Resistant Starch and Inulin
Overview (ref):
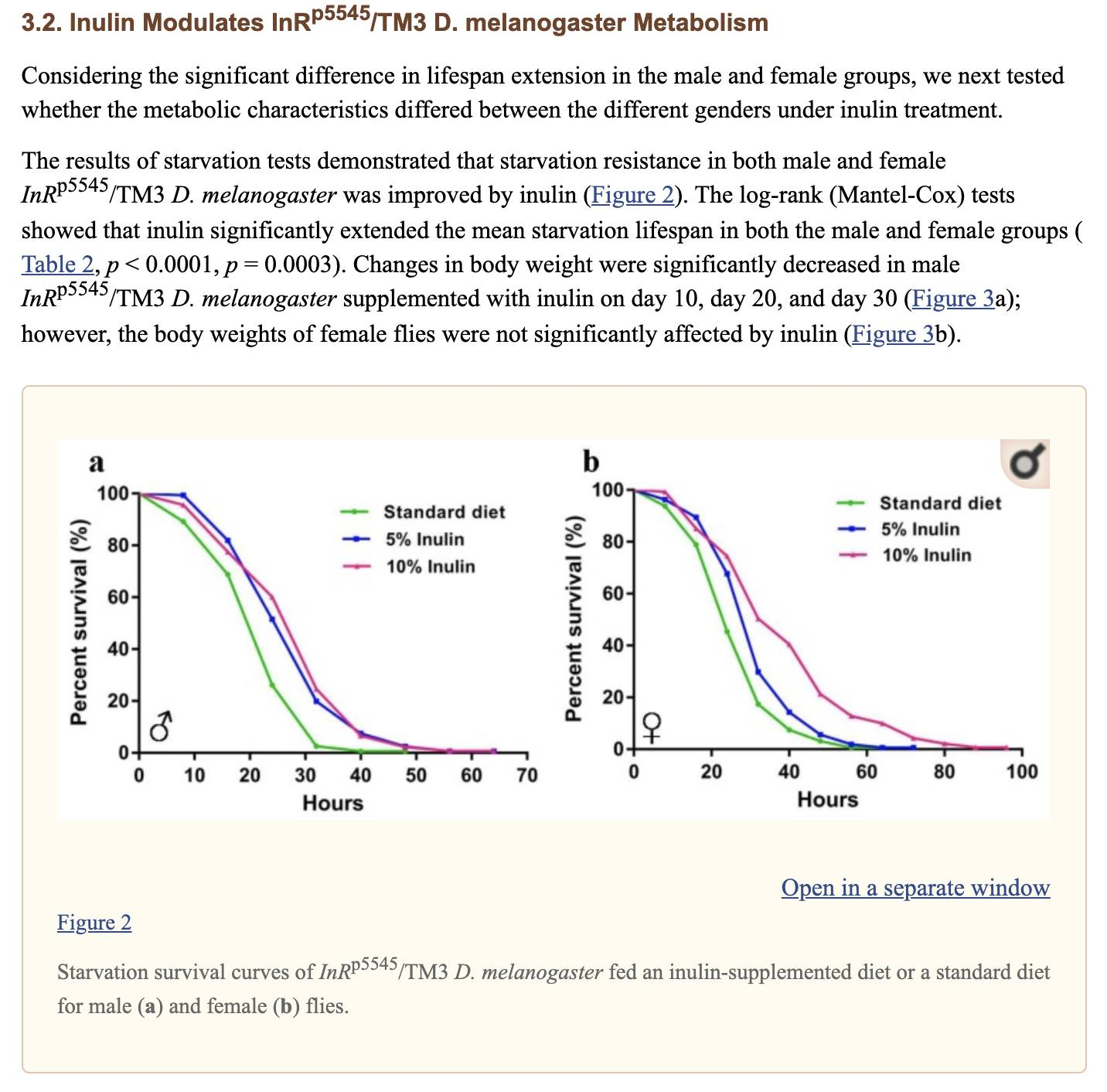
A lot of inflammation and oxidative stress comes from the gut. By fixing the gut microbiota and making the epithelium stronger, oxidation and inflammation comes down (ref). This may result in reduced blood glucose, fasting insulin, and insulin resistance (ref). Resistant starch, like fiber, reduces post-prandial glucose spike when taken with meals (ref).
Short Chain Fatty Acids (SCFA) in general may help resolve IBD (ref). Butyrate is healthy, it may help us age more slowly (HDAC inhibitor).
What type of RS to consume?
Green Banana Flour, which is a kind of RS2, seems to have most consistently increased Butyrate in human subjects (ref).
Oat and/or oat fiber, too, are fairly safe & beneficial based on extensive human studies.
Leek and Garlic powder are rich in FOS (Fructooligosaccharides) and have excellent epidemiology.
Clinical summary:
RS supplementation caused a significant reduction in IL6 (weighted mean difference = − 1.11 pg/mL; 95% CI: − 1.72, − 0.5 pg/mL; P = < 0.001) and TNF-alpha (weighted mean difference = − 2.19 pg/mL; 95% CI: − 3.49, − 0.9 pg/mL; P = 0.001) levels.
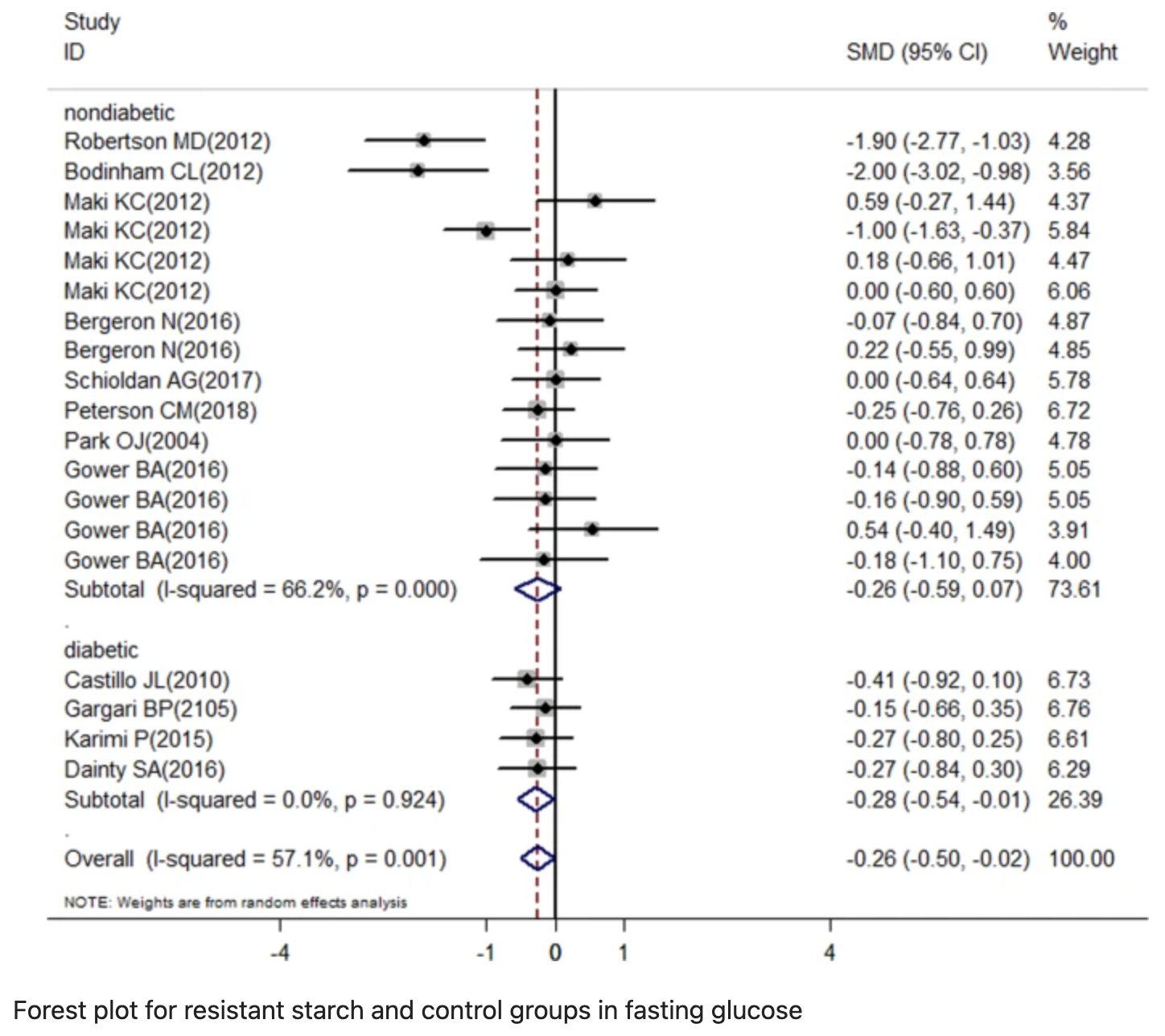
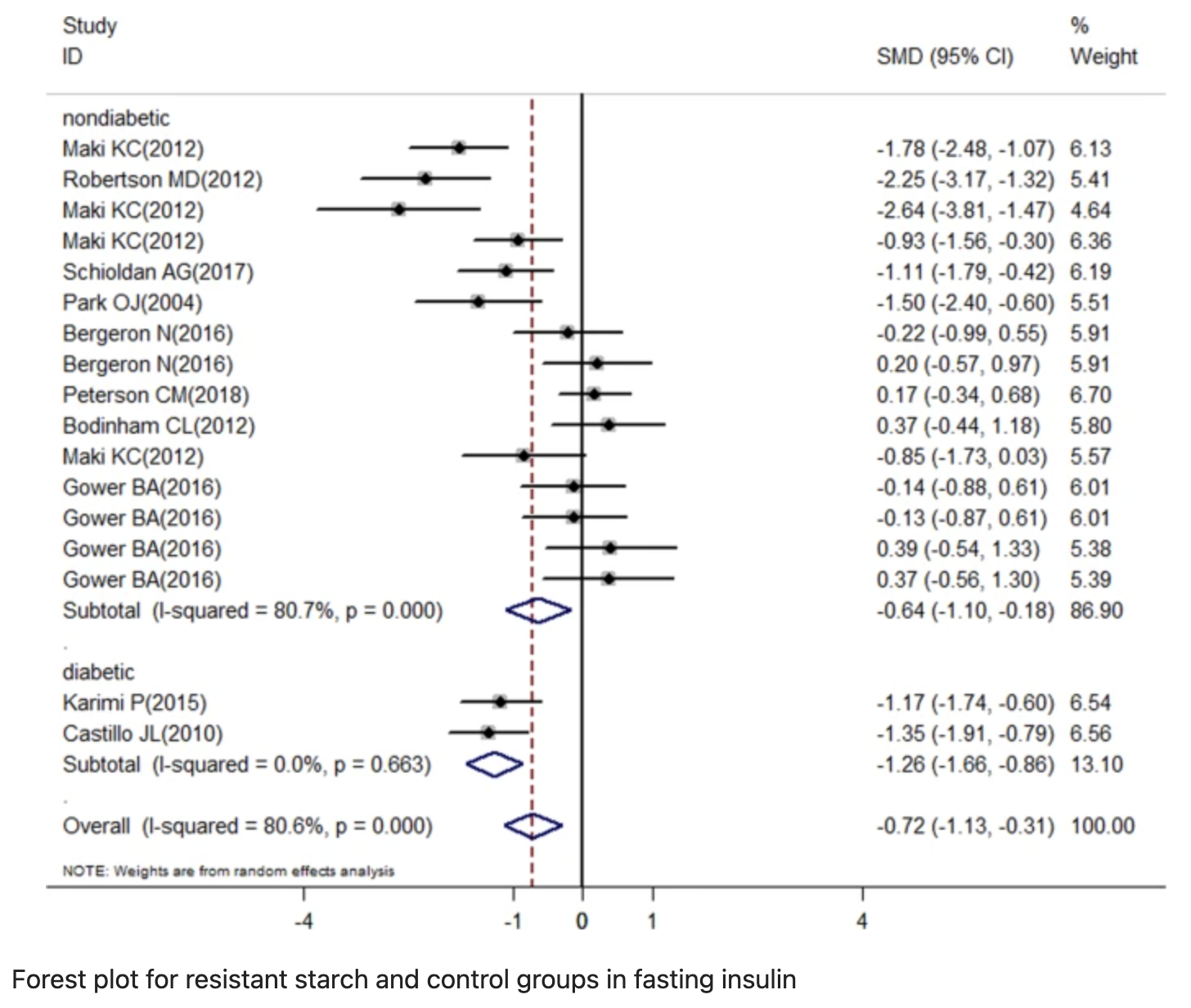
RS supplementation reduced fasting insulin in overall and stratified (diabetics and nondiabetics trials) analysis (SMD = –0.72; 95% CI: –1.13 to –0.31; SMD = –1.26; 95% CI: –1.66 to –0.86 and SMD = –0.64; 95% CI: –1.10 to –0.18, respectively), and reduced fasting glucose in overall and stratified analysis for diabetic trials (SMD = –0.26; 95% CI: –0.5 to –0.02 and SMD = –0.28; 95% CI: –0.54 to –0.01, respectively).
