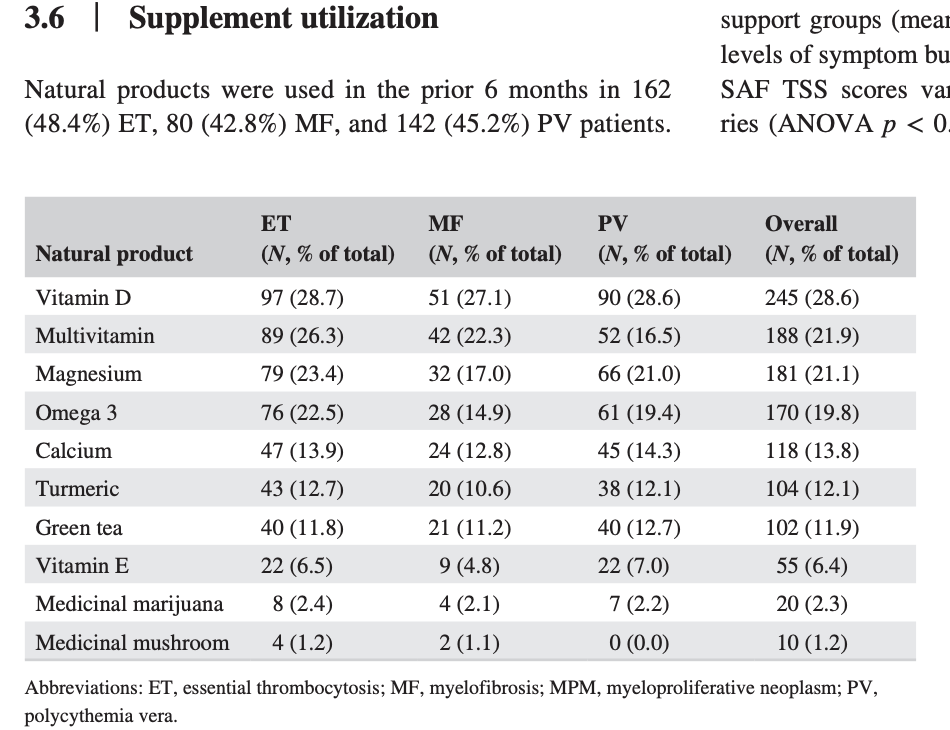
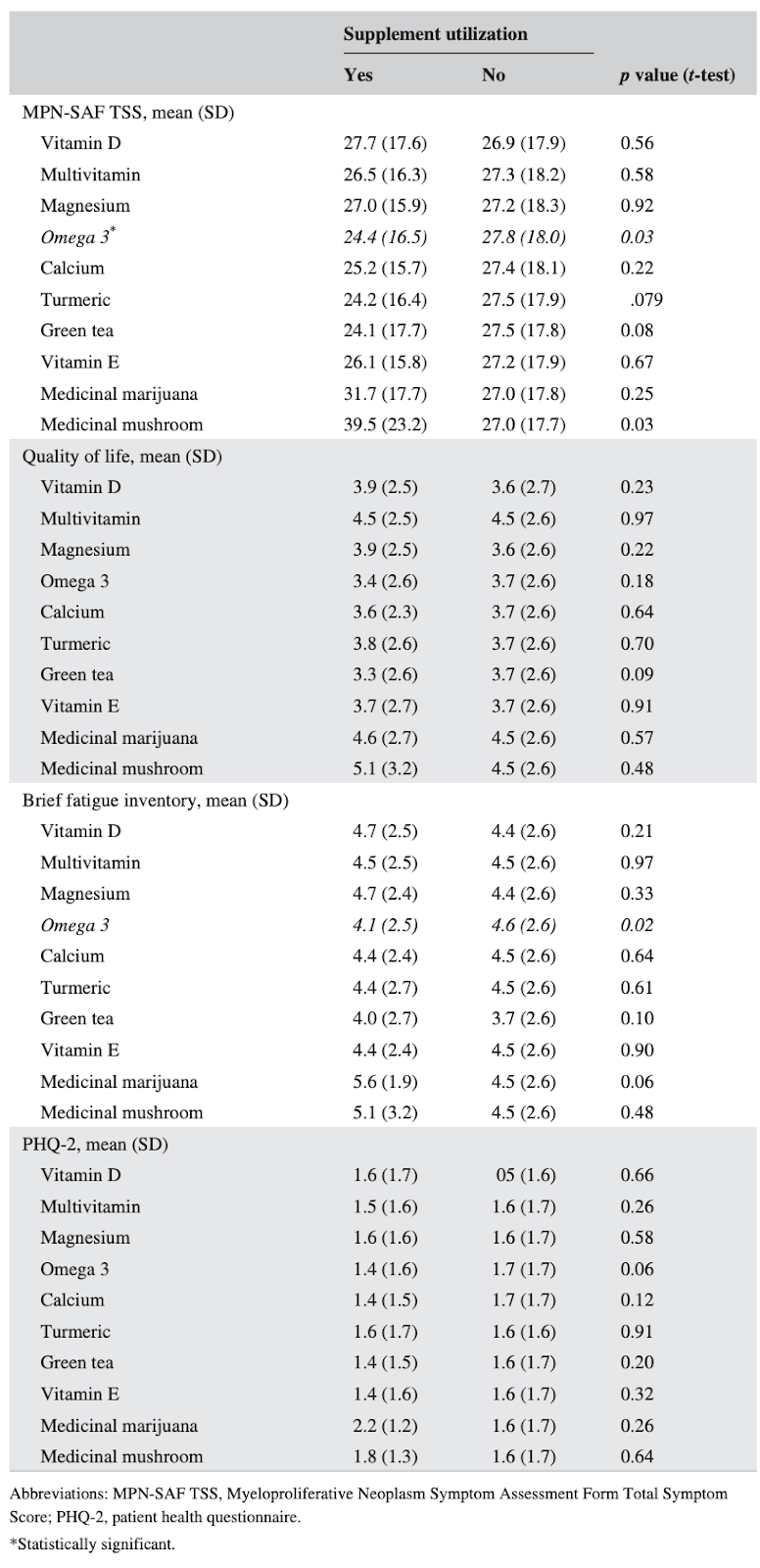
Fish oil
Associated with reduced symptom burden and improved well being scores in MPN.
Helps with Depression: EPA is effective in the prevention of depression receiving IFN-α therapy. 66% reduction in risk of depression (p = .037)
Reduces platelet aggregation, coagulation and thrombosis.
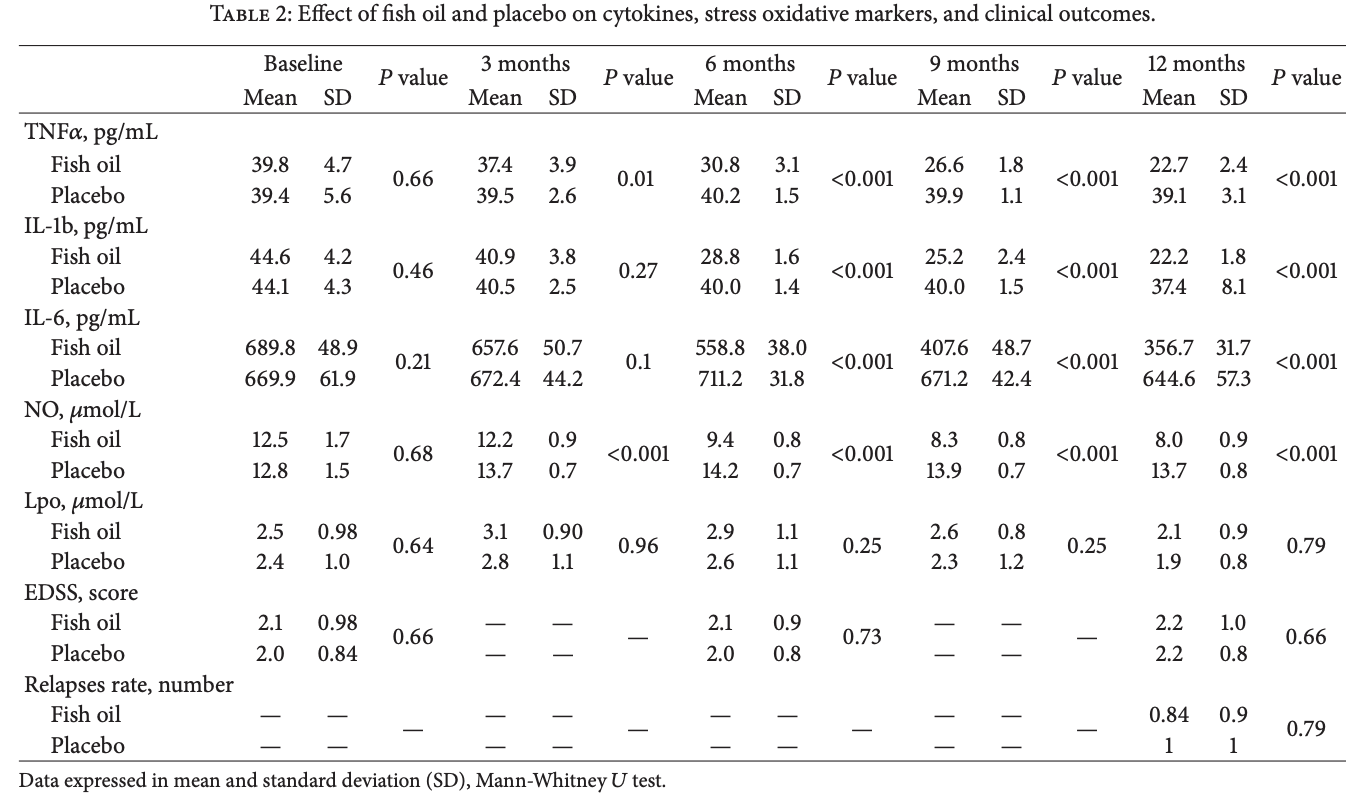
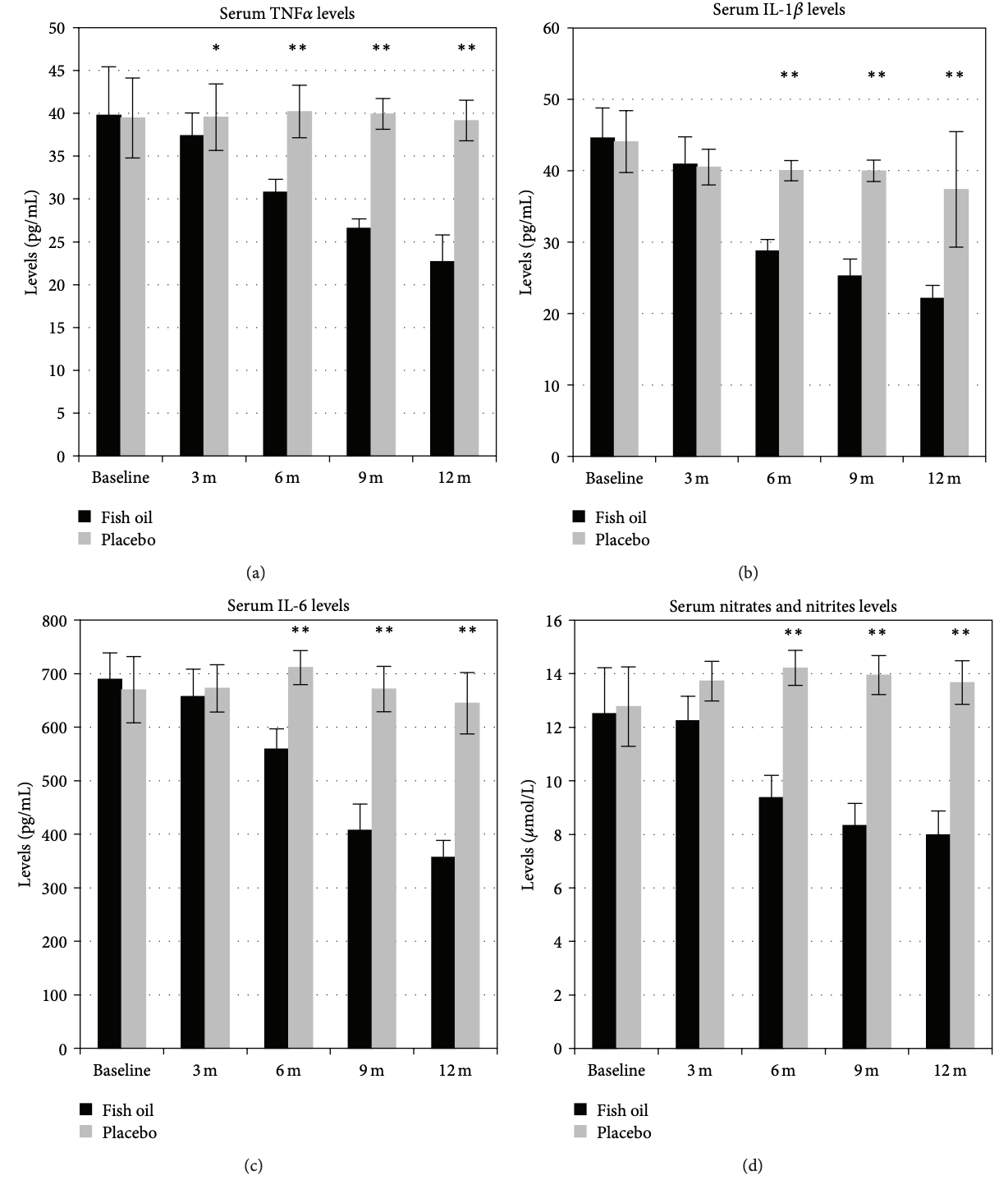
Decreased the serum levels of TNF α , IL-1 β , IL-6, and nitric oxide metabolites over up to 6 months upon continuous use in one study.
