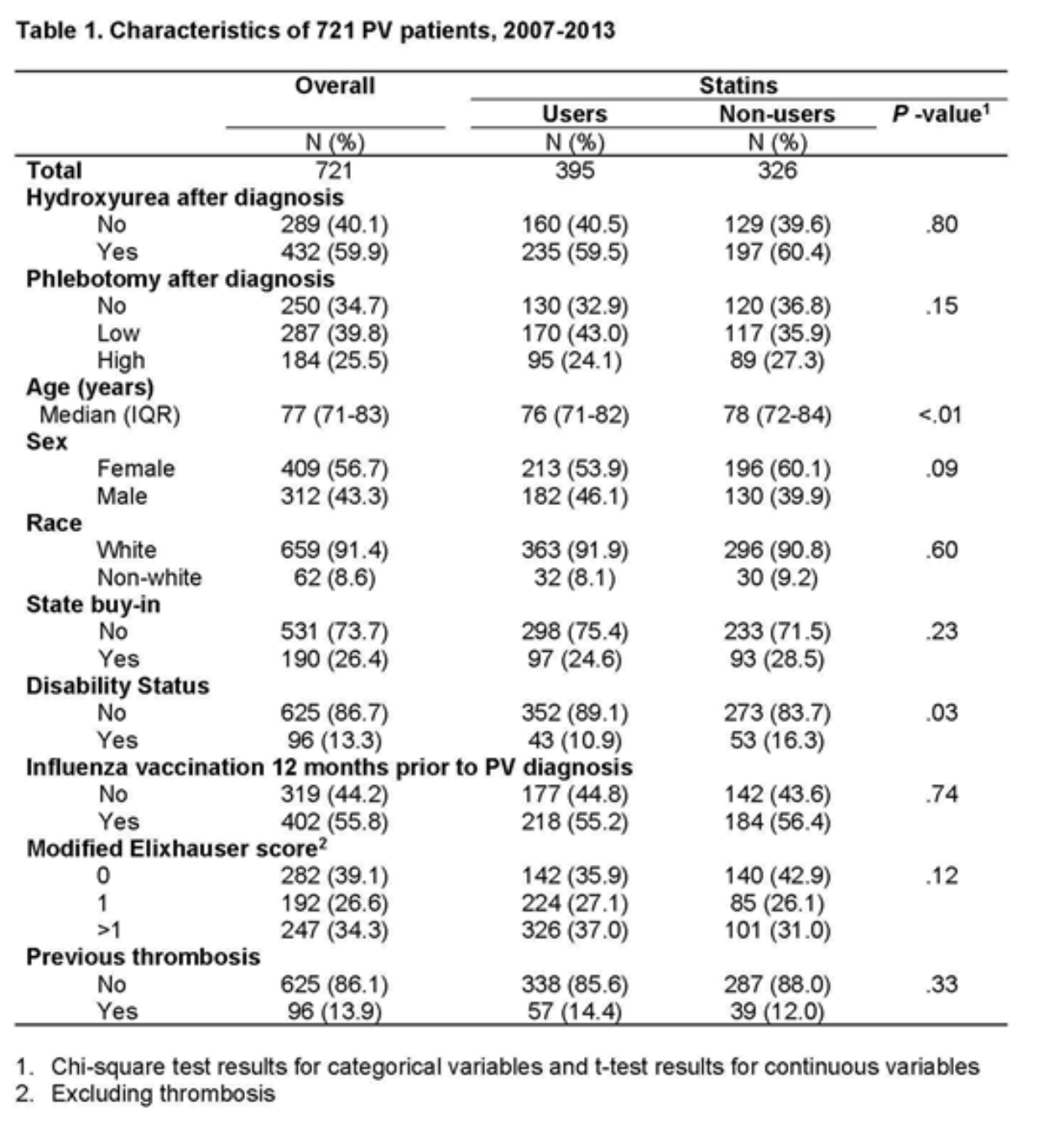
Results: Of the 721 PV patients included in this study (median age = 77 years, interquartile range: 71-83 years), a majority were female (56.7%) and white (91.4%) (Table 1). About 55% of patients used statins, and 72.9% of the 395 users (n=288) started before PV diagnosis. The median statin PDC was 67% among statin users, and most patients (n=361, 91.4%) used only one type of statins (lipophilic: n=295; hydrophilic: n=65).