Oat fiber supplementation was associated with a lower risk of future revascularization (HR = 0.54, 95% CI 0.35–0.85; p = 0.007), and lower risk of major adverse cardiovascular events (HR = 0.62, 95% CI 0.43–0.88; p = 0.008) (ref)
In mice studies, RS was associated with a significant reduction in bowel mucosal damage compared to placebo (standardized mean difference − 1.83, 95% CI − 2.45 to − 1.20). In human experiments, five studies reported data on clinical remission in IBD. In all five, a positive effect was seen in patients who consumed RS (ref).
[NEGATIVE] Optimal formulation and optimal dose are unclear. Every individual responds differently. Negative long term effects unknown.
Effects of resistant starch interventions on circulating inflammatory biomarkers: a systematic review and meta-analysis of randomized controlled trials, 2020
Purpose
This study aimed to summarize earlier studies on the effects of RS consumption on the serum levels of inflammatory biomarkers.
Methods
A comprehensive search was done in the electronic databases that published from 1988 up to May 2019. Two reviewers independently performed screening, data extraction, and risk-of-bias assessment. We used from the effect size, as estimated by the mean difference to perform the fixed method meta-analysis.
Results
Overall, 13 studies with 14 effect sizes met the inclusion criteria and were included in the final analysis. Sample size of these studies ranged from 15 to 75 and intervention duration ranged from 4 to 14 weeks. Meta-analysis revealed that higher consumption of resistant starch caused a significant reduction in the interleukin 6 (weighted mean difference = − 1.11 pg/mL; 95% CI: − 1.72, − 0.5 pg/mL; P = < 0.001) and tumor necrosis factor alpha (weighted mean difference = − 2.19 pg/mL; 95% CI: − 3.49, − 0.9 pg/mL; P = 0.001) levels. However, no significant changes were found in C-reactive protein concentration (weighted mean difference = − 0.21 mg/L; 95% CI: − 1.06, 0.63 mg/L; P = 0.61). Moreover, the changes in interleukin 6 concentration was dependent on study quality and intervention duration.
Conclusion
The current meta-analysis indicated that RS intake can improve some inflammatory biomarkers. More research, with a large sample sizes and accurate design is recommended.
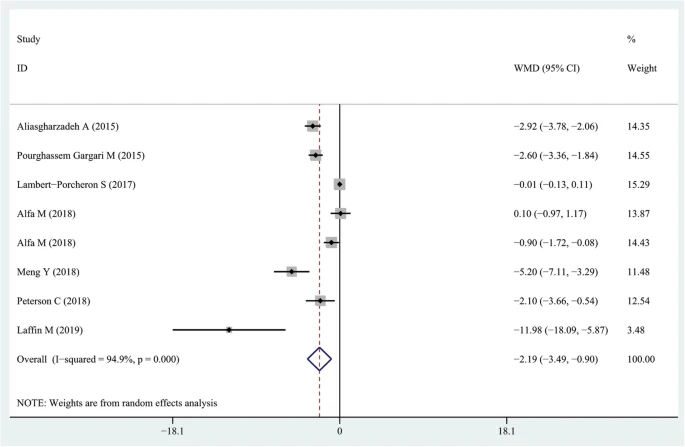
Forest plot summarizing the association between intake resistant starches on circulating TNF-α concentrations
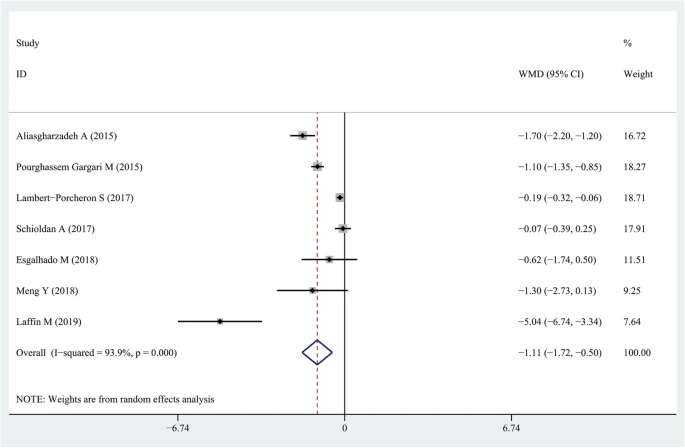
Forest plot summarizing the association between intake resistant starches on circulating IL-6 concentrations
References:
Amylose resistant starch (HAM-RS2) supplementation increases the proportion of Faecalibacterium bacteria in end-stage renal disease patients: Microbial analysis from a randomized placebo-controlled trial, 2019
high-amylose maize resistant starch type 2 (HAM-RS2)
Effect of 12 wk of resistant starch supplementation on cardiometabolic risk factors in adults with prediabetes: a randomized controlled trial, 2018
45 g/d of high-amylose maize (RS2)
High-resistant starch, low-protein flour intervention on patients with early type 2 diabetic nephropathy: a randomized trial, 2019.
50 g of high-RS, low-protein flour
A randomized placebo controlled clinical trial to determine the impact of digestion resistant starch MSPrebiotic((R)) on glucose, insulin, and insulin resistance in elderly and mid-age adults, 2018, result
30g/d MSPrebiotic is a Resistant Starch (RS2) prebiotic, which is naturally extracted from potatoes. This single-ingredient flavourless powder contains 7g of insoluble fiber per each 10g scoop.
Modulation of starch digestibility in breakfast cereals consumed by subjects with metabolic risk: impact on markers of oxidative stress and inflammation during fasting and the postprandial period, 2017.
Is there any place for resistant starch, as alimentary prebiotic, for patients with type 2 diabetes? 2015
10 g/d RS2, also known as high-amylose maize starch.
Resistant dextrin, as a prebiotic, improves insulin resistance and inflammation in women with type 2 diabetes: a randomised controlled clinical trial, 2015
10 g/d Resistant Dextrin(Soluble Corn Fiber)
Effects of the resistant starch on glucose, insulin, insulin resistance, and lipid parameters in overweight or obese adults: a systematic review and meta-analysis, 2019
Results
A total of 13 case–control studies that included 428 subjects with body mass index ≥25 were identified. RS supplementation reduced fasting insulin in overall and stratified (diabetics and nondiabetics trials) analysis (SMD = –0.72; 95% CI: –1.13 to –0.31; SMD = –1.26; 95% CI: –1.66 to –0.86 and SMD = –0.64; 95% CI: –1.10 to –0.18, respectively), and reduced fasting glucose in overall and stratified analysis for diabetic trials (SMD = –0.26; 95% CI: –0.5 to –0.02 and SMD = –0.28; 95% CI: –0.54 to –0.01, respectively). RS supplementation increased HOMA-S% (SMD = 1.19; 95% CI: 0.59–1.78) and reduced HOMA-B (SMD =–1.2; 95% CI: –1.64 to –0.77), LDL-c concentration (SMD =–0.35; 95% CI: –0.61 to −0.09), and HbA1c (SMD = –0.43; 95% CI: –0.74 to –0.13) in overall analysis.
Conclusions
This meta-analysis has provided evidence that RS supplementation can improve fasting glucose, fasting insulin, insulin resistance and sensitivity, especially for diabetic with overweight or obesity.
Robertson, Insulin-sensitizing effects of dietary resistant starch and effects on skeletal muscle and adipose tissue metabolism, 2005.
Bodinham, Fibre improves first-phase insulin secretion in overweight individuals, 2012.
Maki, Resistant starch from high-amylose maize increases insulin sensitivity in overweight and obese men, 2012,
Bergeron, Diets high in resistant starch increase plasma levels of trimethylamine-N-oxide, a gut microbiome metabolite associated with CVD risk, 2016.
Schioldan, Effects of a diet rich in arabinoxylan and resistant starch compared with a diet rich in refined carbohydrates on postprandial metabolism and features of the metabolicsyndrome, 2018.
Peterson, Effect of 12 wk of resistant starch supplementation on cardiometabolic risk factors in adults with prediabetes: a randomized controlled trial, 2018.
Park, Resistant starch supplementation influences blood lipid concentrations and glucose control in overweight subjects, 2004.
Gower, Baseline insulin sensitivity affects response to high-amylose maize resistant starch in women: a randomized, controlled trial, 2016.
An introductory review of resistant starch type 2 from high-amylose cereal grains and its effect on glucose and insulin homeostasis, 2019
High amylose maize-resistant starch type 2
The effects of resistant starches on inflammatory bowel disease in preclinical and clinical settings: a systematic review and meta-analysis, 2020
Background
Inflammatory bowel disease (IBD) is a debilitating chronic disease with limited treatment options. Resistant starches may represent a novel treatment for IBD. However, its efficacy and safety remain unclear. Our objective was to perform a systematic review to summarize the preclinical and clinical effects of resistant starch, which may help guide future studies.
Methods
Medline, EMBASE, and the Cochrane Central Register were searched. Included studies investigated the use of resistant starch therapy in in vivo animal models of IBD or human patients with IBD. Articles were screened, and data extracted, independently and in duplicate. The primary outcomes were clinical remission (clinical) and bowel mucosal damage (preclinical).
Results
21 preclinical (n = 989 animals) and seven clinical (n = 164 patients) studies met eligibility. Preclinically, resistant starch was associated with a significant reduction in bowel mucosal damage compared to placebo (standardized mean difference − 1.83, 95% CI − 2.45 to − 1.20). Clinically, five studies reported data on clinical remission but clinical and methodological heterogeneity precluded pooling. In all five, a positive effect was seen in patients who consumed resistant starch supplemented diets. The majority of studies in both the preclinical and clinical settings were at a high or unclear risk of bias due to poor methodological reporting.
Conclusions
Our review demonstrates that resistant starch is associated with reduced histology damage in animal studies, and improvements in clinical remission in IBD patients. These results need to be tempered by the risk of bias of included studies. Rigorously designed preclinical and clinical studies are warranted.
Increasing Fecal Butyrate in Ulcerative Colitis Patients by Diet: Controlled Pilot Study
Topical butyrate has been shown to be effective in the treatment of ulcerative colitis (UC). Butyrate is derived from colonic fermentation of dietary fiber, and our aim was to study whether UC patients could safely increase the fecal butyrate level by dietary means. We enrolled 22 patients with quiescent UC (mean age, 44 years; 45% women; median time from last relapse, 1 year) in a controlled pilot trial lasting 3 months. The patients were instructed to add 60 g oat bran (corresponding to 20 g dietary fiber) to the daily diet, mainly as bread slices. Fecal short-chain fatty acids (SCFAs) including butyrate, disease activity, and gastrointestinal symptoms were recorded every 4 weeks. During the oat bran intervention the fecal butyrate concentration increased by 36% at 4 weeks (from 11 ± 2 (mean ± SEM) to 15 ± 2 μmol/g feces) (p < 0.01). The mean butyrate concentration over the entire test period was 14 ± 1 μmol/g feces (p < 0.05). Remaining fecal SCFA levels were unchanged. No patient showed signs of colitis relapse. Unlike controls, the patients showed no increase in gastrointestinal complaints during the trial. Yet patients reporting abdominal pain and reflux complaints at entry showed significant improvement at 12 weeks that returned to baseline 3 months later. This pilot study shows that patients with quiescent UC can safely take a diet rich in oat bran specifically to increase the fecal butyrate level. This may have clinical implications and warrants studies of the long-term benefits of using oat bran in the maintenance therapy in UC.