In hypertensives, supplementation resulted in lower SBP 2.56 mmHg (95% CI 0.58 to 4.53) and DBP 1.47 mmHg (95% CI 0.41 to 2.53).
Lowers nuclear factor-kappa B (NF-κB) gene expression.
Inhibited Interferon-mediated NF-κB activation and enhanced apoptotic cell death in IFN-treated cells.
Improved chemotherapy tolerability and cancer patient outcomes in a meta-analysis.
STAT3 Inhibitor: DHA acid inhibits the phosphorylation of STAT3 and the growth and invasion of renal cancer cells (RCC).
Has JAK2 inhibiting effects: Not the strongest JAK2 inhibitor, but it does inhibit in cell studies.
Associated with reduced mortality from all causes: High w3 in blood is associated with reduced mortality from all causes (by 15–18%, p < 0.003).
Fish oil supplementation reduces all cause mortality in a dose dependent manner. Significant heterogeneity exists between study results.
In patients with NAFLD/NASH, Omega-3 PUFAs statistically improved improved liver fat, GGT (-9.02 MD), TG (-35.55 MD), and HDL (+5.51 MD). Improvements in ALT and AST weren’t statistically significant; ALT (MD = −4.97, 95% CI: −11.14 to 1.20, P = 0.11); AST (MD = −2.01, 95% CI: −8.72 to 4.70, P = 0.58).
DHA kills AML Cells: DHA was able to kill AML cells without harming hematopoietic stem cells in a cell culture experiment (Yamagami 2009).
Increases chemo effectiveness in In CLL patients: Omega-3 fatty acids, in daily doses escalating from 2.4 g to 7.2 g, suppressed activation of the inflammatory regulator NF-κB and increased sensitivity of subjects’ lymphocytes to the chemotherapeutic drug doxorubicin (Fahrmann 2013).
Hematological Malignancies: Small prospective study with 22 participants. Survival was significantly better in the fish oil vs control group at 14 months, and the fish oil group received more chemotherapy sessions than the control group.
Associated with reduced occurrence of RCC: Compared with no fish consumption, HR was 0.56 (95%, 0.35-0.91) for women eating fatty fish once a week or more.
Prevents breast cancer cell metastasis to bone in mice.
DHA acts as poison to some tumor cells.
Negative: Doubles the chances of arrhythmia (afib) at high doses (4g/day)
The SIMM study: Survey of integrative medicine in myeloproliferative neoplasms (link)
Omega-3 fatty acids in the prevention of interferon-alpha-induced depression: results from a randomized, controlled trial. 2014
Background: Interferon (IFN)-α therapy for chronic hepatitis C virus infection is frequently associated with depression. The routine prophylaxis with antidepressants might expose patients to adverse effects, hence, the need for alternative preventive interventions. Omega-3 polyunsaturated fatty acids are safe and effective essential nutritional compounds used for the treatment of depression, putatively through an anti-inflammatory action. In addition, lower erythrocyte levels of omega-3 polyunsaturated fatty acids have been associated with an increased risk of IFN-induced depression.
Methods: We conducted a 2-week, double-blind, placebo-controlled trial comparing eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and placebo for the prevention of IFN-α-induced depression. A total of 162 patients consented to participate and were randomized to the study. All of the patients completed the 2-week trial; 152 participants were followed throughout the 24 weeks of IFN-α treatment and were included in the analysis.
Results: Compared with placebo, the incident rates of IFN-α-induced depression were significantly lower in EPA-treated but not in DHA-treated patients (10% and 28%, respectively, versus 30% for placebo, p = .037). Both EPA and DHA significantly delayed the onset of IFN-induced depression (week of onset: 12.0 and 11.7, respectively, versus 5.3 for placebo, p = .002). EPA and DHA were both well tolerated in this population. EPA treatment increased both EPA and DHA erythrocyte levels, but DHA only increased DHA erythrocyte levels.
Conclusions: EPA is effective in the prevention of depression in hepatitis C virus patients received IFN-α therapy. Our study confirms the notion that anti-inflammatory strategies are effective antidepressants in the context of depression associated with inflammation.
Importance of maintaining a low omega-6/omega-3 ratio for reducing platelet aggregation, coagulation and thrombosis
The idea that long-chain marine omega-3s can prevent cardiovascular disease is decades old. This idea began with the Greenland Inuit who were noted to have a lower risk of cardiovascular disease.1 Indeed, the Inuit, with their high intake of long-chain omega-3s, have been noted to have a lower platelet count, reduced platelet reactivity, prolonged bleeding times and a lower ratio of proaggregatory thromboxanes versus antiaggregatory prostacyclins.2 And it has been known for a long time that marine omega-3s (from salmon, mackerel, fish oil or cod liver oil) inhibit platelet aggregation.
Omega-3s reduce platelet aggregation, coagulation and thrombosis
Clinical studies in humans clearly show that marine omega-3s provide antiplatelet effects. Indeed, a meta-analysis of 15 randomised controlled trials (RCT) in humans has confirmed that omega-3 polyunsaturated fatty acids (PUFA) inhibit platelet aggregation.3 Marine omega-3 PUFAs also may help overcome aspirin resistance.4 In healthy borderline overweight men, 3 g of omega-3 PUFAs for 4 weeks lowered fibrinogen, thrombin and factor V levels; these benefits occurred mainly in those with high fibrinogen carrying alpha-chain fibrinogen polymorphism.5
Marine omega-3s also have the ability to reduce von Willebrand factor (vWF; a platelet activator factor), whole blood viscosity, and can improve red blood cell flexibility (deformability).6 7 In a 5-week double-blind placebo-controlled study in 30 healthy subjects, 2.52 g/day of omega-3 PUFAs as compared with 1.26 g/day, significantly decreased plasma viscosity, red blood cell rigidity and systolic blood pressure.8 Thus, higher doses of marine omega-3 seem to be more effective antithrombotic benefits.
One study in healthy adults found that fish oil (providing 6 g of eicosapentaenoic acid (EPA)/day), but not vegetable oil, reduced platelet adhesiveness.9 In another study, supplementation with 3.6 g of omega-3 PUFA from fish oil reduced platelet aggregation, whereas 25 g of soy lecithin (providing 1.5 g omega-6, 0.5 g omega-3) increased platelet reactivity; no effect was found in the control group.10 The omega-6/omega-3 ratio in platelets is also positively correlated with platelet adhesion at rest and after ADP and thrombin platelet stimulation. Another study found that plasminogen activator inhibitor-1 (PAI-1, an inhibitor of fibrinolysis) can be lowered in those consuming fish oil, suggesting a decreased risk of thrombosis.11
In general, approximately 2–4 g of EPA/docosahexaenoic acid (DHA) per day is needed to provide the full antiatherosclerotic, anti-inflammatory and antiplatelet benefits.12 Even plant omega-3s seem to have some benefit in this regard, whereas omega-6 may have a detrimental effect. Indeed, on a diet high in monounsaturated fatty acids (MUFA), as the omega-6 linoleic acid (LA)/omega-3 alpha linolenic acid (ALA) ratio decreases, platelet aggregation decreases.13 In vitro platelet aggregation to both ADP and collagen is even increased after sunflower and rapeseed oil compared with a diet enriched in milk fat.14 This suggests that even compared with saturated fat, a diet high in omega-6 PUFA may actually increase platelet aggregation.
In 24 healthy young males, a Mediterranean diet has been found to reduce the thrombotic state (decreased plasma vWF, tissue factor pathway inhibitor and tissue PAI-1).15 Oleic acid may provide similar, but slightly less antiplatelet effects as long-chain marine omega-3s since the omega-9 fatty acid eicosatrienoic acid has also been found to reduce the production of thromboxane-B2 (TXB2), which is the inactivated metabolite of TXA2 (a platelet activator).16 Moreover, in another study, TXB2 production in platelets was reduced with olive oil supplementation but not with a corn oil-enriched diet.16 Animal studies confirm a reduction in TXB2 with the use of olive oil, an effect which is greater than that found with sunflower oil.17 Another study found a reduction in thromboxane production (urinary excretion of the TXB2 metabolite 11-dehydro-TXB2) with saturated fat and MUFA versus omega-6 PUFA.18 A Mediterranean diet high in MUFA reduces vWF (which is derived from the endothelium and is important in the coagulation process during a platelet thrombus) and PAI-1.15 19
The type of long-chain marine omega-3 may also affect the antiplatelet effects of marine omega-3s. Indeed, platelet aggregation in response to collagen is reduced in just 6 days after pure EPA consumption but platelet response to ADP is not reduced until after at least 4 weeks of intake; however, the inhibition of platelet aggregation with DHA (6 g/day) to both stimuli occurs in just 6 days.20 Thus, both EPA and DHA inhibit platelet aggregation; however, DHA has a faster onset of action in regard to inhibiting ADP-induced platelet aggregation.
Both EPA and DHA get incorporated into platelet phospholipids at the expense of arachidonic acid (AA), which may help reduce platelet aggregation via a reduction in AA-derived platelet-aggregating/procoagulant metabolites. Additionally, EPA competes with AA for cyclo-oxygenase reducing its action on AA. Thus, EPA both directly and indirectly reduces the formation of the AA proaggregatory metabolite TXA2.20 EPA/DHA also gets incorporated into neutrophils and red blood cells at the expense of both LA and AA. The incorporation of omega-3s in red blood cells seems to decrease whole blood viscosity and increase red blood cell flexibility thus likely reducing the risk of thrombosis.6 7
Daily supplementation with 3 g of EPA/DHA for 12 weeks, and especially after 18 weeks, inhibits tissue factor activity in adherent monocytes (a catalyst in the coagulation cascade); this benefit also occurs after 24 weeks in those with hypertriglyceridaemia.21 Thus, the antithrombotic effects of omega-3s in clinical studies may need to be tested for a minimum of 18 weeks in healthy patients and even longer (for 24 weeks) in those with hypertriglyceridaemia.
One study in healthy young men found that both lean meat and fish have antithrombotic effects although some prothrombotic effects (such as an increase in PAI-1) were also noted with increased fish intake.22 A decrease in platelet aggregation but an increase in PAI-1 has sometimes been noted with fish oil supplementation. This increase in PAI-1 may actually occur to naturally counteract any excessive inhibition in the coagulation cascade, which is why supplementing with marine omega-3s is not associated with a significant increase in major or clinically significant bleeds. And considering that marine omega-3s consistently lower the risk of thrombotic events,12 23 there does not appear to be increased coagulation but a decrease. Interestingly, supplementing the diet with olive oil or consuming fish on top of a MUFA-enriched Mediterranean diet has been found to decrease PAI-1.15 24
One double-blind placebo-controlled trial in 59 patients with hypertension with type 2 diabetes compared 4 g/day of EPA, 4 g/day of DHA or 4 g/day of olive oil (‘placebo’) for 6 weeks.25 DHA, but not EPA, significantly reduced collagen aggregation and TXB2 versus placebo (p=0.05 and p=0.03, respectively). The authors concluded, ‘Highly purified DHA may be a more effective anti-thrombotic agent than EPA.’ Thus, supplementing patients with type 2 diabetes with 4 g of DHA per day may be particularly effective for quickly reducing platelet aggregation, reversing impaired fibrinolysis and improving endothelial dysfunction.25 Even so, the REDUCE-IT study found a significant reduction in cardiovascular events in high-risk patients using 4 g of EPA per day.26
The endothelial production of nitric oxide, prostacyclin and tissue-plasminogen activator is very important for preventing platelet aggregation and acute cardiovascular events.27 By damaging the endothelium, consuming isolated sources of LA may actually induce a hypercoagulable state, whereas fish oil has been shown to improve endothelial function28 and enhance fibrinolytic activity.29 DHA, but not EPA, has been found to improve endothelial function, which may be why DHA has been found to have better antihypertensive effects.30 Importantly, in healthy patients, a DHA dose of 6 g/day may be required to significantly reduce platelet aggregation31 32 as 1.62 and 1.68 g of DHA/day have been found ineffective in this regard.33 34
Supplementing the diet with 500 g (about 17.5 oz) of oily fish per week for 4 weeks significantly reduces platelet-monocyte aggregates by 35% versus control, which reverted back to baseline values 4 weeks after discontinuation.35 Platelet-monocyte aggregates may promote atherosclerosis and induce inflammatory cytokine, chemokine and adhesion molecule expression. In fact, the authors concluded, ‘Our results suggest that reduced platelet activation could represent an important mechanism through which dietary fish confer their putative cardiovascular benefits.’35 EPA has also been found to reduce P-selectin, oxidised low-density lipoprotein (LDL) antibodies and glycoprotein IIb/IIIa expression on platelets.36 Another report found that 6.6 g of omega-3 PUFA reduces serum P-selectin expression suggesting a decrease in platelet activation.37 The authors noted, ‘Most previous studies assessing the effects of fish oils on platelet function have used older techniques with limited reproducibility and physiological relevance.’37
Omega-3 Index (link)
@PeterAttiaMD
Very high quality pooled meta-analysis of omega-3 fatty acids just published by Bill Harris et al.
I’m still in the camp at higher levels of RBC EPA/DHA are important and target a minimum of 8% in my patients, and ideally north of 10%.
@Ping Long
- my last test showed a 14%. I guess that might be too high, so I reduced intake somewhat.
- Forgot what was your dose and brand. (I know you massively lowered your HS-CRP 🙂 ).
- I was taking Nordic naturals, Carlson liquid forms, 5-6 g per day, mostly to reduce LP(a). Nowadays I mostly take smash fishes.