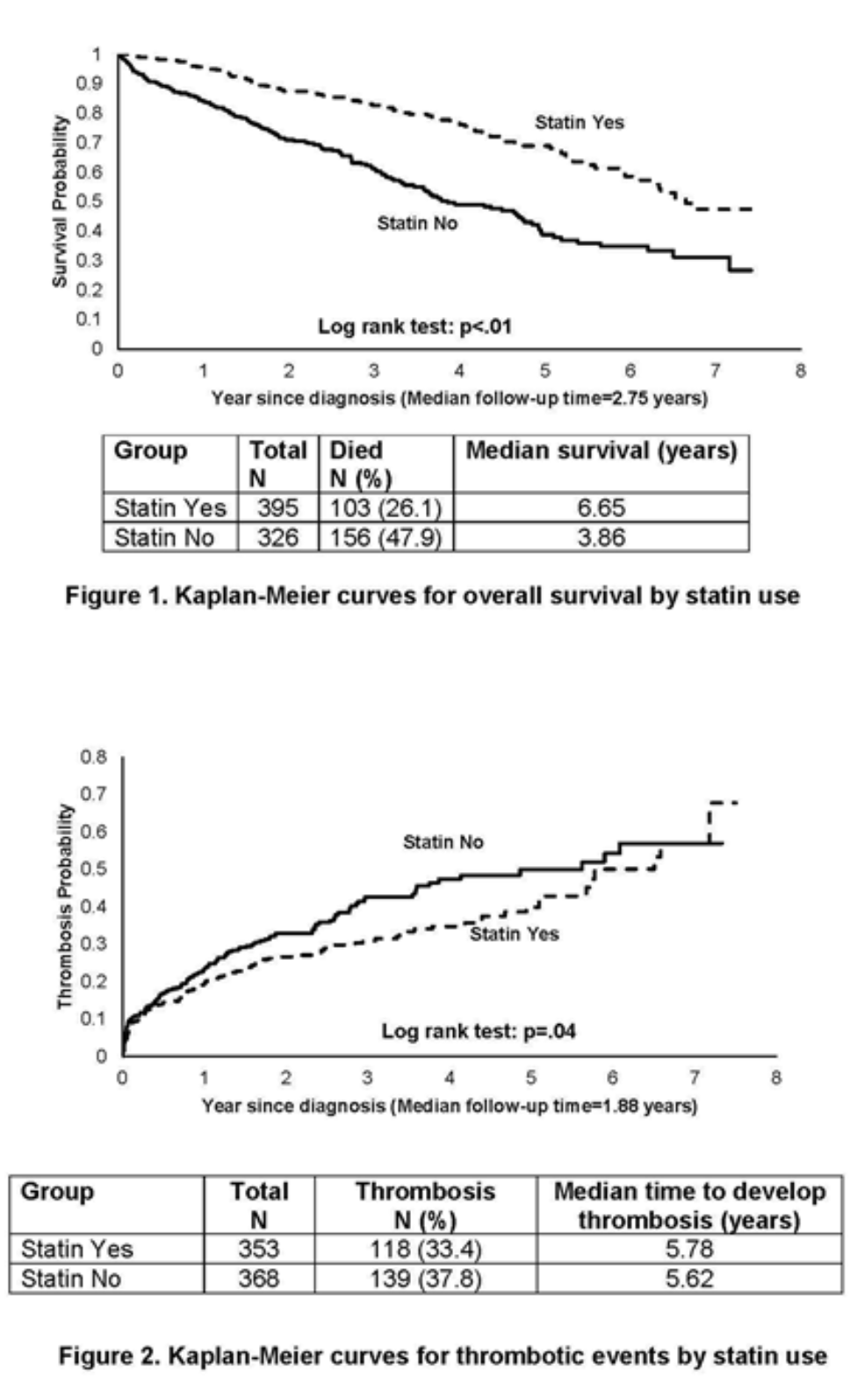
With a median follow-up of 2.75 years, 26.1% (n=103) of statin users and 47.9% (n=156) of statin non-users died; users (median: 6.65 years) had a significantly better overall survival than non-users (median: 3.86 years Log rank test, p<.01) (Figure 1). Adjusting for covariates, every 10% of statin PDC after PV diagnosis was associated with an 18% lower risk of all cause mortality (95% confidence interval [CI]: 0.78-0.86; p<.01). The magnitude of association was very similar for lipophilic and hydrophilic statins.