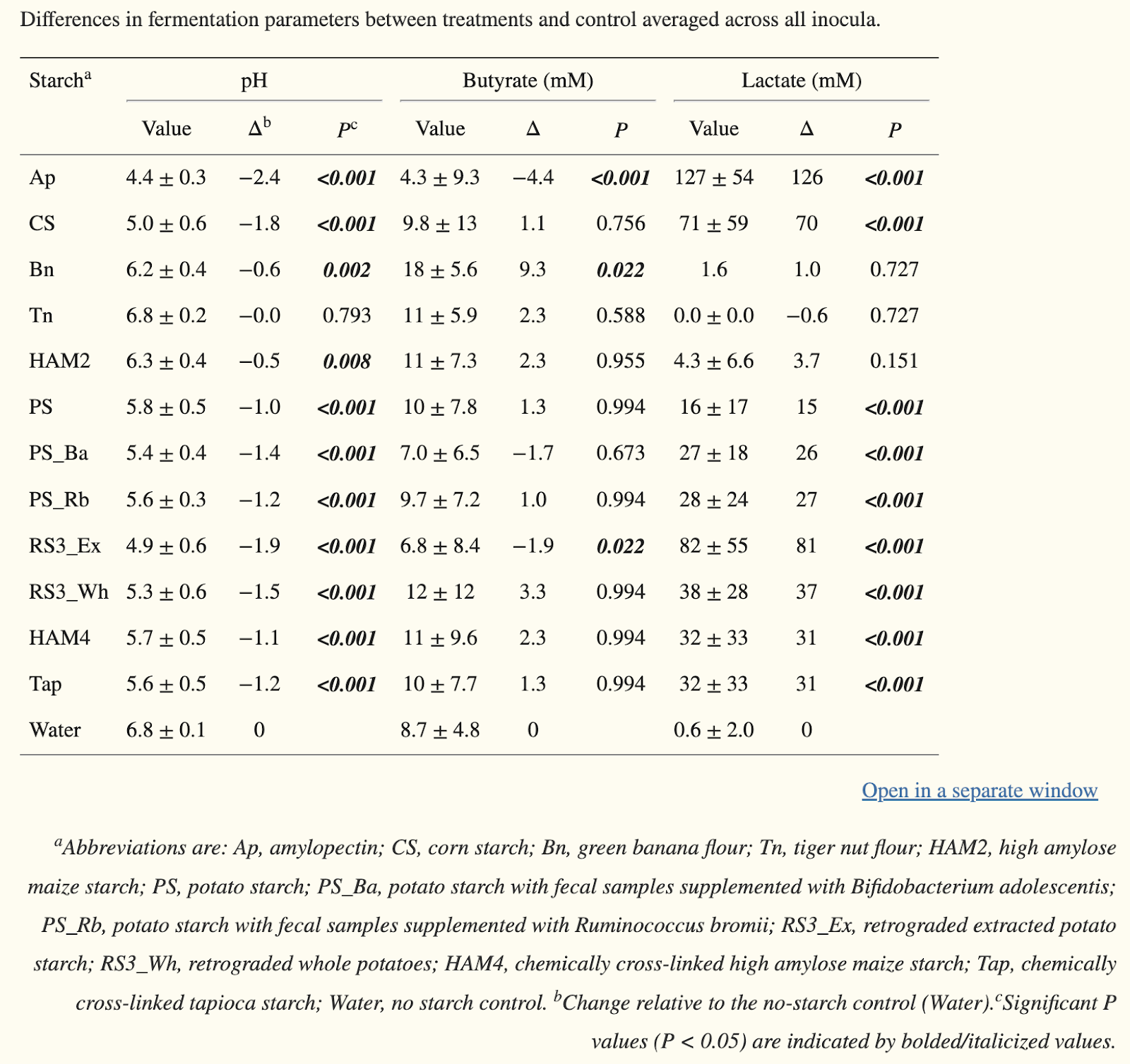
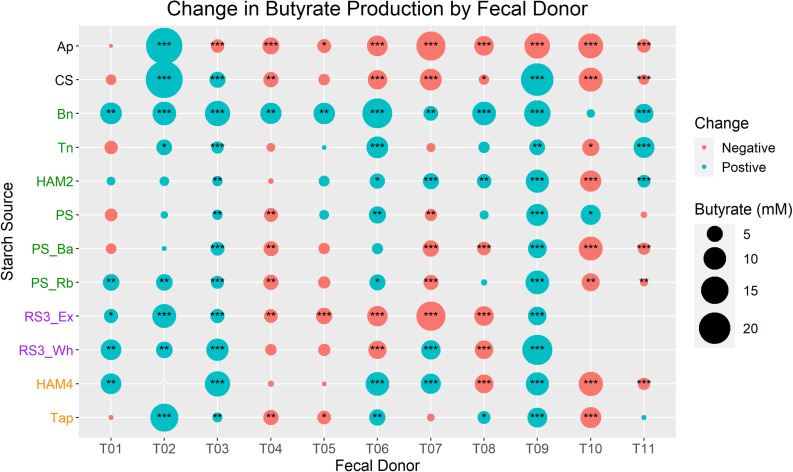
In vitro Fermentation Reveals Changes in Butyrate Production Dependent on Resistant Starch Source and Microbiome Composition, 2021
Fecal samples from 10 individuals were used as the inoculum for fermentation with 10 different starch sources. Butyrate production was heterogeneous across both fecal inocula and starch source, suggesting that a given microbiome is best suited to produce butyrate only from a subset of RS sources that differs between individuals. Interestingly, neither the total amount of RS degraders nor butyrate producers seemed to be limiting for any individual, rather the membership of these sub-populations was more important. While none of the RS degrading organisms were correlated with butyrate levels, Ruminococcus bromii was strongly positively correlated with many of the most important butyrate producers in the gut, though total butyrate production was strongly influenced by factors such as pH and lactate levels. Together these results suggest that the membership of the RS degrader and butyrate producer communities rather than their abundances determine the RS sources that will increase butyrate levels for a given microbiome.
Green banana is considered RS2, as it is indigestible due to the high amylose content in its raw form. (link)
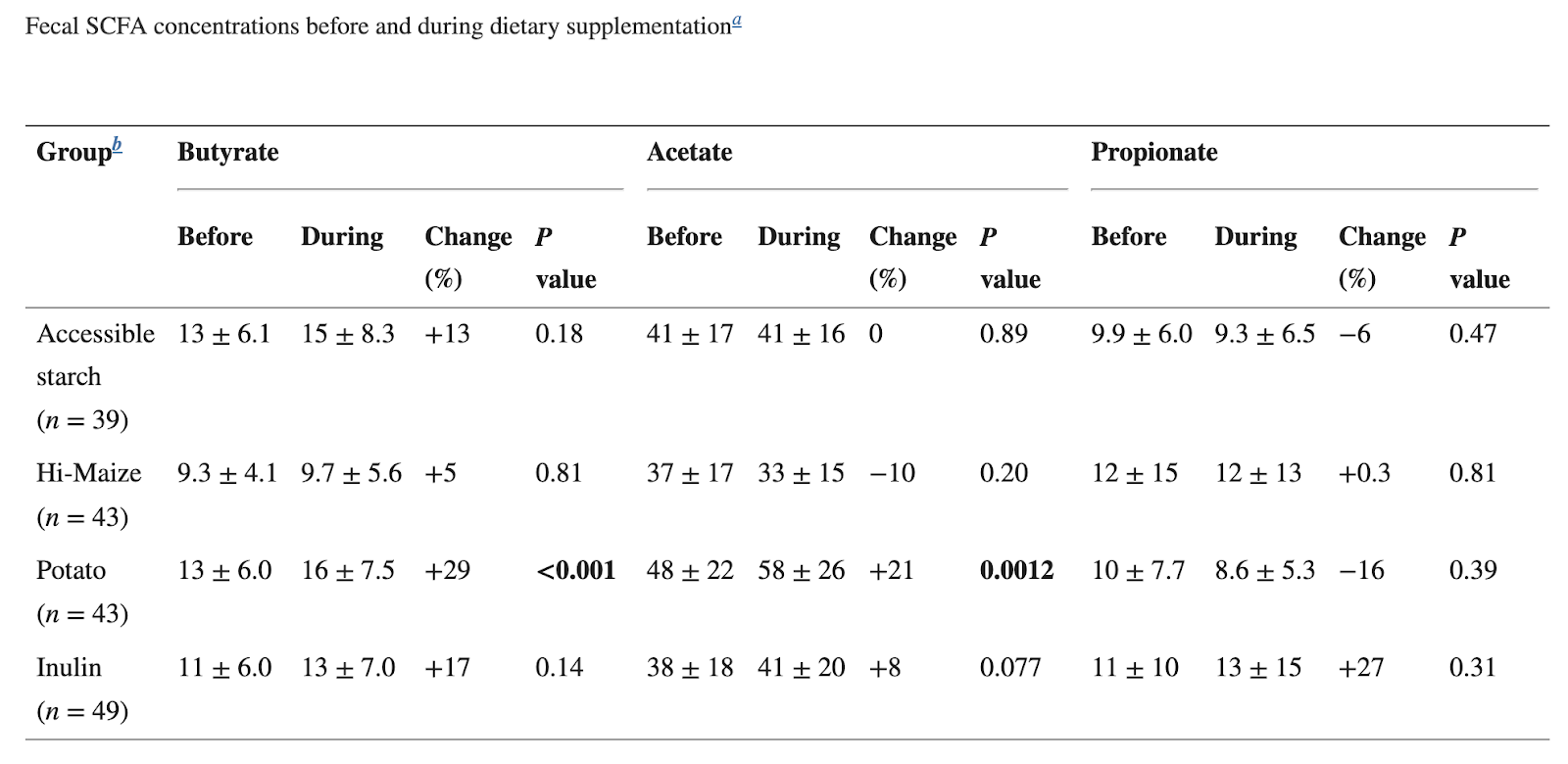
Dynamics of Human Gut Microbiota and Short-Chain Fatty Acids in Response to Dietary Interventions with Three Fermentable Fibers, 2019
Production of short-chain fatty acids (SCFAs), especially butyrate, in the gut microbiome is required for optimal health but is frequently limited by the lack of fermentable fiber in the diet. We attempted to increase butyrate production by supplementing the diets of 174 healthy young adults for 2 weeks with resistant starch from potatoes (RPS), resistant starch from maize (RMS), inulin from chicory root, or an accessible corn starch control. RPS resulted in the greatest increase in total SCFAs, including butyrate. Although the majority of microbiomes responded to RPS with increases in the relative abundance of bifidobacteria, those that responded with an increase in Ruminococcus bromii or Clostridium chartatabidum were more likely to yield higher butyrate concentrations, especially when their microbiota were replete with populations of the butyrate-producing species Eubacterium rectale. RMS and inulin induced different changes in fecal communities, but they did not generate significant increases in fecal butyrate levels.
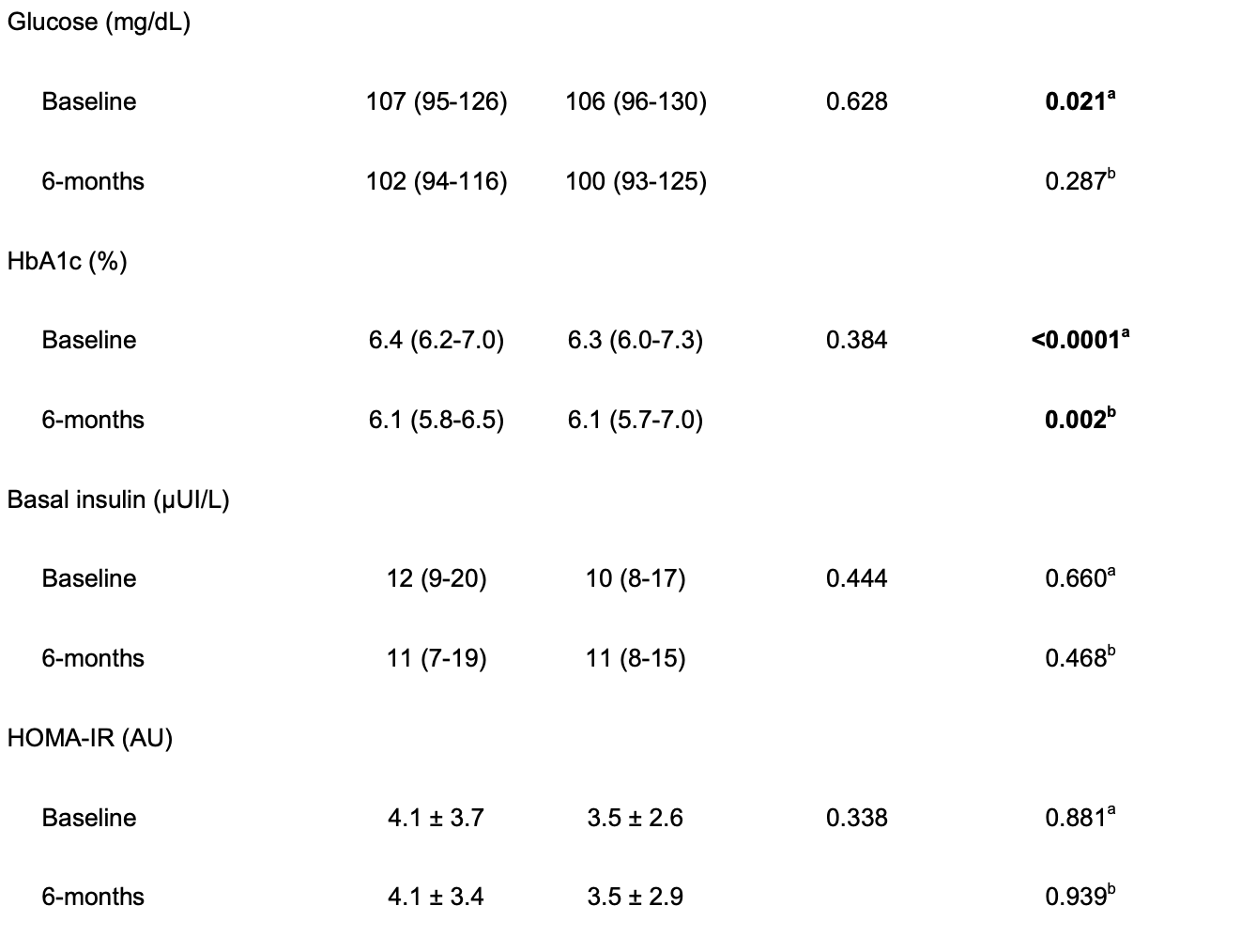
Beneficial effects of green banana biomass consumption in patients with pre-diabetes and type 2 diabetes: a randomized controlled trial, 2019
Middle-aged subjects (n 113) of both sexes with pre-diabetes (HbA1c: 5·7-6·4 %) or diabetes (HbA1c ≥ 6·5 %) were randomised to receive nutritional support plus green banana biomass (40 g) (RS: approximately 4·5 g, G1, n 62) or diet alone (G2, n 51) for 24 weeks. Body composition, biochemical analyses and dietary intake were evaluated at the beginning and end of the study. In the experimental group (G1), consumption of RS was associated with reduction in HbA1c (P = 0·0001), fasting glucose (P = 0·021), diastolic blood pressure (P = 0·010), body weight (P = 0·002), BMI (P = 0·006), waist and hip circumferences (P < 0·01), fat mass percentage (P = 0·001) and increase in lean mass percentage (P = 0·011). In controls (G2), reductions were observed in waist and hip circumferences (P < 0·01), HbA1c (P = 0·002) and high-density lipoprotein-cholesterol (P = 0·020). In pre-diabetes or diabetes, non-significant differences were observed in the percentage reduction in HbA1c and fasting glucose in exploratory analyses. Our results indicate that the consumption of bioactive starches is a good dietary strategy to improve metabolic control and body composition.