Efficacy of fish oil on serum of TNF α , IL-1 β , and IL-6 oxidative stress markers in multiple sclerosis treated with interferon beta-1b
Multiple sclerosis (MS) is a chronic inflammatory disease, which leads to focal plaques of demyelination and tissue injury in the central nervous system. Oxidative stress is also thought to promote tissue damage in multiple sclerosis. Current research findings suggest that omega-3 polyunsaturated fatty acids (PUFAs) such as eicosapenta-enoic acid (EPA) and docosahexaenoic acid (DHA) contained in fish oil may have anti-inflammatory, antioxidant, and neuroprotective effects. The aim of the present work was to evaluate the efficacy of fish oil supplementation on serum proinflammatory cytokine levels, oxidative stress markers, and disease progression in MS. 50 patients with relapsing-remitting MS were enrolled. The experimental group received orally 4 g/day of fish oil for 12 months. The primary outcome was serum TNF α levels; secondary outcomes were IL-1 β 1b, IL-6, nitric oxide catabolites, lipoperoxides, progression on the expanded disability status scale (EDSS), and annualized relapses rate (ARR). Fish oil treatment decreased the serum levels of TNF α , IL-1 β , IL-6, and nitric oxide metabolites compared with placebo group (P ≤ 0.001). There was no significant difference in serum lipoperoxide levels during the study. No differences in EDSS and ARR were found.
Conclusion: Fish oil supplementation is highly effective in reducing the levels of cytokines and nitric oxide catabolites in patients with relapsing-remitting MS.
IFNα/β promotes cell survival by activating NF-κB
IFNs play critical roles in host defense by modulating the expression of various genes via signal transducer and activator of transcription factors. We show that IFNα/β activates another important transcription factor, NF-κB. DNA-binding activity of NF-κB was induced by multiple type 1 IFNs and was promoted by IFN in a diverse group of human, monkey, rat, and murine cells. Human IFN promoted NF-κB activation in murine cells that express the human IFNα/β receptor-1 signal-transducing chain of the type 1 IFN receptor. IFN promotes inhibitor of kappa B α (IκBα) serine phosphorylation and degradation, and stimulates NF-κB DNA-binding and transcriptional activity. Importantly, IFN promotes cell survival by protecting cells against a variety of proapoptotic stimuli, such as virus infection and antibody-mediated crosslinking. Expression of superrepressor forms of IκBα, besides inhibiting IFN-mediated NF-κB activation and IκBα degradation, also enhanced apoptotic cell death in IFN-treated cells. We conclude that NF-κB activation by IFNα/β is integrated into a signaling pathway through the IFNα/β receptor-1 chain of the type 1 IFN receptor that promotes cell survival in apposition to various apoptotic stimuli.
Omega 3 (n-3) fatty acids down-regulate nuclear factor-kappa B (NF-κB) gene and blood cell adhesion molecule expression in patients with homozygous sickle cell disease, 2015
Chronic inflammation and reduced blood levels of omega-3 fatty acids (n-3) are known characteristics of sickle cell disease (SCD).The anti-inflammatory properties of n-3 fatty acids are well recognized. Omega-3 treated (n = 24), hydroxyurea (HU) treated (n = 18), and n-3 untreated (n=21) homozygous SCD patients (HbSS) and healthy (HbAA) controls (n = 25) matched for age (5-16 years), gender and socioeconomic status were studied. According to age (5-10) or (11-16) years, two or three capsules containing 277.8 mg docosahexaenoic (DHA) and 39.0mg eicosapentaenoic (EPA) or high oleic acid placebo (41%) were assigned to n-3 treated and n-3 untreated groups, respectively. Hydroxyurea treated group was on dosage more than 20 mg/kg/day. The effect of supplementation on systemic and blood cell markers of inflammation was investigated. The n-3 treated group had higher levels of DHA and EPA (p < 0.001) and lower white blood cell count and monocyte integrin (p < 0.05) compared with the n-3 untreated. No difference was detected between the two groups regarding C-reactive protein, granulocytes integrin and selectin, plasma tumour necrosis factor-α and interleukin-10. The n-3 treated group had lowered nuclear factor-kappa B (NF-κB) gene expression compared to n-3 untreated and HU treated groups (p < 0.05). This study provides evidence that supplementation with n-3 fatty acids may ameliorate inflammation and blood cell adhesion in patients with SCD.
Omega-3 decreases interleukin-6 levels in HIV and HHV-8 co-infected patients: results from a randomized supplementation trial in Uganda
Objective
Kaposi sarcoma (KS) is an HIV-associated malignancy caused by human herpesvirus-8 that occurs at highest incidence in sub-Saharan Africa. KS patients often present with inflammatory symptoms associated with higher mortality.
We conducted a double-blind, randomized, placebo-controlled study in Uganda to test whether omega-3 (ω-3) supplementation could reduce inflammation in HIV and HHV-8 co-infected adults ≥18 years of age.
ω-3 participants received a 3-gram pill dose daily for 12 weeks (1.8g eicosapentaenoic acid, 1.2mg docosapentaenoic acid); placebo participants received 44.8mg of high oleic safflower oil.
Inflammatory cytokine interleukin-6 (IL-6) concentrations decreased in ω-3 participants (−0.78 pg/mL) but increased in placebo participants (+3.2 pg/mL;P− =0.04). We observed a trend towards decreased IL-6 after ω-3 supplementation specific to KS patients (N=58;P=0.08). CD8+ counts tended to increase in the ω-3 arm KS patients (+60 cells/mm3), while decreasing (−47 cells/mm3) with placebo (P=0.11).
ω-3 supplementation decreased Il-6 concentrations among HIV and HHV-8 co-infected Ugandans, which may have clinical benefit for KS patients.
Keywords: Kaposi sarcoma, human herpes virus-8, inflammation, omega-3 supplementation, Uganda
Omega-3 supplements for patients in chemotherapy and/or radiotherapy: A systematic review, 2014
Background & aims: Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), in vitro and in vivo, used along with anticancer drugs, have improved cancer treatment outcome. Clinical studies have reported positive results with omega-3 supplements in oncologic patients. We summarized only randomized controlled clinical trials involving the administration of DHA and/or EPA during chemotherapy and/or radiotherapy to assess the effects on treatment outcomes.
Methods: We conducted a systematic literature search using specific terms. Of 157 publications, 10 were selected on the basis of their methodological quality, according to the Oxford Quality Scale and the Cochrane Concealment Assessment. Outcome included body weight and composition, peripheral neuropathy, immune, inflammatory and oxidative status, quality of life, and membrane omega-3 fatty acids incorporation.
Results: Treatment regimens included radiotherapy (1), chemotherapy (8), and chemoradiotherapy (1). The number of patients ranged from 11 to 92 and the daily dose of EPA and/or DHA from 600 mg to 3.6 g. For high quality methodology studies only, the combination of omega-3 fatty acids supplements with conventional chemotherapy was beneficial. None of the studies reported a worse outcome for the supplement patients.
Conclusions: There are beneficial effects of omega-3 fatty acids supplements in patients undergoing chemotherapy and/or radiotherapy on different outcomes, being the preservation of body composition the most evident. Some important outcome like decrease tumor size and prolonging patient survival, are not observed.
n-3 polyunsaturated fatty acid supplementation during cancer chemotherapy, 2016
Abstract
Evidence from several clinical trials suggests that n-3 polyunsaturated fatty acid (n-3 PUFA) supplementation during cancer chemotherapy improves patient outcomes related to chemotherapy tolerability, regardless of the type of chemotherapy used. While the effects of n-3 PUFA supplementation during chemotherapy have been the subject of several reviews, the mechanisms by which n-3 PUFA improve patient responses through improved chemotherapy tolerability are unclear. There are several barriers currently hindering interpretation and comparison of studies, including small sample sizes, poor patient compliance, and variation in supplementation format and dose. Expansion of standard-of-care for specific patient populations to include n-3 PUFA supplementation concurrent with chemotherapy may reduce costs associated with delayed treatment, toxicities and unplanned hospitalization during cancer chemotherapy. The purpose of this review is to identify barriers to understanding mechanisms of host protection, highlight considerations for future clinical trials, as well as to propose potential mechanisms by which n-3 PUFA supplementation improves chemotherapy tolerability and ultimately patient outcomes.
2.1.1. Clinical outcomes
Cancer is an important health issue that influences quality of life and survival. Strikingly, breast cancer patients with high incorporation of supplemented DHA (i.e. extent of DHA increase above the median of 2.5% of total fatty acids) experienced longer time to disease progression (8.7 months vs 3.5 months) and significantly longer survival (34 months vs 18 months) compared to patients with lower incorporation of supplemented DHA [31]. Additionally, lung cancer patients receiving platinum-based doublet chemotherapy with concurrent n-3 PUFA supplementation received more chemotherapy cycles, experienced increased clinical benefit (80% vs 42%) and had a significantly greater tumor response rate compared with the control group (60% vs 26%) [35]. In a clinical pilot trial [29], pancreatic and lung cancer patients receiving an n-3 PUFA enriched oral nutritional supplement (ONS) had a significantly improved performance status, which has been shown to correlate with response and tolerability to chemotherapy, and outcomes in cancer patients [42]. Quality of life evaluates general well-being, and a 10% improvement in quality of life indices is recognized as being clinically significant. Arshad et al. [28] found that over 50% of advanced pancreatic cancer patients who were provided with n-3 PUFA had a 10% or greater improvement in quality of life sustained for at least 4 weeks. Similarly, providing n-3 PUFA to cachectic pancreatic and non-small-cell lung cancer patients [29], [41], and advanced colorectal cancer patients [37] resulted in significantly better quality of life and global health status.
2.1.2. Inflammatory status
Markers of immune and inflammatory status are often altered during the course of chemotherapy [11]. C-reactive protein (CRP) is a commonly used marker of inflammation that has been used to prognosticate several cancers [43], [44], [45], [46]; high levels of CRP indicate a worse prognosis. The CRP/albumin ratio has also been shown to be an independent predictor of overall survival in patients with cancer [47], [48]. N-3 PUFA supplementation in patients with colorectal cancer showed significantly lower CRP [34], [37] and CRP/albumin ratios [34]. Lung cancer patients supplementing with n-3 PUFA also had significantly reduced serum CRP levels after two [38] or three [32] cycles of chemotherapy. In addition to reduced CRP levels, n-3 PUFA supplementation during chemotherapy reduced interleukin-6, tumor necrosis factor-α, neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and maintained neutrophil number and function [30], [32], [38], collectively suggesting reduced pro-inflammatory status in response to n-3 PUFA supplementation.
Docosahexaenoic acid inhibits the phosphorylation of STAT3 and the growth and invasion of renal cancer cells, 2017
Docosahexaenoic acid (DHA) has a variety of anti-tumor activities. The present study examined the anti-tumor activity of DHA in renal cancer cells and its underlying mechanisms of action. The effects of DHA on the viability and proliferation of the human renal cancer cell lines Caki-1 and 786-O were examined by an MTS assay and cell counting. In addition, cell cycle distribution and cell apoptosis were analyzed by flow cytometry and Annexin V staining, and modulation of cell mobility and invasiveness was assessed by wound healing and Matrigel invasion assays. Effects of DHA on intracellular signaling pathways were also analyzed by western blotting. It was observed that DHA significantly reduced the viability and proliferation of Caki-1 and 786-O cells (P<0.01). Specifically, there were increases in the sub-G1 and G2/M cell populations, as well as the percentages of cells exhibiting Annexin-positive and propidium-iodide-negative staining. In addition, the covered area in a wound and the number of cells invading through a Matrigel chamber decreased when Caki-1 or 786-O cells were treated with DHA. Phosphorylation of epidermal growth factor receptor was also upregulated following DHA treatment, while phosphorylation of signal transducer and activator of transcription 3 and Akt was downregulated. Collectively, these data suggest that DHA may be useful in the treatment of renal cell carcinoma.