Thrombosis after PV diagnosis was recorded in 257 (35.6%) patients, 177 of whom had arterial thrombosis. One hundred and eighteen (33.4%) statin users and 139 (37.8%) non-users had thrombosis after PV diagnosis. The risk of thrombosis was significantly lower in statin users than in non-users based on Log-rank test (p=.04) (Figure 2) and multivariable competing risk model (every 10% of statin PDC was associated with a 5% lower risk of thrombosis (95% CI: 0.92-0.99; p<.01). Subgroup analyses for lipophilic and hydrophilic statins generated almost identifical results.
Sensitivity analyses that only included patients who started using statins after PV diagnosis revealed similar findings pertaining to both survival and thrombosis.
Conclusions: In this large population-based cohort study of older adults with PV, use of statins was associated with improved survival and decreased risk of thrombosis.
A remarkable hematological and molecular response pattern in a patient with polycythemia vera during combination therapy with simvastatin and alendronate
We report a 57-year old man with polycythemia vera, who had a remarkable hematological and molecular response during treatment with simvastatin and alendronate. The patient was treated with this combination for 56 months, and during this period the patient has been in complete hematological remission. The JAK2-V617F allele burden has dropped from 64% to sustained values below 20%, and follow-up bone marrow biopsies have revealed no change in PV features, without any regular cytoreductive treatment.
The impact of statins on the intensity of phlebotomies in polycythemia vera, 2020
Dear Editor,
The CYTO-PV study demonstrated that polycythemia vera (PV) patients who maintained a target hematocrit (HCT) of < 45% had a lower rate of adverse cardiovascular events [1]. Therefore, all PV patients are phlebotomized until the target HCT is reached [2]. Statins have been suggested for the treatment of PV [3], as they reduce JAK2 localization to lipid rafts, downregulate JAK2/STAT5 activation in JAK2-dependent cell lines, and inhibit JAK2-dependent cell growth [4]. Here, we investigated whether concomitant treatment with statins in PV patients might reduce the number of phlebotomies (PHLs).
This was a retrospective, multicenter study, conducted at three community hospitals in Croatia. PV was diagnosed according to current WHO 2016 criteria [5]. Baseline demographic, clinical, and laboratory data was collected, as well as the number of PHLs needed to achieve the target HCT. PHLs were performed in a similar manner in all three study institutions; once- or twice-weekly, with 350–450 mL of blood drawn per PHL. Statistical analyses were performed with the MedCalc software®. Data was non-normally distributed so we used non-parametric tests. Categorical variables were compared using the χ2 test, and the differences between independent samples were assessed with Mann-Whitney U test. Logistic regression analysis was used to evaluate the potential impact of statins on the number of PHLs. Significant p value was set at < 0.050.
We included 103 JAK2-positive PV patients; 30 (29.1%) used statins, and 79 (76.7%) reached the target HCT. Statin users and non-statin users were equally balanced; there was no difference according to sex, age, blood counts, high-risk disease, hydroxycarbamide treatment, and the median number of PHLs needed to achieve the target HCT, as shown in Table 1. However, the proportion of patients who needed a higher intensity of PHLs (˃ 3) was higher in the non-statin group (72% vs 44%, respectively; p = 0.016). These patients were predominantly male (p = 0.002), with higher hemoglobin (p < 0.001) and HCT (p = 0.031), and were more likely to need hydroxycarbamide (p = 0.004). In the multivariate regression model, the higher intensity of PHLs (> 3) was independently and inversely associated with statin exposure (OR 0.16, 95% CI 0.04–0.62, p = 0.008), when adjusted for age (OR 0.97, 95% CI 0.90–1.03, p = 0.354), female sex (OR 0.16, 95% CI 0.04–0.56, p = 0.004), hydroxycarbamide treatment (OR 0.14, 95% CI 0.03–0.62, p = 0.009), and baseline HCT (OR 0.98, 95% CI 0.81–1.18, p = 0.879).