Resistant starch improves insulin sensitivity in metabolic syndrome. 2010
Aims: Diets rich in non-viscous fibre are linked to a reduced risk of both diabetes and cardiovascular disease; however, the mechanism of action remains unclear. This study was undertaken to assess whether chronic consumption of this type of fibre in individuals with the metabolic syndrome would improve insulin sensitivity via changes in ectopic fat storage.
Methods: The study was a single-blind, randomized, parallel nutritional intervention where 20 insulin resistant subjects consumed either the fibre supplement (resistant starch) (40 g/day) or placebo supplement (0 g/day) for 12 weeks. Insulin sensitivity was measured by euglycaemic-hyperinsulinaemic clamp and ectopic fat storage measured by whole-body magnetic resonance spectroscopy.
Results: Resistant starch consumption did not significantly affect body weight, fat storage in muscle, liver or visceral depots. There was also no change with resistant starch feeding on vascular function or markers of inflammation. However, in subjects randomized to consume the resistant starch, insulin sensitivity improved compared with the placebo group (P = 0.023). Insulin sensitivity correlated significantly with changes in waist circumference and fat storage in tibialis muscle and to a lesser extent to visceral-to-subcutaneous abdominal adipose tissue ratio.
Conclusion: Consumption of resistant starch improves insulin sensitivity in subjects with the metabolic syndrome. Unlike in animal models, diabetes prevention does not appear to be directly related to changes in body adiposity, blood lipids or inflammatory markers. Further research to elucidate the mechanisms behind this change in insulin sensitivity in human subjects is required.
The Therapeutic Potential of Resistant Starch in Modulation of Insulin Resistance, Endotoxemia, Oxidative Stress and Antioxidant Biomarkers in Women with Type 2 Diabetes: A Randomized Controlled Clinical Trial, 2015
Aims: This trial aims to determine the effects of resistant starch (RS) subtype 2 (RS2) on glycemic status, metabolic endotoxemia and markers of oxidative stress.
Methods: A randomized, controlled, parallel-group clinical trial group of 56 females with type 2 diabetes mellitus (T2DM) was divided to 2 groups. The intervention group (n = 28) and control group (n = 28) received 10 g/day RS2 or placebo for 8 weeks, respectively. Fasting blood samples were taken to determine glycemic status, endotoxin, high sensitivity C-reactive protein (hs-CRP), malondialdehyde (MDA), total antioxidant capacity (TAC), antioxidant enzymes concentrations as well as uric acid at baseline and after the intervention.
Results: After 8 weeks, RS2 caused a significant decrease in the levels of MDA (-34.10%), glycosylated hemoglobin (-9.40%), insulin (-29.36%), homeostasis model of insulin resistance (-32.85%) and endotoxin (-25.00%), a significant increase in TAC (18.10%) and glutathione peroxidase (11.60%) as compared with control. No significant changes were observed in fasting plasma glucose, quantitative insulin sensitivity check index, hs-CRP, superoxide dismutase, catalase and uric acid in the RS2 group as compared with the control group.
Conclusion: Supplementation with RS2 may be improved glycemic status, endotoxemia and markers of oxidative stress in patients with T2DM.
Effect of high amylose resistant starch (HAM-RS2) supplementation on biomarkers of inflammation and oxidative stress in hemodialysis patients: a randomized clinical trial, 2018
Abstract
Introduction: Systemic inflammation and oxidative stress play a central role in the pathogenesis of cardiovascular disease and numerous other complications of CKD. Recent studies demonstrated that consumption of a diet enriched with amylose (HAM-RS2), attenuates oxidative stress and inflammation, and improves intestinal microbiome in CKD rats. The present study was designed to explore the effect of dietary amylose supplementation in hemodialysis patients.
Methods: Forty-six stable hemodialysis patients were randomized to receive biscuits containing 20 g/day during the first four weeks and 25 g/day in the next four weeks of either HAM-RS2 or wheat-flour. Fasting predialysis blood samples obtained before, during and at the end of trial were processed for biomarkers of oxidative stress and inflammation.
Findings: There was no significant difference in baseline clinical or biochemical parameters between the two groups. Serum levels of TNF-α, IL-6, and malondialdehyde declined significantly (P < 0.05) in the HAM-RS2-treated group but remained unchanged in the placebo-treated group. No significant difference was observed in serum Interleukin-1β (IL-1β) and hs-CRP concentrations and total antioxidant activity between two groups. Serum urea and creatinine concentrations significantly declined and severity of constipation improved in HAM-RS2-treated patients (P < 0.05). HAM-RS2 consumption was well tolerated and did not cause discernible side effects.
Discussion: Administration of HAM-RS2 for eight weeks significantly reduced levels of inflammatory and oxidative markers in hemodialysis patients confirming the results observed in CKD animals. Long term trials are needed to explore the impact of HAM-RS2 supplementation on clinical outcomes in end stage renal disease population.
Effect of 12 wk of resistant starch supplementation on cardiometabolic risk factors in adults with prediabetes: a randomized controlled trial, 2018
Background: Type 2 resistant starch (RS2) has been shown to improve glycemic control and some cardiovascular endpoints in rodent and human studies.
Objective: The aim of this study was to perform one of the first randomized clinical trials in adults with prediabetes and one of the longest trials to test whether RS2 can improve cardiometabolic health.
Design: 68 overweight [body mass index (BMI) ≥27 kg/m2] adults aged 35-75 y with prediabetes were randomized to consume 45 g/d of high-amylose maize (RS2) or an isocaloric amount of the rapidly digestible starch amylopectin (control) for 12 wk. At baseline and postintervention, ectopic fat depots (visceral adipose tissue, intrahepatic lipids, and intramyocellular lipids) were measured by magnetic resonance imaging/spectroscopy, energy metabolism by respiratory chamber, and carbohydrate metabolism by glycated hemoglobin (HbA1c), an intravenous glucose tolerance test, and a meal tolerance test. Cardiovascular risk factors-serum lipids, blood pressure, heart rate, and inflammatory markers (high-sensitivity C-reactive protein [hs-CRP], interleukin-6, and tumor necrosis factor [TNF]-α)-were also measured. The primary endpoints were insulin sensitivity, insulin secretion, ectopic fat, and markers of inflammation. Data were primarily analyzed as treatment effects via a linear mixed model both with and without the addition of covariates.
Results: Relative to the control group, RS2 lowered HbA1c by a clinically insignificant 0.1 ± 0.2% (Δ = -1 ± 2 mmol/mol; P = 0.05) but did not affect insulin secretion, insulin sensitivity, the disposition index, or glucose or insulin areas under the curve relative to baseline (P ≥ 0.23). RS2 decreased heart rate by 5 ± 9 beats/min (P = 0.02) and TNF-α concentrations by 2.1 ± 2.7 pg/mL (P = 0.004), relative to the control group. Ectopic fat, energy expenditure, substrate oxidation, and all other cardiovascular risk factors were unaffected (P ≥ 0.06).
Conclusions: 12 wk of supplementation with resistant starch reduced the inflammatory marker TNF-α and heart rate, but it did not significantly improve glycemic control and other cardiovascular disease risk factors, in adults with prediabetes. This trial was registered at clinicaltrials.gov as NCT01708694.
Amylose resistant starch (HAM-RS2) supplementation increases the proportion of Faecalibacterium bacteria in end-stage renal disease patients: microbial analysis from a randomized placebo-controlled trial, Laffin et al 2019
Introduction: Many of the deleterious effects associated with chronic kidney disease (CKD) are secondary to the resultant systemic inflammation. The gut microbial changes caused by CKD are thought to perpetuate systemic inflammation. Therefore, strategies aimed at modulating the gut microbiota may be helpful in reducing complications associated with CKD. We hypothesized that supplementation with high-amylose maize resistant starch type 2 (HAM-RS2) would beneficially alter the gut microbiome and lead to lower levels of systemic inflammation.
Methods: A double-blind, parallel, randomized, placebo-controlled trial was performed comparing dietary supplementation of HAM-RS2 with placebo in patients with end-stage CKD. Fecal microbial data were obtained from a subset of patients after DNA extraction and 16s sequencing.
Findings: Supplementation of HAM-RS2 led to a decrease in serum urea, IL-6, TNFα, and malondialdehyde (P < 0.05). The Faecalibacterium genus was significantly increased in relative abundance following HAM-RS2 supplementation (HAM-RS2-Day 0: 0.40 ± 0.50 vs. HAM-RS2-Day 56: 3.21 ± 4.97 P = 0.03) and was unchanged by placebo (Control-Day 0: 0.72 ± 0.72 vs. Control-Day 56: 0.83 ± 1.57 P = 0.5).
Discussion: Supplementation of amylose resistant starch, HAM-RS2, in patients with CKD led to an elevation in Faecalibacterium and decrease in systemic inflammation. Microbial manipulation in CKD patients by using the prebiotic fiber may exert an anti-inflammatory effect through an elevation in the bacterial genera Faecalibacterium.
Resistant Starch Bagels Reduce Fasting and Postprandial Insulin in Adults at Risk of Type 2 Diabetes , 2016
Background: Type 2 diabetes (T2D) incidence continues to rise. Although increasing dietary fiber intake is an established strategy for improved glycemic control, most adults consume insufficient amounts. Fiber-enhanced functional foods can increase fiber intake, and there is particular interest in resistant starch (RS) as a high-fiber ingredient. Studies show that high-amylose maize resistant starch, type 2 (HAM-RS2) improves acute and chronic glycemic responses, but more studies are needed in individuals at high risk of T2D with RS delivered in commonly consumed foods.
Objective: The objective of this study was to examine the chronic effects of consuming bagels high in HAM-RS2 on fasting and postprandial glycemic markers in adults at increased risk of T2D.
Methods: With the use of a randomized, double-blind crossover design, 24 men and women with a mean ± SE age of 55.3 ± 1.59 y and body mass index (in kg/m2) of 30.2 ± 0.57 consumed 1 bagel containing 25 g HAM-RS2/d or 1 control wheat bagel/d for 56 d each, separated by a 4-wk washout. Fasting and postprandial oral-glucose-tolerance test (OGTT) glucose and insulin were measured on study days 1 and 57 of each bagel treatment.
Results: The RS bagel treatment resulted in significantly lower fasting (22.1%, P = 0.04), 2-h (23.3%, P < 0.008), and 3-h (18.9%, P = 0.05) insulin incremental areas under the curve and fasting insulin resistance (homeostasis model assessment of insulin resistance; 23.1%, P = 0.04) than did the control bagel treatment. Fasting and postprandial OGTT glucose concentrations did not differ between the RS and control bagel treatments on study days 1 or 57.
Conclusions: These data suggest that consumption of a high–HAM-RS2 bagel improves glycemic efficiency by reducing the amount of insulin required to manage postprandial glucose while improving fasting insulin sensitivity in adults at increased risk of T2D. This research provides support for a feasible dietary strategy for T2D risk reduction.
Effect of resistant starch type 2 on inflammatory mediators: A systematic review and meta-analysis of randomized controlled trials, 2021
Results
We included eight articles in systematic review and meta-analysis. The overall effect illustrated no significant change in serum levels of hs-CRP, IL-6, and TNF-α in intervention group compared with the control group (WMD: -7.18 pg/mL, 95% CI: −27.80, 13.45; P = 0.495, I2 = 100.0%, WMD: -0.003 pg/mL, 95% CI: −0.07, 0.06; P = 0.919, I2 = 98.1%, WMD: -0.003 pg/mL, 95% CI: −0.004, -0.001; P < 0.0001, I2 = 98.0% respectively).
Conclusion
In conclusion, we found that RS2 could not reduce inflammatory mediators, but we still need more RCTs with longer intervention duration, higher dose, and studies in different countries.