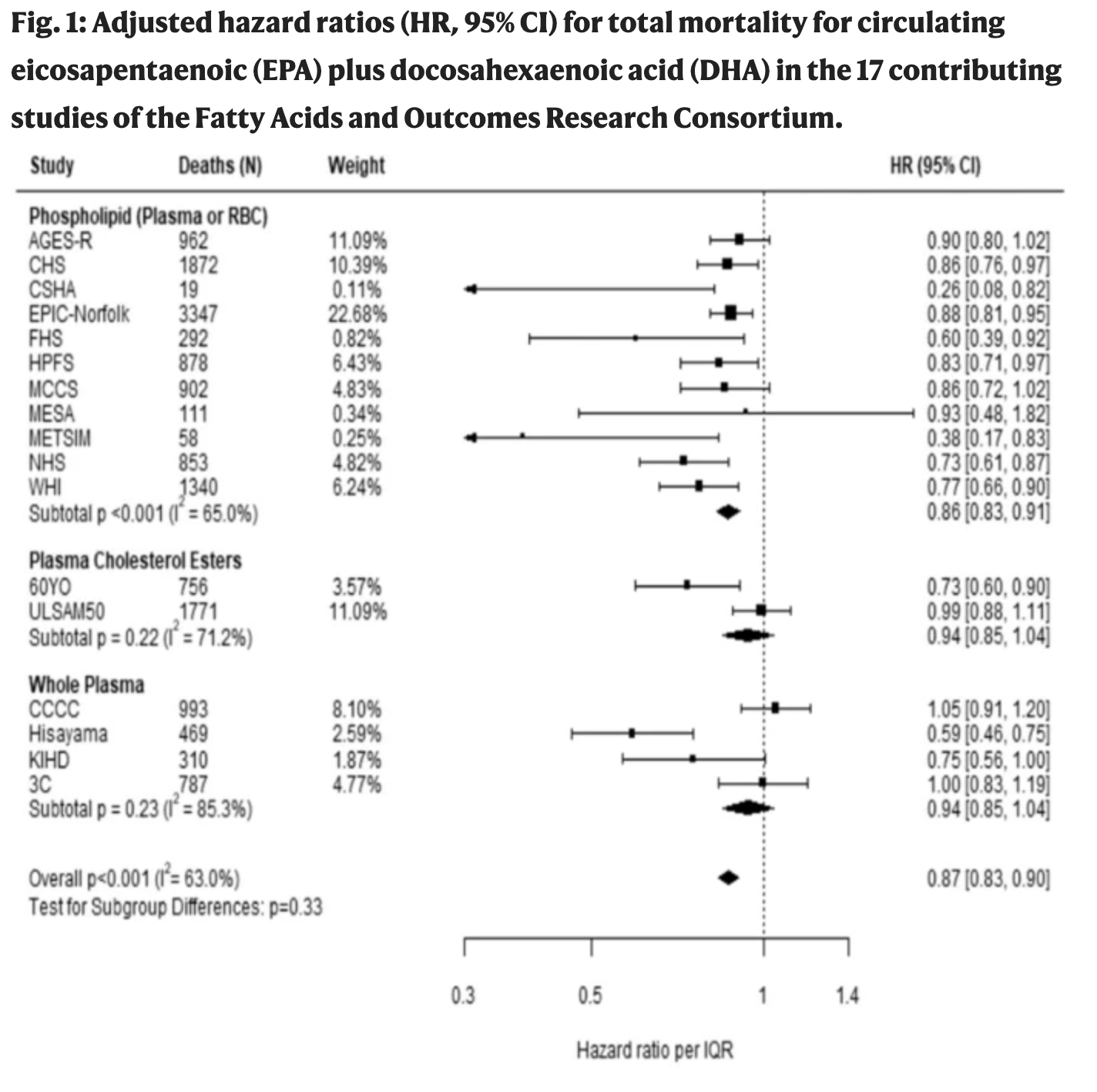
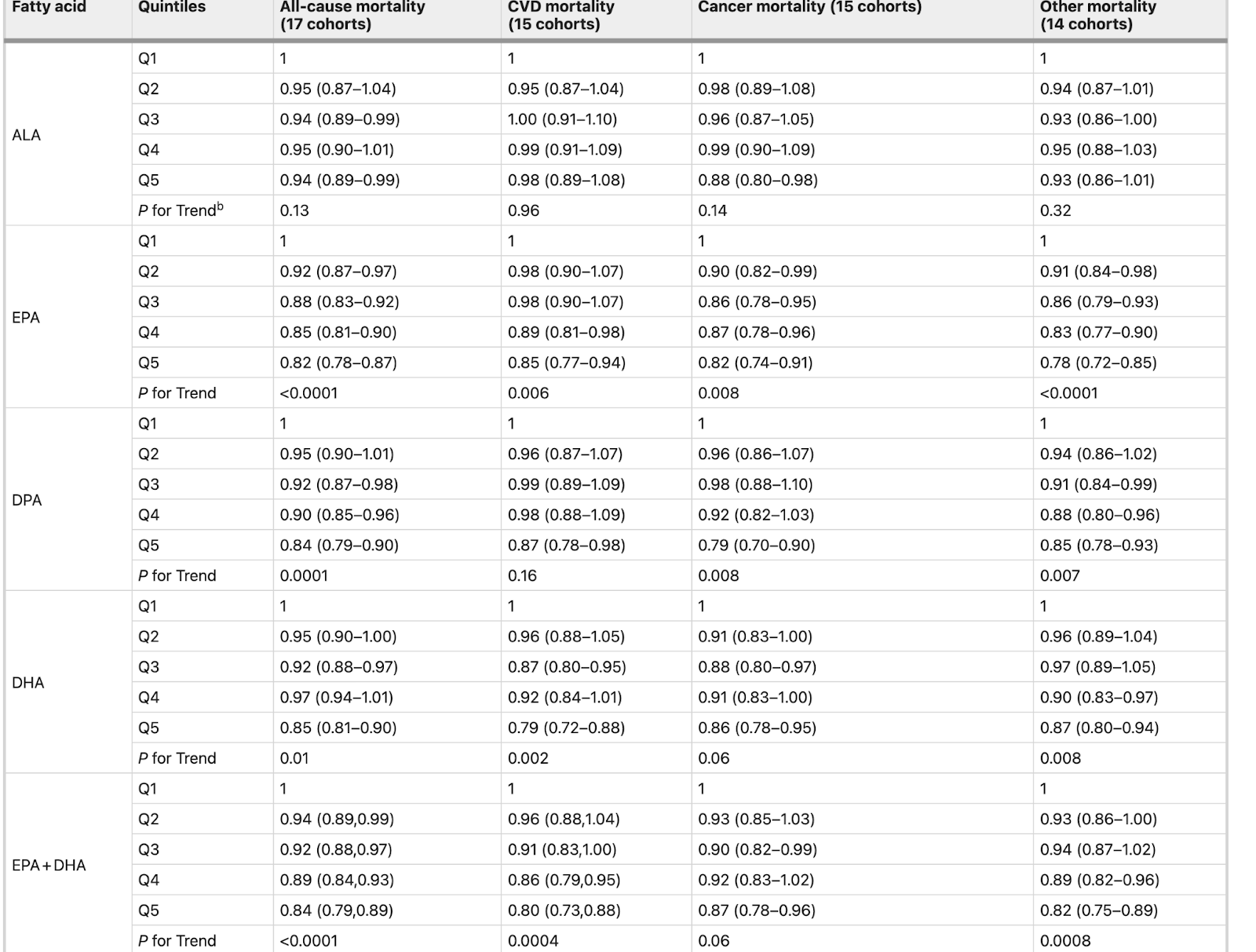
Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies, 2021
The health effects of omega-3 fatty acids have been controversial. Here we report the results of a de novo pooled analysis conducted with data from 17 prospective cohort studies examining the associations between blood omega-3 fatty acid levels and risk for all-cause mortality. Over a median of 16 years of follow-up, 15,720 deaths occurred among 42,466 individuals. We found that, after multivariable adjustment for relevant risk factors, risk for death from all causes was significantly lower (by 15–18%, at least p < 0.003) in the highest vs the lowest quintile for circulating long chain (20–22 carbon) omega-3 fatty acids (eicosapentaenoic, docosapentaenoic, and docosahexaenoic acids). Similar relationships were seen for death from cardiovascular disease, cancer and other causes. No associations were seen with the 18-carbon omega-3, alpha-linolenic acid. These findings suggest that higher circulating levels of marine n-3 PUFA are associated with a lower risk of premature death.
Introduction
The n-3 polyunsaturated fatty acid (PUFA) family has been the subject of intense investigation ever since their inverse associations with risk for acute myocardial infarction were reported in Greenland Eskimos in the 1970s1,2. The PUFAs in this family include the 18-carbon, plant-derived alpha-linolenic acid (ALA,) as well as the 20–22-carbon, long-chain (LC, mostly seafood-derived) eicosapentaenoic (EPA), docosapentaenoic (DPA), and docosahexaenoic (DHA) acids.
The efficacy of the LC n-3 PUFAs in reducing risk for cardiovascular disease (CVD) remains controversial as findings from different randomized controlled trials (RCTs) have been conflicting. Nevertheless, a 2019 meta-analysis of RCTs reported significant reductions in risk for myocardial infarction, coronary heart disease (CHD) events and mortality, and CVD mortality in patients randomized to supplemental LC n-3 PUFAs3. Another meta-analysis of observational studies found that higher levels of circulating LC n-3 PUFA levels were significantly associated with a lower risk for CHD death4. However, no meta-analysis has yet examined the relationship between LC n-3 PUFAs blood levels and risk for all-cause mortality. Indeed, the only meta-analyses to report a beneficial association with all-cause mortality were based on the self-reported intake of fish5,6. Fish contain many nutrients besides just LC n-3 PUFAs, self-reported food intake is memory dependent, food databases can be out of date, and fish meals often replace less healthful choices. As a result, studies that link LC n-3 PUFAs and health outcomes based on self-reported fish intake have potential limitations. A more reliable and objective measure of LC n-3 PUFA consumption is their level in the blood7 which is primarily determined by the consumption of preformed LC n-3 PUFAs (although synthesis from dietary ALA can make a small contribution8). Hence a clearer picture of the biological relationship between LC n-3 PUFAs and disease outcomes may be obtained from biomarker-based investigations.
Some studies have reported inverse relations between n-3 PUFA biomarkers and total mortality9,10,11, while others have not12,13. In the Cardiovascular Health Study, higher LC n-3 PUFA levels also were associated with overall “healthier aging” (i.e., surviving past age 65 free of chronic diseases and maintaining good functional status)14. However, reports from studies of individual cohorts can be limited by insufficient power and inconsistent adjustment for potential confounding factors. In addition, publication bias can distort summary conclusions. To address these challenges, the present study pooled de novo individual-level analyses across 17 prospective cohort studies in the Fatty Acid and Outcome Research Consortium (FORCE)15 to explore the associations of circulating levels of n-3 PUFAs (both plant- and seafood-derived) and all-cause mortality. Secondarily, we examined the associations with mortality from CVD, cancer, and all other causes.
Here, we show significant inverse associations for all mortality endpoints with the LC n-3 PUFA levels. Hence, chronically higher tissue levels of these FAs operating through a variety of potential mechanisms may slow the aging process.
Omega-3 Polyunsaturated Fatty Acids (PUFAs for Cancer (link)
Eicosapentaenoic acid (EPA), an omega-3 polyunsaturated fatty acid (PUFA) found in fish and fish oil, inhibits inflammation and has been associated with better weight maintenance and response to therapy, fewer complications, and improved survival in cancer patients (Murphy 2011; Gogos 1998; Jho 2004; Elia 2006; Zaid 2012).
Docosahexaenoic acid (DHA), another marine PUFA, was able to kill AML cells without harming normal blood-forming (hematopoietic) stem cells in a cell culture experiment (Yamagami 2009). Other evidence from cell culture studies shows that DHA enhances the toxic effect of imatinib on BCR-ABL-expressing human leukemia cell lines and increases arsenic trioxide-mediated apoptosis in arsenic trioxide-resistant human leukemia cells (de Lima 2007; Quesenberry 2009).
Omega-3 PUFAs, in combination with chemotherapeutic drugs and radiotherapy, have shown beneficial effects in several cancers, including leukemia(Calviello 2009; Yamagami 2009).
In a clinical trial on Rai stage 0-I CLL patients, omega-3 fatty acids, in daily doses escalating from 2.4 g to 7.2 g, suppressed activation of the inflammatory regulator NF-κB and increased sensitivity of subjects’ lymphocytes to the chemotherapeutic drug doxorubicin (Adriamycin) (Fahrmann 2013).
Long-term fatty fish consumption and renal cell carcinoma incidence in women
Context: The epidemiological evidence that fatty fish consumption may be associated with the lower risk of several cancers is not consistent and no studies of renal cell carcinoma (RCC) exist.
Objective: To examine the association between fatty and lean fish consumption and risk of RCC in women.
Design, setting, and participants: The Swedish Mammography Cohort, a population-based prospective cohort study of 61,433 women aged 40 to 76 years without previous diagnosis of cancer at baseline (March 1, 1987-December 14, 1990). Participants filled in a food frequency questionnaire at baseline and in September 1997.
Main outcome measure: Incident renal cell carcinoma.
Results: During a mean of 15.3 years (940,357 person-years) of follow-up between 1987 and 2004, 150 incident RCC cases were diagnosed. After adjustment for potential confounders, an inverse association of fatty fish consumption with the risk of RCC was found (P for trend = .02), but no association was found with lean fish consumption. Compared with no consumption, the multivariate rate ratio (RR) was 0.56 (95% confidence interval [CI], 0.35-0.91) for women eating fatty fish once a week or more. Compared with women consistently reporting no fish consumption, the multivariate RR was 0.26 (95% CI, 0.10-0.67) for those women reporting consistent consumption of fatty fish at baseline and 1997 (based on a subset of 36 664 women who filled in the baseline and 1997 questionnaires, with 40 incident RCC cases during the 1998-2004 follow-up period).
Conclusion: Our study suggests that consumption of fatty fish may reduce the occurrence of RCC in women.