Exposure to statins in our study had an 84% decrease in odds of needing a higher intensity of PHLs, which indicates the in vivo potential of statins to inhibit the JAK2-dependent cell growth. These observations might have useful clinical implications, especially for patients with hydroxycarbamide intolerance/resistance [6], and for those who cannot tolerate PHLs [7], as well as for patients for whom a rapid control of HCT is warranted. Limitations of this study are its retrospective design, small number of patients, and the variable intensities of PHLs. Nevertheless, it represents real-world data that clearly reflects the management patterns in a community setting. The potential impact of statins on the intensity of PHLs needs to be confirmed in larger studies, preferentially in a randomized trial.
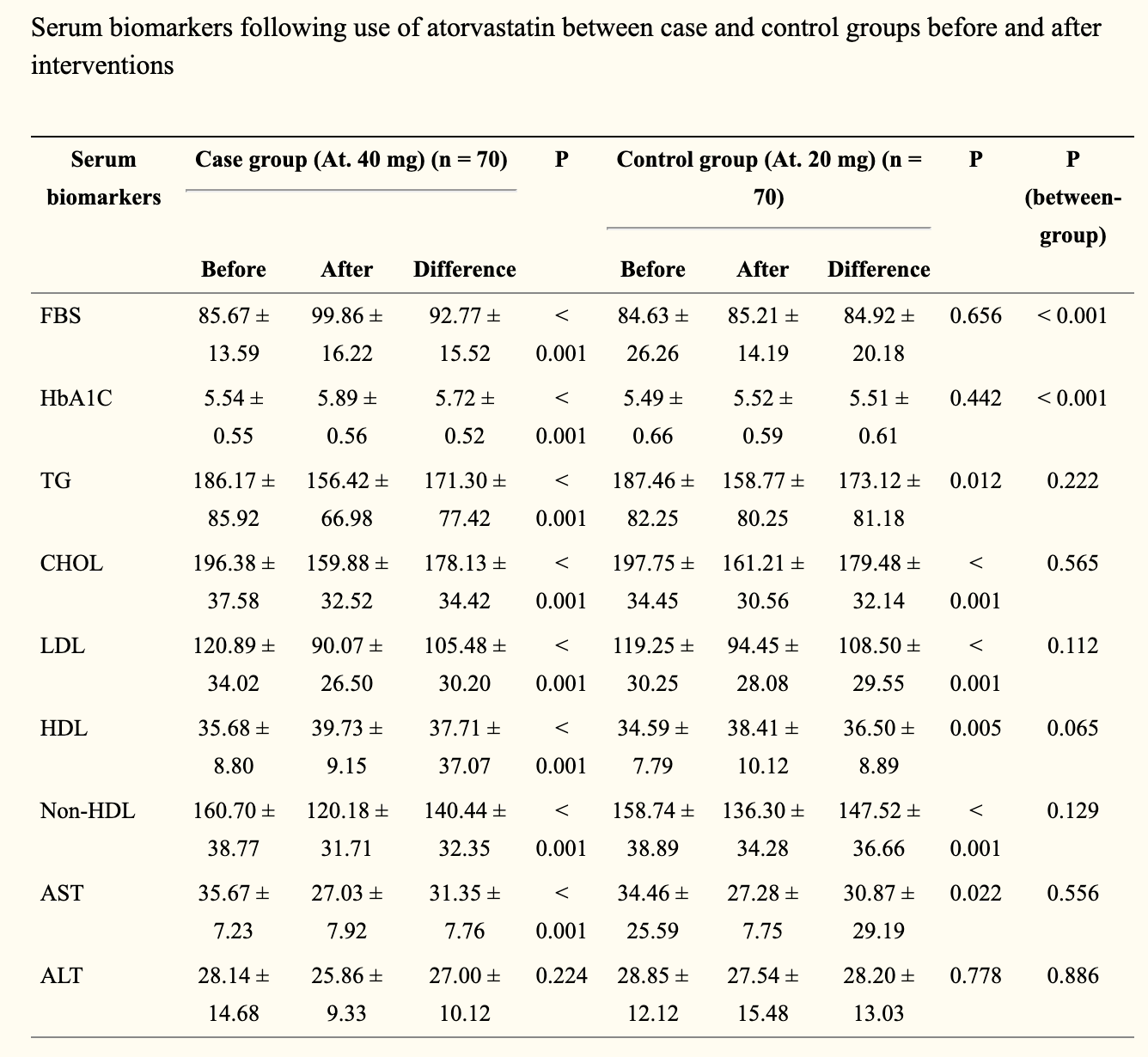
The effects of different doses of atorvastatin on serum lipid profile, glycemic control, and liver enzymes in patients with ischemic cerebrovascular accident
A significant reduction was revealed in serum triglyceride, total cholesterol, low-density lipoprotein, non-high-density lipoprotein (HDL) cholesterol, and also aspartate aminotransferase levels as well as a significant increase in serum HDL level following administration of atorvastatin in both case and control groups who received the atorvastatin 40 mg/day and 20 mg/day, respectively (all P < 0.050). Although a significant increase in fasting blood sugar and hemoglobin A1c was observed in the case group received atorvastatin 40 mg/day (both P < 0.001), but this elevation was not occurred in another group treated with lower dose of the drug (both P > 0.050).