Dietary type 2 resistant starch improves systemic inflammation and intestinal permeability by modulating microbiota and metabolites in aged mice on high-fat diet, 2019
Type 2 resistant starch (RS2) is a fermentable dietary fiber conferring health benefits. We investigated the effects of RS2 on host, gut microbiota, and metabolites in aged mice on high-fat diet. In eighteen-month old mice randomly assigned to control, high-fat (HF), or high-fat+20% RS2 (HFRS) diet for 16 weeks, RS2 reversed the weight gain and hepatic steatosis induced by high-fat diet. Serum and fecal LPS, colonic IL-2 and hepatic IL-4 mRNA expressions decreased while colonic mucin 2 mRNA and protein expressions increased in the HFRS compared to the HF and the control group. 16s rRNA sequencing of fecal microbial DNA demonstrated that RS2 decreased the abundance of pathogen taxa associated with obesity, inflammation, and aging including Desulfovibrio (Proteobacteria phylum), Ruminiclostridium 9, Lachnoclostridium, Helicobacteria, Oscillibacter, Alistipes, Peptococcus, and Rikenella. Additionally, RS2 increased the colonic butyric acid by 2.6-fold while decreasing the isobutyric and isovaleric acid levels by half compared to the HF group. Functional analyses based on Clusters of Orthologous Groups showed that RS2 increased carbohydrate while decreasing amino acid metabolism. These findings demonstrate that RS2 can reverse weight gain, hepatic steatosis, inflammation, and increased intestinal permeability in aged mice on high-fat diet mediated by changes in gut microbiome and metabolites.
Oat Fiber (Beta Glucans)
The benefit of secondary prevention with oat fiber in reducing future cardiovascular event among CAD patients after coronary intervention, 2019
There is limited information about the association between oat fiber intake and future cardiovascular events in CAD patients after coronary intervention for secondary prevention. This study enrolled 716 patients after coronary intervention in clinical stable status from the CAD cohort biosignature study. Patients were analyzed according to whether the presence of regular oat fiber intake during the follow-up period, and the association with endpoints including cardiovascular death, non-fatal myocardial infarction, non-fatal stroke and revascularization procedures were analyzed. The average follow-up period is 26.75 ± 8.11 months. Patients taking oat fiber were found to have lower serum levels of LDL, triglycerides, ratio of TC/HDL, as well as lower inflammatory markers values. After adjusting for confounders in the proportional hazard Cox model, oat fiber intake was associated with a lower risk of future revascularization (HR = 0.54, 95% CI 0.35–0.85; p = 0.007), and lower risk of major adverse cardiovascular events (HR = 0.62, 95% CI 0.43–0.88; p = 0.008), suggesting the association of oat fiber use and lower risk of future adverse event in CAD patients after coronary intervention.
The difference between oats and beta-glucan extract intake in the management of HbA1c, fasting glucose and insulin sensitivity: a meta-analysis of randomized, 2016
Increasing oats and beta-glucan extract intake has been associated with improved glycemic control, which is associated with the reduction in the development of diabetes. This study aims to assess the different effects between oat (whole and bran) and beta-glucan extract intake on glycemic control and insulin sensitivity. PubMed, Embase, Medline, The Cochrane Library, CINAHL and Web of Science were searched up to February 2014. We included randomized controlled trials with interventions that lasted at least four weeks that compared oats and beta-glucan (extracted from oats or other sources) intake with a control. A total of 1351 articles were screened for eligibility, and relevant data were extracted from 18 studies (n = 1024). Oat product dose ranged from 20 g d−1 to 136 g d−1, and beta-glucan extract dose ranged from 3 g d−1 to 10 g d−1. Compared with the control, oat intake resulted in a greater decrease in fasting glucose and insulin of subjects (P < 0.05), but beta-glucan extract intake did not. Furthermore, oat intake resulted in a greater decrease in glycosylated hemoglobin (HbA1c) (P < 0.001, I2 = 0%) and fasting glucose (P < 0.001, I2 = 68%) after removing one study using a concentrate and a different design and fasting insulin of type 2 diabetes (T2D) (P < 0.001, I2 = 0%). The intake of oats and beta-glucan extracted from oats were effective in decreasing fasting glucose (P = 0.007, I2 = 91%) and fasting insulin of T2D (P < 0.001, I2 = 0%) and tented to lower HbA1c (P = 0.09, I2 = 92%). Higher consumption of whole oats and oat bran, but not oat or barley beta-glucan extracts, are associated with lower HbA1c, fasting glucose and fasting insulin of T2D, hyperlipidaemic and overweight subjects, especially people with T2D, which supports the need for clinical trials to evaluate the potential role of oats in approaching to the management of glycemic control and insulin sensitivity of diabetes or metabolic syndrome subjects
Inhibits atherosclerotic progression through improving lipid metabolism in ApoE−/− mice
Attenuates circulating oxysterols levels and hepatic inflammation via targeting TLR4 signal pathway in LDL receptor knockout mice
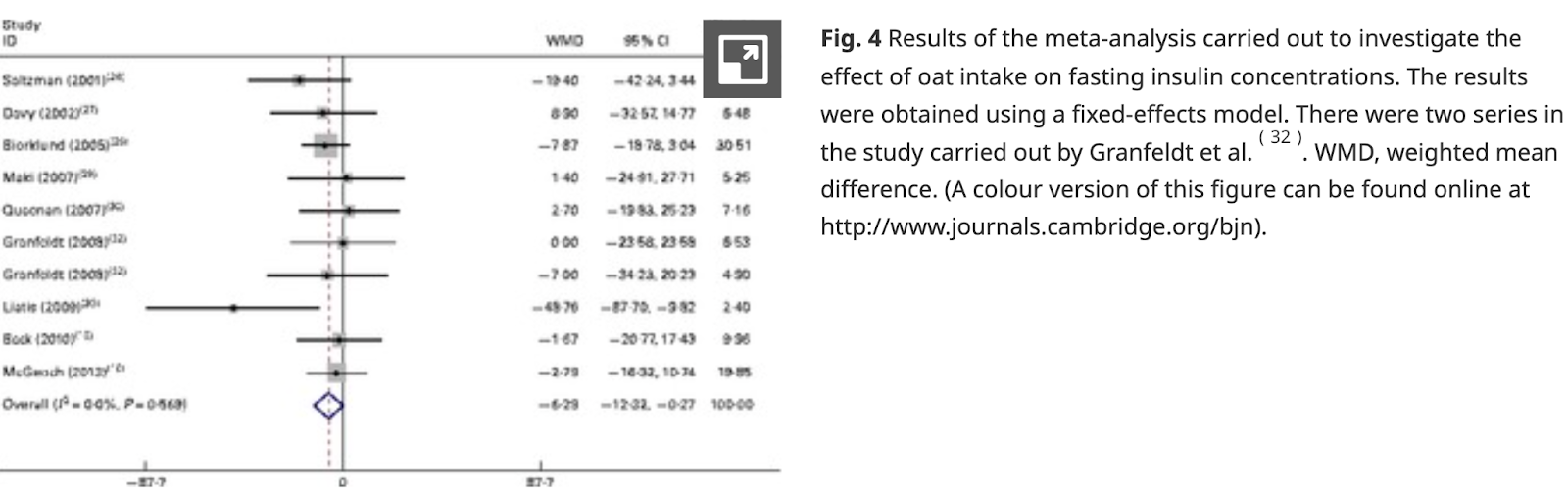
Effect of oat intake on glycaemic control and insulin sensitivity: a meta-analysis of randomised controlled trials, 2014
The present meta-analysis of randomised controlled trials (RCT) aimed to investigate the effect of oat intake on glycaemic control and insulin sensitivity. A literature search was carried out in PubMed, ScienceDirect Online and The Cochrane Library (up to October 2013) for RCT that assessed the effect of oat intake on glucose control and insulin sensitivity. A total of fifteen articles with 673 subjects met the inclusion criteria. A random-effects model was used when the overall pooled studies exhibited significant heterogeneity. Otherwise, a fixed-effects model was used. Compared with controls, oat intake significantly reduced the concentrations of fasting insulin by − 6·29 (95 % CI − 12·32, − 0·27) pmol/l (P= 0·04) and the values of glucose AUC (GAUC; 0–120 min) by − 30·23 (95 % CI − 43·65, − 16·81) min × mmol/l (P< 0·0001). There was a slight decrease in fasting glucose concentrations, glycated Hb concentrations and homeostatic model assessment-insulin resistance values in subjects who consumed oats, but the difference was not significant. In conclusion, oat intake significantly lowers fasting insulin concentrations and GAUC values. To further investigate the effect of oat intake on fasting glucose concentrations, additional long-term and high-quality RCT with a parallel design are required.
Effects of Oats (Avena sativa L.) on Inflammation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials, 2021
Background: Oat and its compounds have been found to have anti-inflammatory effects. Through this systematic review and meta-analysis, we aimed to determine an evidence-based link between oat consumption and inflammatory markers.
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. By the end of April 2021, we included randomized controlled trials (RCTs) that investigated the anti-inflammatory effect of oat and oat-related products through screening PubMed, Embase, Web of Science, ClinicalTrial.gov, and CENTRAL. Meta-analysis was conducted with a random-effect model on the standardized mean difference (SMD) of the change scores of inflammatory markers, including C-reactive protein (CRP), tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-8 (IL-8). Subgroup analyses were conducted to stratify confounding variables. The risk of bias was evaluated using the Cochrane risk of bias tool and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) was applied to report the quality of evidence. This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42021245844).
Results: Systematic screening of five databases yielded 4,119 studies, of which 23 RCTs were finally selected. For the four systemic inflammatory markers analyzed, no significant alterations were found after oat consumption. However, oat intake was found to significantly decrease CRP levels in subjects with one or more health complications (SMD: −0.18; 95% CI: −0.36, 0.00; P = 0.05; I2 = 10%). Furthermore, IL-6 levels were significantly decreased in subjects with dyslipidemia (SMD = −0.34; 95% CI: −0.59, −0.10; P = 0.006; I2 = 0%). These beneficial effects might be attributed to the effects of avenanthramide and β-glucan.
Conclusions: Overall evidence supporting the alleviation of inflammatory response by oat intake was poor, calling for future studies including a larger sample size to confirm the findings.
Beta Glucan as a Cancer Treatment
Cancer affects the blood cells that fight off infections, weakening the immune system. Doctors may recommend biologic response modifiers (BRMs). A BRM is a form of immunotherapy that boosts the immune system and triggers a defense response. Beta glucans are one type of BRM. Beta glucans can help to slow cancer growth, and prevent it from spreading to other parts of the body.
Optimizing Tumor Microenvironment (TME) for Cancer Immunotherapy: β-Glucan-Based Nanoparticles
Recent preclinical mouse studies have demonstrated that the systemic administration of certain β-glucans could effectively manipulate TME, resulting in significant reduction of primary tumor growth and distant metastases (72). These results suggest that β-glucan molecules are potential immune modulator that can manipulate innate and adaptive immune responses within the TME and improve clinical responses of current cancer immunotherapies.
Metastases from renal cell carcinomas (RCC) are resistant to radiation and chemotherapy but are relatively immunogenic. We have investigated the possibility to eliminate human RCC micrometastases using MAb G250. Addition of soluble beta-glucan induced the killing of MAb and iC3b opsonized spheroids by effector cells (6-21%) in vitro.
[Sources of beta glucan: Oatmeal fiber, Triple Mushroom Complex - Maitake - Reishi - Shiitake, Beta 1,3/1,6- D-Glucan 100 mg with Maitake Mushrooms]
Effects of oat β-glucan, oat resistant starch, and the whole oat flour on insulin resistance, inflammation, and gut microbiota in high-fat-diet-induced type 2 diabetic rats
This study was aimed to compare the beneficial effects of oat β-glucan (OG), oat resistant starch (ORS), and whole oat foods (WO), and explore the correlations between the key phylotypes of gut microbiota and type 2 diabetes (T2D) indexes and inflammation indexes in high-fat diet induced T2D rats. WO exhibited better effects on ameliorating insulin resistance and glucose tolerance than OG and ORS (p < 0.05). The three oat products had equal effects on the inhibition of cytokine release (p > 0.05). OG, ORS, and WO altered the gut microbiota composition with increased genus Clostridium, and Butyricoccus, but decreased genus Bacteroides, Lactobacillus, Oscillospira, and Ruminococcus. In addition, the Pearson correlation analysis showed that genus Bacteroides, Butyricoccus, Parabacteroides, Lactobacillus, Oscillospira, Ruminococcus, and Bifidobacterium positively correlated (p < 0.05) with the development of diabetes and inflammation, while genus Clostridium and Faecalibacterium showed a negative correlation (p < 0.05). These results provide valuable information about the beneficial effects of oat products on human health.
Beta-glucans and cancer: The influence of inflammation and gut peptide
Inflammation is an hallmark of cancer.
Β-Glucans are belonging to MedDiet and are a typical example of functional food.
Β-Glucans act at several levels: modulating inflammatory parameters and gut peptide release.
Β-Glucans can be a tool in tumour drug resistance, metastasis, and relapse.
Abstract
Dietary β-glucans are soluble fibers with potentially health-promoting effects. Gut peptides are important signals in the regulation of energy and glucose homeostasis. This article reviews the effects of different enriched β-glucan food consumption on immune responses, inflammation, gut hormone and cancer.
Gut hormones are influenced by enriched β-glucan food consumption and levels of such peptide as YY, ghrelin, glucagon-like peptide 1 and 2 in humans influence serum glucose concentration as well as innate and adaptive immunity. Cancer cell development is also regulated by obesity and glucose dishomeostasy that are influenced by β-glucan food consumption that in turn regulated gut hormones.