Marine omega-3s do not increase the risk of bleeds, and may reduce them
Regarding safety and bleeding with omega-3s, Dr William Harris summarised the evidence nicely in a 2007 publication. The paper included patients undergoing major surgeries (2 studies were in coronary artery bypass graft patients, 2 studies in carotid endarterectomy and 15 studies in femoral artery catheterisation) and Dr Harris concluded, ‘In these studies, the risk for clinically significant bleeding was virtually nonexistent.’38 He also cites a study showing that giving pregnant women 2.7 g/day of omega-3 does not increase blood loss at delivery.39 Dr Harris concluded, ‘Thus, the experience has been virtually unanimous: omega-3 fatty acid supplements do not increase the risk for clinically significant bleeding, even in patients also being treated with antiplatelet or antithrombotic medications.’ Dr Harris considered the level of evidence supporting this notion as the highest we have in medicine (level of evidence A, from well-designed RCTs).38
A recent randomised trial further contradicts the long-held clinical assumption that omega-3 fatty acids increase risk of bleeding during and/or surgery. In the OPERA study, 1516 patients scheduled for cardiac surgery were randomly assigned to matching placebo or fish oil (EPA+DHA; 8–10 g over 2–5 days before surgery, then 2 g/day on the morning of the surgery until discharge). The omega-3 supplementation did not increase the risk of perioperative bleeding and, unexpectedly, significantly reduced the number of units of blood transfused.40 The authors concluded, ‘Higher achieved omega-3 PUFA levels were associated with lower risk of bleeding.’40
A high omega-6/omega-3 ratio increases platelet aggregation
Compared with saturated fat plus trans fat, a meta-analysis of RCTs found an increased risk of all-cause mortality, coronary heart disease mortality and cardiovascular events with omega-6 industrial seed oils.41 This may have to do with the metabolites of omega-6 PUFAs being largely proinflammatory/proaggregatory.42 Indeed, omega-3 and omega-6 PUFAs are supposed to balance each other out when they are consumed in the diet at a ratio of around 1 to 1.43 However, the increase in our omega-6/omega-3 ratio has shifted the balance into a proinflammatory/proaggregatory state. Despite LA’s ability to lower LDL levels, it can increase LDL susceptibility to oxidation and lipid peroxidation levels44 45 and hence may actually increase the risk of coronary artery disease46 as the peroxidation of LA in LDL is thought to be one of the earliest promoters of atherosclerosis. More importantly, oxidised metabolites of LA can increase thrombosis and vasoconstriction by reducing prostacyclin in the vascular wall and increasing TXA2.47 Moreover, consuming LA from industrial seed oils may even increase the susceptibility to fatal arrhythmias.48
One cross-over study compared a low-erucic acid rapeseed oil (canola oil) versus high-oleic acid sunflower oil to see if there were any differences on platelet aggregation by using oils with a high versus a low LA/ALA ratio. The canola oil provided an omega-6/omega-3 ratio of just 2.8, whereas those given the high-oleic sunflower oil were provided with an omega-6/omega-3 ratio of 28. In those provided a high omega-6/omega-3 ratio using the high-oleic sunflower oil there was an increase in platelet aggregation versus the low omega-6/omega-3 canola oil group. Platelet aggregation was also enhanced in the high-oleic sunflower oil group versus the baseline habitual diet. Thus, even a high-oleic acid omega-6 industrial seed oil may increase cardiovascular risk. The authors noted that as the omega-6 (LA) to omega-3 (ALA) ratio increased so did platelet aggregation.13
In summary, the long-chain omega-3 PUFAs EPA and DHA have antiplatelet effects, but do not increase the risk of clinically significant bleeds and may even reduce the risk of bleeding in the surgical setting, whereas the omega-6 PUFA LA has little effect on reducing platelet aggregation and in some instances may even increase platelet activation. Omega-6 industrial seed oils, as well as suboptimal intakes of marine omega-3s, may increase the risk of thrombotic cardiovascular events. This has been suggested in numerous randomised clinical studies in humans.
[NEGATIVE] Effect of High-Dose Omega-3 Fatty Acids vs Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk, November 15, 2020
The STRENGTH Randomized Clinical Trial
Question In statin-treated patients with high cardiovascular risk, high triglycerides, and low HDL cholesterol levels, does adding a carboxylic acid formulation of omega-3 fatty acids (eicosapentaenoic acid and docosahexaenoic acid) to background therapy improve cardiovascular outcomes?
Findings In this randomized clinical trial of 13 078 patients that was stopped early, daily supplementation with omega-3 fatty acids, compared with corn oil, resulted in no significant difference in a composite outcome of major adverse cardiovascular events (hazard ratio, 0.99).
Meaning These findings do not support use of this omega-3 fatty acid formulation to reduce major adverse cardiovascular events in patients with high cardiovascular risk.
Abstract
Importance It remains uncertain whether the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) reduce cardiovascular risk.
Objective To determine the effects on cardiovascular outcomes of a carboxylic acid formulation of EPA and DHA (omega-3 CA) with documented favorable effects on lipid and inflammatory markers in patients with atherogenic dyslipidemia and high cardiovascular risk.
Design, Setting, and Participants A double-blind, randomized, multicenter trial (enrollment October 30, 2014, to June 14, 2017; study termination January 8, 2020; last patient visit May 14, 2020) comparing omega-3 CA with corn oil in statin-treated participants with high cardiovascular risk, hypertriglyceridemia, and low levels of high-density lipoprotein cholesterol (HDL-C). A total of 13 078 patients were randomized at 675 academic and community hospitals in 22 countries in North America, Europe, South America, Asia, Australia, New Zealand, and South Africa.
Interventions Participants were randomized to receive 4 g/d of omega-3 CA (n = 6539) or corn oil, which was intended to serve as an inert comparator (n = 6539), in addition to usual background therapies, including statins.
Main Outcomes and Measures The primary efficacy measure was a composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, coronary revascularization, or unstable angina requiring hospitalization.
Results When 1384 patients had experienced a primary end point event (of a planned 1600 events), the trial was prematurely halted based on an interim analysis that indicated a low probability of clinical benefit of omega-3 CA vs the corn oil comparator. Among the 13 078 treated patients (mean [SD] age, 62.5 [9.0] years; 35% women; 70% with diabetes; median low-density lipoprotein [LDL] cholesterol level, 75.0 mg/dL; median triglycerides level, 240 mg/dL; median HDL-C level, 36 mg/dL; and median high-sensitivity C-reactive protein level, 2.1 mg/L), 12 633 (96.6%) completed the trial with ascertainment of primary end point status. The primary end point occurred in 785 patients (12.0%) treated with omega-3 CA vs 795 (12.2%) treated with corn oil (hazard ratio, 0.99 [95% CI, 0.90-1.09]; P = .84). A greater rate of gastrointestinal adverse events was observed in the omega-3 CA group (24.7%) compared with corn oil–treated patients (14.7%).
Conclusions and Relevance Among statin-treated patients at high cardiovascular risk, the addition of omega-3 CA, compared with corn oil, to usual background therapies resulted in no significant difference in a composite outcome of major adverse cardiovascular events. These findings do not support use of this omega-3 fatty acid formulation to reduce major adverse cardiovascular events in high-risk patients.

Marine Omega-3 Supplementation and Cardiovascular Disease: An Updated Meta-Analysis of 13 Randomized Controlled Trials Involving 127 477 Participants, 2019
This meta-analysis included study-level data from 13 trials. The outcomes of interest included myocardial infarction, coronary heart disease (CHD) death, total CHD, total stroke, CVD death, total CVD, and major vascular events. The unadjusted rate ratios were calculated using a fixed-effect meta-analysis. A meta-regression was conducted to estimate the dose–response relationship between marine omega-3 dosage and risk of each prespecified outcome. During a mean treatment duration of 5.0 years, 3838 myocardial infarctions, 3008 CHD deaths, 8435 total CHD events, 2683 strokes, 5017 CVD deaths, 15 759 total CVD events, and 16 478 major vascular events were documented. In the analysis excluding REDUCE-IT (Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial), marine omega-3 supplementation was associated with significantly lower risk of myocardial infarction (rate ratio [RR] [95% CI]: 0.92 [0.86, 0.99]; P=0.020), CHD death (RR [95% CI]: 0.92 [0.86, 0.98]; P=0.014), total CHD (RR [95% CI]: 0.95 [0.91, 0.99]; P=0.008), CVD death (RR [95% CI]: 0.93 [0.88, 0.99]; P=0.013), and total CVD (RR [95% CI]: 0.97 [0.94, 0.99]; P=0.015). Inverse associations for all outcomes were strengthened after including REDUCE-IT while introducing statistically significant heterogeneity. Statistically significant linear dose–response relationships were found for total CVD and major vascular events in the analyses with and without including REDUCE-IT.
Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis, 2021
Findings
In 149,051 participants, omega-3 FA was associated with reducing cardiovascular mortality (RR, 0.93 [0.88-0.98]; p = 0.01), non-fatal myocardial infarction (MI) (RR, 0.87 [0.81–0.93]; p = 0.0001), coronary heart disease events (CHD) (RR, 0.91 [0.87–0.96]; p = 0.0002), major adverse cardiovascular events (MACE) (RR, 0.95 [0.92–0.98]; p = 0.002), and revascularization (RR, 0.91 [0.87–0.95]; p = 0.0001). The meta-analysis showed higher RR reductions with EPA monotherapy (0.82 [0.68–0.99]) than with EPA + DHA (0.94 [0.89–0.99]) for cardiovascular mortality, non-fatal MI (EPA: 0.72 [0.62–0.84]; EPA+DHA: 0.92 [0.85–1.00]), CHD events (EPA: 0.73 [0.62–0.85]; EPA+DHA: 0.94 [0.89–0.99]), as well for MACE and revascularization. Omega-3 FA increased incident AF (RR, 1.26 [1.08–1.48]). EPA monotherapy vs. control was associated with a higher risk of total bleeding (RR: 1.49 [1.20–1.84]) and AF (RR, 1.35 [1.10–1.66]).
Interpretation
Omega-3 FAs reduced cardiovascular mortality and improved cardiovascular outcomes. The cardiovascular risk reduction was more prominent with EPA monotherapy than with EPA+DHA.
Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies
[Fish oil reduces all cause mortality. It also does double duty as an anti-clotting agent. ]
The health effects of omega-3 fatty acids have been controversial. Here we report the results of a de novo pooled analysis conducted with data from 17 prospective cohort studies examining the associations between blood omega-3 fatty acid levels and risk for all-cause mortality. Over a median of 16 years of follow-up, 15,720 deaths occurred among 42,466 individuals. We found that, after multivariable adjustment for relevant risk factors, risk for death from all causes was significantly lower (by 15–18%, at least p < 0.003) in the highest vs the lowest quintile for circulating long chain (20–22 carbon) omega-3 fatty acids (eicosapentaenoic, docosapentaenoic, and docosahexaenoic acids). Similar relationships were seen for death from cardiovascular disease, cancer and other causes. No associations were seen with the 18-carbon omega-3, alpha-linolenic acid. These findings suggest that higher circulating levels of marine n-3 PUFA are associated with a lower risk of premature death.
Associations of habitual fish oil supplementation with cardiovascular outcomes and all cause mortality: evidence from a large population based cohort study, 2020
Design Population based, prospective cohort study.
Setting UK Biobank.
Participants A total of 427 678 men and women aged between 40 and 69 who had no CVD or cancer at baseline were enrolled between 2006 and 2010 and followed up to the end of 2018.
Main exposure All participants answered questions on the habitual use of supplements, including fish oil.
Main outcome measures All cause mortality, CVD mortality, and CVD events.
Results At baseline, 133 438 (31.2%) of the 427 678 participants reported habitual use of fish oil supplements. The multivariable adjusted hazard ratios for habitual users of fish oil versus non-users were 0.87 (95% confidence interval 0.83 to 0.90) for all cause mortality, 0.84 (0.78 to 0.91) for CVD mortality, and 0.93 (0.90 to 0.96) for incident CVD events. For CVD events, the association seemed to be stronger among those with prevalent hypertension (P for interaction=0.005).
Conclusions Habitual use of fish oil seems to be associated with a lower risk of all cause and CVD mortality and to provide a marginal benefit against CVD events among the general population.
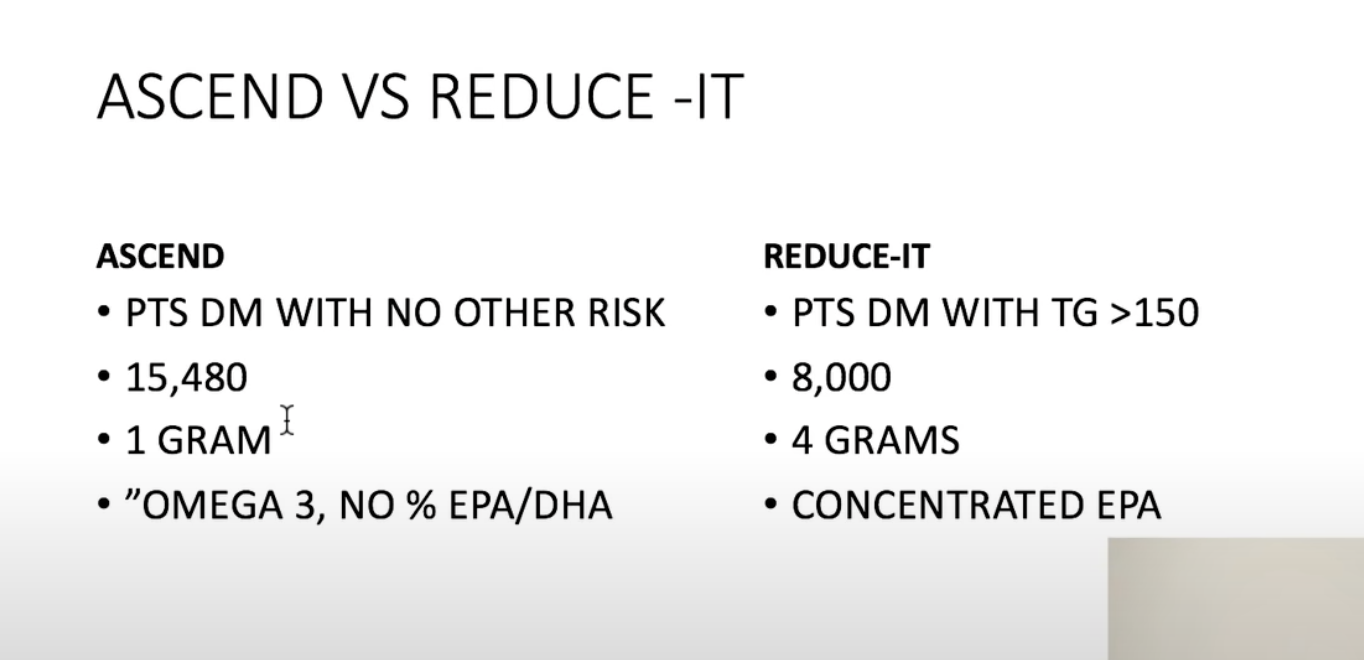
A Study of Cardiovascular Events in Diabetes - ASCEND Omega-3
https://www.acc.org/latest-in-cardiology/clinical-trials/2018/08/25/02/19/ascend-omega-3
New trial data show mixed findings for omega-3s, 2019
https://www.healio.com/news/cardiology/20190306/new-trial-data-show-mixed-findings-for-omega3s
Omega 3 (DHA) Heart & Brain Benefits | New Feb 2020 Research
https://www.youtube.com/watch?v=6RqPGCH90rQ
OMEGA-3 Fatty Acids | Massive Study September 2020
https://www.youtube.com/watch?v=W6KUNxz6eMk
(Positive result; suggests 1g w3 => 9% reduction in heart attack)
Vascepa the "Super Fish Oil" - Is it for you?
https://www.youtube.com/watch?v=XPivOwfnE0I&list=PL0TLaocCMc9yyhRML5hJ7omjbwPLrE1bT&index=8

Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis
8 645 patients with a total cholesterol of 6·5 mmol/L or greater were recruited from local physicians throughout Japan between 1996 and 1999. Patients were randomly assigned to receive either 1800 mg of EPA daily with statin (EPA group; n=9326) or statin only (controls; n=9319) with a 5-year follow-up. The primary endpoint was any major coronary event, including sudden cardiac death, fatal and non-fatal myocardial infarction, and other non-fatal events including unstable angina pectoris, angioplasty, stenting, or coronary artery bypass grafting. Analysis was by intention-to-treat.