Statins decrease mean platelet volume (MPV) irrespective of cholesterol lowering effect.
One hundred and forty five patients were retrospectively included. Atorvastatin and rosuvastatin were also compared in respect to effects on MPV. Statins significantly reduce MPV irrespective of cholesterol levels, and atorvastatin and rosuvastatin have comparable effects in this regard.
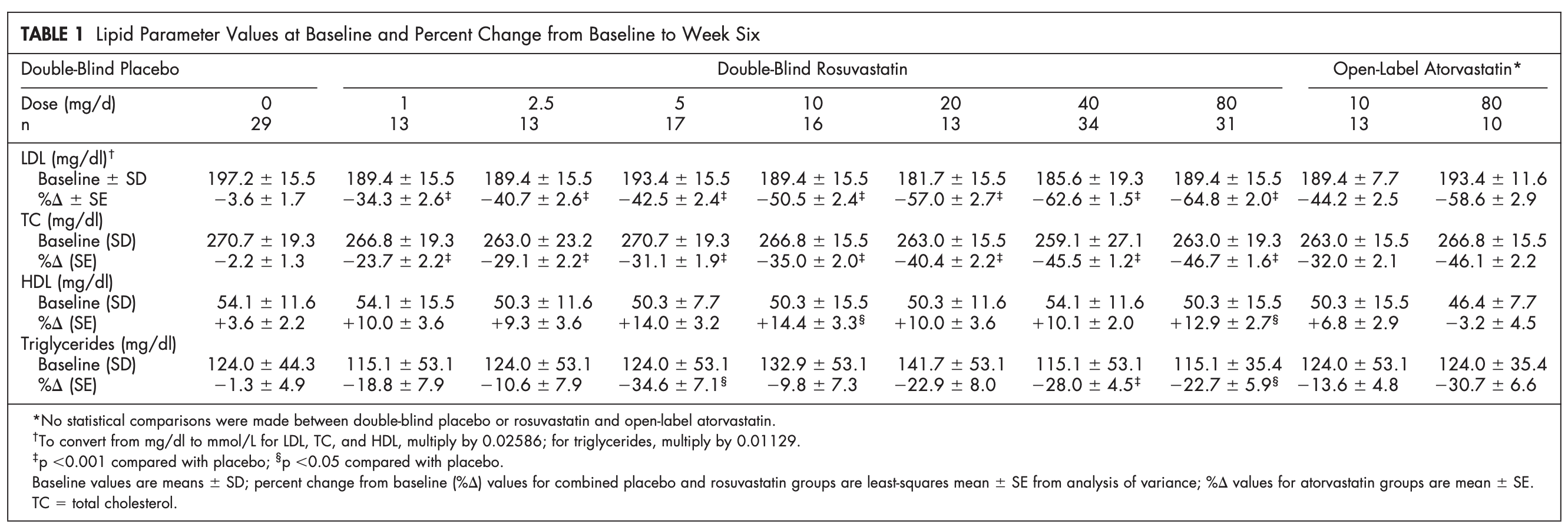
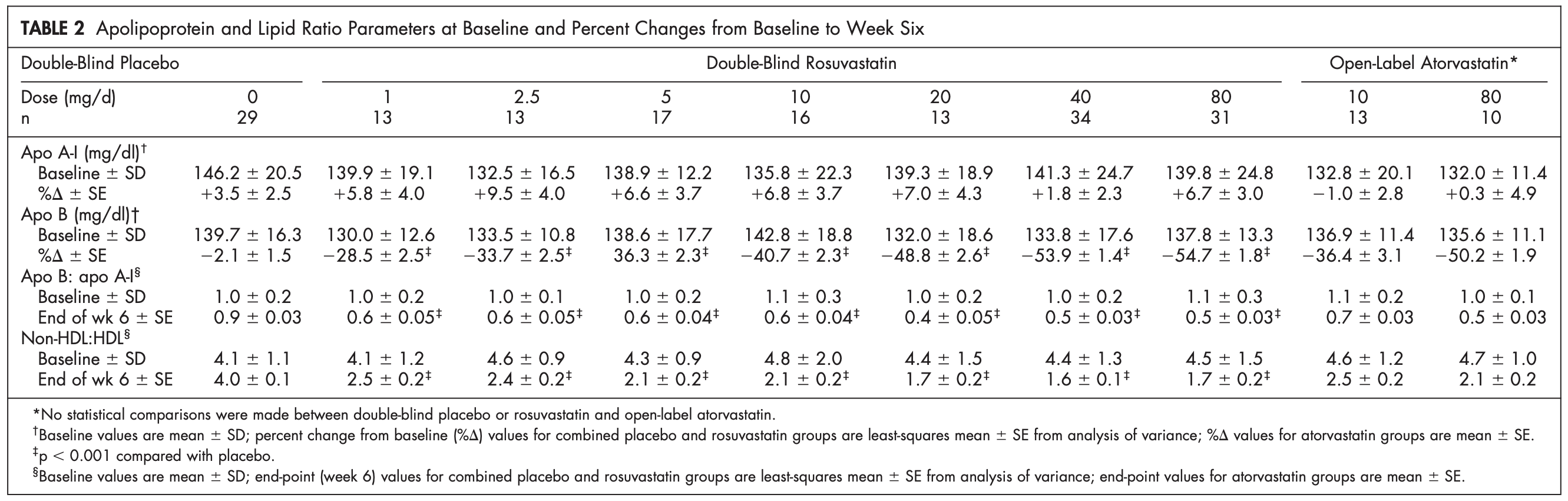
Review of efficacy of rosuvastatin 5 mg (2005)
The prevalence of coronary heart disease (CHD) has been increasing in the past few decades in Japan, as it has in industrialised countries worldwide. CHD risk can be substantially reduced by lowering low-density lipoprotein cholesterol (LDL-C) in patients with dyslipidaemia. Statins are highly effective for this indication, but many patients treated with these drugs still do not meet their treatment goals, often because clinicians fail to titrate these patients to a higher, potentially more effective, dose. Thus, there is a need for more effective agents that can help patients reach their goals at starting doses. This paper reviews key clinical results for a new agent, rosuvastatin. The data show that rosuvastatin 5 mg is highly effective in lowering LDL-C to recommended levels for most patients (mean reductions ranging from 42 to 52%). In addition, rosuvastatin 5 mg effectively lowers triglycerides (-16%), total cholesterol (-30%), non-high-density lipoprotein cholesterol (non-HDL-C; -38%) and apolipoprotein (apo) B levels (-33%) and increases HDL-C (+8.2-13%) in a wide range of patients with hypercholesterolaemia, including the elderly, obese patients, postmenopausal women and patients with hypertension, CHD, diabetes and metabolic syndrome. The 5-mg dose of rosuvastatin dose also produces greater reductions in LDL-C and larger increases in HDL-C than recommended initial doses of atorvastatin, simvastatin or pravastatin (for LDL-C reductions, p <0.001 vs. atorvastatin 10 mg, simvastatin 20 mg and pravastatin 20 mg; for HDL-C elevations, p <0.01 vs. atorvastatin 10 mg). These results demonstrate that rosuvastatin 5 mg produces favourable effects on the lipid profile and helps more patients achieve LDL-C goals than comparator statins.