The effects of β-glucans on cancer metastasis, 2013
Beta-glucans (β-glucans), naturally occurring polysaccharides, are present as constituents of the cell wall of cereal grains, mushrooms, algae, or microbes including bacteria, fungi, and yeast. Since Pillemer et al. first prepared and investigated zymosan in the 1940s and others followed with the investigation of β-glucans in the 1960s and 1970s, researchers have well established the significant role of β-glucans on the immune system relative to cancer treatment, infection immunity, and restoration of damaged bone marrow. However, information on their biological role in anti-metastatic activity remains limited. As an immunomodulating agent, β-glucan acts through the activation of innate immune cells such as macrophages, dendritic cells, granulocytes, and natural killer cells. This activation triggers the responses of adaptive immune cells such as CD4(+) or CD8(+) T cells and B cells, resulting in the inhibition of tumor growth and metastasis. Reports have shown that β-glucans exert multiple effects on cancer cells and cancer prevention. However the mechanisms of their actions appear complex due to differences in source, chemical structure, insufficiently defined preparation, and molecular weight, hence the inconsistent and often contradictory results obtained. This review is focused on the potential of β-glucans as anti-metastatic agents and the known mechanisms underlying their biological effects.
Most oats contain 3-6% β-glucan by weight. (link)
The oat bran contained 20.6% total dietary fiber, of which 41% was β-glucan, whereas the oat bran concentrate contained 40.3% total dietary fiber, of which 53% was β-glucan. (link)
Oat beta glucans (link)
Oat bran is produced by removing the starchy content of the grain. It is rich in dietary fibers, especially in soluble fibers, present in the inner periphery of the kernel. Oats contain more soluble fibers than any other grain, resulting in slower digestion and an extended sensation of fullness, among other things.
Oat is a rich source of the water-soluble fiber (1,3/1,4) β-glucan, and its effects on health have been extensively studied over the last 30 years. Oat β-glucans can be highly concentrated in different types of oat brans. The beta glucan content varies, from 3-5% depending on variety when it grows in the field. Rolled oat/oat flakes is about 4% and also wholemeal oat flour. With Swedish Oat Fiber’s specially developed fractionating process, we can do concentrations of beta glucans from 6% up to 32%.
Beta-D-glucans, usually referred to as beta glucans, comprise a class of indigestible polysaccharides widely found in nature in sources such as grains, barley, yeast, bacteria, algae and mushrooms. In oats, they are concentrated in the bran, more precisely in the aleurone and sub-aleurone layer (see picture above).
Oat beta glucan is a natural soluble fiber. It is a viscous polysaccharide made up of units of the monosaccharide D-glucose. Oat beta glucan is composed of mixed-linkage polysaccharides. This means the bonds between the D-glucose units are either beta-(1→3) linkages or beta-(1→4) linkages. The (1→3)-linkages break up the uniform structure of the beta-D-glucan molecule and make it soluble and flexible. In comparison, the indigestible polysaccharide cellulose is also a beta glucan, but is not soluble. The reason it is insoluble is cellulose consists only of (1→4)-beta-D-linkages.
Oat beta glucans are large molecules. Originally in the oat kernel, it is composed of up to 200,000 glucose units, which gives molecular weights in the range of 1500-3000 kDa. It is this native structure that the production process at Swedish Oat Fiber preserves, not destructing the molecular weight during fractionating into the oat brans with high amount of beta glucans. For more details, see the separate section about molecular weight.
Oats are generally considered more healthy and nutritious than the other main cereals, well-known for the benefits of digestion and eaten during hundreds of years by both animals and humans. Today many health-oriented people have their oat porridge every morning as breakfast.
One of the more clinical breakthroughs was the discovery of oat beta glucan cholesterol-lowering properties, especially for the metabolic syndrome. In the last years, clinical studies have proved health benefits like avoiding heart diseases by maintaining/lowering cholesterol, decreased blood sugar response after eating – and also improving the gut health.
Cardiovascular disease (CVD) has been identified by the World Health Organization as the number one cause of mortality globally. High cholesterol is a risk factor in the development of coronary heart disease. The latest research demonstrates that oats and oat beta glucan can be recommended as part of a healthy diet to reduce the risk of CVD.
Oats are a naturally rich source of beta-glucan. The effect of oat beta-glucan on both serum cholesterol and blood glucose reduction is proven. Internationally recognized associations, such as the European Society of Cardiology and the US National Cholesterol Education Program, and the recent meta-analysis, support the role of oat beta-glucan, and specifically its viscosity in lowering blood cholesterol levels. It has been established that the consumption of at least 3g per day of oat beta-glucan can achieve a reduction in LDL cholesterol of up to 10% and reduce the risk of CVD by as much as 20%.
Probiotics / Prebiotics
[liver detox; healthier colon; stronger gut barrier; reduced systemic inflammation; lower endotoxin; lower IR; better sleep]
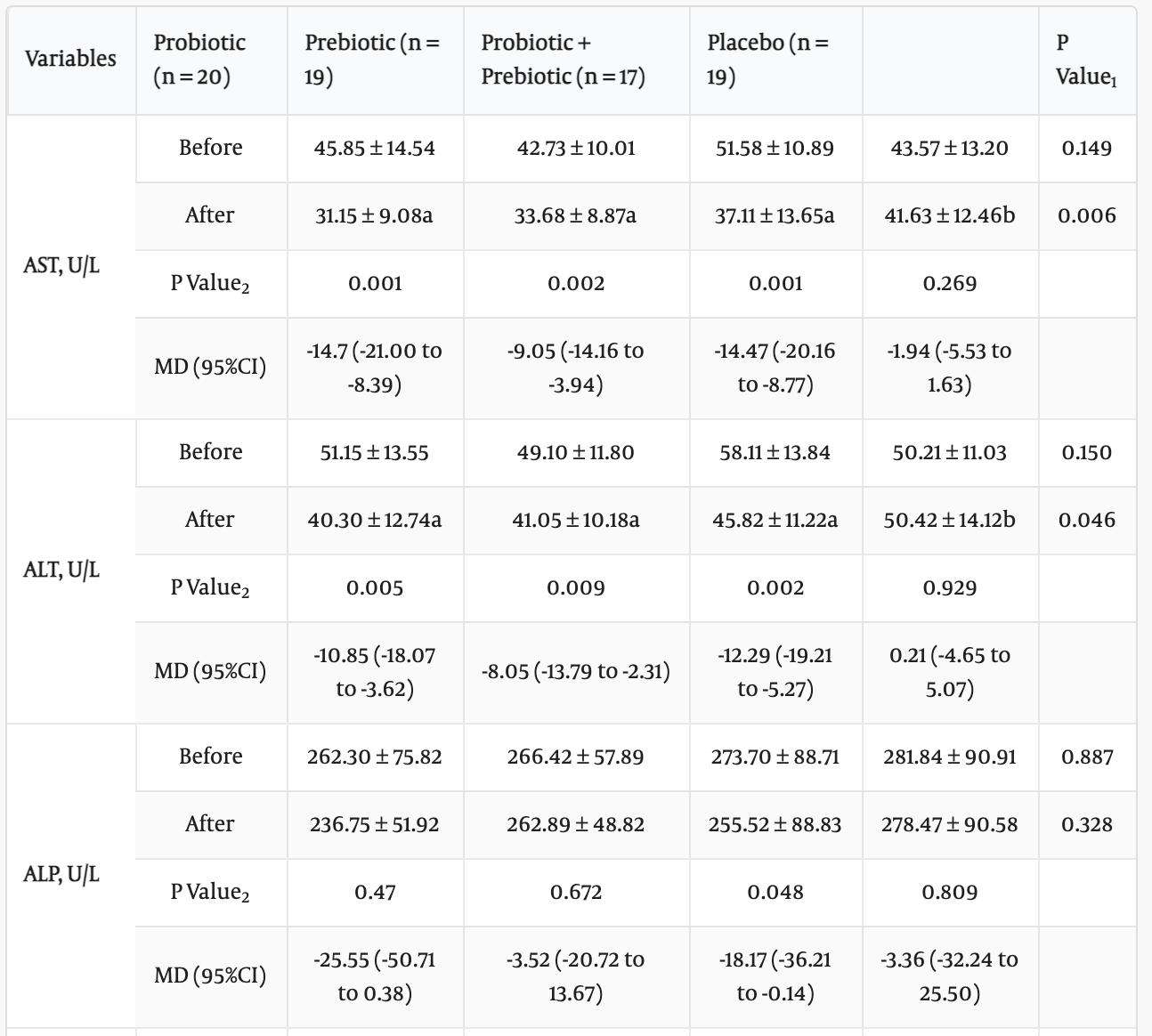
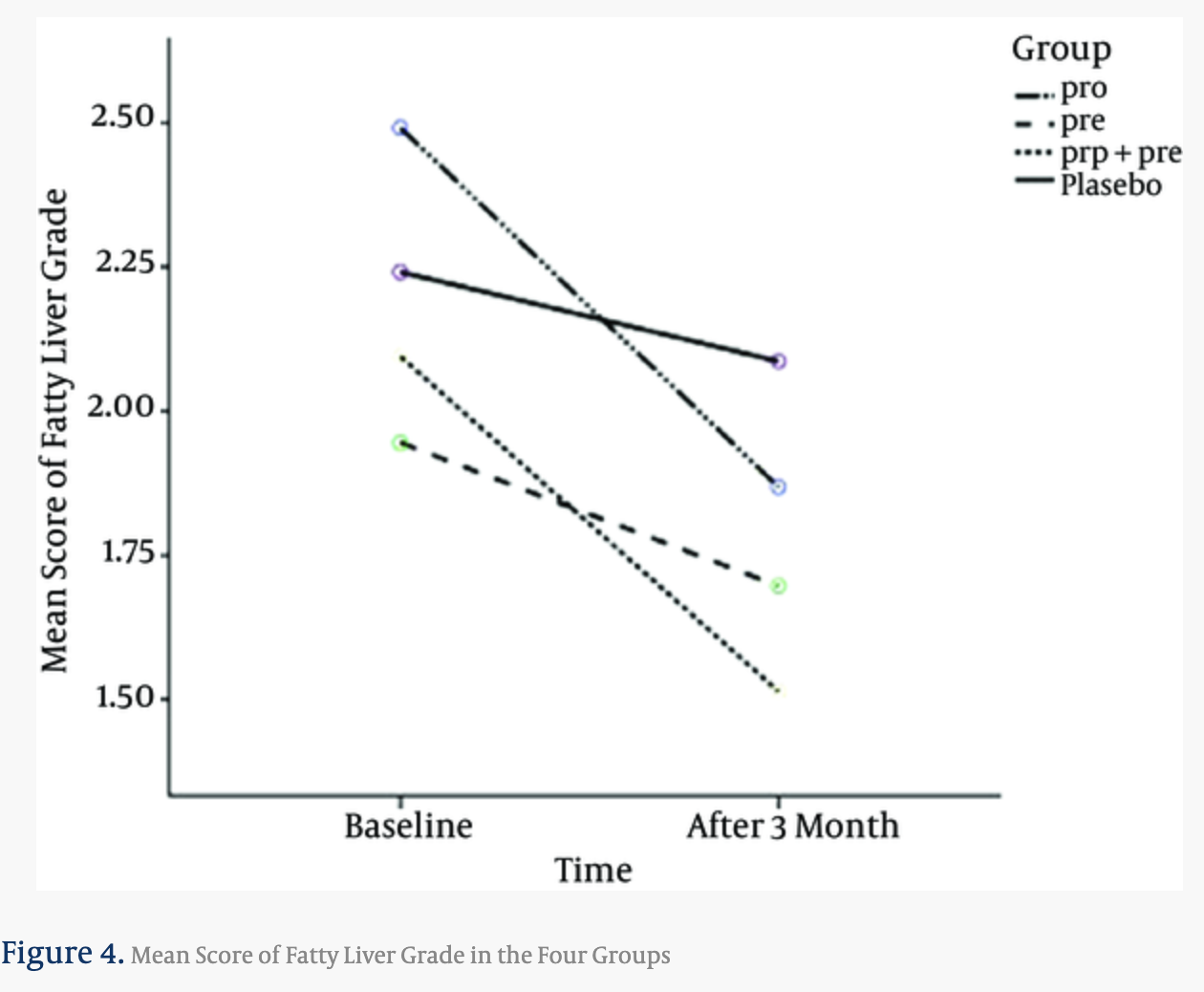
The Effect of Probiotic and/or Prebiotic on Liver Function Tests in Patients with Nonalcoholic Fatty Liver Disease: A Double Blind Randomized Clinical Trial (link)
Methods: In this double blind, placebo-control clinical trial, 75 subjects with NAFLD were voluntarily recruited from May 2013 to March 2014, in Iran. Participants were randomly assigned to 1 of 4 groups using a block randomization procedure. Group 1 received probiotic capsules (Bifidobacterium longum (BL) and Lactobacillus acidophilus (LA): 2 × 107 CFU/day), group 2 received prebiotic inulin high performance (HP): 10 g/day, group 3 received probiotic and the prebiotic, and group 4 received a placebo for 3 months. The sample size was determined on the basis of a primary outcome of a change in aspartate aminotransferase (AST) level.