Findings
At mean follow-up of 4·6 years, we detected the primary endpoint in 262 (2·8%) patients in the EPA group and 324 (3·5%) in controls—a 19% relative reduction in major coronary events (p=0·011). Post-treatment LDL cholesterol concentrations decreased 25%, from 4·7 mmol/L in both groups. Serum LDL cholesterol was not a significant factor in a reduction of risk for major coronary events. Unstable angina and non-fatal coronary events were also significantly reduced in the EPA group. Sudden cardiac death and coronary death did not differ between groups. In patients with a history of coronary artery disease who were given EPA treatment, major coronary events were reduced by 19% (secondary prevention subgroup: 158 [8·7%] in the EPA group vs 197 [10·7%] in the control group; p=0·048). In patients with no history of coronary artery disease, EPA treatment reduced major coronary events by 18%, but this finding was not significant (104 [1·4%] in the EPA group vs 127 [1·7%] in the control group; p=0·132).
Interpretation
EPA is a promising treatment for prevention of major coronary events, and especially non-fatal coronary events, in Japanese hypercholesterolaemic patients.
VITAL researchers announce landmark trial findings
Thanks to your commitment to taking the study capsules and filling out the health questionnaires, we now have the results of the largest and longest randomized trial of daily high-dose vitamin D (vitamin D3 [cholecalciferol], 2000 IU) and omega-3 fatty acid supplementation (Omacor® fish oil, 1 gram) for the prevention of cancer and cardiovascular disease in generally healthy men and women without these conditions at baseline. The trial included 25,871 adults—12,786 men aged 50 years and older and 13,085 women aged 55 and older—who were followed for an average of 5.3 years. All participants were monitored for the occurrence of cancer and cardiovascular events.
The results were presented by Dr. JoAnn Manson at the American Heart Association's annual meeting in Chicago, Illinois on November 10, 2018 and were concurrently published online in the New England Journal of Medicine.
Vitamin D
Cancer. During the trial, 793 cancers occurred among the 12,927 participants assigned to vitamin D, as compared with 824 cancers among the 12,944 participants assigned to vitamin D placebo, a small but nonsignificant reduction. Supplemental vitamin D also did not reduce the occurrence of breast, prostate, or colorectal cancers. However, there was a suggestive 17% reduction in cancer deaths, which became a 25% reduction in analyses that excluded the first two years of follow-up. Excluding early follow-up is a common practice in analyzing data from trials of dietary supplements and cancer because effects of nutritional factors on risk of cancer, a slow-developing disease, typically become clear only after several years.
Although vitamin D did not significantly lower the risk of developing cancer in the total study population, African Americans assigned to vitamin D did experience a suggestive 23% reduction in cancer risk. However, further research is needed to confirm this finding.
Cardiovascular disease. A total of 396 major cardiovascular events—heart attack, stroke, or death from cardiovascular causes—occurred among participants in the vitamin D group, as compared with 409 in the placebo group, a small but nonsignificant reduction. Supplemental vitamin D also did not reduce the occurrence of heart attack, stroke, or cardiovascular death, considered individually, nor did it reduce the risk of death from any cause.
Side effects. There were few side effects of high-dose vitamin D. No significant increases in risk of hypercalcemia (high blood calcium level), kidney stones, or gastrointestinal symptoms were observed.
Clinical perspective. The findings indicate that high-dose vitamin D does not lower the risk of developing cancer or cardiovascular disease in generally healthy men and women, although it appears to lower the risk of cancer death. "The promising results for cancer mortality need to be confirmed in extended follow-up of the study participants and in future trials," said Dr. Manson. "Although our study shows that a vitamin D dose of 2000 IU per day is well tolerated, with few if any side effects, the results do not strongly support the initiation of high-dose vitamin D for prevention of cancer or cardiovascular disease in healthy patients who already meet vitamin D requirements for bone health." National guidelines for vitamin D intake from food and/or supplements recommend 600 IU per day for adults up to age 70 and 800 IU per day for those aged 71 and older. (See Q&A below for additional comments.)
Omega-3 fatty acids
Cardiovascular disease. During the trial, 386 major cardiovascular disease events occurred among the 12,933 participants receiving omega-3 fatty acids, as compared with 419 such events among the 12,938 participants receiving placebo, an 8% reduction that was not significant. Upon closer examination, this result was due almost entirely to a reduction in heart attacks without a reduction in strokes. Specifically, the omega-3 fatty acid intervention lowered the risk of heart attack by 28% and the risk of fatal heart attack by 50% but had no benefit on stroke or cardiovascular deaths not related to heart disease. Additionally, omega-3 fatty acids reduced the rate of angioplasty procedures by 22%.
Cancer. A total of 820 cancers occurred among participants in the omega-3 fatty acid group, as compared with 797 in the placebo group, a small but nonsignificant difference. Omega-3 fatty acid supplementation did not reduce the occurrence of breast, prostate, or colorectal cancers, cancer-related deaths, or deaths from any cause. In analyses excluding early follow-up (see vitamin D discussion above), supplementation was associated with a slight but nonsignificant increase in risk of cancer and had no effect on cancer death.
Side Effects. The omega-3 fatty acid intervention was well tolerated, with no increase in bleeding or gastrointestinal symptoms observed in those assigned to the active supplement.
Subgroup findings. The most consistent cardiovascular benefits of supplemental omega-3 fatty acids were found in participants who reported low fish intake at baseline and in African Americans. In participants with low fish consumption (defined as less than 1½ servings per week; one serving is 3-4 ounces), omega-3 fatty acid supplementation led to a 19% reduction in major cardiovascular events, including a 40% reduction in heart attack, as well as a trend toward a reduction in death from any cause, and no indication of increased cancer risk. In contrast, for participants with higher fish consumption (at least 1½ servings per week), omega-3 fatty acids did not protect against cardiovascular events, including heart attacks, or death from any cause, and there was a suggestive increase in cancer risk. Among African Americans, omega-3 fatty acid supplementation led to a 77% reduction in heart attacks, and a benefit was observed regardless of level of fish intake. Some of these findings may have been due to chance and should not be viewed as conclusive.
Clinical perspective. "The results indicate that people with low dietary intake of fish will likely obtain a heart benefit from omega-3 fatty acid supplementation," said Dr. Manson. "On the other hand, those with higher fish consumption do not appear to benefit, perhaps because they are already meeting their omega-3 requirements by eating fish. This pattern of results implies that, while a modest amount of fish oil is desirable, more may not necessarily be better." She added, "Additional research is needed to confirm the strong heart protection seen in African Americans and to determine whether there are other groups who might benefit from omega-3 therapy. People considering the use of omega-3 fatty acids to prevent heart disease must weigh the overall balance of benefits and risks." (See Q&A below for additional comments.)
Key findings
Vitamin D supplementation
• Did not reduce risk of cancer
• Did not reduce risk of major cardiovascular events (heart attack, stroke, or cardiovascular death considered together)
• Appeared to reduce risk of cancer-related death
Omega-3 fatty acid supplementation
• Did not reduce risk of cancer
• Did not reduce risk of major cardiovascular events in the overall study population, but did reduce risk of these events by 19% in people with low fish intake
• Reduced risk of heart attack by 28%, when heart attack was considered separately from other cardiovascular events; the benefit appeared strongest in African Americans
Fish oil prevents breast cancer cell metastasis to bone, 2010
The data derived from epidemiological and animal models confirm a beneficial effect of fish oil (rich in ω-3 polyunsaturated fatty acids) in the amelioration of tumor growth and progression, including breast cancer. The breast cancer patients often develop bone metastasis evidenced by osteolytic lesions, leading to severe pain and bone fracture. Using a mouse model of MDA-MB-231 human breast cancer cell metastasis to bone, here we show that fish oil diet enriched in DHA (docosahexaenoic acid) and EPA (eicosapentaenoic acid) prevents the formation of osteolytic lesions in bone, indicating suppression of cancer cell metastasis to bone. These results are supported by our data showing both DHA and EPA significantly attenuate the migration/invasion of MDA-MB-231 breast cancer cells in culture. The mechanism that limits breast cancer cells to selective metastasis to bone remains hitherto unexplored. Aberrant increased expression of CD44 is associated with generation of cancer stem cells, which contribute to metastasis of breast cancer cells. We demonstrate that DHA and EPA significantly inhibit the expression of CD44 protein and mRNA by a transcriptional mechanism. Furthermore, we show markedly reduced levels of CD44 mRNA and protein in the tumors of mice, which were fed fish oil diet than those in control diet. Our data provide the first evidence for a salutary effect of fish oil on breast cancer metastasis to bone. Our results identify a novel function of the fish oil active components, DHA and EPA, which target the cell-intrinsic pro-metastatic molecule CD44 to inhibit migration/invasion.
An omega-3 that's poison for tumors (link)
The poison acts on tumour cells via a phenomenon called ferroptosis, a type of cell death linked to the peroxidation of certain fatty acids. The greater the amount of unsaturated fatty acids in the cell, the greater the risk of their oxidation. Normally, in the acidic compartment within tumours, cells store these fatty acids in lipid droplets, a kind of bundle in which fatty acids are protected from oxidation. But in the presence of a large amount of DHA, the tumour cell is overwhelmed and cannot store the DHA, which oxidises and leads to cell death. By using a lipid metabolism inhibitor that prevents the formation of lipid droplets, researchers were able to observe that this phenomenon is further amplified, which confirms the identified mechanism and opens the door to combined treatment possibilities.
Fish Oil and Cancer
https://www.cancertherapyadvisor.com/home/tools/fact-sheets/fish-oil-and-cancer/
Omega-3 Fatty Acids and Cancer Cell Cytotoxicity: Implications for Multi-Targeted Cancer Therapy
Cancer is a major disease worldwide. Despite progress in cancer therapy, conventional cytotoxic therapies lead to unsatisfactory long-term survival, mainly related to development of drug resistance by tumor cells and toxicity towards normal cells. n-3 polyunsaturated fatty acids (PUFAs), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), can exert anti-neoplastic activity by inducing apoptotic cell death in human cancer cells either alone or in combination with conventional therapies. Indeed, n-3 PUFAs potentially increase the sensitivity of tumor cells to conventional therapies, possibly improving their efficacy especially against cancers resistant to treatment. Moreover, in contrast to traditional therapies, n-3 PUFAs appear to cause selective cytotoxicity towards cancer cells with little or no toxicity on normal cells. This review focuses on studies investigating the cytotoxic activity of n-3 PUFAs against cancer cells via apoptosis, analyzing the molecular mechanisms underlying this effective and selective activity. Here, we highlight the multiple molecules potentially targeted by n-3 PUFAs to trigger cancer cell apoptosis. This analysis can allow a better comprehension of the potential cytotoxic therapeutic role of n-3 PUFAs against cancer, providing specific information and support to design future pre-clinical and clinical studies for a better use of n-3 PUFAs in cancer therapy, mainly combinational therapy.
Fish Oil Supplementation in Adults With Hematological Malignancies, 2018
Participants were adults with newly diagnosed leukemia or lymphoma who were about to initiate first-line treatment with chemotherapy. The total population analyzed was 22 individuals (10 women, 12 men). There were no statistically significant differences in characteristics of the participants at baseline, including age, which averaged 53.8 years in the control group and 43.8 years in the fish oil group.
Diagnoses included acute leukemia (n=9), non-Hodgkin lymphoma (n=8), Hodgkin lymphoma (n=4), and chronic leukemia (n=1).
Participants were randomized to receive oral fish oil at a dose of 2 g per day (containing 367 mg eicosapentaenoic acid [EPA] and 243 mg docosahexaenoic acid [DHA]) for 9 weeks, starting on the first day of chemotherapy, or no fish oil (control group). The intervention group was instructed to consume the fish oil 20 to 30 minutes before lunch or dinner.
There were no deaths in the 14-month follow up in the fish oil group. There were 8 deaths in the control group in model 1 and 6 deaths in model 2; these differences were statistically significant compared to the fish oil group (P=0.005 and P=0.008, respectively). The number of chemotherapy sessions was significantly higher in the fish oil group in both models compared to the control group. There was no difference in hospital readmissions. There were no significant changes in weight, MUAC, MUAMC, or TS with either model.