Consumer Confusion about CHOLESTEROL and STATIN DRUGS (site:lifeextension.com)
Newer Trials Show Reduced Mortality
But statin critics may be overlooking newer studies that are showing meaningful mortality benefits. One large-scale meta-analysis published in 2016 showed that statins were significantly more effective for patients in reducing the odds of dying from coronary heart disease and from any cause, compared to control groups. Specifically, statin users had 31% lower odds of dying from coronary heart disease and 16% lower odds of dying from any cause, compared to controls.
20-Year Study Yields Robust Mortality Benefit
At the end of the 20-year follow-up, an analysis was done comparing the placebo group to men with LDL >= 190 mg/dL and originally assigned to the pravastatin group in the initial trial. Here are the findings over this 20-year period:
• The risk of coronary heart disease mortality was reduced by 28% in pravastatin drug users,
• There was a 19% reduced risk of major adverse cardiovascular events (defined as the composite of cardiovascular death, non-fatal heart attack, and non-fatal stroke), and
• Cardiovascular death was reduced by 25% and all-cause mortality by 18% respectively, in people remaining on pravastatin over this 20-year period.
In the participants whose LDL was lower than 190 mg/dL, deaths from all causes including cardiovascular disease were also lower in the pravastatin
group compared to the placebo group. The participants with LDL>=190 mg/dL had greater reductions in cardiovascular and all-cause mortality from pravastatin treatment compared to placebo. The average LDL cholesterol level dropped by 23.3% from its baseline value in the treatment group of those with LDL >=190 mg/dL.
This 23.3% reduction is still a considerable distance from what is generally accepted as a healthy LDL range, which is below 100 mg/dL for primary prevention of cardiovascular disease in people with low risk.
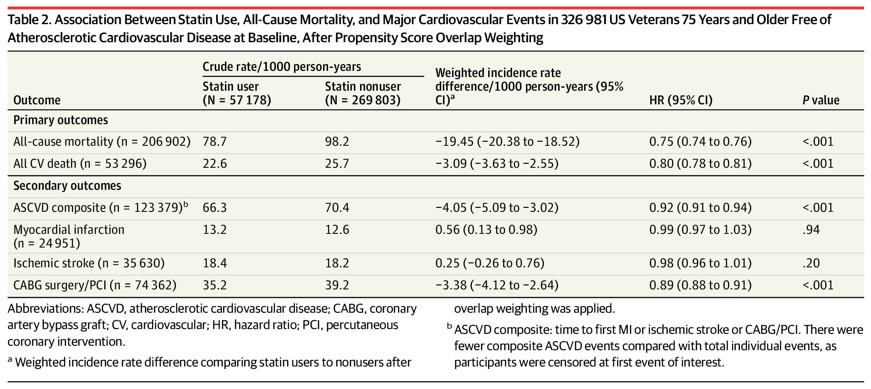
Statins Improve Health Outcomes in US Veterans
A new study published in July 2020 in the Journal of the American Medical Association (JAMA) found that statin use was associated with substantial reduction in all-cause mortality.
The study recruited 326,981 veterans with a mean age of 81 years and followed them for a
mean of 6.8 years from a clinical visit. Compared to non-statin drug users, statin use was associated with a 25% reduction in all-cause mortality, 20% reduction in cardiovascular mortality, and an 8% reduction in a composite of atherosclerotic cardiovascular events.
VA Analysis Finds Significant Benefit for Statins in Veterans 75 and Older (link)
Legacy effect of statins: 20-year follow up of the West of Scotland Coronary Prevention Study (WOSCOPS) (link) - hydrophilic statin

Summarizing the Current State and Evidence on Efficacy and Safety of Statin Therapy (link)
In a meta-analysis of 27 randomized trials and 174,000 participants, for every ~40 mg/dL LDL-C reduction with statin therapy, the relative risk of major adverse cardiovascular events is reduced by ~20-25%, and all-cause mortality is reduced by 10%. More intense statin regimens yield a 15% further proportional reduction in major adverse cardiovascular events compared to less intense regimens. These relative reductions are similar in primary vs. secondary prevention, lower vs. higher-risk, men vs. women, and also similar in other major subgroups.
Effect of Rosuvastatin on Low-Density Lipoprotein Cholesterol in Patients With Hypercholesterolemia
Rosuvastatin lowered CRP levels by 37%, with a 12 month mean of 2.2 mg/L. JUPITER trial (link)


Comments