Results: An intergroup comparison indicated that the AST (P = 0.006) and alanine aminotransferase (ALT) (P = 0.04) levels decreased at the end of the study. Aspartate Aminotransferase (mean difference of group1 versus placebo with P value of 0.001, group2 versus placebo with P value of 0.045, group3 versus placebo with P value of 0.015) and ALT (mean difference of group 1 versus placebo with P value of 0.009, group 2 versus placebo with P value of 0.041, and group 3 versus placebo with P value of 0.046) serum levels decreased significantly in all of the intervention groups compared to the placebo. The grade of fatty liver in group 1 (P of 0.027, and number needed to treat (NNT) = 3) and group 3 (P = 0.019 and NNT = 3) decreased compared to the placebo group with no significant changes in group 2.
Conclusions: Supplementation with probiotics and/or prebiotics improved aminotransferase enzymes, and supplementation with probiotics or pro- and prebiotics recovered the grade of fatty liver in NAFLD patients.
Bifidobacterium longum with fructo-oligosaccharides (FOS) in patients with non alcoholic steatohepatitis (2012 Feb)
Background: Increased exposure to intestinal bacterial products may contribute to the pathogenesis of non alcoholic steatohepatitis (NASH). Bifidobacteria are predominant bacterial species in the human gut microbiota and have been considered to exert a beneficial effect on human health by maintaining the equilibrium of the resident microbiota.
Aims: To evaluate the effects of Bifidobacterium longum with fructo-oligosaccharides (Fos) in the treatment of NASH.
Methods: A total of 66 patients were randomly and equally divided into two groups receiving Bifidobacterium longum with Fos and lifestyle modification (i.e., diet and exercise) versus lifestyle modification alone. The following variables were assessed at -4 (beginning of the dietary lead-in period), 0 (randomization), 6, 12, 18, and 24 weeks: aspartate transaminase (AST), alanine transaminase (ALT), bilirubin, albumin, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, fasting plasma glucose, insulin, C-peptide, C-reactive protein (CRP), tumor necrosis factor (TNF)-α, homeostasis model assessment of insulin resistance (HOMA-IR), and serum endotoxins. Liver biopsies were performed at entry and repeated after 24 weeks of treatment.
Results: At the end of study period, we observed that the Bifidobacterium longum with Fos and lifestyle modification group versus the lifestyle modification alone group showed significant differences in the AST -69.6 versus -45.9 IU/mL (P < 0.05), LDL cholesterol -0.84 versus -0.18 mmol/L (P < 0.001), CRP -2.9 versus -0.7 mg/L (P < 0.05), TNF-α -0.45 versus -0.12 ng/mL (P < 0.001), HOMA-IR -1.1 versus -0.6 (P < 0.001), serum endotoxin -45.2 versus -30.6 pg/mL (P < 0.001), steatosis (P < 0.05), and the NASH activity index (P < 0.05).
Conclusions: Bifidobacterium longum with Fos and lifestyle modification, when compared to lifestyle modification alone, significantly reduces TNF-α, CRP, serum AST levels, HOMA-IR, serum endotoxin, steatosis, and the NASH activity index.
Impact of Probiotic Administration on Serum C-Reactive Protein Concentrations: Systematic Review and Meta-Analysis of Randomized Control Trials, 2017
Nutrients. 2017 Jan; 9(1): 20.
Abstract
We conducted this systematic review and meta-analysis of prospective studies to determine the effect of probiotic administration on serum C-reactive protein (CRP) concentrations. We searched PubMed-Medline, Web of Science, the Cochrane, and Google Scholar databases (until May 2016) to identify prospective studies evaluating the impact of probiotic administration on CRP. We used a random effects models and generic inverse variance methods to synthesize quantitative data, followed by a leave-one-out method for sensitivity analysis. The systematic review registration number was: CRD42016039457. From a total of 425 entries identified via searches, 20 studies were included in the final analysis. The meta-analysis indicated a significant reduction in serum CRP following probiotic administration with a weighted mean difference (WMD) of −1.35 mg/L, (95% confidence interval (CI) −2.15 to −0.55, I2 65.1%). The WMDs for interleukin 10 (IL10) was −1.65 pg/dL, (95% CI −3.45 to 0.14, I2 3.1%), and −0.45 pg/mL, (95% CI −1.38 to 0.48, I2 10.2%) for tumor necrosis factor alpha (TNF-α). These findings were robust in sensitivity analyses. This meta-analysis suggests that probiotic administration may significantly reduce serum CRP while having no significant effect on serum IL10 and TNF-α.
Prebiotics may reduce serum concentrations of C-reactive protein and ghrelin in overweight and obese adults: a systematic review and meta-analysis
Context
Biochemical markers correlate positively with the development and severity of obesity, depression, and anxiety, and can be modulated by changes in intestinal microbiota composition.
Objective
A systematic review and meta-analysis was conducted to determine the effects of prebiotics or synbiotics on blood biomarkers of obesity, depression, and anxiety (including: ACTH [adrenocorticotropic hormone], cortisol, leptin, ghrelin, TSH [thyroid-stimulating hormone], PTH [parathyroid hormone], vitamin D, BDNF [brain-derived neurotrophic factor], and PCR [polymerase chain reaction]) in individuals with overweight or obesity.
Study Selection
RCT in individuals with overweight or obesity, supplemented with prebiotics or synbiotics, assessing any of the outcomes of interest.
Results
Thirteen studies were identified up to March 7, 2018. Regarding outcomes, 1 study assessed leptin, 4 studies assessed ghrelin, and 10 studies assessed CRP (C-reactive protein). Meta-analysis showed reduction in serum concentrations of ghrelin (−37.17 pg/mL; 95%CI = −69.62, −4.73; P = 0.025) and CRP (SMD [standardized mean difference] = −0.31; 95%CI = −0.58, −0.04; P = 0.027) after supplementation of inulin-type fructans.
Conclusions
Prebiotics may help regulate blood concentrations of ghrelin and CRP in overweight or obese individuals.
Short-chain fatty acids, prebiotics, synbiotics, and systemic inflammation: A systematic review and meta-analysis, 2017
Background: Prebiotic soluble fibers are fermented by beneficial bacteria in the colon to produce short-chain fatty acids (SCFAs), which are proposed to have systemic anti-inflammatory effects. Objective: This review examines the effect of SCFAs, prebiotics, and pre- and probiotic combinations (synbiotics) on systemic inflammation. Design: Relevant English language studies from 1947 to May 2017 were identified with the use of online databases. Studies were considered eligible if they examined the effects of SCFAs, prebiotics, or synbiotics; were delivered orally, intravenously, or per rectum; were on biomarkers of systemic inflammation in humans; and performed meta-analysis where possible. Results: Sixty-eight studies were included. Fourteen of 29 prebiotic studies and 13 of 26 synbiotic studies reported a significant decrease in ≥1 marker of systemic inflammation. Eight studies compared prebiotic and synbiotic supplementation, 2 of which reported a decrease in inflammation with synbiotics only, with 1 reporting a greater anti-inflammatory effect with synbiotics than with prebiotics alone. Meta-analyses indicated that prebiotics reduce C-reactive protein (CRP) [standardized mean difference (SMD): -0.60; 95% CI: -0.98, -0.23], and synbiotics reduce CRP (SMD: -0.40; 95% CI: -0.73, -0.06) and tumor necrosis factor-α (SMD -0.90; 95% CI: -1.50, -0.30). Conclusions: There is significant heterogeneity of outcomes in studies examining the effect of prebiotics and synbiotics on systemic inflammation. Approximately 50% of included studies reported a decrease in ≥1 inflammatory biomarker. The inconsistency in reported outcomes may be due to heterogeneity in study design, supplement formulation, dosage, duration, and subject population. Nonetheless, meta-analyses provide evidence to support the systemic anti-inflammatory effects of prebiotic and synbiotic supplementation.
Butyrate, a metabolite of intestinal bacteria, enhances sleep
Emerging evidence suggests that the intestinal microbiota is a source of sleep-promoting signals. Bacterial metabolites and components of the bacterial cell wall are likely to provide important links between the intestinal commensal flora and sleep-generating mechanisms in the brain. Butyrate is a short-chain fatty acid produced by the intestinal bacteria by the fermentation of nondigestible polysaccharides. We tested the hypothesis that butyrate may serve as a bacterial-derived sleep-promoting signal. Oral gavage administration of tributyrin, a butyrate pro-drug, elicited an almost 50% increase in non-rapid-eye movement sleep (NREMS) in mice for 4 hours after the treatment. Similarly, intraportal injection of butyrate led to prompt and robust increases in NREMS in rats. In the first 6 hours after the butyrate injection, NREMS increased by 70%. Both the oral and intraportal administration of butyrate led to a significant drop in body temperature. Systemic subcutaneous or intraperitoneal injection of butyrate did not have any significant effect on sleep or body temperature. The results suggest that the sleep-inducing effects of butyrate are mediated by a sensory mechanism located in the liver and/or in the portal vein wall. Hepatoportal butyrate-sensitive mechanisms may play a role in sleep modulation by the intestinal microbiota.
Inulin / FOS
Can increasing consumption of FOS and inulin improve health and lifespan? To date, dietary supplementation with inulin has been shown to improve cognitive performance (Messaoudi et al. 2005), and, to reduce cholesterol, triglycerides and body weight, and, improved survival in rats (Rozan et al. 2008). (link)
inulin extends lifespan in fruit fly
Inulin extends lifespan in mice in this 2008 study: link
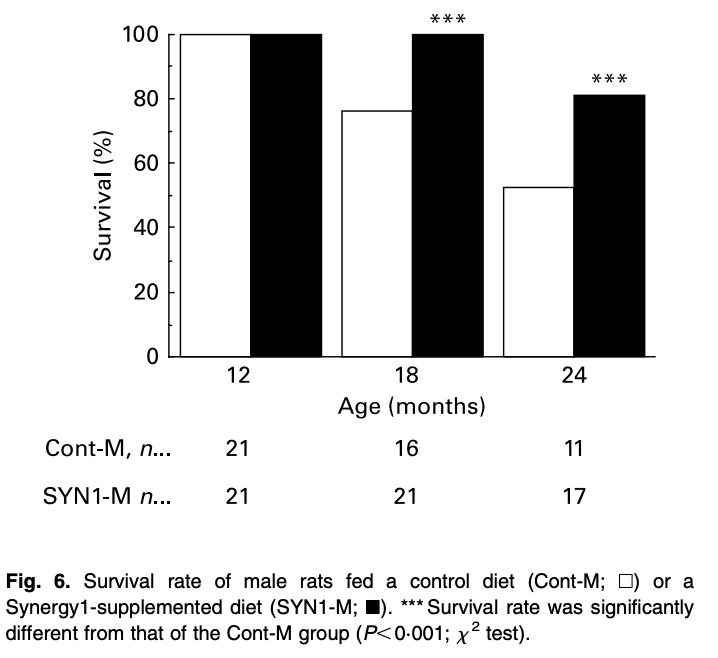
Effects of lifelong intervention with an oligofructose-enriched inulin in rats on general health and lifespan, Rozan 2008
Ageing is associated with changes in physiology and morphology; nutritional strategies to decrease morbidity and to prolong life are of high interest. The aim of the study was to investigate the effects of lifelong supplementation with an oligofructose-enriched inulin on morphological and biological markers and lifespan in male and female rats. Male and female rats, age 3 months, were randomised into two groups to receive either a diet with 10 % of an oligofructose-enriched inulin (Synergy 1) or a standard diet (control) for 27 months. The rats were weighed every 2 weeks and their food intake was evaluated on four successive days every 4-6 weeks. Samples were taken at 12, 18 and 24 months of age. During the whole intervention period, male rats receiving Synergy 1 (SYN1-M) displayed lower body weight, cholesterol and plasma triacylglycerolaemia compared with the controls (Cont-M). The survival rate at 24 months of age of SYN1-M rats was 35.3 % greater than that of Cont-M rats. In female rats, the Synergy 1 supplementation (SYN1-F) group also reduced body weight, cholesterol and triacylglycerolaemia levels, but results were less consistent over the experiment. The survival rate at 24 months of age in SYN1-F rats was 33.3 % greater compared with that of the control (Cont-F) group. To conclude, lifelong intervention with Synergy 1 improved biological markers during ageing and survival rate (lifespan) of rats.

In ITP, these was no effect on mice lifespan: paper, curves.
[NEGATIVE] Gut Bacteria Link Dietary Fiber with Liver Cancer (link)
Mice developed liver cancer (hepatocellular carcinoma; HCC) when fed on diets fortified with refined soluble fibers such as inulin, a probiotic that earlier this year was FDA approved to be marketed as health-promoting.
The discovery puts a question mark over the practice of adding refined fibers to processed foods, the authors suggest. “The results shook us,” comments Dr. Vijay-Kumar. Reporting their findings in Cell (“Dysregulated microbial fermentation of soluble fiber induces cholestatic liver cancer”) the authors conclude, “… benefits notwithstanding, enrichment of foods with fermentable fiber should be approached with great caution as it may increase risk of HCC.”