In summary, fish oil supplementation increased plasma EPA and DHA. Survival was significantly better in the fish oil vs control group at 14 months, and the fish oil group received more chemotherapy sessions than the control group. Improvement in CAR was greater in the fish oil group compared to the control group at 9 weeks.
Effects of the polyunsaturated fatty acids, EPA and DHA, on hematological malignancies: a systematic review
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5837752/
Fish Oil–Rich Diet Promotes Hematopoiesis and Alters Hematopoietic Niche
The self-renewal and differentiation of hematopoietic stem cells (HSCs) in bone marrow are essential to replenish all blood cell types, but how this process is influenced by diet remains largely unclear. Here we show that a diet rich in fish oils promotes self-renewal of HSCs and extramedullary hematopoiesis. Chronic intake of a fish oil–rich diet increases the abundance of HSCs, alters the hematopoietic microenvironment, and, intriguingly, induces the expression of matrix metalloproteinase 12 (MMP12) in the bone marrow. Pointing to a direct effect of fish oil on MMP12 expression, omega-3 polyunsaturated fatty acids induce the expression of MMP12 in a dose-dependent manner in bone marrow cells. Importantly, down-regulation of MMP12 activity using an MMP12-specific inhibitor attenuates diet-induced myelopoiesis in both bone marrow and spleen. Thus, a fish oil–rich diet promotes hematopoiesis in the bone marrow and spleen, in part via the activity of MMP12. Taken together, these data provide new insights into diet-mediated regulation of hematopoiesis.
Fish Oil–Rich Diet Promotes Hematopoiesis and Alters Hematopoietic Niche
The self-renewal and differentiation of hematopoietic stem cells (HSCs) in bone marrow are essential to replenish all blood cell types, but how this process is influenced by diet remains largely unclear. Here we show that a diet rich in fish oils promotes self-renewal of HSCs and extramedullary hematopoiesis. Chronic intake of a fish oil–rich diet increases the abundance of HSCs, alters the hematopoietic microenvironment, and, intriguingly, induces the expression of matrix metalloproteinase 12 (MMP12) in the bone marrow. Pointing to a direct effect of fish oil on MMP12 expression, omega-3 polyunsaturated fatty acids induce the expression of MMP12 in a dose-dependent manner in bone marrow cells. Importantly, down-regulation of MMP12 activity using an MMP12-specific inhibitor attenuates diet-induced myelopoiesis in both bone marrow and spleen. Thus, a fish oil–rich diet promotes hematopoiesis in the bone marrow and spleen, in part via the activity of MMP12. Taken together, these data provide new insights into diet-mediated regulation of hematopoiesis.
Omega 3 fatty acids reduce myeloid progenitor cell frequency in the bone marrow of mice and promote progenitor cell differentiation
Background
Omega 3 fatty acids have been found to inhibit proliferation, induce apoptosis, and promote differentiation in various cell types. The processes of cell survival, expansion, and differentiation are of key importance in the regulation of hematopoiesis. We investigated the role of omega 3 fatty acids in controlling the frequency of various myeloid progenitor cells in the bone marrow of mice. Increased progenitor cell frequency and blocked differentiation are characteristics of hematopoietic disorders of the myeloid lineage, such as myeloproliferative diseases and myeloid leukemias.
Results
We found that increasing the proportion of omega 3 fatty acids relative to the proportion of omega 6 fatty acids in the diet caused increased differentiation and reduced the frequency of myeloid progenitor cells in the bone marrow of mice. Furthermore, this had no adverse effect on peripheral white blood cell counts.
Conclusion
Our results indicate that omega 3 fatty acids impact hematopoietic differentiation by reducing myeloid progenitor cell frequency in the bone marrow and promoting progenitor cell differentiation. Further exploration of this discovery could lead to the use of omega 3 fatty acids as a therapeutic option for patients that have various disorders of hematopoiesis.
Vitamin D and Omega-3 Trial - VITAL
https://www.acc.org/latest-in-cardiology/clinical-trials/2018/11/08/22/42/vital
The results of this trial indicate that supplementation with either n–3 fatty acid at a dose of 1 g/day or vitamin D3 at a dose of 2000 IU/day was not effective for primary prevention of CV or cancer events among healthy middle-aged men and women over 5 years of follow-up.
Consumption of Fish Oil Providing Amounts of Eicosapentaenoic Acid and Docosahexaenoic Acid That Can Be Obtained from the Diet Reduces Blood Pressure in Adults with Systolic Hypertension: A Retrospective Analysis
Background: Although many randomized controlled trials (RCTs) have examined the effects of the n-3 (ω-3) fatty acids eicosapentaenoic acid (EPA; 20:5n-3) and docosahexaenoic acid (DHA; 22:6n-3) on blood pressure (BP) and vascular function, the majority have used doses of EPA+DHA of >3 g/d, which are unlikely to be achieved by dietary manipulation.
Objective: The objective was to examine, by using a retrospective analysis from a multicenter RCT, the impact of recommended EPA+DHA intakes achievable through diet on systolic and diastolic BPs and microvascular function in adults in the United Kingdom.
Methods: In a double-blind, placebo-controlled RCT, healthy men and women (n = 312) consumed a control oil or fish oil (FO) providing 0.7 or 1.8 g EPA+DHA/d, in random order, each for 8 wk. Fasting BP and microvascular function (using laser Doppler iontophoresis) were assessed and plasma collected for the quantification of markers of vascular function. Participants were retrospectively genotyped for the endothelial nitric oxide synthase (eNOS) rs1799983 variant.
Results: No effects of n-3 fatty acid treatment or any treatment × eNOS genotype interactions were evident in the group as a whole for any of the clinical or biochemical outcomes. Assessment of response according to hypertension status at baseline indicated a significant (P = 0.046) FO-induced reduction (mean: 5 mm Hg) in systolic BP, specifically in those with isolated systolic hypertension (n = 31). No dose response was observed.
Conclusions: These findings indicate that in adults with isolated systolic hypertension, daily doses of EPA+DHA as low as 0.7 g show clinically meaningful BP reductions, which, at a population level, could be associated with lower cardiovascular disease risk. Confirmation of findings in an RCT in which participants are prospectively recruited on the basis of BP status is required to draw definite conclusions.
Associations of Fish Oil Supplement Use With Testicular Function in Young Men
Importance Many young men have poor semen quality, and the causes are often unknown. Supplement intake of ω-3 polyunsaturated fatty acid has been found to improve semen quality among men with infertility, but the association with semen quality among healthy men is unknown.
Objective To determine if intake of ω-3 fatty acid supplements is associated with testicular function as measured by semen quality and reproductive hormone levels among healthy men.
Design, Setting, and Participants This cross-sectional study included young Danish men from the general population recruited between January 1, 2012, and December 31, 2017, at compulsory examinations to determine their fitness for military service. Young unselected men were approached after the examination and invited to participate in a study of reproductive function, regardless of their fitness for military service. Data analysis was conducted from September 1, 2018, to June 30, 2019.
Exposures Intake of supplements, including fish oil, during the past 3 months.
Main Outcomes and Measures Semen quality, measured as volume, concentration, total sperm count, percentage of morphologically normal spermatozoa, and motility, and serum reproductive hormone levels, measured as follicle-stimulating hormone, luteinizing hormone, testosterone, free testosterone, and inhibin B levels.
Results Among 1679 young Danish men (median [interquartile range] age, 18.9 [18.7-19.4] years) recruited to participate, 98 men (5.8%) reported use of fish oil supplements during the past 3 months, of whom 53 (54.1%) reported intake on 60 or more days. After adjustment and compared with men with no supplement intake, men with fish oil supplement intake on fewer than 60 days had semen volume that was 0.38 (95% CI, −0.03 to 0.80) mL higher, and men with fish oil supplement intake on 60 or more days had semen volume that was 0.64 (95% CI, 0.15 to 1.12) mL higher (P for trend < .001). Similarly, testicular size in men with supplement intake on fewer than 60 days was 0.8 (95% CI, −0.2 to 1.9) mL larger and in men with fish oil supplement intake on 60 or more days was 1.5 (95% CI, 0.2 to 2.8) mL larger compared with men with no supplement intake (P for trend = .007). After adjustment, men with fish oil supplement intake had a 20% (95% CI, 9%-31%) lower follicle-stimulating hormone level and 16% (95% CI, 8%-24%) lower luteinizing hormone level compared with men with no supplement intake. There were no associations of intake of other supplements with measures of testicular function.
Conclusions and Relevance These findings suggest that intake of fish oil supplements was associated with better testicular function, which is less likely to be due to confounding by indication, as no associations of intake of other supplements with testicular function were found. This cross-sectional study did not examine the actual content of ω-3 fatty acids in the supplements; therefore, these findings need confirmation in well-designed randomized clinical trials among unselected men.
Dr. Rhonda Patrick’s fish oil stack, take 2 capsules daily of Nordic Natural ProOmega 2000, and 4 capsules of Nordic Naturals Phospholipids. This will put you in the 5-6 gram daily range – and by taking it in triglyceride and phospholipid form, you will be able to reap the full benefits of Omega-3 fish oil like Dr. Patrick.
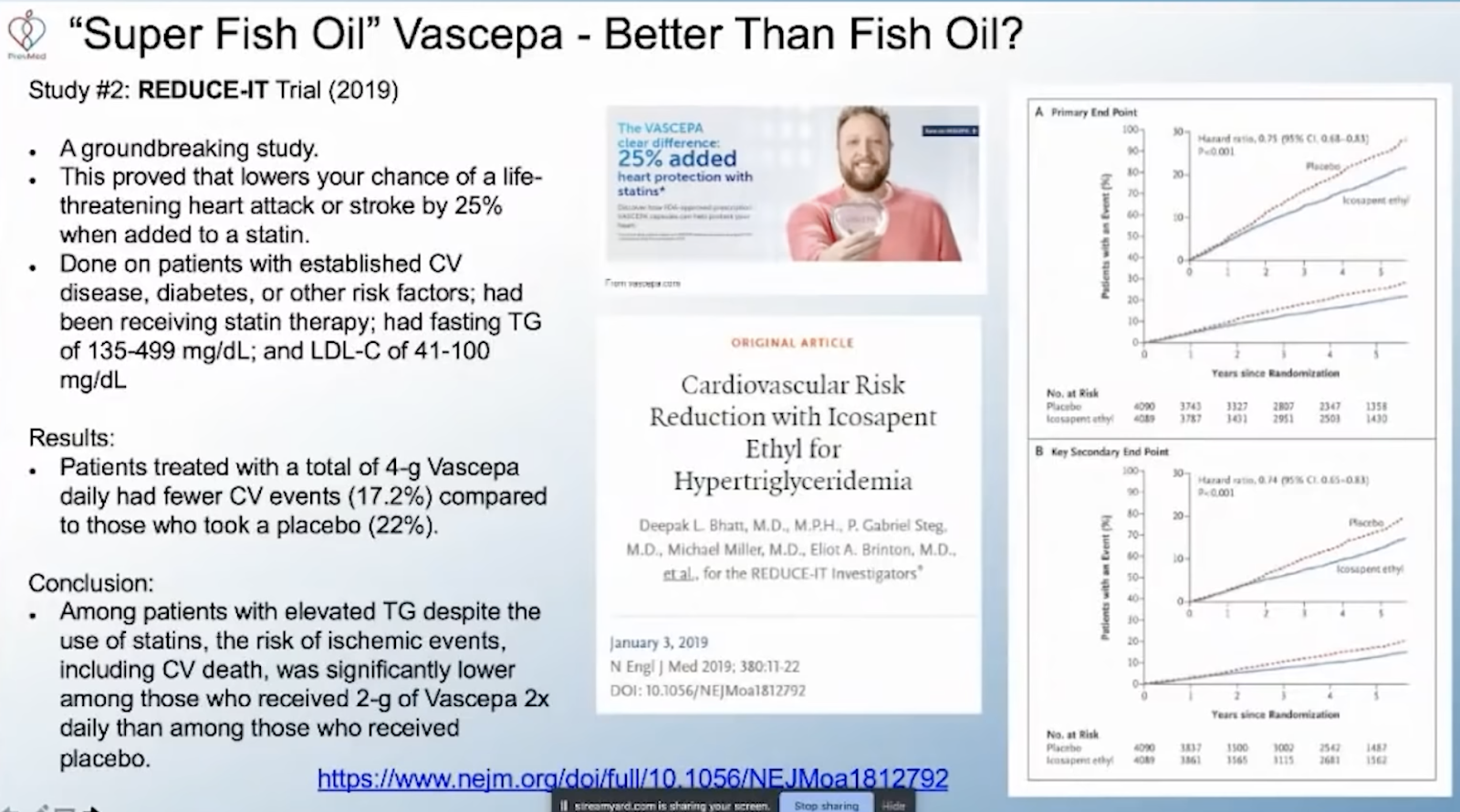
REDUCE-IT USA: Results From the 3146 Patients Randomized in the United States. 2020
Background:
Some trials have found that patients from the United States derive less benefit than patients enrolled outside the United States. This prespecified REDUCE-IT (Reduction of Cardiovascular Events with Icosapent Ethyl - Intervention Trial) subgroup analysis was conducted to determine the degree of benefit of icosapent ethyl in the United States.
Methods:
REDUCE-IT randomized 8179 statin-treated patients with qualifying triglycerides ≥135 and <500 mg/dL and low-density lipoprotein cholesterol >40 and ≤100 mg/dL and a history of atherosclerosis or diabetes mellitus to icosapent ethyl 4 g/d or placebo. The primary composite end point was cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, coronary revascularization, or hospitalization for unstable angina. The key secondary composite end point was cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. A hierarchy was prespecified for examination of individual and composite end points.
Results:
A total of 3146 US patients (38.5% of the trial) were randomized and followed for a median of 4.9 years; 32.3% were women and 9.7% were Hispanic. The primary composite end point occurred in 24.7% of placebo-treated patients versus 18.2% of icosapent ethyl-treated patients (hazard ratio [HR], 0.69 [95% CI, 0.59–0.80]; P=0.000001); the key secondary composite end point occurred in 16.6% versus 12.1% (HR, 0.69 [95% CI, 0.57–0.83]; P=0.00008). All prespecified hierarchical end points were meaningfully and significantly reduced, including cardiovascular death (6.7% to 4.7%; HR, 0.66 [95% CI, 0.49–0.90]; P=0.007), myocardial infarction (8.8% to 6.7%; HR, 0.72 [95% CI, 0.56–0.93]; P=0.01), stroke (4.1% to 2.6%; HR, 0.63 [95% CI, 0.43–0.93]; P=0.02), and all-cause mortality (9.8% to 7.2%; HR, 0.70 [95% CI, 0.55–0.90]; P=0.004); for all-cause mortality in the US versus non-US patients, Pinteraction=0.02. Safety and tolerability findings were consistent with the full study cohort.
Conclusions:
Whereas the non-US subgroup showed significant reductions in the primary and key secondary end points, the US subgroup demonstrated particularly robust risk reductions across a variety of individual and composite end points, including all-cause mortality.
Yuri Granik: 4 to 6 g of fish oil daily.
Anne Mitchell Murphy
I wondered if I was maybe overdoing the supplements. I bled like crazy for 15 minutes after poking my finger and I always fill the bag really fast at the blood bank. Yes, my index was pretty high at 10.9%, so I am cutting back a little. Anything above 8 is considered desirable. I also eat fish weekly. I take about 2200 mg of EPA & DHA a day
Omega-3 Index and Cardiovascular Health
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3942733/

Methotrexate Is a JAK/STAT Pathway Inhibitor
A 2015 paper scanned 2000 drugs and natural molecules to discover new JAK/STAT inhibitors. . I quickly skimmed through. Found the following as the most interesting. Looks like Vit A in various forms suppress JAK/STAT. So does Fish Oil. So does Hydrea :) (effect not as significant as top molecules). They have 4 "z scores" from 4 experiments, then the right-most number is their average.
01500143 beta-CAROTENE 100122-04 F02 sample 7235-40-7 C40H56 536.89232 provitamin A provitamin A; widespread in plants and animals USP, INN -7.36 -1.96 -1.78 -0.40 -2.87
01300030 OMEGA-3-ACID ESTERS (EPA shown) 100122-15 D02 sample 86227-47-6 C22H34O2 330.51508 hypolipidemic semisynthetic; K-85 USAN -5.26 -1.61 -1.50 -1.19 -2.39
01500344 HYDROXYUREA 100122-06 E06 sample 127-07-1 CH4N2O2 76.05523 antineoplastic, inhibits ribonucleoside diphosphate reductase synthetic USP, INN, BAN -4.05 -1.04 -2.79 -1.43 -2.32
01300027 IVERMECTIN 100122-04 B02 sample 70288-86-7 C48H74O14 875.11658 antiparasitic semisynthetic USP, INN, BAN Science 221:823 (1983); J Vet Pharmacol Ther 7:1 (1984) -9.09 -4.82 -3.73 -2.40 -5.01
01503604 RETINYL PALMITATE 100122-10 E04 sample 79-81-2 C36H60O2 524.8784 provitamin, antixerophthalamic semisynthetic; Vitamin A palmitate USP, JAN -9.56 -0.62 -0.83 -0.54 -2.88
01505444 METHYLENE BLUE 100122-12 B05 sample 7220-79-3 C16H20ClN3OS 337.8743 antimethemoglobinemic, cyanide antidote synthetic USP, INN, BAN -3.22 -3.83 -4.25 -2.67 -3.49
01504300 ORLISTAT 100122-11 C02 sample 96829-58-2 C29H53NO5 495.74946 reversible lipase inhibitor, antiobesity synthetic USAN, INN, BAN -4.16 -3.71 -2.26 -1.68 -2.95
01503968 TACROLIMUS 100122-10 H02 sample 109581-93-3, 104987-11-3
[anhydrous]
C44H69NO12 804.04003 immune suppressant, antifungal Streptomyces tsukubaensis USAN, INN, BAN, JAN -9.14 -3.31 -3.47 -2.82 -4.68
01500398 METHOTREX
ATE(+/-) 100122-01 B06 sample 60388-53-6 C20H22N8O5 454.44894 antineoplastic, antirheumatic, folic acid antagonist synthetic; AMETHOPTERIN US
P, INN, BAN, JAN -8.26 -9.36 -8.49 -8.77 -8.72
01500679 AMINOPTERIN 100122-14 A10 sample 54-62-6, 58602-66-7
[aminopterin sodium]
C19H20N8O5 440.42185 antineoplastic, antirheumatic, folic acid antagonist synthetic; NSC-739 INN, BAN -6.65 -7.74 -7.80 -10.61 -8.20
00100009 CEDRELONE 100122-17 B09 sample 1254-85-9 C26H30O5 422.526 Cedrela species undetermined activity J Chem Soc 1963: 2506, 2515 -21.11 -9.87 -6.22 -3.16 -10.09
01504094 TENIPOSIDE 100122-03 C03 sample 29767-20-2 C32H32O13S 656.66804 antineoplastic semisynthetic USAN, INN, BAN -9.31 -11.19 -13.15 -12.42 -11.51
01505708 EPIRUBICIN HYDROCHLORIDE 100122-12 H02 sample 56390-09-1 C27H30ClNO11 579.99325 antineoplastic synthetic; IMI-28 USAN, INN, BAN, JAN -11.12 -16.09 -12.37 -5.86 -11.36
01503904 PATULIN 100122-18 C03 sample 149-29-1 C7H6O4 154.12347 antibacterial Aspergillus clavatus, Penicillium patulum experimental J Chem Soc 1944: 415 -13.10 -12.18 -8.02 -5.32 -9.65
01500835 URSOCHOLANIC ACID 100122-21 A04 sample 546-18-9 C24H40O2 360.5852 Abrus pecatorius undetermined activity Steroids 23:357 (1974) -12.11 -4.31 -2.60 -3.50 -5.63
00100005 ANTHOTHECOL 100122-17 B08 sample 10410-83-0 C28H32O7 480.56304 also as 11-ACETOXYCEDRELONE undetermined activity J Chem Soc 1963:983; 1970: 205; Nature 207:1101(1965) -16.35 -24.62 -23.30 -13.70 -19.49
01505483 DOXORUBICIN 100122-12 D03 sample 23214-92-8 C27H29NO11 543.53228 antineoplastic semisynthetic USAN, INN, BAN -7.58 -9.64 -6.87 -3.89 -6.99
01504412 PODOPHYLLIN ACETATE 100122-17 B06 sample 1180-34-3 C24H24O9 456.45348 derivative undetermined activity -8.29 -7.27 -9.07 -8.36 -8.25
01503076 QUINAPRIL HYDROCHLORIDE 100122-09 E10 sample 82586-55-8, 85441-61-8
[quinapril]
C25H31ClN2O5 474.98922 antihypertensive, ACE inhibitor synthetic USP, INN, BAN -8.06 -1.88 -0.42 -0.39 -2.69
An omega-3 fatty acid plasma index ≥4% prevents progression of coronary artery plaque in patients with coronary artery disease on statin treatment
Background and aims
Higher blood levels of the omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), have been associated with fewer cardiovascular events and lower mortality in prospective studies. Our aim was to determine a target level of EPA and DHA to prevent progression of coronary artery plaque.
Methods
218 subjects with stable coronary artery disease on statins were randomized to highdose EPA and DHA (3.36 g daily) or no omega-3 for 30 months. Coronary plaque volume was measured by coronary computed tomographic angiography. Plasma phospholipid levels of EPA, DHA and total fatty acids were measured by gas chromatography mass spectrometry. The omega-3 fatty acid index was calculated as EPA+DHA/total fatty acid.
Results
Mean (SD) age was 62.9 (7.8) years; mean (SD) LDL-C level 78.6 (27.3) mg/dL and median triglyceride level 122 mg/dL. Subjects assigned to EPA and DHA had increased plasma EPA and DHA levels variably from 1.85% to 13.02%. Plasma omega-3 fatty acid index ≥4% prevented progression of fibrous, noncalcified, calcified and total plaque in nondiabetic subjects whereas those in the lowest quartile (<3.43%) had significant progression of fibrous, calcified and total plaque. No difference was observed in diabetic subjects.
Conclusions
EPA and DHA added to statins prevented coronary plaque progression in nondiabetic subjects with mean LDL-C <80 mg/dL, when an index ≥4% was achieved. Low omega-3 index <3.43% identified nondiabetic subjects at risk of coronary plaque progression despite statin therapy. These findings highlight the importance of measuring plasma levels of omega-3 fatty acids early and at trial conclusion. Targeting an omega-3 index ≥4% maximizes cardiovascular benefit.
High Fish plus Fish Oil Intake Is Associated with Slightly Reduced Risk of Venous Thromboembolism: The Tromsø Study, 2014
Current knowledge of the effect of fish consumption on risk of venous thromboembolism (VTE) is scarce and diverging. Therefore, the purpose of the present study was to investigate the impact of fish consumption and fish oil supplements on the risk of VTE in a population-based cohort. Weekly intake of fish for dinner and intake of fish oil supplements during the previous year were registered in 23,621 persons aged 25–97 y who participated in the Tromsø Study from 1994 to 1995. Incident VTE events were registered throughout follow-up (31 December 2010). Cox-regression models were used to calculate HRs for VTE, adjusted for age, body mass index, sex, triglycerides, HDL cholesterol, physical activity, and education level. During a median of 15.8 y of follow-up there were 536 incident VTE events. High fish consumption was associated with a slightly reduced risk of VTE. Participants who ate fish ≥3 times/wk had 22% lower risk of VTE than those who consumed fish 1–1.9 times/wk (multivariable HR: 0.78; 95% CI: 0.60, 1.01; P= 0.06). The addition of fish oil supplements strengthened the inverse association with risk of VTE. Participants who consumed fish ≥3 times/wk who additionally used fish oil supplements had 48% lower risk than those who consumed fish 1–1.9 times/wk but did not use fish oil supplements (HR: 0.52; 95% CI: 0.34, 0.79; P= 0.002). In conclusion, a high weekly intake (≥3 times/wk) of fish was associated with a slightly reduced risk of VTE, and the addition of fish oil supplements strengthened the inverse effect.
Effects of Omega-3 Fatty Acid in Nonalcoholic Fatty Liver Disease: A Meta-Analysis, 2016
577 cases of NAFLD/NASH in ten randomized controlled trials (RCTs) were included. The results of the meta-analysis showed that benefit changes in liver fat favored PUFA treatment, and it was also beneficial for GGT, but it was not significant on ALT, AST, TC, and LDL. Conclusions. In this meta-analysis, omega-3 PUFAs improved liver fat, GGT, TG, and HDL in patients with NAFLD/NASH. Therefore, n-3 PUFAs may be a new treatment option for NAFLD.
ALT showed a trend toward PUFA therapy versus control on ALT but did not reach statistical significance (MD = −4.97, 95% CI: −11.14 to 1.20, P = 0.11)
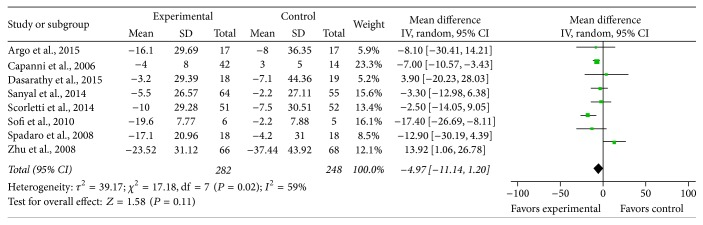
AST (MD = −2.01, 95% CI: −8.72 to 4.70, P = 0.58)
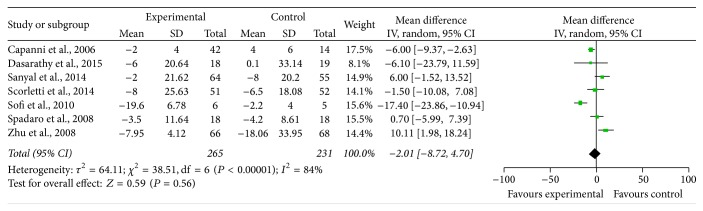
GGT (MD = −9.02, 95% CI: −14.80 to −3.24, P = 0.002)

Triglyceride. (MD = −35.55, 95% CI: −53.90 to -17.19, P = 0.0001)
HDL (MD = 5.51, 95% CI: 0.03 to 11, P = 0.05)
A systematic review of fish-oil supplements for the prevention and treatment of hypertension, 2013
Results: We included 17 studies, with a total of 1524 participants. We explored the effects of fish-oil supplements in both normotensive and hypertensive participants with BP 140/85 mmHg at least. Meta-analyses were performed using the inverse-variance method. Data from eight studies in hypertensive participants found a statistically significant reduction in systolic and diastolic BP; 2.56 mmHg (95% CI 0.58 to 4.53) and 1.47 mmHg (95% CI 0.41 to 2.53), respectively. Nine studies in normotensive participants showed a non-significant reduction in both systolic and diastolic BP. Meta-regression showed no significant relationship between dose of fish oil and the effect on BP.




Comments