Mice that were prone to HCC exhibited gut altered gut microbiota, or dysbiosis, characterized by increased fiber-fermenting bacteria and proteobatceria, and this suggested a link between inulin, bacterial fermentation, and HCC. The possibility of an association was strengthened by the finding that inulin-fed mice that were treated using broad-spectrum antibiotics to reduce gut bacteria didn’t develop HCC. Germ-free mice that completely lacked gut bacteria were also free from liver cancer after being fed an inulin-enriched diet. And when the scientists added dietary beta-acids derived from the hop plant Humulus lupulus, to inhibit fermentation, inulin-fed mice were again spared from developing liver cancer.
[NEGATIVE] Beneficial and detrimental effects of processed dietary fibers on intestinal and liver health: health benefits of refined dietary fibers need to be redefined!, 2020
Consumption of processed foods—which are generally composed of nutritionally starved refined ingredients—has increased exponentially worldwide. A rise in public health awareness that low fiber intake is strongly linked to new-age disorders has spurred food manufacturers to fortify processed foods with refined dietary fibers (RDFs). Consumption of whole foods rich in natural fibers undoubtedly confers an array of health benefits. However, it is not clear whether RDFs extracted from the whole plant, kernel, and fruit peels exert similar physiological effects to their naturally occurring counterparts. Recent studies caution that RDFs are not universally beneficial and that inappropriate consumption of RDFs may risk both gastrointestinal and liver health. Herein, we briefly summarize the beneficial and detrimental effects of RDFs on digestive health and discuss the contribution of metabolites derived from microbial fermentation of RDFs in driving such positive or negative health outcomes.
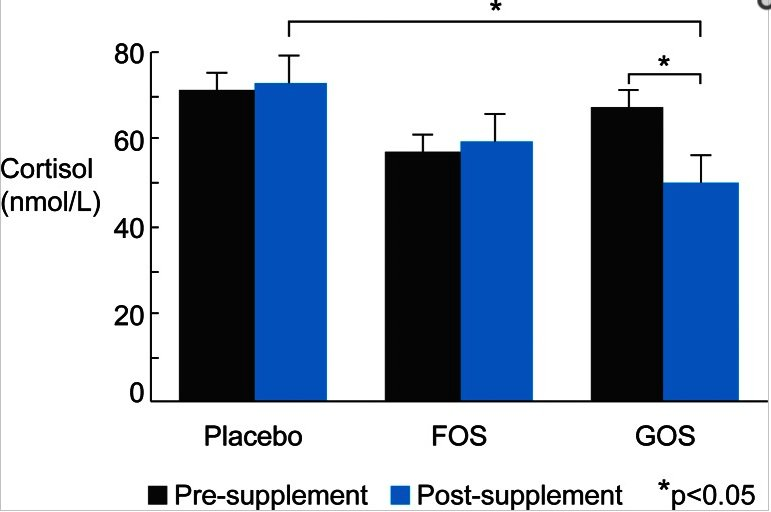
Prebiotic intake reduces the waking cortisol response and alters emotional bias in healthy volunteers, 2015
Forty-five healthy volunteers received one of two prebiotics (fructooligosaccharides, FOS, or Bimuno®-galactooligosaccharides, B-GOS) or a placebo (maltodextrin) daily for 3 weeks.
Eating resistant starch may help reduce red meat-related colorectal cancer risk, 2014, foundmyfitness
300 g of lean red meat per day for 4 weeks increased levels of a biomarker that is linked to cancer development & progression but consuming 40 g of resistant starch along with red meat completely negated this increase.
Dietary prebiotics improve sleep, buffer impacts of stress, says study, 2017
Fiber affecting sleep: prebiotics such as fermentable fiber found in veggies, fruits, and nuts improve sleep in rats
Rhonda Patrick Supplements List – Updated June 2022
Probiotics – Visbiome Probiotic sachets – 1 sachet/every 1-2 weeks
The Effectiveness of Synbiotic Preparation Containing Lactobacillus and Bifidobacterium Probiotic Strains and Short Chain Fructooligosaccharides (FOS) in Patients with Diarrhea Predominant Irritable Bowel Syndrome—A Randomized Double-Blind, Placebo-Controlled Study, 2020
The purpose of the randomized double-blind placebo-controlled trial was to assess the effectiveness of synbiotic preparation containing probiotic Lactobacillus rhamnosus FloraActive™ 19070-2, Lactobacillus acidophilus DSMZ 32418, Bifidobacterium lactis DSMZ 32269, Bifidobacterium longum DSMZ 32946, Bifidobacterium bifidum DSMZ 32403 and fructooligosaccharides (FOS) in adult patients with diarrhea-dominant IBS (IBS-D). The study included eighty patients with moderate and severe IBS-D who were randomized to receive synbiotics or placebo for eight weeks. Finally, a total of sixty-eight patients finished the study. The primary endpoints included the assessment of the symptoms’ severity with IBS symptom severity scale (IBS-SSS), an improvement of IBS global symptoms with Global Improvement Scale (IBS-GIS) and adequate relief of symptoms after four and eight weeks of therapy. Secondary endpoints, which were collected by telephone interviewers three times a week included the assessment of individual IBS symptoms and adverse events. Synbiotic treatment in comparison to placebo significantly improved IBS-GIS (p = 0.043), and IBS-SSS score inducing a decrease in the total IBS-SSS (p = 0.042) and in domain-specific scores related to flatulence (p = 0.028) and bowel habit (p = 0.028) after four and eight weeks. Patients treated with synbiotics reported in weekly observations a significant amelioration in a feeling of incomplete bowel movements, flatulence, pain, stool pressure and diarrheal stools compared to those receiving placebo. There were no differences in adverse events between both groups. Concluding, the multi-strain synbiotic preparation was associated with a significant improvement in symptoms in IBS-D patients and was well-tolerated. These results suggest that the use of synbiotics offers a benefit for IBS-D patients.
Fructooligosaccharides (FOS) on inflammation, immunomodulation, oxidative stress, and gut immune response: a systematic review, 2022
Studies published between December 2000 and January 2020 were systematically searched in four databases: MEDLINE, LILACS, Web of Science, and Scopus. After the screening of 1316 articles, 8 human studies and 20 animal models were included.
A qualitative analysis revealed that FOSs can increase bifidobacteria counts and short-chain fatty acids in the gut, stimulate IgA secretion in the colon, and decrease proinflammatory cytokines, thus influencing metabolic diseases.
Studies suggest that FOS supplementation is positively associated with an anti-inflammatory and antioxidant effect, thus enhancing the gut immune system, which may be beneficial for the host’s health.
[NEGATIVE] Fructooligosaccharide (FOS) and Galactooligosaccharide (GOS) Increase Bifidobacterium but Reduce Butyrate Producing Bacteria with Adverse Glycemic Metabolism in healthy young population, 2017
The gut microbiota has been implicated in glucose intolerance and its progression towards type-2 diabetes mellitus (T2DM). Relevant randomized clinical trial with prebiotic intervention was inadequate. We sought to evaluate the impact of fructooligosaccharides (FOS) and galactooligosaccharides (GOS) on glycemia during oral glucose tolerance test (OGTT) and intestinal microbiota. A randomized double-blind cross-over study was performed with 35 adults treated with FOS and GOS for 14 days (16 g/day). Faeces sampling, OGTT and anthropometric parameters were performed. Short-term intake of high-dose prebiotics had adverse effect on glucose metabolism, as in FOS intervention demonstrated by OGTT (P < 0.001), and in GOS intervention demonstrated by fasting glucose (P < 0.05). A significant increase in the relative abundance of Bifidobacterium was observed both in FOS and GOS group, while the butyrate-producing bacteria like Phascolarctobacterium in FOS group and Ruminococcus in GOS group were decreased. A random forest model using the initial microbiota was developed to predict OGTT levels after prebiotic intervention with relative success (R = 0.726). Our study alerted even though FOS and GOS increased Bifidobacterium, they might have adverse effect on glucose metabolism by reducing butyrate-producing microbes. Individualized prebiotics intervention based on gut microbiome needs to be evaluated in future.
[UNCLEAR] The effects of dietary supplementation with inulin and inulin-propionate ester on hepatic steatosis in adults with non-alcoholic fatty liver disease
The short chain fatty acid (SCFA) propionate, produced through fermentation of dietary fibre by the gut microbiota, has been shown to alter hepatic metabolic processes that reduce lipid storage. We aimed to investigate the impact of raising colonic propionate production on hepatic steatosis in adults with non-alcoholic fatty liver disease (NAFLD). Eighteen adults were randomized to receive 20 g/d of an inulin-propionate ester (IPE), designed to deliver propionate to the colon, or an inulin control for 42 days in a parallel design. The change in intrahepatocellular lipid (IHCL) following the supplementation period was not different between the groups (P = 0.082), however, IHCL significantly increased within the inulin-control group (20.9% ± 2.9% to 26.8% ± 3.9%; P = 0.012; n = 9), which was not observed within the IPE group (22.6% ± 6.9% to 23.5% ± 6.8%; P = 0.635; n = 9). The predominant SCFA from colonic fermentation of inulin is acetate, which, in a background of NAFLD and a hepatic metabolic profile that promotes fat accretion, may provide surplus lipogenic substrate to the liver. The increased colonic delivery of propionate from IPE appears to attenuate this acetate-mediated increase in IHCL.
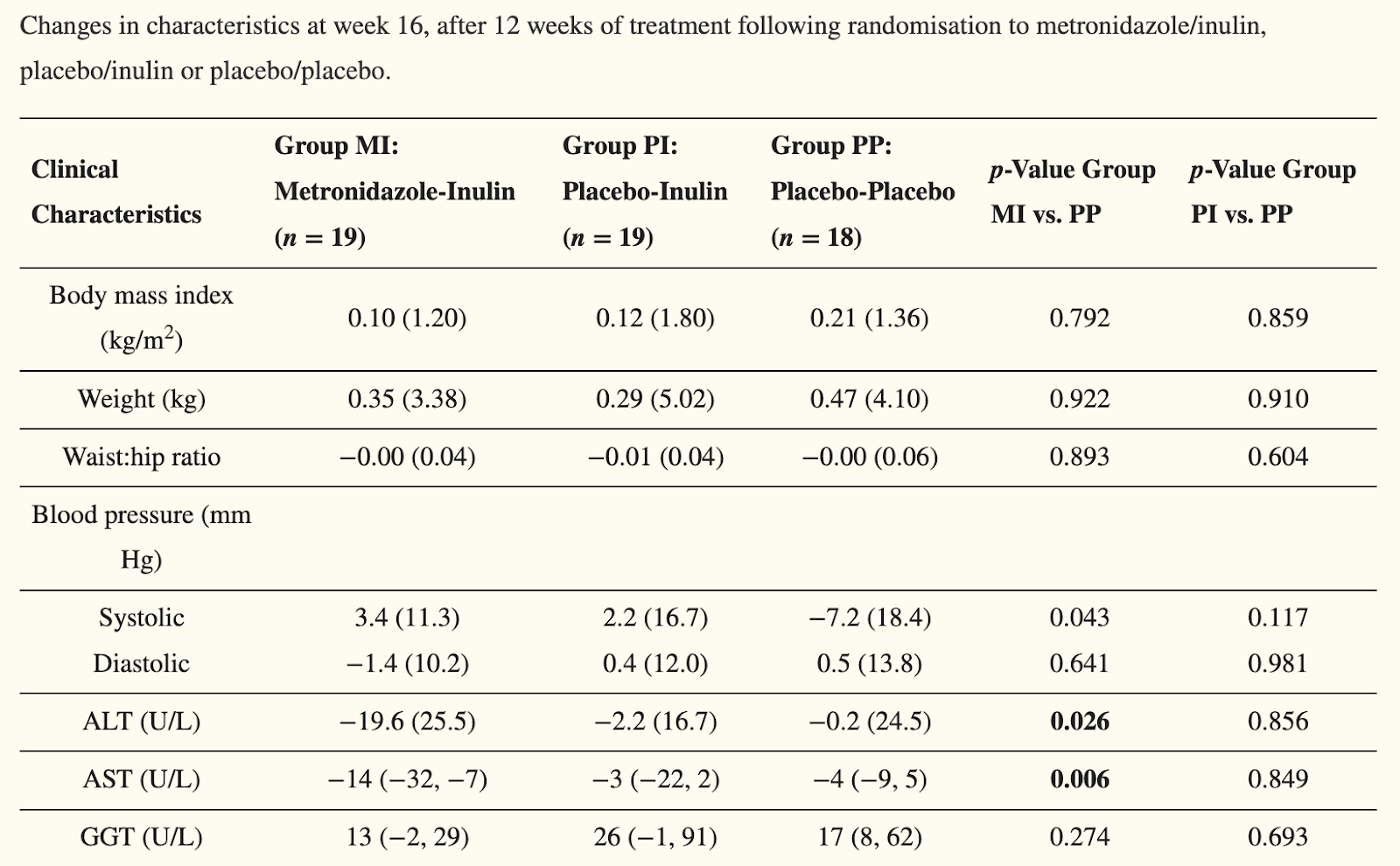
Randomised Double-Blind Placebo-Controlled Trial of Inulin with Metronidazole in Non-Alcoholic Fatty Liver Disease (NAFLD), 2020


Comments